tavr - carondelethealth.carondelet.org/chviconference/ram.pdf · tavr 179 115 100 89 77 64 49 179...
TRANSCRIPT
9/16/2014
1
PERCUTANEOUS STRUCTURAL UPDATES
• TAVR
• WATCHMAN(LEFT ATRIAL APPENDAGE OCCLUDERS)
• MITRACLIP
• PARAVALVULAR LEAK REPAIRS
• ASD/PFO CLOSURES
• VALVULOPLASTIES
Dr.Vinny K.Ram No disclosures
TAVR
9/16/2014
2
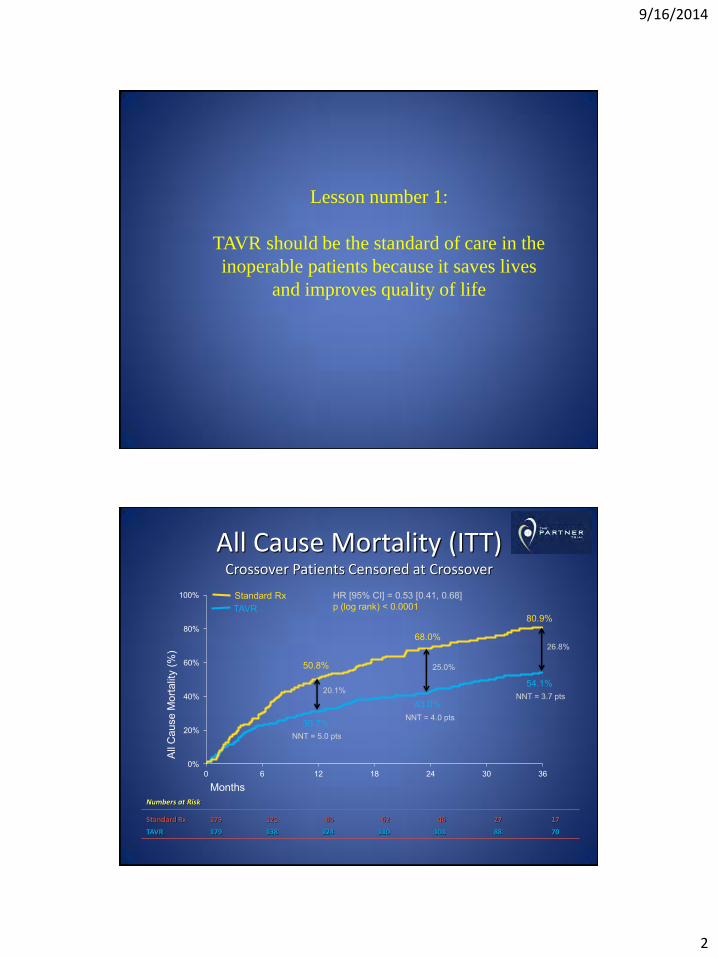
Lesson number 1:
TAVR should be the standard of care in the
inoperable patients because it saves lives
and improves quality of life
0%
20%
40%
60%
80%
100%
0 6 12 18 24 30 36
Numbers at Risk
Standard Rx 179 121 85 62 46 27 17
TAVR 179 138 124 110 101 88 70
All Cause Mortality (ITT) Crossover Patients Censored at Crossover
30.7%
50.8%
43.0%
68.0%
54.1%
80.9%
All
Cau
se M
orta
lity
(%)
Months
HR [95% CI] = 0.53 [0.41, 0.68] p (log rank) < 0.0001
20.1%
25.0%
26.8%
NNT = 5.0 pts
