targeted radiotherapy with an anti-cd66 monoclonal antibody in haematopoietic stem ... · ·...
TRANSCRIPT

Targeted Radiotherapy with an anti-CD66
monoclonal antibody in haematopoietic
stem cell transplantation:
Therapy intensification
without toxicity
Kim Orchard
Southampton University Hospital Medical School and Trust
Targeting the bone marrow

Why transplant?
Improves the outcome for many haematological malignancies
• Autologous - myeloma - lymphoma
• Allogeneic - Acute Leukaemias (donor) - chronic leukaemias
- myeloma - lymphoma

How to Transplant
• Conditioning
– Cytotoxic therapy
– Total body irradiation (TBI)
Problem:
- non-specific toxicity to organs
Role of radiation therapy in
transplantation
� Haematological malignancies are radiosensitive
� Radiotherapy provides effective disease eradication
and immunosuppression
� Dose escalation of radiotherapy increases disease
eradication
BUT: dose escalation increases treatment toxicity

Toxicity and Dose
Toxicity
Treatment dose
Lethal toxicity
‘low dose’ ‘High dose’
Tumour cells surviving

Toxicity and Dose
Toxicity
Treatment dose
Lethal toxicity
‘low dose’ ‘High dose’
Tumour cells surviving

The bone marrow as target for therapy
T
B
I

Toxicity of conditioning
Acceptable
• Haematopoietic
Unacceptable
• Gastro-intestinal
- Mucositis- Diarrhoea
• Hepatic
• Renal
• Neurological
• Pulmonary

Manipulation of TBI to reduce toxicity
• dose fractionation
• shielding sensitive organs
e.g. lungs
• lower dose transplant conditioning
- 200 cGy
- no TBI
Targeted radiotherapy

Principles of targeted radiotherapy
• Vector e.g. monoclonal antibody
• Radioisotope gamma for imaging/dosimetry
beta or alpha for therapy

Selection of therapeutic isotope
Isotope half-life radiation energy (MeV) range(mm)
Iodine-131 8.1d gamma+beta 0.6 0.8
Yttrium-90 2.7d beta 2.3 2.7
Rhenium-186 3.8d gamma+beta 1.1 1.1
Rhenium-188 17hr gamma+beta 2.1 2.4
Holmium-166 1.1d gamma+beta 1.9 2.2
Bismuth-212 1hr alpha 6.1 0.04-0.1
Astatine-211 7.2d alpha 5.9 0.04-0.1

Radionuclide selection: Iodine-131 vs Yttrium-90
Advantages of 131I
- published experience in BMT conditioning
- ‘easy’ to conjugate
- preliminary dosimetry possible
- relatively cheap and easily available
Disadvantages of 131I
- Gamma emission high with therapeutic doses
- problems with patient care, bloods, waste
- relatively long physical t1/2 (8 days)

Radionuclide selection: Iodine-131 vs Yttrium-90
Advantages of 90Y
- high beta emission (2.3 MeV vs 0.6 MeV for 131I)
- no gamma emission
- less toxicity to non-haematological tissues
- short physical t 1/2 (2.7 days)
Disadvantages of 90Y
- conjugation chemistry difficult
- high energy beta-particles may damage BM stroma
- preliminary dosimetry difficult
(Indium-111 substitutes)

Targeted Radiotherapy in Haematological Malignancies
Radiation kills at a distance

Bone marrow as target

Bone marrow as target

Vector - Anti-CD66
Isotopes - In-111 imaging
- Y-90 therapy
Phase I - radiation dose escalation
- 5, 10, 25, 37.5 MBq/kg bw
Phase II - set radiation dose at MTD
Clinical study (Southampton)

CD66 antigen
CEA family
Glycoproteins
Variable number of Ig domains
several related
glycoproteins CD66a-f
CD66a,b,c,e expressed by
myeloid series

Vector:
Anti-CD66
murine IgG1 monoclonal Ab
binds to common epitope on CD66a,b,c,e
manufactured to GMP
conjugated to bifunctional chelator
single patient dose vials

Isothiocyanato-2-benzyl-3-methyl-
diethylenetriaminepentaacetic acid
(ITC-2B3M-DTPA)
N
N
C
O
O-
C
O
O-
M
C O
-O
ANTIBODY
N
C
O-O
C
O
-O
NH
CN
S
CH3
(lysine)
Dr Syed Quadri

Targeted radiotherapy flow diagram 1
Antibody prep Patient prep
- purified Candidate pts.
- viral inact’n - initial discussion
- QC - patient info sheet
- second discussion
Conjugated to DTPA
- HPLC - consent
- immunoreactivity
- Scatchard plot
- LAL on bulk
- microbiological screen Pre-study tests
- protein assay
Conjugated antibody stored
in single patient dose vials
Dry-run labelling x2
- ITLC/TLC/HPLC
- LAL
Labelling for patient Administered to pt.
- ITLC/TLC/HPLC
- LAL

