taxenes in breast cancer (sharm).ppt
DESCRIPTION
powerpointTRANSCRIPT
Do we need a Taxane in the Do we need a Taxane in the treatment of breast cancertreatment of breast cancer
Yes
But not yet
NoI’m not convinced
Do we need a TaxaneDo we need a Taxanein breast cancerin breast cancer
Single agentSingle agentWith AnthracyclineWith AnthracyclineWith other drugsWith other drugsWith biological therapyWith biological therapy
Do we need a Taxane Do we need a Taxane in breast cancer in breast cancer
Adjuvant ? Adjuvant ?
Neoadjuvant ?Neoadjuvant ?
Metastatic ?Metastatic ?

Drug Year of publication
CR + PR (%)
Taxotere (75-100mg/ m²) 1993 - 95 48 - 68 Taxol (175 - 250 mg/ m² : 3-24hr) 1991 - 95 29 - 63 Doxorubicin (60-75mg/ m²) 1974 - 94 43 - 54 Capecitabine 1995 - 99 35 - 50 Navelbine 1992 - 94 30 - 41 Gemcitabine 1995 - 97 25 - 37 Carboplatin 1985 - 93 7 - 35 Cisplatin 1978 -88 9 - 50 Cyclophosphamide 1959 - 68 36 Fluorouracil 1961 - 81 28 Methotrexate 1952 - 81 26 Mitomycin C 1976 - 85 32
Single agents in Breast Cancer (First-line)
Vogel CL, Nabholtz Oncologist 1999; 4: 17-33.Nabholtz et al. Exp. Opin Pharmacother 2000;
1: 187-206.
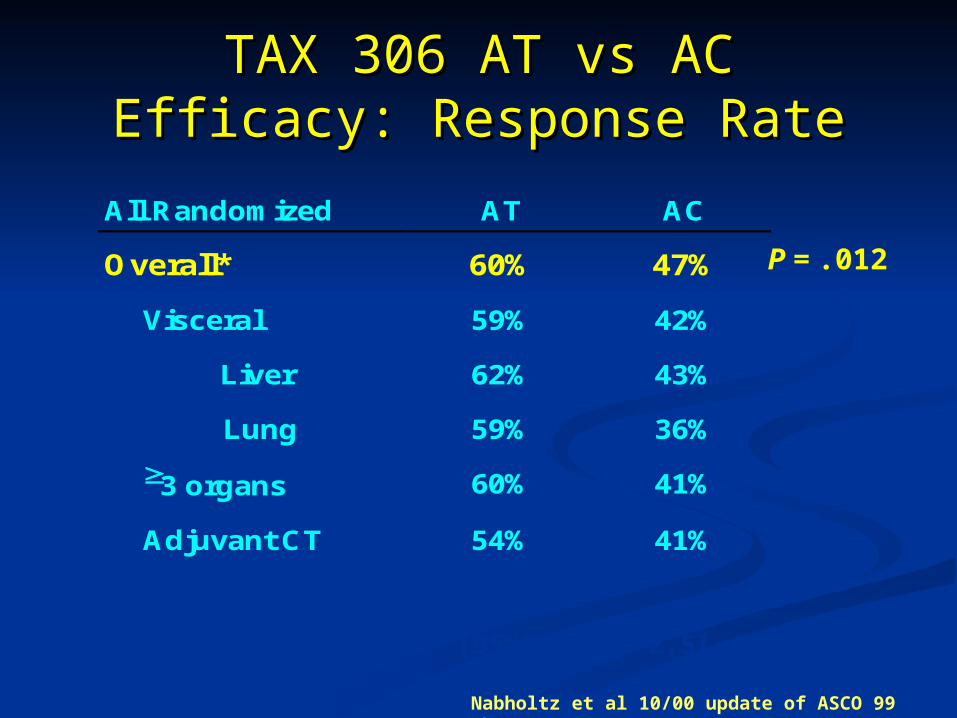
TAX 306 AT vs ACTAX 306 AT vs ACEfficacy: Response RateEfficacy: Response Rate
All Randomized AT AC
Overall* 60% 47%
Visceral 59% 42%
Liver 62% 43%
Lung 59% 36%
3 organs 60% 41%
Adjuvant CT 54% 41%
Nabholtz et al 10/00 update of ASCO 99 abstract 485.
P = .012
*Odds ratio AT/AC 1.7 [95%CI 1.1 -2.5]

TAX306: AT vs AC: Overall TAX306: AT vs AC: Overall SurvivalSurvival
40 months median follow-up40 months median follow-up
Survival Time (months)Cut-off date: 22 Feb 01
Cu
mu
lativ
e P
rob
ab
ility
AT AC
[70,81][70,81][74,85][74,85] [95% CI][95% CI]75%75%79%79%1-yr survival1-yr survival
[19.8,25.2][19.8,25.2][19.0, 26.4][19.0, 26.4] [95% CI][95% CI]21.7 mos21.7 mos22.5 mos22.5 mosMedian survivalMedian survival48 (22%)48 (22%)59 (28%)59 (28%)CensoredCensored
167 (78%)167 (78%)155 (72%)155 (72%)DeathDeath215215214214No Of ptsNo Of ptsACACATAT
Log-rank p-value=0.2432
Nabholtz, May, 2001
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54
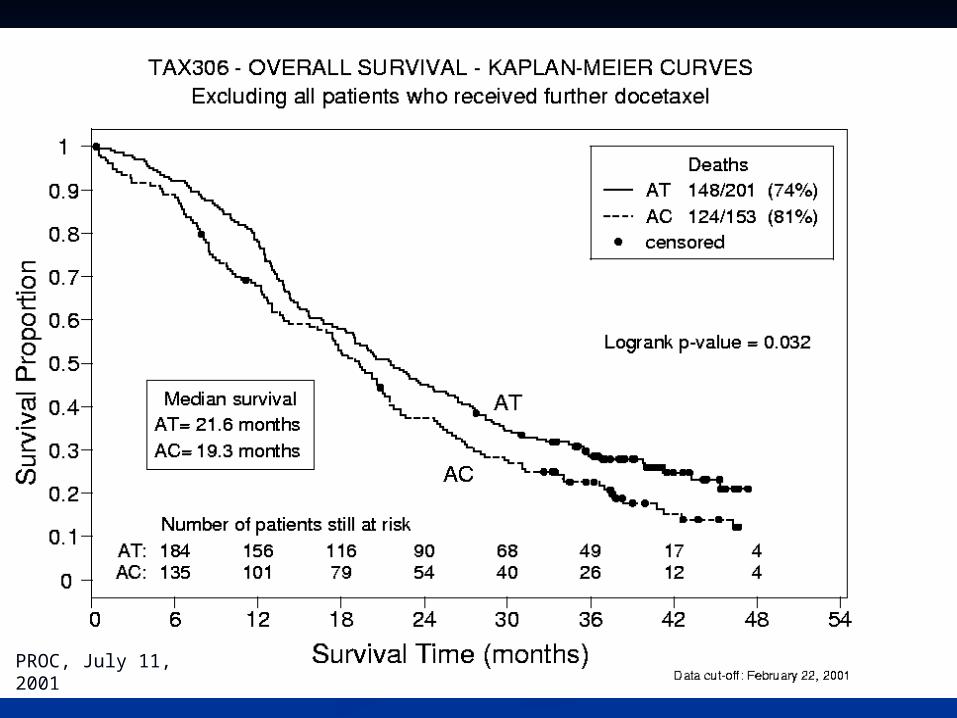
PROC, July 11, 2001

