systemic management of breast cancer dr alice musibi medical oncologist kenyatta national hospital
TRANSCRIPT
SYSTEMIC MANAGEMENT SYSTEMIC MANAGEMENT OF BREAST CANCEROF BREAST CANCER
Dr Alice MusibiDr Alice Musibi
Medical OncologistMedical Oncologist
KENYATTA NATIONAL KENYATTA NATIONAL HOSPITALHOSPITAL

BREAST CANCERBREAST CANCERINTRODUCTIONINTRODUCTION• Is one of the deadliest and most Is one of the deadliest and most
common cancers ailing women all over common cancers ailing women all over the worldthe world
• In Australia 1 in 13 women will develop In Australia 1 in 13 women will develop ca breast at sometime in her lifeca breast at sometime in her life
• In USA 215,990 women will be found to In USA 215,990 women will be found to have invasive ca breast in 2004have invasive ca breast in 2004
• More common in older than younger More common in older than younger women with average age of diagnosis of women with average age of diagnosis of 64 years64 years

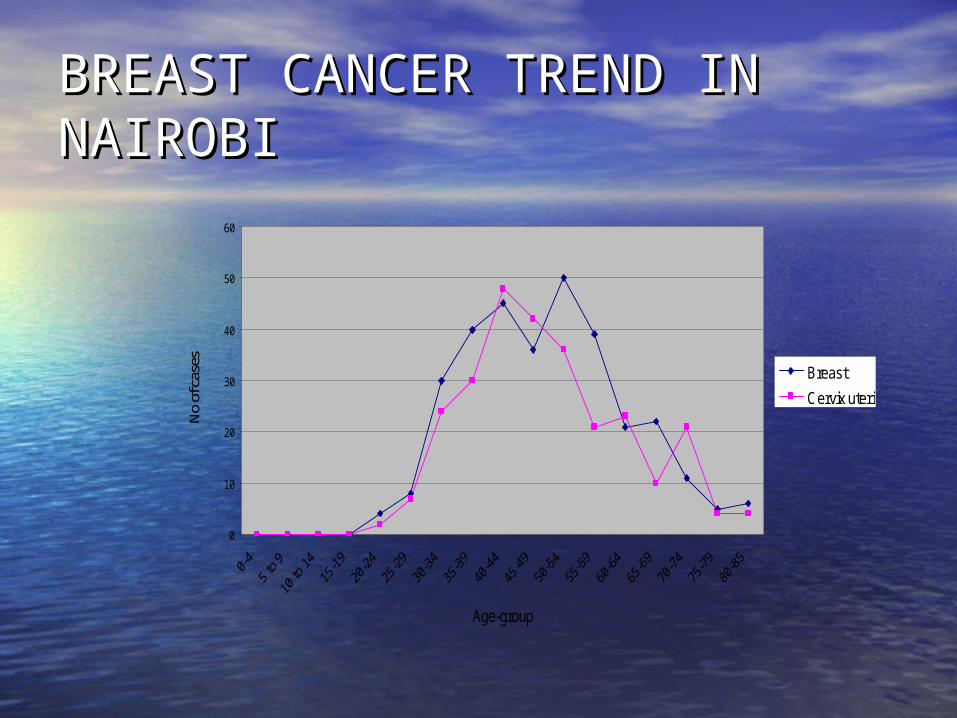
CANCER IN NAIROBI CANCER IN NAIROBI (KENYA)(KENYA)• A total of 2,716 cases were registered, A total of 2,716 cases were registered,
comprising of 1246 men and 1470 comprising of 1246 men and 1470 women between 2000-2003women between 2000-2003
• Breast cancer was leading with 22.9% Breast cancer was leading with 22.9% followed by cervical cancer with 19.3%followed by cervical cancer with 19.3%
• The mean age of diagnosis was 45 The mean age of diagnosis was 45 yearsyears