Preparation of labelled antibody
1 hr RT
DTPA-conjugated Ab Radiolabelled Ab
+ In-111
or Y-90

Patient selection:
Autologous or allogeneic (sibling or VUD) transplant for
an underlying haematological malignancy
- AML in CR1 but with poor prognostic features
- AML > CR1 or in relapse
- ALL
- transformed myelodysplasia
- CML (AP, BT, poor response to Glivec)
- multiple myeloma.
Patients may be in remission, PR or relapse.

For autologous transplant (HD melphalan)
D –14 D –7 D –2 D 0
Y-90 labelled
Anti-CD66Review, fbc HD Melphalan
Autologous stem cells
D –22 to D –16 In-111 imaging Dosimetry

For allogeneic transplantation
D –14 D –7 D –2 D 0
Y-90 labelled
Anti-CD66
Fludarabine 30mg/m2
CAMPATH 1H 10mg/m2
Melphalan 120mg/m2
Allogeneic stem cells
D –22 to D –16 In-111 imaging Dosimetry
CyA 5mg/kg d –3
3mg/kg d –2
level 100-150 ng/ml
tailing from d +60
MTX d 3, 6, 11 10mg/m2

Dosimetry
• Whole body quantitative gamma imaging
D 1, 2, 4, 5
• SPECT of thorax and pelvis
• Serial blood sampling – blood clearance
• BM biopsy D 2

PatientsPhase I
Ages: 21 – 67 yrs (mean 54)
M/F: 16M 4F
Disease: Myeloma 18
AML 2
Transplant: Autologous 16
Allogeneic 4

Clinical results
Infusion related toxicity
In-111 or Y-90
None

Whole body data
24 hrs post infusion
Anterior Posterior


Reconstructed 3D images

Whole body scan: activity remains in BM
1h1h 5h5h
22h22h 47h47h
120h120h
Effective halfEffective half--
life = 50.5hlife = 50.5h

Cross-sectional image created from
thoracic SPECT scan.
Bone marrow
(vertebral body)
Liver
spleen
Ratio of activity: BM vs Liver 4:1

5.3 ± 1.87.75 ± 2.124.32 ± 4.337.5
12.55 ± 6.33.66 ± 1.215.56 ± 2.025
2.38 ± 1.641.30 ± 0.49.14 ± 1.610
1.14 ± 0.41.40 ± 0.44.14 ± 1.65
GyGyGy
SpleenLiverBone marrow90Y dose
level
MBq/kg
Organ dosimetry
Phase I patients

Bone Marrow absorbed radiation dose and
activity of infused 90Y-labelled anti-CD66
BM absorbed radiation dose for each patient
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
0 500 1000 1500 2000 2500 3000
Y-90 dose in MBq
BM absorbed radiation
dose in Gy
Series1

BM Absorbed radiation dose
in Gy at each yttrium-90 dose level
0
5
10
15
20
25
30
0 5 10 15 20 25 30 35
Yttrium-90 dose level in MBq/kg
BM Absorbed radiation
dose in Gy
dose +/- 1 SD

Clinical results contd
Total leukocytes pre and post Y-90 labelled anti-CD66 Mab
Dose level 1 (5 MBq/kg)
0
1
2
3
4
5
6
1 2 3
week of study
Wbc x 10e9/L
pat i ent 1
pat i ent 2
pat i ent 3
pat i ent 4
pat i ent 5
Leucocytes pre and post Y-90 labelled Ab
Dose level 1 (5 MBq/kg)

Clinical results contd
Total leukocytes pre and post Y-90 labelled anti-CD66 Mab
Dose level 2 (10 MBq/kg)
0
1
2
3
4
5
6
7
8
1 2 3
week of study
Wbc x 1039/L
pat i ent 6
pat i ent 7
pat i ent 8
pat i ent 9
pat i ent 10
Leucocytes pre and post Y-90 labelled Ab
Dose level 2 (10 MBq/kg)

Total leukocyte count pre and post Y-90 therapy
Dose level 3 (25 MBq/kg)
0
2
4
6
8
10
12
1 2 3week of study
wcc x10e9/l
bw011
bw012
bw013
bw014
bw015
Leucocytes pre and post Y-90 labelled Ab
Dose level 3 (25 MBq/kg)
Clinical results contd