NNT = 4.0 pts
NNT = 3.7 pts
Standard Rx TAVR
9/16/2014
3
0%
20%
40%
60%
80%
100%
0 6 12 18 24 30 360%
20%
40%
60%
80%
100%
0 6 12 18 24 30 36
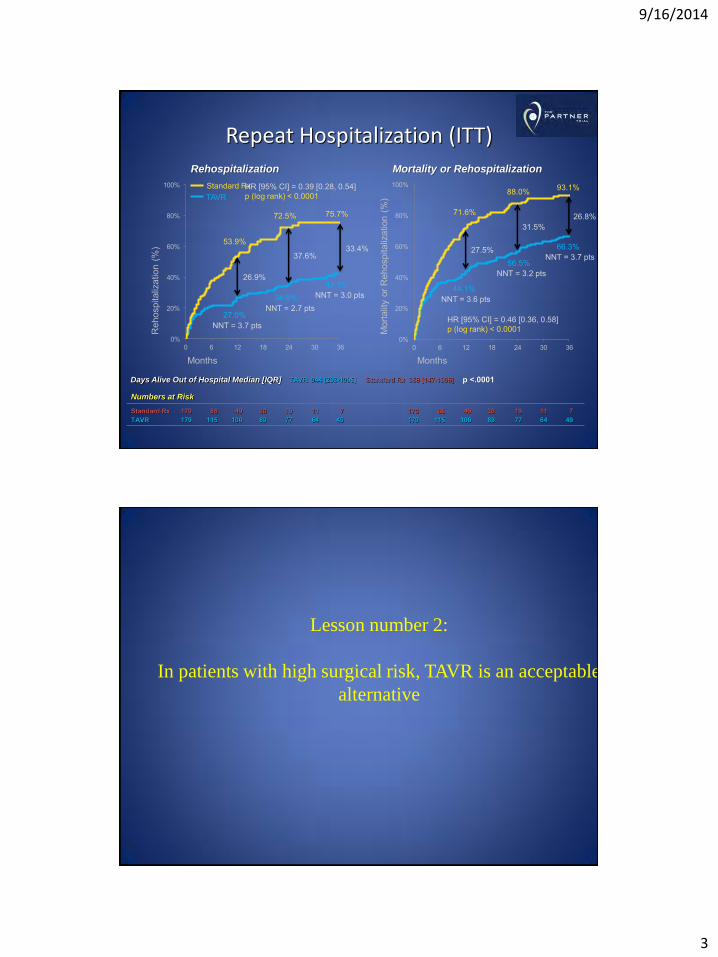
Repeat Hospitalization (ITT)
53.9%
27.0%
72.5%
34.9%
75.7%
42.3%
71.6%
44.1%
88.0%
56.5%
93.1%
66.3%
Numbers at Risk
Standard Rx 179 86 49 30 19 11 7 179 86 49 30 19 11 7 TAVR 179 115 100 89 77 64 49 179 115 100 89 77 64 49
Months Months
Reh
ospi
taliz
atio
n (%
)
Mor
talit
y or
Reh
ospi
taliz
atio
n (%
)
Rehospitalization Mortality or Rehospitalization
Standard Rx TAVR
33.4%
HR [95% CI] = 0.39 [0.28, 0.54] p (log rank) < 0.0001
NNT = 3.7 pts
NNT = 2.7 pts NNT = 3.0 pts NNT = 3.6 pts
NNT = 3.2 pts
NNT = 3.7 pts 37.6%
26.9%
26.8% 31.5%
27.5%
HR [95% CI] = 0.46 [0.36, 0.58] p (log rank) < 0.0001
TAVR 944 [233-1096] Standard Rx 368 [147-1096] p <.0001 Days Alive Out of Hospital Median [IQR]
