systemic disease straight up with a twist of neuro-2 hours
TRANSCRIPT

8/15/2019
1
Beth A. Steele, OD, [email protected]
Systemic Disease Straight Up….with a Twist of Neuro!
AOA’s definition of Optometryapproved Sept 2012
Doctors of optometry (ODs) are the independent primary health care professionals for the eye. Optometrists examine, diagnose, treat, and manage diseases, injuries, and disorders of the visual system, the eye, and associated structures as well as identify related systemic conditions affecting the eye.
PREVENTION
…..where do we fit in?
WELLNESS
TREATING THE WHOLE PATIENT
MEDICAL OPTOMETRY
Not just this…
But also this…

8/15/2019
2
• 52 Caucasian male• Never had an eye exam• No regular health care• Vision goes “out” when he turns his head
•≥70% blockage before ocular manifestations
•5 year mortality rate – 40% • MI is mc• 4/5 strokes are causes
by atherosclerosis atcarotid bifurcation
“Vision went out, but now it’s back”
Only 10% of emboli from ICA end up in OA .. ! (Kaufmann 2012)
• X 2 hours ago• 62 year old white male• Heavy smoker, hxhypercholesterolemia, +HTN
1. Amaurosis Fugax – TMVL2. RAO3. Hollenhorst Plaque4. Ocular Hypoperfusion
Ocular signs of carotid artery disease
Intra‐arteriolar emboli • Increased risk of stroke, mortality, co‐morbidity
• 25% have carotid stenosis >40% (Bakri 2013)
• Symptoms?• Often transient – plaques are pliable• Correlated with degree of occlusion?• Predictive of future events?
• Doppler• EKG/Angiography
11% with symptoms had significant occlusion Wakefield, et al
22% w/o symptoms had 30-60% occlusion Dunlap, et al

