tavi: nuovi orizzonti · paul, mn, usa) valve and either sapien or corevalve systems; 2) salus...
TRANSCRIPT

Giuseppe De Luca, MD, PhD
Professore Associato di Cardiologia
Responsabile Laboratorio di Emodinamica
Universitario
AOU Maggiore della Carità
Novara, Italy
TAVI: Nuovi Orizzonti


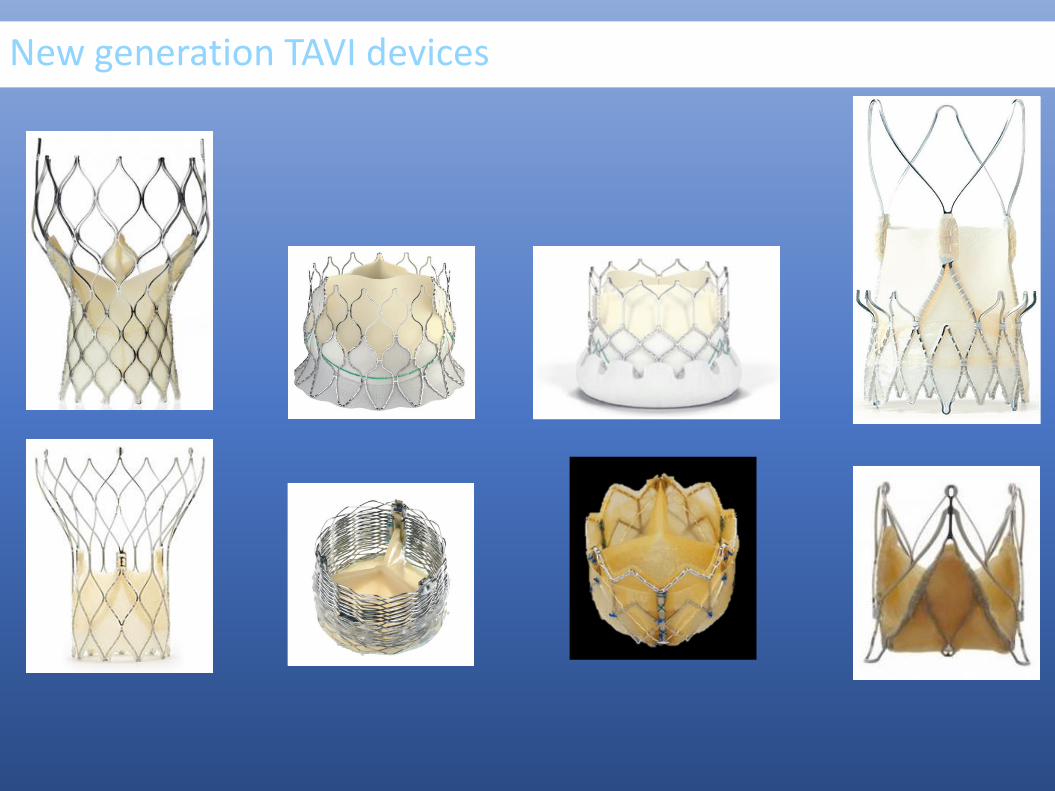
New generation TAVI devices

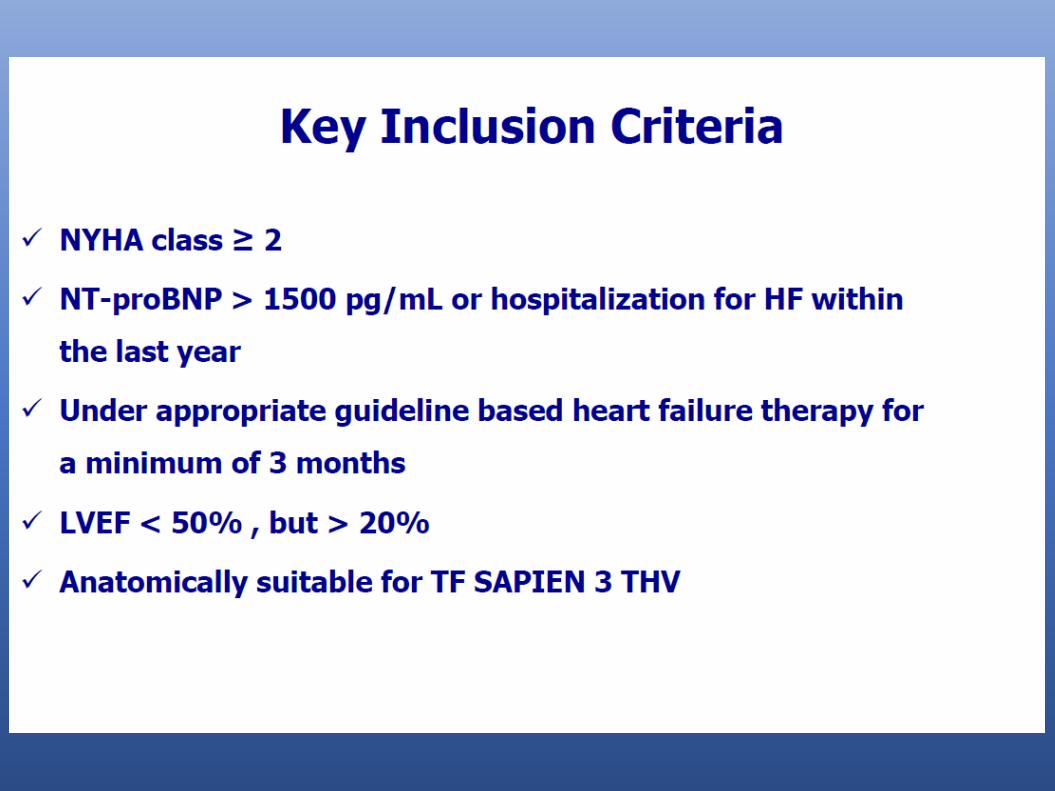
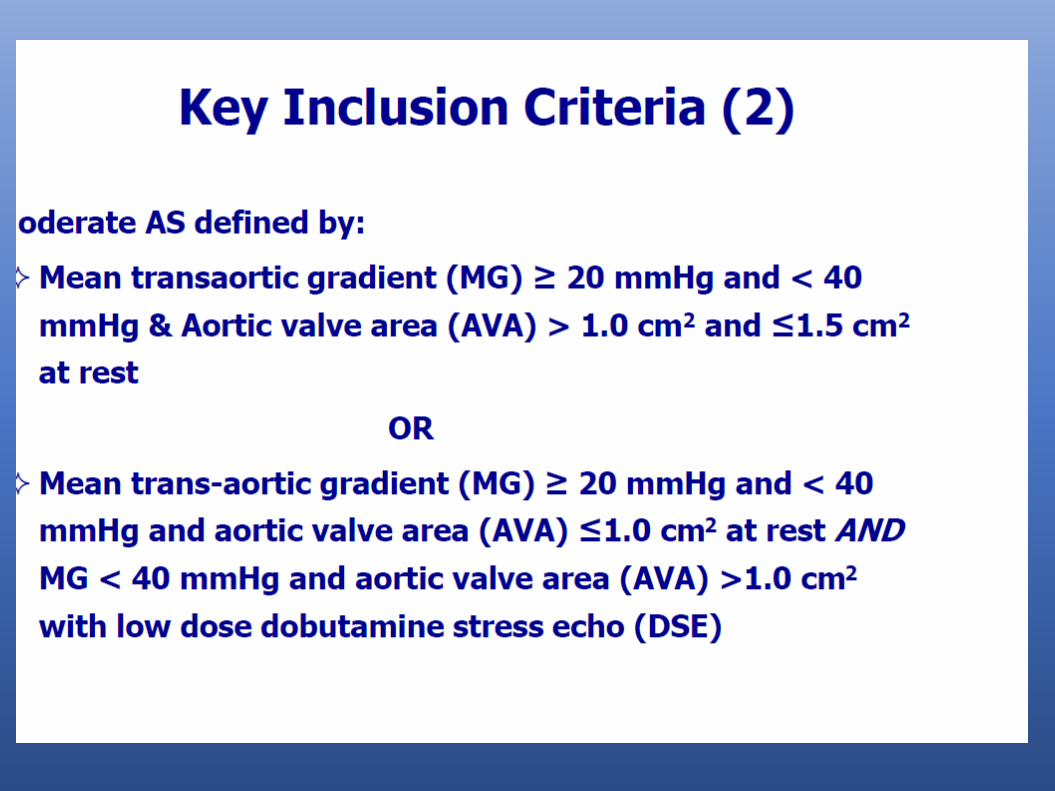