AT(N=134)AT(N=134) FAC(N=133) FAC(N=133)Response rateResponse rate 87 (68%)87 (68%) 72 (5572 (55C.RC.R 24 (19%)24 (19%) 11 (8%)11 (8%)Early toxic deathEarly toxic death 11 0 0TTPTTP 8.3 m 8.3 m 6.2 m 6.2 m P=0.034P=0.034
MSTMST 23.3 m23.3 m 18.3 m18.3 m P=0.013P=0.013
At median followAt median follow 42 % alive42 % alive 26 % alive26 % aliveUp period of 29 mUp period of 29 m
Jassem et al, JCO 2001
East-Central Europe East-Central Europe studystudy
Metastatic Breast Metastatic Breast CancerCancer
Taxanes As Adjuvant Taxanes As Adjuvant TherapyTherapy
First Generation Of First Generation Of RandomizedRandomized
Clinical TrialsClinical Trials
Benefit of sequential Taxanes
Benefit of substituting taxanes with Anthracyclines
Benefit of combining Taxanes with Anthracyclines
Do we need a taxane?Do we need a taxane?
Taxanes As Adjuvant TherapyTaxanes As Adjuvant TherapySecond Generation of Clinical TrialsSecond Generation of Clinical Trials
Ok we’d better use a Taxane, Ok we’d better use a Taxane, BUTBUT we need to know:we need to know:
• Optimal taxane administration: sequence? combinationOptimal taxane administration: sequence? combination
• Optimal taxane dose-density/dose-intensityOptimal taxane dose-density/dose-intensity
• Docetaxel versus PaclitaxelDocetaxel versus Paclitaxel
• Benefit of combining taxanes with HerceptinBenefit of combining taxanes with Herceptin®®
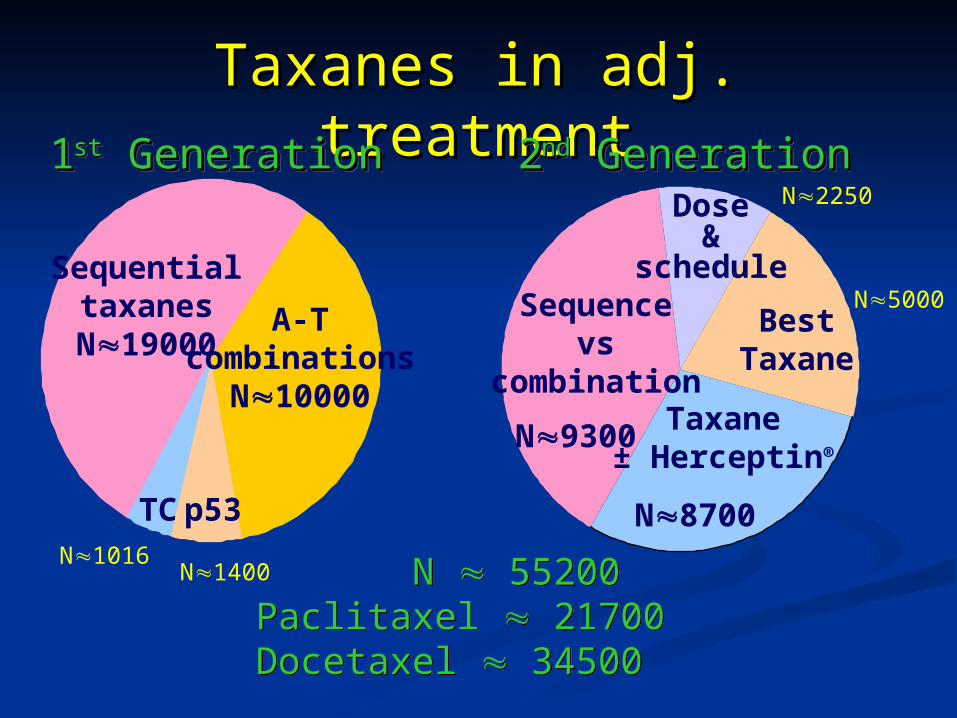
Taxanes in adj. Taxanes in adj. treatmenttreatment
N 55200Paclitaxel 21700Docetaxel 34500
N 55200Paclitaxel 21700Docetaxel 34500
Sequentialtaxanes
N19000A-T
combinationsN10000
TC p53N1016
N1400
Sequencevs
combination
BestTaxane
Dose&
schedule
N9300
N8700
N5000
N2250
Taxane± Herceptin®
11stst Generation Generation11stst Generation Generation 22ndnd Generation Generation22ndnd Generation Generation
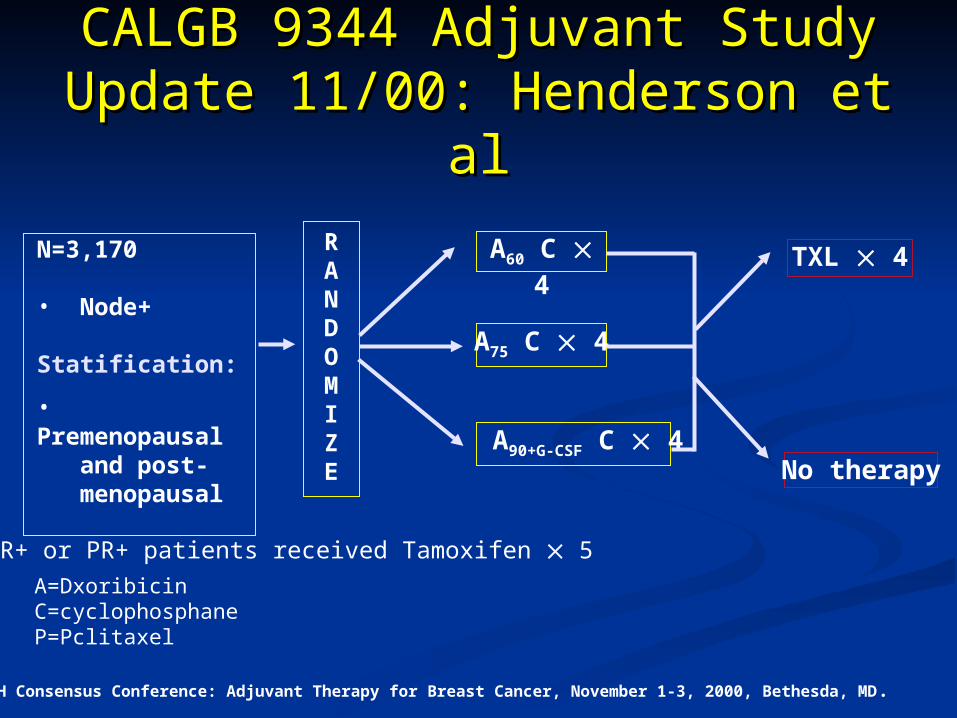
CALGB 9344 Adjuvant StudyCALGB 9344 Adjuvant StudyUpdate 11/00: Henderson et alUpdate 11/00: Henderson et al
NIH Consensus Conference: Adjuvant Therapy for Breast Cancer, November 1-3, 2000, Bethesda, MD .
ER+ or PR+ patients received Tamoxifen 5 y
No therapy
A75 C 4
A60 C 4N=3,170
• Node+
Statification:
• Premenopausal and post- menopausal
TXL 4RANDOMIZE
A90+G-CSF C 4
A=DxoribicinC=cyclophosphaneP=Pclitaxel
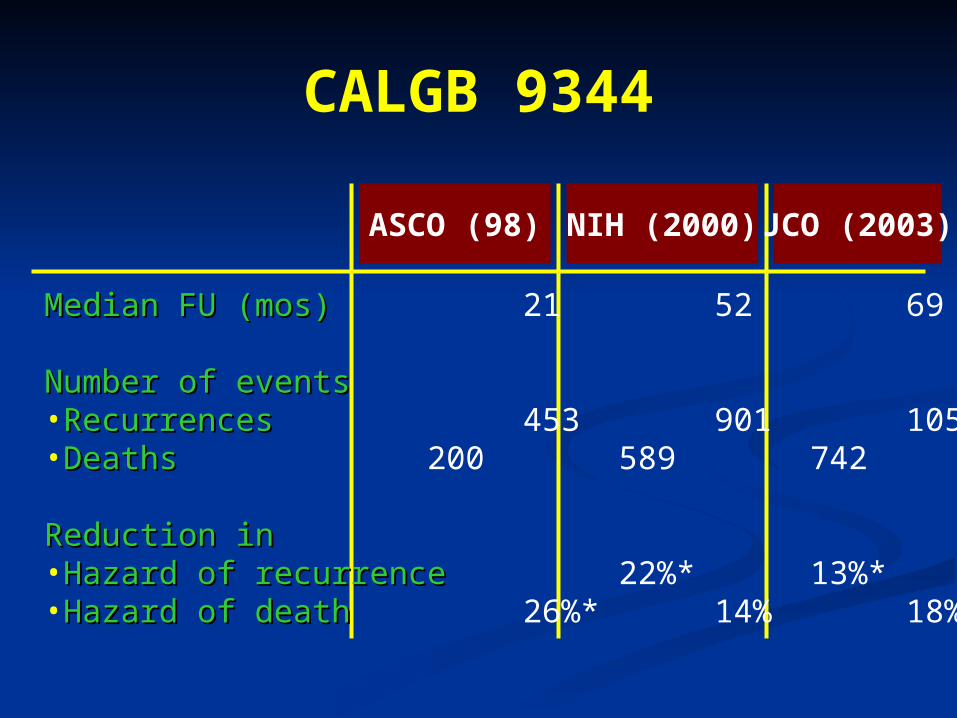
CALGB 9344
Median FU (mos)Median FU (mos) 21 52 69
Number of eventsNumber of events•RecurrencesRecurrences 453 901 1054•DeathsDeaths 200 589 742
Reduction inReduction in•Hazard of recurrenceHazard of recurrence 22%* 13%* 17%*•Hazard of deathHazard of death 26%* 14% 18%*
ASCO (98) NIH (2000)JCO (2003)
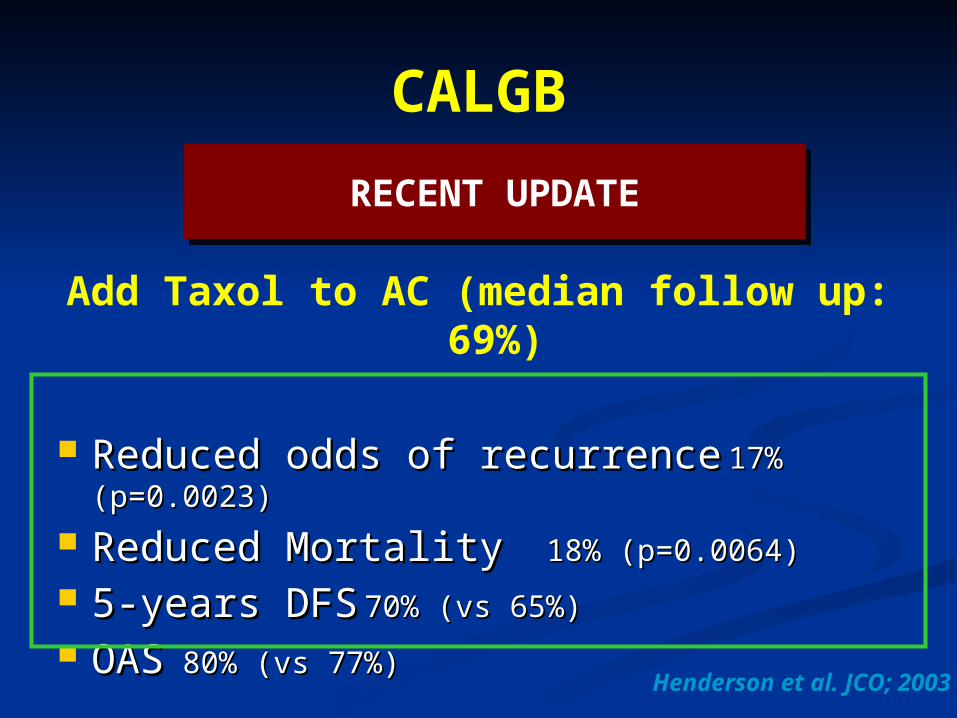
CALGB
Add Taxol to AC (median follow up: 69%)
Reduced odds of recurrenceReduced odds of recurrence 17% 17% (p=0.0023)(p=0.0023)
Reduced MortalityReduced Mortality 18% 18% (p=0.0064)(p=0.0064)
5-years DFS5-years DFS 70% (vs 65%)70% (vs 65%)
OASOAS 80% (vs 77%)80% (vs 77%)
RECENT UPDATERECENT UPDATE
Henderson et al. JCO; 2003
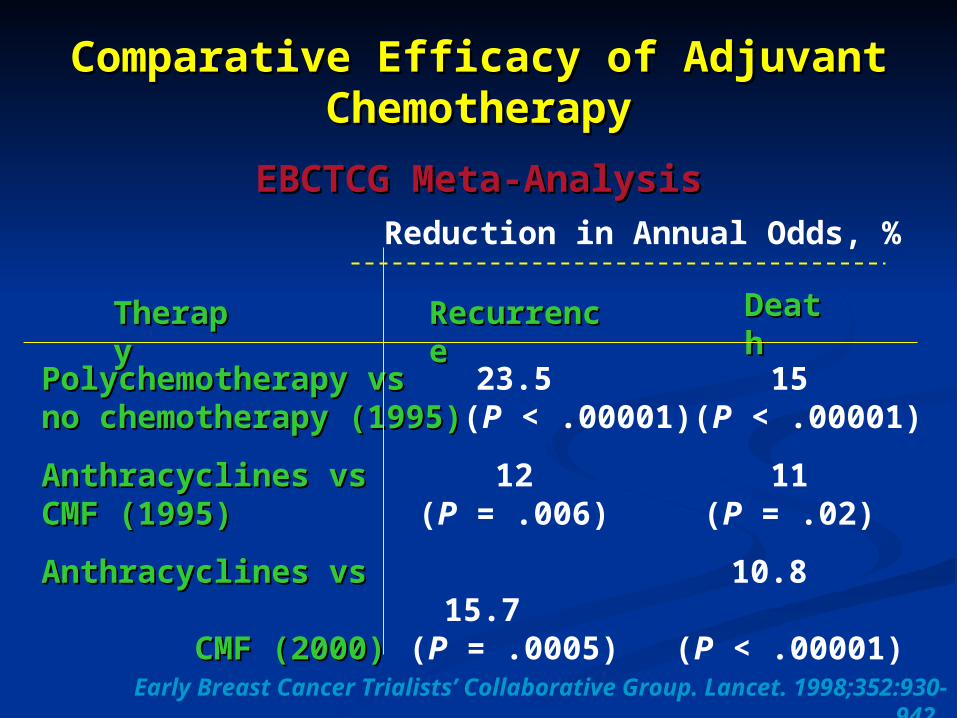
Comparative Efficacy of Adjuvant Comparative Efficacy of Adjuvant ChemotherapyChemotherapy
EBCTCG Meta-AnalysisEBCTCG Meta-Analysis
TheraTherapypy
Reduction in Annual Odds, %
RecurrenRecurrencece
DeatDeathh
Polychemotherapy vsPolychemotherapy vs 23.5 15no chemotherapy (1995)no chemotherapy (1995)(P < .00001)(P < .00001)
Anthracyclines vsAnthracyclines vs 12 11CMF (1995)CMF (1995) (P = .006) (P = .02)
Anthracyclines vsAnthracyclines vs 10.8 15.7 CMF (2000)CMF (2000) (P = .0005) (P < .00001)
Early Breast Cancer Trialists’ Collaborative Group. Lancet. 1998;352:930-942.

CALGB 9344:CALGB 9344:Disease Free Survival by Disease Free Survival by
Subgroup Subgroup Receptor Status
Positive
Receptor Status Negative / Unknown
0.50
0
Pro
po
rtio
n D
ise
as
e-F
ree
AC TXL
AC
Years
AC TXL
AC
Adapted from the 2000 NIH Consensus Development Conference on Adjuvant Therapy for Breast Cancer.
0.75
1.00
0.50
0.75
1.00
1 2 3 4 5 6