Lesson number 2:
In patients with high surgical risk, TAVR is an acceptable
alternative

9/16/2014
4
TAVR 348 298 261 239 222 187 149
AVR 351 252 236 223 202 174 142
All-Cause Mortality (ITT)
No. at Risk
HR [95% CI] = 0.93 [0.74, 1.15] p (log rank) = 0.483
26.8%
24.3%
34.6%
33.7%
44.8%
44.2%
Lesson number 3
TAVR is associated with early stroke hazard
9/16/2014
5
0%
10%
20%
30%
40%
50%
0 6 12 18 24 30 36
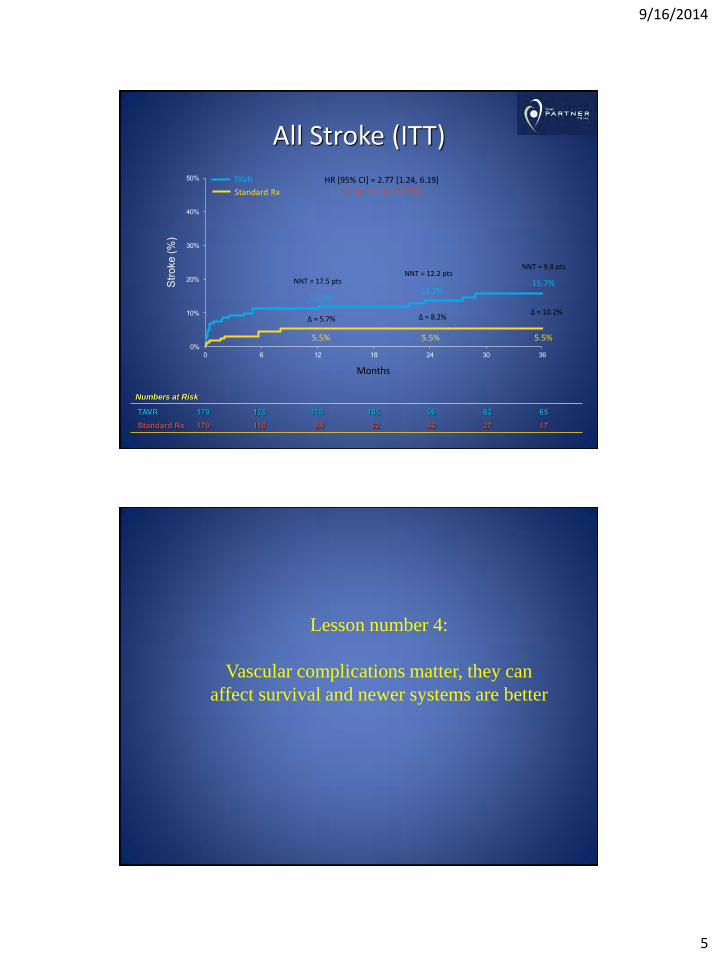
All Stroke (ITT)
5.5%
11.2%
5.5%
13.7%
5.5%
15.7% Stro
ke (%
)
Months
HR [95% CI] = 2.77 [1.24, 6.19] p (log rank) = 0.0094
∆ = 5.7%
NNT = 17.5 pts NNT = 12.2 pts
NNT = 9.8 pts
∆ = 8.2% ∆ = 10.2%
Standard Rx
TAVR
Numbers at Risk
TAVR 179 128 116 105 96 82 65 Standard Rx 179 118 84 62 46 27 17
Lesson number 4:
Vascular complications matter, they can
