tb nurse case management - heartland national … · tb nurse case management san antonio, texas...
TRANSCRIPT

1
TB Nurse Case ManagementSan Antonio, Texas
December 8 10 2009December 8-10, 2009
Quality Improvement in Nurse Case Management
Lynelle Phillips RN MPHLynelle Phillips RN MPH
December 10, 2009
Quality Improvement in
Nurse Case Management
Lynelle Phillips RN MPHLynelle Phillips RN MPHTB Nurse Case Management Course
Heartland National TB CenterDecember 10, 2009

2
Outline• Identify methods of quality improvement in nurse case
management.P ti– Programmatic
• National TB Indicators Project (NTIP)
• Cohort review
• Program assessment
• After Action Reviews
– Nurse Case Management Quality Assurance• NCM case reviews
• NCM Goal Matrix (NTNC)NCM Goal Matrix (NTNC)
• Staffing Standards (NTNC)
• Advantages and Disadvantages
• Resources
Case Management• “Case Management
provides critical servicesCase Management Model
Client
provides critical services to help patients and their caregivers navigate, coordinate, and transition through a dynamic approach to better
CaseManager
Assessment
Planning
FacilitationCoordination
EvaluationEmpowerment
Collaboration Problem Solving
Communication
Advocacy
ppachieve their health care goals.”
• Case Management Society of America, 2009
Case Management Society of America. Standards of Practice for Case Management. Little Rock, AR: CMSA; 1995
Provider Public Health

3

4

5
Case Management• “Case Management
provides critical servicesprovides critical services to help patients and their caregivers navigate, coordinate, and transition through a dynamic approach to better
Case Management ModelClient
Advocacyppachieve their health care goals.”
• Case Management Society of America, 2009
Case Management Society of America. Standards of Practice for Case Management. Little Rock, AR: CMSA; 1995
Provider Public Health
CaseManager
Assessment
Planning
FacilitationCoordination
EvaluationEmpowerment
Collaboration Problem Solving
Communication

6
• “Tuberculosis is a unique disease. For t th di d hi i imost other disorders, achieving cure is
primarily the patient’s concern. With TB, the responsibility for cure rests with the health care professional and ultimately with society.”
» Lee B Reichman, MD
National Tuberculosis Indicators Project (NTIP)
• Discuss utilizing surveillance data to evaluate program progress towards meeting objectives
– Where does data come from?
– Evaluation stepsp
– Assessing progress towards meeting objectives
Ijaz K, Young K, (2008)

7
What is the NTIP?
• Monitoring system– Track progress of US tuberculosis (TB) control– Track progress of US tuberculosis (TB) control
programs
• Provides progress reports to TB programs– Using data already reported to the CDC
• Helps prioritize:– Prevention and control activities (local and national)– Program evaluation
Ijaz K, Young K, (2008)
NTIP Rationale
• Program evaluation is essential to effectiveness of public health programseffectiveness of public health programs
• Limited resources available to TB programs
• NTIP makes efficient use of existing data to help prioritize program activities and evaluations
Ijaz K, Young K, (2008)

8
National TB Program Objectives
• 15 high-priority categories, selected by the CDC Division of Tuberculosis EliminationCDC Division of Tuberculosis Elimination (DTBE) and TB program representatives in 2006
• TB programs funded through cooperative agreements expected to report onagreements expected to report on progress toward all 15 categories starting in 2010
Ijaz K, Young K, (2008)
http://www.nyc.gov/html/doh/downloads/pdf/tb/tb-indicators-project-kai-young.pdf

9
http://www.cdc.gov/TB/Program_Evaluation/Indicators/default.htm
http://www.cdc.gov/TB/Program_Evaluation/Indicators/default.htm

10
http://www.cdc.gov/TB/Program_Evaluation/Indicators/default.htm
http://www.nyc.gov/html/doh/downloads/pdf/tb/tb-indicators-project-kai-young.pdf

11
http://www.nyc.gov/html/doh/downloads/pdf/tb/tb-indicators-project-kai-young.pdf
http://www.nyc.gov/html/doh/downloads/pdf/tb/tb-indicators-project-kai-young.pdf