8/15/2019
3
81 Caucasian female
• Wants new glasses before a trip to Paris
• PMHx: • Atrial fibrillation• Recent falls – due to TIA
• VA 20/30 due to cataracts• DFE – retinal heme and intra‐arteriolar plaque
Atrial Fibrillation
Most common cardiac arrhythmia Increased risk of mortality by 40‐90%
TIA, stroke (x5) and MI
Screen for with RAO patients risk of stroke need for anticoagulant
http://afib.utorontoeit.com/images/afibmain.pngPlunkett O, et al. BMJ Sept 2014
3 categories of stroke
1. Ischemic (85%)2. Hemorrhagic3. Transient Ischemic Attack
• Temporary disruptions in blood flow ‐‐ no permanent damage
• Symptoms last 30 min to 2 hrs ‐‐ often same symptoms as stroke
• Risk of stroke if untreated • 10‐15% in 3 months – 50% of these within next 48 hours
• 33% in the next year CDC 2015AHA 2015Johnston WC, et al. Lancet. 2007; 369: 283‐292.
All are medical emergencies!
“Blood work‐up”….tests driven by differentials
CBC with differential Chem 7 Lipid Profile ESR C‐Reactive Protein
Unexplained vascular changes.. ?
8/15/2019
4
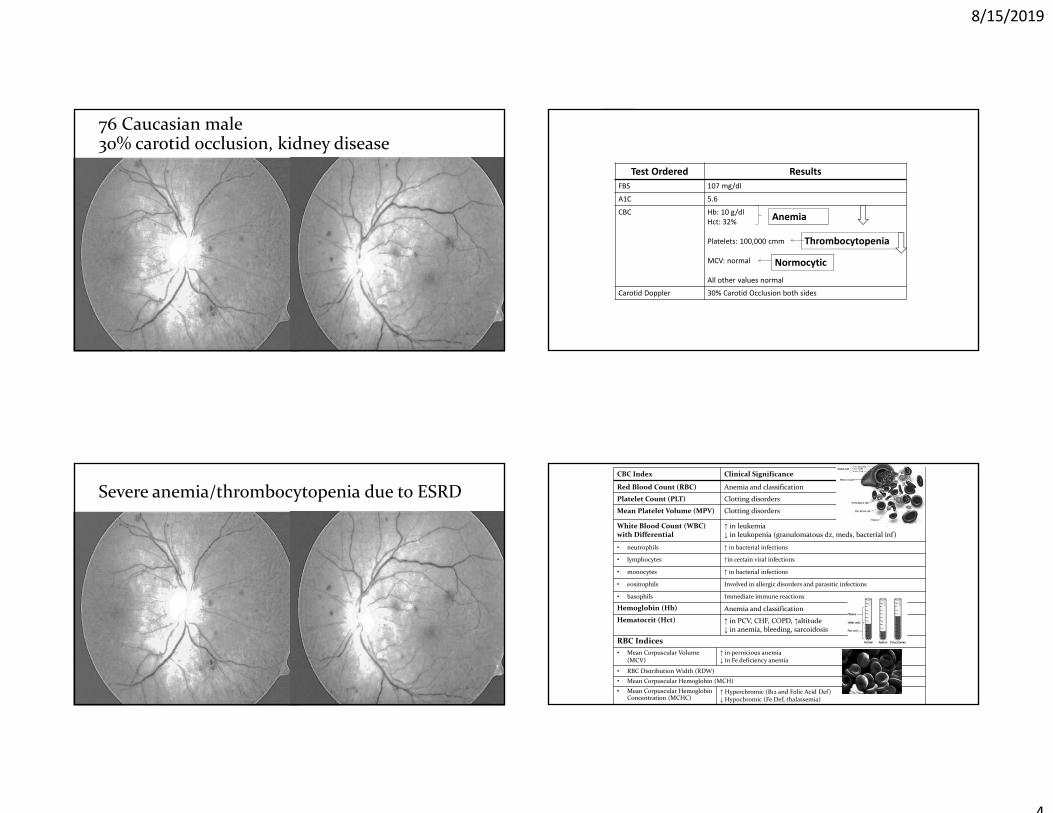
76 Caucasian male30% carotid occlusion, kidney disease
Test Ordered Results FBS 107 mg/dl
A1C 5.6
CBC Hb: 10 g/dlHct: 32%
Platelets: 100,000 cmm
MCV: normal
All other values normal
Carotid Doppler 30% Carotid Occlusion both sides
Anemia
Thrombocytopenia
Normocytic
Severe anemia/thrombocytopenia due to ESRDCBC Index Clinical Significance
Red Blood Count (RBC) Anemia and classification
Platelet Count (PLT) Clotting disorders
Mean Platelet Volume (MPV) Clotting disorders
White Blood Count (WBC) with Differential
↑ in leukemia ↓ in leukopenia (granulomatous dz, meds, bacterial inf)
• neutrophils ↑ in bacterial infections
• lymphocytes ↑in certain viral infections
• monocytes ↑ in bacterial infections
• eosinophils Involved in allergic disorders and parasitic infections
• basophils Immediate immune reactions
Hemoglobin (Hb) Anemia and classification Hematocrit (Hct) ↑ in PCV, CHF, COPD, ↑altitude
↓ in anemia, bleeding, sarcoidosis
RBC Indices• Mean Corpuscular Volume
(MCV)↑ in pernicious anemia ↓ in Fe deficiency anemia
• RBC Distribution Width (RDW)• Mean Corpuscular Hemoglobin (MCH)• Mean Corpuscular Hemoglobin
Concentration (MCHC)↑ Hyperchromic (B12 and Folic Acid Def)↓ Hypochromic (Fe Def, thalassemia)