affect survival and newer systems are better
9/16/2014
6
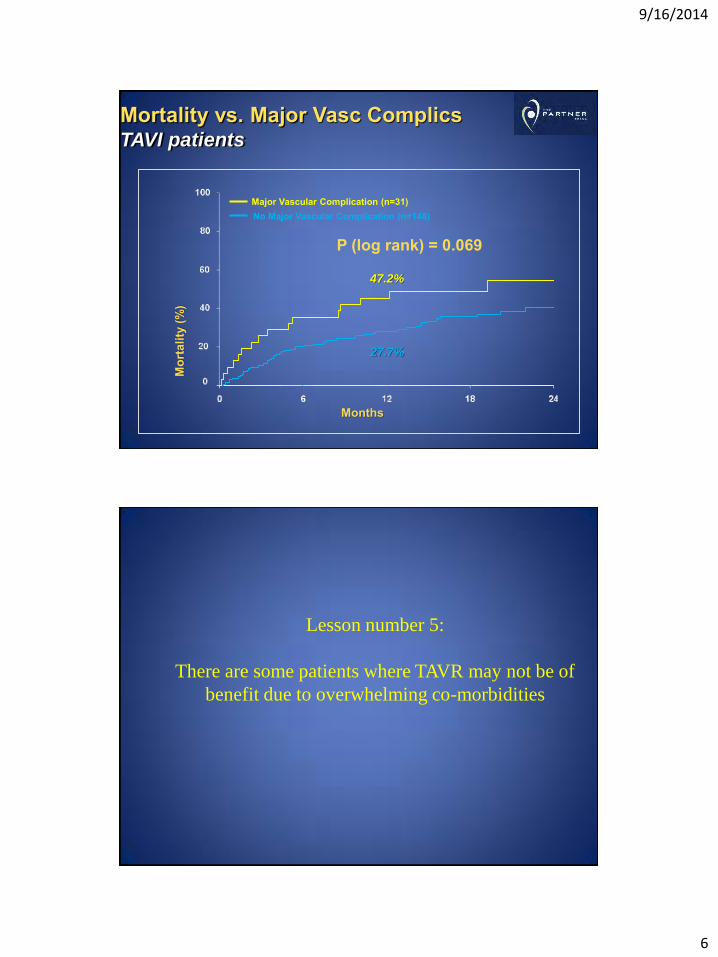
P (log rank) = 0.069
Major Vascular Complication (n=31) No Major Vascular Complication (n=148)
Mor
talit
y (%
)
Months
Mortality vs. Major Vasc Complics TAVI patients
27.7%
47.2%
Lesson number 5:
There are some patients where TAVR may not be of
benefit due to overwhelming co-morbidities
9/16/2014
7
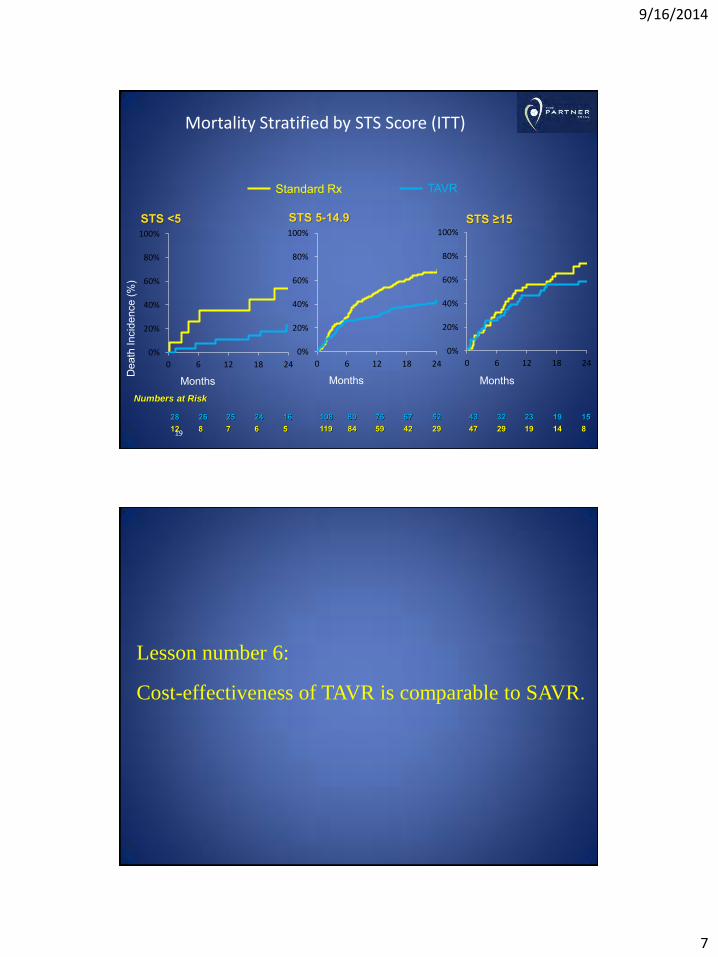
Dea
th In
cide
nce
(%)
Months
0%
20%
40%
60%
80%
100%
0 6 12 18 24
STS 5-14.9
Numbers at Risk
STS <5
Months
0%
20%
40%
60%
80%
100%
0 6 12 18 24
28 26 25 24 16 12 8 7 6 5
Standard Rx TAVR
STS ≥15
0%
20%
40%
60%
80%
100%
0 6 12 18 24
Months
43 32 23 19 15 47 29 19 14 8
108 80 76 67 52 119 84 59 42 29
Mortality Stratified by STS Score (ITT)
19
Lesson number 6: Cost-effectiveness of TAVR is comparable to SAVR.
