susen george thiess
DESCRIPTION
EFFECTIVENESS OF SITZ BATH VERSUS INFRAREDLAMP THERAPY ON EPISIOTOMY PAIN AND WOUNDHEALING AMONG POSTNATAL MOTHERSTRANSCRIPT
A COMPARATIVE STUDY TO ASSESS THE
EFFECTIVENESS OF SITZ BATH VERSUS INFRARED
LAMP THERAPY ON EPISIOTOMY PAIN AND WOUND
HEALING AMONG POSTNATAL MOTHERS
AT SELECTED HOSPITAL,
BANGALORE.
By
Ms. SUSEN GEORGE
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Bangalore.
In partial fulfillment of requirement for the degree of
Master of Science in Nursing
In
Obstetrics and Gynaecological Nursing
Under the Guidance of
Mrs. Kamala J, M.Sc. (N), Ph
Associate Professor
HOD of Obstetrics and Gynaecological Nursing,
Kempegowda College of Nursing,
Bangalore-560 004.
2013

DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “A comparative study to
assess the effectiveness of sitz bath versus infrared lamp therapy on episiotomy
pain and wound healing among postnatal mothers at selected hospital,
Bangalore” bonafide and genuine research carried out by me under the guidance of
Mrs. Kamala J, M.Sc. Nursing, Ph , Associate Professor, HOD, Department of
Obstetrics and Gynaecological Nursing, Kempegowda College of Nursing, Bangalore-
560 004.
Place: Bangalore. Signature of the Candidate
Date: Feb 2013 (Ms. Susen George)

CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “A comparative study to assess
the effectiveness of sitz bath versus infrared lamp therapy on episiotomy pain
and wound healing among postnatal mothers at selected hospital, Bangalore”
is bonafide research done by Ms. Susen George in partial fulfillment of the
requirement for the degree of Master of Science in Obstetrics and Gynaecological
Nursing.
Place: Bangalore. Signature of the Guide
Date: Feb 2013. Mrs. Kamala J, M.Sc. (N), Ph
Associate Professor and HOD, Dept. of
Obstetrics and Gynaecological Nursing,
Kempegowda College of Nusing
Bangalore-560 004.
ENDORSEMENT BY THE HOD, PRINCIPAL/HEAD OF
THE INSTITUTION
This is to certify that the dissertation entitled is “A comparative study to
assess the effectiveness of sitz bath versus infrared lamp therapy on episiotomy
pain and wound healing among postnatal mothers at selected hospital,
Bangalore” bonafide research done by Ms. Susen George under the guidance of
Mrs. Kamala J, M.Sc.Nursing, Ph , Associate Professor, HOD, Department of
Obstetrics and Gynaecological Nursing, Kempegowda College of Nursing,
Bangalore-560 004.
Seal & Signature of the HOD Seal & Signature of the Principal
Mrs. Kamala J, M.Sc. (N), Ph Mrs. V. T. Lakshammama, M.Sc.(N), Ph
Place: Bangalore. Place: Bangalore.
Date: Feb 2013. Date: Feb 2013

COPYRIGHT
Declaration by the Candidate
I hereby declare that Rajiv Gandhi University of Health Sciences, Karnataka,
shall have the rights to preserve, use and disseminate this dissertation/thesis in print
or electronic format for academic/research purpose.
Place: Bangalore. Signature of the Candidate
Date: Feb 2013 (Ms. Susen George)
Rajiv Gandhi University of Health Sciences, Karnataka.

ACKNOWLEDGEMENTS
First of all, I thank Lord Almighty for his abundant grace and blessings that
he has showered on me throughout the course of this study.
I convey my sincere indebtedness to the Kempegowda College of Nursing,
Bangalore-04, for providing me an opportunity to be a student of this esteemed
institution and to conduct this study.
It is my privilege to express my sincere thanks and profound gratitude towards
my esteemed teacher and guide Mrs. Kamala J, M.Sc Nursing, Ph , Associate
professor, HOD, Department of Obstetrics and Gynecologcal Nursing. She is a
mentor who infused me in confidence and encouragement in my endeavour, whenever
needed. It has been my good fortune to have her as my guide. Her contagious
enthusiasm gave me a hope to surmount all the obstacles and hurdles in the study. It
has been an invaluable experience working under her. We fall short of words to
“Thank you madam”.
I extend my sincere thanks to Mrs. V. T. Lakshamamma., M.Sc. N, Ph ,
Principal and HOD, Community Health Nursing, Kempegowda College of Nursing,
Bangalore-04, for encouragement, constructive criticism and timely help to make this
research experience a rich and rewarding one.
I owe a special thanks to Medical superintendent, HOD of OBG dept, and
Nursing superintendent of Kempegowda Institute of Institute of Medical Sciences,
Hospital and Research Centre, Bangalore for granting me permission to conduct
study.
I would like to extend my deepest gratitude to all the Experts who have
contributed in the form of constructive criticism and suggestions to formulate the tool.
I extend my sincere thanks to all the M.Sc Nusing Faculty of Kempegowda
College of Nursing, Bangalore-4, for their constructive criticism and valuable
suggestions.
I express my words of appreciation to Dr. Gangaboraiah, PhD (statistics),
Department of Community Medicine, KIMS, Bangalore for his valuable suggestions
and guidance in statistical analysis.
I owe a deep sense of gratitude to all Office staffs and Librarian of our
college who have contributed for the successful completion of the study.
I would fail in my duty if I forget the postnatal mothers who participated in
this study. It is because of them this thesis has seen the light of the world.
My healthy ovation of gratitude to my beloved parents Mr. George Joseph and
Mrs. Omana George, my loving brothers Mr. Rajesh George and Mr. Rejeesh
George, my dearest sister in law Mrs. Aswathy Rejeesh who laid foundation to my
higher studies, I want to thank you for your unconditional love and unending support
across the distance.
I thank all my friends, classmates, my seniors and juniors for their co-
operation and help rendered during my study. I strongly acknowledge that they have
positively contributed to my personal growth.
Finally, I thank all those well-wishers of mine who have directly or indirectly
contributed to the success of this work.
Place: Bangalore.
Date: Ms.Susen George
ABSTRACT
Background
Episiotomy is a common surgical procedure performed during second
stage of labour to enlarge the vaginal introits and facilitate delivery. Although
episiotomy aids in safe delivery of the child, the discomfort of episiotomy is an
added concern in the already over stressed situation of puerperium. Episiotomy
pain and delayed wound healing often interferes with even basic daily activities
of the postnatal mother. Considering the high rates of episiotomy , following
vaginal deliveries, we need to offer patients treatment alternatives for perineal
pain , based on scientific evidence.
The study was undertaken to assess the effectiveness of sitz bath versus
infrared lamp therapy on episiotomy pain and wound healing in selected
hospital, Bangalore.
Objectives
i. To assess the level of pain and wound healing status among postnatal mothers
with episiotomy.
ii. To assess the effectiveness of sitz bath and infrared lamp therapy on
episiotomy pain and wound healing among postnatal mothers.
iii. To compare the effectiveness between sitz bath and infrared lamp therapy on
episiotomy pain and wound healing among postnatal mothers.
iv. To determine an association between pain level & wound healing status with
selected demographic variables.
Method
A quasi experimental prê test and post test design with a comparison group was
used for the present study. The sample size consisted of 60 postnatal mothers who had
normal delivery with episiotomy and of which 30 were assigned to control group and
30 were assigned to the experimental group. Purposive sampling technique was used
to select the samples. Data was collected by using verbal descriptive pain scale for
assessing episiotomy pain and REEDA scale for assessing wound healing. When
subjects in the control group have given with routine sitz bath, subjects in the
experimental group have administered with infrared lamp therapy which is introduced
by the investigator. Interventions continued for three days both morning and evening.
Data was analyzed using descriptive and inferential statistics.
Result
The paired ‘t’ test score shows that there is a significant difference between
pre test pain scores at 0.05 levels in both control (13.68) and experimental group
(14.69) at 0.05 level. Student ‘t’ test score (2.62) shows that there is significant
difference between control and experimental group.
The paired ‘t’ test score shows that there is a significant difference between pre
test wound scores at 0.05 levels in both control and experimental group at 0.05 level.
Student‘t’ test score shows that there is no significant difference between control and
experimental group.
There was no significant association between pre test pain & wound scores and
selected demographic variables with an exemption of religion (x2 = 8.57)which has
shown a significant association with pre test pain scores only in experimental group.

Interpretation and conclusion
Mothers who had undergone the treatment of infrared lamp therapy expressed
decreased pain intensity compared to the mothers who had undergone treatment of sitz
bath. However sitz bath and infrared therapy were found to have same effect on
episiotomy wound healing.
Key words
- Sitz bath
- Infrared lamp therapy
- Episiotomy pain
- Episiotomy wound
- Post natal mothers.

LIST OF ABBREVIATIONS
1. REEDA Scale Redness Edema Ecchymosis Discharge
Approximation Scale
2. H Hypothesis
3. n1 Number of samples in control group
4. n2 Number of samples in experimental group
5. F Frequency
6. RMLE Right mediolateral episiotomy
7. LMLE Left mediolateral episiotomy
8. SD Standard deviation
9. P Probability
10. Df Degree of freedom
11. N Number of respondents
12. Α Alpha
13. FEP Fisher’s Exact Probability
14. *S Significant
15. NS Not significant

TABLE OF CONTENTS
Sl. No.
Particulars
Page No.
1. Introduction
Background of the study
Need for the study
1-8
2. Objectives
Statement of the problem
Objectives
Operational definition
Hypothesis
Conceptual framework
9-14
3.
Review of Literature
Reviews related to episiotomy
Reviews related to effectiveness of sitz bath
Reviews related to effectiveness of infrared
lamp therapy
15-30
4. Methodology
Research approach
Research design
Research setting
Population
Sample
Sample size
sampling technique
Sampling criteria
Data collection tool
Pilot study
Data collection process
Plan for data analysis.
31-40
5.
Results
41-66
6. Discussion 67-73
7. Conclusion
Implications of the study
Limitations of the study
Recommendations
74-77
8. Summary
Statement of the problem
Objectives of the study
Hypotheses
Findings of the study.
78-82
9. Bibliography 83-89
10. Annexure
90-101
LIST OF TABLES
Sl. No. Title of the Table Page
No.
1. Distribution of Subjects by Age 44
2. Distribution of Subjects by Religion 45
3. Distribution of Subjects by Education 46
4. Distribution of Subjects by Occupation 47
5. Distribution of Subjects by Type of family 48
6. Distribution of Subjects by Diet 49
7. Distribution of Respondents by Place of living 50
8. Distribution of Respondents by Parity 51
9. Distribution of Respondents by Type of episiotomy 52
10. Assessment of episiotomy pain level 53
11. Comparison of pain scores among control and experimental
group 53
12 Pre test and post test pain scores in control group 54
13 Pre test and post test pain scores in experimental group 55
14 Comparison of post test wound scores in control and
experimental group 56
15 Association of pre test pain scores with selected demographic
variables in control group 57
16 Association of pre test pain scores with selected demographic
variables in experimental group 58
17 Assessment of episiotomy wound status 59
18 Comparison of wound scores among control and experimental
group 60

19 Pre test and post test wound scores in control group 61
20 Pre test and post test wound scores in experimental group 62
21 Comparison of post test wound scores in control and
experimental group 63
22 Association of pre test wound scores with selected
demographic variables in control group 64
23 Association of pre test wound scores with selected
demographic variables in experimental group 65

LIST OF FIGURES
Sl.
No. Title of the Figure
Page
No.
1 Conceptual Framework based on Imogene King’s Goal Attainment
theory. 11
2 Schematic Representation of the Study Design. 40
3 Distribution of Respondents by Age. 44
4 Distribution of Respondents by Sex. 45
5 Distribution of Respondents by Education. 46
6 Distribution of Respondents by Occupation. 47
7 Distribution of Respondents by Type of family 48
8 Distribution of Respondents by Diet 49
9 Distribution of Respondents by Place of living 50
10. Distribution of Respondents by Parity 51
11. Distribution of Respondents by Type of episiotomy. 52

LIST OF ANNEXURE
ANNEXURE
NO.
ANNEXURE
INDEX
CONTENTS
PAGE
NO.
1. Annexure –A Copy of letter seeking permission to
conduct the study 91
2. Annexure –B
Copy of the letter seeking expert’s opinion
for the content validity of the tool 92-93
3. Annexure –C Content validity certificate 94
4. Annexure –D
Criteria rating scale for evaluation 95-96
5. Annexure –E
List of experts consulted for content
validity of the tool 97
6. Annexure –F Copy of consent form 98
7. Annexure -G Tool used for the study 99-102

1
1. INTRODUCTION
"Women, because of their closer affinity to their children,
suffer more keenly than do men.”
(Elizabeth Braxter)
Post partum is a very special period for a woman and her family.
It is usually joyful when a pregnant mother gives birth to a baby she has
expected. Despite the pain and discomfort, birth is a long awaited grand
ending of a pregnancy and a start of a new life. A mother is the beginning
of a new chapter of human life. The process of labour not only generates
new life but also it creates new species in the world thereby makes the
world as an ever ending place for the human beings to live. That’s why
mothers are special and labour is precious1.
Following the birth of the baby and expulsion the placenta, the
mother enters a period of physical and psychological recuperation. From
a medical and physiological view point this period is called the
puerperium, which is a crucial period for the mother. During this period a
mother is going through the physiological process of uterine involution
and at the same time adapting to her new role in the family2.
Mothers experience some discomforts after delivery although they
are considered normal common discomforts of puerperium period are
after birth pain, perineal pain, fatigue, constipation, breast engorgement,
lactation suppression, headache, backache, can lead to physical

2
discomfort, psychological distress and a poor quality of life for the
mothers3.
Pain in labour is a universal experience for childbearing women.
It may be as a result of trauma during child birth, due to an episiotomy, a
spontaneous tear or a combination of both. The discomfort of episiotomy
is an added concern in the already overstressed situation3. Episiotomy
pain often interferes with basic daily activities for the woman such as
walking, sitting, and passing urine and also negatively impacts on
motherhood experiences2.
Episiotomy was not widely used until the 1920s. In addition to the
strong advocacy for the use of episiotomy of the day, changes in
maternity practices also affected the use of episiotomy. The shift from
home birth to hospital deliveries contributed to a shift in the
conceptualization of the nature of childbirth. This shift made Episiotomy
as a common surgical procedure performed during second stage of labour
to enlarge the vaginal intriotus and to shorten the second stage of labour
in cases of fetal distress. Episiotomy is protective against more severe
perineal lacerations4.
Considerable evidences of risks are also associated with
episiotomy such as pain, edema, infection, and ultimately dyspareunia.
However, appropriate treatment can resolve or reverse all these after
effects. The prompt use of the best selected treatment for any injury

3
including, an episiotomy, ensures it will heal completely, in the shortest
possible time, with the least amount of complications. So midwives have
an important role to play in the care of perineal wounds following child
birth. The maintenance of effective pain relief must be balanced with the
need to promote wound healing5.
There are several treatments for relieving perineal pain and
promoting wound healing. Pharmacological and non-pharmacological
methods are used to treat this discomfort. Pharmacological pain relief
methods include non-steroidal anti-inflammatory drugs, oral analgesics,
local anaesthetics and opioids. But this method is associated with serious
adverse effects such as constipation, gastric irritation, passage of the drug
to maternal milk, and prolonged bleeding time6
With regard to non-pharmacological methods, common practice
are the use of ice packs, and heat application. Ice packs during the first 24
hours postpartum is a traditional method used for the immediate
symptomatic relief of pain since it anesthetizes the perineum, but this
relief is generally short-lived, and there is no evidence of any long-term
benefit. After 24 hours, heat is recommended because it increases
circulation to the region. Forms of heat used are sitz bath or infrared lamp
therapy application. It helps to reduce perineal edema, to avoid the
formation of hematomas, to relieve discomfort, to promote recovery of
the wound by cleaning the perineum and anus, and reduces
inflammation7,8

4
It is vital that health professionals who care for the puerperant
patient know how to evaluate and treat perineal pain. Considering the
high rates of perineal trauma after normal deliveries that still exist in our
population, it is necessary to offer these patients alternative treatments for
perineal pain &wound healing based on scientific evidence9.
NEED FOR THE STUDY:
Labour is a wondrous act of nature, and unique to every
childbearing woman. It is a transformative event in a women’s life. The
onset of motherhood presents a unique set of physical, emotional and
psychological challenges. The post-partum phase can become even more
challenging when the new mother experiences perineal or genital tract
trauma as a result of child birth10
.
Episiotomy (“unkindest cut of all”), defined as a surgical incision
in the perineum to enlarge the vaginal opening for birth, was introduced
as an obstetric procedure more than 200 years ago and became a common
practice from the beginning 20th
century. It is the only surgical procedure
in obstetrics is performed without the patient’s specific consent11
.
Studies about the episiotomy rates around the world showed that
this surgery ranged from 9.7%(Western Europe – Sweden) to

5
96.2%(South Africa – Ecuador) with lowest episiotomy rates in English –
speaking countries(North America- Canada and United States) and it
remained high in many counties (centred south-America like Brazil:
94.2%, South Africa – 63.3% and Asia like China 82%)12.
In India, the
overall rate of episiotomy was 40.6%. Among that midwives performed
episiotomies at a lower rate (21.4%) than faculty(33.3%) and private
providers(55.6%)13
. The episiotomy rate in Karnataka is approximately
88% in women who are undergoing difficult labour. In Bangalore rates of
episiotomy for vaginal birth range from 31% to 95% of the grand total of
3590 vaginal deliveries14
.
A cross sectional study conducted on “population based study of
episiotomy” in Chennai, India among a sample of 442 women who had
vaginal delivery. The result revealed that the rate of overall episiotomies
was 67%. For women whose delivery conducted by doctors the
episiotomy rate was 77.4% and conducted by nurses it was 53.1%.
Episiotomy rate was very high (91.8%) when delivery was conducted in
private medical colleges. In conclusion, episiotomy rate in the study
population is high. The probability of episiotomy is very high when
doctors conducted the delivery and when place of delivery is private
medical college hospital15
Pain following episiotomy appears to be universal. The mother
undergoing episiotomy is characterised by greater blood loss in
6
conjunction with delivery, and there is a risk of improper wound healing
and increased pain during early puerperium2.
A study conducted to establish the prevalence of perineal pain, the
effects of pain on postnatal recovery in Royal Women’s Hospital,
Victoria, Australia. Researchers conducted structured interviews of 215
women in the postnatal ward of tertiary hospital, within 72 hours of
vaginal birth. Results revealed that 90% of women reported some peineal
pain, with 37% reporting moderate or severe pain. Over a third of women
experienced moderate or severe perineal pain, particularly when walking
(33%) or sitting (39%), while 45% noted that pain interfered with their
ability to sleep. Women reported moderate or severe perineal pain when
they undertook activities involving feeding their infant (12%) or caring
for their infant(12%). The researchers suggested that the prevalence of
peineal pain and the associated impact on women’s from childbirth
warrants midwives’ proactive care in offering a range of effective pain
relief options to women16
Various intervention are found to reduce episiotomy pain and
enhance healing process, which include administration of analgesics,
cleanliness, applying ice pack , topical application by dry heat (infra red
therapy), sitz bath, performance of Kegel’s exercise and perineal care2.