8/15/2019
5
Chem 7 / Basic Metabolic Panel
1. Creatinine2. Blood urea nitrogen
(BUN)3. Glucose
4. Carbon dioxide5. Chloride6. Sodium7. Potassium 8. (Sometimes Calcium)
• Screens for• Kidney disease • Liver Disease • Diabetes and other blood sugar disorders
electrolytes
Also Consider: Common Coagulopathies
Condition Name of Lab Test
Antiphospholipid Antibody / Antiphospholipid Syndrome
Antiphospholipid Antibody Panel
Protein C and/or S deficiency Protein C and S Activity with Reflex to Protein C and/or S Antigen
Antithrombin III deficiency Antithrombin III Panel
Elevation of platelet factor 4 Platelet Factor 4
Factor V Leiden Factor (V) Leiden Mutation Analysis
Factor V Leiden??? What’s that?!!
• Factor V – clotting protein• gene c muta on: ↑clo ng in veins • Mc prothromobotic gene mutation in Caucasians – 5% population
• Caucasians of European descent
• Often undiagnosed, however….• deep vein thrombosis• pulmonary embolisms • CRVO• 11% of ocular vasc occlusions assoc with FVL (Schockman 2015; Fegan 2002)
57 Caucasian female with borderline HTN and Factor V
LeidenManucci P, et al. Thrombosis and Haemostasis 2015
• 43 AA FM• History of recur ring eye pain
• Joint pain • …lots of issues

8/15/2019
6
Laboratory Testing for Differentials –Inflammatory Conditions
• Approach ? • ESR• C‐reactive protein• Rh‐Factor• ANA• ACE• Lysozyme• PPD• Lyme titer• VDRL, FT‐ABS• ……
• OD: NLP• OS: 20/80 with dense inferior loss
Sarcoidosis
• Multisystem granulomatous disease• Subacute/acute or chronic
• Unknown etiology• Environmental, possibly infectious, and/or genetic predisposition
• Up to 40 per 100,000 in US• 8:1 African Americans, and more virulent in AA’s• 2:1 females• Generally presenting 20‐30’s (40‐60’s)

8/15/2019
7
Sarcoidosis: Diagnosis
• Lab testing• Serum ACE—90% with active disease (+)• Serum Lysozyme• ESR• Calcium and liver function tests
• Tissue biopsy, brush smear
• Other lab/radiographic test to rule out other diseases• PPD• Chest x‐ray, CT, MRI
Sarcoid: Ocular Manifestations in up to 50%
• Most common—granulomatous uveitis• secondary glaucoma• Posterior uveitis/vitritis/chorioretinitis
• Eyelid—up to 27%• Granulomatous lid lesion• Lacrimal gland enlargement • Lid retraction
• Conjunctival granuloma—up to 56%• DES from lacrimal gland involvement—up to 66%
Posterior Segment— up to 25%Inflammatory conditionsChoroidal granulomasRetinal and ONH NVCRVO‐rare
Neuro‐ophthalmic – 5‐10%CN palsiesPapilledema from intracranial lesions Direct ON infiltration –5%
• Disc edema, VA and VF loss, color vision defectOptic Neuropthy / Neuritis
Optic Neuropathy• Women • AA• 2 subtypes
• Sub‐acute, neuritis• Progressive neuropathy
• 2/3 are unilateral• 1/3 later involving other eye
• 1/3 with intraocular inflammation• 1/3 with pain • Treatment: steroids, immunosuppressants
• Function varies • Early treatment – better outcome
Kidd DP, et al. Am Academy Neurology 2016

8/15/2019
8
Nejm.org
Rheumatolgist.com
Plaquenil Toxity 2016 ‐ Revised Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy Marmor MF, et al. Ophth Feb 2011. Melles RB, Marmor MF. JAMA Ophthalmol 2014. Melles RB, Marmor MF. Ophthalmology 2015.
Risk of toxicity increases sharply towards 1% after 5‐7 yrs of use, or cumulative dose of 1000 g HCQ
Initial baseline exam, then annual screenings after 5 years
Screening: Regular exams with DFE 10‐2 24‐2 or 30‐2 for Asian patients
SD OCT*, FAF or mfERG*most objective, lowest variability Melles RB, Marmor MF. Ophthalmology 2015.
Damage is not always parafoveal!!
• Subtypes: 1. Parafoveal2. Pericentral3. Mixed
Melles, Marmor, Ophthal Aug 2014
• 10% of patients with a ring scotoma did NOT show damage with SD‐OCT!
Marmor MF, Melles RB. Ophthalmology. Jan 2014.