Total leukocyte count pre and post Y-90-Labelled anti-CD66
Dose level 4 (37.5 MBq/kg)
0
1
2
3
4
5
6
7
1 2 3
week o f study
Series1
Ser ies2
Ser ies3
Ser ies4
Ser ies5
Leucocytes pre and post Y-90 labelled Ab
Dose level 4 (37.5 MBq/kg)
Clinical results contd

Toxicities
Haematological: 20/20 grade 3 - 4
GI:
mucositis 8/20 grade 1
5/20 grade 2
5/20 grade 3
diarrhoea 12/20 grade 2 – 3
No worse than anticipated for standard
transplant conditioning
No SAEs

Clinical results contd
Engraftment
19/20 full engraftment
(1 patient delayed platelet engraftment)
Neuts > 0.5 mean 13.8 days (11 – 22)
Plts > 50 mean 12.7 days (10 – 22)
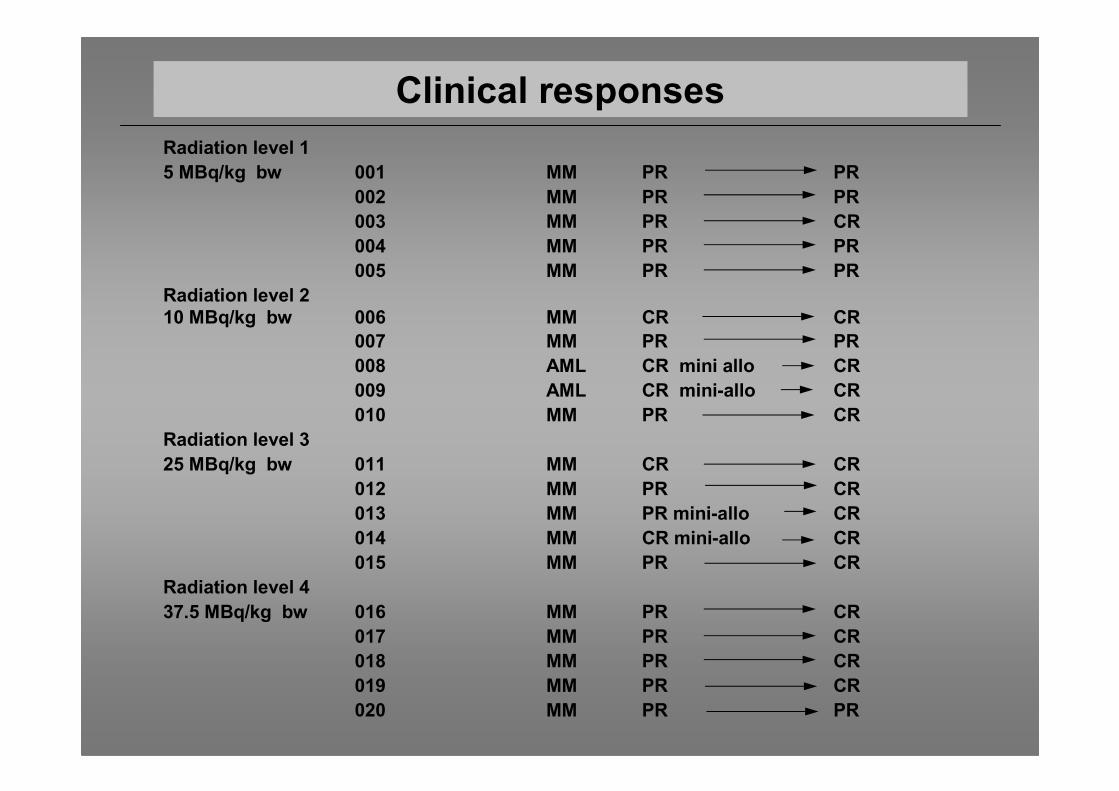
Clinical responses
Radiation level 1
5 MBq/kg bw 001 MM PR PR
002 MM PR PR
003 MM PR CR
004 MM PR PR
005 MM PR PR
Radiation level 2
10 MBq/kg bw 006 MM CR CR
007 MM PR PR
008 AML CR mini allo CR
009 AML CR mini-allo CR
010 MM PR CR
Radiation level 3
25 MBq/kg bw 011 MM CR CR
012 MM PR CR
013 MM PR mini-allo CR
014 MM CR mini-allo CR
015 MM PR CR
Radiation level 4
37.5 MBq/kg bw 016 MM PR CR
017 MM PR CR
018 MM PR CR
019 MM PR CR
020 MM PR PR

Proposed study 1
• Phase II trial (randomised 2 arm)
• RIT with HD melphalan
• Cohort of patients with Myeloma (45)
• 4 centres participating
– Southampton
– Bart’s
– Birmingham
– Mainz
Funded by the Leukaemia Research Fund £250,000