7
A sitz bath involves immersion of the perineal area/ buttocks in
warm water (medicated if ordered) at a temperature of 105 to 110 degree
F for 15 to 20 minutes. It is used to relive discomfort. The bath promotes
wound healing by cleaning the perineum and anus, increasing circulation,
and reducing inflammation, it also helps to relax local muscles.
Infrared light therapy is a unique form of treatment where the
healing effects of the light is utilized for treating episiotomy. In this
therapy, the injury site or the diseased part of the body is exposed to
infrared radiation with a light source of 245 volts at a distance of 45- 50
cm from it, and for 10 – 15 minutes which provides relief from the
discomfort. It is very simple, absolutely painless and no major side
effects17
.
A study conducted on “Pharmacological and non pharmacological
treatment for relief of perineal pain after vaginal delivery” in Brazil to
identify the types of pharmacological and non pharmacological treatment
used during hospitalization, in the relief of perineal pain after vaginal
deliveries. Result reveals that among 130 patients 98.5% used drugs, and
62.3% of them also used non- drug treatments such as Ice pack, warm
sitz bath and Hot compress. The study concluded that health care
professionals, who attend to puerperas, know how to assess and treat
peineal pain. Considering the high rates of peineal trauma, following

8
vaginal deliveries, we need to offer patients treatment alternatives for
perineal pain, based on scientific evidence18
.
Based on review of literature and clinical experience of the
investigator, it is seen that in many postnatal mothers, episiotomy pain
and discomfort dominate the feeling of motherhood and it has many
negative impacts on women’s ability to care for their newborns, their
ability for breast feeding and attending to their baby’s need would
decrease significantly. Hence the investigator rightly felt to conduct a
comparative study on the effectiveness of sitz bath versus infrared lamp
therapy in the management of episiotomy pain and wound healing among
postnatal mothers.

9
2. OBJECTIVES
This chapter consists of the statement of problem, objectives, operational
definitions & theoretical framework selected for the study.
STATEMENT OF THE PROBLEM:
“A comparative study to assess the effectiveness of sitz bath versus infra red
lamp therapy on episiotomy pain and wound healing among post natal mothers at
selected hospitals, Bangalore.”
OBJECTIVES OF THE STUDY:
i. To assess the level of pain and wound healing status among postnatal mothers with
episiotomy.
ii. To assess the effectiveness of sitz bath and infrared lamp therapy on episiotomy pain
and wound healing among postnatal mothers.
iii. To compare the effectiveness between sitz bath and infrared lamp therapy on
episiotomy pain and wound healing among postnatal mothers.
iv. To determine an association between pain level & wound healing status with selected
demographic variables.
HYPOTHESES:
H1: There is a significant difference between the mean pre test and post test pain &
wound healing scores in sitz bath and infrared lamp therapy group.

10
H2: There is a significant difference in the mean post test scores between sitz bath and
infrared lamp therapy group.
H3: There is a significant association between pain &wound healing scores with
selected demographic variables in sitz bath and infrared lamp therapy group.
OPERATIONAL DEFINITIONS:
Comparative: It refers to statistical measurement of difference between infrared lamp
therapy versus sitz bath on level of episiotomy pain and wound healing.
Effectiveness: Refers to the extent to which sitz bath/ infrared lamp therapy helps in
relieving episiotomy pain and enhancing wound healing in postnatal mothers which is
measured by Verbal Descriptive Pain Scale and REEDA scale (Redness, Edema,
Ecchymosis, Discharge, Approximation).
Sitz bath: A bath in which perineal area / buttocks are submerged in 4 litre of warm
water added with 5-6 drops of 10% Providone iodine (Betadine) solution having a
temperature of 105 to 110 0
F for 20 minutes for three days both morning and evening.
Infra red lamp therapy: Refers to a lamp which emits infrared rays with a light
source of 245volts (150 watts power ) and a frequency of 50 Hz, focused on
episiotomy suture site at a distance of 45-50 cm from it and lasting for a duration of
10- 15 minutes for three days both morning and evening.
Episiotomy: A surgically planned incision on the perineum and posterior vaginal wall
during the second stage of labour to enlarge the vaginal introitus to facilitate easy and
safe delivery
11
Pain: An unpleasant, subjective, sensory, and emotional experience by postnatal
mothers due to tissue damage resulted from episiotomy incision which is assessed by
Verbal Descriptive Pain scale.
Wound healing: It is a dynamic process of regaining the skin integrity of episiotomy
wound which is assessed by REEDA scale (Redness, Edema, Ecchymosis, Discharge,
Approximation).
Postnatal mothers: It denotes to a women who had normal vaginal delivery with
episiotomy, up to fourth day of childbirth, irrespective of her parity.
CONCEPTUAL FRAMEWORK
A conceptual frame work is a group of concepts and a set of prepositions that
spell out the relationship between them. The overall purpose is to make scientific
findings meaningful and generalize. Concepts are the building blocks of the theory.
Polit and Hungler states that conceptual frame work is inter related concepts or
abstractions that are assembled together in some rationale scheme by virtue relevance
to a common thing. The device that helps to stimulate research and the extension of the
knowledge of providing both direction and impetus.
It’s a frame work which provides the investigator the guidelines to proceeds in
attaining the objectives of the study based on theory. It is a scientific representation of
the steps, activities and outcome of the study19
.
The present study was aimed at assessing the effectiveness of sitz bath versus
infrared lamp therapy on episiotomy pain and wound healing among post natal
mothers with episiotomy.

12
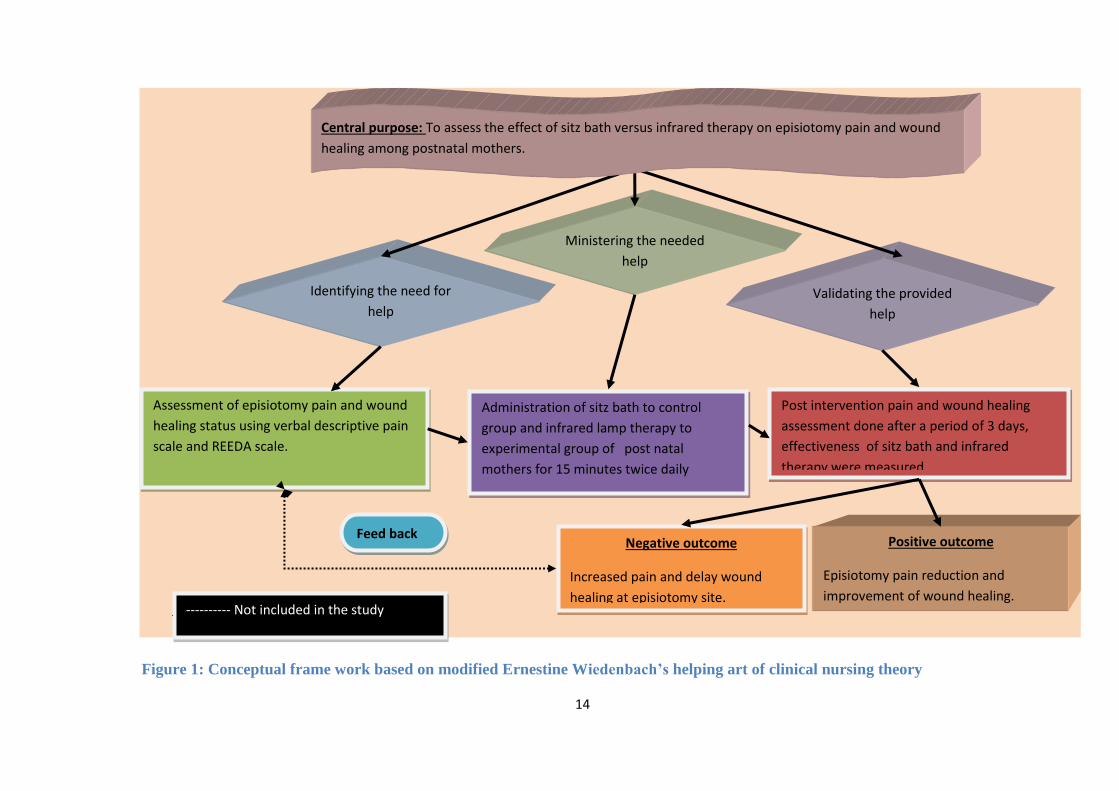
The conceptual frame work of the present study is based on Ernestine
Wiedenbach’s helping art of clinical nursing theory (Figure-1), consists of three steps
that is central purpose, prescription and realities.
Wiedenbach proposes a prescriptive theory for nursing which is described as
conceiving of a desired situation and the ways to attain it. Prescriptive theory directs
action toward an explicit goal. A nurse develops a prescription based on a central
purpose and implements it according to the realities of the situation20
.In the present
study Weidebach, nursing practice consists of identifying the patients needed help and
validating the provided help.
Central purpose: It refers to what the nurse (investigator) wants to accomplish. It is
the overall goal which acts dynamically in relation to one’s belief.
Identification: The present health needs of postnatal mothers are the pain and delayed
healing of episiotomy wound. The nurse investigator identifies the level of pain and
wound healing status of postnatal mothers with episiotomy and sets a goal to reduce
pain and improve wound healing of post natal mothers with episiotomy.
Prescription: Refers to the plan of activity directed. It specifies the nature of the
action that will fulfil the nurse’s central purpose and the rationale for that action. A
prescription may indicate the broad general action appropriate to implementation of
the basic concepts and suggest the kind of behaviour needed to carry out these actions
in accordance with the central purposes. Here the investigator review interventions
(sitz bath and infrared lamp therapy), formulate plan for administration and develop
Verbal Descriptive Pain Scale and REEDA Scale for the episiotomy pain and wound
healing assessment.
13
Realities: Refers to the physical, physiologic, emotional and spiritual factors that
come into play in a situation involving nursing actions. The realities are
Agent – is the investigator
Recipients – are the postnatal mothers
Goal – to reduce episiotomy pain and improve episiotomy wound healing
Means : Sitz bath and infrared lamp therapy.
Frame work: Kempegowda Institute Of Mediacal Sciences and Research Centre.
In this phase the investigator carry out interventions such as sitz bath and infrared
lamp therapy.
Validation: In this phase, the episiotomy pain level and wound status reassessed by
using Verbal Pain Scale and REEDA Scale to determine the effectiveness of sitz bath
and infrared lamp therapy. The pain level is categorised in to no pain, mild pain,
moderate pain, and severe pain. Similarly wound healing status divided into no
infection, mild infection, moderate infection and severe infection. These
categorisations have been done to find out the extent of effectiveness. Reinforcement
is suggested to the subjects with positive outcome, whereas negative outcome is again
identified as a need for continuation of treatment (feedback)
SUMMARY
This chapter deals with the statement of the problem, objectives, hypothesis,
operational definitions and conceptual frame work.
14
Identifying the need for
help Validating the provided
help
Post intervention pain and wound healing
assessment done after a period of 3 days,
effectiveness of sitz bath and infrared
therapy were measured.
Administration of sitz bath to control
group and infrared lamp therapy to
experimental group of post natal
mothers for 15 minutes twice daily
Assessment of episiotomy pain and wound
healing status using verbal descriptive pain
scale and REEDA scale.
Negative outcome
Increased pain and delay wound
healing at episiotomy site.
Positive outcome
Episiotomy pain reduction and
improvement of wound healing.
Ministering the needed
help
Feed back
---------- Not included in the study
Central purpose: To assess the effect of sitz bath versus infrared therapy on episiotomy pain and wound
healing among postnatal mothers.
Figure 1: Conceptual frame work based on modified Ernestine Wiedenbach’s helping art of clinical nursing theory

15
3. REVIEW OF LITERATURE
Review of literature is a systematic identification, scrutiny and
summary of written material that contains information on research problem.
The researcher presents the review of literature, which helps to
study the problem in depth. It also serves as a valuable guide to understand
what has been done and what is still unknown and untested.
The reviewed literature provides the evidence of what has been
studied in the past and published; paving way for further study in the
chosen subject. It justifies the need for study; throws light on the feasibility
of the study, reveals methodology and relates the findings from one to
another with a hope to establish a comprehensive study of scientific
knowledge. The researcher did an extensive search of existing literature,
and organized it under following heading:
1. Reviews related to episiotomy
2. Reviews related to effectiveness of sitz bath
3. Reviews related to effectiveness of infrared lamp therapy

16
Reviews related to episiotomy
A study was conducted in Denmark to evaluate the influence of
episiotomy on the perineal state after spontaneous singleton vaginal
deliveries. Two approaches were used in the analysis. Initially the 2188
parturient were quasi randomised to one of three equally sized groups of
midwives with different attitude towards episiotomy. Secondly, the study
was continued to find out the effect of episiotomy on the state of anal
sphincter. The results revealed that women allocated in the group with
lowest rate of episiotomy were more likely to have intact perineum after
delivery (OR = 1.8(1.4-2.2)), had a tendency towards more perineal
lacerations (OR(1.3(1.0-1.5)). The study concluded with a consecutive
approach to the use of mediolateral episiotomy and suggests that
episiotomy should be used in, ‘one in five’, spontaneous vaginal
deliveries21
.
A retrospective cross sectional study was conducted to determine
the prevalence and factors associated with episiotomy in a reference
centre in Brazil. The study included 495 women who had a normal
delivery, assessed for factors such as issues preceding birth,
characteristics of labour and perinatal outcome. The study concluded that
presence of perineal lacerations was higher in the group not subject to
episiotomy and factors associated with episiotomies were maternal
disease and absence of previous vaginal delivery22
.
17
A study was conducted in UK with the objective of analysing the
significance of risk factors and the role of episiotomy in preventing
obstetric anal sphincter injury (OASI) at vaginal delivery. A study
population of 10,314 post natal women who had vaginal delivery were
assessed to identify the factors that had a significant association with
OASI. Factors included parity, age, gestation, labour induction method,
duration of second stage, use of epidural analgesia, episiotomy, method
of delivery, time and month of delivery, and birth weight. The results
revealed that parity, age, birth weight, method of delivery and shoulder
dystocia are strongly associated with obstetric and sphincter injury.
Women giving birth without a mediolateral episiotomy were 1.4 ties
more likely to experience OASI (95% CI 1.021-1.983). The study
concluded that mediolateral episiotomy appears to be protective against
OASI23
.
A population based observational study was conducted to
determine the risk factors for anal sphincter injuries during operative
vaginal delivery in Netharlands. The study included 21254 postnatal
women who underwent operative vaginal delivery. Risk factors were
determined with multivariate logistic regression analysis. The results
revealed that primiparity and occipito posterior presentation are strong
risk factors for the occurrence of anal sphincter injury during operative
vaginal delivery. Mediolateral episiotomy protected significantly for anal

18
sphincter damage in both vacuum extraction (OR 0.11, 95% CI 0.09-
0.13) and forceps delivery (OR 0.08, 95% CI 0.07-0.11) The study
concluded that highly significant protective effect of mediolateral
episiotomies in both types of operative vaginal delivery warrants the
conclusion that this type of episiotomy should be used routinely during
these interventions to protect the anal sphincters24
.
A randomised controlled trail was conducted with the objective to
assess the effects of restrictive use of episiotomy compared with routine
episiotomy during vaginal birth in Argentina. Trial quality was assessed
and data were extracted independently by two reviewers from six studies
which included 4850 samples. In the routine episiotomy group, 72.7% of
women had episiotomies while the rate in the restrictive episiotomy
group was 27.68%. The results revealed that compared with routine use,
restrictive episiotomy involved less posterior perineal trauma (RR=1.11)
and less suturing (RR=0.74), but there was increased risk of anterior
perineal wall trauma (RR=1.79) with restrictive episiotomy. In
conclusion, restrictive episiotomy is associated with increased anterior
perineal wall trauma25
.
A study was conducted to assess the relationship between hospital
episiotomy and the incidence and risk of perineal trauma among women
in Pennsylvania, USA. The relationship between episiotomy use and
perineal trauma at the hospital level was examined using regression

19
analysis. The results revealed that hospital episiotomy rates ranged from
approximately 20 to 73%. The rate of third or fourth degree perineal
lacerations varied from a low of 4% to a high of more than 13 % among
hospitals. In conclusion, rates of episiotomy were significantly correlated
with rates of third or fourth degree perineal laceration (r=0.70;
puerperium<0.001)26
.
A retrospective case control study was conducted to determine
risk factors for third degree obstetric perineal tears and to give
recommendations for prevention, in Amsterdam, Netherlands. One
hundred and twenty cases of vaginal delivery complicated by third degree
perinal tear and 702 uncomplicated vaginal deliveries were compared,
with respect to possible risk factors. The results revealed that high birth
weight, forceps delivery, induced labour, epidural anaesthesia and parity
were risk factors for anal sphincter tear. In addition, mediolateral
episiotomy was associated with fewer sphincter injuries. The study
concluded that mediolateral episiotomy may be sphincter – saving and
therefore prevent from chronic faecal incontinence27
.
A study was conducted in San Francisco to examine the
association between maternal vaginal and perineal morbidity and
episiotomy performed at operative vaginal delivery. Data obtained from
2041 consecutive operative vaginal deliveries and compared yearly rates
of episiotomy, lacerations, and potential confounders with linear

20
regression and stratified analyses. The results revealed that the use of
episiotomy for operative vaginal deliveries fell significantly (93.4% to
35.7%, R2=0.85, puerperium-0.0001). This change was associated with a
rise in the rate of vaginal lacerations (16.1% to 40.0%, R2=0.80,
puerperium=0.0002). The study concluded that a statistically and
clinically significant reduction in the use of episiotomy for operative
vaginal deliveries was associated with an increase in the rate of vaginal
lacerations28
.
A review was conducted to assess the role of episiotomy in
current obstetric practice in USA. The modern indications for episiotomy
including the procedures place at operative vaginal delivery are
discussed. Although the role of the episiotomy in modern obstetrics may
be limited, the procedure is important in situations involving non
reassuring fetal status, shoulder dystocia, and operative vaginal delivery.
The optimal type of episiotomy, if any, at forceps or vaccum delivery is
yet to be determined29
.
Reviews related to effectiveness of sitz bath
A randomized controlled clinical trial conducted to determine the
effect of Povidone Iodine sitz bath versus lavender Oil sitz bath treatment
on episiotomy wound healing in Iran. Through randomization 120
primipararous women who underwent vaginal delivery with episiotomy

