teachers' evaluations for the detection of primary‐school children with attention deficit...
TRANSCRIPT

This article was downloaded by: [Ams/Girona*barri Lib]On: 17 October 2014, At: 05:18Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
European Journal of Special NeedsEducationPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rejs20
Teachers' evaluations for the detectionof primary‐school children withattention deficit hyperactivity disorderMaria Kypriotaki a & George Manolitsis aa Department of Preschool Education , University of Crete , GallosUniversity Campus, Rethymno, Crete, GreecePublished online: 26 Jul 2010.
To cite this article: Maria Kypriotaki & George Manolitsis (2010) Teachers' evaluations for thedetection of primary‐school children with attention deficit hyperactivity disorder, European Journalof Special Needs Education, 25:3, 269-281, DOI: 10.1080/08856257.2010.492940
To link to this article: http://dx.doi.org/10.1080/08856257.2010.492940
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
European Journal of Special Needs EducationVol. 25, No. 3, August 2010, 269–281
ISSN 0885-6257 print/ISSN 1469-591X online© 2010 Taylor & FrancisDOI: 10.1080/08856257.2010.492940http://www.informaworld.com
Teachers’ evaluations for the detection of primary-school children with attention deficit hyperactivity disorder
Maria Kypriotaki* and George Manolitsis
Department of Preschool Education, University of Crete, Gallos University Campus, Rethymno, Crete, GreeceTaylor and FrancisREJS_A_492940.sgm(Received 18 August 2009; final version received 8 February 2010)10.1080/08856257.2010.492940European Journal of Special Needs Education0885-6257 (print)/1469-591X (online)Original Article2010Taylor & Francis253000000August [email protected]
The early detection of children with attention deficit hyperactivity disorder(ADHD) by teachers can contribute to the prevention of secondary disorders in achild and this can have serious implications for the child’s overall development.The aims of the present study were to examine: (1) the validity of the originalassessment of the teachers in detecting school-age children nominated as childrenwith ADHD by their teachers; and (2) the factors that influence teachers’evaluations on a rating scale assessing ADHD, such as child’s gender, the parents’level of education, the child’s social and academic behaviour in the classroom, theteacher–student relationship, as well as the teachers’ cooperation with the parents.Teachers were asked to fill in a Greek standardised rating scale for the detectionof children with ADHD and a student behaviour questionnaire for 420 primary-school students nominated as children with ADHD by teachers. The study’sfindings showed that teachers detect far more students with ADHD than thenumber expected from the norms based on the standardised ADHD rating scale.Teachers not only nominated more boys than girls as students with ADHD, butalso made more accurate identifications for girls than for boys, particularly in thelater primary-school grades. Children’s age or parental educational backgrounddid not influence the teachers’ initial nominations or their later ratings. Multipleregression analyses indicated that the teachers’ beliefs about a child’s peerrelations and the quality of teacher–child relationships predicted teachers’ ratingson the ADHD scale more than other factors did.
Keywords: attention deficit hyperactivity disorder; primary school; teachers;evaluation
Introduction
Attention deficit hyperactivity disorder (ADHD) is central among the disorders ofchildhood (Kerns, Eso, and Thomson 1999) and constitutes the most common schoolproblem presenting serious consequences for the learning processes. The frequencythe disorder is met among school-age children varies between 3% and 7% (AmericanPsychiatric Association 2000). This percentage rises significantly when children eval-uation scales are administered to parents and teachers (Havey et al. 2005; Rinn andNelson 2009). The basic symptoms of this disorder are inattention, impulsiveness andhyperactivity (Brandau and Pretis 2004; Pisecco, Huzinec, and Curtis 2001) or acombination of the three (Nowacek and Mamlin 2007). The criteria for determining
*Corresponding author. Email: [email protected]
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4