9/16/2014
8
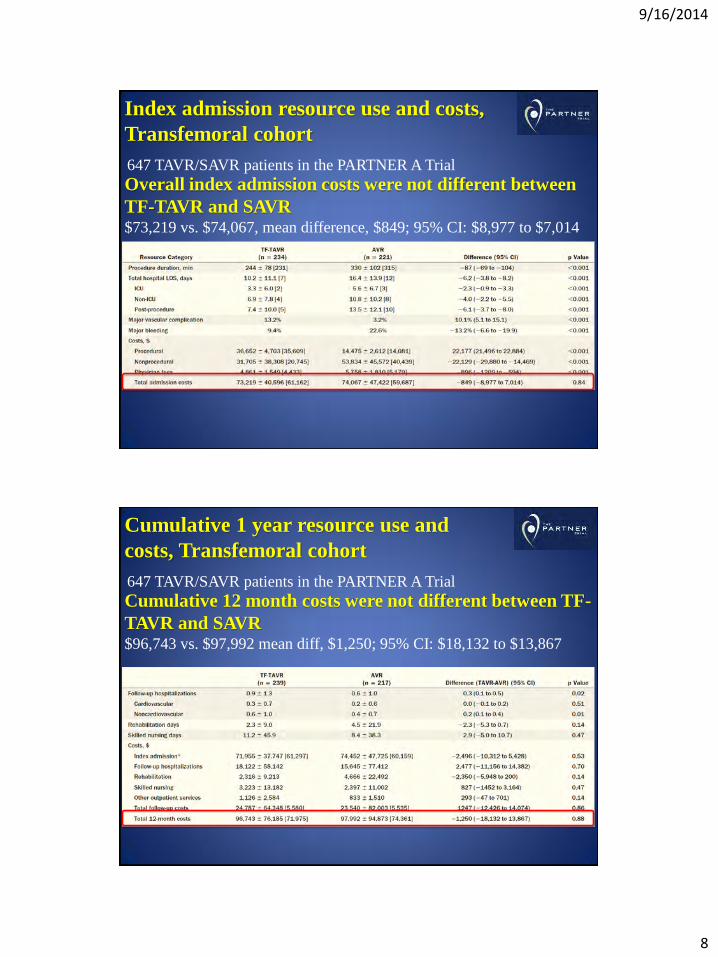
Index admission resource use and costs,
Transfemoral cohort
647 TAVR/SAVR patients in the PARTNER A Trial
Overall index admission costs were not different between
TF-TAVR and SAVR $73,219 vs. $74,067, mean difference, $849; 95% CI: $8,977 to $7,014
Cumulative 1 year resource use and
costs, Transfemoral cohort
647 TAVR/SAVR patients in the PARTNER A Trial
Cumulative 12 month costs were not different between TF-
TAVR and SAVR $96,743 vs. $97,992 mean diff, $1,250; 95% CI: $18,132 to $13,867
9/16/2014
9
Lessons from the PARTNER Trial
1. Outcomes in Inoperable patients
2. Outcomes in high risk patients
3. Complications • Stroke
• Vascular complications
• Aortic regurgitation
4. Hemodynamics
5. Futility
6. Learning curve
7. Risk scores
8. Sapien XT/Novaflex
9. Cost effectiveness
LEFT ATRIAL APPENDAGE OCCLUDERS
1)People with AF have 5 times the risk of stroke compared to people without AF⁸ 2)Stroke is more severe for patients with AF, as they have a 70% chance of death or