21
divided into 2 groups: control (n=60) and experimental (n=60) group.
The control group took sitz bath with 5-7 drops of Povidone Iodine
whereas experimental group with 5-7 drops of lavender oil in 4 L of
water twice daily for 10 days. The study concluded that both therapies are
significantly effective (P=0.003) in treating postpartum episiotomy pain,
edema and preventing infection30
.
A Quasi experimental study was conducted on Sitz bath versus
Self perineal care on episiotomy wound healing. 40 postnatal mothers
were taken for the study. 20 postnatal mothers were given Sitz bath and
20 postnatal mothers were given Self perineal care. The findings of the
study denote that the application of sitz bath has significant influence in
episiotomy wound healing. The study revealed that the REEDA score
was significantly low (p=0.007) in the experimental group. The study
concluded that Sitz bath is effective in episiotomy healing31
.
A study conducted on “post episiotomy pain: warm versus cold
sitz bath” in Colombia. Study included 20 samples to assess the
effectiveness of a warm versus cold sitz bath in relieving post episiotomy
pain. Sensation, distress, edema, and hematoma rating were obtained pre
– and post treatments. In conclusion, both therapies were found
comparable and significantly effective in managing post episiotomy
pain32
.
22
A study was conducted to examine the effect of aroma sitz bath
therapy on postpartum mother’s perineal healing in Korea. In this clinical
trial, postnatal mothers who delivered vaginally with an episiotomy were
allocated to aroma sitz bath group and control group. The perineal
healing status was measured using the REEDA Scale and smears for
episiotomy wound were obtained. The results revealed that REEDA
Scale was significantly low in the experimental group at postpartum 5th
and 7th
days (P=.009, P=.003), respectively. Most were observed ‘few’
(5-10 bacteria per field) bacteria in the smears of episiotomy wound. In
conclusion, these findings indicate that postpartum aroma sitz bath
therapy is effective in healing the perineum33
.
An experimental study conducted at Coimbatore in Tamil Nadu to
determine the effectiveness of infrared therapy and sitz bath. 30 samples
were randomly selected for the study, out of that 15 each has been
assigned to two experimental groups. Two experimental groups were
selected for infrared therapy and sitz bath and treatment were given for
three days in the morning and in the evening. Results revealed that
mother who had undergone the treatment of infrared therapy expressed
decreased pain intensity compared to mothers who had undergone the
treatment of sitz bath. In conclusion, infrared light therapy and sitz bath
were found to have same effect in the episiotomy34
.
23
A comparative Study was conducted on effects of medicated sitz
bath and non- medicated sitz bath on the episiotomy site at Chicago. The
objective of the study was to evaluate postpartum healing of the perineum
sample of 60 subjects were taken. 30 were given with medicated sitz bath
and 30 with non-medicated sitz bath. Analysis of variance indicated no
difference in REEDA score before or two hours after treatment35
.
An experimental study was conducted to assess the effectiveness
of sitz bath at California, the objective of the study was to determine
effectiveness of sitz bath and recommendation of sitz bath in the
management of episiotomy wound. 50 articles were taken The results
showed that 36 articles were found with highlighted the physiology
benefits risks complication and techniques of sitz bath one randomized
study comparing sitz bath to placebo found. Two articles speculated that
sitz bath induces relaxation of the muscle. Cold sitz bath was reported to
decrease perineal edema more than warm bath. The study concluded that
sitz bath is recommended in the treatment of episiotomy36
.
A comparative study was conducted to assess the effectiveness of
warm sitz bath and ice pack on intensity perineal pain after episiotomy in
primipara women, in Sydney. The objective of the study is to evaluate the
effectiveness of two devices. Perineal pain after episiotomy 121
primipara mothers was chosen. The results of the study showed that
wound healing in the warm sitz bath was better when compared to the ice

24
pack on intensity perineal pain. In conclusion, warm sitz bath and ice
pack were found to have varied effect on episiotomy pain intensity37
.
A comparative study was done to find the effect of Sitzbath
versus GuggulDhupan on episiotomy pain in postnatal mother admitted
in Pune hospital. 60 postnatal mothers were used in this study, 30
postnatal mothers were given Sitzbath and 30 postnatal mothers were
given Guggul Dhupan. According to self - assessment score, maximum
(53.3%) postnatal mothers were having mild pain after giving Sitzbath
and this difference was statistically significant, maximum (63.3%)
postnatal mothers were having severe episiotomy pain before Guggul
Dhupan and 80% of postnatal mothers were having mild pain after
Guggul Dhupan. The study concluded that Sitz bath is effective in
reducing episiotomy pain38
.
A quasi randomized study was conducted to assess the effects of
water compared with other solutions for wound cleansing, in Australia.
Eleven trials were included in this review. Seven trials were identified
that compared rates of infection and healing in wounds cleansed with
water and normal saline, three trials compared cleansing with no
cleansing and one trial compared procaine spirit with water, the relative
risk of developing an infection when cleansed with tap water compared
with normal saline was 0.16, (95% CI 0.01 to 2.96). The study
25
concluded that tap water was more effective than saline in reducing the
infection rate in adults with acute wounds39
.
Reviews related to infrared therapy
An experimental study conducted at selected Hospitals in
Kovilpatti, Tamil Nadu to determine the effectiveness of infra red lamp
therapy on episiotomy wound healing and pain. The control group (n=30)
used the existing methods of episiotomy care whereas, the subjects of the
experimental group (n=30) were provided with the infrared therapy for
10 minutes for 3 days. Results reveals that the mean episiotomy pain
score of the control group participants was high on all three days in
comparison with the experimental group and 10% of the participants in
the control group developed mild infection whereas none of the
participants in the experimental group, the results was statistically
significant (p<0.001). The study concluded that infrared therapy is
effective in managing episiotomy pain and wound healing40
.
An experimental study was conducted in Coimbatore, TamilNadu,
India to assess the effectiveness of infrared therapy in healing of
episiotomy wound. Through random sampling 20 postnatal women were
divided into control and experimental group. Comparative approach
using two group quasi experimental research designs was adopted for the

26
study. The results revealed that in experimental group, 75% of the
mothers who received infrared radiations showed adequate wound
healing and 25% showed poor wound healing, where as 70% of the
mothers in control group showed poor wound healing. The calculated
value of ‘t’ was greater (4.05) than the expected value of ‘t’(1.96). Study
concluded that there was a significant difference between healing scores
of experimental and control group after the administration of infrared
radiation for three days41
.
A study aimed at developing the new effective method of
treatment with an application of magnet laser (near infrared) radiation as
a stimulating aid in healing perineum injuries in the maternity patients, in
Russia. In this study 86 maternity patient with episiotomy were studied.
In treatment, the injury on the perineum was conventionally treated by
antiseptic in 40 maternity patients (control group); the laser therapy was
applied to another 46 maternity patients in concomitantly with the
conventional method.
Study concluded that laser therapy improves
process of the healing considerably, promotes the rapid disappearance of
inflammatory signs and renders analgesic effect42
.
A study was conducted in Coimbatore, Tamil Nadu, India to
compare the effectiveness of infrared therapy and sitz bath. In this
experimental study, 30 samples were randomly assigned in to
experimental group 1 and experimental group 2 for sitz bath and infrared

27
therapy respectively. The pain and wound score were assessed after a
period of 3 days by using Verbal Descriptive pain scale and Modified
Southampton Scale . Results revealed that infrared light therapy and sitz
bath were found effective in the healing of episiotomy, but mothers who
had undergone the treatment of infrared therapy expressed decreased pain
intensity (p<0.05=1.701) compared to mothers who had undergone the
treatment of sitz bath. In conclusion, infrared light is a better pain relief
intervention in comparison with sitz bath in treating episiotomy43
.
A study conducted to estimate the contribution of phototherapy to
the treatment of episiotomies in Czech Republics. In this study the
researchers treated a total of 2,436 postnatal women with episiotomies.
The light sources were: a laser (near infrared) of a wave length 670 nm
with continuous alternations of frequencies, a polarized light source of a
400-2,000 nm wavelength and frequency 100 Hz and a monochromatic
light source of a 660 nm wave length with simultaneous application of a
magnetic field at an induction 8 mT. The study concluded that high
healing effects with minimum secondary complications in the treatment
of episiotomies using a therapeutic laser at an energy density of 2J/cm44
.
An experimental study conducted to compare the effects of ice
bag and heat lamp, for the relief of perineal discomfort and to identify the
sustaining time of each effect, in Korea. Eighty postnatal women with
28
episiotomy were randomly selected and divided into two experimental
groups. Both experimental groups received ice bag therapy and heat lamp
therapy simultaneously. Pre test was conducted prior to the study to
identify the degree of perineum discomfort. Post test was conducted soon
after each therapy. A comfort scale, 18cm graphic scale was used. The
results revealed that ice bag group showed significantly lower discomfort
(p<0.05) than the heat group at the half an hour, two hour and four hours
of the therapy45
.
An experimental study was conducted in Vellore to compare the
effect of cold pack versus infrared radiation on episiotomy wounds
among 60 postnatal mothers. They were randomly divided into cold
therapy group and infrared therapy group. One hour after the completion
of the intervention, the results reveals that 76.6 % mothers did not had
pain at all and 23.3% mothers experienced very mild pain in cold therapy
group whereas 66.6% had mild pain and 33.7% had moderate to severe
pain in infrared therapy group. This difference was statistically
significant. In conclusion, both cold pack and infrared therapy
recommended for treating episiotomy wound46
.
An experimental study was conducted in Hyderabad, to assess the
effectiveness of electric heat lamp on healing of episiotomy wound.
Samples were divided into control group and experimental group. Result
29
reveals that there was a significant difference in rates of healing between
control and experimental groups. Those who received heat lamp therapy
had faster healing compared to those mothers who did not receive
therapy47
.
A study was conducted to investigate potential effects of a newly
developed specific near infrared light source on wound repair, in Shiga
university of medical sciences, Otsu. In this .study, cultured human
keratinocytes, endothelial cells and fibroblasts were 'exposed to the light
and the production of transforming growth factor (TGF) was examined
by enzyme immuno assay. Incisional wounds were treated with rays and
the effect of rays on the wound closure was followed photographically.
The rate of wound closure was significantly accelerated by repeated
exposures. The study concluded that near infrared rays potentially
enhances wound-healing process, presumably by its bio stimulatory
effects48
A study was conducted at Japan University to review the
outcomes and estimate the usefulness of linearly polarized near infrared
rays therapy. A total of 35 consecutive patients complained of vague and
deep pain in the ano-rectum. 14 patients had a history of lower abdominal
surgery. 18 patients had disordered defecation. The linearly polarized
near infrared light was radiated to the strongly tender point on or a few

30
centimetres apart from the skin for 10 minutes. The effect of the therapy
was assessed as excellent, good, no change or worse by the patients
themselves. 5 patients estimated as excellent, 28 as good and 2 as no
change. The mean total number of rays was 18.8 and mean number of
rays for relief from pain was 2.5. Anorectal pain recurred in 4 patients,
who received the same therapy and improved. The study was concluded
that the linearly polarized near infrared rays therapy is a simple, safe and
effective modality for relief from intractable anorectal pain and
recommended for primary therapy49
.
SUMMARY
This chapter had dealt with the review of literature related to
episiotomy, sitz bath and infrared therapy. In brief the literature review
has provided an understanding and broadened the investigator’s outlook
necessary for designing the conceptual framework, research design and
construction of the tool of the study

31
4. METHODOLOGY
Methodology of research indicates the general pattern of organizing the
procedure for gathering valid and reliable data for the problems under investigation19
.
The methodology is the most important part of research as it is the framework
for conducting the study. This chapter comprises of the research approach used,
research design, setting of the study used, population, sample selection, sampling
technique, development and description of the tool, pilot study, method of data
collection and plan for data analysis. The study conducted was to compare the
effectiveness of sitz bath versus infrared lamp therapy on episiotomy pain and wound
healing among postnatal mothers.
RESEARCH APPROACH
In the view of the nature of the problem selected for the study and the
objectives to be accomplished, a comparative approach was considered an appropriate
research approach for the present study regarding the effectiveness of sitz bath versus
infrared lamp therapy on episiotomy pain and wound healing among postnatal
mothers.
RESEARCH DESIGN
Research design incorporates the most important methodological decisions that
a researcher makes in conducting a research study (Figure-2). The research design

32
selected for the present study was quasi experimental with pre-test and post-test
design with comparison group to achieve the objectives of the study.
E = O1 - X1 - O2
C = O1 - X - O2
Where as, C is the control group
E is the experimental group
O1 is the pre intervention assessment
O2 is the post intervention assessment
X is the intervention routinely administered in the hospital (sitz bath)
X1 is the intervention which is introduced by the investigator ( Infra red therapy)
SETTING OF THE STUDY:
The study subjects were selected from Kempegowda Institute Of Medical
Sciences and Research Centre.
Target Population
The target population for the present study was postnatal mothers who had
normal vaginal delivery with episiotomy.
Sample
A sample consists of a subset of the units that comprises the population.
Postnatal mothers who had normal vaginal delivery with episiotomy, admitted in
postnatal ward of Kempegowda Institute Of Medical Sciences, Hospital and Research
Centre

33
Sample Size
The sample size was 60 postnatal mothers who had vaginal delivery divided 30
each in control and experimental group.
Sampling Technique
Sampling is the process of selecting a portion of the population to represent the
entire population. In this study the purposive sampling was used to collect data from
the available samples falling under inclusion criteria.
Criteria for selection of sample
Inclusion criteria:
Mothers who had full term vaginal delivery with episiotomy.
Mothers with episiotomy who are willing to participate in the study
Exclusion criteria:
Mothers with infected perineum.
Mothers with medical disorders or abnormal purerperium.
Mothers with operative vaginal delivery
TOOL FOR RESEARCH
Data collection tools are the procedures or instruments used by the researcher
to observe or measure the key variables in the research problem
The episiotomy pain and wound healing and pain was assessed with the
following instruments: Demographic variables, Modified Verbal Descriptive Pain
Scale, REEDA Scale.

34
Modified Verbal Descriptive Pain Scale is the tool to assess the level of pain &
REEDA Scale is the tool used for recording the wound healing.
DEVELOPMENT OF THE TOOL
The tool was prepared on the basis of the objectives of the study. The
researcher did an extensive review of literature to collect relevant materials and based
on it selected the tool for the study.
The following steps were undertaken to prepare the final tool:
Tool was developed based on related literature review and experts suggestions
Demographic and clinical variables were developed to obtain baseline characteristics
Modified Verbal Descriptive Scale was developed to assess the level of pain in the
episiotomy area.
REEDA scale was developed to assess the level of wound healing in episiotomy area.
Content Validity
Content validity is the extent to which a measuring instrument provides
adequate coverage of the topic under the study. A criterion rating scale of the tool was
developed. It consisted of columns like Very relevant, Relevant, Need modification,
Not relevant and remarks for suggestions from the experts for each item regarding
accuracy, relevancy and appropriateness of the content. To establish the content
validity of the tool, the tool was given to 10 experts in the field of nursing, one expert
in the field of medicine. Modifications were made based on suggestion and comments
given by the experts and the guide.

35
Reliability
Reliability is defined as the extent to which the instrument yields the same
result on repeated measures. It is thus concerned with consistency, accuracy, stability
and homogeneity. The reliability of the Verbal Descriptive Pain Scale and REEDA
Scale was established for its equivalence by inter rater method after administering the
tool to ten postnatal mothers in selected hospitals. Karl – Pearson’s Correlation
Coefficient formula was used to find the reliability.
The reliability of Verbal descriptive pain scale is 0.89 and for the REEDA
scale reliability is 0.96, thus the tools were found to be reliable.
DESCRIPTION OF THE TOOL:
Demographic data
Demographic variables and clinical variables consisted of total 9 variables
like, age, religion, education, occupation, type of occupation, dietary pattern, place of
living, parity and type of episiotomy.
Verbal Descriptive Pain Scale
The pain scale was constructed based on the Verbal Descriptive Pain Scale
given by Jack Harich (2002). It is a pain scale ranging 0 to 3. Point 0 indicates no pain
and point 3 indicates severe pain. The maximum score is 3. It was used to identify the
level of pain in the episiotomy area. The subjects in the study were asked to specify the
point at which they feel pain.

36
REEDA Scale
The wound scoring scale was constructed based on the REEDA Scale given by
Nancy Davidson (1972). Redness, edema, ecchymosis, discharge, approximation are
the five categories of the scale. The scoring for each category ranges from 0 to 3. The
total score is 15
PILOT STUDY
After having obtained formal administrative approval from the Medical
superintendent, HOD of OBG department and Nursing Superintendent of the
Kempegowda Institute of Medical Science and Research Centre, Bangalore, the pilot
study was conducted from 3’rd
September ’2012 to 11th
September’2012 to find out the
feasibility of the study. Totally 10 postnatal mothers with episiotomy were selected by
using purposive sampling technique. Five samples are assigned to the control group
(sitz bath) and five to the experimental group (infra red lamp therapy group).The
subjects for the pilot study possessed the same characteristics as that of the sample for
the main study.
DATA COLLECTION PROCESS
Data collection was done in Kempegowda Institue Medical sciences and
Research centre, Bangalore. The data collection done from 1st of November 2012 to
30th
of November. Formal written permission obtained from the respective authorities.
37
Based on inclusion criteria, 60 postnatal mothers were selected from the postnatal
ward. Thirty(30) postnatal mothers got selected to the control group and another
thirty(30) to the experimental group. Samples were selected by purposive sampling
technique. Subjects were selected for postnatal ward on each day based on the
inclusion criteria. The mothers were intimated regarding the purpose of the study and
their consent was secured. Pre test was conducted for both control and experimental
group on the first day before starting therapy. The episiotomy pain was assessed by
Modified Verbal Descriptive pain Scale and wound healing was assessed by REEDA
scale. Sitz bath was given to control group and infrared therapy to the experimental
group for three days in the morning and evening for 15 minutes. Post test was
conducted on third day for both control group and experimental group by using the
same tool.
PLAN FOR DATA ANALYSIS
Analysis is the systematic organization and synthesis of research data and
testing of research hypothesis by using those data. A master data sheet was prepared
by the investigator to organize and compute data. The data would be analysed using
both descriptive and inferential statistics based on the objectives and hypothesis stated.
The plan of data analysis includes the following
Section I: Distribution of demographic and clinical characteristics of the subjects is
done by descriptive statistics.
38
Pain
Section II: Assessment of episiotomy pain and comparison of pain scores among
control &experimental group.
Section III: Effectiveness of sitz bath on episiotomy pain reduction among control
group is assessed by using paired t test
Section IV: Effectiveness of infrared therapy on episiotomy pain reduction among
experimental group is assessed by using paired t test.
Section V: Comparing the effectiveness between sitz bath and infrared lamp therapy
on episiotomy pain reduction among control and experimental group is assessed by
using student t test.
Section VI: Association between pre test pain scores and selected demographic and
clinical variables is done by using chi – square test.
Wound healing
Section VII: Assessment of episiotomy wound status and comparison wound healing
scores among control &experimental group is done by descriptive statistics.
Section VIII: Effectiveness of sitz bath on episiotomy wound healing among control
group is assessed by using paired t test.
Section IX: Effectiveness of infrared therapy on episiotomy wound healing among
experimental group is assessed by using paired t test.
Section X: Comparing the effectiveness between sitz bath and infrared lamp therapy
on episiotomy wound healing is done by using student t test.