Most Common Cancers for all Cases Registered (2000 - 2002)
4.2
3.0
9.4
0.9
6.9
3.7
5.7
3.4
7.1
10.0
14.8
2.4
2.1
3.3
20.0
23.3
2.4
2.6
2.1
2.0
3.3
4.4
7.2
20.0 15.0 10.0 5.0 0.0 5.0 10.0 15.0 20.0 25.0 30.0
C82-C85;C96 Non-Hodgkin lymphoma
C69 Eye
C61 P rostate
C56 Ovary
C53 Cervix Uteri
C50 Breast
C46 Kaposi sarcoma
C44 Other Skin
C22 Liver
C18 Colon
C16 Stomach
C15 Oesophagus
C00-C14,C30-C32 & C73 Head & neck
ICD-10
Percentage (%) of All Cases
Male Female
0
10
20
30
40
50
60
Age-group
No
of c
ases Breast
Cervix uteri
BREAST CANCER TREND IN BREAST CANCER TREND IN NAIROBINAIROBI



TreatmentTreatment
• Local managementLocal management– 18th century – Louis Petit 18th century – Louis Petit
of France - total of France - total mastectomy and excision mastectomy and excision of axillary's lymph nodesof axillary's lymph nodes
– 1895 - William Halstead - 1895 - William Halstead - popularized radical popularized radical mastectomy mastectomy
– Harvey Cushing - Harvey Cushing - extended radical - internal extended radical - internal mammary chain excised mammary chain excised after splitting the after splitting the mediastinummediastinum
– 1923-1937 - local excision 1923-1937 - local excision and radium needles. and radium needles.
– Conventional radiotherapyConventional radiotherapy
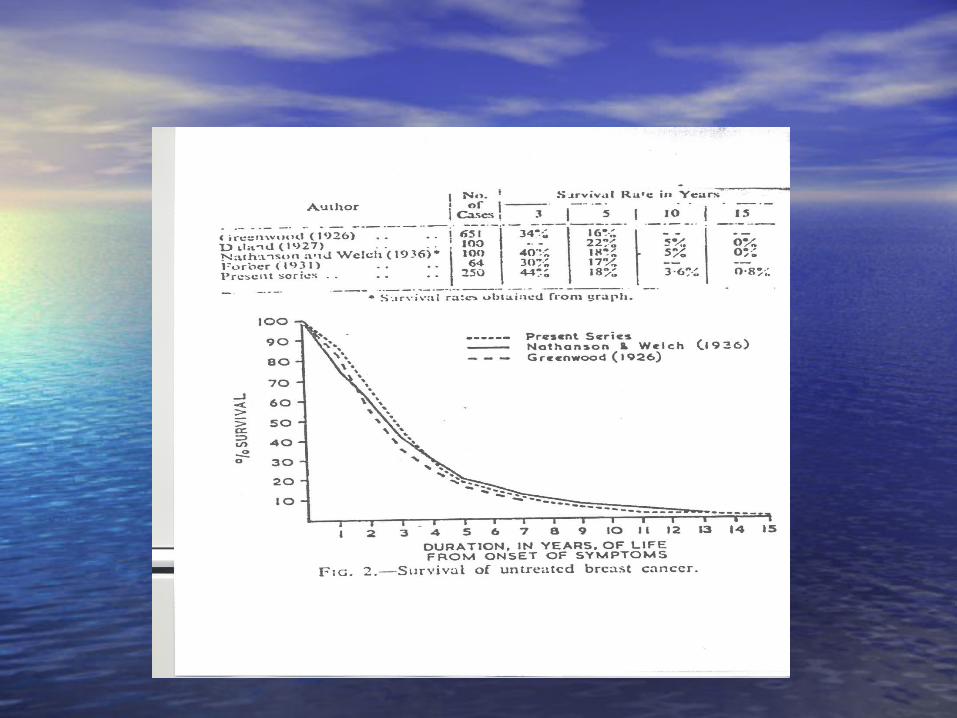
Out-comeOut-come
• Poor overall results of survival Poor overall results of survival
• Frequent local recurrence and distant Frequent local recurrence and distant metastasesmetastases
• Treatment worse than diseaseTreatment worse than disease• Concept of quality lifeConcept of quality life• Women’s insistence for breast Women’s insistence for breast
preservationpreservation