Lessons from CALGB 9344 (N=3121)
MORE IS NOT ALWAYS BETTERMORE IS NOT ALWAYS BETTER
Increase ADRIAMYCINE dose Increase ADRIAMYCINE dose from 60mg/m2 from 60mg/m2
90mg/m2 didn’t improve 90mg/m2 didn’t improve treatment outcome in any treatment outcome in any
subsetsubset
Lessons from CALGB 9344 (N=3121)
Better outcome may be Better outcome may be achieved using achieved using
PACLITAXEL x 4 PACLITAXEL x 4 following AC x 4 or following AC x 4 or simply by using 8 simply by using 8
cyclescycles
Lessons from CALGB 9344 (N=3121)
Do we need Do we need molecular molecular
selection for selection for adjuvant adjuvant cases ??cases ??
ER +ve NO benefit
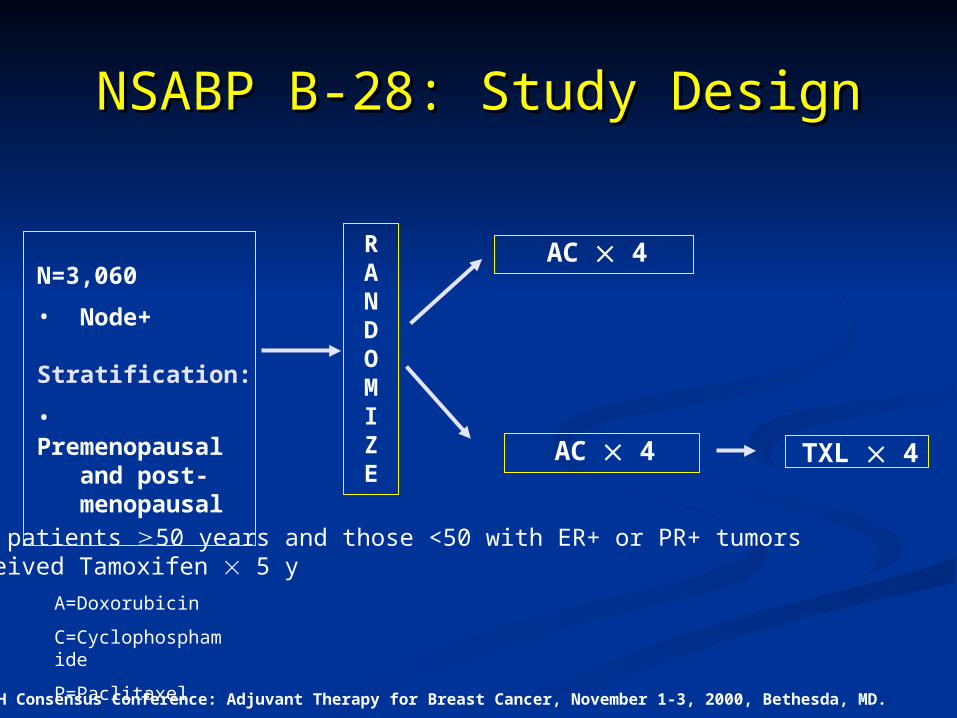
TXL 4
NSABP B-28: Study DesignNSABP B-28: Study Design
NIH Consensus Conference: Adjuvant Therapy for Breast Cancer, November 1-3, 2000, Bethesda, MD.
A=Doxorubicin
C=Cyclophosphamide
P=Paclitaxel
All patients 50 years and those <50 with ER+ or PR+ tumorsreceived Tamoxifen 5 y
RANDOMIZE
N=3,060
• Node+
Stratification:
• Premenopausal and post- menopausal
AC 4
AC 4
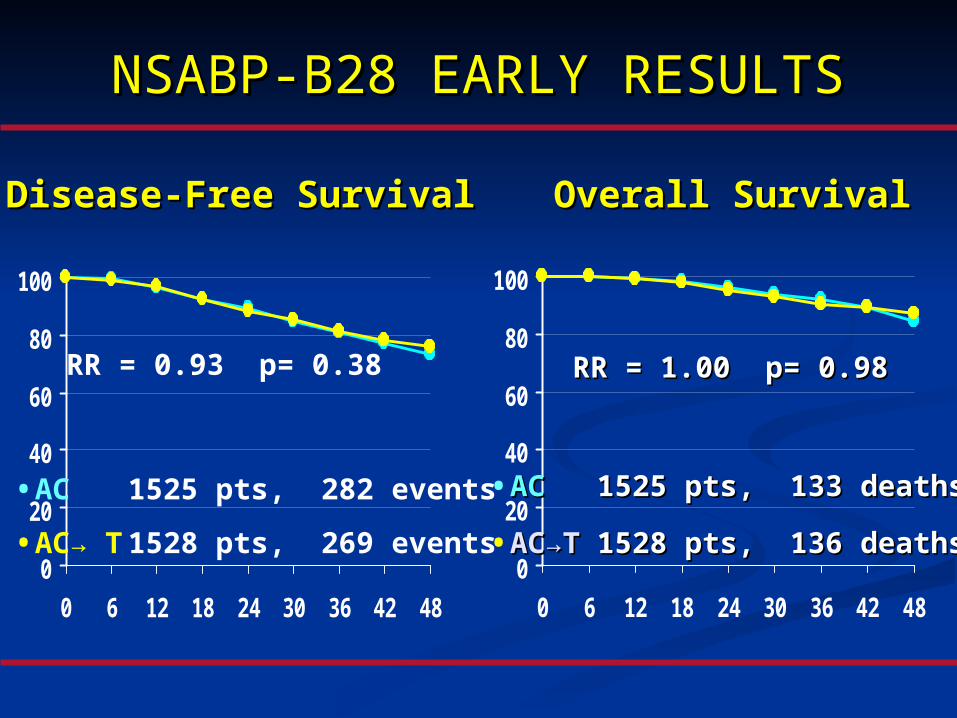
NSABP-B28 EARLY RESULTSNSABP-B28 EARLY RESULTS
Disease-Free SurvivalDisease-Free Survival
0
20
40
60
80
100
0 6 12 18 24 30 36 42 48
•AC→ T 1528 pts, 269 events
•AC 1525 pts, 282 events
RR = 0.93 p= 0.38
0
20
40
60
80
100
0 6 12 18 24 30 36 42 48
•ACAC→→TT 1528 pts, 136 deaths1528 pts, 136 deaths
•ACAC 1525 pts, 133 deaths1525 pts, 133 deaths
RR = 1.00 p= 0.98RR = 1.00 p= 0.98
Overall SurvivalOverall Survival
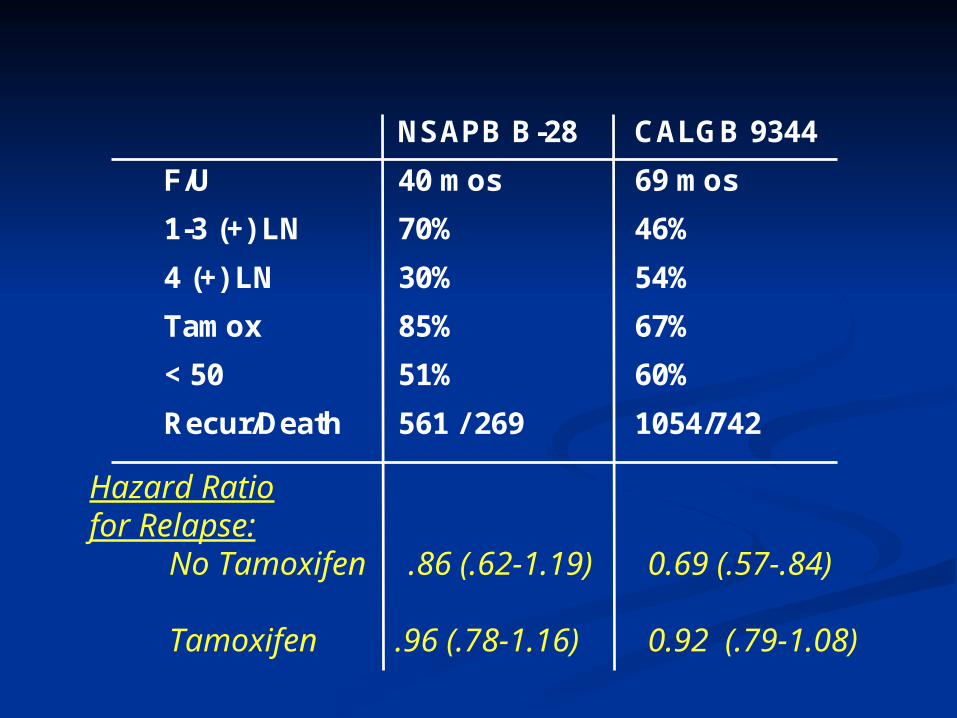
NSAPB B-28 CALGB 9344
F/U 40 mos 69 mos
1-3 (+) LN 70% 46%
4 (+) LN 30% 54%
Tamox 85% 67%
< 50 51% 60%
Recur/Death 561 / 269 1054/742
Hazard Ratio for Relapse:
No Tamoxifen .86 (.62-1.19) 0.69 (.57-.84)
Tamoxifen .96 (.78-1.16) 0.92 (.79-1.08)
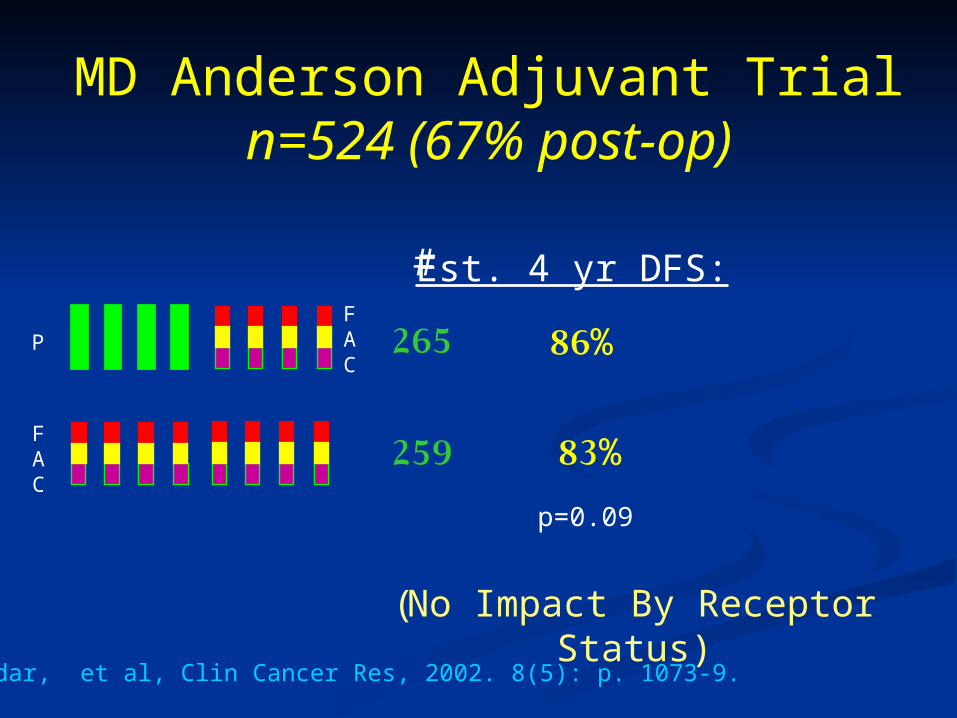
MD Anderson Adjuvant Trialn=524 (67% post-op)
Est. 4 yr DFS:
86%
83%
p=0.09
Buzdar, et al, Clin Cancer Res, 2002. 8(5): p. 1073-9.
#
265
259
(No Impact By Receptor Status)
FAC
P
FAC
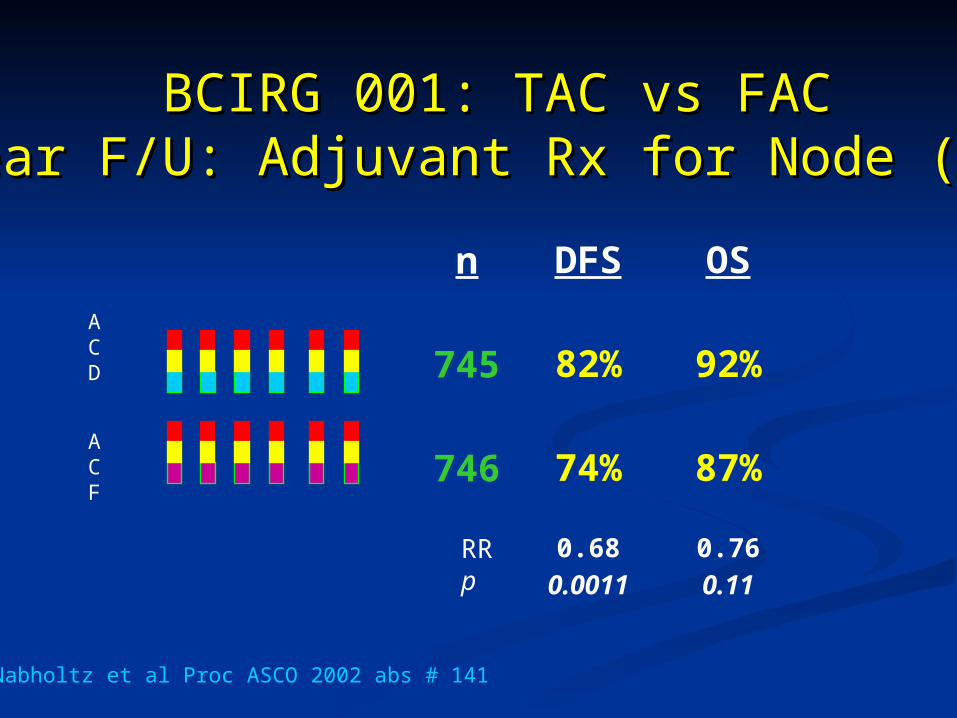
BCIRG 001: TAC vs FACBCIRG 001: TAC vs FAC3 Year F/U: Adjuvant Rx for Node (+) BC3 Year F/U: Adjuvant Rx for Node (+) BC
n
745
746
DFS
82%
74%
0.680.0011
OS
92%
87%
0.760.11
Nabholtz et al Proc ASCO 2002 abs # 141
RRp
ACD
ACF
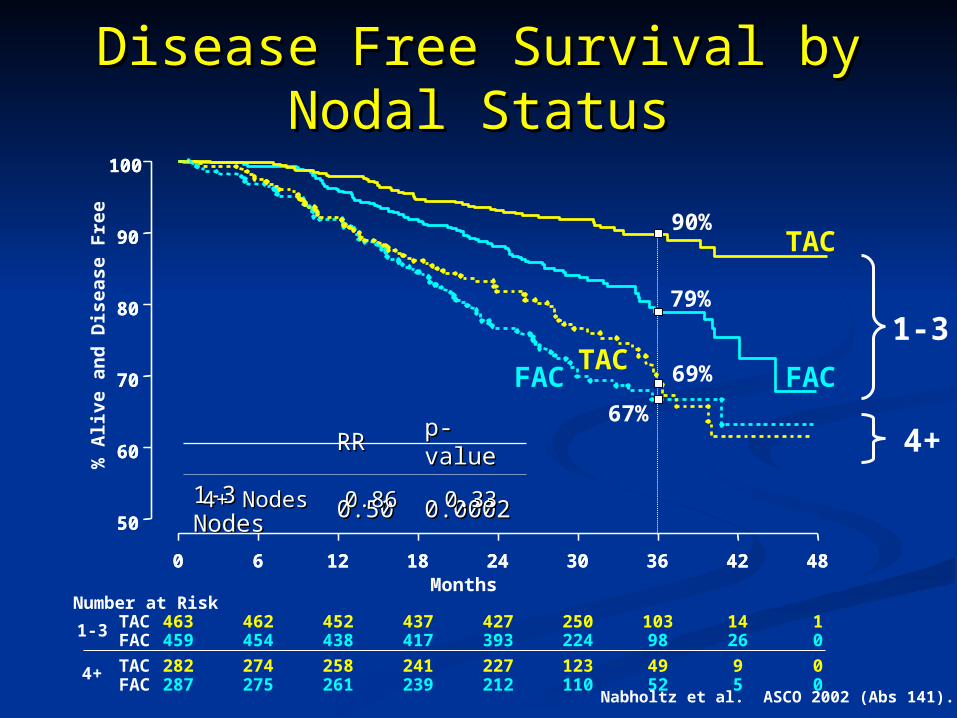
Disease Free Survival by Nodal Disease Free Survival by Nodal StatusStatus
RRRR p-valuep-value
1-3 Nodes1-3 Nodes 0.500.50 0.00020.0002
TAC
FAC
0 6 12 18 24 30 36 42 48Months
Number at RiskTACFAC
463 462 452 437 427 250 103 14 1459 454 438 417 393 224 98 26 0
50
60
70
80
90
100
% A
live
an
d D
ise
ase
Fre
e
1-3
1-3
90%
79%
TACFAC
0 6 12 18 24 30 36 42 48
4+ TACFAC
282 274 258 241 227 123 49 9 0287 275 261 239 212 110 52 5 0
50
60
70
80
90
100
0.330.330.860.864+ Nodes4+ Nodes
4+
69%
67%
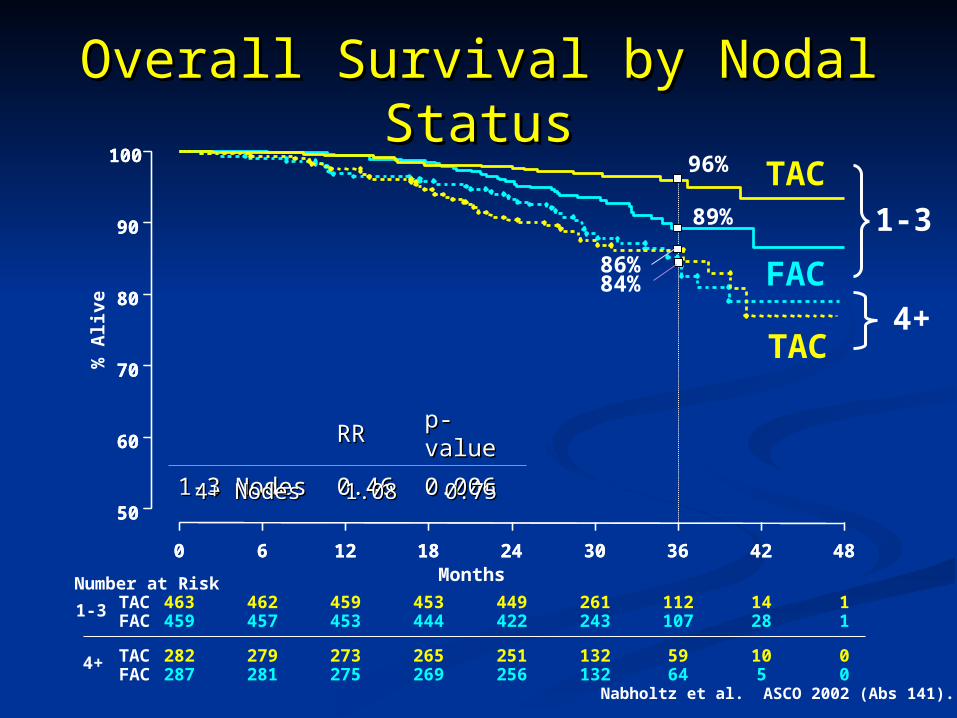
Nabholtz et al. ASCO 2002 (Abs 141).
TAC
FAC
0 6 12 18 24 30 36 42 48MonthsNumber at Risk
TACFAC
463 462 459 453 449 261 112 14 1459 457 453 444 422 243 107 28 1
50
60
70
80
90
100
% A
live
Overall Survival by Nodal Overall Survival by Nodal StatusStatus
96%
89%
RRRR p-valuep-value
1-3 Nodes1-3 Nodes 0.460.46 0.0060.006
1-3
1-3
TAC
0 6 12 18 24 30 36 42 48
4+ TACFAC
282 279 273 265 251 132 59 10 0287 281 275 269 256 132 64 5 0
50
60
70
80
90
100
0.750.751.081.084+ Nodes4+ Nodes
4+
86%84%
Nabholtz et al. ASCO 2002 (Abs 141).