In vivo targeting of
myeloma

Phase II
10 patients transplanted
Ages: 21-62 yrs (mean 57.7)
Donor: Sibling 5; Unrelated donor 5
Indications: CML 2
AML 5
Myeloma 3
Allogeneic reduced toxicity transplants

Mr CG
63 yr male
CML diagnosed 2003
Chronic phase
Poor response to Glivec
Sib allo PBSCT May 2006
Grade 3 mucositis
Normal renal, liver tests
Engraftment: neut D + 15
plts D + 18
Chimaerism 100% donor
BCR-ABL negative
bw021

Mr RO
61 yr male
CML diagnosed 1999
Accelerated phase 2003
Autologous PBSCT 2003 (Poole)
Co-morbid problems:
low transfer factor
poor exercise tolerance
Unrelated donor PBSCT Feb 2006
1 antigen mismatch
Grade 2/3 mucositis
Normal liver, renal function
Engraftment: plt D + 23
neuts D + 24
Chimaerism 100% donor
BCR-ABL PCR Negative
bw022

Mr AG
61 yr male
AML diagnosed 2005
Not in CR after induction
CR after salvage chemo
Unrelated donor PBSCT Apr 2006
1 antigen mismatch
Grade 2/3 mucositis
Normal liver, renal function
Engraftment: plts D + 20
neuts D + 13
Cutaneous GvHD (topical Rx)
Chimaerism: 100% D 30
bw023

Mr ML
54 yr male
Myeloma diagnosed 2004
Autologous PBSCT Sept 2005
Recurrent disease
Sibling allo PBSCT June 2006
Grade 2 mucositis
Normal liver, renal function
Engraftment: plt D + 14
neut D nr
Chimaerism 100% donor
bw024

Mr JK
22 yr male
Secondary AML diagnosed Nov 2005
HD age 10 yr
upper mantle DXT
relapse
APBSCT age 12 yr
Unrelated donor PBSCT
July 2006
Engraftment plt D +15
neut D + 16
Chimaerism 99% donor
bw025

bw026 Mr KG
55 yr male
Previous MI, x4 CABG
Secondary AML (MDS)
Sibling allo PBSCT
Aug 2006
Engraftment plt D +16
neut D +14
Chimaerism 98% donor

Mr KL
45 yr male
Relapsed MM
1 Ag mismatch VUD allo BM
21st Sept 2006
Engraftment
plt D + 12
neut D + 14
No fever
minimal mucositis
normal LFTs, renal function
Chimaerism 100% donor
bw027

Mr FH
45 yr male
Relapsed MM
Sib allo PBSCT 25.10.2006
Engraftment plt D + 14
neut D + 14
Chimaerism d + 30
- 100% donor
bw028

bw029 Mr KS
57 yr male
Relapsed AML M2
VUD (full match) allo
14.12.06
No mucositis
No fever
Engrafted
Chimaerism 98% donor

11 months4.423.3bw029
12 months4.829.6bw028
13 months9.931.0bw027
14 months4.528.1bw026
15 months3.434.5bw025
16 months10.526.8bw024
19 months10.228.3bw023
21 months5.227.9bw022
18 months4.519.5bw021
postLiverBMPatient
Phase II patients - dosimetry
6.427.7Average

Targeted R/T OSn = 13
0 12 24 36 48 600
10
20
30
40
50
60
70
80
90
100
Months
% Survival

Targeted R/T EFSn = 13
0 12 24 36 48 600
10
20
30
40
50
60
70
80
90
100
Months
% Survival

Targeted radiotherapy with anti-CD66
• Effectively delivers radiation to BM and
spleen
• Up to 35 Gy to BM
• 2-10 fold excess to BM and spleen vs other
organs
• Linear relationship between infused dose of
Y-90 and radiation dose delivered to BM
Summary

Targeted radiotherapy with anti-CD66
• Phase I dose escalation completed
- No increased toxicity
- MTD not reached
• Phase II progressing
• Multi-centre randomised phase II
Summary

Targeted radiotherapy for BMT conditioning
Southampton TheraPharm (Germany)
Nuclear Medicine Dr Maria Tristam Dr Silke Thomsen
and Med Physics Sr Louise Causer Dr Ivan Benes
John Langford
Oncology Prof Peter Johnson
Radiopharmacy James Thom Mainz Dr Ralf Meyer
Clive Jenkins Dr Wolgang Herr
Dr Andreas Helish
St Bart’s
Nuclear Medicine Dr. Maggie Cooper Acknowledgements
Prof. Grant Prentice
Prof John Goldman
USA (Arlington) Dr. Paul Borchardt
Dr. Syed Quadri
Patients participating in study
Staff of Wessex Blood and Marrow Transplantation Unit

SUHT NHS Research and Development

The future for TBI?