Expanding TAVI Indications: low-risk vs SurgeryMODERATE SVA WITH HEART FAILURE Asyntomatic SVALow-Flow Low GradientBicuspid valveAortic regurgitation
Comparing TAVI options
Simplifying the TAVI procedure
Stroke and CEREBROVASCULAR EMBOLIC PROTECTION
Antithrombotic therapy post-TAVI
VALVE LEAFLET INTEGRITY, THICKENING AND THROMBOSIS
TAVI: Nuovi orizzonti
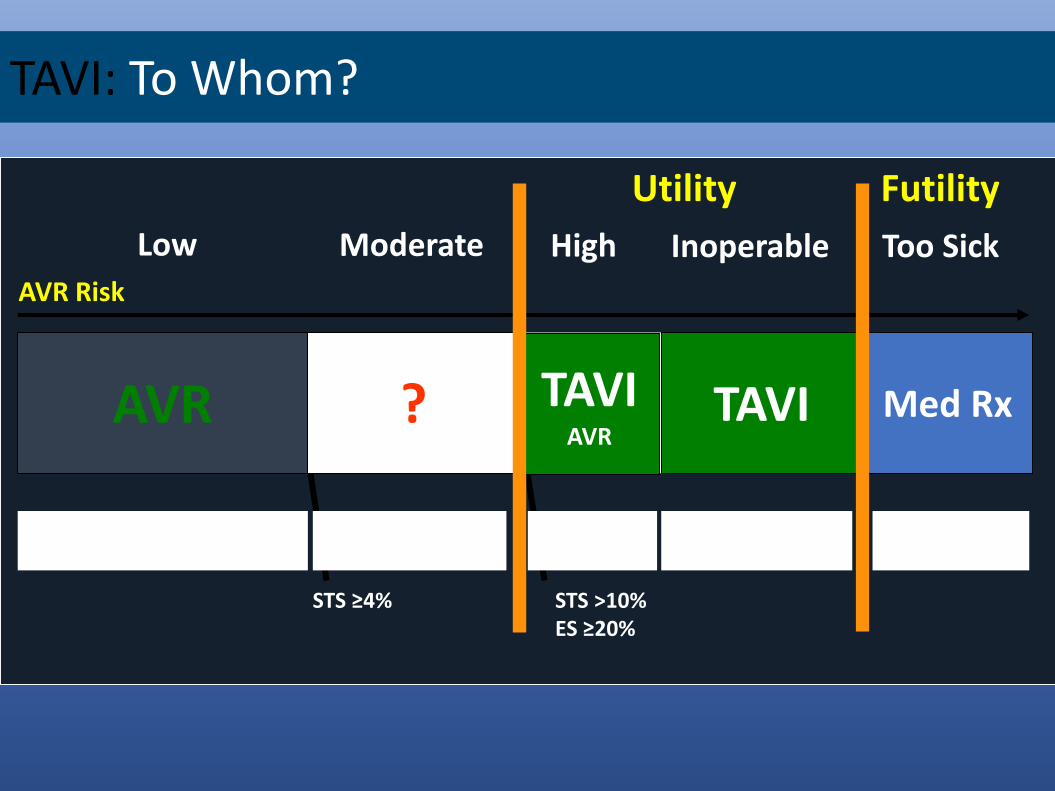
AVR Risk
Low High
TAVI Med Rx
Inoperable
Utility Futility
Too Sick
STS >10%ES ≥20%
AVR
Irrational
Moderate
?
STS ≥4%
? NoYesOK
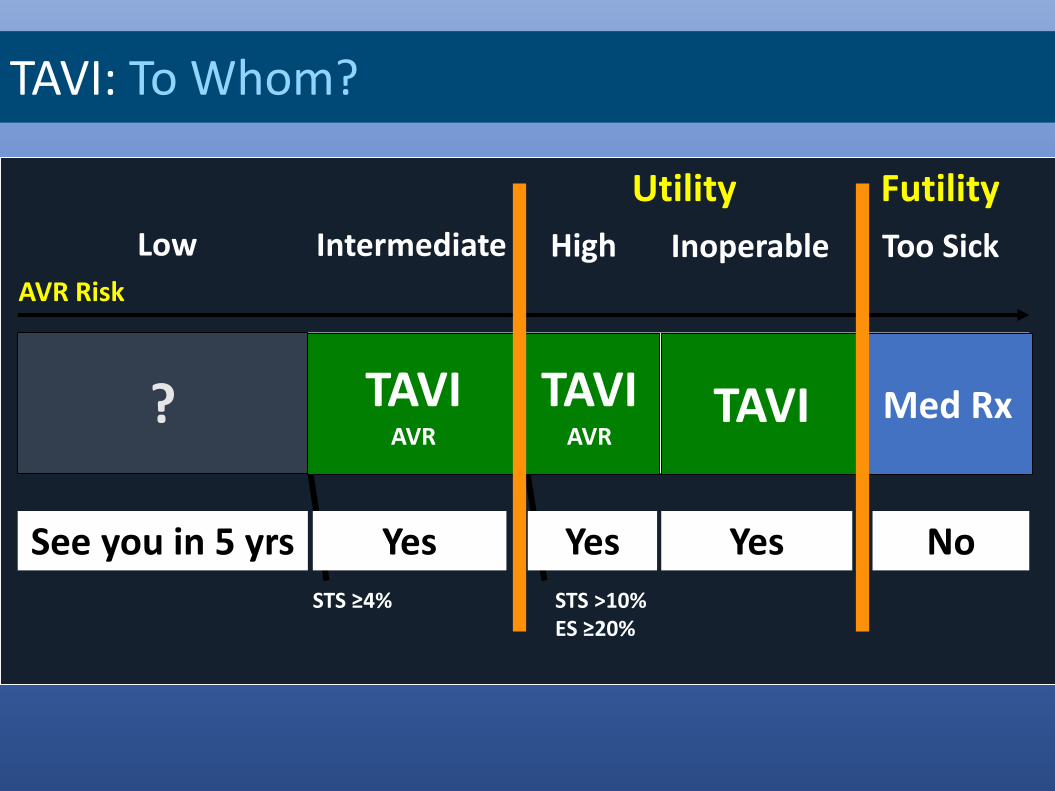
TAVI: To Whom?
TAVIAVR