Disease Free Survival by Disease Free Survival by Hormonal StatusHormonal Status
TAC
FAC
0 12 24 36 48Months
N at RiskTACFAC
231 217 188 47 0228 202 158 34 0
50
60
70
80
90
100
% A
live
an
d D
ise
ase
Fre
e
TAC
FAC
0 12 24 36 48Months
N at RiskTACFAC
514 493 466 105 1518 497 447 116 0
50
60
70
80
90
100
Negative Positive
RR = 0.62p = 0.005
RR = 0.68p = 0.02
Nabholtz et al. ASCO 2002 (Abs 141).
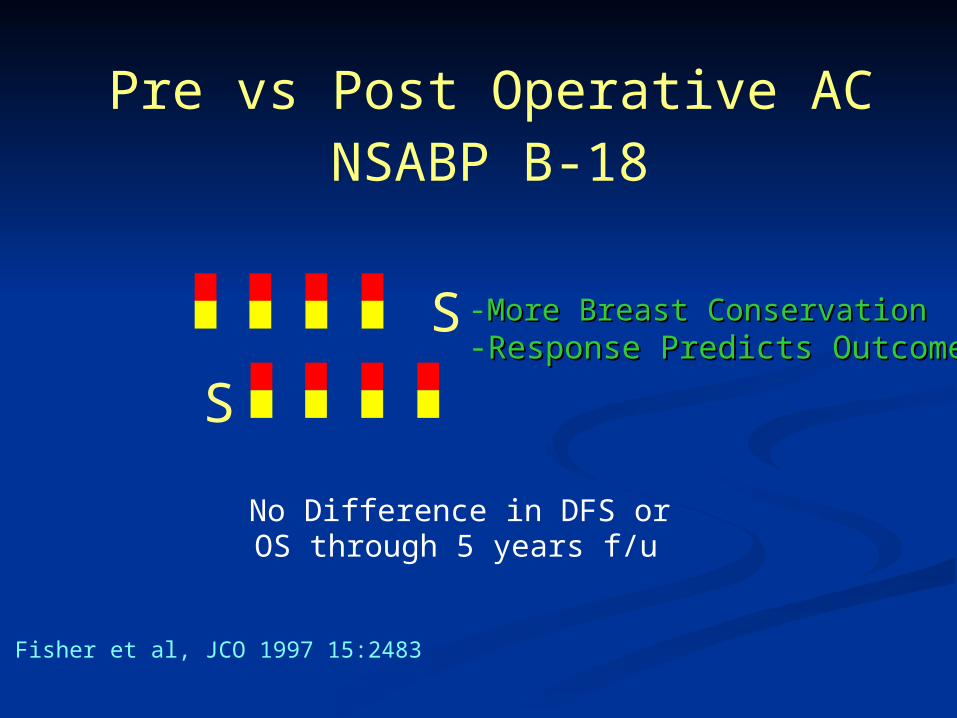
Pre vs Post Operative ACNSABP B-18
Fisher et al, JCO 1997 15:2483
S
S -More Breast ConservationMore Breast Conservation-Response Predicts OutcomeResponse Predicts Outcome
No Difference in DFS or OS through 5 years f/u

B-18B-18Disease-Free and Overall Disease-Free and Overall
SurvivalSurvivalAccording to ResponseAccording to Response
00
20%20%
40%40%
60%60%
80%80%
100%100%
22 44 66 88YearYear
P=0.00005P=0.00005pINVpINVcPRcPRcNRcNR
pCRpCR
22 44 66 88
pINVpINVcPRcPRcNRcNR
pCRpCR
P=0.0008P=0.0008
Wolmark N: CDC, 2000Wolmark N: CDC, 2000
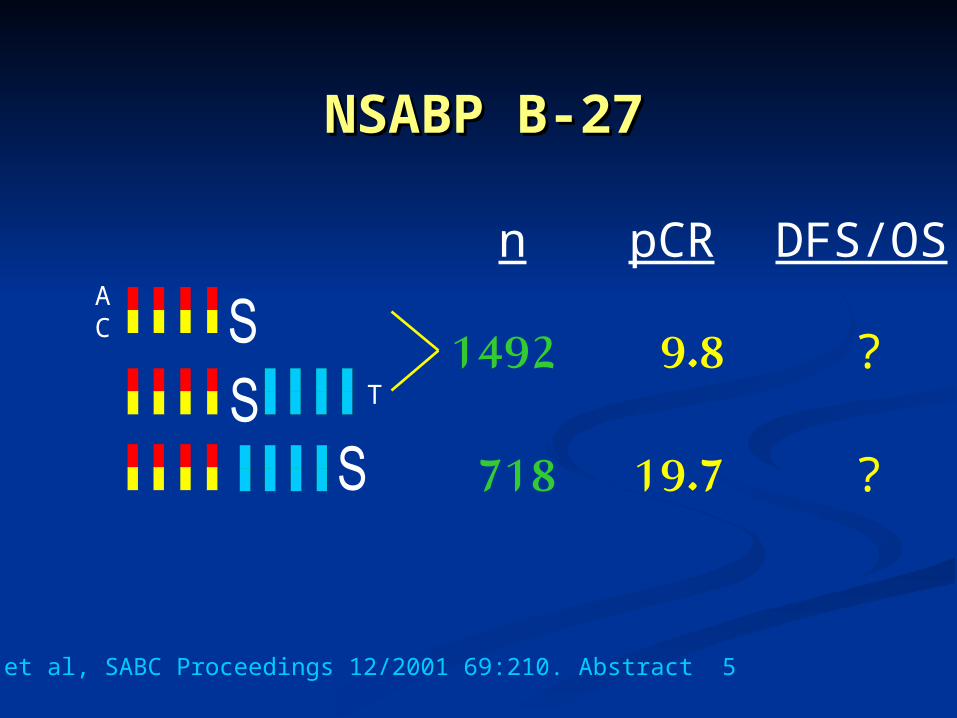
NSABP B-27NSABP B-27
1492
718
9.8
19.7
?
?
n pCR DFS/OS
Bear et al, SABC Proceedings 12/2001 69:210. Abstract 5
AC
T
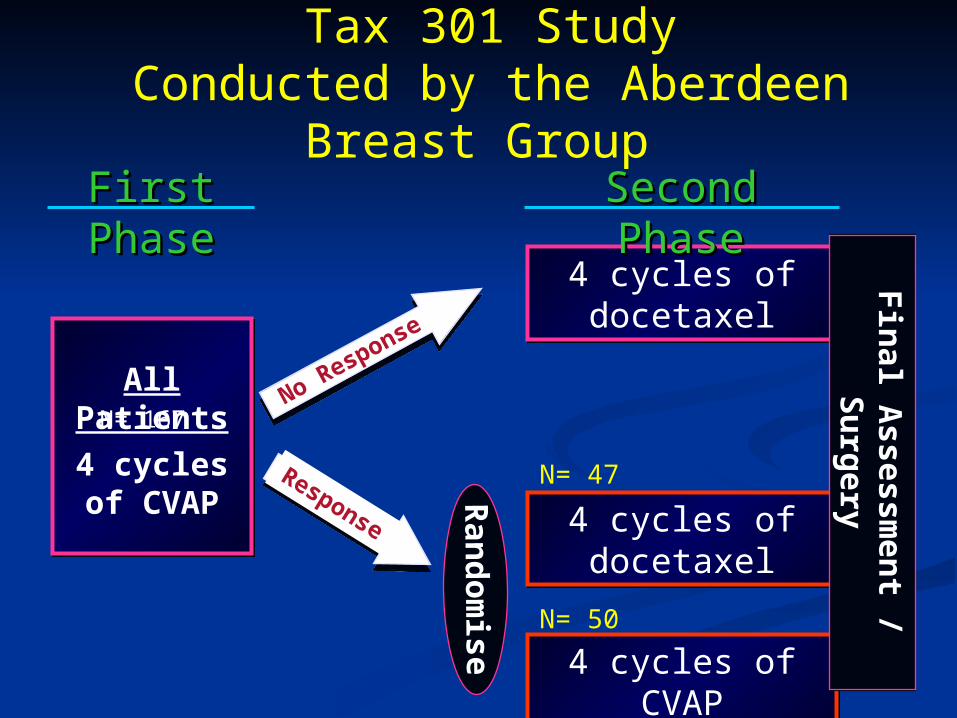
All Patients
4 cycles of CVAP
4 cycles of docetaxel4 cycles of docetaxel
4 cycles of docetaxel4 cycles of docetaxel
4 cycles of CVAP4 cycles of CVAP
No Response
Response
Ran
do
mise
First First PhasePhase
Second Second PhasePhase F
inal A
ssessmen
t / Su
rgery
Tax 301 StudyConducted by the Aberdeen
Breast Group
Fin
al Assessm
ent / S
urg
ery
N= 47
N= 50
N= 167
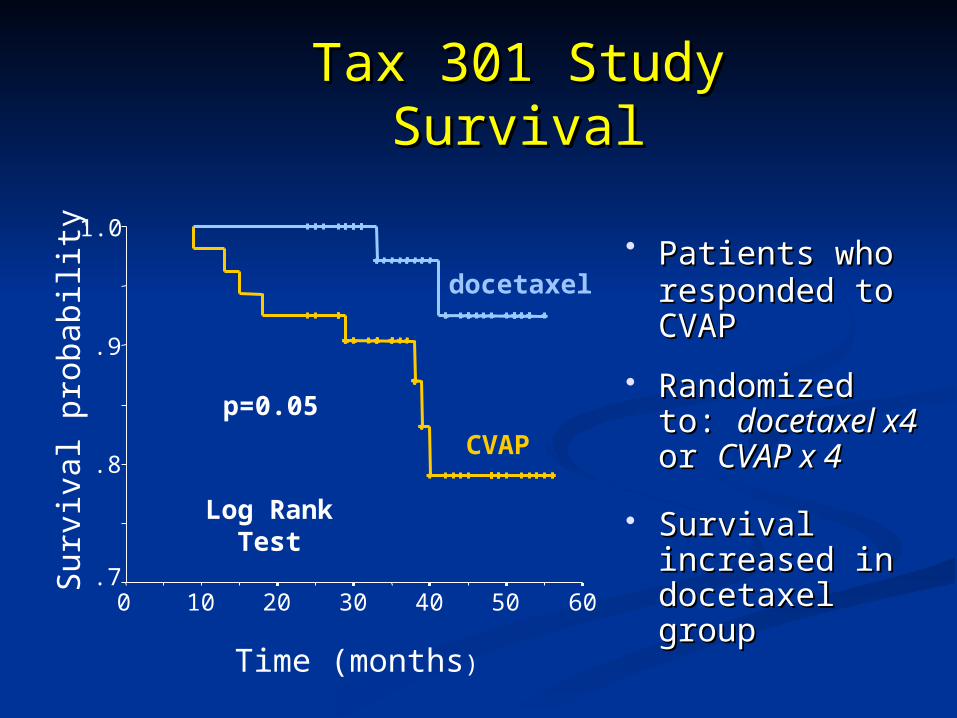
Tax 301 StudyTax 301 StudySurvivalSurvival
Patients whoPatients who responded to responded to CVAP CVAP
Randomized Randomized to: to: docetaxel docetaxel x4x4 or or CVAP x 4CVAP x 4
Survival Survival increased in increased in docetaxel docetaxel groupgroupTime (months)
6050403020100
Sur
viva
l pro
babi
lity
1.0
.9
.8
.7
docetaxel
CVAP
p=0.05
Log Rank Test

Taxanes as Adjuvant or Neo-Adj. Rx:
Available Randomized Trials
Study Design ResultCALGB 9344 AC +/-P POSITIVENSABP B-28 AC +/-P NEG. / EARLYMD Anderson P->FAC vs FAC Too Small...?POS.BCIRG 001 TAC vs FAC POSITIVENSABP B-27 AC +/-D POSITIVEAberdeen CAVp +/D POSITIVE
P = paclitaxelD = docetaxel
Taxanes in Breast Cancer
1.1. Better schedulingBetter scheduling
2.2. Dose – Dense programsDose – Dense programs
3.3. Synergy with other drugsSynergy with other drugs
4.4. Synergy with biological therapySynergy with biological therapy
5.5. Predict benefitPredict benefit
6.6. Newer generation of Taxanes Newer generation of Taxanes
How to Improve Outcome ??How to Improve Outcome ??
Scheduling of TaxolScheduling of Taxol
Advantages:Advantages:
1- Better toxicity profile- Less alopecia- Less neuropathy- Less myelosuppression
Perez et.al.Proc. ASCO, 1998 Abs #480
Weekly TaxolWeekly Taxol
Advantages:Advantages:Weekly TaxolWeekly Taxol
2- Better Tumour cell kill- More frequent drug exposure
Dose dense (Seidman et.al., JCO, 1998)
- Enhancement of Anti Angiogenic propertyof Taxol (Belotti et.al., Cancer Res.,1998)
- Enhancement of Apoptosis induction by Taxol (Milross et.al., JNCI, 1996)
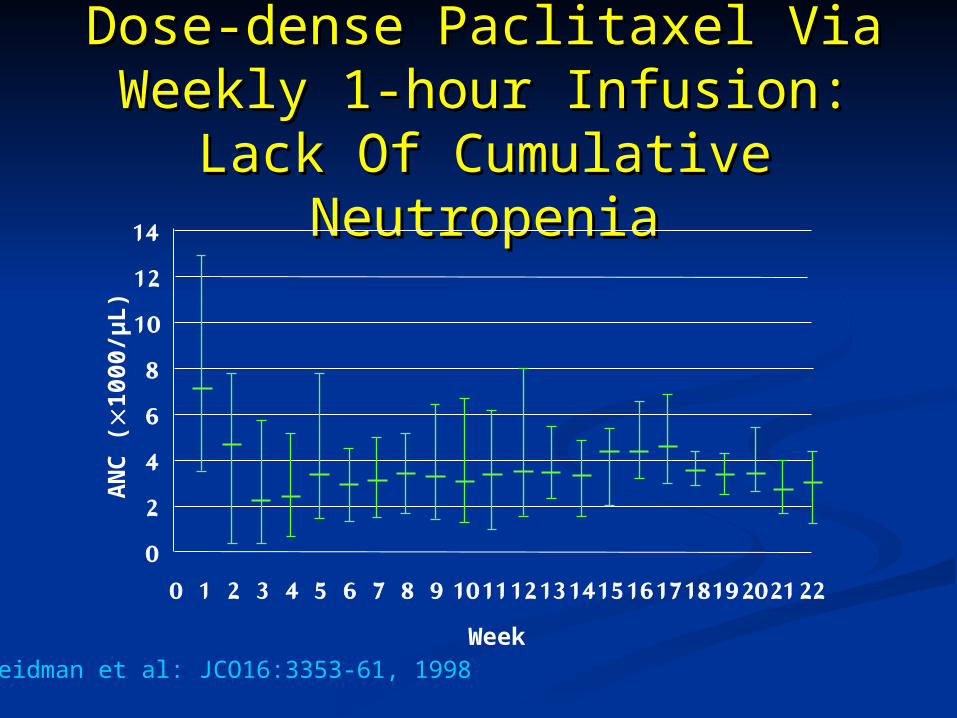
Dose-dense Paclitaxel Via Dose-dense Paclitaxel Via Weekly 1-hour Infusion: Lack Weekly 1-hour Infusion: Lack Of Cumulative NeutropeniaOf Cumulative Neutropenia
0
2
4
6
8
10
12
14
0 1 2 3 4 5 6 7 8 9 10111213141516171819202122
AN
C (
1000
/µL
)
WeekSeidman et al: JCO16:3353-61, 1998
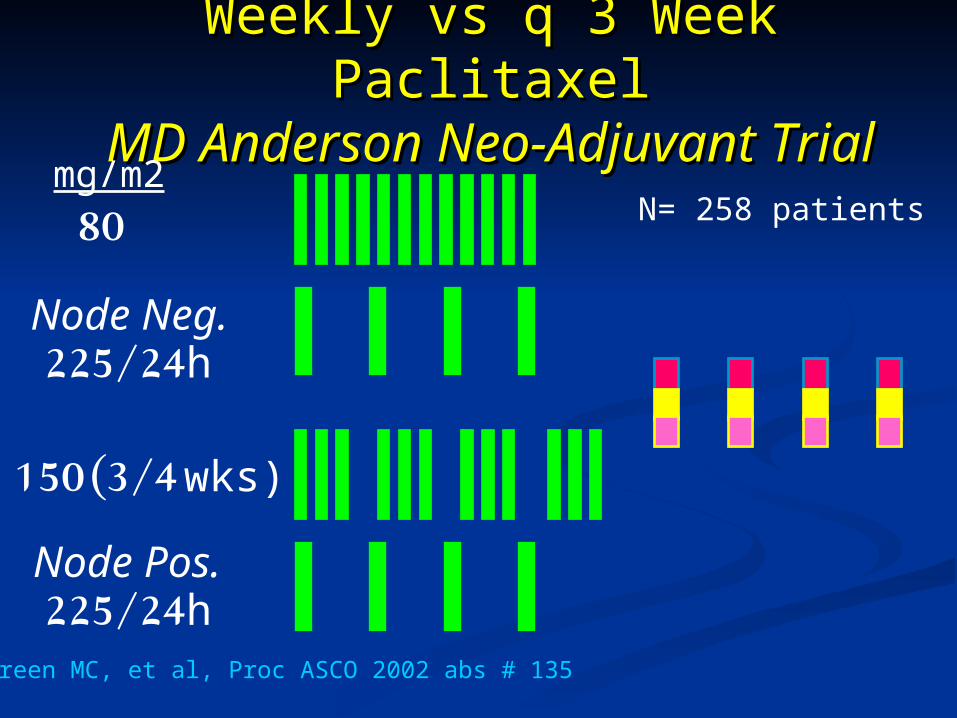
Weekly vs q 3 Week PaclitaxelWeekly vs q 3 Week PaclitaxelMD Anderson Neo-Adjuvant MD Anderson Neo-Adjuvant
TrialTrial
225/24h
80mg/m2
Green MC, et al, Proc ASCO 2002 abs # 135
225/24h
150 (3/4 wks)
Node Neg.
Node Pos.
N= 258 patients
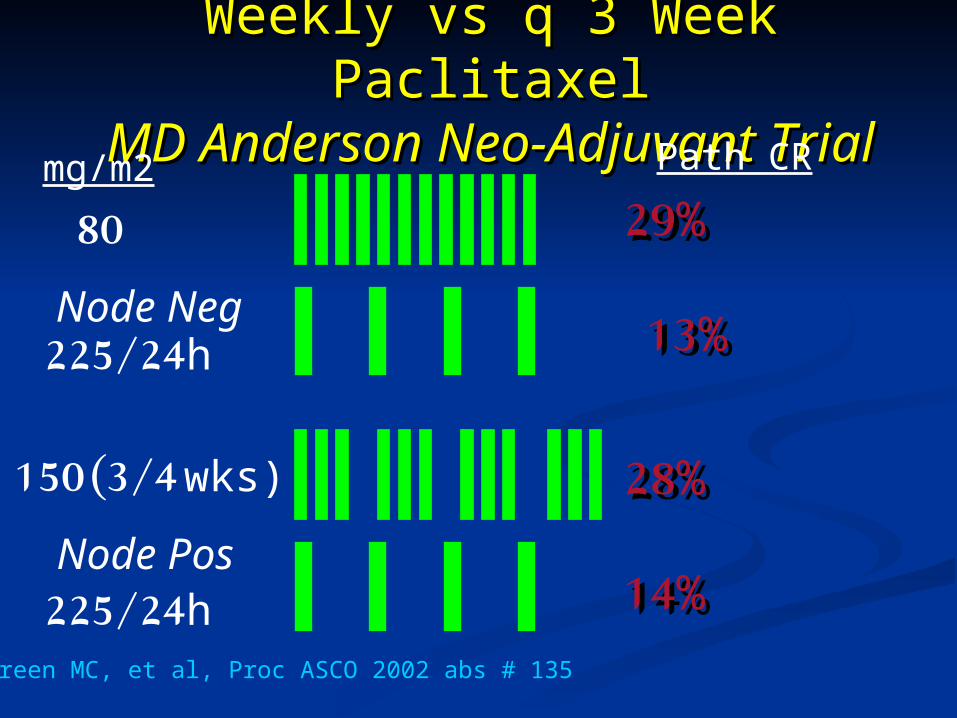
Weekly vs q 3 Week PaclitaxelWeekly vs q 3 Week PaclitaxelMD Anderson Neo-Adjuvant MD Anderson Neo-Adjuvant
TrialTrial
225/24h
80
mg/m2
Green MC, et al, Proc ASCO 2002 abs # 135
225/24h
150 (3/4 wks)
Path CR
29%29%
13%13%
28%28%
14%14%
Node Neg
Node Pos

