tackling child poverty egistered nurse - speaking out for...
TRANSCRIPT

January/February 2009
J O U R N A LRegistered NurseTackling child poverty • Helping those at risk of suicide • Discovering hope in the NICU
SAYNO TONAUGHTYNURSE IMAGE
RNs speak out against ad campaigns that stereotype nurses to sell everything from vodka to gum.
Registered Nurse Journal 3
Registered NurseJ O U R N A L
T H E L I N E U P
EDITOR’S NOTE 4
PRESIDENT’S VIEW 5
EXECUTIVE DIRECTOR’S DISPATCH 6
NURSING IN THE NEWS 7
OUT AND ABOUT 9
MAILBAG 10
POLICY AT WORK 25
NEWS TO YOU/NEWS TO USE 26
CALENDAR 27
Volume 21, No. 1, January/February 2009
F E A T U R E S
11 LIFE AND DEATH IN THE NICUBy Olivia GerardiA McMaster University nursing student explainshow her first experience in a critical situation helped her to realize that RNs don’t just care for bodies,they care for lives.
12 SAY NO TONAUGHTY NURSE IMAGEBy Jill ScarrowRNs are outraged and insulted over advertising and media images that depict them – and the profession – as sexy.
17 EASING POVERTY THROUGH EDUCATION By Jill ScarrowCarolyn Acker launched Pathways to Education eight years ago to encourage kids to stay in school.
18 BELOW THE POVERTY LINE By Jill ScarrowOntario’s much-anticipated poverty reduction strategy lays out measures to decrease the number of children living in poverty.
22 A CRY FOR HELP By Kimberley KearseyRNAO’s new suicide prevention BPG puts nurses in a position to provide resources and help to patients at risk of taking their own lives.
24 FORTY MINUTES TO SAVE A LIFE By Helena MoncrieffCardiac patient with rare but deadly condition thanks “powerhouse” RN for keeping her alive.
18
Cover illustration: Maurice Vellekoop

4 January/February 2009
Editor ’s NoteThe journal of the REGISTERED NURSES'ASSOCIATION OF ONTARIO (RNAO)158 Pearl Street Toronto ON, M5H 1L3Phone: 416-599-1925 Toll-Free: 1-800-268-7199Fax: 416-599-1926Website: www.rnao.org E-mail: [email protected] to the editor: [email protected]
EDITORIAL STAFFMarion Zych, PublisherKimberley Kearsey, Managing Editor Jill Scarrow, WriterStacey Hale, Editorial Assistant
EDITORIAL ADVISORY COMMITTEECarmen James-Henry (Chair)Joseph Gajasan, Shannon Landry,Nancy Purdy, Ruth Schofield, Nathan KellyPauline Tam (journalist),Carol Mulligan (journalist)
ART DIRECTION & DESIGNFresh Art & Design Inc.
ADVERTISINGRegistered Nurses' Association of OntarioPhone: 416-599-1925, Fax: 416-599-1926
SUBSCRIPTIONSRegistered Nurse Journal, ISSN 1484-0863, is a benefit tomembers of the RNAO. Paid subscriptions are welcome. Full sub-scription prices for one year (six issues), including taxes: Canada$37.80 (GST); Outside Canada: $42. Printed with vegetable-based inks on recycled paper (50 per cent recycled and 20 percent post-consumer fibre) on acid-free paper.
Registered Nurse Journal is published six times a year byRNAO.The views or opinions expressed in the editorials, articles oradvertisements are those of the authors/advertisers and do notnecessarily represent the policies of RNAO or the EditorialAdvisory Committee. RNAO assumes no responsibility or liabilityfor damages arising from any error or omission or from the use ofany information or advice contained in the Registered NurseJournal including editorials, studies, reports, letters and advertise-ments.All articles and photos accepted for publication becomethe property of the Registered Nurse Journal. Indexed inCumulative Index to Nursing and Allied Health Literature.
CANADIAN POSTMASTER: Undeliverable copiesand change of address to: RNAO, 158 Pearl Street,Toronto ON, M5H 1L3. Publications Mail AgreementNo. 40006768.
RNAO OFFICERS AND SENIOR MANAGEMENTWendy Fucile, RN, BScN, MPA, CHEPresident, ext. 504
Mary Ferguson-Paré, RN, PhD, CHEImmediate Past President, ext. 502
Doris Grinspun, RN, MSN, PhD (c), O.Ont.Executive Director, ext. 206
Robert Milling, LL.M, LLB Director, Health and Nursing Policy
Daniel Lau, MBA Director, Membership and Services, ext. 218
Anitta Robertson, RN, BAAN, MPADirector, Centre for Professional Nursing Excellence, ext. 240
Irmajean Bajnok, RN, MScN, PhDDirector, International Affairs and Best PracticeGuidelines Programs, ext. 234
Marion Zych, BA, Journalism, BA, Political ScienceDirector, Communications, ext. 209
Nancy Campbell, MBADirector, Finance and Administration, ext. 229
Louis-Charles Lavallée, CMC, MBADirector, Information Management and Technology
BPG brings back memories of decades-old loss
While researching and writing this issue’s feature aboutRNAO’s new suicide prevention best practice guideline (pg.22), I was surprised to learn 4,000 Canadians die by suicideevery year. Each of those 4,000 people has family, colleagues,and friends who are left grieving the loss and trying to makesense of the tragedy.
“In every family and in each community, the aftermath of adeath by suicide is as painful and tragic as it is profound and far-
reaching,” the guideline states.Given this reality, I bet you too can recall your own feelingsof sorrow that someone you knew – up close or from a distance – took their own life.
My experience with suicide takes me back to high school, when one of my bestfriends found her life grinding to a halt after her mother – depressed and in an unhappymarriage – tried to ease her pain by drinking a fatal cocktail of washer fluid. Her deathtouched our tight-knit group in a profound way because we simply didn’t know it wascoming.“Who could have predicted it?” we all asked as we tried to make sense of it.
Reading the new BPG more than 20 years later, I was taken back to that time. Istarted to relate my own experience to the evidence revealed in the guideline andbegan to realize there likely was someone who could have predicted it. And thatsomeone was probably a nurse.
Statistically, it’s safe to assume my friend’s mother cried out for help before shedecided to end her life. Most suicidal individuals do.The only question is whether shefound someone who would listen and act on her behalf.
Knowing what I do about nursing after eight years at RNAO, I shouldn’t be sur-prised by the instrumental role RNs would have played in the lives of both my friendand her mother. As a typical teenager when this tragedy took place, I didn’t realizehow a nurse could help. But I’m glad I see it now. It sheds a new light on that heart-break so long ago, and it provides me with a sense of hope that if a young teenagerfinds themselves in the same situation my friend did all those years ago, they may justmeet a nurse who has read the BPG and can provide the hope and guidance they need.
Kimberley KearseyManaging Editor

Registered Nurse Journal 5
It’s been 10 years.A decade of energy,commitment andever-increasing effec-tiveness. In January,RNAO went toQueen’s Park for the10th year in a row.
We were 135 strong and we connectedwith 47 political leaders and/or their staff,including 20 cabinet ministers.What a day.
RNAO’s annual visit to Queen’s Park,at which time we have the opportunity notonly to hear but to be heard, is at its heart afundamental exercise of our basic demo-cratic responsibility to participate, to speakup, and to engage with our political leadersin respectful discussion and debate.
My introduction to politics was bothsimple and profound. Coming of age, atleast politically, in the Canada of the 60s,my beliefs and hopes were in large partkindled by the wave of ‘Trudeau-mania’that swept our country. Although thosesame beliefs and hopes were shaken onedark, cold October night as the WarMeasures’ Act was proclaimed, they havenonetheless remained with me these manyyears. We are called, as individuals, as citi-zens, as nurses, to step up, not back; to givevoice, not silence; to lead, not acquiesce, inthe face of challenges.
And those challenges are many.The issues that we addressed at Queen’s
Park run the gamut from the need tostrengthen Medicare to the value of a com-prehensive provincial breastfeeding strategy.From the critical role that nurses can play innew and emerging roles (as exemplified byNP-led clinics and registered nurse firstassistants) to the urgent need to address vio-lence in our workplaces and threats to thenursing education system. Above all, a clearmessage was sent to government that it mustget back on track and deliver the 9,000additional nurses it committed to during the2007 election and Throne Speech.The pub-lic – and nurses – expect it.
When I was a much younger woman, Ilearned an important lesson in politics, andit did not come from the Canadian con-text. Rather, this particular learning camefrom a series of books by Allen Drury, anAmerican author, beginning with Adviseand Consent. These books, fictional innature but set within the context of theAmerican political system, taught mesomething that I hadn’t until then realized:politicians are just like you and me. Theyare individuals – good, bad, indifferent.
They have strengths – few, some, many.And they enter public life, most often, withthe intent to do something to improve thelives and situations of others. Sound likesomeone you know? Sound like a nurse,perhaps? Discovering this human face ofthe political leader was an importantmoment for me, although I did not realizethat for a number of years.
Over time it has become popular tobash our politicians. Sometimes this may bemerited. In fact, many people delight indisparagement and sarcasm. It’s something Iam ashamed to say I too have stooped tofrom time to time. But if we consider whatwe know from our nursing practice – thatrelationship is the foundation for every-thing and that respectful honesty is the keyto moving that relationship forward – thenit seems to me that we are best served by
practising that same approach in our politi-cal dealings.
Offering encouragement at difficulttimes, praise for success achieved, challengefor commitments missed, clarity of goal,and sustained engagement; these approach-es work with patients, and they can workwith our political representatives too.
Each of you can become engaged in thepolitical life of our province. And youropportunity is now.
During Nursing Week (May 11-17),RNAO will again be organizing Take YourMPP to Work. I have been involved in thisinitiative many times over the years, withmy own MPP and last year with thenMinister of Health George Smitherman.The chance to spend time speaking direct-ly with our MPPs, to put a human face onwhat nurses do every day, to underline thebreadth and depth of our skills – it’s price-less. And although we may not see aninstant change in policy, every time weengage in this way we are building the roadthat leads us towards healthy public policy.
I hope that you will step up and beheard at a Take Your MPP to Work event inyour community. Lead the way by invitingyour local representative to see what youdo, to experience the strength of nurses inyour workplace, to witness first-hand thechallenges that RNs face, and to see thethanks of patients and colleagues for thework you do 24/7.
As we have for the past decade, RNAOand its members will spend one day duringNursing Week with individual men andwomen who, like nurses across our province,have chosen to serve.They, like nurses, willhave had moments of great joy and greatsadness, moments of courage and of fear,moments of clarity and confusion. We willmeet with them as individual RNs who rep-resent the faces and voices of the thousandsof patients we serve every day. RN
WENDY FUCILE, RN, BScN, MPA, CHE, IS
PRESIDENT OF RNAO.
Pres ident’s View with Wendy Fuci le
Political activity a basic democratic responsibility
‘‘Each of you can
become engaged in the
political life of our
province. And your
opportunity is now. ”