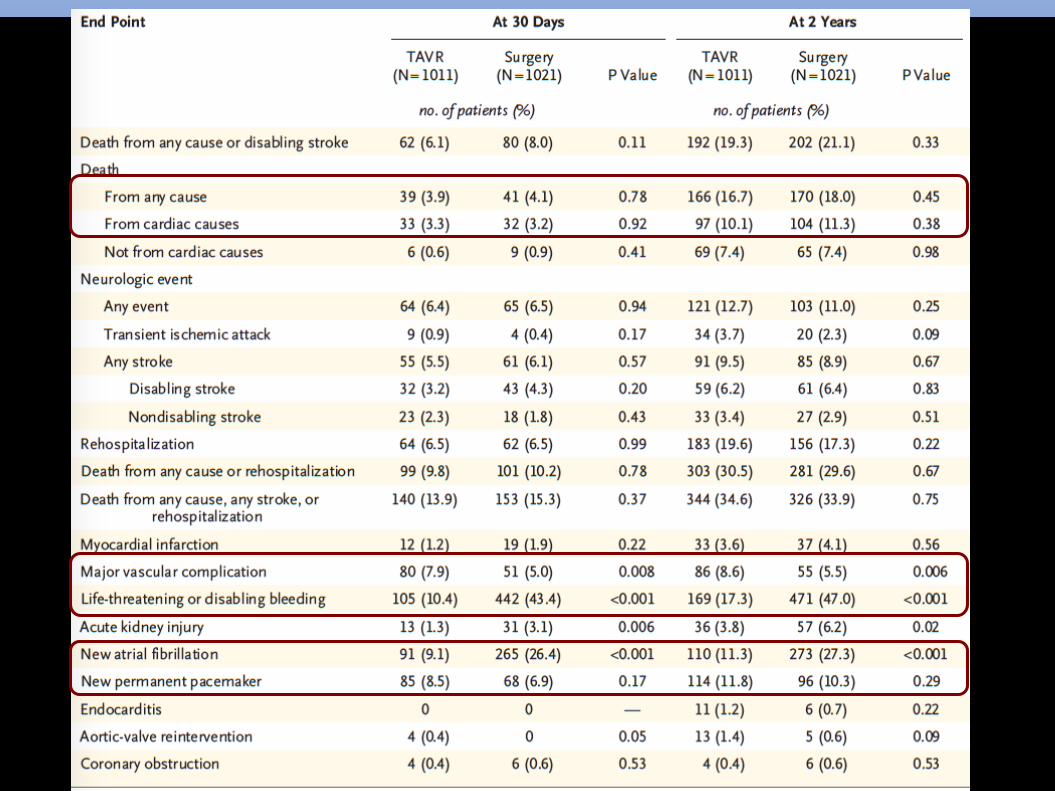
Leon MB et al, NEJM 2016
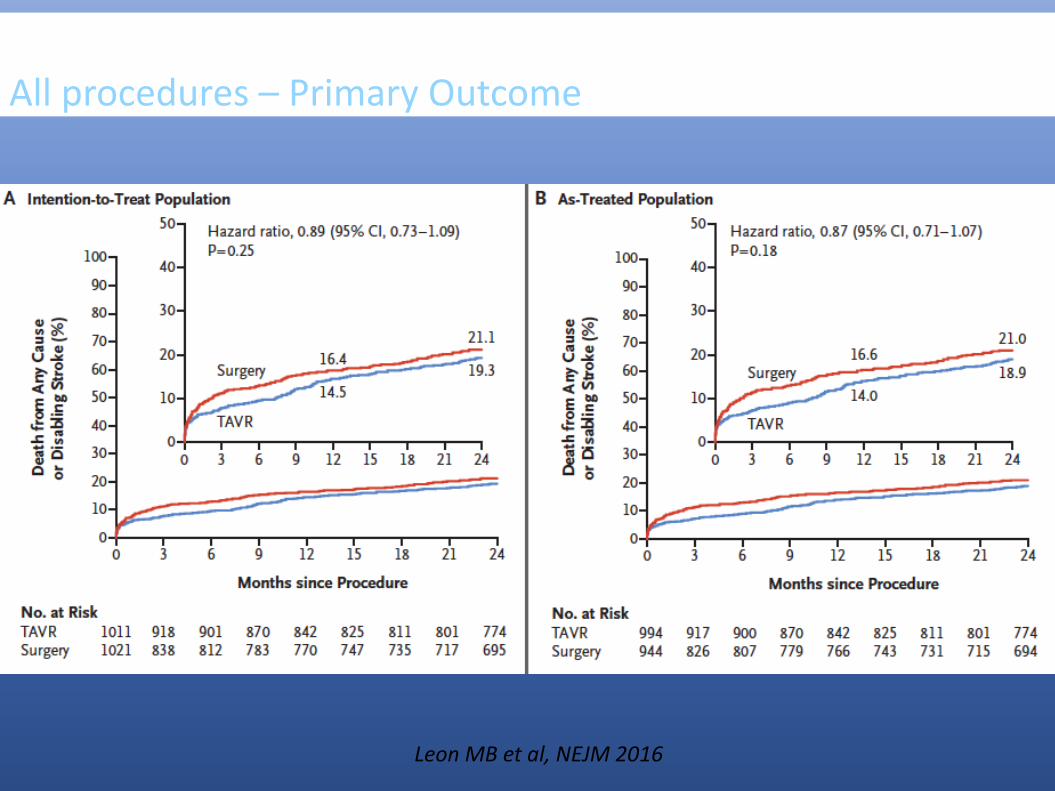
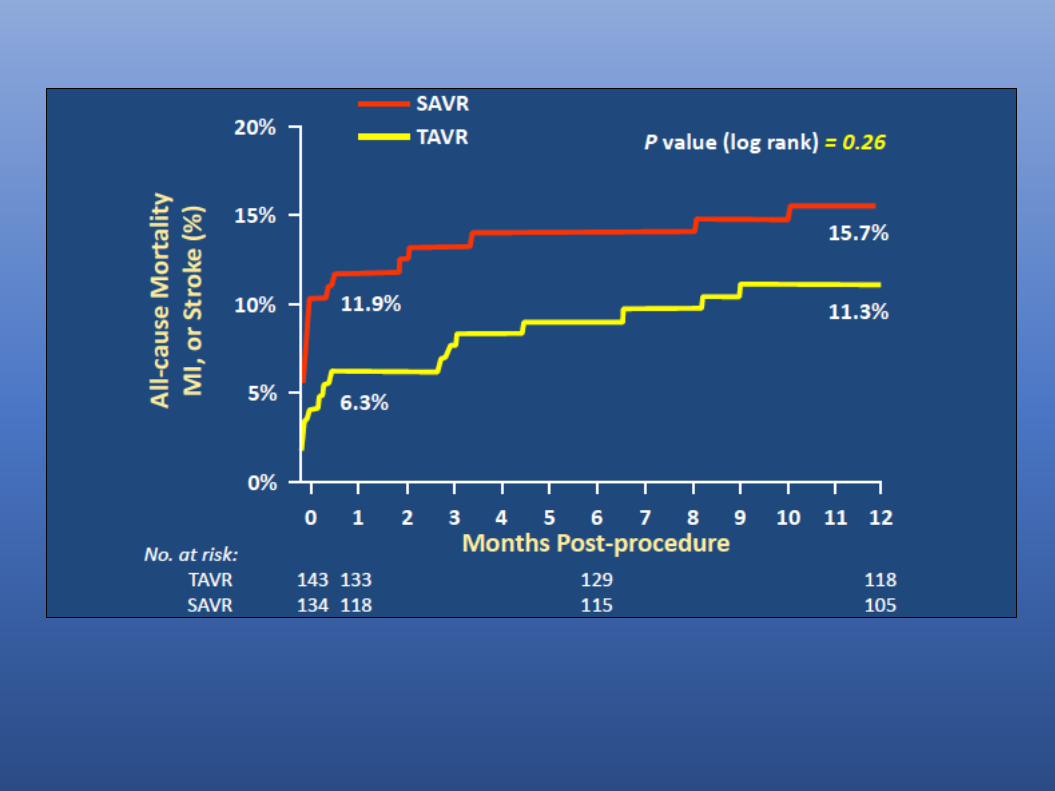
PARTNER II TrialAll procedures – Primary Outcome
Leon MB et al, NEJM 2016