Taxanes in Breast Cancer
1.1. Better schedulingBetter scheduling
2.2. Dose – Dense programsDose – Dense programs
3.3. Synergy with other drugsSynergy with other drugs
4.4. Synergy with biological therapySynergy with biological therapy
5.5. Predict benefitPredict benefit
6.6. Newer generation of Taxanes Newer generation of Taxanes
How to Improve Outcome ??How to Improve Outcome ??
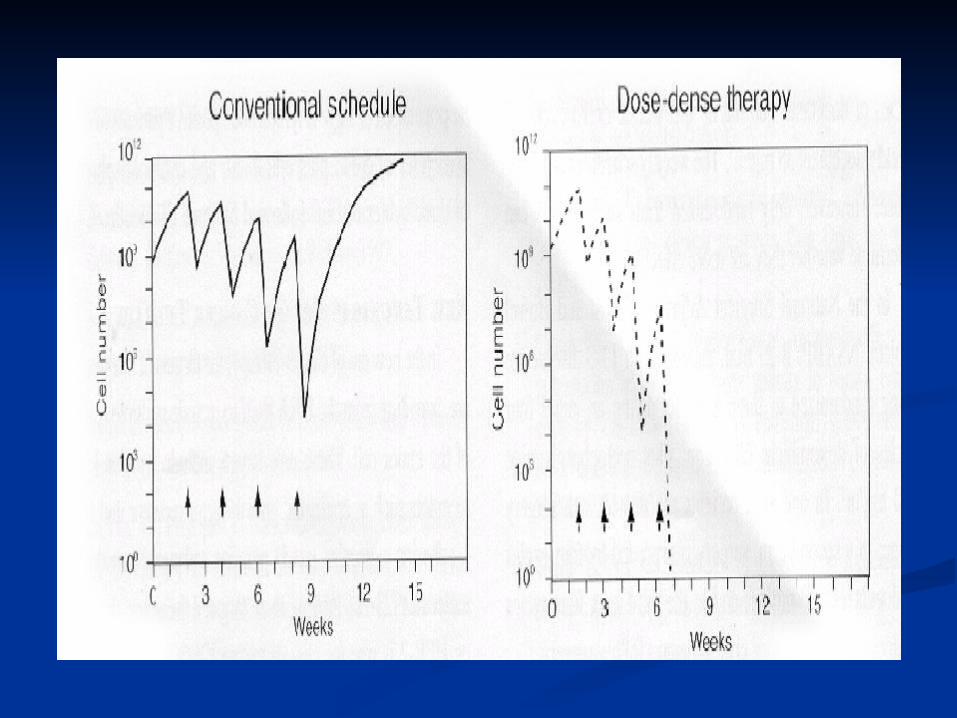

1012
108
104
100
0 20 40 60
WeeksWeeks
Cel
l Num
ber
Cel
l Num
ber
Why conventional sequential therapy may fail?Why conventional sequential therapy may fail?
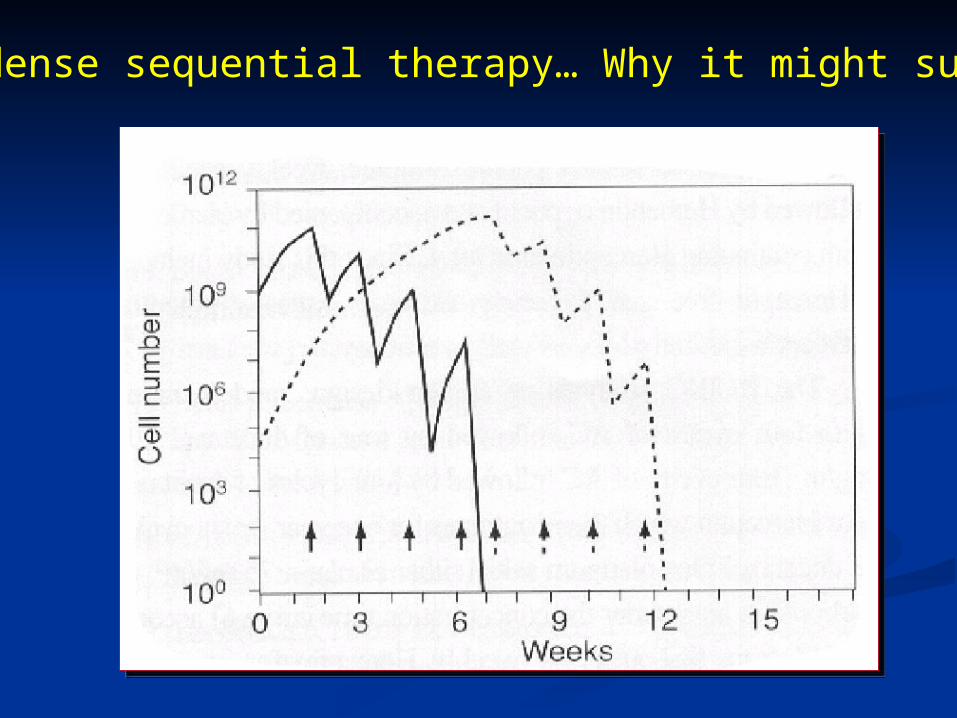
Dose dense sequential therapy… Why it might succeed?
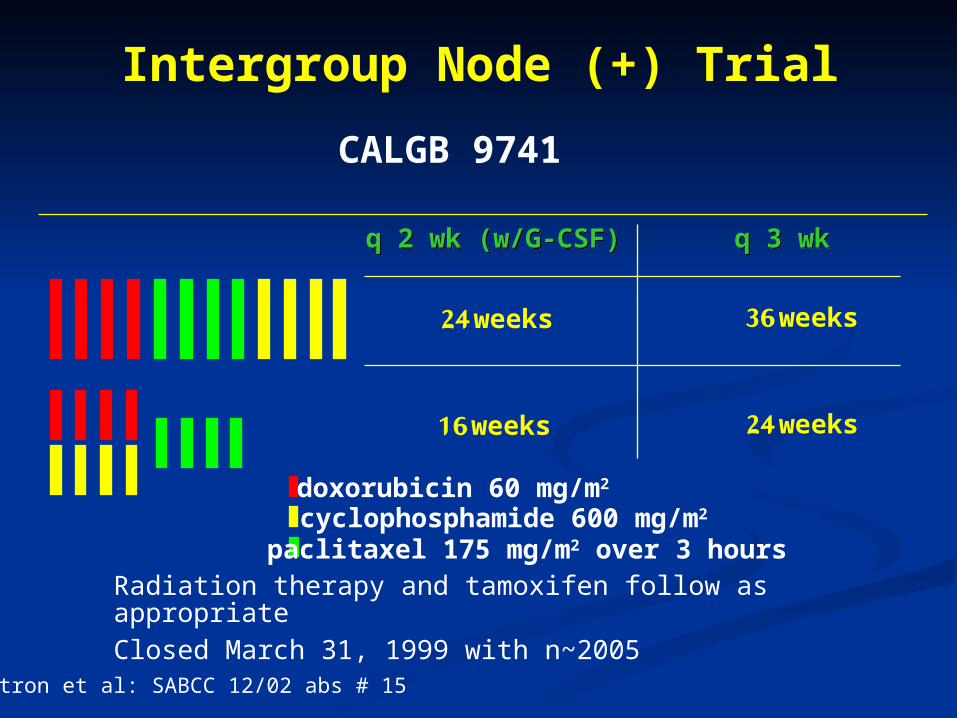
q 2 wk (w/G-CSF)q 2 wk (w/G-CSF) q 3 wkq 3 wk
24 weeks
16 weeks 24 weeks
36 weeks
Radiation therapy and tamoxifen follow as appropriateClosed March 31, 1999 with n~2005
doxorubicin 60 mg/m2
cyclophosphamide 600 mg/m2
paclitaxel 175 mg/m2 over 3 hours
CALGB 9741
Intergroup Node (+) Trial
Citron et al: SABCC 12/02 abs # 15
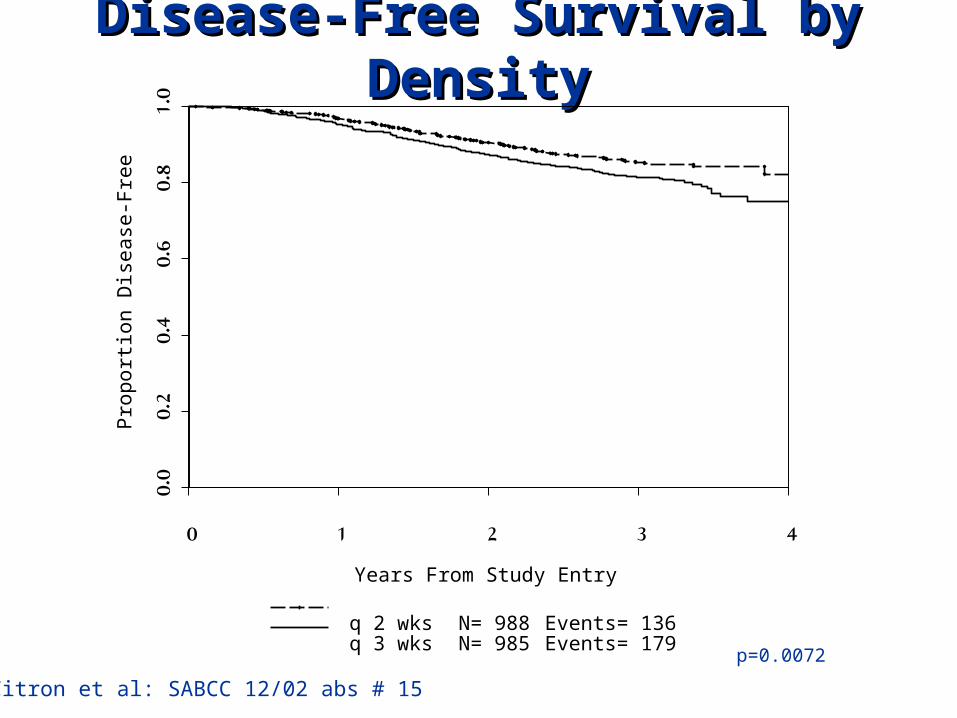
Disease-Free Survival by Disease-Free Survival by DensityDensity
Years From Study Entry
Pro
po
rtio
n D
ise
ase
-Fre
e
0 1 2 3 4
0.0
0.2
0.4
0.6
0.8
1.0
q 2 wksq 3 wks
N= 988N= 985
Events= 136Events= 179
p=0.0072
Citron et al: SABCC 12/02 abs # 15
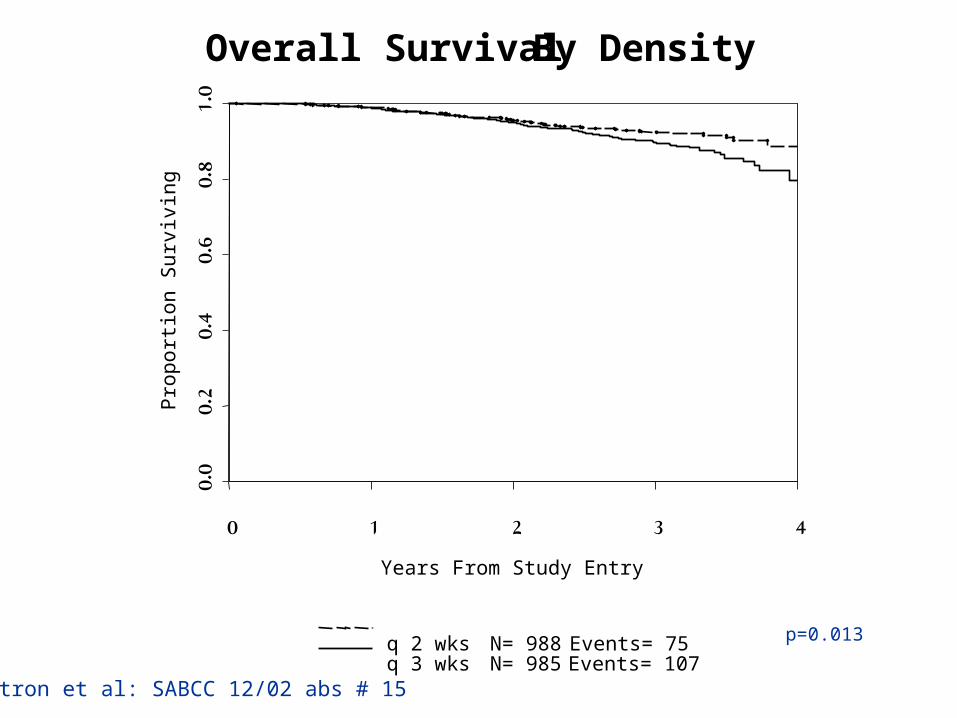
Overall Survival by Overall Survival by DensityDensity
Years From Study Entry
Pro
po
rtio
n S
urv
ivin
g
0 1 2 3 4
0.0
0.2
0.4
0.6
0.8
1.0
Overall Survival By Density
q 2 wksq 3 wks
N= 988N= 985
Events= 75Events= 107
p=0.013
Citron et al: SABCC 12/02 abs # 15