12
http://www.nyc.gov/html/doh/downloads/pdf/tb/tb-indicators-project-kai-young.pdf
http://www.nyc.gov/html/doh/downloads/pdf/tb/tb-indicators-project-kai-young.pdf

13
INDICATOR YEAR CURRENT STATEWIDE NATIONAL MOYEAR OBJECTIVE OBJECTIVE DATA
*2004 dataGOAL: Ensure early identification and reporting of all persons with tuberculosis.TB Case Rate 2005 3.4 0.5 0.5 1.9Reported within 2 weeks diagnosis 2005 100% 85% 85% nap gGOAL: All TB patients complete treatmentRecommended Initial Therapy 2005 100% na na 92%HIV testing for 25-44 year olds 2005 100% 90% 75% 82%Culture Conversion 2005 100% na na 76%*Appropriate DOT 2005 100% na na 77%*Timely completion of therapy within 12 months 2005 88% 95% 90% 91%*GOAL: Prevent TB transmissionContact Identification 2005 100% 90% 90% 97%C t t E l ti 2005 92% 100% 95% 64%Contact Evaluation 2005 92% 100% 95% 64%Contact Treatment Initiation 2005 93% na na 79%Contact Treatment Completion 2005 84% 60% 85% 63%*GOAL: Reduce the occurance of sentinel events.Pediatric TB Cases 2005 0% na na 3%TB Deaths 2005 33% na na 12%
INDICATOR YEAR CURRENT STATEWIDE NATIONAL MOYEAR OBJECTIVE OBJECTIVE DATA
*2004 dataGOAL: Ensure early identification and reporting of all persons with tuberculosis.TB Case Rate 2005 3.4 0.5 0.5 1.9Reported within 2 weeks diagnosis 2005 100% 85% 85% naGOAL: All TB patients complete treatmentRecommended Initial Therapy 2005 100% na na 92%HIV testing for 25-44 year olds 2005 100% 90% 75% 82%Culture Conversion 2005 100% na na 76%*Appropriate DOT 2005 100% na na 77%*Timely completion of therapy within 12 months 2005 88% 95% 90% 91%*GOAL: Prevent TB transmissionContact Identification 2005 100% 90% 90% 97%Contact Evaluation 2005 92% 100% 95% 64%Contact Evaluation 2005 92% 100% 95% 64%Contact Treatment Initiation 2005 93% na na 79%Contact Treatment Completion 2005 84% 60% 85% 63%*GOAL: Reduce the occurance of sentinel events.Pediatric TB Cases 2005 0% na na 3%TB Deaths 2005 33% na na 12%

14
INDICATOR YEAR CURRENT STATEWIDE NATIONAL MO
YEAR OBJECTIVE OBJECTIVE DATA
*provisional *2004 dataGOAL: Ensure early identification and reporting of all persons with tuberculosis.TB Case Rate 6.1 0.5 0.5 1.9Reported within 2 weeks diagnosis 100% 85% 85% naReported within 2 weeks diagnosis 100% 85% 85% naGOAL: All TB patients complete treatmentRecommended Initial Therapy 100% na na 92%HIV testing for 25-44 year olds 100% 90% 75% 82%Culture Conversion 67% na na 76%*Appropriate DOT 93% na na 77%*Timely completion of therapy within 12 months 100%* 95% 90% 91%*GOAL: Prevent TB transmissionContact Identification 93% 90% 90% 97%C t t E l ti 48% 100% 95% 64%Contact Evaluation 48% 100% 95% 64%Contact Treatment Initiation 100% na na 79%Contact Treatment Completion 60% 60% 85% 63%*GOAL: Reduce the occurance of sentinel events.Pediatric TB Cases 4% na na 3%TB Deaths 4% na na 12%
INDICATOR YEAR CURRENT STATEWIDE NATIONAL MO
YEAR OBJECTIVE OBJECTIVE DATA
*provisional *2004 dataGOAL: Ensure early identification and reporting of all persons with tuberculosis.TB Case Rate 6.1 0.5 0.5 1.9Reported within 2 weeks diagnosis 100% 85% 85% naReported within 2 weeks diagnosis 100% 85% 85% naGOAL: All TB patients complete treatmentRecommended Initial Therapy 100% na na 92%HIV testing for 25-44 year olds 100% 90% 75% 82%Culture Conversion 67% na na 76%*Appropriate DOT 93% na na 77%*Timely completion of therapy within 12 months 100%* 95% 90% 91%*GOAL: Prevent TB transmissionContact Identification 93% 90% 90% 97%C t t E l ti 48% 100% 95% 64%Contact Evaluation 48% 100% 95% 64%Contact Treatment Initiation 100% na na 79%Contact Treatment Completion 60% 60% 85% 63%*GOAL: Reduce the occurance of sentinel events.Pediatric TB Cases 4% na na 3%TB Deaths 4% na na 12%