Executive Director ’s Dispatch with Doris Grinspun
In this issue of theJournal, we tackle thenaughty nurse personathat has been infuriat-ing nurses – myselfincluded – for years. Itis mind-boggling thatdespite the many public
opinion polls that have rated nurses moretrustworthy than any other professionalgroup, advertising companies and marketingmoguls continue to pitch their products byperpetuating damaging images of nurses assex objects. I say: shame on them.
Not only are naughty nurse imagestremendously wrong and obnoxiouslyoffensive, they also contribute to harass-ment in the workplace and disrespect forwomen in general, nurses in particular. It’sgot to stop.
Stereotypes such as these start with anoverall perception of women as sex objects,which disregards their personal and intel-lectual capabilities, and reduces women toinstruments of sexual pleasure. In somecases, this objectification can be accompa-nied by violence.
It’s a gendered script, ingrained in ourpsyches since we were little boys and girls. It’sfed by images in books, movies, video gamesand, of course, advertising campaigns. It goesback to a time well before Nightingale, andstretches well beyond nursing.
These stereotypes reflect the statusafforded to women by society. Althoughthat status is slowly changing – women arefree to work and vote, which was not thecase in much of the 20th century – thereare still substantive differences betweenmen and women across most of the world,including right here at home.You can see itin indicators of income. Who earns morethan whom for equal work? You can see itin power distribution.Who holds politicaland corporate power? And you can see it inthe tragic statistics of violence againstwomen. It’s even present at some of ourown dinner tables.
Nursing does not stand alone on thereceiving end of these societal ills, but as aprofession we are an easy target because ofour female predominance and our closecontact with the human body.There is lit-tle doubt that if the majority of nurseswere men, we wouldn’t be writing as manyaction alerts and letters of complaint toadvertising companies or their regulators.
You might be asking yourself: ‘Whatcan I do about it?’The answer is simple. Itdoesn’t require picket signs or protests.Andit’s not going to detract from the importantwork you do every day. In fact, your day-to-day nursing practice is the key. Talk itup and talk it loud, in richness of detail,with knowledge and compassion.
Tell the public, through your deeds andwords, that you and all nurses are knowl-edge workers. Remind them that nursesare neither angels nor sex objects, and thatsuch images are demeaning to the profes-sion at large, to us as individuals, and to ourfamilies and friends. Just imagine theinstant respect we would gain if every oneof the 91,000 RNs practising in Ontariowere to talk each and every day about theknowledge and skill she/he brings to their
work, the difficult activities they engage in,and the procedures they perform.Think ofthe power this truly authentic image ofnursing would have, especially when it’scoupled with the public trust we alreadyknow exists.
Talking about our knowledge is notsomething nurses naturally do. I meet anddialogue with hundreds of RNs across thisprovince every year. Most instinctively placecaring and nurturing at the forefront oftheir conversations, leaving little or no timefor sharing details of the breadth and depthof their clinical expertise. This inclinationwas particularly clear when we called onyou, our members, to tell us your nursingstories for publication in the Journal lastsummer. The majority of submissions, allcompelling, focused on reflections of com-passion and humanity.Almost none featuredreflections of knowledge and skill. There’sno doubt both are important, but we needto see more of the latter if we are to gener-ate the essential respect to augment the trustour profession has so deservedly earned.
It’s our collective and individual respon-sibility to remind everyone we meet – andto consistently remind ourselves – thatnursing is about thinking, doing and being.It’s as much about cognitive capabilities andeffort as it is about physical and emotionalwork. It’s about comforting wounded soulsand curing wounded bodies.
Knowledge and advocacy, combined,offer a unique opportunity to trigger sys-temic change that serves nurses and theirpatients and creates egalitarian societiesthat benefit both women and men.
Meanwhile, if you see more ads thatperpetuate damaging images, let us knowand we will remind those advertising com-panies and the marketing moguls who leadthem that nurses help people and commu-nities to stay healthy. We prevent disease.And we save lives. RN
DORIS GRINSPUN, RN, MSN, PhD (CAND),
O.ONT, IS EXECUTIVE DIRECTOR OF RNAO.
Nurses are knowledge workers, not angels or sex objects
6 January/February 2009
It’s our collective
and individual
responsibility
to remind everyone
we meet – and to
consistently remind
ourselves – that nursing
is about thinking,
doing and being.

Registered Nurse Journal 7
Nursing inthenewsRNAO & RNs weigh in on . . .
by Stacey Hale
Jan. 5, Sudbury NPs Marilyn Butcher and Roberta Heale
announced they were expanding their nurse practitioner-
led clinics with a new location set to open its doors in Lively, Ontario.
“It has been a very long time in the making,” Butcher told the Sudbury
Star (Jan. 5). The new location is scheduled to open in December 2009,
and will place a strong emphasis on disease prevention and manage-
ment. Combined, the two clinics are expected to treat about 5,000
patients. Staff will include six nurse practitioners, one registered nurse,
two physicians, a social worker, a dietitian, and a pharmacist. Butcher
and Heale are excited about opening the second clinic because it will
give them the space they need to offer a range of health-care services.
“It certainly will be a significant site,” Butcher said.
The Ontario government has promised 25 additional nurse
practitioner-led clinics across the province. Locations for three have
already been announced: Sault Ste. Marie, Erie St. Clair LHIN and
North West LHIN. RNAO is calling on the government to announce
funding for 10 of the remaining 22 clinics this year so that patients
without access to a health provider can get the care they need. RN
RIGHT: NPs MarilynButcher (left) andRoberta Heale (right)host a press confer-ence to announce theexpansion of theSudbury NursePractitioner-Led Clinicsinto Lively, Ontario.LEFT: NPs JenniferClement (centre) andKim Demers (right)will begin working atLively’s NP-led clinic.Physician Tara Leary(left) will join them.
SUDBURY NP CLINIC EXPANDS ITS OPERATION
ON
Time to put competitive bidding to rest In mid-December, Health Minister DavidCaplan announced the government waslifting a province-wide moratorium on thecompetitive bidding of home-care con-tracts.The moratorium was put into placea year ago by former Health MinisterGeorge Smitherman following anannouncement that the Victorian Order of Nurses (VON) and St. Joseph’s HomeCare had been disqualified from biddingon contracts in Hamilton. Residentsprotested after learning the news, angeredthat the two non-profit organizations wereout of the running despite having servedthe community for more than a century.
“By opening up the delivery of care tocompetitive bidding (and) askingagencies…to submit bids and try and find thelowest cost to deliver care,we tremendously
undermine and devalue the importance ofthat care,”RNAO President Wendy Fuciletold 820 AM radio listeners in Hamilton(Dec. 20).“It’s often hard for vulnerable people, especially seniors, to accept someonecoming into their home.To think that the(caregivers) they’ve become comfortable withcan’t come anymore because of this contractbidding issue, it’s just reprehensible.”
RN returns from Saudi Arabia to take on new duties After five years of nursing in Saudi Arabia,RNAO member Barbara Savage is backhome in Ontario and ready to take on thenew role of Manager, Nursing Services,at Kemptville District Hospital (KDH).Savage moved to Riyadh, Saudi Arabia’scapital city, in September 2001 and begancaring for members of the country’s royalfamily. She also worked at an 850-bed
hospital.“It’s just very different there,”she said, adding that she had to wear abulky black gown to work and in publicto conceal her figure. In her new positionat KDH, Savage’s management style ismore in line with Canadian culture.“I’m a facilitator. I want to make it easierfor nurses to come to work and be happy.”(Kemptville EMC, Jan. 1)
Barbara Savage on camel-back in Saudi Arabia

Coalition calls on government toprotect vulnerable populationsOn Dec. 18, a network of agencies,poverty activists and business people calledon the federal government to create aRecession Relief Fund for agencies providingservices to children, the unemployed,seniors, people with disabilities, and othergroups at risk during an economic crisis.Street nurse Cathy Crowe, a member of
the Recession Relief Coalition, says she hasnever seen the kind of response from business that she has seen for this initiative.“I’ve never really been at the formation of a coalition around housing and home-lessness that happened in the boardroomsof (Toronto’s) Bay Street,” she said (TheGlobe and Mail, Dec. 19).“I think (BayStreet) is very sympathetic when a crisislike this…hits their bank accounts andmembers. But they also know that it’s evenworse for people living on the edge.”
RN teaches parents how to copewhen baby’s cryingRNAO member and advanced practicenurse Ranjan Nimkar is part of an innovative, one-of-a-kind program fornew parents at London’s St. Joseph’sHospital. She talks to new moms and dadsabout how to handle their baby’s crying.The purpose of the role is to address thedangerous – even deadly – consequencesof shaken baby syndrome (SBS).“Thereare a small, small percentage of babies thatdo die,” she told London’s CFPL-TV(Dec. 18). Sometimes the effects areimmediate, and sometimes they might not
become obvious for years. Nimkar helps to teach parents coping strategies, and pro-vides a DVD and booklet about SBS.
Nursing students get a glimpse of trauma in the emergencydepartmentIn early December, third- and fourth-yearnursing students from Brock Universitygot a dose of what it’s really like in thehigh-stress, fast-paced world of emergencynursing.“It’s a special breed of nursing:very high pressure, high stress,” saidRNAO member Elaine Burr, clinicalmanager in the emergency department atSt. Catherines General Hospital. UnderBurr’s direction, the students spent a daytraining in the nursing lab at the hospital.They cared for both real-life actors andhigh-tech mannequins, allowing them tolisten to mechanical lungs, insert cathetersand take blood pressure.According toBurr, people in a lot of pain and who arevery distressed and fearful quickly get surlyin the emergency department.“That’s thereality…but you get to make an immedi-ate impact on people’s lives.” (Niagara ThisWeek, Dec. 4)
Nursing inthenewsRNAO & RNs weigh in on . . .
Pho
to: C
ou
rtes
y M
elis
sa G
old
stei
n
8 January/February 2009
On Dec. 10, Irmajean Bajnok,Director of RNAO’s InternationalAffairs and Best Practice Guidelines(IABPG) Programs, wrote a letter tothe Toronto Sun admonishing one of itscolumnists for mocking governmentdecisions that focus on public healthrather than the economy.BustedThe Toronto Sun, Dec. 10, 2008 Re:A realistic poverty strategy,Christina Blizzard While jobs, the economy and nationalunity are crucial issues for our provincial government, the health ofOntarians is just as important.The government’s decision to ban flavouredcigarillos was essential because theyencourage young children to take upsmoking, an addiction which annuallykills more than 47,000 Canadians aged35 and over.Your columnist also suggested that asking health-careproviders to support new moms whobreastfeed was unnecessary. In fact,breast milk contains antibodies thatpromote optimal brain developmentand protect infants from a variety ofillnesses. Government initiatives aimedat preventing disease and promotinghealthy lifestyles make good financialsense.They should be applauded, notmocked.
Irmajean Bajnok,Director, RNAO’s IABPG Programs
A community forum in Toronto on Jan. 22 helped to raise awareness of the need to support the not-for-profit sector in a period of declining revenues and increased demand. The public wasasked to sign a Recession Relief Fund Declaration, endorsed by more than 200 organizations and900 individuals since it was launched on Dec. 18.

Guidebook helps residentsmake green choices Community and PrimaryHealth Care (CPHC), a non-profit health agency inBrockville, launched a booklate last year designed to educate the public on simpleways to make greener choicesat home.The 128-page publication includes tips on everything from naturalhome cleaning products, tothe issue of bottled water,how to plan a greener birthday party, andhow to make arrangements for an envi-ronmentally friendly funeral.“(We) recog-nized the need for such a resource in thecommunity as individuals were becomingincreasingly conscious of environmentalissues…” said RNAO member and CPHCExecutive Director Ruth Kitson. It Startsat Home - Optimal Environmental LifestyleResource Guide, was published with thehelp of a provincial grant. It advocatescommon sense and natural solutions.(St. Lawrence EMC, Dec. 25)
Taming Ontario’s health-care budget RNAO Immediate Past President MaryFerguson-Paré joined a panel of healthprofessionals and policy makers on TVO’sThe Agenda Dec. 9 to discuss changes tohealth-care budgets during tough eco-nomic times. Host Steve Paikin asked panelists how they might cut $1 billionfrom Ontario’s health spending.Amongthe suggestions offered up by guests: wagefreezes, service cuts, the implementation of e-health records, the subscribing ofgeneric drugs to save money, and, as a lastresort, layoffs. Ferguson-Paré stressed smartplanning as key:“It’s time for us to haveintegrated planning,” she said, specificallyrecommending rehabilitation services bebolstered to cut down on the length ofstay in hospital.“The real need is forstrong community-based rehab services.”
Letting nursepractitionerswork to their fullscope of practicewould also savemoney, she added.“Liberate nurses to do a lot more.”(TVO-TV,Toronto,Dec. 9)
Nursing shortage leads to ER closure Stratford’s Seaforth
Community Hospital announced inJanuary it is closing its ER between 8:00p.m. and 8:00 a.m. due to a nursing shortage.“We have a gap in the nursingworkforce. If we do not take concertedaction, we’ll see the nursing shortageworsen,” RNAO President Wendy Fucilesaid, adding that RNAO will continue to
press the government to fund the 9,000additional nurses it promised.“There’s noreason to delay hiring, there’s reason toaccelerate it.” (Stratford Beacon-Herald, Jan. 22)
No place for physician assistants in health systemOntario is moving ahead with a plan to addphysician assistants (PA) to the health-caresystem, but RNAO says there should be noplace for this role. Executive Director DorisGrinspun says she is especially worried thatsome PAs are being asked to perform surgi-cal procedures, which could put patients atrisk. She says Ontario should be educatingmore NPs instead, because they have moreeducation, knowledge and autonomy (CBC.ca, Jan. 23). Unlike NPs, PAs in Ontario arenot regulated and are only required to havetwo years of post secondary educationbefore entering McMaster University’s PAprogram.They must work under the supervision of a licensed physician. RN
Registered Nurse Journal 9
For complete versions of any of these stories, contact
Kitchener’s Forest Heights Long-Term Care
Centre and St. Mary’s General Hospital
partnered in November to host Champions
of Care, a conference that allowed nursing
leaders from both facilities to share details
of best practice guideline (BPG) initiatives.
RN Rahim Charania (left) is one of eight
RNAO long-term care BPG coordinators
and was on-hand at the event to raise
awareness of the new coordinator role.
(L to R) Patti Fetter (Forest Heights), Susan
Oates (St. Mary’s) and Stephanie Battler
(Forest Heights).
RNAO Executive Director Doris Grinspun
(left) and federal MP Carolyn Bennett place
roses in a vase in memory of the 14 victims
of the Montreal Massacre at l’Ecole
Polytechnique in 1989. A 15th rose was
added to the vase in memory of women
and children who have been victims of
violence over the past year. Hosted by
Toronto’s Women’s College Hospital, the
annual event takes place on Dec. 6, the
National Day of Remembrance and Action
on Violence Against Women.
OU
T & A
BOU
T