4.5%4.5%3.9%3.9%1.9%1.9%1.9%1.9%Neurologic: Severe Sensory Neurologic: Severe Sensory Loss or Motor WeaknessLoss or Motor Weakness
0%0%0%0%0%0%0%0%Platelet TransfusionPlatelet Transfusion
13%13%3%3%2%2%0%0%Red Cell TransfusionRed Cell Transfusion
2%2%5%5%2%2%3%3%Febrile Neutropenia Febrile Neutropenia HospitalizedHospitalized
9%9%43%43%3%3%24%24%Granulocytes < 0.5/ulGranulocytes < 0.5/ul
10110110110196969999No. DataNo. Data
495495501501493493488488No. TreatedNo. Treated
IVIVCon q 2Con q 2
IIIIIICon q 3Con q 3
IIIISeq q 2Seq q 2
IISeq q 3Seq q 3
Citron et al: SABCC 12/02 abs # 15
Taxanes in Breast Cancer
1.1. Better schedulingBetter scheduling
2.2. Dose – Dense programsDose – Dense programs
3.3. Synergy with other drugsSynergy with other drugs
4.4. Synergy with biological therapySynergy with biological therapy
5.5. Predict benefitPredict benefit
6.6. Newer generation of Taxanes Newer generation of Taxanes
How to Improve Outcome ??How to Improve Outcome ??

Capecitabine
TPupregulation1
Bcl-2downregulation2
Taxane
Potential mechanisms Potential mechanisms underlying underlying
Capecitabine plus Taxane Capecitabine plus Taxane synergysynergy
1Sawada N et al. Clin Cancer Res 1998;4:1013–92Fujimoto-Ouchi K et al. Proc Am Assoc Cancer Res 2001 (Abst 463)
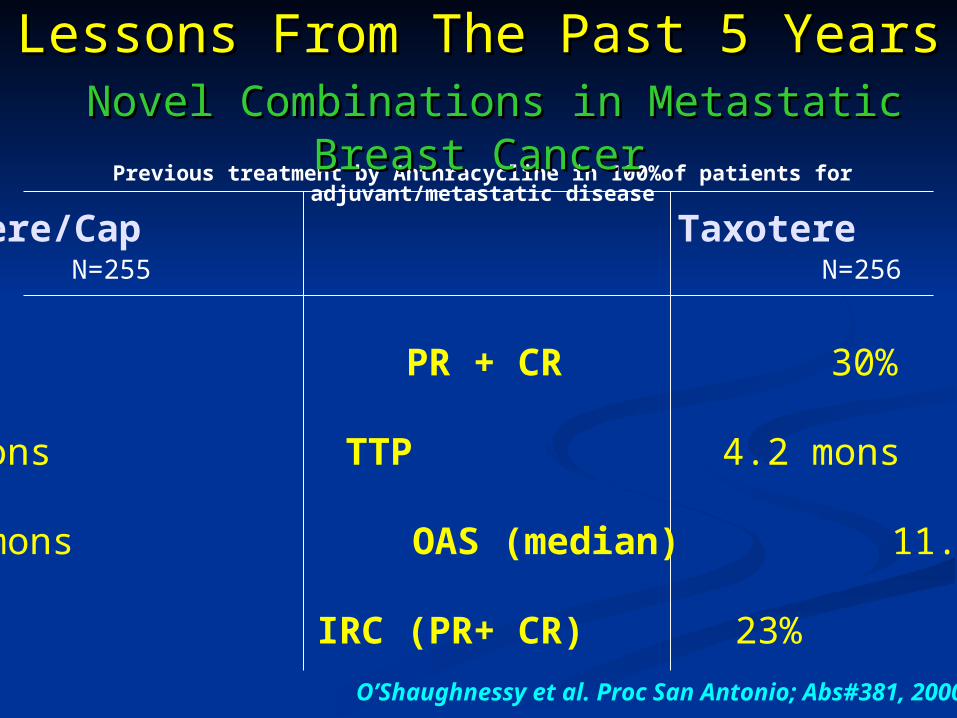
Taxotere/Cap Taxotere
42% PR + CR 30%
6.1 mons TTP 4.2 mons
13.7 mons OAS (median) 11.1 mons
32% IRC (PR+ CR) 23%
O’Shaughnessy et al. Proc San Antonio; Abs#381, 2000
Previous treatment by Anthracycline in 100%of patients for adjuvant/metastatic disease
N=255 N=256
Lessons From The Past 5 YearsLessons From The Past 5 Years Novel Combinations in Metastatic Breast Novel Combinations in Metastatic Breast
CancerCancer
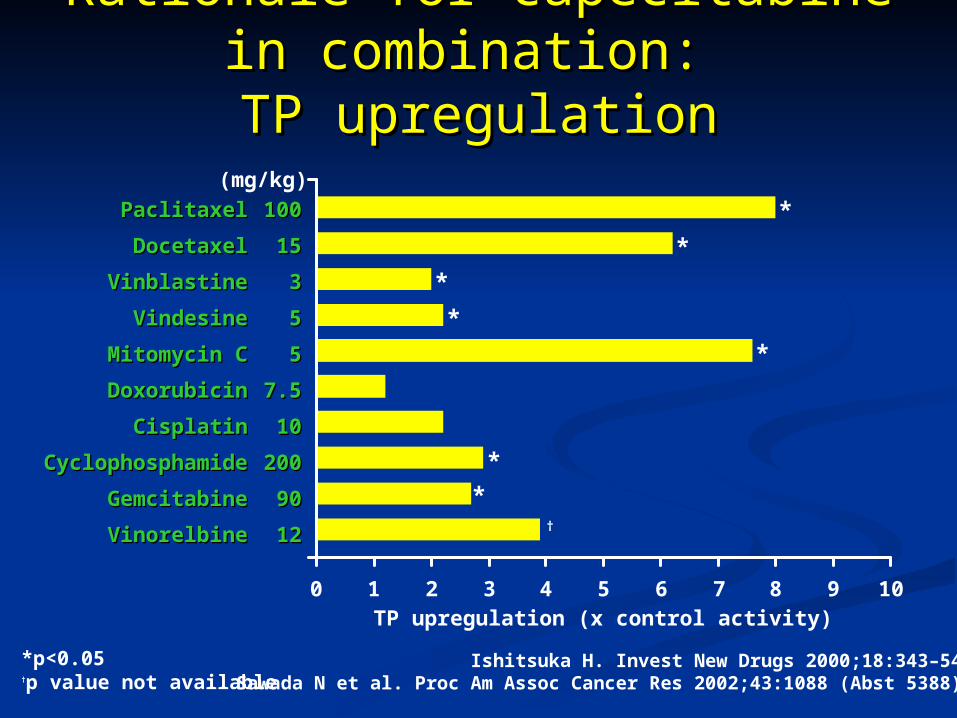
Rationale for capecitabine in Rationale for capecitabine in combination: combination:
TP upregulationTP upregulation
PaclitaxelPaclitaxel 100100
DocetaxelDocetaxel 1515
VinblastineVinblastine 33
VindesineVindesine 55
Mitomycin CMitomycin C 55
DoxorubicinDoxorubicin 7.57.5
CisplatinCisplatin 1010
CyclophosphamideCyclophosphamide 200200
GemcitabineGemcitabine 9090
VinorelbineVinorelbine 1212
0 1 2 3 4 5 6 7 8 9 10
*
*
*
*
*
*
*†
*p<0.05†p value not available
TP upregulation (x control activity)
Ishitsuka H. Invest New Drugs 2000;18:343–54Sawada N et al. Proc Am Assoc Cancer Res 2002;43:1088 (Abst 5388)
(mg/kg)
Taxanes in Breast Cancer
1.1. Better schedulingBetter scheduling
2.2. Dose – Dense programsDose – Dense programs
3.3. Synergy with other drugsSynergy with other drugs
4.4. Synergy with biological therapySynergy with biological therapy
5.5. Predict benefitPredict benefit
6.6. Newer generation of Taxanes Newer generation of Taxanes
How to Improve Outcome ??How to Improve Outcome ??
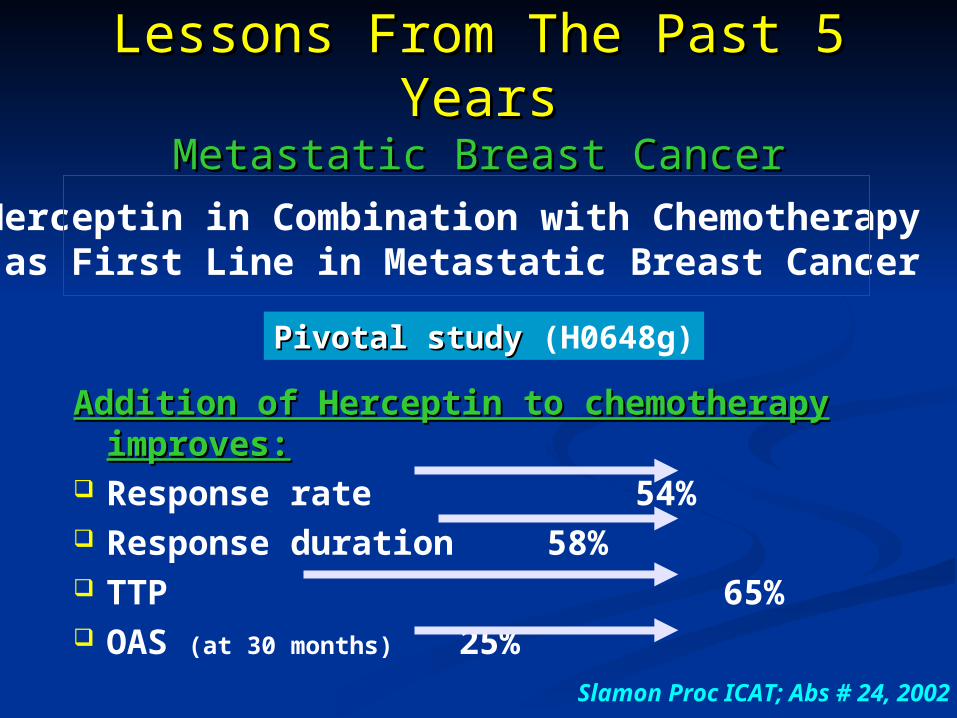
Addition of Herceptin to chemotherapy Addition of Herceptin to chemotherapy improves:improves:
Response rate 54% Response duration 58% TTP 65% OAS (at 30 months) 25%
Slamon Proc ICAT; Abs # 24, 2002
Pivotal study Pivotal study (H0648g)
Herceptin in Combination with Chemotherapy as First Line in Metastatic Breast Cancer
Lessons From The Past 5 Lessons From The Past 5 YearsYears
Metastatic Breast CancerMetastatic Breast Cancer
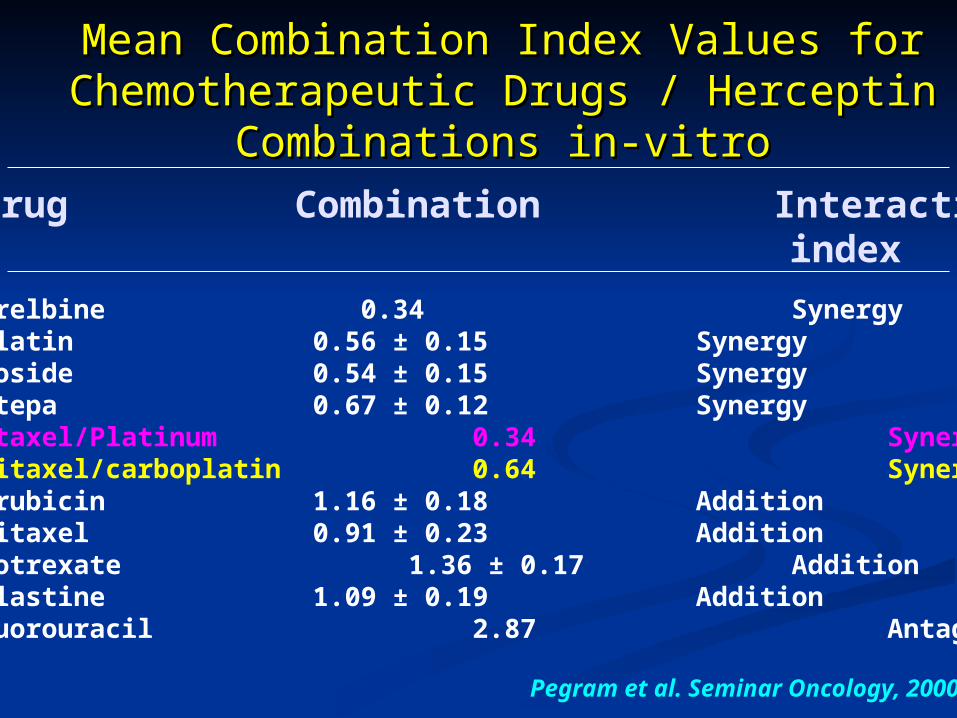
Mean Combination Index Values for Mean Combination Index Values for Chemotherapeutic Drugs / Herceptin Chemotherapeutic Drugs / Herceptin
Combinations in-vitroCombinations in-vitro Drug Combination Interaction index
Vinorelbine 0.34 SynergyCisplatin 0.56 ± 0.15 SynergyEtoposide 0.54 ± 0.15 SynergyThiotepa 0.67 ± 0.12 SynergyDocetaxel/Platinum 0.34 SynergyPaclitaxel/carboplatin 0.64 SynergyDoxorubicin 1.16 ± 0.18 AdditionPaclitaxel 0.91 ± 0.23 AdditionMethotrexate 1.36 ± 0.17 AdditionVinblastine 1.09 ± 0.19 Addition5-fluorouracil 2.87 Antagonism
Pegram et al. Seminar Oncology, 2000