15
Potential problems?• Difficult/high acuity patients
– “..it will likely become more difficult to treat patients…because of their social situations and ptreatment will be more labor intensive..the complexity of investigations will increase” IOM (2000)
• Training need– “…key challenge will be to maintain competency..”
IOM (2000)
• Not enough staff– “ …develop strategies for ensuring that resources for
TB elimination are available, despite a diminishing and unpredictable demand for services. IOM (2000)
• Management issues
• Unmotivated/morale problem
Drilling down….
• Evaluation process– Cohort review
– Program Assessments
• Nurse case management quality assurance– Case management review– Case management review
– Goal Matrix evaluation
– Staffing Standards
16
What is Cohort Review (1)
• Cohort review is a systematic review of patients with tuberculosis (TB) disease andpatients with tuberculosis (TB) disease and their contacts.
• A “cohort” is a group of TB cases identified over a specific period of time, usually 3 months.
• The cases are reviewed approximately 6 - 9 months after they are reported, so that many of the patients have completed or are nearing the end of treatment.
http://www.harlemtbcenter.org/cohort_review.htm
What is Cohort Review (2)
TB cases are reviewed in a group setting with g p gthe following information presented on each case by the case manager:
• Patient's demographic information• Patient’s status: clinical, lab, radiology• Drug regimen, adherence, completiong g , , p• Results of contact investigation
http://www.harlemtbcenter.org/cohort_review.htm

17
What is Cohort Review (3)
• Individual outcomes are assessedIndividual outcomes are assessed
• Group outcomes are also assessed
– Indicators track progress toward national, state, and local program objectives.
– Everyone leaves the meeting knowing the results.
http://www.harlemtbcenter.org/cohort_review.htm
RolesTB Program
Manager
Medical Reviewer
Data Ana lyst
Supervisor
Case Manager
Outreach Staff
DOT Staff
Community Providers
TB Contro l Cohort Review Team Members
TB Contro l Support S taff and Community Providers

18
Timeline1ST QUARTER
JAN FEB MAR
2ND QUARTER
APR MAY JUN
3RD QUARTER
JUL AUG SEP
4TH QUARTER
OCT NOV DEC
1ST QUARTER
JAN FEB MAR
2ND QUARTER
APR MAY JUN
• TB cases identified
• Treatment started
• Contact investigation initiated
• Ongoing treatment of patients with TB disease
• Contacts evaluated and started on treatment, as necessary
• TB disease treatment completed
• Infected contacts continue on treatment for LTBI
1st quarter contacts complete treatment
COHORT • Continue follow up on issues CO OREVIEW SESSION
• Begin follow up on issues identified
Co t ue o o up o ssuesidentified during cohort review session
• Treatment completion rate presented for contacts of cases from previous 1st quarter
Timeline1ST QUARTER
JAN FEB MAR
2ND QUARTER
APR MAY JUN
3RD QUARTER
JUL AUG SEP
4TH QUARTER
OCT NOV DEC
1ST QUARTER
JAN FEB MAR
2ND QUARTER
APR MAY JUN
• TB cases identified
• Treatment started
• Contact investigation initiated
• Ongoing treatment of patients with TB disease
• Contacts evaluated and started on treatment, as necessary
• TB disease treatment completed
• Infected contacts continue on treatment for LTBI
1st quarter contacts complete treatment
COHORT • Continue follow up on issues CO OREVIEW SESSION
• Begin follow up on issues identified
Co t ue o o up o ssuesidentified during cohort review session
• Treatment completion rate presented for contacts of cases from previous 1st quarter