8/15/2019
9
OCT – what to look for early
• Scans• High resolution• Raster or radial• Enhanced depth imaging (EDI)• Macular cube – quantifiable
• Outer retinal thinning • Disruption to PIL
• Damage can progress up to 3 years after discontinuation….
Plaquenil Toxicity – Optical Coherence Tomography (OCT)
• Defects:• Are located 1.0mm (2‐8 degrees) from foveala
• Tend to deepen…not expand• Are eventually shaped like a “flying saucer” [sign]
• Inner retina: • Parafoveal thinning of GCL, IPL
• Outer retina: • Loss of IS/OS line
• “photoreceptor integrity line” (PIL)
• Thinning of PR layer • Thickening of outer band of RPE
Marmor MF, et al. Ophthalmology. AAO Revised Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy. Feb 2011.
FAF: Plaquenil Toxicity
Normal
mixed
• May contribute to earlier detection
• Before RPE degeneration develops
• Early change: • hyper AF • 2‐6 degree ring around fovea• Early photoreceptor damage –subtle
• Later change:• hypo AF• Coalesces into dark absence of FAF‐cells are dead
parafoveal
pericentral
Toxicity is Dose‐Dependent• Typical dose
• 300‐400mg daily for hydroxychloroquine• 250mg daily for chloroquine
• Mostly clinically significant cases of toxicity are iatrogenic
• Overdosing (>10%)• Lack of or inadequate screening/missed findings
• These recommendations are ok for most patients….NOT for:
• short/small• obese• liver/kidney disease
Browning DJ Hydroychloroquine and Chloroquine Retinopathy 2015American Journal of Ophthalmology October, 2016
• <1% risk within 5 yrs of tx• <2% risk within 10 yrs
8/15/2019
10
Ideal/Lean body weight ?
• Concept is controversial • Historically: 6.5mg/kg based on IDEAL weight, or• 2016: 5mg/kg based on ACTUAL weight