PARTNER II TrialTransfemoral procedures – Primary Outcome
Leon MB et al, NEJM 2016

1746 pts

All-Cause Mortality or Disabling Stroke
SURTAVI TrialAll-Cause Mortality or Disabling Stroke at 24 Months

Thourani et al, Lancet 2016
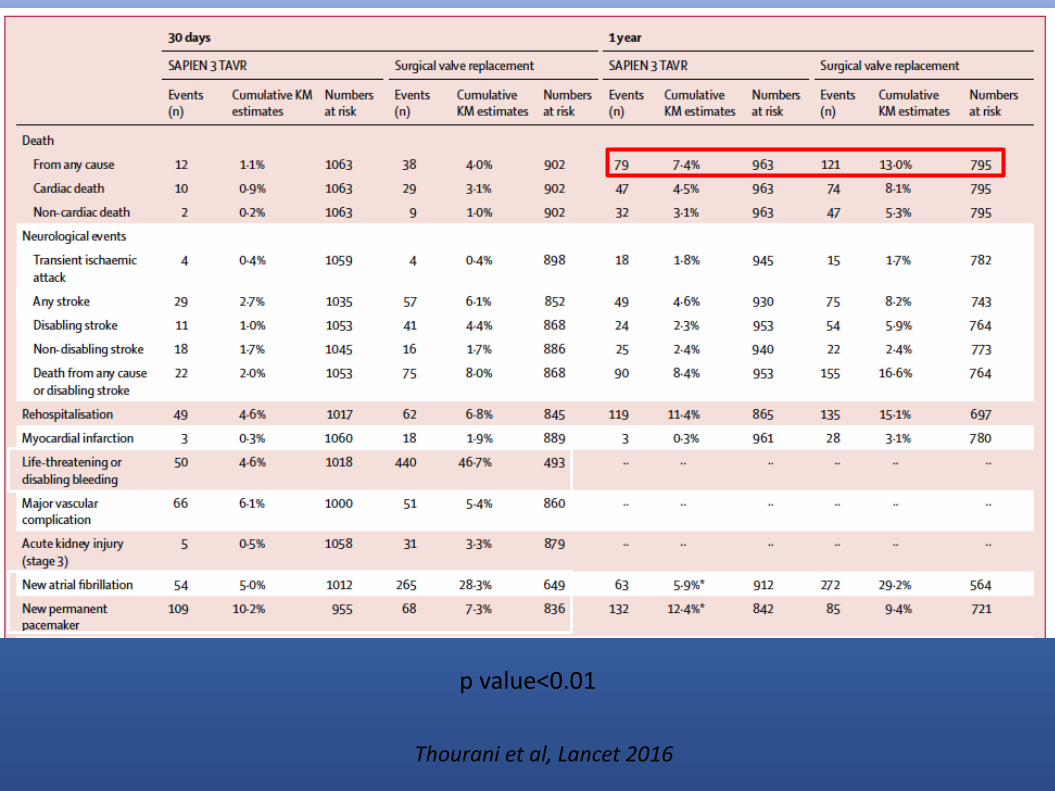
p value<0.01
Thourani et al, Lancet 2016

AVR Risk
Low High
TAVI Med Rx
Inoperable
Utility Futility
Too Sick
STS >10%ES ≥20%
AVR
Irrational
Intermediate
STS ≥4%
OK NoYesYes
TAVI: To Whom?
TAVI or AVR TAVIAVR
AVR Risk
Low High
TAVI Med Rx
Inoperable
Utility Futility
Too Sick
STS >10%ES ≥20%
?
See you in 5 yrs
Intermediate
STS ≥4%
Yes NoYesYes
TAVI: To Whom?
TAVIAVR
TAVIAVR