19
Essential Elements
Cohort Review ProcessPreparation Presentation Follow up
http://www.harlemtbcenter.org/cohort_review.htm
Essential Elements of the Cohort Review Process
What are you already doing?YES
NO
What may need to be enhanced in order to conduct a cohort review:
1. Preparation
Ensuring that TB program staff know TB program objectives
Delineate local and regional objectives for your program Communicate these objectives to all TB program staff
Using a comprehensive case management system
Ensure that case management protocols are clearly written, comprehensive and practical for staff to implement
Using a reliable TB registry Specify data elements that need to be collected to evaluate program objectives Ensure that staff update registry information regularly Use the registry to generate cohort lists for TB control team members
Carefully preparing cases for presentation
Use periodic case reviews to ensure that case and contact information needed for the cohort review is collected Consider adding practice sessions to hone case presentation skills Implement a standard presentation format to ensure consistent, concise and complete presentations

20
2. Presentation
Present each case in detail to the TB control team
Allow team members sufficient time to analyze and evaluate TB cases and contact investigations
Providing on-the-spot feedback to staff, aggregate reporting, and troubleshooting
Allow time for troubleshooting of case management issues Develop a standard format for aggregate reporting of data
3. Follow up
Follo p of identified Team members use information gathered at cohort Follow up of identified problems
Team members use information gathered at cohort to follow up on cases/contact investigations, identify staff training issues, and solve programmatic problems
Cohort Review ProcessWhat is Evaluated?
• Current status of each patientCurrent status of each patient– Cured or current to care and likely to complete in 365 days– Died, moved, lost, refused treatment or unlikely to complete
treatment within 365 days– Directly Observed Treatment (DOT) status and compliance
to DOT– Review of contact or source case investigation
• Measurable resultsMeasurable results– Completion of treatment within 365 days– Contact index– Contact evaluation and outcome of those on treatment of
LTBI
http://www.harlemtbcenter.org/cohort_review.htm

21
Cohort Review Process Goals
• Evaluate process of public health intervention to:intervention to:– ensure appropriate regimen used– ensure timely treatment completion– improve timeliness of interventions– shorten time between contact identification
and testingand testing– improve management of infected contacts– analyze outcome to develop appropriate
interventionshttp://www.harlemtbcenter.org/cohort_review.htm
Cohort Review Approach
• Most important meeting of TB program
L t h b d b h d• Low tech, can be done by hand
• Closely linked to CDC objectives
• Group process
• Every one leaves meeting knowing results
• Teaching opportunityg pp y
• Gives director feeling for current issues
http://www.harlemtbcenter.org/cohort_review.htm

22
Cohort Review Process Strengths
• Informational and systematic– Director reviews every caseDirector reviews every case
• TB staff collaboration• Public accountability for case management and follow-up
of contacts• National objectives tracked• Can be modified to add/delete items as needed• Consistent with global principles of TB control• Consistent with global principles of TB control
http://www.harlemtbcenter.org/cohort_review.htm
Cohort Review Process Limitations
• Retrospective• Retrospective – Timeliness of some aspects of care cannot be assessed– May be too late to make interventions– Monday-morning quarterbacking dynamic
• Details of problems in case management cannot be addressed
• Several items we want to evaluate are not easily captured in TB Registry– e.g. Non adherent contacts, mental health issues

23
Program Assessments
• Annual
• Typically for high morbidity areas
• Formal report process
• Assessment team
• Independent reviewers included on team– State advisory committee
TB Case Rates by Area 1991-2005cases per 100,000
TB Case Rates by Area 1991-2005cases per 100,000
16
18 MissouriSt. Louis County
2
4
6
8
10
12
14
16 St. Louis CountySt. Louis CityKansas CitySpfd/Grn
0
2
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005