39
Section XI: Association between pre test wound scores and selected demographic and
clinical variables is done by using chi – square test.
SUMMARY
This chapter deals with the methodology adopted for this study. This included
Research approach, Research design, Variables under study, Setting, Population,
Sample size, Sampling criteria, Development of tool, Validity, Reliability, Data
collection method and Plan for data analysis.

40
FIGURE :2 SCHEMATIC REPRESENTATION OF STUDY DESIGN.
Research approach: Comparative
Research design: Quasi experimental pre test post
test design with a comparison group
Target population:
Postnatal mothers
Data collection tool: Questinonnaire,
Verbal descriptive pain scale and REEDA
Scale
Data collection technique: Structured interviews
schedule & clinical assessment.
Data analysis: Descriptive and
inferential statistics
Findings and conclusion
Report writing
Accessible population: Postnatal
mothers admitted KIMS, Bangalore.
Samples:60 post
natal mothers (30
in control &30 in
experimental
group)
Sampling
technique:
Purposive
sampling
technique
Research purpose: To assess the effectiveness of sitz bath
versus infrared lamp therapy on episiotomy pain and wound
healing among postnatal mothers with episiotomy.
41
5. RESULTS
Analysis and interpretation of data
This chapter presents the results of the study conducted to compare the
effectiveness of sitz bath versus infrared therapy in reducing pain and improves wound
healing among postnatal mothers of selected hospitals, in Bangalore.
Analysis is the process of categorizing, ordering, manipulating and
summarizing of data to obtain an answer to the research question. The purpose of
analysis is to reduce the data to an intelligible and interpretable form so that relations
for the research problem can be studied and tested19
.
Objectives of the study
i. To assess the level of pain and wound healing status among postnatal mothers with
episiotomy.
ii. To assess the effectiveness of sitz bath and infrared lamp therapy on episiotomy pain
and wound healing among postnatal mothers.
iii. To compare the effectiveness between sitz bath and infrared lamp therapy on
episiotomy pain and wound healing among postnatal mothers.
iv. To determine an association between pain level & wound healing status with selected
demographic variables

42
Hypotheses:
H1: There is a significant difference between the mean pre test and post test pain &
wound healing scores in sitz bath and infrared lamp therapy group.
H2: There is a significant difference in the mean post test scores between sitz bath and
infrared lamp therapy group.
H3: There is a significant association between pain &wound healing scores with
selected demographic variables in sitz bath and infrared lamp therapy group.
Presentation of data:
To begin with, data were entered in a master sheet, for tabulation and statistical
processing. The findings were presented under the following heading
Section I: Distribution of demographic and clinical characteristics of the subjects.
Pain
Section II: Assessment of episiotomy pain and comparison of pain scores among
control &experimental group.
Section III: Effectiveness of sitz bath on episiotomy pain reduction among control
group.

43
Section IV: Effectiveness of infrared therapy on episiotomy pain reduction among
experimental group.
Section V: Comparing the effectiveness between sitz bath and infrared lamp therapy
on episiotomy pain reduction among control and experimental group.
Section VI: Association between pre test pain scores and selected demographic and
variables.
Wound healing
Section VII: Assessment of episiotomy wound status and comparison wound healing
scores among control &experimental group.
Section VIII: Effectiveness of sitz bath on episiotomy wound healing among control
group.
Section IX: Effectiveness of infrared therapy on episiotomy wound healing among
experimental group.
Section X: Comparing the effectiveness between sitz bath and infrared lamp therapy
on episiotomy wound healing.
Section XI: Association between pre test wound healing scores and selected
demographic variables.
44
Section I: Distribution of demographic and clinical characteristics of the subjects
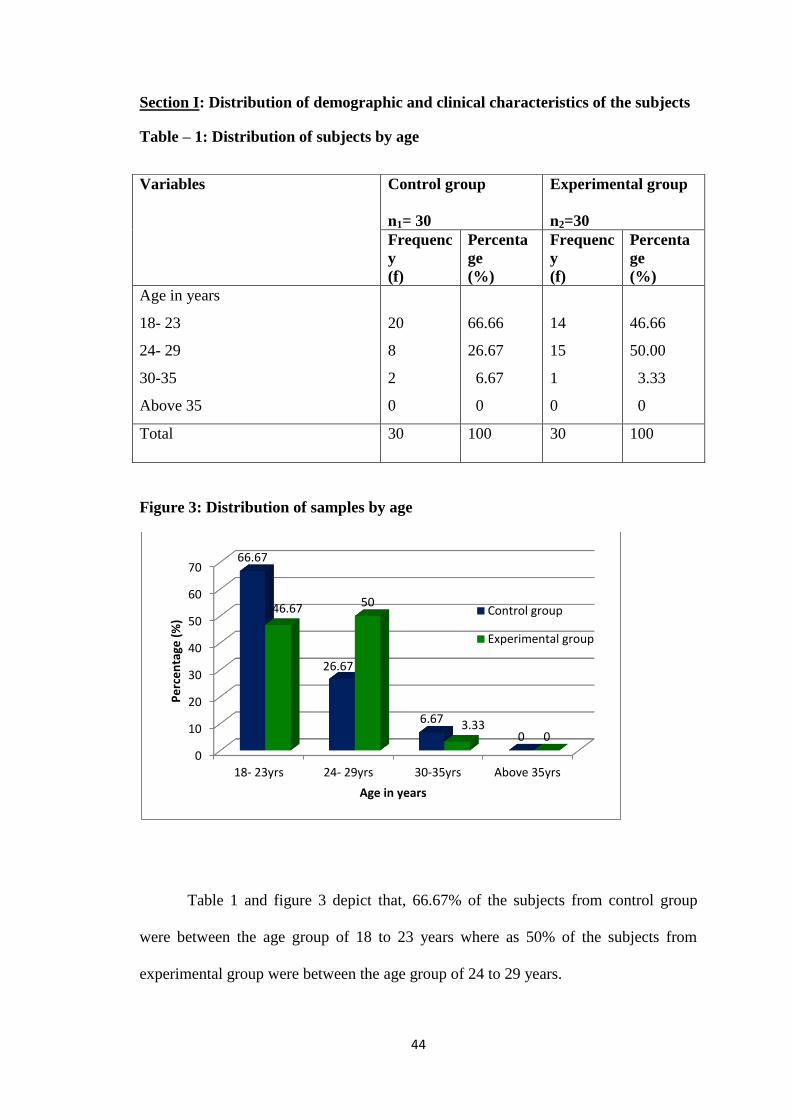
Table – 1: Distribution of subjects by age
Figure 3: Distribution of samples by age
Table 1 and figure 3 depict that, 66.67% of the subjects from control group
were between the age group of 18 to 23 years where as 50% of the subjects from
experimental group were between the age group of 24 to 29 years.
0
10
20
30
40
50
60
70
18- 23yrs 24- 29yrs 30-35yrs Above 35yrs
66.67
26.67
6.67
0
46.67 50
3.33 0
Pe
rce
nta
ge (
%)
Age in years
Control group
Experimental group
Variables
Control group
n1= 30
Experimental group
n2=30
Frequenc
y
(f)
Percenta
ge
(%)
Frequenc
y
(f)
Percenta
ge
(%)
Age in years
a) 18- 23
b) 24- 29
c) 30-35
d) Above 35
20
8
2
0
66.66
26.67
6.67
0
14
15
1
0
46.66
50.00
3.33
0
Total 30 100 30 100
45
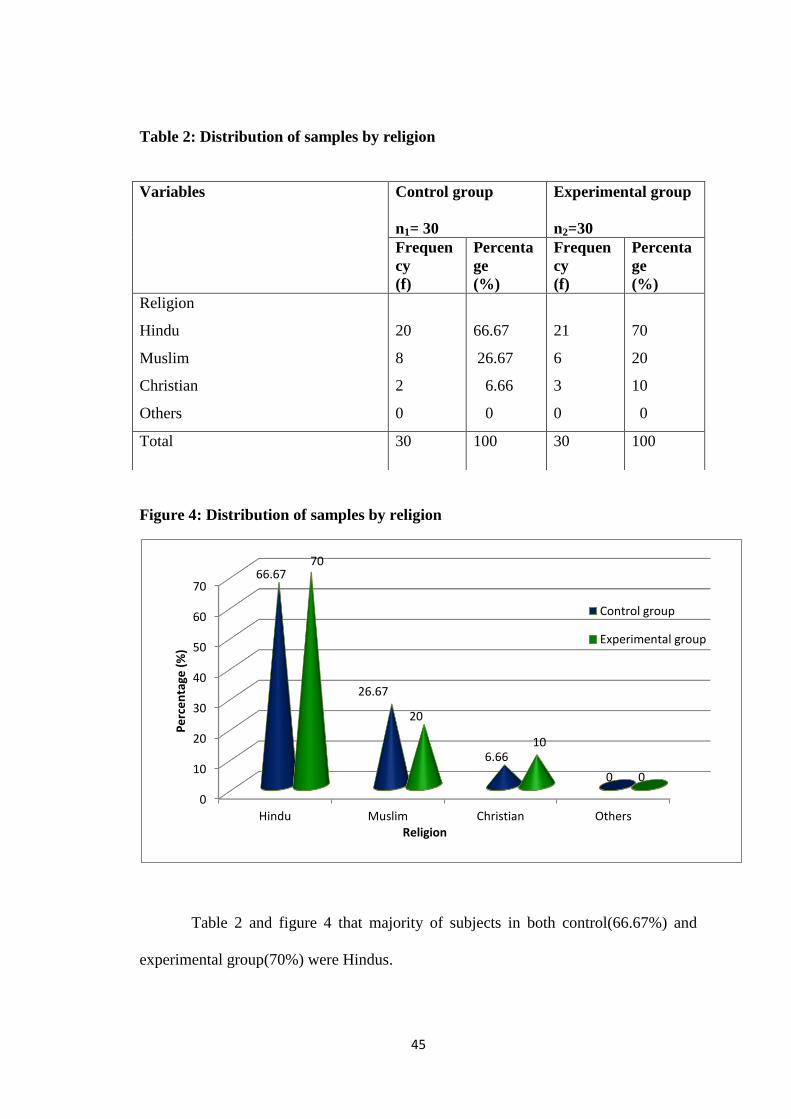
Table 2: Distribution of samples by religion
Figure 4: Distribution of samples by religion
Table 2 and figure 4 that majority of subjects in both control(66.67%) and
experimental group(70%) were Hindus.
0
10
20
30
40
50
60
70
Hindu Muslim Christian Others
66.67
26.67
6.66
0
70
20
10
0
Pe
rce
nta
ge (
%)
Religion
Control group
Experimental group
Variables
Control group
n1= 30
Experimental group
n2=30
Frequen
cy
(f)
Percenta
ge
(%)
Frequen
cy
(f)
Percenta
ge
(%)
Religion
a) Hindu
b) Muslim
c) Christian
d) Others
20
8
2
0
66.67
26.67
6.66
0
21
6
3
0
70
20
10
0
Total 30 100 30 100

46
Table 3: Distribution of samples by education
Figure 5: Distribution of samples by education
Table 3 and figure 5 depict that majority of subjects in both control(73.33%)
and experimental(83.33%) groups were having secondary/diploma education.
0 10 20 30 40 50 60 70 80 90
0
16.67
73.33
10 0
6.67
83.33
10
Pe
rce
nta
ge (
%)
Education
Control group
Experimental group
Variables
Control group
n1= 30
Experimental group
n2=30
Frequency
(f)
Percentage
(%)
Frequency
(f)
Percentage
(%)
Education
a) No formal
b) Primary
c) Secondary/Diploma
d) Graduation and above
0
5
22
3
0
16.66
73.33
10
0
2
25
3
0
6.66
83.33
10
Total 30 100 30 100
47
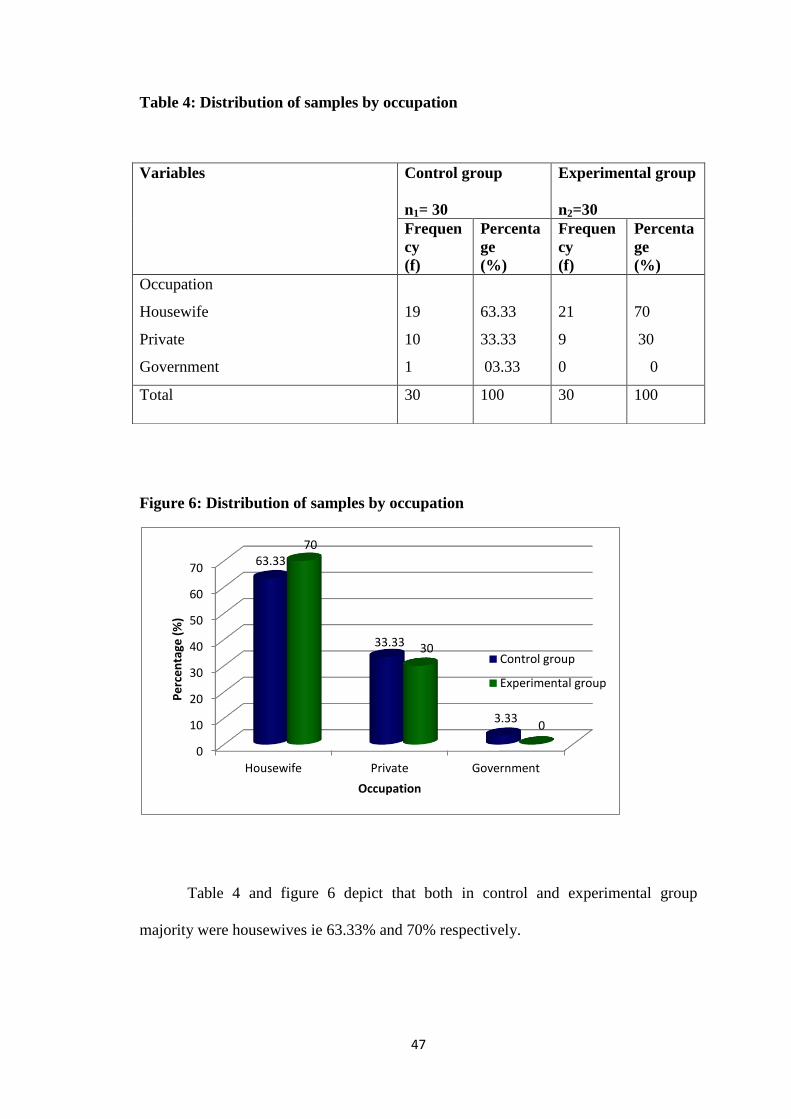
Table 4: Distribution of samples by occupation
Figure 6: Distribution of samples by occupation
Table 4 and figure 6 depict that both in control and experimental group
majority were housewives ie 63.33% and 70% respectively.
Variables
Control group
n1= 30
Experimental group
n2=30
Frequen
cy
(f)
Percenta
ge
(%)
Frequen
cy
(f)
Percenta
ge
(%)
Occupation
a) Housewife
b) Private
c) Government
19
10
1
63.33
33.33
03.33
21
9
0
70
30
0
Total 30 100 30 100
0
10
20
30
40
50
60
70
Housewife Private Government
63.33
33.33
3.33
70
30
0
Pe
rce
nta
ge (
%)
Occupation
Control group
Experimental group
48
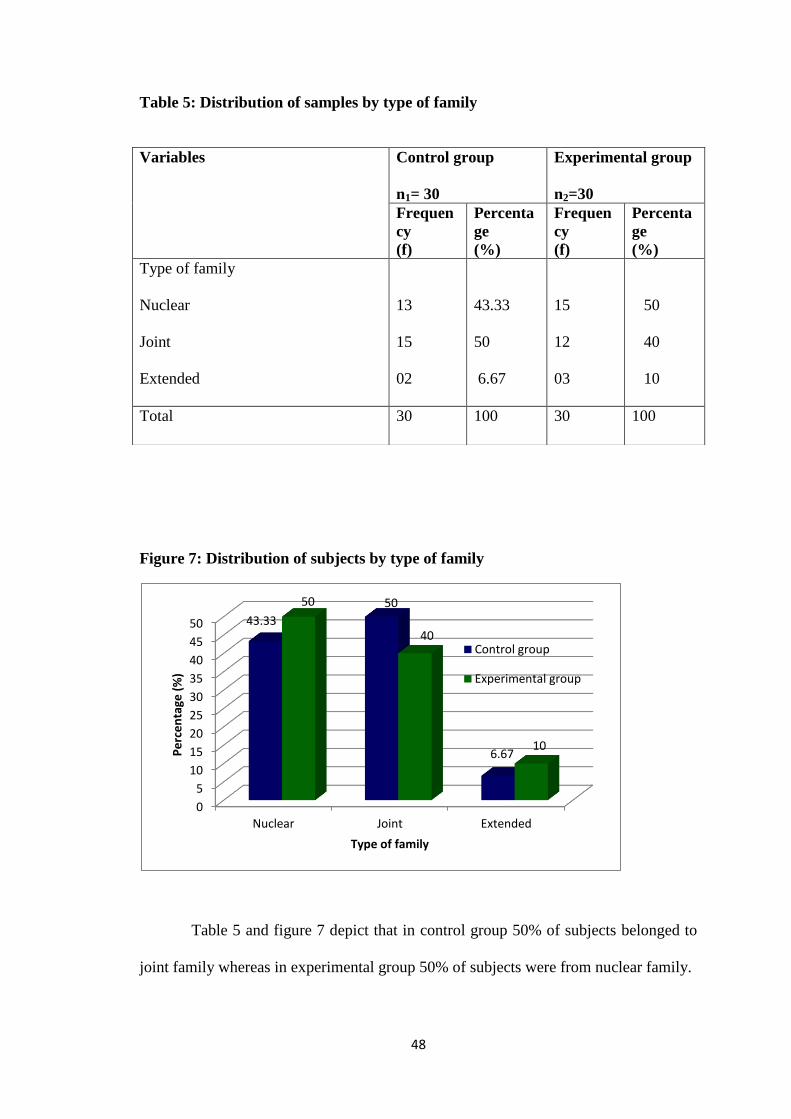
Table 5: Distribution of samples by type of family
Figure 7: Distribution of subjects by type of family
Table 5 and figure 7 depict that in control group 50% of subjects belonged to
joint family whereas in experimental group 50% of subjects were from nuclear family.
0
5
10
15
20
25
30
35
40
45
50
Nuclear Joint Extended
43.33
50
6.67
50
40
10 Pe
rce
nta
ge (
%)
Type of family
Control group
Experimental group
Variables
Control group
n1= 30
Experimental group
n2=30
Frequen
cy
(f)
Percenta
ge
(%)
Frequen
cy
(f)
Percenta
ge
(%)
Type of family
a) Nuclear
b) Joint
c) Extended
13
15
02
43.33
50
6.67
15
12
03
50
40
10
Total 30 100 30 100
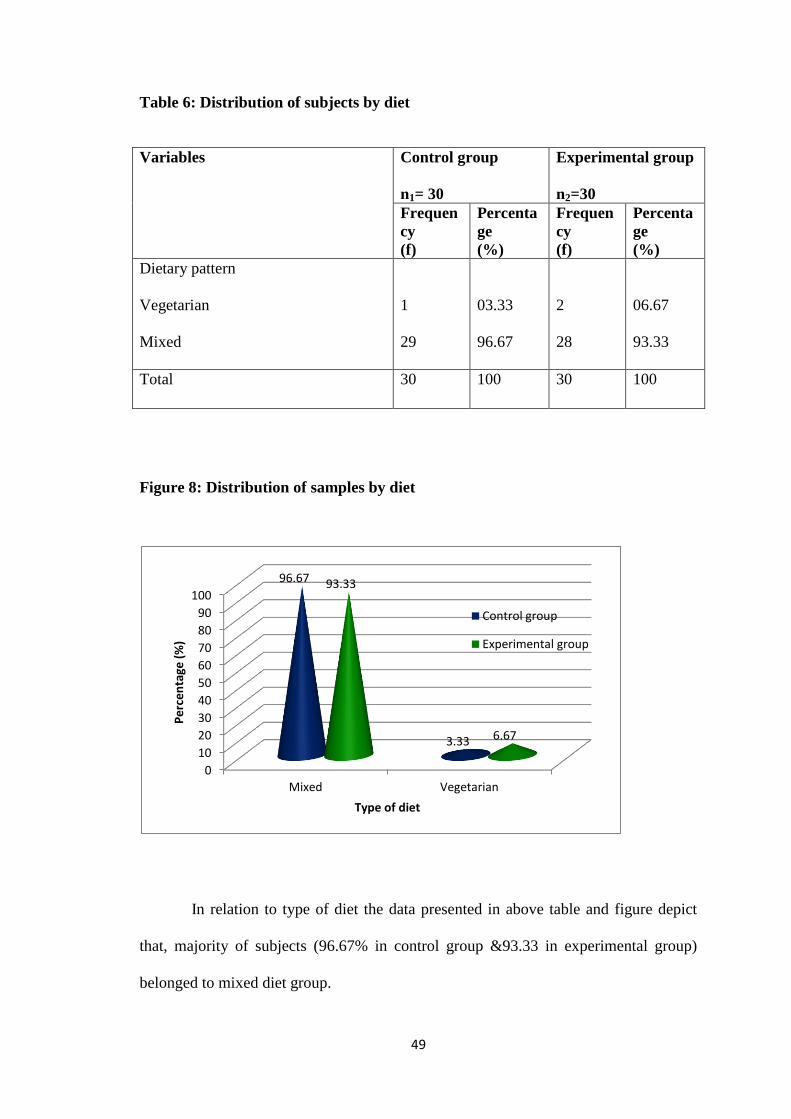
49
Table 6: Distribution of subjects by diet
Figure 8: Distribution of samples by diet
In relation to type of diet the data presented in above table and figure depict
that, majority of subjects (96.67% in control group &93.33 in experimental group)
belonged to mixed diet group.
0
10
20
30
40
50
60
70
80
90
100
Mixed Vegetarian
96.67
3.33
93.33
6.67
Pe
rce
nta
ge (
%)
Type of diet
Control group
Experimental group
Variables
Control group
n1= 30
Experimental group
n2=30
Frequen
cy
(f)
Percenta
ge
(%)
Frequen
cy
(f)
Percenta
ge
(%)
Dietary pattern
a) Vegetarian
b) Mixed
1
29
03.33
96.67
2
28
06.67
93.33
Total 30 100 30 100