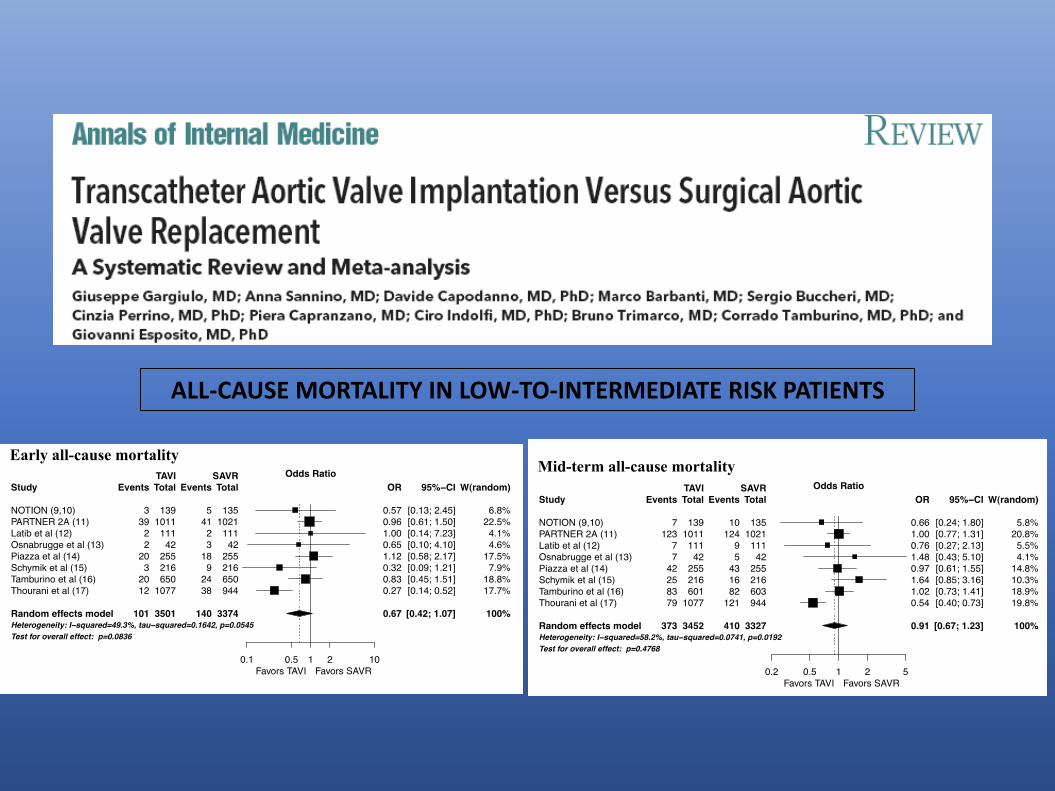
ALL-CAUSE MORTALITY IN LOW-TO-INTERMEDIATE RISK PATIENTS


EARLY TAVR Trial
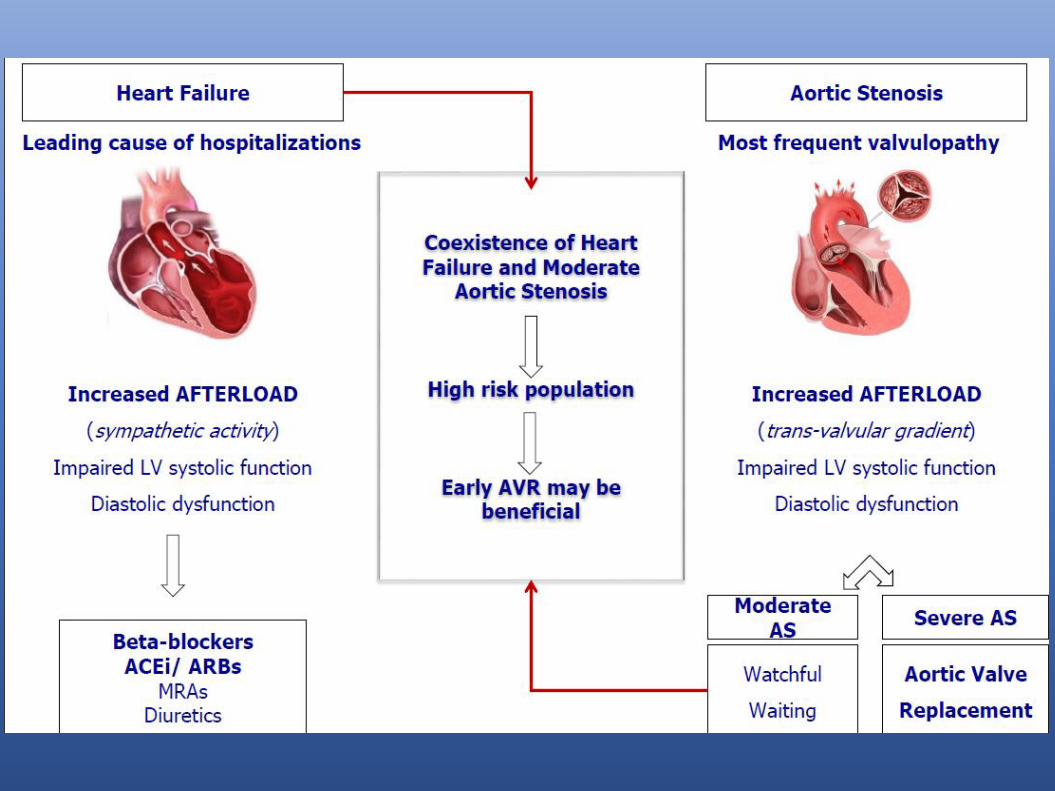
TAVR UNLOAD Trial
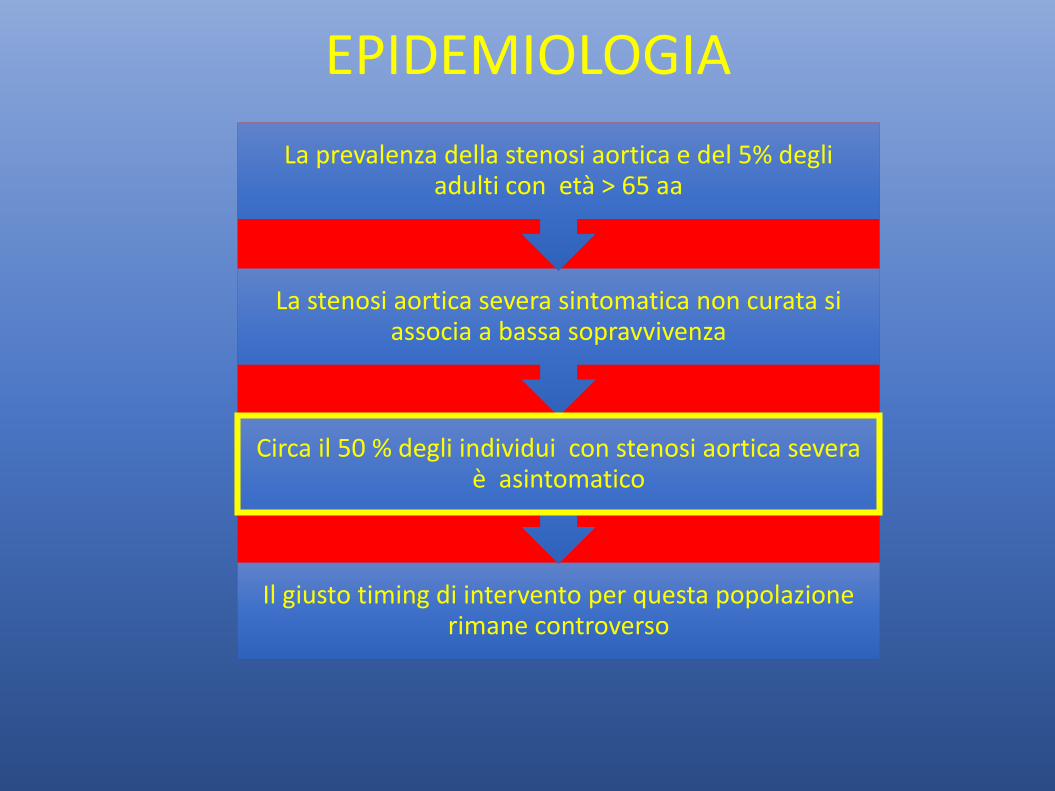
EPIDEMIOLOGIA
Il giusto timing di intervento per questa popolazione rimane controverso
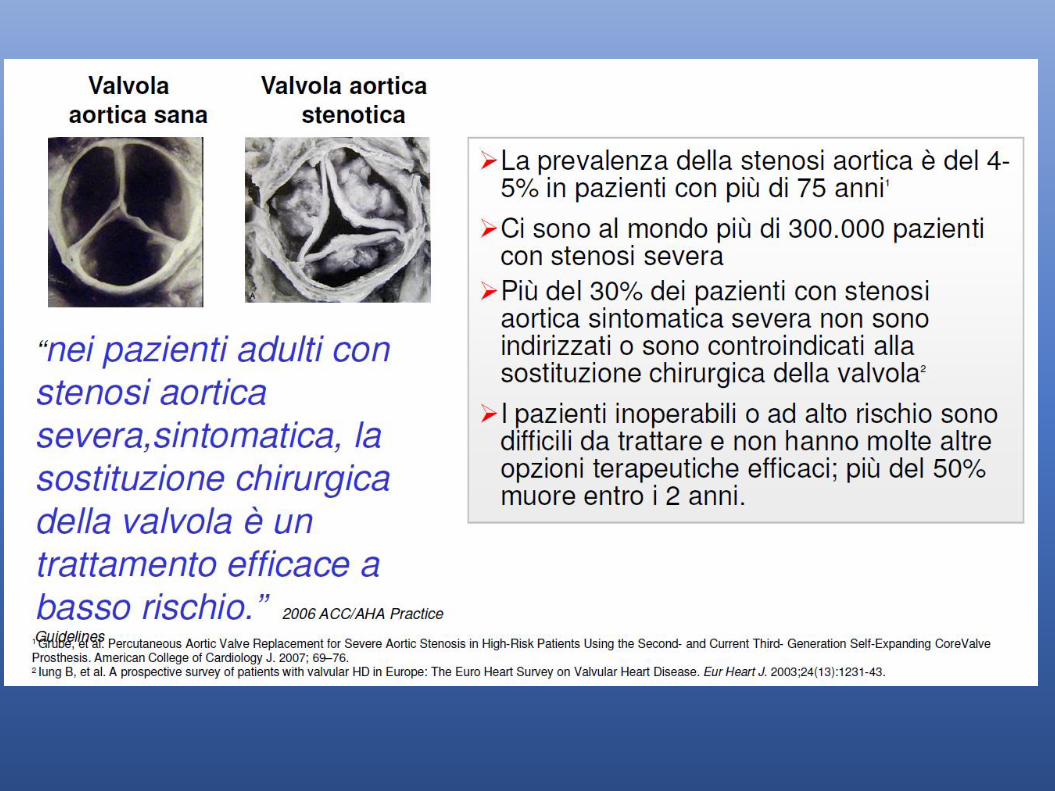
Circa il 50 % degli individui con stenosi aortica severa è asintomatico
La stenosi aortica severa sintomatica non curata si associa a bassa sopravvivenza
La prevalenza della stenosi aortica e del 5% degli adulti con età > 65 aa