24
Program Assessment Format
• Assessment tool
• Process– Jurisdiction prepares report
– In-person review between state/regional staff and jurisdiction
• Team of reviewers
– Reviewers prepare a report with recommendations
Sample of Program AssessmentIII. SURVEILLANCE (LTBI AND DISEASE)1.What is the number and percentage of new cases reported within 24 – 72 hours from time of suspected diagnosis or positive laboratory result obtained? , %
2. HIV and TB2. HIV and TBa) Number and percentage of patients co-infected with TB/HIV: , %(b)Number of patients age 25-44 offered testing for HIV:(c)Number of patients age 25-44who accepted testing for HIV: • Number of any age patient offered testing for HIV: • Number of any age patient who accepted testing for HIV: • What is your policy on HIV counseling:
3.This is what the state shows for your risk groups. Please verify.
4. How do you share surveillance data with local medical professionals and community leaders?
5. Number of TB cases reported by:i h i i•Private Physicians:
•Hospitals: •Laboratories: •Other (please name):
6. Number of TB cases provided nursing case management by the local TB program: 7. The DHSS TB Program performs preventable case/death analysis on all TB cases.8. The number of preventable cases for your area. # and %.

25
Strengths/Limitations
• Strengths– Build rapport/mutual respect between state and local staffpp p– Therapeutic– Opportunity to problem solve – understand problems more
thoroughly• Say what needs to be said
– Learning experience
• Limitations– Formalo a– Potentially threatening– Labor intensive– Aggregate information only
TB Case Rates by Area 1991-2005cases per 100,000
TB Case Rates by Area 1991-2005cases per 100,000
16
18 MissouriSt Louis County
2
4
6
8
10
12
14
16 St. Louis CountySt. Louis CityKansas CitySpfd/Grn
0
2
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
26
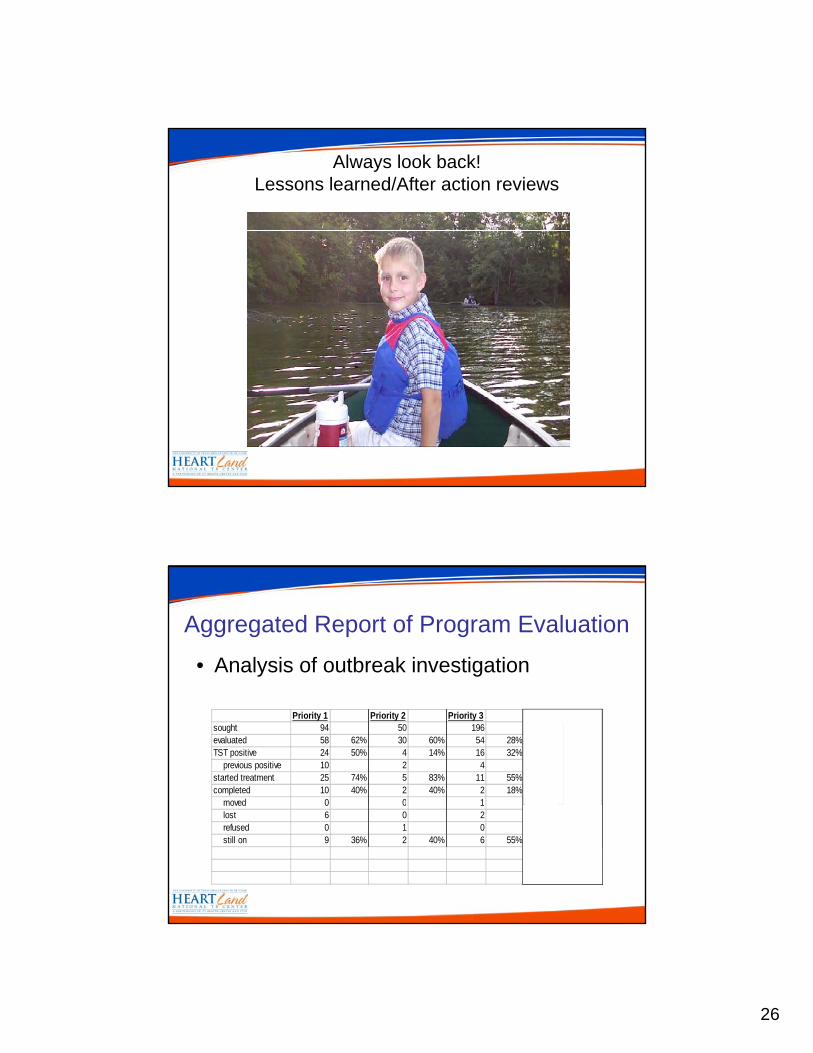
Always look back!Lessons learned/After action reviews
Aggregated Report of Program Evaluation
• Analysis of outbreak investigation
Priority 1 Priority 2 Priority 3 Employees onlysought 94 50 196 65evaluated 58 62% 30 60% 54 28% 20 31%TST positive 24 50% 4 14% 16 32% 7 37% previous positive 10 2 4 1started treatment 25 74% 5 83% 11 55% 6 75%completed 10 40% 2 40% 2 18% 1 17%
moved 0 0 1 0 moved 0 0 1 0 lost 6 0 2 2 refused 0 1 0 0 still on 9 36% 2 40% 6 55% 3 50%