Advanced Breast CancerFirst Line
HER2 +HER2 +
TP Paclitaxel 175 mg/m2 q 21d
TPC Paclitaxel 175 mg/m2/Carboplatin (AUC 6) q 21d
Trastuzumab until progression
Trastuzumab until progression
Roberts et al; SABCC 2002
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3 6 9 12 15 18 21 24 27 30 33 36
Months
Pro
gres
sion
Fre
e
P=0.007
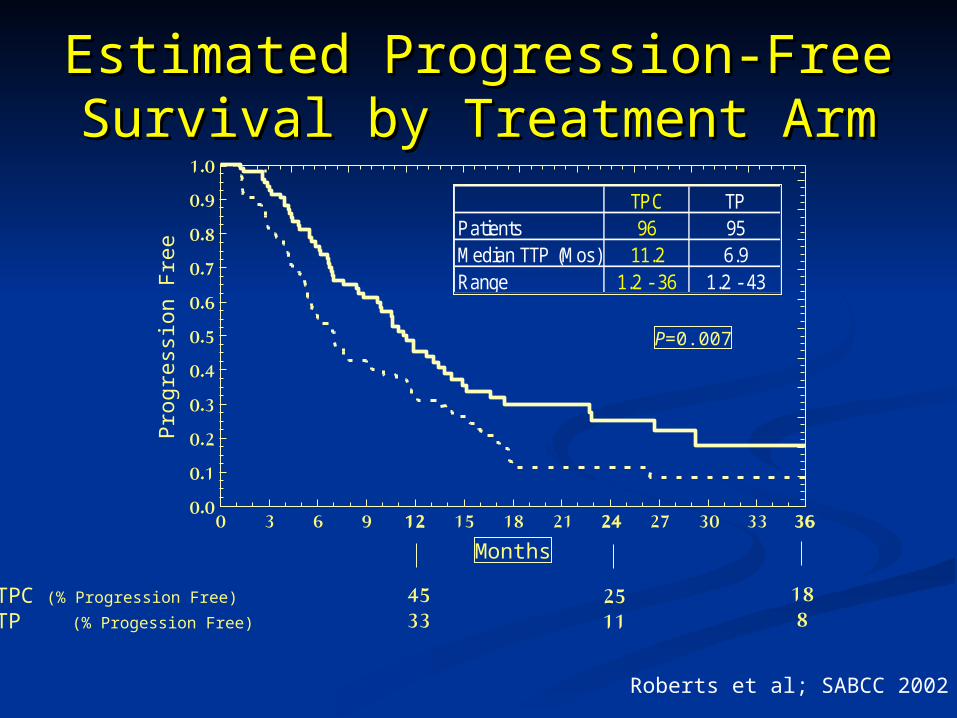
Estimated Progression-Free Estimated Progression-Free Survival by Treatment ArmSurvival by Treatment Arm
TPC (% Progression Free)
TP (% Progession Free)
4533
2511
18 8
TPC TPPatients 96 95Median TTP (Mos) 11.2 6.9Range 1.2 - 36 1.2 - 43
Roberts et al; SABCC 2002

ConclusionsConclusions• The addition of Carboplatin to TP significantly
increases the overall response and time to progression
RRRR
TTPTTP
TP3+TP3+TPCTPC TPC3+TPC3+
37%52% 57%
7.2 mo11.2 mo 13.5 mo
TPTP
36%
6.9 mo
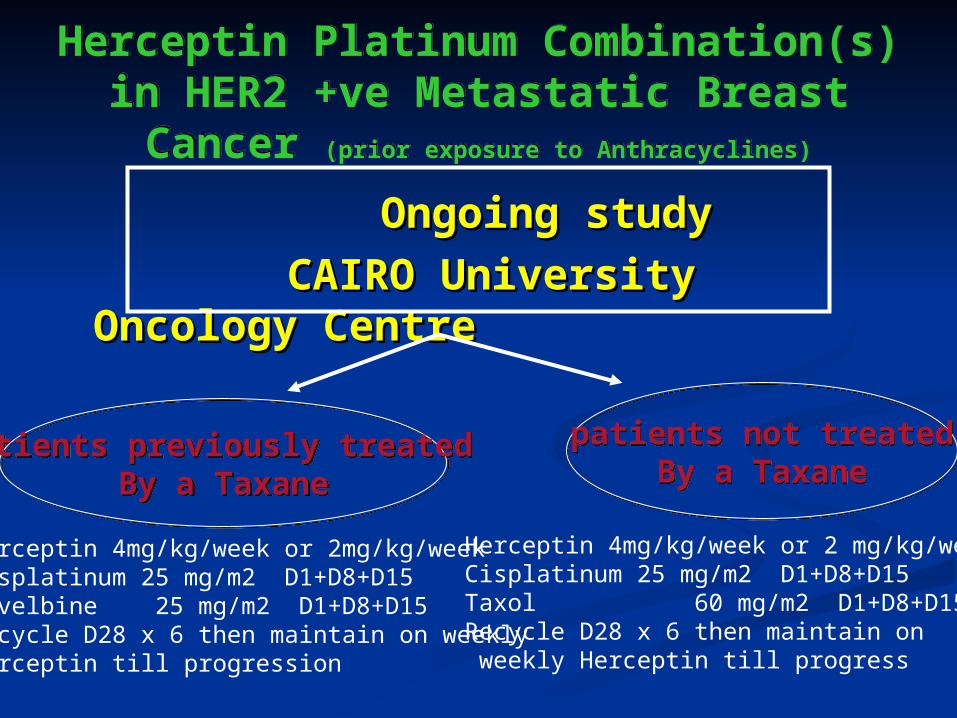
Herceptin Platinum Combination(s) in HER2 +ve Metastatic Breast
Cancer (prior exposure to Anthracyclines)
Herceptin Platinum Combination(s) in HER2 +ve Metastatic Breast
Cancer (prior exposure to Anthracyclines)
Ongoing study Ongoing study
CAIRO University Oncology CAIRO University Oncology CentreCentre
Herceptin 4mg/kg/week or 2mg/kg/weekCisplatinum 25 mg/m2 D1+D8+D15Navelbine 25 mg/m2 D1+D8+D15 Recycle D28 x 6 then maintain on weekly Herceptin till progression
Herceptin 4mg/kg/week or 2 mg/kg/weekCisplatinum 25 mg/m2 D1+D8+D15Taxol 60 mg/m2 D1+D8+D15Recycle D28 x 6 then maintain on weekly Herceptin till progress
patients previously treated By a Taxane
patients previously treated By a Taxane
patients not treatedBy a Taxane
patients not treatedBy a Taxane
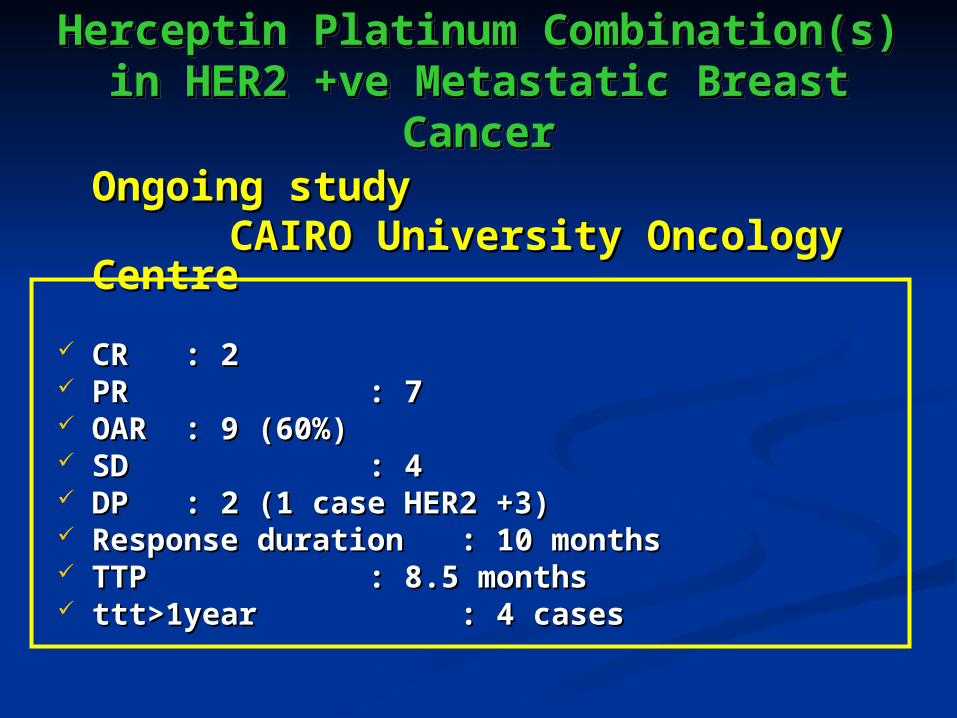
Herceptin Platinum Herceptin Platinum Combination(s) in HER2 +ve Combination(s) in HER2 +ve
Metastatic Breast CancerMetastatic Breast Cancer
Herceptin Platinum Herceptin Platinum Combination(s) in HER2 +ve Combination(s) in HER2 +ve
Metastatic Breast CancerMetastatic Breast CancerOngoing study Ongoing study
CAIRO University Oncology CAIRO University Oncology CentreCentre
CR CR : 2: 2 PR PR : 7: 7 OAROAR : 9 (60%): 9 (60%) SD SD : 4: 4 DP DP : 2 (1 case HER2 +3): 2 (1 case HER2 +3) Response duration Response duration : 10 months: 10 months TTP TTP : 8.5 months: 8.5 months ttt>1yearttt>1year : 4 cases: 4 cases
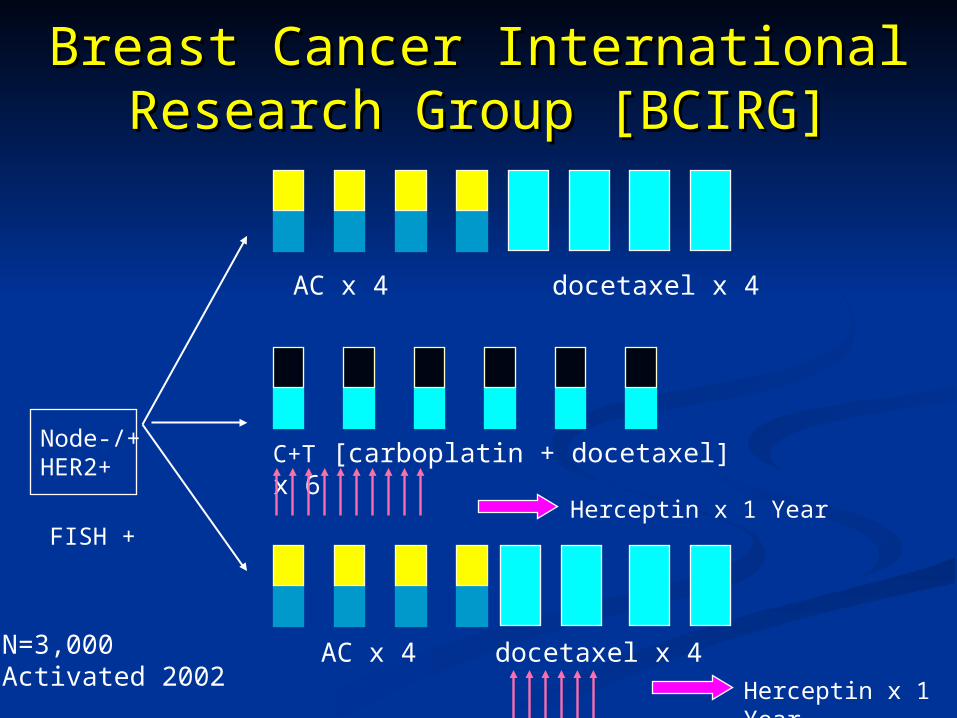
Breast Cancer International Breast Cancer International Research Group [BCIRG]Research Group [BCIRG]
Node-/+HER2+
AC x 4 docetaxel x 4
C+T [carboplatin + docetaxel] x 6
Herceptin x 1 Year
AC x 4 docetaxel x 4
Herceptin x 1 Year
N=3,000Activated 2002
FISH +
Taxanes in Breast Cancer
1.1. Better schedulingBetter scheduling
2.2. Dose – Dense programsDose – Dense programs
3.3. Synergy with other drugsSynergy with other drugs
4.4. Synergy with biological therapySynergy with biological therapy
5.5. Predict benefitPredict benefit
6.6. Newer generation of Taxanes Newer generation of Taxanes
How to Improve Outcome ??How to Improve Outcome ??
Design of Design of Treatment Treatment
According to According to Molecular Profile Molecular Profile
of the Diseaseof the Disease
FUTUR PROMISES
Design of treatment according to molecular profile of the disease
CHANGINGCONCEPTS
• ? Need for adequate doses of Anthracycline • ? Need for a Taxane
• Need for Herceptin in metastatic phase ?adjuvant phase
• Herceptin synergy with other drugs
HER2/neu+ve
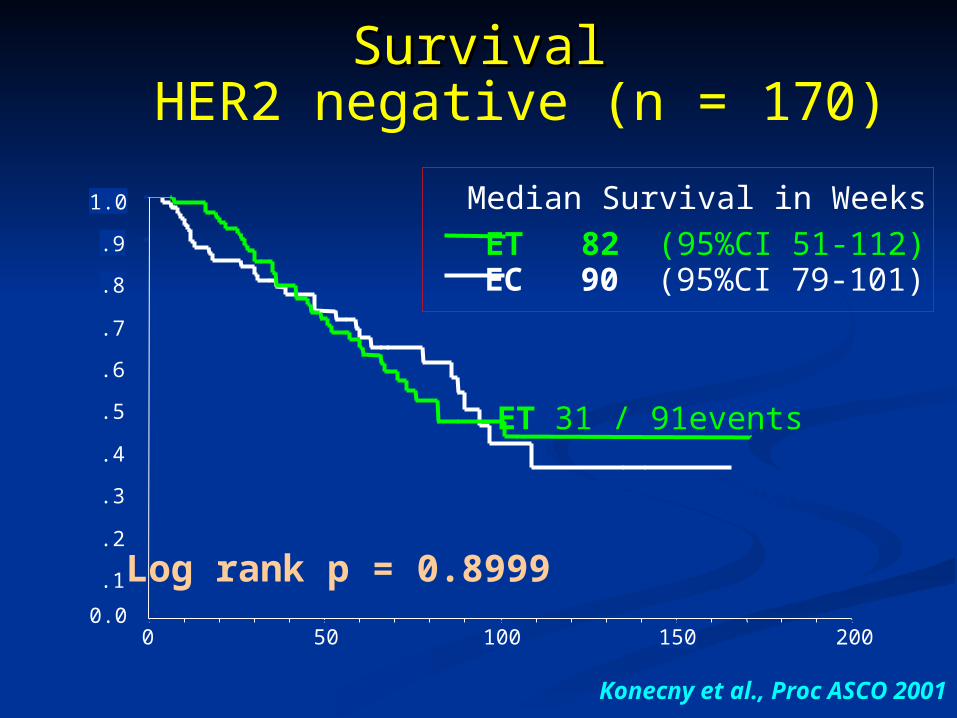
SurvivalSurvivalHER2 negative (n = 170)
ET 82 (95%CI 51-112) EC 90 (95%CI 79-101)
Median Survival in Weeks
200150100500
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
Log rank p = 0.8999
ET 31 / 91events
EC 29 / 79 events
Weeks
Cu
m S
urv
ival
Konecny et al., Proc ASCO 2001