10 January/February 2009
Restraint standards exist, but arethey enough?Re: Coroner’s inquest a daunting but impor-tant task, President’s View,November/December 2008In trying to focus on the systemic issuesrelating to the use of restraints, the state-ment was made that “there is not as yetone comprehensive, system-wide standardexpectation related to the use ofrestraints.”This statement may be confus-ing as the College of Nurses of Ontariopublishes the practice standard Restraints,which outlines practice expectations fornurses. As with all practice standards, thepurpose of the document is to help nursesto understand their responsibilities andsupport safe, effective and ethical decisionsin providing client care. It is a professionalexpectation that all nurses will be familiarwith all of the practice standards to whichthey are held accountable. When RNAOwas recommending the development of abest practice guideline for restraints at theinquest, it would have been an excellentopportunity to acknowledge CNO’sRestraints practice standard and the relatedpractice expectations. CNO supportsRNAO’s suggestion and the jury’s recom-mendation that a best practice guideline
for restraints be developed to further sup-port safe nursing practices. Furthermore,CNO would like to work together withRNAO in this important initiative.
Heather CampbellDirector, Practice and Policy
DepartmentCollege of Nurses of Ontario
A note from RNAO PresidentWendy Fucile:In 2001, Ontario passed Bill 85, the PatientRestraints Minimization Act, which applies tohospitals regulated under the Public HospitalsAct and Private Hospitals Act. It does not applyin circumstances in which the Mental HealthAct governs the use of restraints on patientsor other persons in psychiatric facilities.During my testimony at the coroner’sinquest,which was investigating the death ofan individual in a psychiatric facility, I identi-fied and supported CNO’s Restraint stan-dard. However, the intent of my testimonywas to seek support for the development of aBPG – a more detailed document – thatidentifies accountability not only for nursesbut also for employers.The BPG would alsoprovide specific tools for the rollout andongoing education of staff, including staffwho are not registrants of CNO. RNAO
will work together with various stakehold-ers, including CNO, as it proceeds with thisimportant work.
RNJ helps student with classassignmentRe: Dispelling the Myths of Methadone,September/October 2008I am a 4th year nursing student at HumberCollege.This article caught my interest as Irecently had to administer methadone to aclient in my last clinical placement. I thinkit would make a great topic for my semi-nar course. Thanks for publishing suchinformative articles which help to keepme abreast of current issues in nursing. Ican’t tell you how many times I’ve usedthe RN Journal for topic suggestions andI’ve made it this far.
Janet HebertNursing student member
CLARIFICATIONThe November/December 2008 issue of
Registered Nurse Journal featured a pro-
file of RN Nancy Muller. We neglected to
mention she is a member of the Diabetes
Nursing Interest Group and a recipient of
its Smith and Nephew bursary award.
We apologize for the oversight. RN
MailbagRNAO wants to hear your comments, opinions, suggestions
It’s time to think outside the box. Last year, RNAO member Sherri Polos won the association’s first
Nursing Week Photo Contest with this image of a high-risk dad and
nurse building a therapeutic relationship based on trust. The photo is
conceptual and creative because it depicts something seemingly
unrelated to nursing. Once you look at it, and understand the meaning
behind it, you realize just how related to practice it actually is. It captures –
visually – how nurses can use unconventional techniques to foster
relationships with clients who may be difficult to reach, or untrusting.
Challenge yourself. Stretch your imagination.
Submit your creative take on nursing for our 2009 competition.
Visit www.rnao.org for more details. Or contact [email protected],
1-800-268-7199/416-599-1925, ext. 233.
Nursing Week Photo Contest 2009

Registered Nurse Journal 11
Itwas an ordinary night shift, charac-terized by the kind of silence thatmakes you want to doze off, but
charged with a sense of uneasiness that atany moment my preceptor – a neonatalintensive care (NICU) nurse – might bepaged down to labour and delivery for anemergency.As a student, this sense of beingon the verge of something big was unset-tling but exciting at the same time.At 2:00a.m., when it seemed the rest of the worldwas fast asleep, the pager started buzzing.
As we ran down several flights of stairstowards the emergency, I realized I was fullyawake and prepared. Well…that’s what Ithought anyway.We reached the resuscitationroom and found a group of awaiting health-care professionals discussing what wouldcome next. Some were anxiously peeking inon the doctors performing the C-section inthe next room, attempting to gain sight ofthe little girl who was in trouble.
Finally, a nurse brought the baby intothe room.The chatter stopped. She was notcrying. She was motionless and breathless.A scene of controlled chaos followed as theNeonatal Resuscitation Team (or NRT)pulled out their stethoscopes, suctioningtubing and other monitoring equipmentand began to save her life.
I anxiously watched for what seemedmuch longer than 10 minutes.What relief Ifelt when the little girl began to cry, andturned pinker and pinker with each passingsecond.
As I stood in the corner, away from thecrowd of health-care professionals who heldthe life of this little girl in their hands, manythoughts and questions streamed throughmy mind.Was this baby going to die in frontof my eyes? Were her parents going to havethe chance to hug, kiss and love her? Doesshe feel any pain? How would I feel if I wasthe mom in post-op,not knowing what washappening to my baby?
Ten per cent of newborns need help tobreathe post-delivery. One per cent needventilation or other special measures tohelp them survive their first hours of life.
Knowing this now, I realize my questionswere reasonable and warranted.
The NRT team looked nervous butthey were highly focused on what neededto be done and how they were going to doit. I’m almost certain they were not think-ing about death the way I was at thatinstant. Survival was their focus and theywanted to hear that baby cry.
I felt scared during this first experiencein a critical situation. I thought about thedevastated parents and also the health-careprofessionals. How would they feel if thebaby didn’t survive? How would theydeliver the message to the parents? Wouldthey reflect on this ‘close call’ if the experi-ence ended badly? Or are some health-careprofessionals immune to tragedy in theworkplace?
I feel troubled to think about those par-ents losing out on the opportunity to adaptto their child’s cues. No chance to form theinitial bonds between mother, father andbaby.To this day, I have witnessed my ownparents shedding tears when they see mehurt.Though my family provides me withstrength, they also break down with mewhen they see me sad. If parents are capableof feeling hurt for their living children, Icannot even begin to understand the hurtthat parents feel over the loss of their child.
My sister and I have brought joy toour parents’ lives and, fortunately,the baby that was resuscitated thatday will also bring joy to her fami-ly thanks to the NRT team andtheir efficient and orderly action.
With an interest in pediatrics,especially the NICU, I reflect onthis experience and wonder if Imay one day become desensitizedand ultimately lose the feelings Ihave today. There is a life behindevery breathless body. There is afamily. There are awaiting parentsand grandparents. And there maybe awaiting siblings.There is a life-time of ups and downs, wrongs andrights, and hopes and dreams.
No matter how many times as health-care professionals we find ourselves in criti-cal situations and wonder if our patients willsurvive, I only hope we always realize thatwe’re not just caring for a body, but a life.Asmy placement continues, I hope to learnmore about the RN role on the NRT team.I think it was important that I was abystander in the resuscitation room that daybecause the experience allowed me to standaway from the incident and reflect on myown life and how important and fragile it is.
Thanks to this experience, I’ve decidedto complete the Neonatal ResuscitationProgram (NRP) to obtain my certification.I want to be of assistance in neonatal resus-citation and the training will allow me to bea more confident and skilled professional.
Albert Einstein once said: “Only a lifelived for others is a life worth living.”
As a health-care professional, helpingpatients through tough times in their livesmakes me feel useful and energized. I feel honoured knowing I’ve monitoredneonates in the NICU. RN
OLIVIA GERARDI HAS HER BACHELOR OF
SCIENCE DEGREE AND IS CURRENTLY IN
HER 4TH YEAR OF NURSING IN THE
ACCELERATED STREAM AT MCMASTER
UNIVERSITY IN HAMILTON.
Life and death in the NICU A late-night emergency in the neonatal intensive care unit gives soon-to-be RN a glimpse of her own mortality. BY OLIVIA GERARDI
Illu
stra
tio
n: T
race
y W
alke
r

12 January/February 2009
RNs speak out against ad campaigns that stereotype nurses to sell everythingfrom vodka to gum. by Jill Scarrow
tonaughty nurse imageN

TORONTO EMERGENCY RN LAURIE SPOONER WAS TAKING PUBLIC
transit to work in July of 2006 when a five-foot poster hanging on the opposite side of the subway tracks
grabbed her attention. Under a slogan that read‘Water made naughty,’ a young, slender, blonde
woman was floating in a pool of water andpulling a long latex glove over her hand as
she gazed seductively at transit riders.Themost offensive thing about the ad,
Spooner says, was the outfit.The long,spiked heels, thigh-high stockings,garter belt and mini skirt weren’twhat Spooner or any of herHospital for Sick Children nursingcolleagues would be wearing towork that day, but the messagescreaming from this woman’swhite cap was clear: she was anurse.The ad ignited the samefeelings of anger, disgust andfrustration in Spooner thathave surfaced every other time she’s seen her professiondemeaned in the media.
“When I see images of sexy,naughty nurses, I really believethey contribute to a general mis-
understanding of what we do,” shesays.Turning nurses into sex objects
is offensive enough, she adds, butthat’s not the worst part. “Over the
years it has become clearer and clearerthat the shortages and the lack of funding
– not just for staffing, but for educationand research – it’s all a result of no one hav-
ing a clear picture of what nurses are doing.”Enraged, Spooner wrote to Vincor
International, the company behind the ad, and tothe Toronto Transit Commission to complain that not
only was it offensive, but it did little to reflect nursing as a
Registered Nurse Journal 13
Illu
stra
tio
n: M
auri
ce V
elle
koo
p

life-saving profession. She also contactedRNAO, which partnered with theBaltimore-based Center for NursingAdvocacy – an organization that worked toimprove nurses’ media image – to solicitapologies and promises from theAmerican-owned beverage maker towithdraw the campaign by month’s end.
Spooner is just one of thousands ofRNAO members who have spoken outagainst advertising campaigns that depictnurses as sex objects. The year before herangry letter to Vincor, hundreds of Spooner’sequally outraged colleagues confrontedVirgin Mobile after company owner RichardBranson launched a new cellphone plan byleaping from buildings to rescue womendressed as nurses who were chained to cars ata busy downtown Toronto intersection.Morerecently, members vocally objected to aDentyne gum commercial that showed ayoung nurse crawling into bed with a patient,and to an online Neilson Dairy ad thatdressed women up as ‘nurses’ in short skirtsand caps and invited consumers to come andmeet the models at promotional events.
RN Sandy Summers is the former exec-utive director of the Center for NursingAdvocacy and now leads The Truth AboutNursing, an organization that promotes pos-itive images of the profession. She is also co-author of Saving lives: why the media’s portray-al of nursing puts us all at risk, released inFebruary 2009. Summers has lobbied exten-sively to protect nursing’s image in the U.S.,and has helped RNAO in its actions againstadvertisers. She says marketers aren’t theonly ones guilty of running the professionthrough the mud.Hollywood writers, direc-tors and producers do it too. In her role, shehas lobbied against shows like Grey’sAnatomy and ER for their portrayal of nurs-es as either love interests, or simply non-existent. Physician characters play doctor,nurse, social worker and physiotherapist allat once, she says. But thanks, in part, to theCenter’s work with writers on ER, theimage of nurses on that show has started toimprove.Writers recently introduced a char-acter studying to be a nurse anaesthetist.But, prior to that, Summers says, the onlyway ER nurses could prove how smart theywere was by applying to medical school.
Summers believes other professions maynot grapple with the same kind of negativemedia persona because of the implicitrespect society bestows on them.Lawyers, forexample, don’t score highly in polls about
public trust, but the amount of money theycan earn and the perceived rigours of lawschool send the message that it’s a career forsmart, talented people. Physicians are also agroup that seem to garner that same level ofrespect, although Summers says that’s comewith a little gentle nudging of television pro-ducers and writers by the American MedicalAssociation (AMA). In the 1950s and 60s,AMA was vocal about the need to portraydoctors as respectable professionals on TV.And because of strict ideas about genderroles more than five decades ago, nurses wereonce leading ladies in medical dramas. Butsince it’s now acceptable for women to bephysicians – in reality and fiction – leadingfemale characters are now doctors, and nurs-ing is often just left out altogether.
In Summers’ view, every nurse shouldspeak out against the often offensive andinaccurate portrayal of the profession on television – and during commercial breaks –because unless nurses get respect in popularculture, the public won’t get a sense of howimportant the profession really is. She alsobelieves that in the U.S., that lack of aware-ness about the role has led to political deci-
sion making that leaves fewer nurses work-ing at the bedside, or available to care forfamilies in communities.
“Until we get the world to see nursingas a valuable career in which smart menand women save lives and improvepatient outcomes, we’re never going toget the funding we need to resolve theglobal nursing shortage,” Summers says.“I really think the most important pub-lic health crisis facing the world is the
global nursing shortage.”Battling back against today’s unsavoury
nursing stereotypes requires a closer look atsome centuries-old ideas about nursing,according to Sioban Nelson, Dean of theLawrence S. Bloomberg Faculty of Nursingat the University of Toronto.Nelson has writ-ten extensively about the profession’s historyand traces the image of the naughty nurse asfar back as the nursing nuns of 17th centuryEurope. Their work took them beyond theboundaries of contemporary, polite societyand into close contact not only with diseaseand death,but also with men.Nurses protect-ed themselves from the perceived shame bytaking religious vows, wearing veils andhabits, and cloaking themselves in the notionthat they were following a calling from God.
When Florence Nightingale broughtnursing into the secular world, she under-stood that if it was going to be respectable, ithad to be desexualized. She weaved religiousimagery into the profession by clothing hernurses in conservative dress, ensuring eachread the Bible and prayed. Still, Nelson saysthat illicit association between nurses andmale bodies means that, in cultural memory,nursing sits in a balance between “nun andwhore.” And getting beyond 400-year-oldideas doesn’t happen quickly. Even in the21st century, Nelson says, the notion ofequality between the sexes may be foreignto many people’s grandmothers.
“It’s actually only in the 20th century thatwomen have had agency in the world, thatthey can go on public transport by them-selves, go to work, and be colleagues withmen,” Nelson says.“These things seem obvi-ous because they’re a couple of generationsold, but stigmas last a lot longer than genera-tions.They’re imprinted on our culture.”
Still, journalist and author SuzanneGordon says that doesn’t mean nurses shouldjust accept the damage these ideas can do.
Gordon has written eight books onnursing, and this February led a seminar atRNAO to encourage members to talk
14 January/February 2009
“Until we get the
world to see nursing as a
valuable career in which
smart men and women save
lives and improve patient
outcomes, we’re never going
to get the funding we
need to resolve the global
nursing shortage.”