STORIA NATURALE DELLA STENOSI AORTICA ASINTOMATICA
Registro di Taniguchi et al.- 1.517 pazienti trattati conservativamente con AS asintomatica i tassi di sopravvivenza ad 1 anno e 5 anni sono del 92,8% e 73,6% rispettivamente
Nei pazienti con stenosi artica asintomatica grave, la sopravvivenza ad 1 anno e 5 anni riportata in letteratura oscilla dal 67% al 97%(1 aa) e dal 38% al 83%(2 aa)
A 5 anni circa il 75% dei pazienti diventa sintomatico 75% di questi morirà o farà la AVR/ TAVI
I pazienti asintomatici hanno una prognosi migliore rispetto a quelli sintomatici
Rischio di morte improvvisa 1-1,5% anno


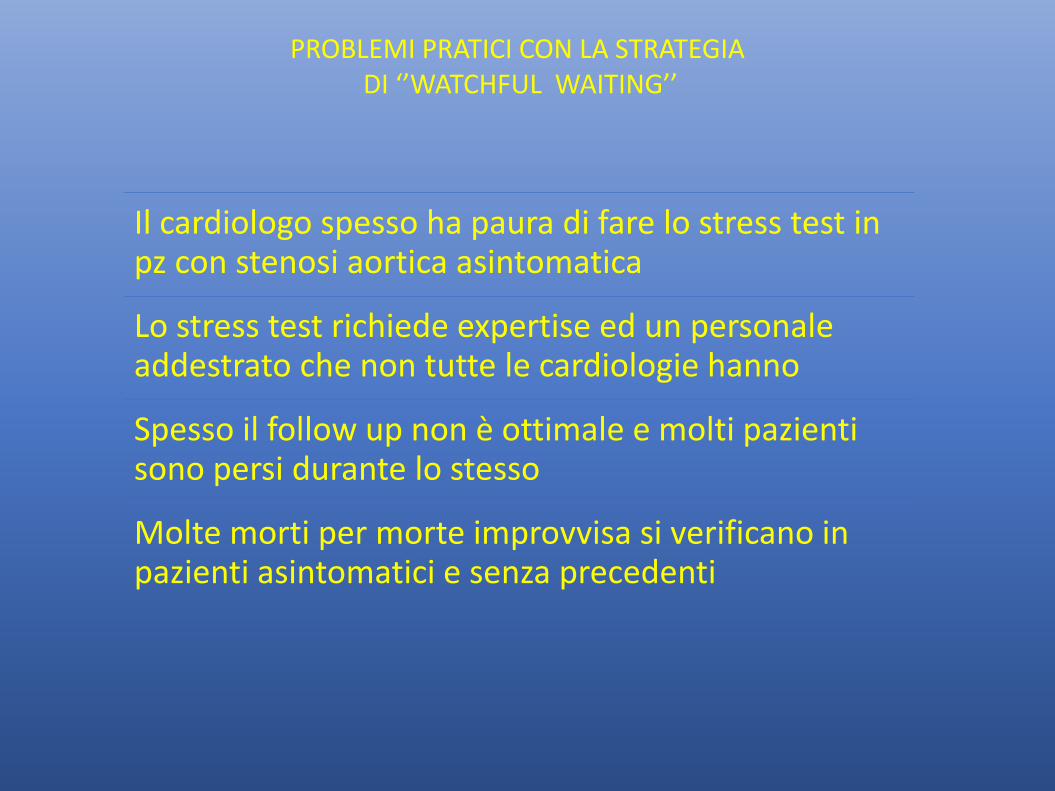
PROBLEMI PRATICI CON LA STRATEGIA DI ‘’WATCHFUL WAITING’’
Il cardiologo spesso ha paura di fare lo stress test in pz con stenosi aortica asintomatica
Lo stress test richiede expertise ed un personale addestrato che non tutte le cardiologie hanno
Spesso il follow up non è ottimale e molti pazienti sono persi durante lo stesso
Molte morti per morte improvvisa si verificano in pazienti asintomatici e senza precedenti

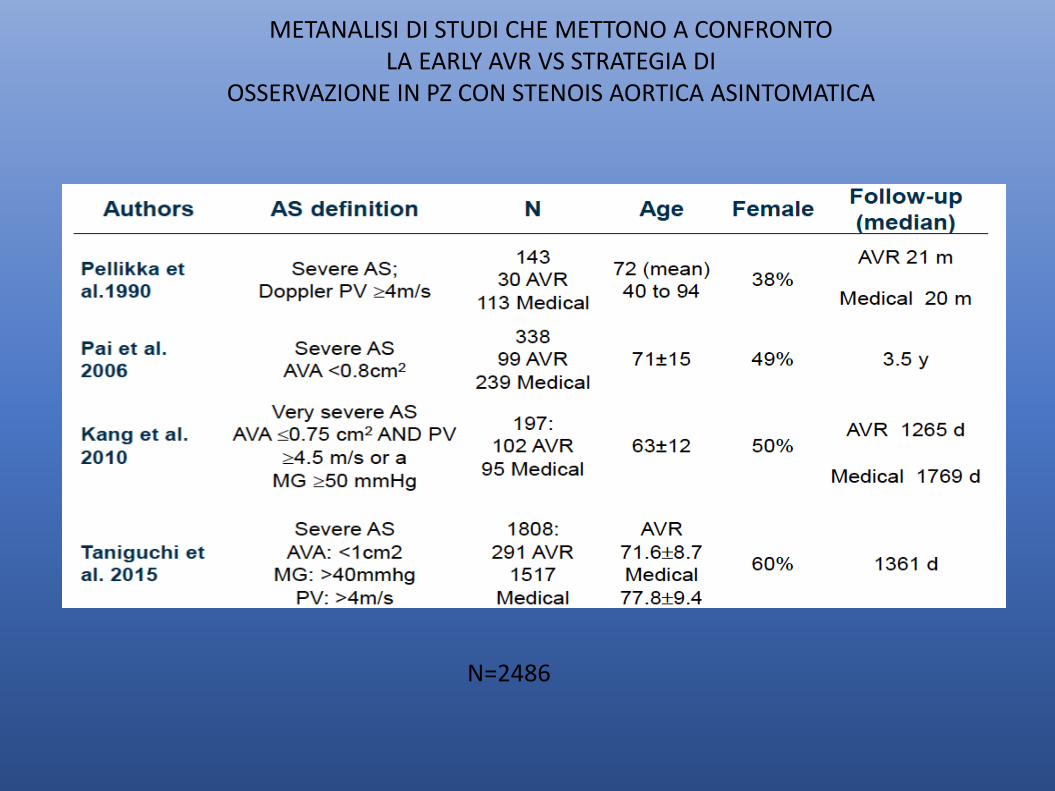
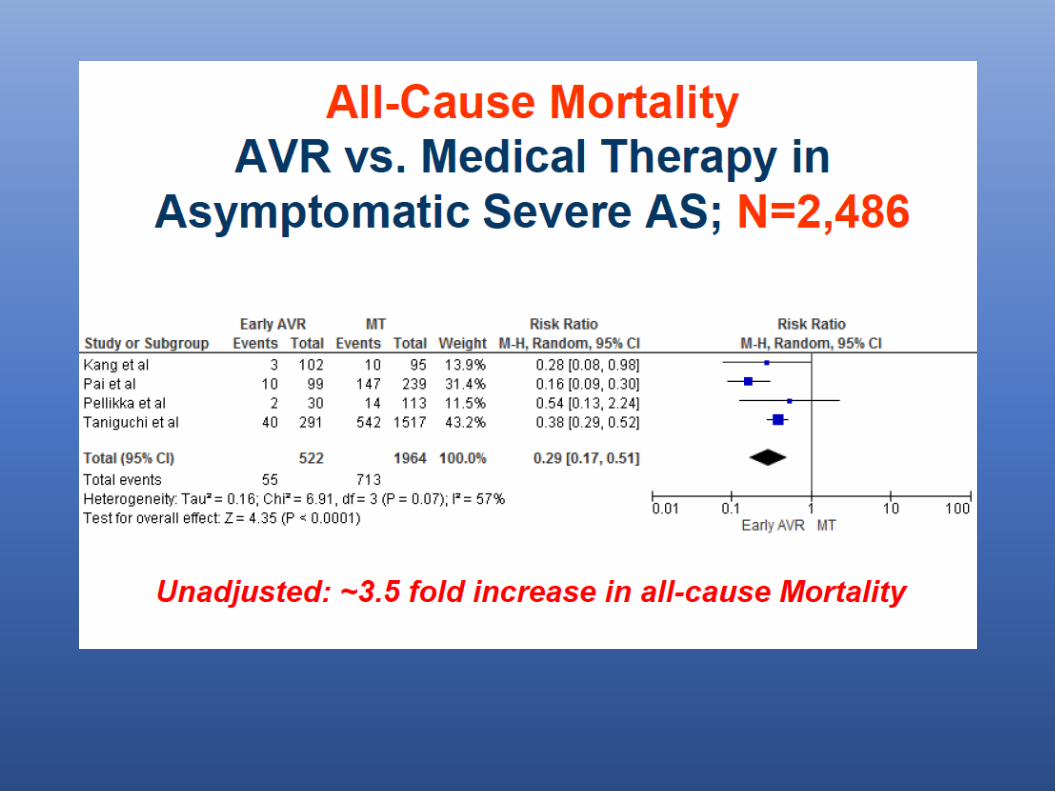
N=2486
METANALISI DI STUDI CHE METTONO A CONFRONTOLA EARLY AVR VS STRATEGIA DI
OSSERVAZIONE IN PZ CON STENOIS AORTICA ASINTOMATICA