permanent disability⁹ AF-associated ischemic strokes generally occlude large intracranial arteries depriving a more extensive region of the brain of blood flow⁸ 3)Compared with non-AF patients, AF patients have poorer survival and more recurrences of stroke during the first year of follow-up⁷ 4)Relative or absolute contraindications to long-term anticoagulation are present in up to 40% of AF patients, usually due to a history of bleeding or an elevated risk of falls and trauma. In fact, anticoagulation is not currently utilized in up to 50% of eligible AF patients 5)The economic burden of stroke will continue to rise globally as the incidence of stroke increases⁴ 6)91% of stroke in AF is caused by thrombus formed in the LAA⁵
8-Holmes DR. Seminars in Neurology. 2010;30:528–536 9-Tu HT et al, Cerebrovascular Disease. 2010;30(4):389-95 7-Patel et al, Cardiol Res Pract. 2012; 2012: 610827 4Klein A et al, Datamonitor. July 2011 5Blackshear JL, Odell JA, Ann of Thor Surgery , 1996;61:755-759
Caution: In the United States, WATCHMAN is an investigational device limited by Federal law and investigational use only. Not for sale in the US. Prior to use please review device indications, contraindications, warnings, precautions, adverse events, and operational instructions. Only available according to applicable local law. CE Mark received in 2005
9/16/2014
10
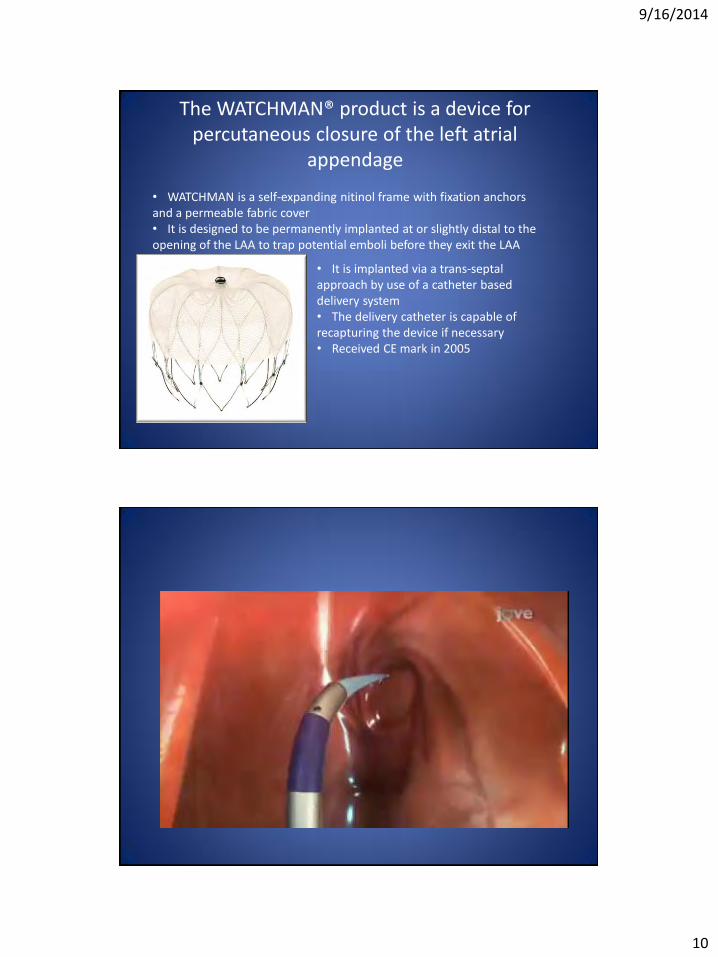
The WATCHMAN® product is a device for percutaneous closure of the left atrial
appendage
• WATCHMAN is a self-expanding nitinol frame with fixation anchors and a permeable fabric cover • It is designed to be permanently implanted at or slightly distal to the opening of the LAA to trap potential emboli before they exit the LAA
• It is implanted via a trans-septal approach by use of a catheter based delivery system • The delivery catheter is capable of recapturing the device if necessary • Received CE mark in 2005
9/16/2014
11
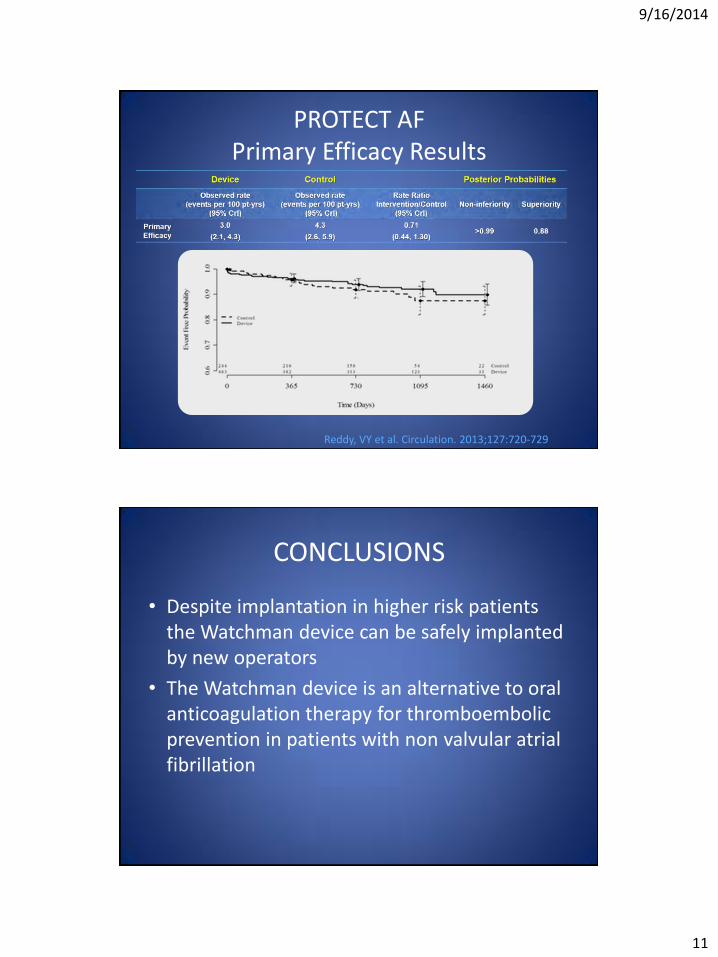
PROTECT AF Primary Efficacy Results
Reddy, VY et al. Circulation. 2013;127:720-729