about their knowledge and work, and why itmakes a difference to patient care. Shebelieves if more nurses tell patients whythey’re taking certain medications, or whyrehab exercises they’re doing will help themrecover, people will get the message nursesaren’t just nice, they’re smart.
“I really don’t think the public needs tohave one more person tell them nurses arecaring. People know that.They need to havepeople tell them nurses are smart,” she says.
Ashwin Joshi, Director of the MBA pro-gram at York University’s Schulich School ofBusiness, agrees that the profession shouldstand up and object to the way RNs are tart-ed-up in advertisements. He says thesestereotypes may be acceptable today in muchthe same way that it was once consideredacceptable to depict Asians with exaggerated,stereotypical accents or African Americans aspoor criminals.Thanks to vocal opposition,those images now cause viewers to cringe.
“There’s a bottom-up resistance to it,which is nurses’ organizations saying ‘cut thecrap,’ but there also needs to be a change inthe cultural climate as a whole.”
Joshi says companies often use sex, fear,or humour to convey the message theywant consumers to remember about theirproducts. Sex does sell, but it can alsobackfire. In September 2007, themakers of Dentyne Ice gumlaunched a television commercialfeaturing a young male hospitalpatient putting a piece of guminto his mouth before pressingthe call bell. Unable to resist hisfresh breath, his attractive femalenurse slides onto his bed andleans in for a kiss before drawingthe privacy curtain. Obviouslyhoping for similar treatment, theolder man in the next bed grabs thegum. An older, grey-haired nurse appearswith a flirtatious grin, causing a look ofexasperation to flit across the man’s face.Joshi says Dentyne’s commercial is attempt-ing to appeal to teenaged males, but it maynot have been edgy enough to tap into thissavvy demographic.Young consumers knowchewing gum won’t guarantee successfullove lives.
In response to the campaign, RNAOfiled a complaint against Cadbury Adams(the makers of Dentyne) with AdvertisingStandards Canada, the marketing industry’sself-regulating body. Thanks to email com-plaints from more than 1,300 RNAO mem-
Registered Nurse Journal 15
August 2004Skechers shoes uses images of singer Christina Aguilera dressed as a ‘naughty nurse’ to promote its products. Then RNAO President JoanLesmond writes a letter to the company…“By promoting nurses as sex objects,Skechers not only performed a disservice to the profession, but also to the general public who need anddeserve high-quality nursing care …RNAO has actively promoted nursing as a challenging career choice … our efforts to promote nursing anddebunk the sexist, negative stereotypes perpetuated by ill-conceived ad campaigns are of the utmost importance if we are to stem the coming shortage.”
March 2005Sir Richard Branson, founder of VirginMobile, launches the company’s cellphone service in Canada by slidingdown a cable from the top of a building at a busy Toronto intersectionand rescuing three ‘nurses’ chained tocars. Hundreds of RNAO membersexpress their outrage…
“I have helped new moms learn to care for their babies. I have cared forpeople after life-altering illness and surgery. I have comforted patientswho are dying, and cared for their bodies after they die. If you questionour professionalism, I challenge you to spend a day in any of our well-worn shoes.”
Leslie Inglis, RN, Kingston
August 2005Motts Clamato launches a campaign in which a woman dressed as a ‘nurse’rings the doorbell of a young man who,presumably, invites her in for some sexual activity…“I am so tired of this kind of thing. I think we’re doing our job to get themessage across, but others just don’tget it … your portrayal of nurses servesonly to perpetrate an insulting imageof a dedicated professional group.”
Elizabeth Edwards, RN, Belleville
September 2007RNAO launches a campaign againstDentyne Ice gum for a commercial featuring nurses climbing into bed with patients…“There is nothing “sexy” about this career. It is a combination of knowledge, clinical judgment, and skill.To continue being portrayed as sexually available to patients increasesthe potential for assault on the job.And yes, we do get assaulted andsometimes have to deal with inappropriate patients because of thisongoing fight to inform people ofexactly what it is we do for a living.”
Lorraine Dunn, RN, Toronto
RNAO executive and general members are vocal about why advertisers need to stop using naughty nurse images in their campaigns…
Image is everything
Pho
to: C
ou
rtes
y H
ans
Der
yk/T
oro
nto
Sta
r

bers, Cadbury pulled the ad off the air inOctober of that same year.
Jennifer Bennett, a public health nurse inGuelph, says that when she heard Cadburycanned the commercial, she felt empowered.Bennett was one of the thousands whoresponded to RNAO’s action alert. It gaveher a way to react to a 30-second commercialthat made her angry for weeks she says. It alsoreminded her of some of the negative experi-ences she’s had in her career. “Working in ahospital, I have had to cope with harassmentand inappropriate behaviour,” she wrote. “(I)find it disgusting that you would advertiseyour product in this manner.”
Bennett was also angry because the adsent the message that nurses enjoy beingseduced by patients.A mother of two youngboys, she worried that she would one dayhave to reassure them she doesn’t get intobed with strange men at work.
For Emmet O’Reilly, a primary carenurse in Toronto, portraying nurses as young,sexy women leads to a larger challenge forthe profession:convincing more men to join.
“These sexualized stereotypes are just
going to continue to perpetuate that it’s awoman’s only role,”he says, adding that’s toobad, because it should be just as acceptableand normal for a man to be a nurse as it isfor a woman to be a physician.
Last summer, O’Reilly responded to atroubling ad campaign for flavoured milkproducts produced by Neilson Dairy. Theonline promotion bothered him because itattempted to associate a healthy lifestyle withan ill portrayal of his profession. Naughtynurse-themed images – complete with shortskirts and high heels – appeared on the com-pany’s website, which encouraged people tocome out and meet the ‘nurses’ touring sum-mer hot spots like Muskoka.
In July, RNAO called on Neilson toremove the ads. The company apologizedfor any offence taken, but defended thecampaign as a humourous, healthy andwholesome pitch to a hard-to-reach youth-ful demographic.An action alert was distrib-uted among members, asking them toappeal directly to Neilson in emails. OnAug.8 – after receiving 1,000 messages fromRNs like O’Reilly – the company with-
drew the images from its website, promisedto stop using them at public events, andcommitted to not using nurses in future ads.
Paula Dawson,care coordinator at a men-tal health outpatient clinic for adults andadolescents at St. Joseph’s Healthcare inHamilton, says it was satisfying to be one ofthe nurses who got Neilson’s attention. Shewasn’t just offended by the campaign images;Neilson’s response also bothered her.Dawson works with teenagers and says she’snot sure the sexy-nurse campaigns reallyinfluence what they buy.“My work is in anEarly Intervention Program for Psychosis... Iam highly aware that it is important to relateto youth on terms that have meaning tothem,” Dawson wrote to the milk company.But she worries that such campaigns can bedetrimental to the relationship she and herstaff rely on having with their patients. Shesays young people need to trust health-careproviders enough to talk about the symp-toms of their illnesses,or any side effects fromthe drugs they might be taking.
While Dawson is confident her patientscan differentiate between the smart health-care providers in their real lives and the racypictures in the media, she hopes the rest ofthe public can too. Belonging to RNAO,she says, is a good first step toward makingsure everyone gets the message that nursesaren’t sex objects.Through action alerts andother lobbying activities, RNs can collec-tively talk about how rich and diverse theprofession actually is. “If ads are offensiveand we don’t say so, advertisers won’t changetheir behaviour,” she says.
Spooner couldn’t agree more. She stillemails corporations that tamper with nurs-ing’s image, and she doesn’t shy away fromwriting letters to the editor in response tonews articles that glorify how caring nursesare, but omit that they’re also smart andknowledgeable. Spooner wants to make sureeveryone understands what the professioncan offer, especially potential recruits.
“If you’re a 16-year-old … you mightwant to do something exciting that is goingto challenge you, let you travel, go on to geta PhD or do research,” she says.“All of that isnursing,but people don’t know that … if wespeak out one little bit at a time, we canslowly increase knowledge of what we do.That will increase the respect we get, andthat’s going to improve our numbers andmake us a better profession.” RN
JILL SCARROW IS STAFF WRITER AT RNAO.
16 January/February 2009
October 2008RNAO urges members to say ‘No Deal’when the popular television gameshow Deal or No Deal dresses its models up in naughty nurse outfits because a contestant is a nurse.“Spend an hour in a trauma unit beside a real nurse…spend an hour in a burnunit…side-by-side with a real nurse…comfort and care for a dying child…provide dignity to an incontinentelder...talk to your viewing audienceabout what you have seen…We will notbe in short skirts. We will not be inrevealing tops. We may be in scrubsstained with blood. We may be taking a quiet moment to clear our heads ofthe sounds a patient makes when theymust endure a painful burn dressing. We may be holding the hand of a motherwho is losing her child in the traumaroom. We are amazing, intelligent, compassionate women and men. Yourchoice to portray us as anything less is adiscredit to our work and to your show.”
Sue Chapman, RN, Palgrave
July 2008Neilson Dairy promotes a newflavoured milk drink by featuring‘naughty nurses’ in online ads and atpublic events. More than 1,000 members write letters to the company…“Would you depict women doctors in this way? If not, why not? …Would yourdaughter or the other young womenyou are targeting apply to university tostudy nursing if that is the image ofnursing as depicted by your company?”
Anne Marie Webster, RN, Waterloo
Image is everything

