synthesizing evidence on the front line – can it work?€¦ · the culture values and supports...
TRANSCRIPT

© SEARCH Canada
Synthesizing Evidence on the Front Line – Can it Work?
Experiences from SEARCH.
Sarah Hayward, Jeanne Annette, Mark Watt, Mary Nugent, Sharon Matthias
A health system where..
Health professionals in the RHAs use current, relevant and appropriate information to assist in identifying priority health issues and making decisions on these issues based on research results.
There is a collaborative network of expertiseacross Alberta to initiate and carry out health research on a local, regional or provincial basis.
The culture values and supports policy-responsive research.

Evolution
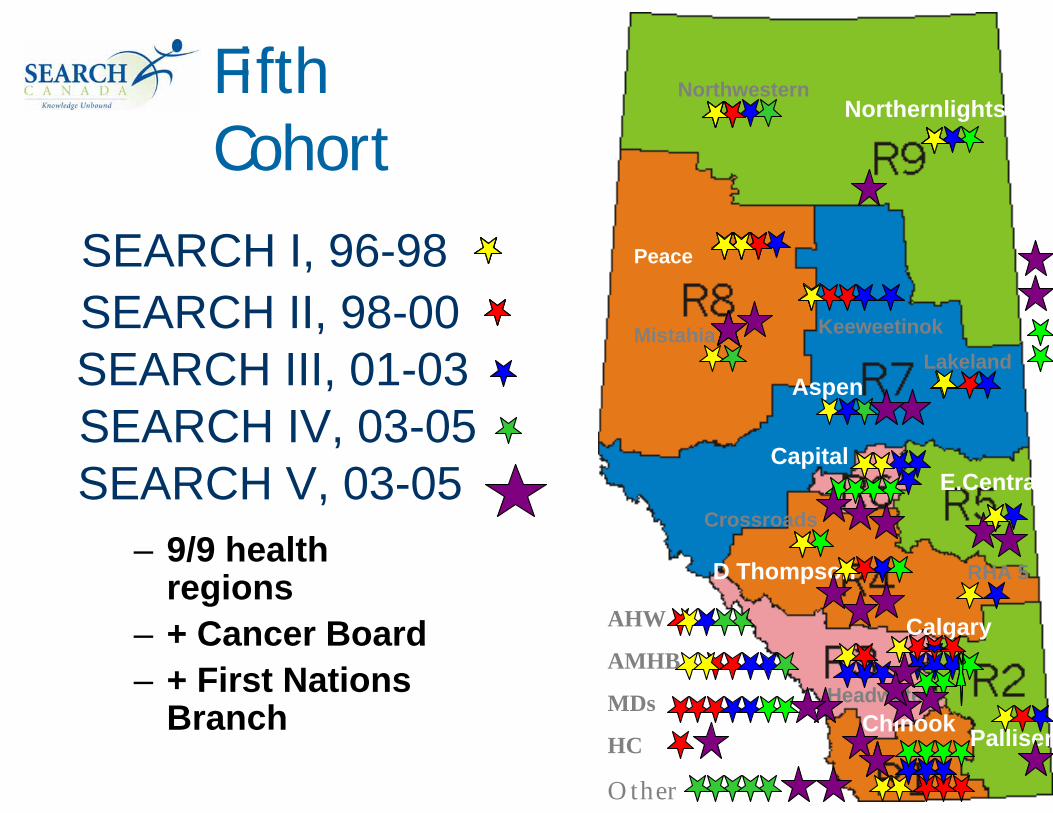
SEARCH I, 96-98
SEARCH II, 98-00
SEARCH III, 01-03
SEARCH IV, 03-05AHW
AMHB
MDs
HC
Other
NorthwesternNorthernlights
LakelandMistahia Keeweetinok
Peace
Aspen
Capital
Crossroads
E.Central
D Thompson RHA 5
Palliser
Calgary
Headwaters
Chinook
SEARCH I, 96-98
– 9/9 health regions
– + Cancer Board– + First Nations
Branch
NorthwesternNorthernlights
LakelandMistahia Keeweetinok
Peace
Aspen
Capital
Crossroads
E.Central
D Thompson RHA 5
Palliser
HeadwatersChinook
Calgary
Fifth Cohort
AHW
AMHB
MDs
HC
Other
SEARCH II, 98-00SEARCH III, 01-03SEARCH IV, 03-05SEARCH V, 03-05