CONCLUSIONS
• Despite implantation in higher risk patients the Watchman device can be safely implanted by new operators
• The Watchman device is an alternative to oral anticoagulation therapy for thromboembolic prevention in patients with non valvular atrial fibrillation
9/16/2014
12
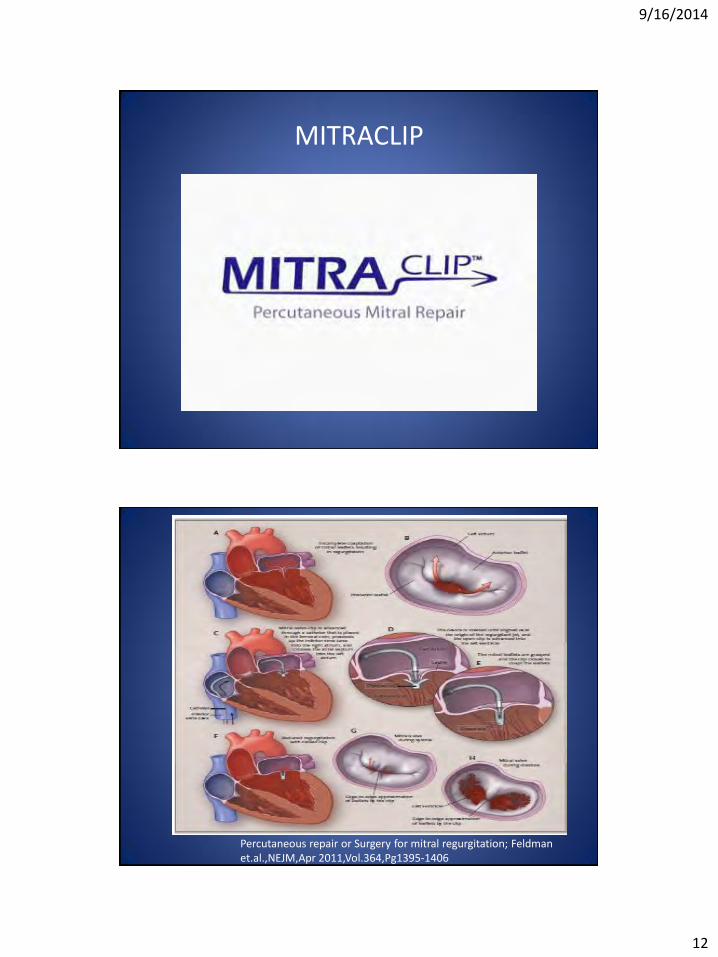
MITRACLIP
Percutaneous repair or Surgery for mitral regurgitation; Feldman et.al.,NEJM,Apr 2011,Vol.364,Pg1395-1406

9/16/2014
13
Percutaneous Mitral repair, Feldman et.al, JACC 2005 Dec:Vol.46,Pg2135-40
EVEREST II
Percutaneous repair or Surgery for mitral regurgitation; Feldman et.al.,NEJM,Apr 2011,Vol.364,Pg1395-1406
9/16/2014
14
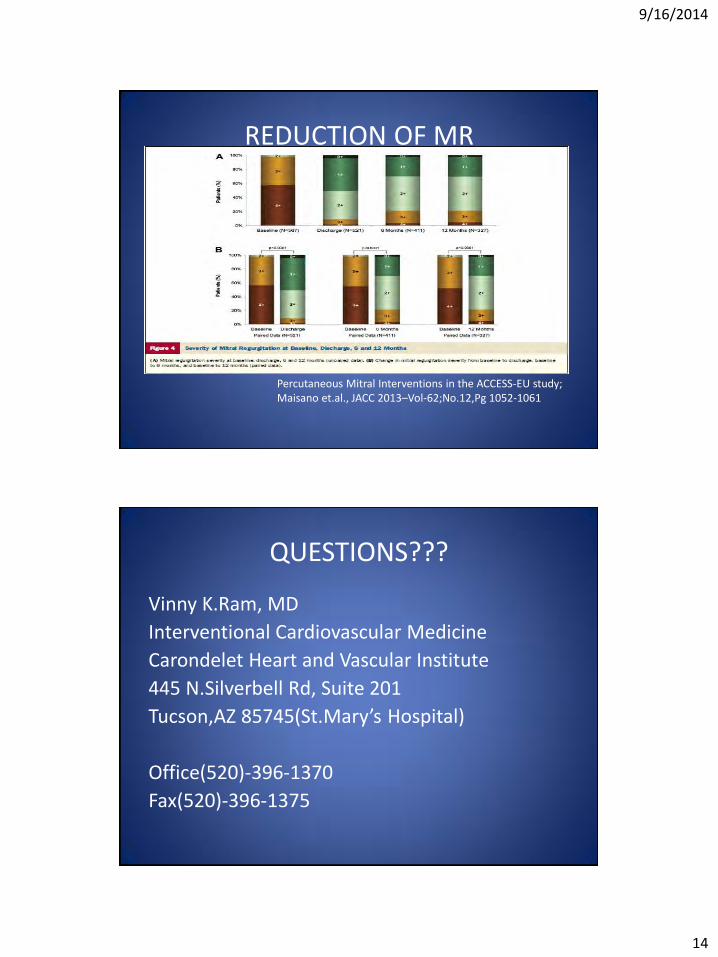
REDUCTION OF MR
Percutaneous Mitral Interventions in the ACCESS-EU study; Maisano et.al., JACC 2013–Vol-62;No.12,Pg 1052-1061
QUESTIONS???
Vinny K.Ram, MD
Interventional Cardiovascular Medicine
Carondelet Heart and Vascular Institute
445 N.Silverbell Rd, Suite 201
Tucson,AZ 85745(St.Mary’s Hospital)
Office(520)-396-1370
Fax(520)-396-1375