50
Table 6: Distribution of samples by place of living
Figure 8: Distribution of samples by place of living
The table 6 and figure 8 reveals that majority of subjects from both control and
experimental group were living in urban area ie 80% and 60% respectively.
0
10
20
30
40
50
60
70
80
Urban Rural
80
20
60
40
Pe
rce
nta
ge(%
)
Place of living
control group
Experimental group
Variables
Control group
n1= 30
Experimental group
n2=30
Frequenc
y
(f)
Percenta
ge
(%)
Frequenc
y
(f)
Percenta
ge
(%)
Place of living
a) Rural
b) Urban
6
24
20
80
9
21
40
60
Total 30 100 30 100

51
Table 8: Distribution of subjects by parity
Figure 10: Distribution of subjects by parity
The table 8 and figure 10 depicts that 63.33% of subjects were primiparas and
in control group and in experimental group majority (53.33%) were multiparas
0
10
20
30
40
50
60
70
Primi Multi Grand multi
63.33
36.67
0
46.667
53.33
0
Pe
rce
nta
ge (
%)
Parity
Control group
Experimental group
Variables
Control group
n1= 30
Experimental group
n2=30
Frequenc
y
(f)
Percenta
ge
(%)
Frequenc
y
(f)
Percenta
ge
(%)
Parity
a) Primi
b) Multi
c) Grand multi
19
11
0
63.33
36.66
0.0
14
16
0
46.66
53.33
0.0
Total 30 100 30 100

52
Table 9: Distribution of samples by type of episiotomy
Figure11: Distribution of samples by type of episiotomy
It revealed from the figure 9 and table 11 that 100% subjects form control
group and 80% of subjects from experimental group were having right mediolateral
episiotomy (RMLE).
0
10
20
30
40
50
60
70
80
90
100
Median Lateral RMLE LMLE
0 0
100
0 0 0
80
20 Pe
rce
nta
ge (
%)
Type of episiotomy
Control group
Experimental group
Variables
Control group
n1= 30
Experimental group
n2=30
Frequenc
y
(f)
Percenta
ge
(%)
Frequenc
y
(f)
Percenta
ge
(%)
Type of episiotomy
a) Median
b) Lateral
c) RMLE
d) LMLE
0
0
30
0
0
0
100
0
0
0
28
2
0
0
80
20
Total 30 100 30 100
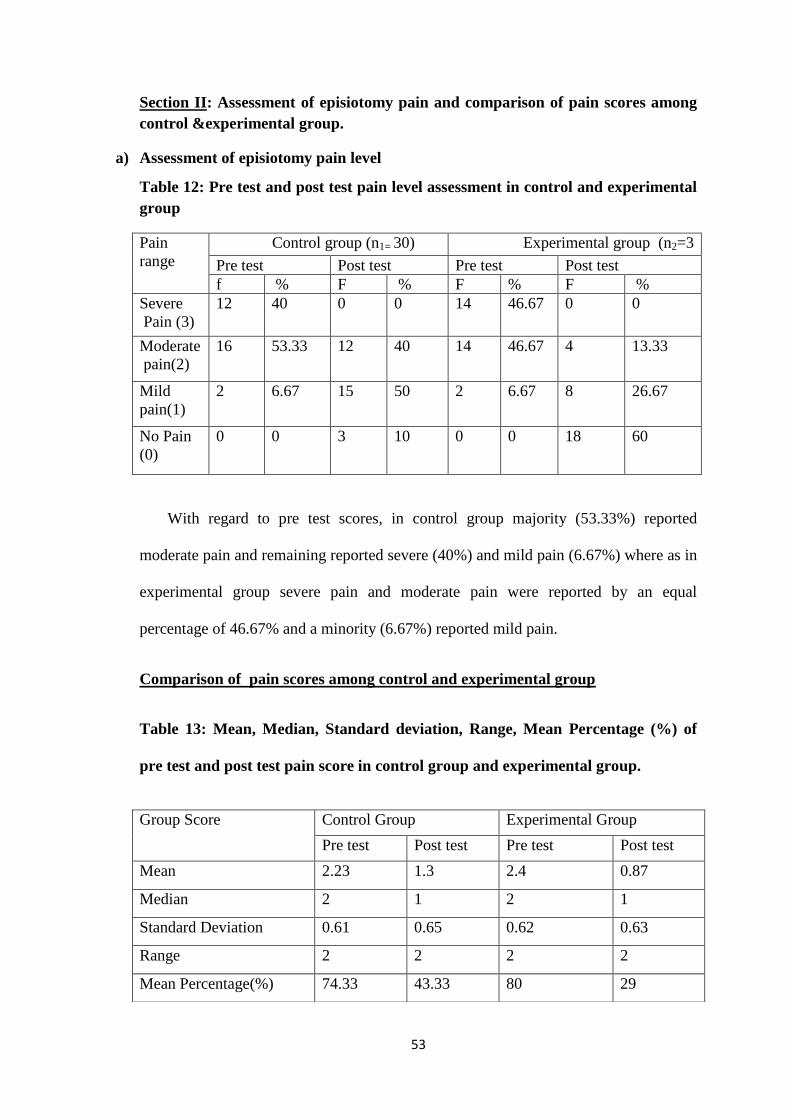
53
Section II: Assessment of episiotomy pain and comparison of pain scores among
control &experimental group.
a) Assessment of episiotomy pain level
Table 12: Pre test and post test pain level assessment in control and experimental
group
Pain
range
Control group (n1= 30) Experimental group (n2=3
Pre test Post test Pre test Post test
f % F % F % F %
Severe
Pain (3)
12 40 0 0 14 46.67 0 0
Moderate
pain(2)
16 53.33 12 40 14 46.67 4 13.33
Mild
pain(1)
2 6.67 15 50 2 6.67 8 26.67
No Pain
(0)
0 0 3 10 0 0 18 60
With regard to pre test scores, in control group majority (53.33%) reported
moderate pain and remaining reported severe (40%) and mild pain (6.67%) where as in
experimental group severe pain and moderate pain were reported by an equal
percentage of 46.67% and a minority (6.67%) reported mild pain.
Comparison of pain scores among control and experimental group
Table 13: Mean, Median, Standard deviation, Range, Mean Percentage (%) of
pre test and post test pain score in control group and experimental group.
Group Score Control Group Experimental Group
Pre test Post test Pre test Post test
Mean 2.23 1.3 2.4 0.87
Median 2 1 2 1
Standard Deviation 0.61 0.65 0.62 0.63
Range 2 2 2 2
Mean Percentage(%) 74.33 43.33 80 29
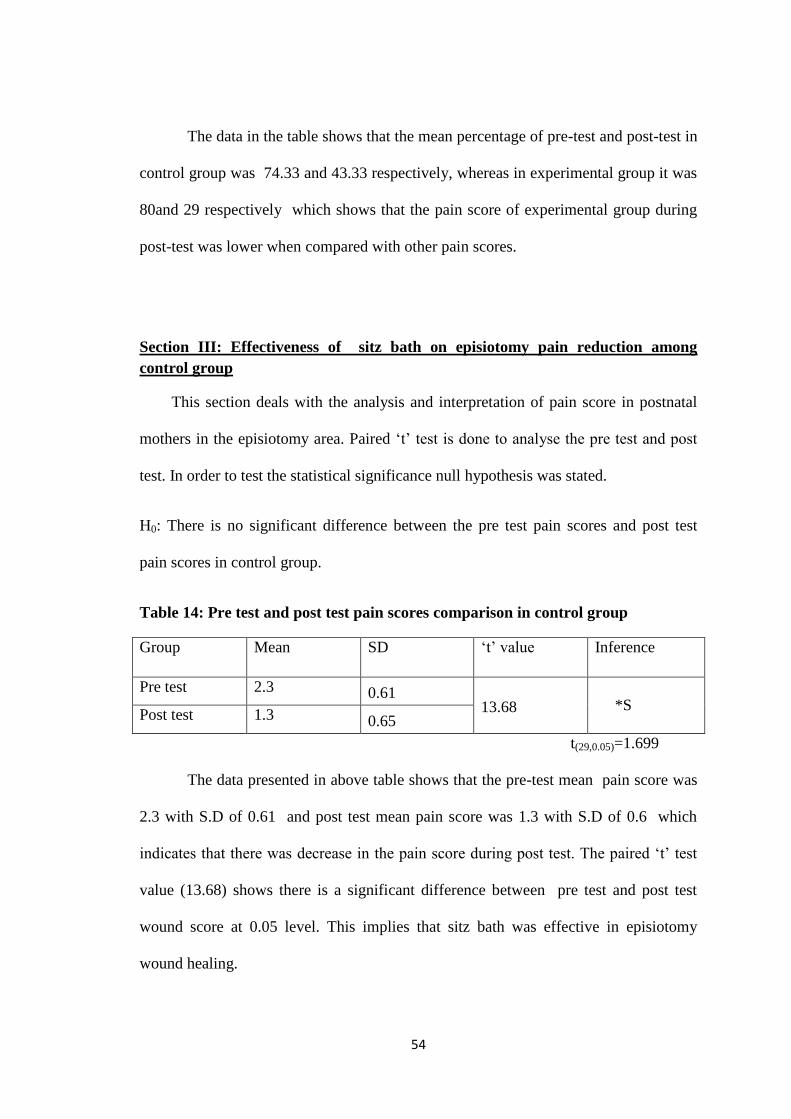
54
The data in the table shows that the mean percentage of pre-test and post-test in
control group was 74.33 and 43.33 respectively, whereas in experimental group it was
80and 29 respectively which shows that the pain score of experimental group during
post-test was lower when compared with other pain scores.
Section III: Effectiveness of sitz bath on episiotomy pain reduction among
control group
This section deals with the analysis and interpretation of pain score in postnatal
mothers in the episiotomy area. Paired ‘t’ test is done to analyse the pre test and post
test. In order to test the statistical significance null hypothesis was stated.
H0: There is no significant difference between the pre test pain scores and post test
pain scores in control group.
Table 14: Pre test and post test pain scores comparison in control group
Group Mean SD ‘t’ value Inference
Pre test 2.3 0.61 13.68
*S Post test 1.3 0.65
t(29,0.05)=1.699
The data presented in above table shows that the pre-test mean pain score was
2.3 with S.D of 0.61 and post test mean pain score was 1.3 with S.D of 0.6 which
indicates that there was decrease in the pain score during post test. The paired ‘t’ test
value (13.68) shows there is a significant difference between pre test and post test
wound score at 0.05 level. This implies that sitz bath was effective in episiotomy
wound healing.

55
Section IV: Effectiveness of infrared therapy on episiotomy pain reduction among
experimental group
This section deals with the analysis and interpretation of pain score in postnatal
mothers in the episiotomy area. Paired ‘t’ test is done to analyse the pre test and post
test. In order to test the statistical significance null hypothesis was stated.
H0: There is no significant difference between the pre test pain scores and post test
pain scores in experimental group.
Table 15: Pre test and post test pain scores comparison in experimental group
Group Mean SD ‘t’ value Inference
Pre test 2.4 0.62 14.69
*S Post test 0.87 0.63
t(29,0.05)=1.699
The data presented in above table shows that the pre-test mean pain score was
2.4 with S.D of 0.62 and post test mean pain score was 0.87 with S.D of 0.6 3 which
indicates that there was decrease in the pain score during post test. The paired ‘t’ test
value (14.69) shows there is a significant difference between pre test and post test pain
score at 0.05 level. This implies that infrared therapy was effective in episiotomy
wound healing.
The student t test shows that infrared therapy is effective in reducing
episiotomy pain as the calculated t value is greater than the table t value.

56
Section V: Comparing the effectiveness between sitz bath and infrared lamp
therapy on episiotomy pain reduction
This section deals with the analysis and interpretation of pain score after sitz bath
and infrared therapy on postnatal mothers. Student ‘t’ test was used to compare the
effectiveness between sitz bath and infrared therapy in control and experimental
group. In order to test the statistical significance null hypothesis is stated.
H0: There is no significant difference between the post-test pain scores of control and
experimental group.
Table 16: Comparison of Post test pain scores in control and experimental group
Group Mean SD ‘t’ value Inference
Control 1.3 0.65 2.62
*S
Experimental 0.87 0.63
t(58,0.05)=1.67
The data presented in above table shows that mean post test score of control
group (1.3) was higher than the experimental group score (0.87). Student‘t’ test value
(2.62) shows that there is significant difference between post- test pain scores of
control and experimental group. It means that infrared therapy was effective in
episiotomy pain reduction

57
Section VI: Association between pre test pain scores and selected demographic
and clinical variables
a) Control group
Demographic
variables
Responses Overall pre test
knowledge
Chi-
square
value
df
Below
median
Above
median
Age (yrs)
18-23 1 19
0.67NS
2 24-29 1 7
>35 0 2
Religion
Hindu 2 18
1.07NS
2 Muslim 0 8
Christian 0 2
Education
Primary 0 18
0.78NS
2 Secondary 2 8
Graduation 0 2
Occupation
House wife 2 18
1.72NS
2
Private 0 9
Family
Nuclear 1 12
1.17NS
2 Joint 1 14
Extended 0 2
Diet
Vegetarian 0 1
0.07NS
1
Mixed 2 27
Place of living
Rural 2 6
0.54NS
1
Urban 20 22
Parity Primi 1 8
0.16NS
1
Multi 1 10

58
a) Experimental group
Demographic
variables
Responses Overall pre test
knowledge
Chi-
square
value
Df
Below
median
Above
median
Age (yrs) 18-23 2 13
2.14NS
2 24-29 0 14
>35 0 1
Religion
Hindu 0 21
8.57S
2 Muslim 2 4
Christian 0 3
Education
Primary 0 2
0.43NS
2 Secondary 2 23
Graduation 0 3
Occupation House wife 1 31
0.59NS
2
Private 1 7
Family Nuclear 2 13
2.14NS
2 Joint 0 12
Extended 0 3
Diet
Vegetarian 0 2
0.15NS
1
Mixed 2 26
Place of living Rural 0 9
0.92NS
1
Urban 2 19
Parity Primi 1 `13
0.10NS
1
Multi 1 15
Episiotomy RMLE 0 2
0.15NS
1
LMLE 2 26