ORGANIZATIONS
System Engagement
PEOPLE
PROJECTS

Using Evidence
Creating Evidence
Choosing Evidence
CONTEXT
Competency Framework

ProjectsAn Investigation
– Disciplined enquiry– Using an established method– Systematic data use
Embedded– Relevant to Organization / Practice– Involves collaboration– Includes dissemination and debrief
Focussed– On any topic– Within any of three curriculum themes

Projects
Local Projects : Choosing and Using– identification, selection, interpretation and
application of existing research knowledge– work with organization to identify question,
communicate results and facilitate application.
Provincial Projects : Creating and Using– one of five pre-identified topics, a literature
review, research question, project design.– collection and analysis of primary data,
preliminary results

Projects - supportsInformation resources
– SEARCH Desktop: knowledge access and tools– Document retrieval
Faculty team– initial ‘faculty contact’– faculty mentors: content, method and other needs– additional linkages
Organizational mentor/champion– mentor : support and advice– champion : communications, guidance in
negotiating topics and organizational support. Seed Funding
– $5000 for provincial, $1000 for local– ethics approval

© SEARCH Canada
Knowledge Transfer on the Front Lines
Beyond Peer Education for Health Promotion
Jeanne AnnettSEARCH IV
Aspen Regional Health
SEARCH Local ProjectSystematic Review of Literature
Understanding the Key Aspects of Peer Education as an Intervention in Health Promotion (Annett, J. 2005)
PurposeBuild on lessons learnedHelp inform future practice
OutcomeReady resourceEnhancement of skills and resources

Applying the Process
Impact of the SEARCH training
Streamlining the process
Building capacity
Having impact in the Health Region

Informing nursing policy
Regional screening
program for developmental delays in young
children
Becoming more Research-Friendlyin a Rural Health Region
Building the Capacity to Select and UseInformation
Supportingthe process
Increasing Access to Information

Aspen Learning Centre

© SEARCH Canada
The Path of Least Resistance Managing Community Acquired Pneumonia
Mark WattSEARCH IV
Chinook Health Region

The Team Back Home
Dr. Duncan Mackey
Marlene Myles (missing)
Diane Carter
Susan Wojtowicz
Annella Wehlage
Becky Marshall
Sarah Baker
Kevin Reedyk

My Journey
• An experiment of building research capacity at the front-line
• The ‘problem’ as seen by the Region– Admission rates of pneumonia 50%
higher and LOS 25% longer than the Capital Health Region

Setting the Stage
• How do you facilitate an organizational change towards evidence based practice?– Demonstrate a need– “We’re different” attitude– Identify barriers to using evidence based
decision making– Reconstruct the system aligning supports
towards the change in practice

Obtaining Evidence
• Plethora of evidence on best practice for management of CAP– Typically conducted at Teaching
Institutions (Different patients)– Focused on medical management of
pneumonia (not a group responsive to outside change)

Using a New Lens
• Intentional Blindness of Medical Literature
• Reviewed the Medical Literature from the lens of Registered Nurse scope of practice
• Identified System Processes directly affected by nursing intervention

Take Away Thoughts
•Team•Avoid Intentional Blindness•Context of Medical Literature•Path of least resistance

© SEARCH Canada
Key Learnings in Integrating Evidence Into Practice
Hypertension Management in a Primary Care Setting
Mary Nugent, SEARCH IVTaber Associate Medical Centre

Learning from Past SuccessTaber Asthma Program (TAP)
– Interdisciplinary (NP, GP, RRT, support staff, specialist prn)
– Structured practitioner communication and education strategy
– Evidence based management– Self-care model / Coaching model
Outcomes:– 61% decrease in ER-related asthma visits;– 41% decrease in asthma related hospital
admissions.– High practitioner and patient satisfaction– Shifted burden of care

SEARCHing for the Evidence
Research Questions:1. What are the existing delivery models used
in a multidisciplinary, evidence-based, nurse-coordinated**, hypertension program?
2. What are the key understandings from these models that can be used to inform the development of a multidisciplinary, evidence-based, nurse-coordinated**, hypertension program?
**Nurse-coordinated is defined as one portion of the nursing role – the responsibility to ensure seamless patient navigation through theprogram.