• Females• Baseline: 5 feet, 100 lbs• Add 5 lbs for each additional inch • Example – 5 feet, 7 inches100 + (5 x 7) = 135
• Males • Baseline: 5 feet, 105 lbs• Add 5 lbs for each additional inch
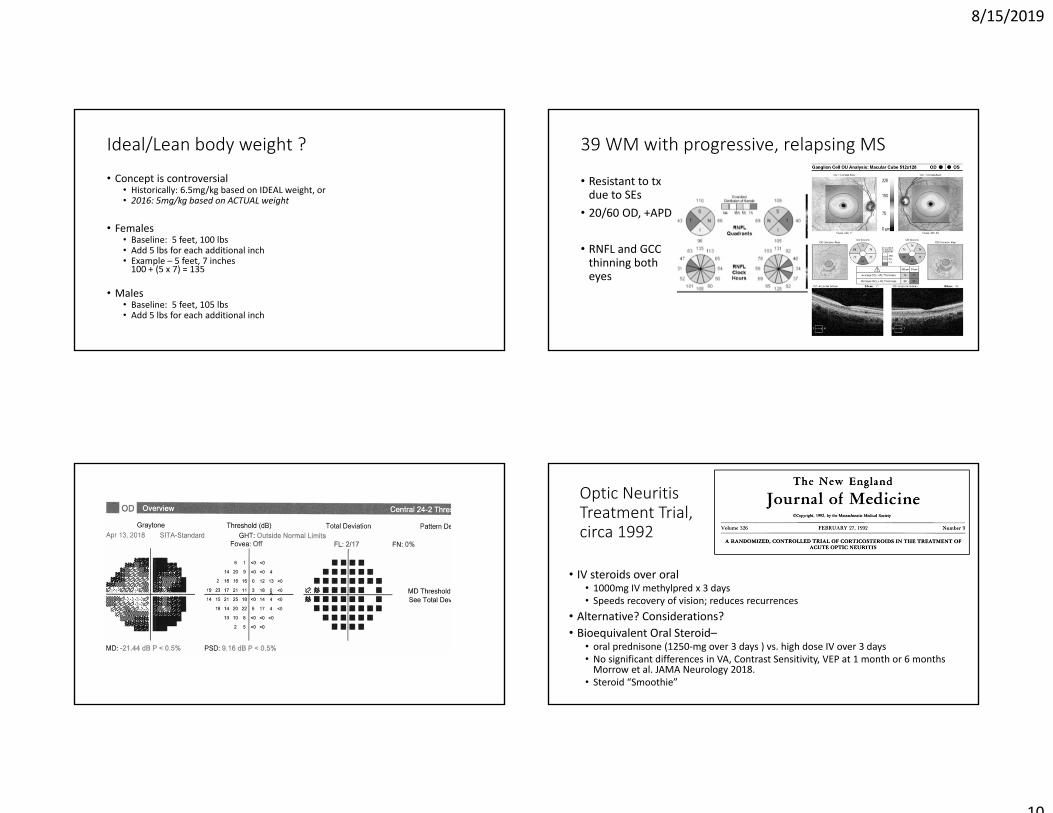
39 WM with progressive, relapsing MS
• Resistant to txdue to SEs
• 20/60 OD, +APD
• RNFL and GCC thinning both eyes
Optic Neuritis Treatment Trial, circa 1992
• IV steroids over oral • 1000mg IV methylpred x 3 days • Speeds recovery of vision; reduces recurrences
• Alternative? Considerations?• Bioequivalent Oral Steroid–
• oral prednisone (1250‐mg over 3 days ) vs. high dose IV over 3 days • No significant differences in VA, Contrast Sensitivity, VEP at 1 month or 6 months Morrow et al. JAMA Neurology 2018.
• Steroid “Smoothie”
8/15/2019
11
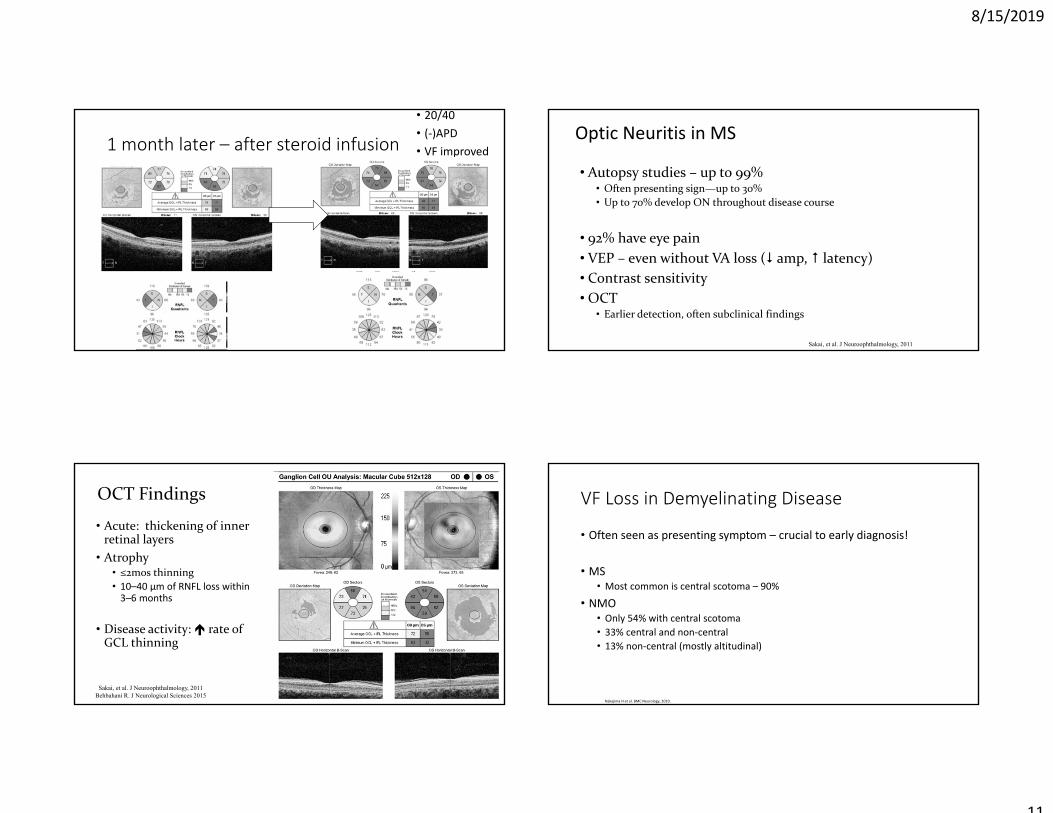
1 month later – after steroid infusion
• 20/40• (‐)APD• VF improved
Optic Neuritis in MS
• Autopsy studies – up to 99%• Often presenting sign—up to 30%• Up to 70% develop ON throughout disease course
• 92% have eye pain• VEP – even without VA loss ( amp, latency)• Contrast sensitivity• OCT
• Earlier detection, often subclinical findings
Sakai, et al. J Neuroophthalmology, 2011
OCT Findings
• Acute: thickening of inner retinal layers
• Atrophy• ≤2mos thinning • 10–40 μm of RNFL loss within 3–6 months
• Disease activity: rate of GCL thinning
Sakai, et al. J Neuroophthalmology, 2011Behbahani R. J Neurological Sciences 2015
VF Loss in Demyelinating Disease
• Often seen as presenting symptom – crucial to early diagnosis!
• MS• Most common is central scotoma – 90%
• NMO• Only 54% with central scotoma• 33% central and non‐central• 13% non‐central (mostly altitudinal)
Nakajima H et al. BMC Neurology, 2010.