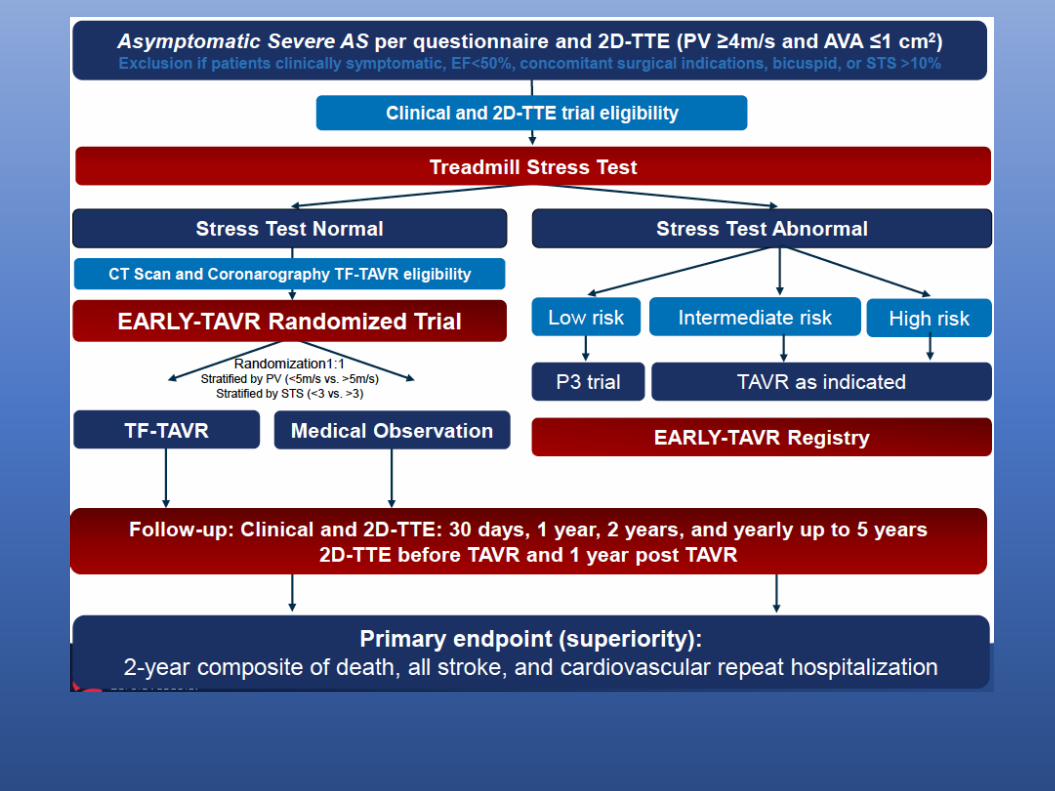
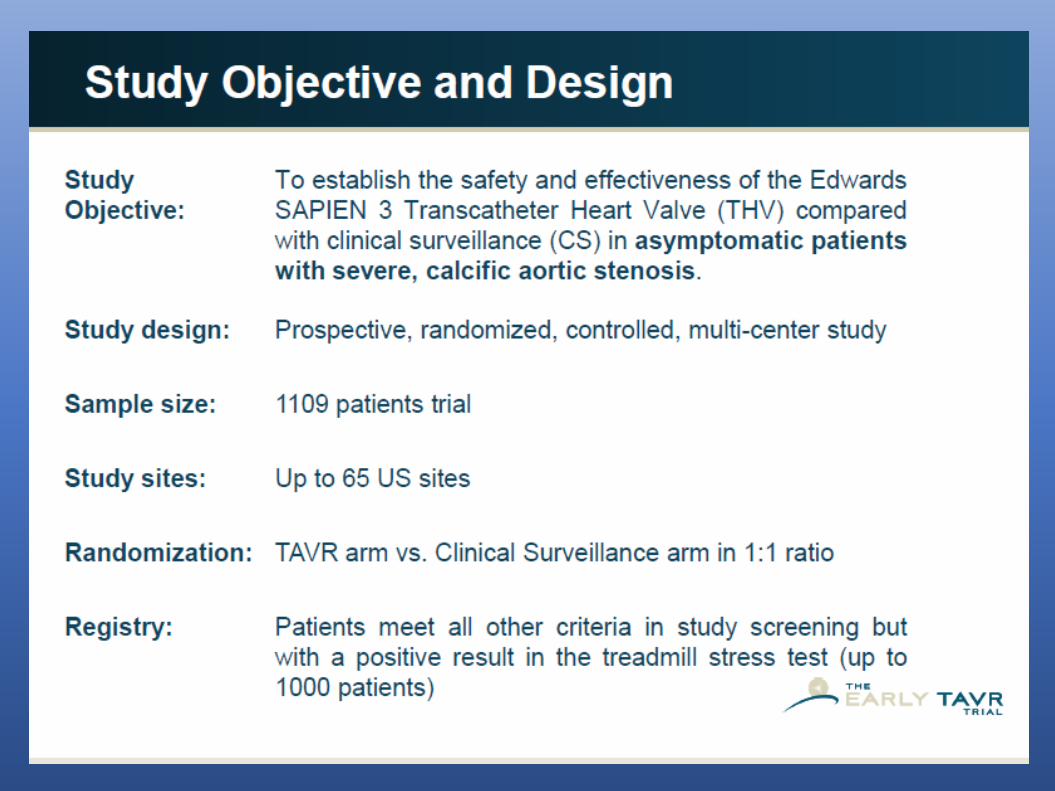