What did the evidence say?Global strategy of cardiovascular protection.Most successful programs combine
pharmacological and non-pharmacological interventions.
Canadian Consensus Guidelines help support evidence based decision-making.
Patient centred care is critical.Currently recognized there is no available
published literature regarding practical ‘how-to’ set up a hypertension program (grey literature).
Information technology could facilitate efficient and effective care (grey literature).

Challenges Of The ‘Scholar-Practitioner’
Finding ‘perfect’ literatureIntegrating systematic synthesis in
the real world:– Time – competing demands– Space – a place to work ; a place to
reflect– People – skeptics and critics
• Expertise in change management
Challenges of Integrating Something New Into Local Practice
After the literature search…Easy:
– Deciding on high leverage interventions; setting achievable outcomes
Moderately difficult:– Measuring outcomes using technology
Very difficult:– Changing embedded practitioner and patient flow
regarding CVD and HTN; – Changing practitioner view of ‘target’ BPs and
CVD reduction; – increasing use of non-pharmacological
interventions

Diagnosing the ‘Problem’
Framework (Dr. Gill Chard*, U of A)– Barriers:
• Organizational (workplace barriers)• Professional (individual barriers)• Social (barriers toward innovation) – new
knowledge or research may be used but not sustained.
– Facilitators*Chard G (2006) Adopting the Assessment of Motor and Process skills into practice: Therapists’ voices, British J. Occupational Therapy, 69(2) 50-57.

Facilitating ChangeTeam approachEducational strategy
– Making evidence easy to use– Using stepped approach
Outcome data collection– Setting achievable, measurable goals
Flow mapping – Simplifies processes– Allows identification of potential problems– Illuminates documented evidence or
recommendations

Key LearningsTeam approach.
– Keeping the right people involved
– Getting buy-in from all the team
Identify a starting point.– Logic model– Having a communication
and education strategy; Make the evidence simple to use.Know setbacks are inevitable.
– anticipate them, find a way around them if possible, and being kind to yourself when things don’t go according to plan or timing (diagnose the problem)
– Time, space and people will be areas to anticipate barriers.
PDSA or Action Learning cycle
http://hixie/w3c-snakes-and-ladders.png

© SEARCH Canada
Research, Decision Making and the Scholar Practitioner
Sharon MatthiasLead Faculty Team and Director of Programs
SEARCH Canada

Scholar Practitioner
• a person who, through their training and experience, combines two realms traditionally separated and often seen as opposites: scholar and practitioner. These individuals incorporate scientific approaches of knowledge making and knowledge use, while being grounded in the everyday endeavor of service delivery or product manufacture.
Scholar Practitioner• combines personal and professional
practical knowledge with conceptual, theoretical and empirical research knowledge to address health service problems.
• conscious of the quality of evidence and other parameters in a decision, and the decision process.
• not an independent researcher, but uses / recognizes quality research methods in evaluations, needs assessments,

Scholar Practitioner
• front line clinical, population health professional
• manager• policy decision support / policy analyst• specialists and managers in HR,
finance, IT/IM, physical plant• executive• governance

Scholar Practitioner
Practice Academic
Practice Academic

Scholar PractitionerDevelopment
Individual: Foundation of practice competence; Personal Practical Knowledge
Develop key competencies in:• Creating, Choosing and Using Evidence• Recognizing, Assessing and Navigating Context• Health Information Mgt / Computer Skills • Working in Interprofessional teams / learning
community • Policy / Organization• Impact on population (acute care, public health or
continuing care)• Change Management• Personal and Professional Development

Individual –> Network / Organization
Ongoing • Stimulating and Sustaining
Scholar-Practitioner / Academic networks
• Supporting Organizations to develop systems and procedures, culture that supports policy-relevant research

Evidence Blind
Evidence Tolerant
Evidence Friendly
EvidenceBased
?
Individual Learning Organizational Development
A Journey to (and beyond) Evidence Based Organization
Evidence Committed
Using Evidence
Unit Department Multi-units Institution Region System

To be crocus-minded


Acknowledgements

© SEARCH Canada
Creating Knowledge CulturesOur mission is to help health organizations make the best decisions through development of people, relationships and information.