8/15/2019
12
31 AA maleHx of MS

8/15/2019
13
Imaging considerations for this patient…??
• CT vs. MRI• With FLAIR
• ±contrast• ±angiography• Location to scan• ±urgency
Fingolimod‐Associated Macular Edema (FAME)
• 0.5% of patients taking lower dose (?)• Increased risk for patients with diabetes or hx uveitis (up to 20%!)
• Baseline exam and then 3‐4 mos after therapy
• Majority are unilateral• Patients may be asymptomatic
Retinal Ganglion Cell – promising biomarker in MS• GCIPL thickness measurements were reduced within the first 5 weeks of presentation, unlike the RNFL measurements.
• GCIPL thickness was reduced in MS eyes both with and without prior ON
• may be used to examine in vivo and predict visual function • thickness of the GCIPL after 1 to 2 months predicted visual function after 6 months
• GCIPL thickness correlated with visual function, EDSS score, electrophysiological data andMRI findings.
Using RNFL progression to recommend therapy changes, even w/o visual symptoms • Britze J. J Neurology, 2017. • Balk L, et al. Multiple Sclerosis 2017. • Garcia‐Martin. Ophth 2017.

8/15/2019
14
double vision
• Head injury 3 months ago – Imaging in ER all negative
• Vertical diplopia– Worse in down gaze– Right head tilt
double vision
Under‐action LSO
1⁰ gaze – note head posture
Double Maddox Rod??
• Can help determine if SOP is bilateral• often missed due to asymmetry
• MR over both eyes• Small vertical prism over one eye • Cyclodeviated eye will report a “tilted” line
Rotating MR to straighten image of line
Torsion noted on DFEs! Use Double Maddox Rod to help determine if SOP is bilateral ‐‐often missed due to asymmetry

8/15/2019
15
76 year old male with double vision
• Left‐sided headache• Denies Trauma
1⁰ gaze
SO Palsy
• Etiology• Trauma• Decompensated congenital – slow onset
• Least likely of EOM palsies to have underlying etiology, BUT….
• Microvascular disease• Brain abnormality
• Treatment • Prism, surgery, botox
Imaging, careful follow up
EOM palsies: Do not assume……
1. Vasculopathic 16.5% thought to be ischemic had another cause (neoplasm, MS, GCA)
Tamhankar, et al. Ophthalmology Nov 2013
2. True isolation
And don’t forget about…• GCA• Carotid Artery Dissection • Aneurysm• …