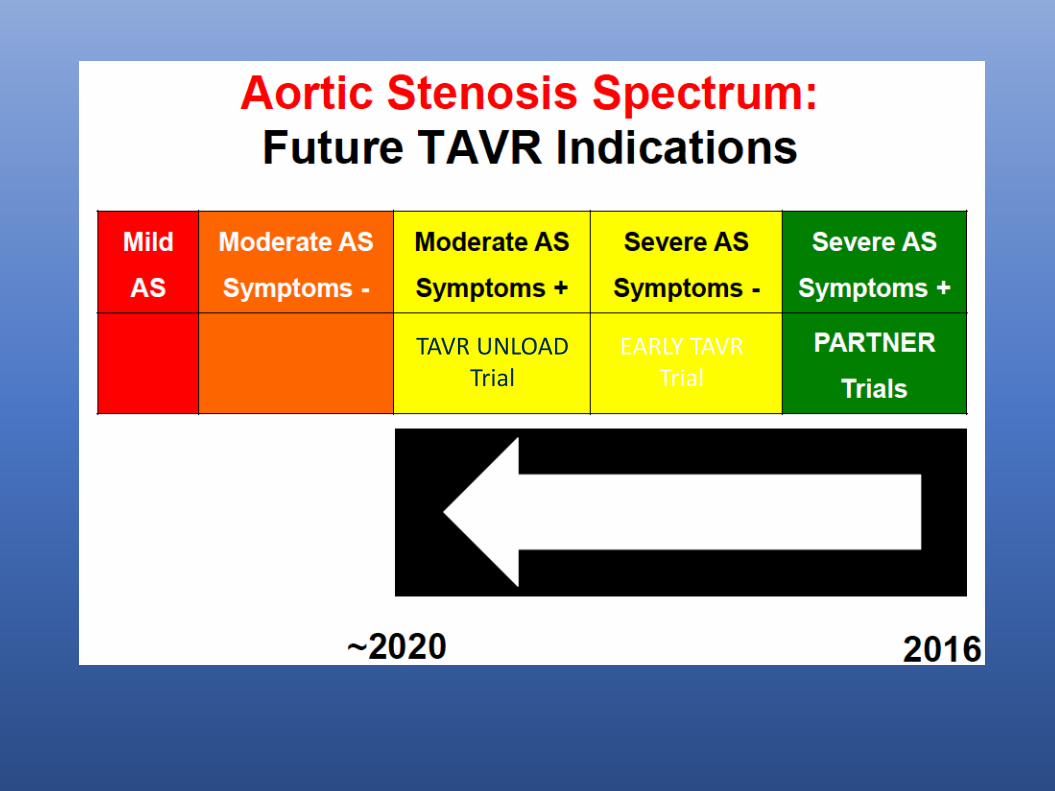
EARLY TAVR Trial
TAVR UNLOAD Trial




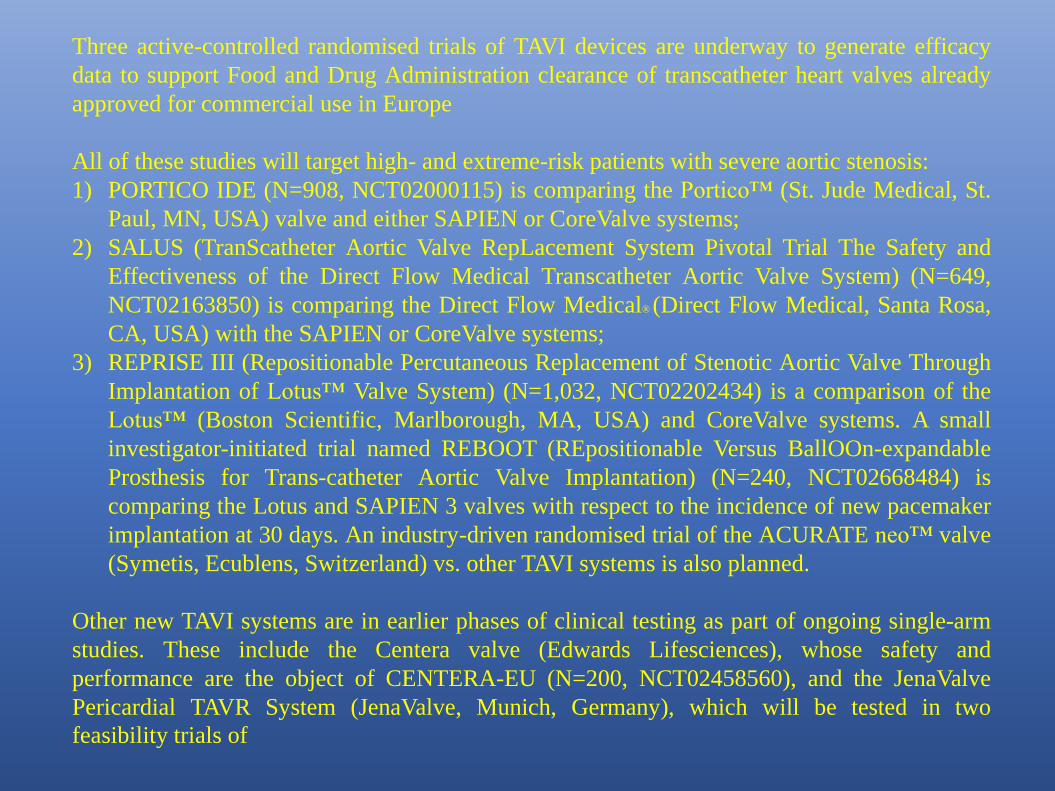
Three active-controlled randomised trials of TAVI devices are underway to generate efficacy
data to support Food and Drug Administration clearance of transcatheter heart valves already
approved for commercial use in Europe
All of these studies will target high- and extreme-risk patients with severe aortic stenosis:
1) PORTICO IDE (N=908, NCT02000115) is comparing the Portico™ (St. Jude Medical, St.
Paul, MN, USA) valve and either SAPIEN or CoreValve systems;
2) SALUS (TranScatheter Aortic Valve RepLacement System Pivotal Trial The Safety and
Effectiveness of the Direct Flow Medical Transcatheter Aortic Valve System) (N=649,
NCT02163850) is comparing the Direct Flow Medical® (Direct Flow Medical, Santa Rosa,
CA, USA) with the SAPIEN or CoreValve systems;
3) REPRISE III (Repositionable Percutaneous Replacement of Stenotic Aortic Valve Through
Implantation of Lotus™ Valve System) (N=1,032, NCT02202434) is a comparison of the
Lotus™ (Boston Scientific, Marlborough, MA, USA) and CoreValve systems. A small
investigator-initiated trial named REBOOT (REpositionable Versus BallOOn-expandable
Prosthesis for Trans-catheter Aortic Valve Implantation) (N=240, NCT02668484) is
comparing the Lotus and SAPIEN 3 valves with respect to the incidence of new pacemaker
implantation at 30 days. An industry-driven randomised trial of the ACURATE neo™ valve
(Symetis, Ecublens, Switzerland) vs. other TAVI systems is also planned.
Other new TAVI systems are in earlier phases of clinical testing as part of ongoing single-arm
studies. These include the Centera valve (Edwards Lifesciences), whose safety and
performance are the object of CENTERA-EU (N=200, NCT02458560), and the JenaValve
Pericardial TAVR System (JenaValve, Munich, Germany), which will be tested in two
feasibility trials of


CONCLUSIONSTAVI has revolutioned the management of aortic stenosis
TAVI has replaced Surgery in high and intermediate risk patients.
Several studies are ongoing to further expand the indication to low-riskpatients, asyntomatic patients and those with moderate SVA and Leftventricular dysfunction. Additonal studies are certainly needed inthose LFLG
The evolving technology will certainly contribute to simplify theproceudre, reduce complications, increase durability and enlarge theindication.
While the availability of several valves will facilitate a tailoredapproach, large randomized trials are certainly needed to define asuperiority of a valve over the others.