Treatment Treatment
• MultidisciplinaryMultidisciplinary– SurgerySurgery– Chemotherapy, Chemotherapy,
hormonal therapy, hormonal therapy, immunotherapyimmunotherapy
– Radiation therapyRadiation therapy– Palliative therapyPalliative therapy– Occupational/Occupational/
physiotherapyphysiotherapy• Lymph edema therapyLymph edema therapy
– etcetc

Systemic therapySystemic therapy
•Types Types – Primary induction Primary induction
therapytherapy– Neo-adjuvant Neo-adjuvant
chemotherapychemotherapy– Adjuvant Adjuvant
chemotherapychemotherapy– Palliative Palliative
• Associated withAssociated with– a decrease in the a decrease in the
death rate death rate – prolonged prolonged
relapse-free relapse-free survivalssurvivals
• Acute and Acute and chronic side chronic side effectseffects

Systemic therapy- Systemic therapy- combinationcombination
– Maximum cell kill Maximum cell kill – Tolerable range of Tolerable range of
toxicity for each toxicity for each drugdrug
– Broader range of Broader range of interaction between interaction between drugs and tumor drugs and tumor cellscells
– Less chance of Less chance of developing cellular developing cellular drug resistancedrug resistance
Adjuvant systemic therapyAdjuvant systemic therapy
• For patients at risk of For patients at risk of disease recurrence after disease recurrence after treatment of primary treatment of primary tumiortumior
• Known tumor or maximum Known tumor or maximum bulk should be removedbulk should be removed
• Chemotherapy started as Chemotherapy started as soon as possible post opsoon as possible post op
• Effective chemotherapy Effective chemotherapy must be used at maximally must be used at maximally tolerated dosestolerated doses
• Usually for a period (6-8 Usually for a period (6-8 cycles)cycles)
• Milan CMF trial Milan CMF trial (overview)- (overview)- – CMF vs. surgery aloneCMF vs. surgery alone
• Relapse free survival- Relapse free survival- median 19.4median 19.4
– benefits in pre-benefits in pre-menopausal patientsmenopausal patients
(Bonnadona G et al N Engl. J Med (Bonnadona G et al N Engl. J Med 1995;332;901)1995;332;901)
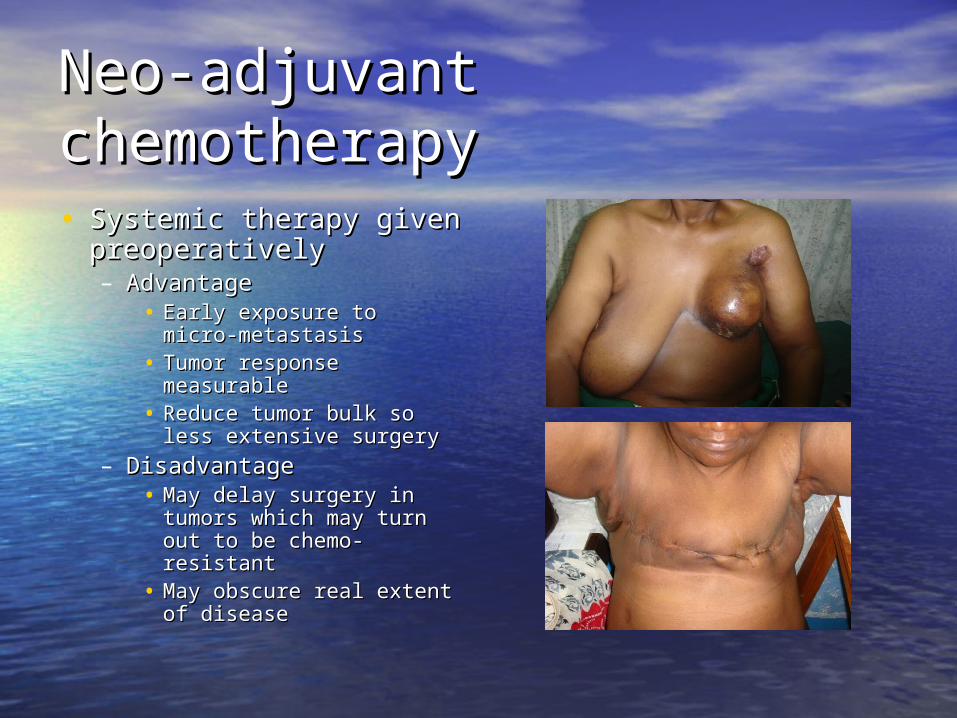
Neo-adjuvant chemotherapyNeo-adjuvant chemotherapy
• Systemic therapy given Systemic therapy given preoperativelypreoperatively– Advantage Advantage
• Early exposure to micro-Early exposure to micro-metastasismetastasis
• Tumor response Tumor response measurable measurable
• Reduce tumor bulk so Reduce tumor bulk so less extensive surgeryless extensive surgery