Registered Nurse Journal 17
If you ask Carolyn Acker whatdespair looks like, she’ll tell youabout the shame that forces kids to
get off the streetcar at a different stop soother people don’t know they have the‘wrong’ address. She’ll tell you aboutmothers who forgo meals so their childrencan eat, street gangs, and a flourishing drugtrade. But perhaps most frustrating forAcker is the sound of children sayingthey’ll never be anything but poor.
“It upsets me to hear that. It makes meangry,” she says. “We’ve got to do some-thing about it.These kids are no differentfrom you and me.”
The kids she refers to are living inRegent Park, a 28-hectare Toronto neigh-bourhood home to one of the oldest pub-lic housing developments in Canada.Nearly 80 per cent of the residents are vis-ible minorities, more than half are immi-grants, and the average household incomeis just $15,000. It’s also a postal codewhere, in 2001, more than half theteenagers didn’t finish high school.
Eight years ago, Acker worked at theRegent Park Community Health Centre asexecutive director. She saw first-hand howviolence, homelessness and poverty grippedthe community. She and fellow CHC staffand board members knew that if theywanted to boost the overall health of thoseliving in Regent Park, they’d have toaddress some of the social factors plaguingthe community. The solution was to helpchildren grow up to become the next gen-eration of community leaders and profes-sionals.And the first step to that end was totackle the staggering school drop-out rate.
Local parents, Acker explains, wantedtheir kids to get a good education, butthey didn’t speak English and didn’t knowhow the Canadian system worked. Thenearest high school was a bus ride away,but many families couldn’t afford the fare.And for those students lucky enough tomake it through high school, the cost toapply for college or university made post-secondary education impossible.
In 2001, Pathways to Education was bornto tackle these challenges. More than 90per cent of all the high-school-aged kidswho live in Regent Park are now part ofthe program, which offers financial, socialand academic supports from the first day ofGrade 9 until graduation. Young studentslearn teamwork skills when they gettogether to bake cookies, and older stu-dents pair up with mentors to talk aboutoptions that await them after graduation.
“It’s all of the supports taken together asa whole that are making the difference,”Acker explains. “Maybe Grade 9 boysaren’t concerned about the scholarship.Maybe for them the group mentoring andthe tutoring and the bus ticket are moreimportant.But by the time they’re in Grade11, that scholarship is extremely important…otherwise, they have no hope.”
Acker is proud that Pathways’ compre-hensive formula is working. The drop outrate in Regent Park is now just 10 per cent,and in 2008 the first 12 Pathways studentsgraduated from post-secondary school.That’s a stat that brings tears to her eyes.“Seeing these young kids, how they’re blos-
soming and doing so well, the results areamazing,” she gushes.“I’m a nurse. I want tomake a difference…I feel very fortunatethat I’ve been able to do this kind of work.”
In 2006,Acker became the chief exec-utive officer of Pathways to EducationCanada. She now oversees the expansionof the program into other Toronto neigh-bourhoods, as well as Ottawa, Kitchenerand Montreal. She says it’s a role that helpsher live out her childhood dream to be ahome-care nurse in a different way.
After graduating from St. Michael’sHospital school of nursing and working inthe hopital’s intensive care unit in the 1970s,Acker spent 16 years as a community nursefor Saint Elizabeth Health Care. She earnedher bachelor’s and master’s degrees in man-agement studies because she always knewshe wanted to be in a formal managementrole. Although her academic studies werecomplete in 1991,Acker knew her on-the-job education was far from over.
She joined Regent Park CommunityHealth Centre in 1992 and quickly learnedfrom her nursing colleagues that whenworking with marginalized populations,health care has to be brought to peoplewhere they live – whether that’s an apart-ment block or a homeless shelter.Today, herwork gives her a chance to reach directlyinto the lives of families by bringing thePathways program directly to some of thecountry’s poorest neighbourhoods.
As CEO, she is also a full-time fundrais-er for the program, and helps potentialdonors and governments understand thatwhen it comes to improving the health oflow-income people, clinical services areonly part of the puzzle. The real solutionlies in the layers of social, political and eco-nomic forces that shape their lives.
“I’m still working as a nurse, only nowI’m working on the determinants ofhealth and I’m focused on the most pow-erful one,” she says, adding vehementlythat “education can change lives.” RN
JILL SCARROW IS STAFF WRITER AT RNAO
Easing poverty through education RN heads up successful program that builds on a fundamental determinant of health: a child’s time in school. BY JILL SCARROW
NAME: Carolyn AckerOCCUPATION: Chief Executive Officer,Pathways to Education CanadaHOME TOWN: Thorold, Ontario
18 January/February 2009
Pho
to: C
ou
rtes
y R
ick
Mad
on
ik/T
oro
nto
Sta
r
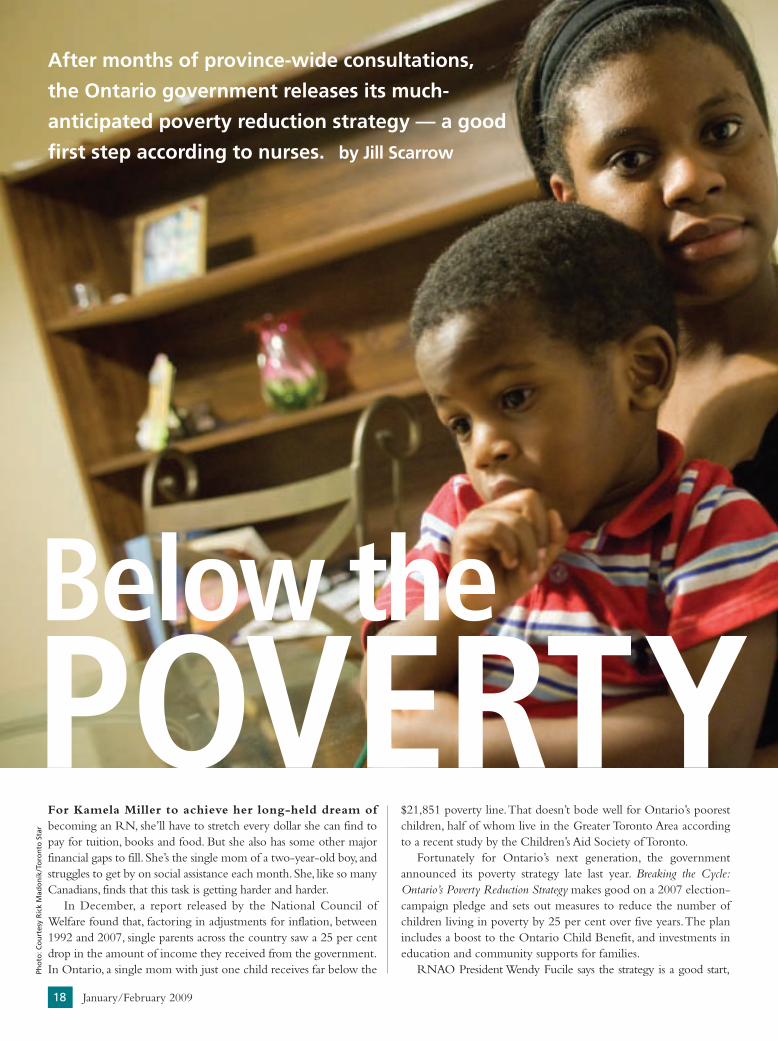
For Kamela Miller to achieve her long-held dream ofbecoming an RN, she’ll have to stretch every dollar she can find topay for tuition, books and food. But she also has some other majorfinancial gaps to fill. She’s the single mom of a two-year-old boy, andstruggles to get by on social assistance each month. She, like so manyCanadians, finds that this task is getting harder and harder.
In December, a report released by the National Council ofWelfare found that, factoring in adjustments for inflation, between1992 and 2007, single parents across the country saw a 25 per centdrop in the amount of income they received from the government.In Ontario, a single mom with just one child receives far below the
$21,851 poverty line.That doesn’t bode well for Ontario’s poorestchildren, half of whom live in the Greater Toronto Area accordingto a recent study by the Children’s Aid Society of Toronto.
Fortunately for Ontario’s next generation, the governmentannounced its poverty strategy late last year. Breaking the Cycle:Ontario’s Poverty Reduction Strategy makes good on a 2007 election-campaign pledge and sets out measures to reduce the number ofchildren living in poverty by 25 per cent over five years.The planincludes a boost to the Ontario Child Benefit, and investments ineducation and community supports for families.
RNAO President Wendy Fucile says the strategy is a good start,
POVERTY LINEBelow the
After months of province-wide consultations,
the Ontario government releases its much-
anticipated poverty reduction strategy — a good
first step according to nurses. by Jill Scarrow

Registered Nurse Journal 19
especially since it sets firm targets. It’s also important that the govern-ment has promised to introduce legislation this spring that willenshrine the plan in law.Fucile is concerned,however, that there is nomention of adults without children who also need help to lift themout of poverty. She says RNAO will continue to advocate for every-one living in poverty, regardless of age, and to ensure the upcomingprovincial budget allocates the dollars to programs outlined in thestrategy so it can start to make a real difference for people.
“Nurses don’t exist in a vacuum, isolated from the social andpolitical forces around us,” Fucile says. “We are all too aware thatincome has a tremendous affect on people’s health.”
ONDec. 4, the Ontario government released
details of its long-awaited poverty reduc-
tion strategy. With a goal to see 25 per cent fewer
children living in low-income families over the next
five years, the plan is expected to cost $1.4 billion
to implement. The provincial government says it
will call on Ottawa to help achieve its ambitious
goal. Deb Matthews, Minister of Children and
Youth Services, led the cabinet committee that
developed the strategy and told Ontarians that
the government plans to measure its progress
and report back on an annual basis.
NEW MEASURES TO REDUCE POVERTY INCLUDE:
• Increases to the Ontario Child Benefit so that children in low-
income families receive up to $1,310 annually beginning in
2012. Currently, families receive up to $600 annually.
• Investments in education, literacy, and school programs, including
those that bring together community partners to address the
needs of disadvantaged communities. The government also plans
to implement full-day learning for four- and five-year-olds.
• Double the funding – up to $22 million annually – for the
Youth Opportunities Strategy, created in 2006 to give lower-
income youth the chance to learn new skills.
• An additional $19 million annually to help those under the care
of Children’s Aid Societies make the transition from childhood
to adulthood.
• Targeted funds for low-income youth struggling with mental
illness or addictions.
• Development of culturally sensitive programs for Aboriginal
children.
• Financial support for a new Community Opportunities Fund
($5 million annually) to encourage businesses, governments,
volunteers, residents and community agencies to work together
to revitalize neighbourhoods.
• An additional $10 million to hire employment standards offi-
cers who will improve compliance with the Employment
Standards Act to ensure workers receive wages and benefits
owed to them.
• Stabilized funding of $5 million per year for the Provincial Rent
Bank Program, which provides resources to families at risk of
being evicted.
• Promises to examine existing social programs to assess their
effectiveness. The government will review some of the barriers
facing those on social assistance. For example, it will eliminate
penalties on social assistance earnings for people who are
attending post-secondary school. It will also provide more child
care benefits to help parents stay in the workforce.
• The establishment of a Social Policy Institute to evaluate policy
and identify best practices in other jurisdictions. The govern-
ment will encourage the development of businesses that use
the skills of low-income Ontarians, and study the possibility of
creating a Social Investment Exchange. RN
What’s new for Ontario?
Y LINE

20 January/February 2009
Last year, RNAO memberstook that message to publicmeetings on poverty reduc-tion, organized by anti-povertycommunity groups and politi-cians across the province.
Janet Cormier, co-chair ofRNAO’s Hamilton chapter,attended a meeting in her com-munity. A clinical manager oftwo surgical units at HamiltonHealth Sciences, Cormier hasseen the impact of povertythroughout her career. Sheremembers homeless individu-als seeking refuge from the coldinside the emergency department when she worked as a nurse there 15years ago. One man in particular will always stand out in her memory.He couldn’t speak clearly, and Cormier remembers the difficulty hercolleague was having trying to understand him.When Cormier walkedby with some cookies and juice she was carrying to another patient,theman suddenly grabbed them out of her hands and began feasting onthem. It was then she realized how hungry he must have been.
At the meeting last May, Cormier heard many all-too-familiarstories about how health concerns have kept people trapped in thecycle of poverty.That includes, for example, a woman who told thecrowd about how her struggles with epilepsy kept her from work-ing. She desperately wanted her daughter to go to university butwas having trouble coming up with the funds to pay for it.
“When you look at people in a poverty situation, they often
have some kind of illness that prevents them from working,”Cormier explains.“Why are we punishing these people?”
Illness isn’t always the reason people have trouble getting ahead.Parents like Miller need support just to afford the nutritious foodand shelter that keep them healthy. She had her son just after fin-ishing high school and couldn’t find a job. Now, as she takes cours-es to upgrade her high school marks so she can apply to universi-ty, Miller’s set a strict budget that’s vital if she’s to have enoughmoney to survive. A welfare cheque for $1,121 is deposited intoher bank account each month. Once the rent is paid, there’s $222left for everything else.That means the 20-year-old must also relyon the $430 in government child benefits she receives to buy gro-ceries, clothes and diapers, and to pay the phone bill.
“It’s not supposed to be for me…it’s supposed to be about mychild,” she acknowledges of the baby bonus cheques. “But that’swhat I end up living off of.”
Miller also gets some help from a neighbourhood program thatoffers young, single moms the chance to take courses that will helpprepare them for post-secondary education and a career.The pro-gram offers breakfast and lunch every day, vouchers for local gro-cery stores, and a monthly $100 transportation allowance, whichMiller puts towards food rather than bus tickets.
“I want to finish university,” she says of her resolve to create abetter life.“My son really drives my lifestyle and my goals.”
Miller acknowledges that her determination isn’t alwaysenough to get by. She’s hopeful the government’s plan will make adifference, but she also worries about the possibility that it willlanguish on a dusty shelf unless politicians continue to hear frompeople like her who can describe what it’s like to count pennies.
“If we all come together and say,‘Listen, (poverty) is a problem,
Addressing the needs of Ontario chil-
dren may be a good first step toward
reducing poverty across the province, but
those who work with the elderly say that
population’s needs cannot be forgotten.
During a November think tank organ-
ized by the Elder Health Coalition, which
RNAO helped found in 1998, advocates
for seniors pressed government officials
about the importance of addressing the
needs of all Ontarians who struggle in
poverty, not only children.
“Elderly, single, poor women spend
most of their income on rent,” said coali-
tion member Bea Levis, adding that’s why
affordable housing is vital for all low-
income individuals, regardless of age.
Coalition co-chairs Gerda Kaegi and
Doris Grinspun formally reiterated the
group’s call for affordable housing, plus
other support measures, in a letter deliv-
ered to Premier Dalton McGuinty and provincial ministers just two
days after the think tank. All Ontarians should be able to live in
health and dignity, the letter states, espe-
cially the 57,000 seniors who are poor.
That same day, more than 100 RNAO
members echoed this call when they
responded to an association action alert
urging government to address the needs
of seniors who require affordable hous-
ing and a guaranteed, liveable income.
“Each day I work with members of the
(seniors) community, including veterans
of the Second World War, to help them
improve their function and quality of
life,” wrote Loretta McCormick, a nurse
practitioner at Cambridge Memorial
Hospital. “I see the financial struggles
that these people are faced with (to
afford) nutrient-rich foods, sub-prime
housing, and paying for parking for
appointments. Ontarians want to partner
with health-care professionals; they know
the benefits of good nutrition, affordable
housing and supportive communities. I feel confident that Ontario
can change this situation.” RN
Elder care advocates say seniors in poverty need attention too
A RECESSION IS
NO REASON FOR
THE PROVINCE
TO CLAIM IT CAN’T
AFFORD TO
ADDRESS POVERTY.
IT’S EXACTLY THE
TIME TO ACT.