8/15/2019
16
Myasthenia … If/when diplopia doesn’t make sense!
• Tensilon Test – low sensitivity• Icepack Test • Sustained upgaze x 2 min
• Bloodwork – high false negatives • ACH, thymic panel, ANA, DM
• Imaging – 70% have thymic hyperplasia (mediastinal imaging)
Don’t forget about giant cell arteritis!
• Clinical presentations• Arteritic ION• CN palsies • CRAO
• Labs ‐ if suspected, send to ER and order all of the following:• ESR – 13% are normal • C‐reactive protein – 1% are normal • Platelet count, CBC with differential (anemia often present)
• Biopsy indicated for anyone who is suspected, regardless of ESR• Ultrasound, CTA, …
Patient Labs
CBC – all normal ESR – 15CRP ‐ < 1
If you want to find something wrong, do an MRI…..
• MRI revealed small saccular anneurysm at Right MCA• Brain aneurysm: incidental finding?• Likelihood of relation to problem? • Size
• Unruptured smaIl aneurysms • 3 % of the population
• Risk of rupture• Size• anatomical location
• VOMIT = Victims of Modern Imaging Technology British Med Journal, 2003
Caro d Artery Dissec on → Painful Horner’s
• 48 year old male presents with a big pupil in the left eye.
• ROS: right‐sided neck pain, headache
• Exam• Right eye – miosis, ptosis • Dilates with 0.5% apraclonidine
• Horner’s – 3rd order neuron defect along sympathetic pathway
http://www.cmaj.ca

8/15/2019
17
Carotid Artery Dissection
• Traumatic or spontaneous • Cause of 2.5% of strokes
• 10‐25% of ischemic events in patients <45Rao, J Vasc Surg 2011
Lu A, et al. Emerg Radiol Feb 2015
Carotid Artery Dissection
• Presentation• Headache – up to 69%‐ most common presenting symptom
• Unilateral neck pain – up to 49%• Ipsilateral Horner’s – up to 60% • Visual manifestations associated with artery dissections
• Photopsia• VF defect
• Mgmnt• Immediate Imaging: CT/CTA, MRI/A, T1W with contrast and fat suppression, Doppler
• Anti‐platelets, anti‐coagulant txKwak JH, et al. Neurointervention, 2011.
Pupils can be scary!
Little Pupil Problems Big Pupil Problems APDHorner’s• Neck trauma/surgery• Lung tumor• Lesion sympathetic pathway
Argyll – Robertson • Tertiary syphilis• Diabetic encephalopathy
Adie’s• Idiopathic• Viral
3rd Nerve• Ischemia • Tumor• Aneurysm
Optic nerve diseaseVascular event Demyelinating disease Brain tumor
Don’t forget – Pharmacologic Causes!
Big pupil problem think 3rd N
• Parasympathetic pupillary fibers are located superficially along 3rd CN
• Likely to be affected early with compressive lesion
• Anatomically at risk for aneurysm • 85% are within anterior Circle of Willis• 30‐35% are adjacent to 3rd CN • PCA – most common
• Imaging Considerations
Kanski. Clinical Ophthalmology, 4th Ed

8/15/2019
18
3rd Nerve –a nice overview
Presentation bilateral in 11% complete in 33% isolated in 36%
Etiology trauma (26%) tumor (12%) diabetes (11%) aneurysm (10%) surgery (10%) stroke (8%) infection (5%)
Of 234 patients with diabetes 2/3 due to microvascular ischemia
53% had pupillary involvement-often bilateral
5 had aneurysms
Only 2% of aneurysms spared the pupil.
Painful onset 94% of aneurysm 69% of diabetic cases.
Keane JR, Can J Neuro Sci. 2010 Sep;37(5):662-70.
1400 personally examined patients – 37 years
73 WF, unexplained APD OS
• 20/20• Recent history of vertigo
• MRI revealed small, insignificant meningioma
Incidental Finding: Meningioma
• Most common primary intracranial tumor • 1‐8 per 100,000, increasing with age • If symptomatic: H/A, seizures, neurologic deficit• Tx: surgical, radiosurgical
• Our patient• Size: 6mm is TINY
• <2cm = typically not problematic • 50‐75% will grow over time
• Location? • What now?