– DisadvantageDisadvantage• May delay surgery in May delay surgery in
tumors which may turn tumors which may turn out to be chemo-resistantout to be chemo-resistant
• May obscure real extent May obscure real extent of diseaseof disease
Choice of treatment regimeChoice of treatment regime
• Depends on prognostic Depends on prognostic factors for factors for recurrence/survivalrecurrence/survival– Age Age – tumour size, tumour size, – nodal status nodal status – histologic grade, histologic grade, – hormone receptors, hormone receptors, – ??Her-2/neu over-??Her-2/neu over-
expression (about expression (about 40% of breast 40% of breast cancers)cancers)
– ?Lymphatic/vascular ?Lymphatic/vascular invasion) invasion)
– Estimated benefit of Estimated benefit of therapy in terms of therapy in terms of absolute risk reduction absolute risk reduction of relapse and death.of relapse and death.
– Estimation of the Estimation of the toxicity associated with toxicity associated with therapytherapy
– [COST][COST]
Prognosis Prognosis
• Five year relative survival is dependent on the Five year relative survival is dependent on the stage of breast cancer at diagnosisstage of breast cancer at diagnosis
StageStage Survival rateSurvival rate00 100%100%II 98% 98%
IIAIIA 88% 88%IIBIIB 76% 76%
IIIAIIIA 56% 56% IIIBIIIB 49% 49%
IVIV 16% 16%*(Overview American Cancer Society –2003)**(Overview American Cancer Society –2003)*
Post-surgical Mx of breast Post-surgical Mx of breast cancer (KNH) [1989-2000]cancer (KNH) [1989-2000]
• SurgerySurgery -- 374 patients374 patients• ChemotherapyChemotherapy
– Adjuvant -Adjuvant - 22 (5.8%)22 (5.8%)– MetastaticMetastatic -21-21
• RadiotherapyRadiotherapy– AdjuvantAdjuvant -- 46 (12.4%)46 (12.4%)– PalliationPalliation -- 5353
• Hormone therapy (tamoxifen)Hormone therapy (tamoxifen) -- 126 126 (33.7%)(33.7%)
• East African Medical Journal: 2002 79(3): 156-162 East African Medical Journal: 2002 79(3): 156-162
Metastatic breast cancer (MBC)Metastatic breast cancer (MBC)
• MBC is considered an incurable disease.MBC is considered an incurable disease.• majority of patients with MBCmajority of patients with MBC do not do not
survive beyond 5 years after diagnosis.survive beyond 5 years after diagnosis.• TreatmentTreatment usuallyusually is palliative with is palliative with
systemic therapysystemic therapy includingincluding– chemotherapychemotherapy– hormonal treatmenthormonal treatment– biologic therapy (e.g. Trastuzumab)biologic therapy (e.g. Trastuzumab)
• Pain controlPain control