59
This section explains association between episiotomy pain scores and selected
demographic variables. For the purpose of establishing the association between the
demographic variables and the overall pain score is divided into two categories as
below median and above median The chi – square test analysis shows that there is no
significant association between pre test episiotomy wound scores and selected
demographic & clinical variables at 0.05 level in both control and experimental group
with an exemption of religion which has shown significant association (x2= 8.57)only
in experimental group.
WOUND HEALING GRADING
Section VII: Assessment of episiotomy wound status and comparison pain scores
among control & experimental group
a) Assessment of episiotomy wound status
Pre test and post test wound healing grading in control and experimental group
With regard to pre-test scores, all subjects (100%) had moderate wound
infection in both control and experimental group.
Wound healing Control group(n1=30) Experimental group(n2=30)
Pre test Post test Pre test Post test
f % F % F % F %
No infection
(0)
0 0 0 0 0 0 0 0
Mild infection
(1-5)
0 0 7 23.33 0 0 5 16.67
Moderate infection
(6-10)
30 100 23 76.67 30 100 25 83.33
Severe Pain
(11-15)
0 0 0 0 0 0 0 0
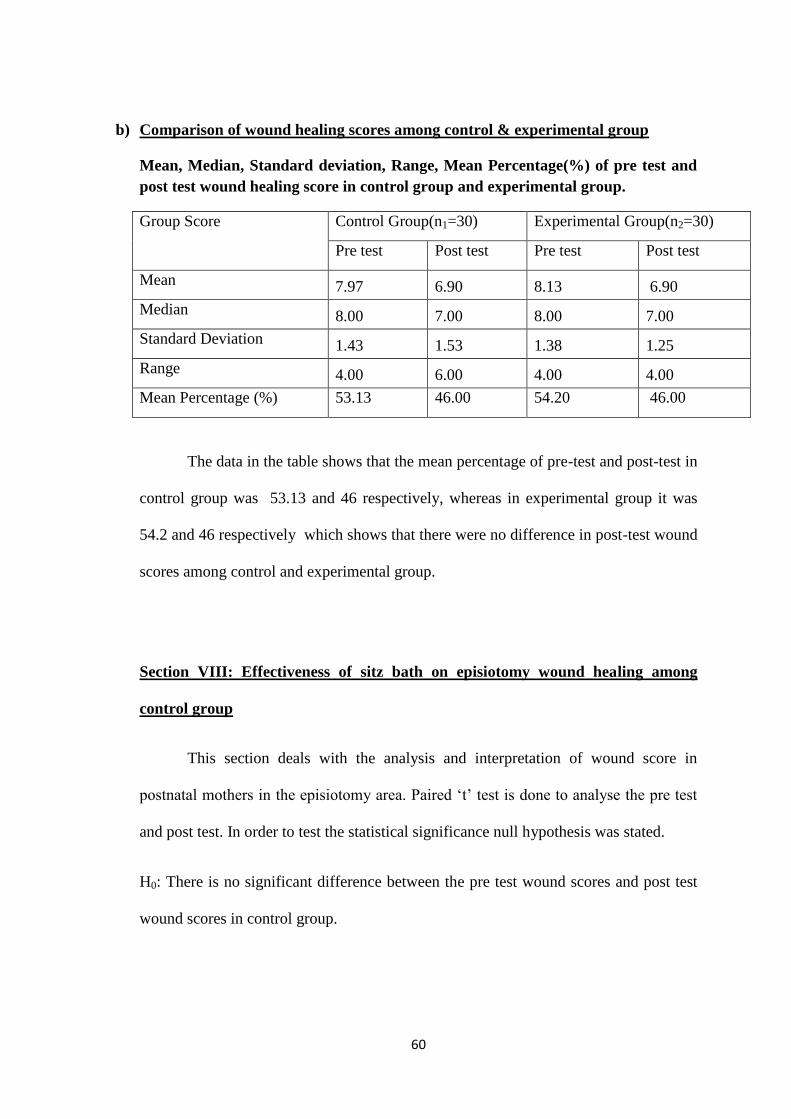
60
b) Comparison of wound healing scores among control & experimental group
Mean, Median, Standard deviation, Range, Mean Percentage(%) of pre test and
post test wound healing score in control group and experimental group.
Group Score Control Group(n1=30) Experimental Group(n2=30)
Pre test Post test Pre test Post test
Mean 7.97 6.90 8.13 6.90
Median 8.00 7.00 8.00 7.00
Standard Deviation 1.43 1.53 1.38 1.25
Range 4.00 6.00 4.00 4.00
Mean Percentage (%) 53.13 46.00 54.20 46.00
The data in the table shows that the mean percentage of pre-test and post-test in
control group was 53.13 and 46 respectively, whereas in experimental group it was
54.2 and 46 respectively which shows that there were no difference in post-test wound
scores among control and experimental group.
Section VIII: Effectiveness of sitz bath on episiotomy wound healing among
control group
This section deals with the analysis and interpretation of wound score in
postnatal mothers in the episiotomy area. Paired ‘t’ test is done to analyse the pre test
and post test. In order to test the statistical significance null hypothesis was stated.
H0: There is no significant difference between the pre test wound scores and post test
wound scores in control group.

61
Table 17: Pre test and post test wound healing scores in control group
Group Mean SD ‘t’ value Inference
Pre test 7.97 1.43
4.96
S Post test
6.86 1.53
t(29,0.05)=1.699
The data presented in above table shows that the pre-test mean wound score
was 7.97 with S.D of 1.43 and post test mean wound score was 6.86 with S.D of 1.53
which indicates that there was decrease in the wound score during post test. The
paired‘t’ test value (4.96) shows there is a significant difference between pre test and
post test wound score at 0.05 level. This implies that sitz bath was effective in
episiotomy wound healing.
Section IX: Effectiveness of infrared therapy on episiotomy wound healing among
experimental group
This section deals with the analysis and interpretation of wound score in postnatal
mothers in the episiotomy area. Paired ‘t’ test is done to analyse the pre test and post
test. In order to test the statistical significance null hypothesis was stated.
H0: There is no significant difference between the pre test wound scores and post test
wound scores in experimental group.

62
Table 18: Pre test and post test wound healing scores in experimental group
Group Mean SD ‘t’ value Inference
Pre test 8.13 1.38 6.59
S Post test 6.93 1.25
t (29,0.05)=1.699
The data presented in above table shows that the pre-test mean wound score
was 8.13 with S.D of 1.38 and post test mean wound score was 6.93 with S.D of 1.25
which indicates that there was decrease in the wound score during post test. The paired
‘t’ test value (6.59) shows there is a significant difference between pre test and post
test wound score at 0.05 level. This implies that infrared therapy was effective in
episiotomy wound healing.
Section X: Comparing the effectiveness between sitz bath and infrared lamp
therapy on episiotomy wound healing among control & experimental group
This section deals with the analysis and interpretation of wound healing score
after sitz bath and infrared therapy on postnatal mothers. Student ‘t’ test was used to
compare the effectiveness between sitz bath and infrared therapy in control and
experimental group. In order to test the statistical significance null hypothesis is stated.
H0: There is no significant difference between the post test wound healing scores of
control and experimental group.

63
Table 19: Post test wound healing scores in control and experimental group
Group Mean SD ‘t’ value Inference
Control 5.13 1.67 0.19
NS Experimental 5.07 1.34
t (58, 0.05)=1.67
The data presented in above table shows that mean post test score of
experimental group (5.07) was slightly lower than the control group score (5.13).
Student ‘t’ test value (0.19) shows that there is no significant difference between
post- test wound scores of control and experimental group. It means that there is no
comparable difference among sitz bath and infrared therapy in promoting episiotomy
wound healing.
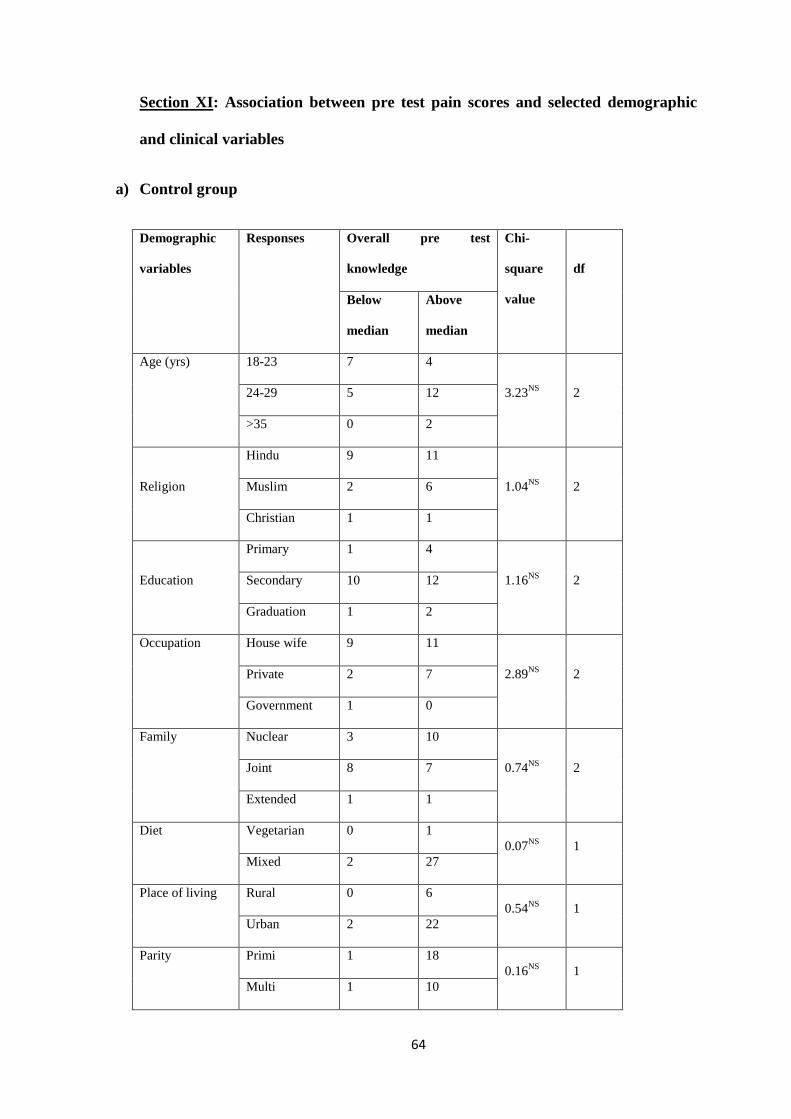
64
Section XI: Association between pre test pain scores and selected demographic
and clinical variables
a) Control group
Demographic
variables
Responses Overall pre test
knowledge
Chi-
square
value
df
Below
median
Above
median
Age (yrs) 18-23 7 4
3.23NS
2 24-29 5 12
>35 0 2
Religion
Hindu 9 11
1.04NS
2 Muslim 2 6
Christian 1 1
Education
Primary 1 4
1.16NS
2 Secondary 10 12
Graduation 1 2
Occupation House wife 9 11
2.89NS
2 Private 2 7
Government 1 0
Family Nuclear 3 10
0.74NS
2 Joint 8 7
Extended 1 1
Diet
Vegetarian 0 1
0.07NS
1
Mixed 2 27
Place of living Rural 0 6
0.54NS
1
Urban 2 22
Parity Primi 1 18
0.16NS
1
Multi 1 10
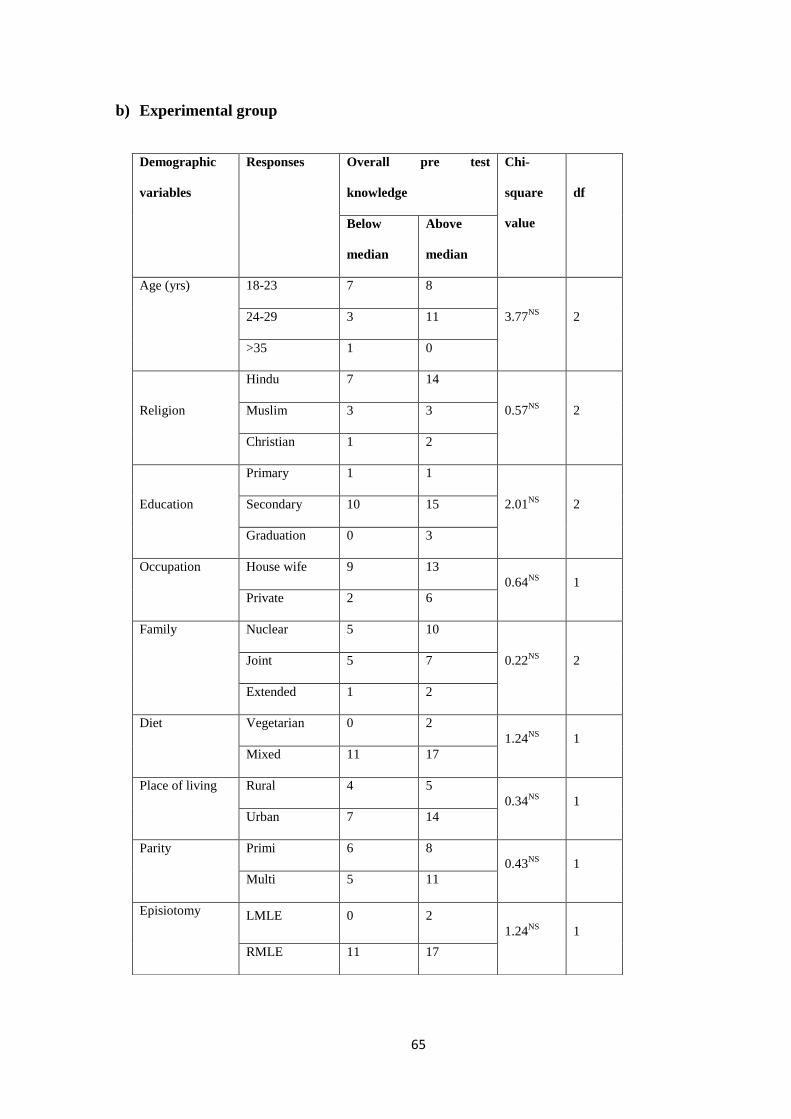
65
b) Experimental group
Demographic
variables
Responses Overall pre test
knowledge
Chi-
square
value
df
Below
median
Above
median
Age (yrs) 18-23 7 8
3.77NS
2 24-29 3 11
>35 1 0
Religion
Hindu 7 14
0.57NS
2 Muslim 3 3
Christian 1 2
Education
Primary 1 1
2.01NS
2 Secondary 10 15
Graduation 0 3
Occupation House wife 9 13
0.64NS
1
Private 2 6
Family Nuclear 5 10
0.22NS
2 Joint 5 7
Extended 1 2
Diet
Vegetarian 0 2
1.24NS
1
Mixed 11 17
Place of living Rural 4 5
0.34NS
1
Urban 7 14
Parity Primi 6 8
0.43NS
1
Multi 5 11
Episiotomy LMLE 0 2
1.24NS
1
RMLE 11 17

66
This section explains association between episiotomy wound scores and selected
demographic variables. For the purpose of establishing the association between the
demographic variables and the overall wound score is divided into two categories as
below median and above median The chi – square test analysis shows that there is no
significant association between pre test episiotomy wound scores and selected
demographic & clinical variables such as age, religion, education, occupation, type of
family, diet, place of living, parity and episiotomy at 0.05 level in both control and
experimental group.
Note:
Critical value for 1 degree of freedom at 5%level of significance=3.841.
Critical value for 1 degree of freedom at 5%level of significance=5.99
SUMMARY
This chapter has dealt with the analysis and interpretation of the findings of the
study. Sitz bath were received by control group and infrared therapy was administered
for experimental group for three days after conducting pre-test. Post test conducted
after the completion of three days therapy. The data obtained was entered in the master
sheet and computed using descriptive and inferential statistics. The result concluded
that mothers who had undergone the treatment of infrared light therapy expressed
decreased pain intensity compared to mothers who had undergone the treatment of sitz
bath. With regard to wound healing, infrared light therapy and sitz bath were found to
have same effect in healing and condition of healing.

67
6. DISCUSSION
In order to find meaningful answers to research questions, the collected data
must be processed, analyzed in an orderly and coherent fashion, so that patterns and
relationship can be discussed.
The present study was done to compare the effectiveness of sitz bath versus
infrared lamp therapy on episiotomy pain and wound healing among post natal
mothers at selected hospitals, Bangalore.
In this study, quasi experimental pre-test and post-test design with a
comparison group was adopted to compare the effectiveness of sitz bath versus
infrared lamp therapy on episiotomy pain and wound healing. The study was
conducted at Kempegowda Institute of Medical Science, Hospital and Research
Centre, Bangalore. The sample size comprised of 60 postnatal mothers (30 in control
&30 in experimental group). The purposive sampling technique was used to select the
sample. Data collected from the subjected were tabulated, analyzed and interpreted by
using descriptive and inferential statistics, based on the objectives of the study.
Findings of the study: The findings of the study have been organized and
discussed under the following sections:
The findings of the study are discussed under the following headings:
1. Demographic characteristics of the subjects.
2. Assessment of level of pain and wound healing status among postnatal mothers.
3. Evaluation of effectiveness of sitz bath and infrared lamp therapy on episiotomy pain
and wound healing.
4. Association between demographic variables and pre test pain & wound healing scores.
68
5. Discussion on testing of the hypothesis.
DEMOGRAPHIC CHARACTERISTICS OF THE SUBJECTS.
The findings of the study shows that,
1. Age:
In control group, most of the subjects that is 66.66% were between 18-25 years,
26.67% belonged to 24 -29 years, and remaining 6.67 % belonged to 26-33 years.
In experimental group, most of the subjects that is 50% were between 18-25
years, 46.67% belonged to 24 -29 years, and remaining 3.33 % belonged to 26-33
years.
2. Religion:
In control group, majority 66.67% of the subjects belonged to Hindu religion,
26.67% belonged to Muslim and remaining 6.66% belonged to Christian.
Similarly in experimental group, majority 70% belonged to Hindu religion,
20% belonged to Muslim and remaining 10% belonged to Christian.
3. Education:
In control group, majority 73.33% of subjects had secondary/ Diploma
education, 16.66% had primary education, and 10% had attained graduation.
In experimental group, majority 83.33% of subjects had secondary/ Diploma
education, 6.66% had primary education, and 10% had attained graduation.
4. Occupation:
In control group, majority 63.33% were house wives, 33.33% were private
employees and remaining 03.33% were government employees.
Similarly, in experimental group, majority 70% were house wives, and
remaining 30% were private employees.