27
Aggregated Report of Program Evaluation
• Analysis of outbreak investigation
One's Two's Three's Employees onlysought 94 50 196 65evaluated 58 62% 30 60% 54 28% 20 31%TST positive 24 50% 4 14% 16 32% 7 37% previous positive 10 2 4 1started treatment 25 74% 5 83% 11 55% 6 75%completed 10 40% 2 40% 2 18% 1 17%
moved 0 0 1 0 moved 0 0 1 0 lost 6 0 2 2 refused 0 1 0 0 still on 9 36% 2 40% 6 55% 3 50%
Aggregated Report of Program Evaluation
• Analysis of outbreak investigation
One's Two's Three's Employees onlysought 94 50 196 65evaluated 58 62% 30 60% 54 28% 20 31%TST positive 24 50% 4 14% 16 32% 7 37% previous positive 10 2 4 1started treatment 25 74% 5 83% 11 55% 6 75%completed 10 40% 2 40% 2 18% 1 17%
moved 0 0 1 0 moved 0 0 1 0 lost 6 0 2 2 refused 0 1 0 0 still on 9 36% 2 40% 6 55% 3 50%

28
Lessons learned
• Reprioritized contacts b dbased on investigation results
• Abandoned field-search for contacts
• Emphasized active• Emphasized active surveillance at the jail.
Looking back – you’ll be glad you did!
• Regroup and document whatdocument what worked and what did not work– All participants
• Lessons learned -implement changeimplement change for the next investigation

29
Case Management Evaluation
• Periodic / routine case management ti ith l lmeeting with local nurse case managers
• Snap shot of cases at the time of the meeting– Individual report of cases
• Real time problem solving of barriers to• Real-time problem solving of barriers to treatment or isolation adherence and contact investigation problems.
Assessment essentials
• Patient name or identifier/history
Cli i l• Clinical– TST
– CXR - improvement
– Bacteriology – smear/culture conversion
– Med regimen – appropriate/tolerated/adherence
B i t t t t/i l ti• Barriers to treatment/isolation
• Contacts – barriers to contact investigation

30
Case Management Format
Name/Identifier and history
Follow-up
Actions:
TST/IGRA
CXR
Bacteriology
Meds
Contacts
Barriers
Case Management Model• Advantages
– Opportunity to build rapport with TB case managers– Real-time problem solvingReal time problem solving– Share information and expertise– Learning opportunity for both nurses and program
managers– Less threatening/informal
• Disadvantages– Does not provide view of cases in aggregatep gg g– Difficult to juggle busy schedules– Informal– Less peer pressure

31
Performance Measures (Goal Matrix) and Tools
• Developed by nurse consultants
• Tested by record reviews in 12 LHJ in 8 states
Used to teach monitor and evaluate• Used to teach, monitor, and evaluate practice
Performance Measures and Tools
Help Us To -p• Compare case manager performance to
expected standard
• Witness and mentor performance
• Describe, implement, record, and evaluate measures
• Identify needs for procedure development