8/15/2019
19
31 AAF “nasal margins mildly indistinct; RTC x 1 week for further evaluation”
Early on – can appear as a nasal “C‐shaped” edema
• Temporal area spared
• VA often normal
6 years later…. • 21 AAF• High BMI • MRI clear • Initial opening pressure of 52

8/15/2019
20
Globe Convexity
• Increased ICP will push the globe anteriorly
• Easiest to appreciate with a 9mm scan
• With EDI, can see an anteriorly displaced Bruch’s membrane
Globe convexity is normal here…
Vs…
Normal ONH Sheath Diameter can ease your mind as well…
• Axial images of the optic nerve (V and H)
• 3 mm behind the posterior eye wall

8/15/2019
21
34 year old Caucasian FM• (+) H/A • BMI 34• Meds – Mirena IUD
• MRI – empty sella, flattened sclera, distended ONH sheaths
• hgh
Idiopathic Intracranial HTN
• 90‐98% complain of headache• Nausea/vomiting/dizziness – 40%• Pulsatile tinnitus – 16‐60% • Visual disturbances – 30% • No other neurologic findings (some with VIth palsy)
Mollan SP, et al. Pract Neurol 2018

8/15/2019
22
IIHT – Who Gets It?
• BMI >30• >40 – worse visual outcome• Rapid weight gain – more severe
• Mostly females• Males 10% of the time • Not as likely to have H/A – may not come in
• Race – more aggressive in AA• 3 x more likely to have vision loss• 5 x increase in blindness
• Co‐morbidities • HTN• Sleep apnea
Biousse V et al. Am J Oph 2007, 2012.
Idiopathic Intracranial HTN– Differential Diagnoses
Toxic Oral contraceptivesTetracyclinesSteroidsVitamin ARetinoidsTamoxifenNalidixic Acide
Other Obesity
Disc characteristics: • Tortuous vessels• Blurred margins
• Elevated topography• Disc hemorrhages
Etiologies
• Idiopathic But what causes the papilledema ?
Axoplasmic flow stasis → swollen nerve fibers → compression of venulesin the area and so venous stasis/leakage → accumula on of extracellular fluid
Toxic Oral contraceptivesTetracyclinesSteroidsVitamin ARetinoidsTamoxifenNalidixic Acide
Other Obesity
IIH Treatment Trial – JAMA, April 2014
• acetazolamide + a low‐sodium weight‐reduction diet vs. diet alone → modest improvement in visual field function
• OCT Substudy of the IITT, Ophthalmology, Sept 2015
• RNFL and Total Retinal Thickness (TRT) useful in following and monitoring response to treatment
• Better RNFL thickness, TRT, and ONH volume swelling measurements

8/15/2019
23
Acetazolamide + Low Sodium/Wt Loss Diet • Contraindications:
• Sulfa allergy? • chemical structure different than antibiotics – little evidence of cross‐sensitivity
• consider avoiding if hx of severe reaction • Long‐term: liver, kidney disease, severe COPD• Caution with sickle cell• Caution with low potassium
Common Side Effects
paresthesia metallic tastefatiguemalaiseGI disturbancesdecreased libido
metabolic acidosiselectrolyte imbalance (including hypokalemia)renal calculiblood dyscrasias
Than T, Smith H. http://www.reviewofoptometry.com/ce/10‐must‐have‐oral‐meds.
125,250mg tablets, and 500mg SR capsules (Diamox Sequels, DuramedPharmaceuticals)
The Idiopathic Intracranial Hypertension Treatment Trial. JAMA 2014
Treatment Goals …
• Visual Fields – for life • OCT • Labs ? • Co‐management ?
Mollan SP, et al. Pract Neurol 2018Cello KE J Neuroophth 2016
After 1 month of 250mg Diamox BIDstill (+) H/A
2 mos, then 5 mos(now TID Diamox)Denies H/A

8/15/2019
24
Watching VF carefully…
• H/A’s improved• RNFL thickness reduced
• Total volume reduced
And now… • Extracellular edema leads to venous stasis…
Other treatment options….
• Surgical – controversial and provider‐dependent • Ventricular‐peritoneal shunt • Optic nerve sheath fenestration
• Repeated lumbar puncture ? • Not well reported • Procedure ‐ causes anxiety, local discomfort, complications, headache • LP‐induced reduction of ICP is only short‐lived
• On the horizon • Topamax – off label • Bariatric surgery – in trials