69
5. Type of family:
In control group, 50% of the subjects belonged to joint family, 43.33%
belonged to nuclear family and remaining 6.67% belonged to extended family.
In experimental group, 50% of the subjects belonged to joint family, 40%
belonged to nuclear family and remaining 10% belonged to extended family.
6. Diet:
In control group, majority 96.67% of the subjects belonged to mixed diet
group, and remaining 3.33% belonged to vegetarian diet group.
Similarly in experimental group, majority 93.33% of the subjects belonged to
mixed diet group, and remaining 6.67% belonged to vegetarian diet group.
7. Place of living:
In control group, majority of the subjects that is 80% were from urban area and
remaining 20% from rural area.
Similarly in experimental group, majority of the subjects that is 60% were from
urban area and remaining 40% from rural area.
8. Parity:
In control group, majority 63.33% of subjects were primiparas and remaining
36.67% were multiparas.
In experimental group, 53.33% of subjects were multiparas and remaining
46.67% were primiparas.
9. Type of episiotomy:
In control group, all subjects (100%) had right mediolateral episiotomy.
In experimental group, majority 80% had right mediolateral episiotomy and remaining
20% had left mediolateral episiotomy.

70
The findings are supported by a similar study conducted to identifying the
frequency, the types and the criteria adopted to recommend episiotomy, by De Oliveira
SM and Miquilini EC in Portuguese. In this study 12 doctors and 12 nurses who attend
women at birth interviewed. The results show that episiotomy was performed in 76.2%
of the normal births; the most frequent indications were perineal rigidity and
primiparity. The most mentioned type was the right medio- lateral episiotomy (92%),
and the justifications were: it was learned during academic formation(25.9%); it is
adopted routinely((19.4%); with it there is a lesser chance for causing lesions to the
anal sphincter(16.1%); with it there is a lesser risk of complications(16.1%)50
.
ASSESSMENT OF LEVEL OF PAIN AND WOUND HEALING STATUS
AMONG POSTNATAL MOTHER
The present study confirms that with regard to pre test scores, in control group
majority (53.33%) reported moderate pain and remaining reported severe (40%) and
mild pain (6.67%) where as in experimental group severe pain and moderate pain were
reported by an equal percentage of 46.67% and a minority (6.67%) reported mild pain.
All (100%) had moderate wound infection in both control and experimental group.
The findings of related to the pain level in the present study supported by a
similar study conducted by Imarengiaye CO and Andet AB in Nigeria to identify the
place of postpartum perineal pain as morbidity in the immediate postpartum period.
All women over 18 years who were delivered of a live neonate vaginally and were in
hospital for at least 3 days after delivery were studied. The results revealed that
episiotomy was twice likely to produce perineal pain than no trauma group at time of

71
discharge on day 3 (RR=2.4). The study concluded that perineal pain increased with
perineal trauma and episiotomy and the current management of post partum perineal
pain is inadequate51
.
The findings of related to the wound healing status in the present study supported
by a similar study conducted by Uygur D, Yesildaglar N in Turky to determine the
outcome of episiotomy. In the study period, there were 37 patients with episiotomy
wound dehiscence. Infection was obvious cause of dehiscence in the majority (25 out
of 37) of women. The study concluded that the rate of episiotomy wound infection was
high in the study population52
.
EVALUATION OF EFFECTIVENESS OF SITZ BATH AND INFRARED
LAMP THERAPY ON EPISIOTOMY PAIN AND WOUND HEALING.
The present study shows that there was a considerable improvement of the
episiotomy pain and wound healing scores after administration of the sitz bath and
infrared lamp therapy and is statistically established as significant. In control group,
mean post pain and wound scores (1.3 & 6.9 respectively) are lower than that of the
mean pre test pain & wound scores (2.23 & 7.9 respectively). Similarly in
experimental group, mean post pain and wound scores (0.84 & 6.9respectively) is
lower than that of the mean pre test pain & wound scores (2.4 & 8.13 respectively).
This implies that sitz bath and infrared therapy was effective in reducing episiotomy
pain and wound healing. Similar results were also found in the studies reviewed.

72
The findings of the present study supported by a similar study conducted by
V. Dhanalakshmi in Coimbatore, India to assess the effectiveness of infrared therapy
and sitz bath. Two experimental group were selected in terms of infra red lamp
therapy and sitz bath, which influence the wound healing process and pain perception.
The results revealed that sitz bath and infrared lamp therapy and sitz bath found to be
effective in healing episiotomy and mothers underwent for infra red lamp therapy
experienced decreased pain intensity (t=2.82) and the results were statistically
significant43
.
ASSOCIATION BETWEEN DEMOGRAPHIC VARIABLES AND PRE TEST
PAIN & WOUND SCORES.
In this study when demographical variables were analyzed, there was no
significant association found at 0.05 level between pre-test pain & wound scores of
postnatal mothers and demographic variables in both control and experimental group. .
However, there was a significant association only between religion and the pre-test
pain scores in experimental group (x2=8.57 is more than the table value at 0.05 level of
significance).
The finding of the present study was similar to a study conducted by John
Esther on “Effectiveness of infrared therapy on healing episiotomy wound in postnatal
mothers” in which there was no association between healing of episiotomy wound
with selected demographic and obstetrical variables such as age, education, income,
obstetrical score, mode of delivery, number of vaginal examinations, haemoglobin,
mother’s weight and previous infection41
.
73
DISCUSSION ON TESTING OF THE HYPOTHESIS.
H1: There is a significant difference between the mean pre test and post test pain &
wound healing scores in sitz bath and infrared lamp therapy group.
The research hypothesis H1 stated in the study is accepted since there is significant
difference between the mean pre test and post test pain & wound healing scores in
control and experimental group at P<0.05 level after administration of sitz bath and
infrared lamp therapy administration respectively.
H2: There is a significant difference in the mean post test scores between sitz bath and
infrared lamp therapy group.
The investigator accepts the research hypothesis H2 as there is significant difference in
the mean post test pain scores between sitz bath and infra red lamp therapy group.
However, significant difference in the mean post test wound scores was not evident.
H3: There is a significant association between pain &wound healing scores with
selected demographic variables in sitz bath and infrared lamp therapy group.
The investigator accepts the research hypothesis H3 because there is significant
association between religions in experimental group with pre test pain scores.

74
SUMMARY
This chapter dealt with the discussion of results under various headings.
Demographical variables discussed in the beginning section followed by effectiveness
of sitz bath and infrared therapy and its association with demographic variables. The
result was discussed in terms of objectives and the hypothesis formulated.

75
6. CONCLUSION
This chapter presents the conclusion which has drawn based on the findings of
the study. It also include the implications for nursing practice, education,
administration and research
The pain and delayed healing of the episiotomy wound are the main problems
of postnatal mothers in the puerperium. The present study was conducted in order to
find the effectiveness of sitz bath versus infrared therapy in reducing episiotomy pain
and wound healing. Administration of sitz bath and infrared therapy were found to
be effective in reducing episiotomy pain , and promoting wound healing, the result
showed significant difference between the mean scores of pain and wound healing in
both control and experimental group before and after administration of sitz bath &
infrared therapy and was demonstrated using ‘t’ test analysis. And student ‘t’ test
showed that there was significant difference between post-test scores of pain in both
control and experimental group. The computed chi- square test showed that there was
no significant association between pre test pain scores and selected baseline
characteristic in both control and experimental group with an exemption of religion
which has shown significant association with pre test pain score only in experimental
group.
Implications in Nursing
The findings of the study have several implications for nursing education,
administration, practice and research.
76
Nursing education
Nursing education prepares the nurses to function as a good educator. The
nurse educators have the responsibility to update the knowledge of the nursing
personnel in order to meet the needs of postnatal mothers and solve their difficulties
related with episiotomy wound. The use of non-pharmacological measures like
infrared therapy can be incorporated in nursing education along with other
contemporary therapies. To equip nurses to provide holistic care to their clients, the
nursing curriculum should be covered with several types of non – pharmacological
measures such as infrared therapy for episiotomy pain and wound healing. Thus the
student nurses can be guided in developing the right attitude and skills required for
caring the patients with episiotomy wound.
Continuing education is the key component to update and improve the
knowledge of the individual. It has a vital role in the field of the nursing profession.
Nursing administration
There is an increasing need for quality and holistic care in today’s health care
system. The findings of this study can be utilized by nursing personnel while providing
care for the postnatal mothers. Nursing administrator should organize periodic
educational programme for nursing staff to improve their knowledge and skill. In
collaboration with education department, nursing administrator can arrange the
periodic in service education programme for the staff nurses regarding uses of infrared
therapy. The knowledge about infrared lamp therapy will help the nurses to provide
beneficial care to the postnatal mothers during puerperium.

77
Nursing practice
Confronting with episiotomy pain and delayed wound healing are the common
problems that interfere in the care of the baby and also in the self care during the
puerperium. The appropriate measures and proper management of episiotomy pain and
wound healing will help in reducing the sufferings during postnatal period. in the area
of clinical practice, in service education programme regarding infrared therapy can be
conducted to know the various upcoming benefits of infrared therapy for providing
care for the episiotomy wound , as it was found to be one of the effective measures in
reducing pain and improves wound healing with no side effects. Since it is a new
method nurses as well as postnatal mothers need to be introduced to this method of
treatment. Each hospital can make their own practice models for this type of treatment.
Nursing research
Episiotomy pain and delayed wound healing will extent the number of days of
hospital stays among postnatal mothers with normal vaginal delivery. Therefore there
is great need for adopting more measures for the management of episiotomy during the
puerperial period. Several researches on non – pharmacological therapies like heat
therapy, cold therapy, lavender oil application and self care on episiotomy wound will
help the nurses attain more knowledge and it will initiate them to provide more quality
care for the patients. Such knowledge generated through research will help in more
popular implementation of different type of therapy in this area. For the generalization
of infrared light application, further studies could be conducted in the hospital with
increased frequency for larger samples.

78
Limitation
1. The study was confined to only 60 postnatal mothers and limited to one hospital
2. Infrared therapy was limited to three days therapy for each patient.
3. The time duration for therapy was limited to 15 minutes in morning and evening.
Recommendation
1. A similar study can be conducted with increased frequency of administration of
infrared lamp therapy which may yield more reliable result.
2. A similar study can be conducted by selecting a larger sample on a long-term basis
3. The study can be conducted in different settings with similar facilities
4. A comparative study can be conducted with hot and cold therapy
5. A comparative study can be conducted between infrared therapy and other non
pharmacological measures
6. A comparative study can be conducted between infrared therapy and pharmacological
measures.
7. A comparative study can be conducted on the effectiveness of infrared therapy
between urban and rural area
8. A comparative study can be conducted between primiparous women and multiparous
women to assess the effectiveness of infrared therapy
9. A descriptive study can be conducted on the awareness of postnatal mothers about non
pharmacological methods of care of episiotomy
79
SUMMARY
The present chapter dealt with the findings of the study related to demographic
characteristics, effectiveness of sitz bath & infrared lamp therapy and includes the
major implications of the nursing service related to nursing education, nursing
practice, nursing administration and nursing research areas.

80
8. SUMMARY
This chapter presents the summary of the study. With the increasing needs of
the postnatal mothers having episiotomy, meeting the needs of the patients becomes a
major challenge in the current nursing practice. The main aim of the study was to
assess the effectiveness of infrared therapy on episiotomy pain and wound healing.
The main objectives of the study were:-
I. To assess the level of pain and wound healing status among postnatal mothers with
episiotomy.
II. To assess the effectiveness of sitz bath and infrared lamp therapy on episiotomy pain
and wound healing among postnatal mothers.
III. To compare the effectiveness between sitz bath and infrared lamp therapy on
episiotomy pain and wound healing among postnatal mothers.
IV. To determine an association between pain level & wound healing status with selected
demographic variables.
The study attempted to examine the following research hypothesis:-
H1: There is a significant difference between the mean pre test and post test pain &
wound healing scores in sitz bath and infrared lamp therapy group.
H2: There is a significant difference in the mean post test scores between sitz bath and
infrared lamp therapy group.
H3: There is a significant association between pain &wound healing scores with
selected demographic variables in sitz bath and infrared lamp therapy group.

81
The conceptual frame work utilized in this study was based on Ernestine
Wiedenbach’s helping art of clinical nursing theory, consist of three steps that is
central purpose, prescription and realities.
In this study various literatures were reviewed which includes, literatures
related episiotomy, effectiveness of sitz bath and effectiveness of infrared lamp
therapy.
The research design selected for the study was quasi experimental, pre-test and
post-test design with comparison group. The independent variable was infrared
therapy and dependent variables were episiotomy pain level and wound healing status
in pre-test and post-tests.
The target population was postnatal mothers. 60 postnatal mothers were
selected by purposive sampling technique.
The tool developed and used for the data collection was Verbal descriptive pain
scale and REEDA Scale. 9 experts validated the content validity of the tools and tool
was found to be reliable and feasible. The reliability of the tools were established by
Spearman’s Brown Prophecy formula where r=0.89 for Verbal descriptive pain scale
and r=0.96 for REEDA Scale.
Pilot study was conducted on 3/10/12 to 12/10/12 as a part of the major study,
tool proved to be comprehensible, feasible and acceptable. The permission was
obtained from authorities of hospitals and consent taken from study subjects.
82
Data collection procedure for main study began from 01/11/2012 to
30/11/2012. The investigator personally explained the need and assured them of the
confidentiality of their responses.
The pre-test was administered followed by interventions (sitz bath to control
group & infrared therapy to experimental group for 3 days for twice daily); post-test
was taken after 3 days of administering the interventions by using the same Verbal
descriptive pain scale and REEDA scale used in the pre-test.
The Data gathered were analyzed and interpreted according to objectives.
Descriptive statistics like mean, median and standard deviation, and inferential
statistics like paired ‘t’ test was included to test the hypothesis and Chi-square test was
included to test the association of pain scores with demographic and clinical variables
and the data obtained are presented in the graphical form.
Major findings of the study
In control group
Majority (66.67%) of the subjects belong to the age group of 18-23 years.
Most of the subjects were Hindus (66.67%).
Majority (73.33%) were educated till secondary/diploma education .
Majority (63.33%) of subjects were housewives.
Half of the subjects (50%) were belonged to joint family and remaining to nuclear and
extended family.
All most all subjects (96.67%) were non vegetarians.
Majority of subjects (80%) resided in urban area.
Most of subjects (63.33%) were primiparas.
All subjects (100%) had right mediolateral episiotomy.

83
In experimental group
Half (50%) of the subjects belong to the age group of 24-29 years.
Majority of subjects (70%) were Hindus.
Most of the subjects (83.33%) were educated till secondary/diploma education.
Majority of the subjects (70%) were housewives.
Half of the subjects (50%) were belonged to nuclear family and 40% to joint family,
and reaming 10% were from extended family.
Majority of subjects (93.33%) were from mixed diet grop.
Majority of subjects (60%) resided in urban area.
Majority of subjects (60%) were multiparas.
Most of the subjects (80%) had right mediolateral episiotomy.
The mean percentage of pre-test and post-test in control group was 74.33 and 43.33
respectively, whereas in experimental group it was 80and 29 respectively which
shows that the pain score of experimental group during post-test was lower when
compared with other pain scores.
There was a significant difference between pre test and post test pain score and wound
healing score in both control and experimental group at 0.05 level. This implies that
sitz bath and infrared therapy was effective in reducing episiotomy pain and wound
healing.
The unpaired t test values 2.62 (pain) and 0.19 (wound healing) shows that there is
significant difference only between post test pain scores, not between post test wound
scores. It means that infrared therapy more effective than sitz bath in episiotomy pain
reduction where as with regard to wound healing, both sitz bath and infra red therapy
have same effect.

84
The association between pre test pain &wound healing scores and demographic
variables were computed by using Chi- square test. There were no significant
association between age, religion, education, occupation, family, diet, place of living,
parity and type of episiotomy with pre test pain & wound healing scores in both
control and experimental group. However, there was significant association only
between religion and the post-test pain scores in experimental group.
The investigator accepts the research hypotheses stated in the study at 0.05 level of
significance.
85
9. BIBLIOGRAPHY
1. Z Zainur. “Postpartum morbidity - What we can do” Med J Malaysia 2006 Dec 61(5)
2. Fraser D M, Cooper M.A. Myles text book for midwives. 14th
ed: Philadelphia;
Churchill Livingstone;2003.P .632
3. Noronha Judith. Effectiveness of self perineal care on Episiotomy wound healing. The
Indian Journal of Nursing and Midwifery 2003 Sep; 6(1): 25-39
4. Thacker SB, Banta HD Benefits and risks of episiotomy; an interpretive review of the
English language literature 1860 Obst Gynecol.Survey 1983: 38(6): 322-338.
5. Thorpe H, Bowes W, Brame R, et al :Selected use of : Effect on perineal trauma.
Obstet Gynecol 79: 945 –949,1992
6. Ana Carolina Sartorato Beleza,
Cristine Homsi Jorge, Ferreira,
Ligia de Sousa,
Ana
Márcia Spanó Nakano. Measurement and characteristics of pain after episiotomy and
its relationship with the activity limitations. Rev. bras. enferm. vol.65(2).
7. Robinson S, Thompson A. Midwives, research and childbirth. In: Sleep J. Perineal
care: a series of five randomised controlled trials. London: Champman & Hall; 2007.
p. 199-251.
8. Enkin M, Keirse MJNC, Neilson J, Crowther C, Duley L, Hodnett E, Hofmeyr J. A
Guide to Effective Care in Pregnancy and Childbirth, 3rd ed. Oxford: Oxford
University Press, 2000
9. Joyce Hasegwa, Lucila Coca Levenhal. Pharmacological and non pharmacological
treatment for relief of perineal pain after vaginal delivery. Einstein. 2009; 7(2):194-20
10. Therapy for management of childbirth perineal tears. Available from:
URL:http://www.practicalpainmanagement.com Januvary 1, 2011
86
11. John Martin Munro Kerr, Thomas F Baskett, Andrew A Calder, Sabaratnam Arul
kumaran. Munro. Kerr’s operative obstetrics, 11th
ed. London. Elsevier Sounders;
2009. P 253
12. Graham, I.D, G. Carroli, C. Davies, and J.M. Medves, 2005, Episiotomy rates around
the world: An update. Birth, 32: 219-22
13. Episiotomy rate in India: URL:http://jpubhealth.oxfordjournals.org/.Accessed2010
14. EpisiotomyrateinBangalore:URL:http://www.jabfmorg/cgi/content/full/18/1/18.2010
15. B.W.C. Sathiyasekaran, Gopal Palani, Ramesh Harihara Iyer, Shanthi Edward,
Chithraa Devi Dharmappal “et al”. Popualtion based study of episiotomy.
Sriramachandra journal of medicine. 2007 Nov
16. East CE, Sherburn M, Nagle C, Said J, Forster D. Perineal pain following childbirth:
Prevalence, effects on postnatal recovery and analgesia usage. Midwifery. 2011 Jan;
17. Annamma Jacob, Rekha R, Jadhav Sonali Tarachand. Clinical nursing procedures: The
arts of nursing practice. 1st ed: New delhi; Jaypee publications 2007.P.105-106.
18. Joyce Hasegawa, Lucila Coca Leventhal. Pharmacological and non pharmacological
treatment for relief of pain after vaginal delivery. Einstein, 2009; (7): 194 – 200.
19. Denise F Polit, Bernadette P. Hungler. Nursing research. 6th
ed. Philadelphia:
Lippincott company; 1999.P.155-159
20. George B Julia B. Nursing theroies. 4th
ed. Non walk: Appleton and Lange publishers;
1977.P. 179-191
21. HenriksenTB, BekKM, HedegaardM, SecherNJ.Episiotomy and perineal lesions in
spontaneous vaginal deliveries Br J Obstet Gynaecol. 1992 Dec; 99(12): 950-4
22. CarvalhoCC, SouzaAS, MoraesFilhoOB.Prevalence and factors associated with
practice of episiotomy at a maternity school in Recife, Pernambuco, Brazil. Rev Assoc
Med Bras. 2010 May-Jun;56(3):333-9

87
23. Revicky V, Nirmal D, Mukhopadhyay S, Morris EP, Nieto JJ. Could a
mediolateral episiotomy prevent obstetric anal sphincter injury? Eur J Obstet Gynecol
Reprod Biol. 2010 Jun;150(2):142-6.
24. De Leeuw JW, De Wit C, Kuijken JP, Bruinse HW. Mediolateral episiotomy reduces
the risk for anal sphincter injury during operative vaginal delivery. BJOG. 2008
Jan;115(1):104-8.
25. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009
Jan 21;(1).
26. Webb DA, Culhane J. Hospital variation in episiotomy use and the risk of perineal
trauma during childbirth. Birth. 2002 Jun;29(2):132-6
27. Poen AC, Felt-Bersma RJ, Dekker GA, Devillé W, Cuesta MA, Meuwissen SG. Third
degree obstetric perineal tears: risk factors and the preventive role of mediolateral
episiotomy. Br J Obstet Gynaecol. 1997 May;104(5):563-6
28. Ecker JL, Tan WM, Bansal RK, Bishop JT, Kilpatrick SJ. Is there a benefit
to episiotomy at operative vaginal delivery? Observations over ten years in a stable
population. Am J Obstet Gynecol. 1997 Feb;176(2):411-4
29. Cleary-Goldman J, Robinson JN. The role of episiotomy in current obstetric practice.
Semin Perinatol. 2003 Feb;27(1):3-12.
30. Katayon Vakilian, Mahtab Atarha , Reza Bekhradi, Reza Chaman. Healing advantages
of lavender essential oil during episiotomy recovery: A clinical trial. Complementary
Therapies in Clinical Practice 2011;(17): 50-52
31. Ramler D, Roberts J. A comparison of cold and warm sitz baths for relief of
postpartum perineal pain. .Journal of Obstetrics Gynecol ogy and Neonatal Nurse.
1986 November-December. 15(6):471-4.