32
Nursing Interventions (NIC)
1. Risk identification2. Health screening3. Culture brokerage 4. Sustenance support
1. Lack of health seeking behaviors2. Risk for infection3. Communication impairment4 Ineffective health maintenance
1. Health seeking behavior 2. Risk detection 3. Communication ability 4 Social support
Patient Diagnosis (NANDA)
Short-Term Patient Outcomes (NOC)
Social Behavioral Approach to Treatment Adherence: Patient-Centered Care
pp5. Infection control6. Mutual goal setting7. Patient contracting8. Emotional support9. Patient’s rights protection10.Teaching
- disease process - treatment regimen
11. Medication management12. Health policy monitoring13. Discharge planning14 P t ti f
4. Ineffective health maintenance 5. Ineffective protection 6. Decisional conflict: whether to
participate in treatment7. Defensive coping8. Fear (stigma)9. Powerlessness: perceived threat10. Knowledge deficit
- disease process- treatment regimen
11. Ineffective therapeutic regimenmanagement
12. Noncompliance13. Ineffective family therapeutic
regimen management 14 Adjustment impairment:
4. Social support5. Immune status6. Participation in health care decisions7. Coping8. Fear self-control9. Health beliefs: perceived ability to perform10. Knowledge of
- disease process- treatment regimen
11. Medication response12. Compliance13. Family participation
in professional care
14. Well-being15. Community risk control
14. Protection from infection/disease15. Surveillance
14. Adjustment impairment:treatment behavior
15. Ineffective community coping
Long-TermOutcomes
Gibson et al., 2002. Johnson et al., 2006
Core Interventions - NIC
• Risk identification • Patient’s rightsRisk identification
• Health screening
• Culture brokerage
• Sustenance support
• Infection control
• Mutual goal setting
Patient s rights protection
• Teaching
• Medication management
• Health policy monitoring
• Discharge plang g
• Patient contracting
• Emotional support
• Protection from disease
• Surveillance
Gibson et al, 2002

33
Nursing Intervention: Mutual Goal Setting Identify and Prioritize Care Goals and Develop a Plan for Achieving Goals
Goal Attainment Level Definition
Unacceptable Performance (0) Substandard: Does NONE of standard measures
Inadequate Performance (1) Substandard: Does >1 but not all of standard measures
Expected or Standard Performance (2)
Standard: Does ALL of following: 1. Assess for presence of DOT indicators 2. Assess for potential treatment barriers 3. Select enablers and/or incentives with patient’s input 4. Develop written plan 5. Review and implements plan with patient6. Use standard time frame for testing, x-rays, clinic visits, DOT, and drug
supply pp y
Good Performance (3) Does standard plus >1 of following: 1. Occasionally review adherence barriers with patient 2. Review plan, enablers and/or incentives at least once
Outstanding Performance (4) Does ALL standard, good, and outstanding measures: Review adherence barriers with patient at each visit
Self Evaluation Tool for Case Manager
• Mark selected goal interventions
• Record performance score for each selected intervention
• Sum performance scores for selected interventionsinterventions
• Divide sum by number of selected interventions

34
Mark the box when standard measure is found in program policy/procedure, recorded or not on clinical record form
Program Evaluation Tool for NCM
recorded or not on clinical record form, or is performed but not recorded.
Goal Standard MeasuresProgram Policy
(yes/no)Recorded(yes/no)
Performed Not
Recorded(yes/no)
1 Risk Identification
TB-related risk factors
Symptoms of active TB
Changes in risk
Risk reduction steps
Results
Additional information helpf l to clinic• Additional information helpful to clinic nurses
• Example – Preference for food vehicle used to mix with patient’s medication was noted in chart. This made DOT successful in the field AND in the clinic setting
35
Summary (I)• Goal not being met was identified early
• Using the Matrix Tool an adherence barrier was gidentified - DOT was 75% when done at the clinic site
• Working with the child and the family the barrier was overcome and the food vehicle was changed resulting in DOT adherence of 95-100%
• The Matrix Tool allows for a proactive approach and early identification of case management problems
Summary (II)Systematic and thorough review of NCM
documentation for quality improvement.
Attempts to assess processes towards treatmentAttempts to assess processes towards treatment completion and contact evaluation and treatment.
Disadvantages -
R t ti• Retrospective
• Complex
• Relies heavily on documentation