200150100500
HER2 positive (n =102)
ET 103 (95%CI 64-142) EC 56 (95%CI 41-71)
Median Survival in Weeks
SurvivalSurvival
ET 14 / 49 events
EC 27 / 53 events
Log rank p = 0.035
Weeks
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
Cu
m S
urv
ival
Konecny et al. Proc ASCO, 2001
TAC
FAC
0 12 24 36 48Months
N at RiskTACFAC
485 467 433 102 1478 455 402 108 0
40
50
60
70
80
90
100
% A
live
an
d D
ise
ase
Fre
e
TAC
FAC
0 12 24 36 48Months
N at RiskTACFAC
138 131 118 32 0148 135 107 26 0
40
50
60
70
80
90
100
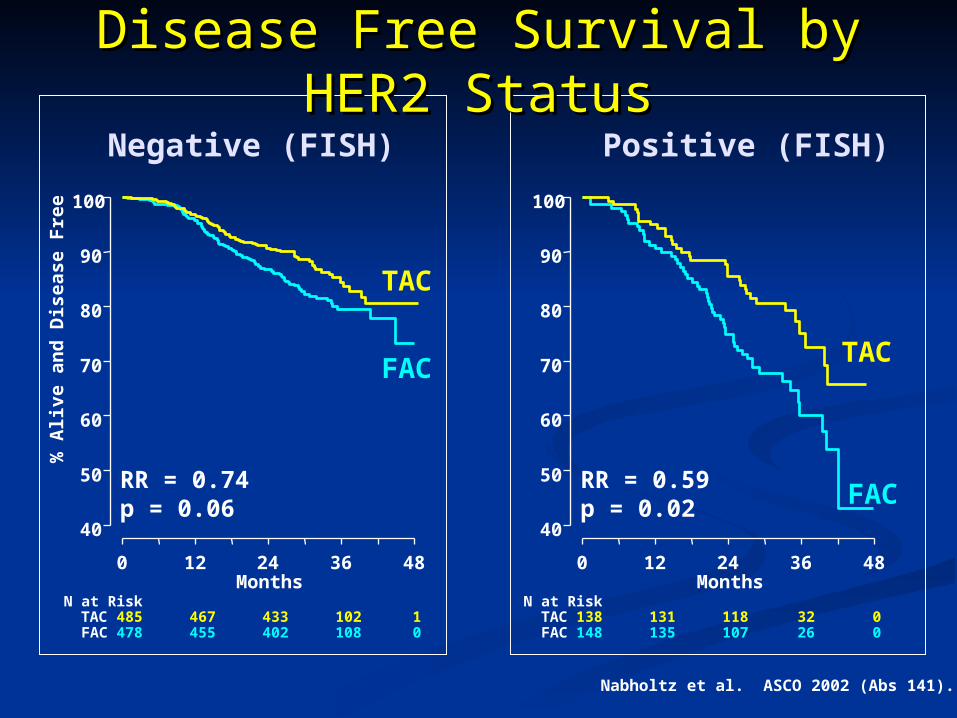
Disease Free Survival by Disease Free Survival by HER2 StatusHER2 Status
Negative (FISH) Positive (FISH)
RR = 0.74p = 0.06
RR = 0.59p = 0.02
Nabholtz et al. ASCO 2002 (Abs 141).

CHANGINGCHANGINGCONCEPTSCONCEPTS
Design of treatment according to molecular profile of the disease
• ?? Resistance to Anthracycline
• ?? Sensitivity to Taxanes
Mutant P53

Taxol induced rapid onset of P53Independent apoptotic pathway
Taxanes may induce tumor cell apoptosis independent on P53 status
Lanni et cell biology;1997
Wood et al Mol Med;1995
A potential for Predictive A potential for Predictive Value of P53Value of P53
Patients with P53 deficient tumors may benefit
from Paclitaxel
Kandiokr-Eckersberger Clin CancerRes;2000

Anthracycline and radiation therapy requireIntact P53 for efficient tumor cell death
P53 mutations are associated with de novo resistance to Anthracyclines
In breast cancer patients
Lawe et cell biology;1993
Aas et al Nat Med;1996

CHANGINGCHANGINGCONCEPTSCONCEPTS
Design of treatment according to molecular profile of the disease
• SensitivityTo
Anthracycline
Overexpression of Topo II
Taxanes in Breast Cancer
1.1. Better schedulingBetter scheduling
2.2. Dose – Dense programsDose – Dense programs
3.3. Synergy with other drugsSynergy with other drugs
4.4. Synergy with biological therapySynergy with biological therapy
5.5. Predict benefitPredict benefit
6.6. Newer generation of TaxanesNewer generation of Taxanes
How to Improve Outcome ??How to Improve Outcome ??

Taxane resistant Pat-21 breast cancerTaxane resistant Pat-21 breast cancer
Novel epothilone BMS-Novel epothilone BMS-247550: 247550:
Activity against clinical taxane Activity against clinical taxane resistanceresistance
Rx
Time post tumor implantation (days)
Rx
ControlPaclitaxel (36 mpk x5)
BMS-247550 (10 mpk x3)
Me
dia
n t
um
or
we
igh
(m
g)
10
100
1000
40 50 60 70 80
Years0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8 2
Pat-21(Breast)
Biopsied
ADR + CMF (10 cycles)TAXOL + Dexverapamil
(4 cycles)
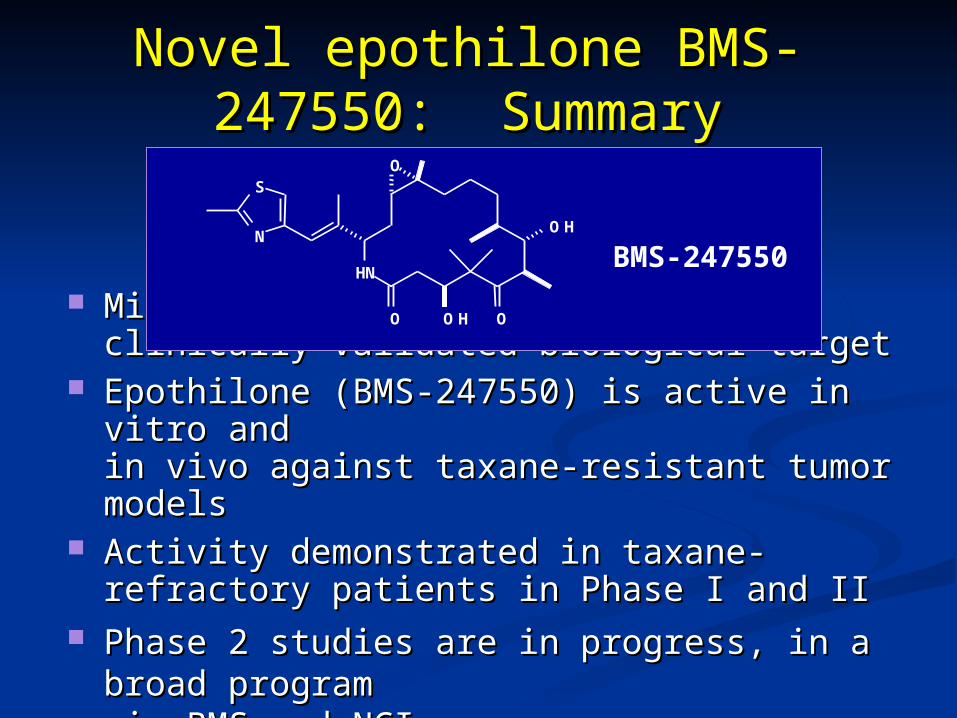
Microtubule stabilization is a clinically Microtubule stabilization is a clinically validated biological target validated biological target
Epothilone (BMS-247550) is active in vitro Epothilone (BMS-247550) is active in vitro and and in vivo against taxane-resistant tumor modelsin vivo against taxane-resistant tumor models
Activity demonstrated in taxane-refractory Activity demonstrated in taxane-refractory patients in Phase I and IIpatients in Phase I and II
Phase 2 studies are in progress, in a broad Phase 2 studies are in progress, in a broad program program via BMS and NCI via BMS and NCI
Novel epothilone BMS-Novel epothilone BMS-247550: Summary247550: Summary
HN
O
O
O H
O H
S
N
O
BMS-247550
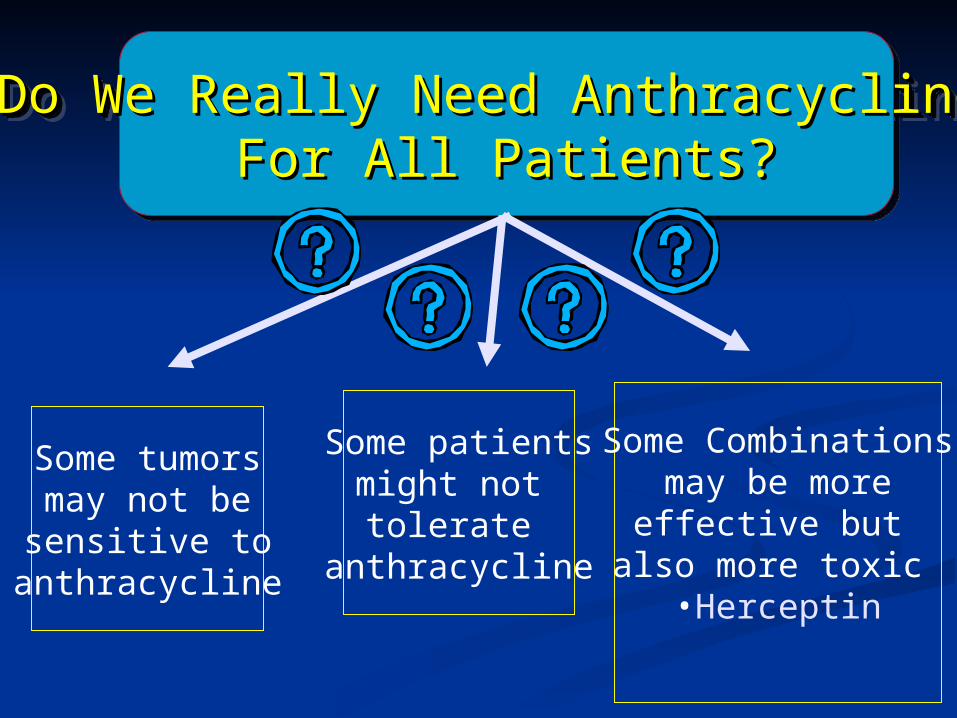
Do We Really Need Anthracycline Do We Really Need Anthracycline For All Patients?For All Patients?
Do We Really Need Anthracycline Do We Really Need Anthracycline For All Patients?For All Patients?
Some tumorsmay not besensitive to
anthracycline
Some patientsmight not tolerate
anthracycline
Some Combinationsmay be moreeffective but
also more toxic •Herceptin
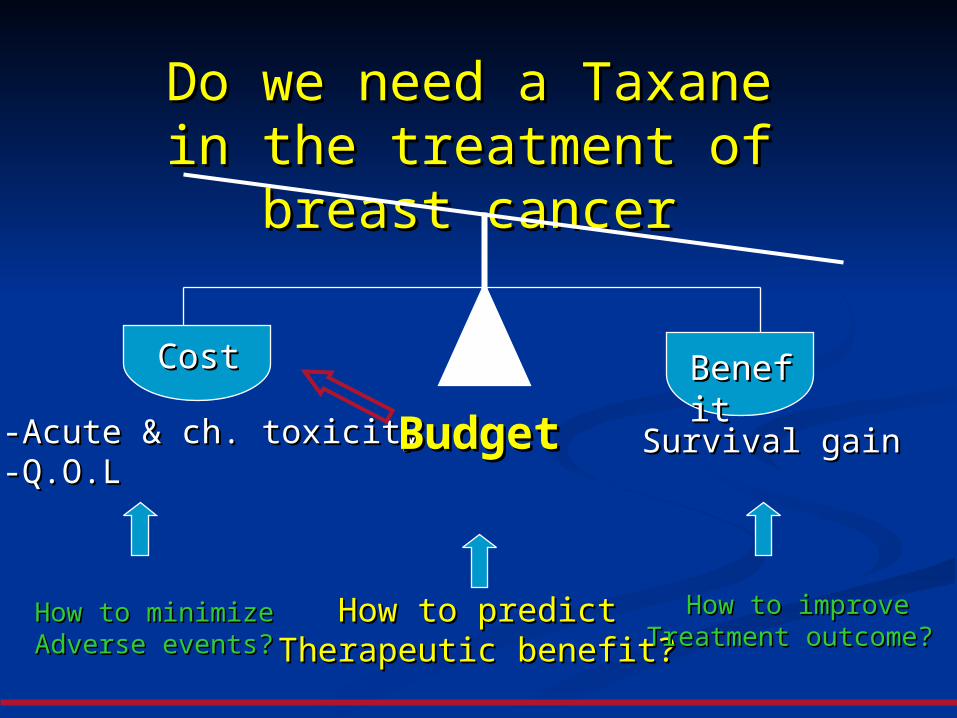
Do we need a Taxane in Do we need a Taxane in the treatment of breast the treatment of breast
cancercancer
CostCost BenefitBenefit
-Acute &-Acute & ch.ch. toxicitytoxicity-Q.O-Q.O..LL
Survival gainSurvival gain
How to minimizeHow to minimizeAdverse events? Adverse events?
How to predictHow to predictTherapeutic benefit?Therapeutic benefit?
BudgetBudget
How to improveHow to improveTreatment outcome? Treatment outcome?