we’re not tolerating it’…I believe a change can come.”Over the last several years, RNAO has done plenty of work at
both the national and provincial levels to add nurses’ voices to thatcall. In August, members responded to an action alert calling onOttawa to introduce a national poverty plan, and during last fall’sfederal election, Executive Director Doris Grinspun participated ina town hall meeting on poverty and health care at RyersonUniversity.The association has been vocal about the need to pushahead the province’s povertyreduction plans and is part ofthe 25 in 5 Network for PovertyReduction. Creating a HealthierSociety, the document that laidout Ontario nurses’ expecta-tions of political parties duringthe last provincial election,called for basic income supports for individuals,including: immediate increasesto minimum wage and socialassistance rates that reflect theactual cost of living; and a sub-stantive increase in affordablehousing. RNAO provided aformal submission to the cabi-net committee that developedthe new strategy, pointing outthe irrefutable link betweeneconomic status and health.And, throughout 2008, nursesparticipated in RNAO’s advo-cacy work to urge the premierto take decisive action despitethe economic downturn.
Grinspun says a recession isno reason for the province toclaim it can’t afford to addresspoverty. Rather, it’s exactly thetime to act. “We welcome the$2 billion allocated for socialhousing in the recent federalbudget, but the requirement tosecure matching funds fromprovinces and already cash-strapped municipalities willlimit the benefit for those whourgently need a roof over their heads,” she explains. “RNAO alsodecries that the budget left thousands of unemployed without accessto Employment Insurance, while providing tax cuts that don’t bene-fit those in greatest need.”
RNAO will be watching the upcoming provincial budgetclosely, and will urge Premier McGuinty to put much-needed dol-lars into Ontario’s poverty reduction strategy.“The Premier has theopportunity to show real leadership on this issue,” Grinspun says.“He can define his time in office by taking bold action to make adifference for thousands of Ontarians.”
Carine Gallagher agrees. Last July, the nursing professor inThunder Bay attended a town hall meeting on poverty, organized
by the Ontario NDP. She listened as single parents, the disabledand elderly shared their stories and asked the government toaddress the hardships they face every day. Now that the economy issliding, and mills in the area’s pulp and paper industry are laying offstaff or closing, Gallagher wonders how many people she met atthat meeting are finding it even harder to afford the basics, despiteany government promises.
“It’s very sad that we have poverty in this country.The meetingpointed out so many things that need to be addressed in the socialsystem,” Gallagher says. RN
JILL SCARROW IS STAFF WRITER AT RNAO.
Registered Nurse Journal 21
Two new documentaries are exploring the struggles of several
Canadian families coping with poverty, and the solutions
they need to find adequate housing and food. RNAO has provid-
ed expertise and financial support to both.
Home Safe, produced by Sky Works Charitable Foundation,
follows children and families in Calgary, Sault Ste. Marie,
Hamilton, and Toronto as they cope with the hardships and
stigma associated with homelessness. RNAO member Cathy
Crowe is lending her years of experience as a street nurse to the
project as its executive producer. While the films based in
Ontario cities are still in progress, the first instalment, which
examines the affordable housing crisis in Calgary, was released
last fall. For more information about the project, visit www.
skyworksfoundation.org.
Poor No More, hosted by actress and comedienne Mary
Walsh, introduces viewers to Canadians who have lost their jobs
because of factory closings, or who have worked years for
companies that offer little pay and no benefits. The film also
examines how other countries such as Ireland and Sweden have
taken strides to address poverty and have improved the lives of
people living within their borders. For more information, visit
www.poornomore.ca. RN
ABOVE: Rowan and Delilah, two of the kids featured in the Sky
Works documentary, Home Safe Calgary.
Documentary filmmakers tell thestories of families facing poverty
THE PREMIER HAS
THE OPPORTUNITY
TO SHOW REAL
LEADERSHIP ON
THIS ISSUE. HE
CAN DEFINE HIS
TIME IN OFFICE BY
TAKING BOLD
ACTION TO MAKE A
DIFFERENCE
FOR ONTARIANS.
22 January/February 2009
At 57 years of age, Carol is a frail, thinwidow. Her husband passed away a year agoand she was the victim of a burglary whilestill grieving the loss. Tearful and at timesdistant, she tells her nurse about how shecan only sleep for short periods beforebeing startled awake by sounds she imaginesare those of an intruder. She hasn’t seen herclosest friend since her husband’s deathbecause he used to drive her for visits, butshe’s too frightened to go on her own now.“It’s no fun to cook for one,” she says as theRN takes notes.“I’m so tired of it all.”
Carol’s nurse, like many of her col-leagues, knows there are any number of sit-uations which may lead an individual totake his or her own life. Carol finds herselfin at least two of them: she’s older and she’sdepressed. Economic hardship, professionalstress, or feelings of being weighed down bypersonal responsibility can also prompt vul-nerable people to believe life is too over-whelming, and death an escape.
Almost 4,000 Canadians die as a result ofsuicide each year. With the publication inJanuary of RNAO’s best practice guideline(BPG), Assessment and Care of Adults at Riskfor Suicidal Ideation and Behaviour, nurses arenow in a better position to help decreasethis troubling statistic.The guideline focuseson ‘adults at risk,’ which includes anyoneover the age of 17. Their motivations maybe physical, psychological, spiritual, social,economic, political, cultural or environmen-tal. The BPG provides comprehensive evi-dence and a roadmap to more effectivelyidentify who is at risk, and to provide themwith the help they need.
The first stumbling block, according toElaine Santa Mina, is overcoming the stigmaassociated with suicide. “There are groups(of people) who come forward and try togive this a voice,” the RN and chair of theBPG panel says.“But it’s still a bit of a cry inthe wilderness. The overwhelming socialperspective is still quite laden with stigma.”
With the release of the guideline, nursesare being asked to recognize – in themselvesand others – pre-existing social attitudesabout people who consider suicide, and toget beyond them by asking the hard ques-tions about whether or not someone isthinking about taking their life.
“It’s very difficult for people to asksomebody ‘Are you thinking about killingyourself?’ because there is a myth out therethat by asking that question, you’ve plantedthe idea in their mind,”explains Santa Mina,
adding this myth is one of many dispelled bythe guideline. An associate professor ofnursing at Toronto’s Ryerson University,Santa Mina’s PhD dissertation in 2005focused on self harm and suicide, particular-ly the intentions behind such behaviour.
She says another stumbling block to car-ing for these vulnerable people is nurses’ ten-dency to downplay negative comments andignore the subtle signs they see when talkingto patients. According to Santa Mina, themost important thing for RNs to rememberin their practice is that suicidal thoughtsmust be taken seriously at all times.
“Our very first hope is that we willincrease the awareness of nurses,” she says.“When we say ‘take it seriously,’ we meanask those very difficult questions and thenget a team response, get other peopleinvolved, get the physician…the socialworker…and get help started early.”
Obvious signs of suicidal thoughts arejust that:obvious.Someone may say “life isn’tworthwhile” or “I have nothing to live for.”The less obvious, non-verbal signs take a bitmore effort to pursue and assess.These mayinclude patients’ sudden sense of urgency tostore medications, give things away, or neg-
A CRYNew RNAO best practice guideline helps nurses identifythose at risk of taking their own life. by Kimberley Kearsey
Illu
stra
tio
n: S
and
ra D
ion
isi

Registered Nurse Journal 23
lect personal care or the care of loved ones.“Nothing else works if you don’t
acknowledge first that the person is con-templating suicide,” Santa Mina says.“We’retrying very hard to help nurses move awayfrom keeping this a hidden illness.”
Fourteen of the 26 recommendations inthe guideline focus on areas of clinical prac-tice that can be improved,while the remain-ing recommendations cover educational,political and organizational change thatcould make a difference. Clinically, nursesare being advised to not only take the signsseriously, but to also build therapeutic rela-tionships with clients through active listen-ing, trust, respect, genuineness, tolerance,validation and empathy. Helping at-riskindividuals also means:• minimizing their feelings of shame, guilt
and stigma associated with suicide • assessing and managing environmental fac-
tors that may impact the physical safety of apatient or their health-care provider(s)
• documenting the details of a suicide plan ifthe individual is willing to share them
• obtaining additional medical informationabout your patient from family, friendsand other health-care professionals
• problem-solving to facilitate the patient’sunderstanding of their predicament andsome potential solutions, and
• fostering hope According to evidence summarized in
the BPG, it’s not uncommon for people whotake their own lives to see a health-care pro-fessional a few weeks prior to their death. Inmany cases, it’s for complaints about some-thing physical, such as pain. By establishingtherapeutic relationships with patients beforeit’s too late, nurses can help them feel safeand dignified if they are looking for help.Affirming a patient’s sense of self-worthminimizes feelings of hopelessness, shame,guilt and fear that feed suicidal behaviour.
Santa Mina admits some people are verygood at hiding what’s really happeningbehind the scenes. They may say they’vethought about suicide but they would neverdo it for religious reasons or because they
have children to raise. Santa Mina remindsnurses it’s important not only to ask if some-one’s thinking about it, but to also ask whatwould help them to not think about it.There’s a lot of help that can be given to alle-viate the suffering,even if the person says theywould never attempt suicide, she explains.
“The person is obviously living in agreat deal of distress and needs help…youdon’t know at what point in time the scalesmay tip…and they decide indeed that theirreasons for living are not strong enough,”she says. “What an awful way to live yourlife, feeling like you would like to end it.”
Trust between the patient and the nurseis, without question, the first step. But oncethat’s been established,nurses must continue tohelp. In cooperationwith their patients, theycan, for instance, clearthe immediate area ofhazardous items such asbelts, shoelaces, cords,lighters, linens, medica-tions, plastic bags, orsharp/glass objects.Theycan talk to patientsabout their relationshipswith family and friends,and link them to com-munity resources thatwill help should theyfind themselves in adangerous situation.
The guideline also suggests nurses talk toother people close to the patient. Gettingadditional medical information from family,friends and other health-care professionalswill help nurses to determine recent stres-sors that are influencing an individual’s stateof mind. By understanding these triggers,nurses can begin to problem solve. SantaMina says doing this in partnership withpatients encourages their involvement ingenerating strategies and gives them a senseof control over their lives.
When people are suicidal, their feelingsof hopelessness can be overwhelming. The
BPG addresses this, and touches on the pos-sibility that nurses may also begin to feeloverwhelmed if they think there’s nothingthey can do to help.The BPG is intended asa quick resource when these feelings surface.It recommends nurses turn to their fellowteam members or supervisors for support.
In addition to these and other compre-hensive recommendations, the guidelineprovides notes on cultural considerations,debriefing strategies, suggested interviewquestions, check lists to consider whenassessing patients, and a list of educationalsources to learn more about suicidal behav-iour. Heather McConnell, AssociateDirector for RNAO’s International Affairs
and Best PracticeGuidelines Programs,believes these tools will be well received.“Nurses asked us for abest practice guidelineon suicide prevention,”she says. “This is aresponse to their call.”At least 300 BPG topicareas have been sug-gested via RNAO’son l ine sugge s t ionform. Suicide, she says,consistently came upfrom front-line nursesand from former BPGpanel members.
It’s a timely topic,Santa Mina adds.With the economy in suchturmoil, nurses need to be on the alert.“Aswe see things unfold over the next six, 18,24 months, if it rolls through the economywith job losses, that’s tough for people,” shesays. “Nurses have a frontline, primary roleto play in detecting individuals who arehighly vulnerable…and ensuring that theprocesses and interventions get put intoplace quickly…to give them the supportthey need to get through a tough time.”
KIMBERLEY KEARSEY IS MANAGING
EDITOR FOR REGISTERED NURSE JOURNAL.
FOR HELP
WHO’S AT RISK?Following is a small sampling of
the risk factors for suicide…
age (older adults)
demographic (male, Aboriginal, wid-
owed/divorced)
poverty or social isolation
family history of suicide
psychiatric illness (bipolar,
schizophrenia, depression)
addiction
childhood trauma
To access the full list, and RNAO’s
Assessment and Care of Adults at
Risk for Suicidal Ideation and
Behaviour, visit www.rnao.org.