36
TB STAFFING STANDARDS• WAY OF DETERMINING THE NUMBER OF
STAFF REQUIRED TO DO THE WORK OF ASTAFF REQUIRED TO DO THE WORK OF A TB CONTROL PROGRAM
• QUANTITATIVE STATEMENT DERIVED BY:– Determining hours of nursing staff time available in
the coming month to do the workg– Scope of work to be done throughout the coming
month which includes utilization of an acuity system which identifies patients’ needs
High Acuity Patients
–Substance abuse
H l–Homelessness
–Contacts not adherent
–Not adherent case
–Non-acceptance of TB
–Medical mismanagement/provider g pissues
–Treatment with IV medication and no home health

37
Exercise:
PATIENT ACUITY ASSESSMENT
FACTORS IN DETERMINING WORKLOAD
• Amount of available work hours per month • Scheduled time off per month • The number of planned visits per month based
on acuity• Collaboration time per month (Providers, other
members of multi disciplinary team)members of multi-disciplinary team)• Non-household worksite or institutional
investigations • Other time
38
Results - KC• Kansas City
– Median 410 deficit hours or shortage 2 FTE– Issues
• Epidemiology specialists devoting hours to TB –actually paid out of bioterrorism $$$
• Nursing shortage– Results
• Added staff – prophy RN• New refugee nurse• Cooperative agreement – adding one FTE nurse
(.5 funded through cooperative agreement)
Staffing Standards
• AdvantagesProvides a meaningful assessment of time– Provides a meaningful assessment of time management and staff needs of a program
– Takes patient acuity into account
– Prospective method also facilitates management decisions.
• DisadvantagesDisadvantages– Complex
– Non-standard terminology/definitions

39
You are not alone!
• National TB Nurse CoalitionT d i d h TB l ffi i l f– To advise and support the TB control officials of state, local, and territorial governments by providing, within NTCA, a coordinated nursing perspective on issues vital to the success of TB prevention and control programs.
– http://tbcontrollers.org/?page_id=4
• Division of TB Elimination – Nurse Consultant: Judy Gibson (404) 639-5322
[email protected] – join the listserve!
Heartland National TB Center
• Access
1 800 TEX LUNG (1 800 839 5864)– 1-800-TEX-LUNG (1-800-839-5864)
– Nurse Consultants: (210) 531-4546 or 4569
– Monday-Friday, 8:00 AM – 5:00 PM (CT)
• Barbara Seaworth: [email protected]
• Catalina Navarro: [email protected]
• Debbie Onfore: [email protected]

40
Quality Improvement• Its all about meeting objectives!
– NTIP
– Cohort Review
– Program Assessments
• NCM Quality Improvement– Case Reviews
– Performance Measures (Goal Matrix)
– Staffing Standards
References• Case Society of America Home Page, Available at: http://www.cmsa.org/default.aspx
Accessed 11-9-2009.• Case Management Adherence Guidelines (2006), Available at:
http://www.cmsa.org/portals/0/pdf/CMAG2.pdf Accessed 11-9-2009http://www.cmsa.org/portals/0/pdf/CMAG2.pdf Accessed 11 9 2009• Ijaz K, Young K, (2008) Program Evaluation: New Directions – Presentation, National
TB Controllers Association, June 11, 2008 Available at: https://www.signup4.net/public/ap.aspx?EID=2004179E&OID=110 Accessed 10-20-2008
• IOM (2000) Ending neglect: the elimination of TB in the United States. N. A. Press. Washington DC, Institute of Medicine (IOM).
• TB Cohort Review Process, Available at: http://www.harlemtbcenter.org/cohort_review.htm Accessed 10-13-2008
• Gibson J et al (2009) DTBE/FSEB Brown Bag Seminar Available at: htt // li ti / / d / i R di ID 3WNRF6 1 A d 11 6https://www.livemeeting.com/cc/cdc/view Recording ID: 3WNRF6-1 Accessed 11-6-2009.