88
32. Jo Lafoy, Elizabeth A. Geden.Post episiotomy pain: warm versus cold sitz bath. J of
obstet gynecol neonat nsg 2006 Jan – Feb: 19 (1): 13.
33. Hur MH, Han SH. Clinical trial of Aromotherapy on postpartum mothers perineal
healing, Taechan Kanho Hakhoe Chi 2004 Feb; 34(1): 53-62.
34. Rakel D. Episiotomy discomforts relief using infrared light therapy. Nightingale
Nursing Times 2010 Mar;9(6):14-5.
35. Hill PD. Effects of heat and cold perineum after episiotomy laceration. Journal of heat
and cold on the perineum after episiotomy. J Obstet Gynecol Neonatal Nurs. March –
April; 18(2) 124-9
36. Talar tejirian. An experimental study to assess the effectiveness of sitz bath department
of obg surgery California publication 2005 June.
37. Oan Lingen, Department of Obstetrics and Gynecology, Onley Community Health
Center, Onancock, VA., Health line Pregnancy Guide, 2006 Feb.
38. Anita Sali. Effect of sitz bath versus guggul dhupan on pain related to episiotomy in
postnatal mothers. Journal of Nursing research Society of India 2007 Oct-Nov; No-2,
Vol-1, 19-21.
39. Henton J, Jain A. Cochrane corner: water for wound cleansing. J Hand Surg Eur
Vol. 2012 May;37(4):375-6.
40. Venkadalakshmi.V, Venkatesan Latha, Perdita M.Helen. Effectiveness of infrared
therapy upon Episiotomy pain and Wound healing in postnatal mothers. The Official
Journal of Trained Nurses’ Association of India 2009Jul-Sep;4(3):19
41. John Esther, R Sheeba, M. Vimiji, S. Seena. Effectiveness of infrared radiations in
healing of episiotomy wound in postnatal mothers. Nightingale Nursing Times 2009;
Feb; 4(11): 60-1,67.

89
42. Jaroslava Kymplova, Leos Navratil, and Jirl Knizek. Contribution of phototherapy to
the treatment of episiotomy. Journal of Clinical Laser Medicine & Surgery. February
2003, 21(1): 35-39.
43. V. Dhanalakshmi. Best remedial measure after Episiotomy? Sitz bath? Or Infrared
Light Therapy?. Nightingale Nursing Times 2010 Mar;5(12):12-6.
44. Rzakulieva LM, Israfilbeili SG, Gasymova G. Application of magnet laser radiation to
stimulate healing of perineum injuries in the maternity patients.
GeorgiaMedNews. 2006Sep;(138):71-3.
45. Nam HK, Park YS. A study on comparison of ice bag and heat lamp for the relief of
perineal discomfort Kanho Kakhoe Chi, 1991, Apr;21(1):27-40.
46. Bowel Rina. A study to compare the effect of cold pack versus infrared radiation on
episiotomy wounds in postnatal mothers in a selected hospital, Vellore. Unpublished
thesis, the tamil nadu Dr. MGR Medial university Chennai.
47. Varalakshmi K Y. A study to compare the effect of cold pack versus infrared radiation
on episiotomy wounds in postnatal mothers in a selected hospital, Hyderabad.
Unpublished thesis. The University of Andra Pradesh.
48. K Danno, N Mori, K Toda, T Kobayashi, A Utani. Near-infrared irradiation stimulates
cutaneous wound repair: laboratory experiments on possible
mechanisms.Photodermatol PhotoimmunolPhotomed. 2001 Dec;17(6)
49. Bogacheva ON, Samoĭlova KA, Zhevago NA, et al. Enhancement of fibroblast growth
promoting activity of human blood after its irradiation in vivo (transcutaneously) and
in vitro with visible and infrared polarized light. Tsitologiia 2004; 46(2):159-71.
50. De olivera SM, Miquilini EC. Frequency and criteria for the indication of episiotomy.
Rev Esc Enferm USP 2005 Sep; 39(3): 288-95

90
51. Imarengiaye CO, Andet AB. Postpartum perineal pain among Nigerian women. West
Afr J Med. 2008 Jul;27(3):148
52. UygurD, YesildaglarN, KisS, SipahiT.Earlyrepairof episiotomy dehiscence. AustN Z J
Obstet Gynaecol. 2004 Jun;44(3):24
91
ANNEXURE A
COPY OF LETTER SEEKING PERMISSION TO CONDUCT THE STUDY

92
ANNEXURE B
COPY OF THE LETTER SEEKING EXPERT’S OPINION FOR THE
CONTENT VALIDITY OF THE TOOL
From,
Mr. Susen George
II Year M.Sc Nursing
Kempegowda College of Nursing
Bangalore-560004.
To,
Forwarded through,
The Principal,
Kempegowda College of Nursing
Bangalore-560004.
Respected Sir/Madam,
Sub: Requisition for expert opinion on content validity of the research tool.
I, Susen George, a post graduate student of Kempegowda College of Nursing,
Bangalore, as a partial fulfillment of the master degree in Medical-Surgical Nursing of
Rajiv Gandhi University of Medical science, Bangalore, have selected the below
mentioned topic for the dissertation.
Title of the project: “A comparative study to assess the effectiveness of sitz bath
versus infrared lamp therapy on episiotomy pain and wound healing among post natal
mothers at selected hospitals, Bangalore”.

93
Objectives:
v. To assess the level of pain and wound healing status among postnatal mothers with
episiotomy.
vi. To assess the effectiveness of sitz bath and infrared lamp therapy on episiotomy pain
and wound healing among postnatal mothers.
vii. To compare the effectiveness between sitz bath and infrared lamp therapy on
episiotomy pain and wound healing among postnatal mothers.
viii. To determine an association between pain level & wound healing status with selected
demographic variable
With regard to this I kindly request you to validate my tool for its appropriateness and
relevancy.
Here with I am enclosing a copy of
a) Numerical intensity pain scale for diabetic foot pain
b) Criteria rating scale/ check list
c) Content validity certificate.
I request you to kindly go through the content and give your expert and valuable
suggestion in the columns given and mark ( ) if you agree.
Your expert opinion and kind cooperation will be highly appreciated and
gratefully acknowledge.
Thanking you in anticipation,
Yours faithfully
(Ms. Susen George)
Place: Bangalore
Date: Signature of Principal
94
ANNEXURE C
CONTENT VALIDITY CERTIFICATE
This is to certify that the tool developed by Ms. Susen George, II Year M.Sc Nursing
student of Kempegowda College of Nursing, Bangalore (Affiliated to Rajiv Gandhi
University of health Science) is validated by the undersigned and can proceed to
conduct the main study for dissertation entitled as “A comparative study to assess the
effectiveness sitz bath versus infra red lamp therapy on episiotomy pain and
wound healing among postnatal mothers at selected hospital, Bangalore”.
Place:
Date: (Name and signature of the expert)
95
ANNEXURE D
CRITERIA RATING SCALE FOR EVALUATION
Respected Madam/Sir,
Kindly go through the content and place the tick mark ( ) against the
questionnaire in the following columns ranging from very relevant to not relevant.
When the question is found not relevant and need modification kindly give your
opinion in the remarks column. The tool is present in two parts.
Part I: Consists of 10 items related to demographic variable under the study.
Part II: a) Verbal descriptive pain scale
b) REEDA Scale.
Part I
Demographic data
Item Very
Relevant
Relevant
Need
modification
Not
Relevant Remarks
1
2
3
4
5
6
7
8
9
10
96
Part II
a) Verbal descriptive pain scale to assess episiotomy pain.
Item Very
Relevant
Relevant
Need
modification
Not
Relevant
Remarks
1
2
3
4
b ) REEDA Scale to assess episiotomy wound healing.
Item Very
Relevant
Relevant
Need
modification
Not
Relevant
Remarks
1
2
3
4
Suggestions if any:
Over all opinion of the validator:
Signature of the validator
Name and address of the validator

97
ANNEXURE E
LIST OF EXPERTS CONSULTED FOR CONTENT VALIDITY OF THE
TOOL
1. Mrs. Lalitha Haemorrhage
Professor, Dept. of OBG
Government college of nursing
Bangalore.
7. Mrs. Sabina Monica
Associate Professor, Dept. of OBG
HMH College of nusing,
Mysore
2. Mrs. Maria Preethi Miranda
HOD of OBG dept.
Krupanidhi college of nursing
Bangalore
8. Mrs. Shenbagalakshmi
Principal, HOD of OBG dept.
Kauvery College of Nurisng
Mysore
3. Mrs. Gouri Sai
Associate Professor, Dept. of OBG
Fortis College of Nursing
Bangalore.
9. Mrs. Bhavya
Associate professor, HOD of OBG
JSS College of nursing
Mysore.
4. Mrs. Sabitha Sibbla
Assistant Professor, Dept. of OBG
Fortis college of nursing
Bangalore
10. Mr. Gangaboraiah
Professor of Statistics
KIMS,
Bangalore.
5. Mrs. Swarna Latha Puerperium
Principal, HOD of OBG dept.
BMS hospital nursing college
Banglore
11. Mrs. Rajeshwari
Associate professor
Dept. of English, V.V. Puram College
of Arts and commerce,
Bangalore
6. Mrs. Tajnisha Bhanu
Professor, HOD of OBG dept
HMH college of nursing
Mysore.

98
ANNEXURE F
COPY OF CONSENT FORM
I am voluntarily willing to participate in the study conducted by Ms. Susen
George, II year M.Sc. Nursing (OBG) student of Kempegowda College of nursing
on “A comparative study to assess the effectiveness of sitz bath versus infrared
lamp therapy on episiotomy pain and wound healing among postnatal mothers at
selected hospital, Bangalore”. I will also co-operate with the researcher in providing
necessary information. I was explained that the information provided would be kept
confidential and used only for above mentioned study purpose.
Signature of the Investigator Signature of the participant
Date:
Place: Bangalore
99
ANNEXURE - G
TOOL USED FOR THE STUDY
The data collection tool has two parts
Part- I: Questionnaire consists of 10 items related to demographic variables under
study.
Part- II:
a) Verbal descriptive pain scale to assess the episiotomy pain level
b) REEDA Scale to assess the episiotomy wound healing.
PART – I
Demographic data
Instructions to the respondent:
Dear participant,
I Susen George, II year M. Sc Nursing student would request you to answer some
questions related to your background. So listen carefully to the questions and respond
as accurately as possible. I assure you that the provided information will be exclusively
utilized for the partial fulfillment of P.G. programme and the information will be kept
confidential.
Sample code
1. Age ( in years)……………………………………………………
2. Religion
a. Hindu ( )
b. Christian ( )
c. Muslim ( )
d. Any others specify..........................................................................
3. Educational status of parents………………………………………..
4. Occupational status………………………………………………….
100
5. Type of the family
a. Nuclear ( )
b. Joint ( )
c. Extended ( )
6. Dietary pattern
a. Vegetarian ( )
b. Mixed ( )
7. Place of living
a. Rural ( )
b. Urban ( )
8. Parity
a. Primi ( )
b. Multi ( )
c. Grand multi ( )
9. Type of episiotomy
a. Median ( )
b. Lateral ( )
c. Right mediao lateral ( )
d. Left medio lateral ( )

101
PART - II
a) Verbal descriptive pain scale (Jack Harich, 2002)
POINTS LEVEL OF PAIN DESCRIPTION
0
No pain
No pain. Feeling perfectly normal.
1 Mild pain
Does not interfere with most of the activities. Able
to adapt to pain psychologically and with
medication or comfort devices.
2 Moderate pain
Interferes with many activities. Requires lifestyle
changes but patient remains independent. Unable to
adapt pain.
3 Severe pain Unable to engage in normal activities. Patient is
disable and unable to function independently.
Verbal pain scales, as the name suggests, use words to describe pain. Words
such as no pain, mild pain, moderate pain, and severe pain are used to describe pain
levels. A score from 0 to 3 is assigned to each of those word pairs and is used to
measure the pain level.
No pain - 0
Mild pain -1
Moderate pain -2
Severe Pain -3
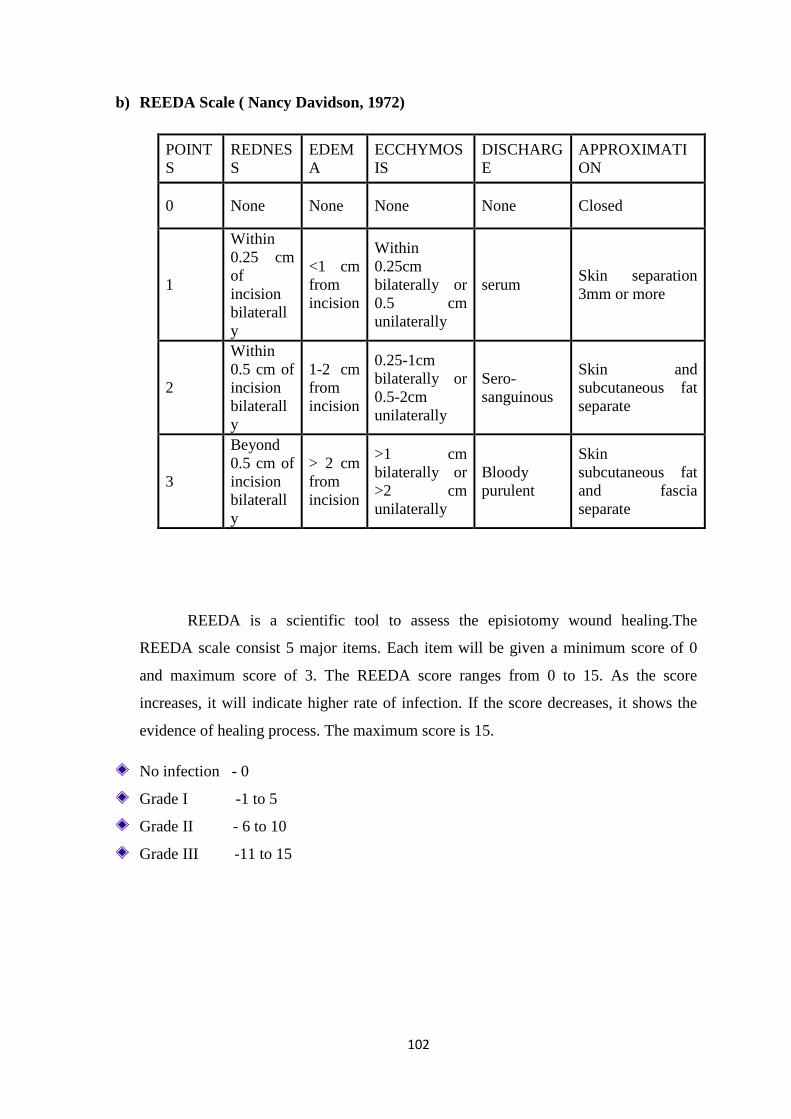
102
b) REEDA Scale ( Nancy Davidson, 1972)
POINT
S
REDNES
S
EDEM
A
ECCHYMOS
IS
DISCHARG
E
APPROXIMATI
ON
0 None None None None Closed
1
Within
0.25 cm
of
incision
bilaterall
y
<1 cm
from
incision
Within
0.25cm
bilaterally or
0.5 cm
unilaterally
serum Skin separation
3mm or more
2
Within
0.5 cm of
incision
bilaterall
y
1-2 cm
from
incision
0.25-1cm
bilaterally or
0.5-2cm
unilaterally
Sero-
sanguinous
Skin and
subcutaneous fat
separate
3
Beyond
0.5 cm of
incision
bilaterall
y
> 2 cm
from
incision
>1 cm
bilaterally or
>2 cm
unilaterally
Bloody
purulent
Skin
subcutaneous fat
and fascia
separate
REEDA is a scientific tool to assess the episiotomy wound healing.The
REEDA scale consist 5 major items. Each item will be given a minimum score of 0
and maximum score of 3. The REEDA score ranges from 0 to 15. As the score
increases, it will indicate higher rate of infection. If the score decreases, it shows the
evidence of healing process. The maximum score is 15.
No infection - 0
Grade I -1 to 5
Grade II - 6 to 10
Grade III -11 to 15