MBC -2MBC -2
• The surgery of breast tumors with distant The surgery of breast tumors with distant metastases has been indicatedmetastases has been indicated to to – prevent local complications (toilet surgery)prevent local complications (toilet surgery)– Removal of the metastatic lesions in selectedRemoval of the metastatic lesions in selected
patients (single brain, liver, bone or pulmonary patients (single brain, liver, bone or pulmonary lesions).lesions).
• Surgery of the primary tumor can actually Surgery of the primary tumor can actually improveimprove survival of metastatic breast cancer.survival of metastatic breast cancer.– especially in patients with only bone metastasesespecially in patients with only bone metastases
• (JCO(JCO, Vol 24, No 18 (June 20), 2006: pp. 2743-2749), Vol 24, No 18 (June 20), 2006: pp. 2743-2749)

Many of our women are Many of our women are presenting like this!!presenting like this!!
Lack of information
Poverty
Fears
Fatalism
Lack of medical
insurance
False beliefs
Language
Knowledge Attitude Behavior

Risk factorsRisk factors
• Normal lifetime risk of developing Normal lifetime risk of developing breast cancer in white women is 1 in breast cancer in white women is 1 in 8 or 98 or 9
• There is no family history in over There is no family history in over 75% of patients75% of patients
• Most women with breast cancer do Most women with breast cancer do not have any identifiable risk factorsnot have any identifiable risk factors
Risk factorsRisk factors
• AgeAge• Ethnicity – more cancer in white Ethnicity – more cancer in white
women but more mortality in women but more mortality in blacksblacks
• Family history of breast cancerFamily history of breast cancer• Previous history of personal breast Previous history of personal breast
cancer gives 1-2% risk of cancer gives 1-2% risk of contralateral breast cancer/yearcontralateral breast cancer/year
• Previous history of ovarian or Previous history of ovarian or endometrial cancersendometrial cancers
• Prolonged estrogen exposureProlonged estrogen exposure– Early menarche (under age 12)/late Early menarche (under age 12)/late
menopause (after age 50)menopause (after age 50)– Late first pregnancy/nulliparous/no Late first pregnancy/nulliparous/no
full-term pregnancy (1.5 times full-term pregnancy (1.5 times higher incidence)higher incidence)
– Hormone replacement therapy Hormone replacement therapy especially high estrogen based pills especially high estrogen based pills but more so the combined pillsbut more so the combined pills
• Genetic predispositionGenetic predisposition• BRCA1 (85%) BRCA1 (85%) • BRCA2BRCA2• p53 gene – 1% in women with p53 gene – 1% in women with
cancer of breast below 40 yearscancer of breast below 40 years
• Lifestyle factorsLifestyle factors– Dietary factors – particularly Dietary factors – particularly
increased fat consumptionincreased fat consumption– ObesityObesity– Lack of exerciseLack of exercise– Alcohol consumptionAlcohol consumption– Smoking (???)Smoking (???)
• Prior Radiation therapyPrior Radiation therapy• Atypical epithelial hyperplasia of Atypical epithelial hyperplasia of
the breastthe breast• Fibrocystic disease with Fibrocystic disease with
proliferative changesproliferative changes• Lobular carcinoma in situ (LCIS)Lobular carcinoma in situ (LCIS)

Recommendations Recommendations
Government-Acknowledge
the volcano in cancer
Policy National guidelinesClinical practice
guidelines

Recommendations Recommendations
• Clinical breast Clinical breast examination examination
• U/SU/S
• MammographyMammography
• MRI scans of breastMRI scans of breast
• Genetic mappingGenetic mapping

RecommendationsRecommendations
• FacilitiesFacilities– Cancer centres – 1 (KNH) Cancer centres – 1 (KNH) – Laboratories Laboratories
• ordinary histopathology ordinary histopathology
• immunohistochemical immunohistochemical studiesstudies
– KEMRI mainly research KEMRI mainly research purposespurposes
– Private hosp (Nbi, Private hosp (Nbi, AKUH) – all send the AKUH) – all send the specimens to SA or Italyspecimens to SA or Italy
– Radiotherapy units – 2Radiotherapy units – 2