24 January/February 2009
Pho
to: C
ou
rtes
y R
VH
Co
rpo
rate
Co
mm
un
icat
ion
s
Itis not unusual for RNs to encouragepatients in distress to hang on andkeep fighting. But last spring, the
tables were turned when,one extraordinarymorning at Barrie’s Royal Victoria Hospital(RVH), cardiac patient Diana Rogler sig-nalled her support and encouragement toemergency nurse and RNAO memberTerri Reid as she pumped her way throughan unprecedented 40 minutes of cardiopul-monary resuscitation.
Rogler says she owes her life to Reidand will never forget the day she and herhusband, who works at RVH, were on the15-minute drive to the hospital whensevere chest pains suddenly hit.
“I don’t remember going into triage,”Rogler says “but I walked into the emergand layed down on a stretcher. The nursedid an ECG right away. I remember think-ing ‘what’s going on?’Then I looked at myhusband and said ‘I’m going to pass out.’”
She did, and Reid was called over.“We grabbed the cart and I took over
the CPR,” the 43-year-old RN remem-bers. Hospital protocol calls for ‘fast andhard’ compressions, which can be exhaust-ing.Three other nurses pitched in, but onlyReid was able to keep a good pulse.“It wasdecided, I’m it,” she recalls.
Forty minutes is almost double the usualtime allotted to perform CPR, but Reidand her colleagues knew this was no ordi-nary case. Rogler was just 42, a mother ofthree, and she had no history of heart trou-ble. But perhaps more remarkable was thefact that as the team continued its work,their patient appeared to be watchingthem.They knew they couldn’t give up.
“Her eyes were open and she had purpose-ful movement,” Reid recounts. “With eachcompression I did, there was a ‘huhh’ sound. Iwas hurting her.Every so often she just reachedup and held my arm, as if to tell me ‘I’m stillhere. Just keep fighting,keep going.’”
Rogler can only speculate on what shewas signalling.“I don’t know in what con-text (I reached for her arm). Probably ‘thishurts like hell but don’t stop. It’s OK... I
know you’re doing what you have to.’”Whatever she meant, it was a motivator
for Reid.“The adrenaline was just rushing.You don’t think of how tired you are; youare so consumed by the moment.”
“We just kept pumping her with medsand kept defibrillating her heart,” she con-tinues. “For the sixth defibrillation at the40-minute mark, we turned her on herside, put one (paddle) on front and one onback and got a heart rate. It was a hugerelief. I thought ‘Oh my God, we did it.’”But there wasn’t time to celebrate. Thephysician did a quick ultrasound, looked upand said:“Get her out of here now.”
That’s when Rogler’s memory kicksback in. “When I woke up, I was in theambulance and came to enough for themto tell me I was on my way to Southlake(Regional Health Centre in Newmarket).”
The caring face she saw was Reid’s.Once there,Rogler was whisked into the
cardiac catheterization lab with Reid andthe RVH team watching from the nursingstation. They discovered a dissecting leftanterior descending (LAD) artery, a rarecondition with a high mortality rate.Therewasn’t time to move her to an operatingroom. It was a few days later when Roglersays the reality hit. Not knowing how muchshe would remember, her husband had shel-tered her from the details of her ordeal untilshe was strong enough to absorb them. “Hesaid,‘I’ve got a story for you.’ ”
Rogler was amazed when she discov-ered what Reid and the RVH team haddone.She likened the experience to findingout there was a bad storm while she wassleeping. “You are like ‘huh?’ I don’t evenknow what happened.” She spent the nextdays piecing together the events and recov-ering. “The worst pain was my chest,” shesays. Many ribs had been cracked by Reid’sstellar technique,but there was no opportu-nity to complain. “If you think you aresore,” one of her Southlake nurses told her,“go see the lady who did CPR on you.She’ll be worse.”
Rogler did, indeed, see her lifesaver justa few weeks later. But she kept the hugsgentle. “She’s just a powerhouse,” Roglersays of Reid. “Everyone did an awesomejob but she had the greatest impact.”
“There are only so many words you cansay for something like that,” she adds oftheir emotional meeting.“Thank you.”
In September, Rogler was back at workas a part-time dental hygienist. She finishedher cardio rehabilitation program early inDecember. RN
HELENA MONCRIEFF IS A FREELANCE
WRITER IN TORONTO.
Forty minutes to save a life Barrie RN leaves cardiac patient and mother of three thankful to be alive.BY HELENA MONCRIEFF
We’re looking for more extraordinary stories about RNs who have made a difference to patients,
their families and friends. Has someone shared with you their gratitude for what an RN has done
for them? Have you got a personal story to tell about a nurse who cared for you? Please contact
[email protected] and share your experiences. Stories may be published in future issues of
Registered Nurse Journal.
Diana Rogler (left) made a special trip back toRoyal Victoria Hospital in Barrie to thank RNTerri Reid for her life-saving measures.

Registered Nurse Journal 25
When the federal budget wasunveiled in late January, RNAOissued a press release praising the
government for its plan to spend $2 billion onsocial housing, including money to repairexisting homes. The commitment also ear-marked funds to improve housing for peo-ple living in Aboriginal communities, forseniors, and for those with disabilities.However, the requirement to secure match-ing funds from provinces andalready cash-strappedmunicipalities will limitthe benefit for those whourgently need a roof overtheir heads. “As nurses weknow that shelter is a basichuman right, just likehealth. So, if the moneyindeed flows, measures likethis will help. What was really lacking in the federalbudget was an overallnational housing strategy,”said President Wendy Fucile.
On the broader issue of poverty, Fucilesaid changes in the Canada Child TaxBenefit would help some families but theywouldn’t be enough to help the more than788,000 children who live in poverty acrossthe country.The fact that there wasn’t a sin-gle mention of poverty or child poverty inthe whole budget document is unaccept-able, she added.
In terms of health, RNAO welcomedthe government’s $500 million investmentto encourage greater use of electronichealth records. However, it was most disap-pointing that the plan didn’t include specificinvestments to address the nursing shortage,including funds to create more seats in nurs-ing programs and to add more nursing fac-ulty to help educate tomorrow’s RNs.
Executive Director Doris Grinspun saidthe government “opted again not to use itspower to protect the country’s publicly-funded, not-for-profit health-care systemby withholding health transfers whenprovinces violate the Canada Health Act.” It
also missed a golden opportunity to investtaxpayers’ dollars into developing a nationalpharmacare program covering essentialdrugs, she added. RN
Provincial budgetWith the federal budget behind us, RNAOis now focusing on the upcoming provin-cial budget, expected within the next fewweeks. In December, President Wendy
Fucile appeared before theStanding Committee on Financeand Economic Affairs to presentRNAO’s pre-budget submis-sion. She used the occasionto again spell out the needfor 9,000 additional nurses, acommitment the govern-ment had pledged to dur-ing the 2007 election andThrone Speech, butbacked away from last fallwhen Finance Minister
Dwight Duncan said the promisewould be delayed given the economicdownturn. Fucile told the committee thatRNAO expects funding for 3,000 addi-tional nurses in 2009 as well as funding for10 of the 22 additional NP-led clinicsalready promised. Fucile thanked theMcGuinty government for acting on itspromise to set up NP-led clinics in SaultSte. Marie and the Erie St. Clair andNorth-West LHINs. Executive DirectorDoris Grinspun commended the govern-ment for its poverty reduction strategy,
released in December 2008.The associationis especially pleased with the hard targets toreduce child poverty by 25 per cent overfive years, but said the promises must bebacked up with earmarked funds in theupcoming provincial budget. RN
Why reinstatement of competitivebidding a bad move for taxpayers Competitive bidding of home-care con-tracts is front and centre again followingHealth Minister David Caplan’s decision inlate December to reinstate the practice andlift the moratorium put in place by hispredecessor George Smitherman. RNAOwas quick to respond, issuing a mediarelease and action alert. More than 290members wrote letters condemning thegovernment’s decision.
RNAO argues the steps announced byCaplan to improve accountability, such aspublic reporting and quality measures, arefine, but do nothing to address the funda-mental problems with competitive bidding.Through this practice, health-care providersare pitted against one another to win con-tracts. Executive Director Doris Grinspunsaid a competitive system undermines con-tinuity of care and caregiver for patients,and it threatens job satisfaction for healthproviders.
“Competitive bidding will continue tocreate uncertainty and disruption for home-care clients and health-care providers alike,”she said.“What we really need is a substan-tive investment in dollars and cents.” RN
Despite hopeful signs, federal budget misses the mark
This spring, the government’s new pesticide law will take effect. The association’s advocacy
campaign to ensure the legislation includes protective regulations governing the use of
certain cosmetic chemicals included many meetings with other health and environmental
stakeholders and government officials, numerous action alerts, and hundreds of letters to
MPPs. RNAO is now awaiting the final list of regulations which will govern the sale and use
of prohibited chemicals on lawns and gardens.
Despite heavy resistance and lobbying from the pesticide industry, it appears the
province is on the verge of enacting one of the toughest pesticide bans in North America.
Thanks to each of you who took the time to write and speak out on this important issue. RN
POLICYAT WORK
PESTICIDE UPDATE

The Dufferin Area Family Health Team (FHT), led by
RNAO member Lianne Davies, has launched Weigh 2 Go!,
a new program to help overweight children avoid early
onset diabetes, high cholesterol, arthritis, depression,
anxiety and many other illnesses linked to childhood obesity.
“It’s about getting the kids active and really making that
lifestyle change to get them on the road to success,” explains
Davies, who is executive director of the FHT.
Starting in March, at least 15 families will be the first
in Dufferin County to attend workshops and family activity days
to learn more about how to make healthier choices.
The Canadian Nurses Foundation (CNF) has announced a new $100,000 fund to support Aboriginal nurses studying at the bachelor, master’s, PhD and nurse practitioner levels.Working with the Aboriginal Nurses
Association of Canada, and with financial support from TD Bank Financial Group, CNF will provide research awards for Aboriginal students and research teams conducting studies with the goal of improving
health outcomes for Aboriginal Canadians.Visit www.cnf-fiic.ca for more information.
Seniors at the Snow Centre, a nursing home in Hampton, Ontario, are exercising their bodies and minds
with a new Nintendo Wii system, playing virtual video games that reflect players’ body movements on a TV screen.
“Even if they have a physical or mental disability, they can still play and benefit from it,” says recreational
therapist Gloria Baird, adding that many seniors have fun from their wheelchairs. As long as they can move
their arms, residents can play anything from tennis to bowling to boxing.
According to figures released by the Ontario Universities’Application Centre on Jan. 19,students’ interest in nursing programs is up 11 per cent compared to January of 2008.These Preliminary
Undergraduate Application Statistics are released each year to provide a snapshot of applications from Ontario secondary school students. Statistics on applications from individuals who are not in secondary school
will be released in the spring.To find out more, visit www.ouac.on.ca.
According to the study published in December by The American Journal of Bioethics,
84 per cent of medical students and 81 per cent of nursing students surveyed at Baltimore’s Johns Hopkins
University in 2007 watched medical dramas such as House and Grey’s Anatomy. The study recommends that
medical schools supplement typical class work, which involves reading a case study, with a brief clip from a medical
drama to stimulate students’ ethical analysis. “Actually seeing an interaction can convey a lot more than reading
about it,” says co-author Matthew Czarny, a third year Johns Hopkins medical student.
The Ontario government is hoping to increase organ and tissue donations across the province by implementing a new way of collecting consent: affirmative registration.
Traditionally, Ontarians would consent to donation when they renewed their health cards or driverslicences.The new system, which is electronic and only records ‘yes’ responses in a provincial
database, will replace the donor card in order to enable Trillium Gift of Life Network to better support families by sharing their loved one’s donation decisions.The government is recommending
everyone register their consent online to ensure their decision is respected. Only 12.5 per cent of Ontarians have consented to donation.Visit www.giftoflife.on.ca for more information.
26 January/February 2009
toYoutoUseNEWS

Calendar
Registered Nurse Journal 27
FebruaryFebruary 17Preceptorship for nursesVideo conference – workshopThunder Bay Regional Health CentreThunder Bay, Ontario
AprilApril 17-18 10th Annual Options forDiabetes ConferenceHoliday Inn, Kingston, OntarioTopics: The miracle of insulin;embracing diabetes; community advocacy; workingeffectively with clients fromdifferent generations; clinicalpractice guidelines; sleepapnea in diabetes; mind-fulness-based diabetes management; oral hygiene;wound management.Contacts: Margaret [email protected] 613-547-3438 Joan Ferguson613-239-0551
April 23-24 RNAO’s 84th Annual General MeetingHilton SuitesToronto/Markham ConferenceCentre and SpaMarkham, Ontario
April 27-May 1Designing and DeliveringEffective Education Programs89 Chestnut ResidenceToronto, Ontario
May
May 27Clinical Nursing Symposium –Knowledge on the FrontlineMississauga Convention CentreMississauga, Ontario
CALL FOR ENTRIES!This is an opportunity for individual nurses to submit stories that demonstrate theiruse of nursing knowledge onthe frontline. One author willwin a copy of esteemed artistMicheline Montgomery’sacrylic on linen painting, The Soul Worker. Deadline for submissions: Friday, March 13, 2009 4:00 PM EST.
For more information:visit www.rnao.org or contact Vanessa Mooney, [email protected] or 1-800-268-7199/416-599-1925 ext. 265.
MarchMarch 29-April 3 2nd Annual Wound Care InstituteWhite Oaks Conference Resort and SpaNiagara-on-the-Lake, Ontario
NATIONAL NURSINGWEEK 2009
Monday, May 11 toSunday, May 17
This year’s theme…Nursing – You can’t
live without it.Mark your calendarFriday, May 15, 2009
RNAO Nursing Career Fair & ExpoDelta Chelsea Hotel
Toronto, Ontario
Unless otherwise noted, please contact RNAO’s Centre forProfessional Nursing Excellence
for further information 416-599-1925
1-800-268-7199 Victoria van Veen ext. 227
[email protected] orVanessa Mooney ext. 265
It’s not too early to plan ahead to 2010!
Join us in Toronto for RNAO’s 5thInternational Nursing EducationConference: Exploring Practice
Education in NursingNov. 29 to Dec. 1, 2010
**New this year**Exciting networking reception
Dec. 1, 2010
This networking opportunity, jointly hosted by RNAO andWorkplace Integration of
New Nurses (WINN), bridgesbetween RNAO’s Education
Conference and WINN’s Nursing the Future Conference
(Dec. 3-5, 2010)For more information, visit
www.RNAO.org

DO YOU HAVE FINANCIAL PLANNING QUESTIONS AS YOU NEAR RETIREMENT?I will assist you with your retirement plan-
ning questions, which may include informa-
tion on: HOOP Pension Plan; Canada Pension
Plan; RRSPs; taxation; investment and estate
planning. With over 19 years of consulting/
planning experience, I have insight into your
professional/financial issues. As a certified
financial planner with a fee-based business,
I am also licensed to sell some products. For
an appointment at your convenience, please
contact Gail Marriott CFP at 416-421-6867.
DIABETES UPDATE 2009: ADVANCESAND CHALLENGES IN MANAGINGDIABETES IN AN ERA OF CHOICE: Friday, April 3, 2009, Metro Toronto
Convention Centre, South Building,
700 Level, 222 Bremner Boulevard,
Toronto, Ontario. For program and
registration information, please go to
http://events.cmetoronto.ca/website/index/
BDC0901 or contact: Office of Continuing
Education & Professional Development,
Faculty of Medicine, University of Toronto.
Phone: 416.978.2719 / 1.888.512.8173.
Fax: 416.946.7028.
Email: [email protected]
Classifieds
REGISTERED NURSES PROMOTING HEALTH INFAITH COMMUNITIES… AND BEYOND
Have you thought about Parish Nursing Ministry?Wholistic Nursing in a congregational setting?
Would You like to know more?
Openings available for parish nurses across Ontario especially in the Waterloo Wellington area supported by the
Ontario Aging at Home Strategy of the Waterloo Wellington Local Health Integration Network.
Attend our free Information Forum on Saturday, April 18, 2009Register by calling 1-888-433-9422 (Registration at 8:30 a.m.)
Location: Jubilee United Church 9:00 a.m. to 12:15 noon
40 Underhill Drive, Toronto, Ontario, M3A 2J5(1 traffic light east of DVP, 2 blocks north of Lawrence)
INTERCHURCH HEALTH MINISTRIES44 Metcalfe Avenue. Aurora, Ontario, L4G 1E6Phone: 905-841-7619 Toll Free: 1-888-433-9422 Fax: 905-841-4051Website: www.ichm.ca E-mail: [email protected]
Fostering healthy communities through Christ’s healing ministryICHM Registered Charitable No. 890261175RR0001
ONTARIO ASSOCIATION OF NON-PROFIT HOMES & SERVICES FORSENIORS (OANHSS) ADMINISTRATORCERTIFICATION PROGRAMFebruary 22-27, 2009 at the Sutton Place
Hotel, Toronto. Recognized by the Ministry
of Health and Long-Term Care. Directors of
Nursing: Thinking of becoming an adminis-
trator in long-term care? This is the course
for you. Contact: Stuart, certification
registrar, at (905) 851-8821 ext. 240,
[email protected], www.oanhss.org
ALZHEIMER SOCIETY OF TORONTO. PLACEMENT SERIES. MARCH 5/12/19,2009. This set of three workshops provides family
caregivers with an overview of the issues
related to long-term care placement. Guest
speakers from the Community Care Access
Centre and the Advocacy Centre for the
Elderly will be facilitating. Family members
may choose to attend one session or all
three. Time: 2:00 to 4:00 p.m.
Location: Alzheimer Society of Toronto,
20 Eglinton Avenue West, 16th floor.
Please contact one of our counsellors to
register. Call 416-322-6560 or
Caring for you.Caring for you.Caring for our community. Caring for our community.www.tsh.to
At The Scarborough Hospital (TSH), Canada’s largest urban community
hospital, Nurses are central to delivering unique services and programs
specifically designed to meet our patients’ diverse healthcare needs.
That’s why we provide professional development support and in-house
resources in the areas of practice, education and research. Caring and
compassionate, our 1,600 Registered and Registered Practical Nurses are
committed to health and wellness in the community.
Exciting opportunities await both:
Experienced Registered Nurses and Nursing Graduates
If you share our values of leadership and compassion, join our team. Find out more
about the rewarding careers at TSH and apply online by visiting: www.tsh.to
Committed to the future of
urban healthcare
106926tsh_RNAO.indd 1 11/7/2008 12:35:37 PM
Leadership andManagement
Program
GRANTING UNIVERSITY CREDIT ANDLEADERSHIP AND MANAGEMENT
PROGRAM CERTIFICATE OF COMPLETIONEndorsed by the CNA.
All courses individually facilitated by anEducational Consultant
Courses Offered:
Leadership and Management (6 units)
• 9 month course completion • both theoretical and practical content important
in today’s work environment
Leading Effective Teams (3 units)
• 6 month course completion • study of leadership, team dynamics impactingthe workplace, types of and team structure in
health care organizations
Conflict Management (3 units)
• 6 month course completion • explores the types and processes of conflict inhealth care organizations and applies theory and
research to conflict situations in the currentworkplace
Quality Management (3 units)
• 6 month course completion• theories, concepts including safety culture
leadership in creating a culture of accountability• critically analyzes and applies paradigms to
address quality and safety issues in the workplace
Advanced Leadership and Management (6 units)
• 9 month course completion • builds on the Leadership/Management course
• topics include transformational and quantumleadership, emotional intelligence and
organizational culture
Integrative Leadership Project (3 units)• Final course integrates theories and concepts ofthe Program and provide opportunities to apply
these to a real situation in the workplace • Through the use of a champion leader, the
student develops and understanding of managingkey organizational processes
PROGRAM COURSES AVAILABLE IN TUTORIALCLASSROOM FORMAT (OVER 12 WEEKS)
For further information please contact:Leadership and Management Program
McMaster UniversityPhone: (905) 525-9140 Ext 22409 Fax: (905) 529-3673
Email [email protected]: www.leadershipandmanagement.ca
Programs starting every January,April & September
CALL FOR ABSTRACTS
For details, please visit:www.rnao.org/centreevents
Contact Vanessa Mooney, Conference Coordinator at:
[email protected] 416-599-1925/800-628-7199
Call For AbstractsSubmission Deadline: March 27, 2009
Assistant Professor/AssociateDEPARTMENT OF NURSING
canadian nurse 1/4 page — 3 3/8” W X 4 7/8”H
S T . C A T H A R I N E S O N T A R I O C A N A D A
Approved by:
Title:
Date:A signature on this material signifies that it is perfect. If thereare any changes to be made, do not sign. Any changesrequested after the material is signed will be the financialresponsibility of the signator.
The Department of Nursing invites applications for a probationary/tenure-trackposition at the rank of Assistant or Associate Professor, effective July 1, 2009. One offive departments within the Faculty of Applied Health Sciences, the Department ofNursing currently offers an accredited BScN Degree in collaboration with LoyalistCollege and a BScN Degree Completion Program with foundations on the principlesPrimary Health Care. The Canadian Association for Schools of Nursing have awardedBrock’s nursing programs a seven-year accreditation. Brock has a strong commitmentto students and to the highest standards of teaching and research excellence. As adestination of choice for Ontario students, Brock has recently experienced one of thehighest increases in student applications among Ontario universities.
Successful candidates will have a Bachelors degree in Nursing, a PhD in Nursing ora related discipline and a focused program of research and publications. (Candidateswith a Masters in Nursing nearing completion of a PhD may be considered). We invitecandidates with clinical expertise in a variety of areas. Preference will be given tocandidates with expertise in acute care medical or surgical nursing. Additionalpreference will be given to candidates with graduate teaching experience. Applicantsmust be qualified for Registration with the College of Nurses of Ontario.
Please send a letter of application, curriculum vitae and three letters of referenceto: Dr. Lynn Rempel, Chair, Department of Nursing, Faculty of Applied Health Sciences,Brock University, St. Catharines, Ontario, Canada L2S 3A1; Tel. 905-688-5550, ext.4774; Fax 905-688-6658. Closing date for applications is January 15, 2009 or until asuitable candidate is found. These positions are subject to final budgetary approval.All qualified candidates are encouraged to apply, however, Canadians and permanentresidents will be given priority. Brock University is actively committed to diversity andthe principles of Employment Equity and invites applications from all qualifiedcandidates. Women, Aboriginal peoples, members of visible minorities, and peoplewith disabilities are especially encouraged to apply and to voluntarily self identify asa member of a designated group as part of their application. Candidates who wish tohave their application considered as a member of one or more designatedg roups shou l d f i l l ou t t he Se l f- I den t i f i ca t i on Fo rm ava i l ab l e a thttp://www.brocku.ca/humanrights and include the completed form with theirapplication.
Mark your calendars and plan your year!The CAWC’s S-Series has been developed by
wound-care leaders from Canada and aroundthe world. Featuring: S1 – A completeoverview of the CAWC’s Best Practice
Recommendations; and S2 – Hands-onworkshops in the fundamental woundhealing skills. If you are looking for a
valuable, interactive educational experiencein wound care, you won’t want to miss out!
Join us for two great days of learning in:VANCOUVER · February 13–14Sheraton Wall Centre (in English)
TORONTO · March 6–7Sheraton Toronto (in English)MONTRÉAL · April 17–18Delta Centre-Ville (in French)
Complete information: visit www.cawc.net, call 416-485-CAWC (2292)or e-mail [email protected].
DO YOU KNOW A SPECIAL NURSE?Toronto Star readers are being asked to
nominate someone in the Nursing Profession for the TORONTO
STAR NIGHTINGALE AWARD 2009.
Information on Award Criteria and where to send your nomination will be
published in the Star and online at www.thestar.com/nightingale
Deadline for nominations is March 25, 2009. Winner will be announced during
Nursing Week 2009.
2009
Faculty of Nursing –Tenure-Track PositionsWe are poised for growth and renewal,and are seeking exceptional faculty tojoin us in our initiatives, including a Centre for Excellencein Gerontological Nursing, a Clinical Simulation andLearning Centre, an integrated model for undergraduatecurriculum, and a nursing program in Qatar.
ProfessorsOf particular interest are applicants with a backgroundin gerontological nursing, health outcomes research,cardiovascular health, palliative care or nursing education.
InstructorsOf particular interest are applicants with a backgroundin clinical practice and teaching across the lifespan,illness trajectories or service-delivery settings.
For more about these positions and working at theUniversity of Calgary, visit ucalgary.ca/hr/careersand ucalgary.ca/hr/frro.
Canadian citizens and permanent residents will be givenpriority in their applications.
The University of Calgary respects, appreciates andencourages diversity.
UFN18987_TTP_JanFeb2009_RNAO:Layout 1 10/23/08 1:12 PM Page 1

AccreditationMatters
Not all retirement residencesare accredited by the Ontario Retirement Communities Association,
only those that meet the highest industry standards
Contact us to locate ORCA approved retirement residencesin your area
Visit our website www.orca-homes.comor call 1-866-927-6722
Online Education forHealth Professionals�� 0DVWHU RI +HDOWK 6WXGLHV
�� 0DVWHU RI 1XUVLQJ- ANP: Primary Health Care- Generalist
ZZZ�DWKDEDVFDX�FD�FQKV
CENTRE FOR NURSING AND HEALTH STUDIES
Advance online!D F F H V V L E O H � I O H [ L E O H � D F K L H Y D E O H
$SSOLFDWLRQ 'HDGOLQH�AGD:ANP & MN:ANP - December 1, MHS & MN: GEN - March 1

On The Pulse of HEALTH CARE
S•R•T Med-Staff is a trusted leader in the healthcare community with
a reputation for excellence in quality of care. With the greatest variety
of shifts and top pay rates to the highest quality of nurses, it’s no wonder
Toronto RNs & RPNs continue to rank S•R•T Med-Staff number one
or that so many healthcare providers trust S•R•T Med-Staff personnel
to provide an exceptional level of care.
Contact us today for your personal interview at 416•968•0833
SRT Medstaff 4 Colour Ad – RNAO. 2007. 7.125 inches wide x 9.875 inches deep. Contact: Eric Bell 416 961 4060 ext 224