270 M. Kypriotaki and G. Manolitsis
ADHD require the presence of symptoms in two or more settings, such as school andhome (De Nijs et al. 2004) with a duration of at least six months (Mrug, Hoza, andGerdes 2001). The determination of the frequency of ADHD presents a considerablediscrepancy owing to the conceptual approach of the researchers, the data collectiontools, and the size and type of the population in question (Kalantzi-Azizi andKarademas 2004). This disorder is diagnosed at least three times more often in boysthan in girls (Barkley 1998).
As a result of ADHD symptoms, impulsiveness and hyperactivity, a considerablenumber of children that suffer from this disorder face major difficulties at school (Kos,Richdale, and Hay 2006) and home. They are being rejected by their peers (Mrug,Hoza, and Gerdes 2001), and later when they become teenagers and adults withADHD they will often have social and communication skills deficits (Robbins 2005).Children with ADHD are in danger of school failure (LeFever et al. 2002), pooracademic achievement (Pisecco, Huzinec, and Curtis 2001), and they are more proneto accidents (Barkley 1998) and exhibiting delinquent behaviour. The increasedfrequency of the disorder, its chronic nature – if it is not addressed in time – and alsothe presence of multiple problems in children with ADHD, makes necessary the useof valid and reliable psychometric tools that will identify children with this disorder(Kalantzi-Azizi, Aggeli, and Efstathiou 2005).
The importance of early detection of children with ADHD and children in dangerof developing ADHD is essential to ensure proper psychoeducational treatment(Sauver et al. 2004). Early diagnosis is often a difficult process, because manyproblems associated with ADHD are characteristics of other disorders as well(Sciutto, Terjesen, and Bender Frank 2000). What is more, ADHD characteristics aremanifested together with other related problems, such as learning difficulties, stressand depression (Reuner and Oberle 2000), oppositional defiant disorder (Döpfner,Schürmann, and Fröhlich 1998), conduct disorder (Pelham, Fabiano, and Massetti2005), Tourette syndrome (Spencer et al. 1998) and so on. Owing to the complexityof the disorder and associated problems, an assessment from an interdisciplinarygroup is necessary (Kypriotaki 2004; Sciutto, Terjesen, and Bender Frank 2000).
The role the teacher plays in this assessment is determinative (Kypriotakis 2001)because of his immediate involvement in the learning process, the consequent behav-iour of the student inside the school environment, the student’s performance, and therelationship of the student with other fellow students. Further, the teacher can detectearly, unidentified deficiencies and contribute to the prevention of secondarydisorders in a child through the learning requirements established in the classroom.Teachers contribute important information, because of their extensive contact withchildren in structured and unstructured activities and social situations (Atkins,Pelham, and Licht 1985; De Nijs et al. 2004) and their knowledge of abilities/behaviours that suit the children’s age (Lauth, Heubeck, and Mackowiak 2006). Often,the teacher becomes part of the referral procedure of a child with special educationalneeds (Rinn and Nelson 2009; Stevens, Quittner, and Abikoff 1998). In addition, his/her reports are used in the assessment (Biederman et al. 2004; Sciutto, Terjesen, andBender Frank 2000) and in the implementation of an individualised educationalprogramme (Vereb and DiPerna 2004).
Many times the teachers are the first to acknowledge that a child cannot concen-trate or is hyperactive; nevertheless, they often make mistaken judgments concerningstudents with ADHD (Amador-Campos et al. 2006; Rinn and Nelson 2009; Sciutto,Terjesen, and Bender Frank 2000; Stevens, Quittner, and Abikoff 1998) and many
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4

European Journal of Special Needs Education 271
teachers have limited knowledge of the nature, the symptoms, the causes, the manage-ment and the interventions that are related to ADHD (Jerome, Gordon, and Husler1994).
Previous studies have indicated that teachers’ knowledge of ADHD primarilycomes from media or friends and relatives and not from scientific resources (Ghani-zadeh, Bahredar, and Moeini 2006; Stormont and Stebbins 2005). Furthermore,parents often complain that their children with ADHD do not get the proper guidanceand support at school owing to lack of teacher knowledge (Concannon and Tang2005). Inconsistent diagnosis can worsen a situation and contribute to the recurrentfailure of a student inside the classroom (Baum and Olenchak 2002).
Research studies concerning teacher assessment of children with ADHD focus onthe teachers’ knowledge (for review see Kos, Richdale, and Hay [2006]) of the symp-toms of ADHD (Bacchini, Affuso, and Trotta 2008; Nowacek and Mamlin 2007;Vereb and DiPerna 2004), the causes, the frequency the disorder is manifested (Glassand Wegar 2001; Havey et al. 2005), the treatment (Glass and Wegar 2001; Haveyet al. 2005; Kerns Eso, and Thomson 1999; Snider, Busch, and Arrowood 2003;Kasten, Coury, and Heron 1992) and the potential referral of children that are consid-ered to have ADHD (Yang and Schaller 1997). Moreover, previous studies examinedfactors associated with teachers which influence their judgment of children withADHD (Kos, Richdale, and Jackson 2004; Sciutto, Terjesen, and Bender Frank 2000;Stevens, Quittner, and Abikoff 1998; Stormont and Stebbins 2005; Vereb and DiPerna2004), factors that influence students’ behavioural and academic outcomes (Sherman,Rasmussen, and Baydala 2008) and the traits of students that influence teacherassessment of therapy approval (Pisecco, Huzinec, and Curtis 2001) and referral ofthese children (Sciutto, Nolfi, and Bluhm 2004).
For example, Kos, Richdale, and Jackson (2004) conclude that the experience ofan ADHD student in the classroom is related to teachers’ knowledge of the disorder.Accordingly, Sciutto, Terjesen, and Bender Frank (2000) showed that experience withan ADHD student was an important factor which allowed teachers to learn more aboutthe disorder and that their self efficacy and years of teaching experience are factorsthat are associated with their knowledge of ADHD. In contrast, Stevens, Quittner, andAbikoff (1998) found that teachers’ experience with a student with ADHD, teachers’knowledge and their educational status were not significant predictors of theirestimations of ADHD and oppositional defiant disorder (ODD).
In a recent study, Stormont and Stebbins (2005) showed that the educational statusof primary-school teachers is related to their knowledge of the disorder; however, theyears of teaching experience, the nature of occupation (full- vs. part-time) and theknowledge they think they possess were not related to the disorder. In another studyby Vereb and DiPerna (2004), who conducted research on teacher knowledge ofADHD and its treatment and teachers’ beliefs on the different forms of treatment,found that the teachers’ knowledge of the disorder, the years of educational experiencewith students with ADHD and their training were positively correlated with theirtemperate attitude towards medication. To summarise, teachers’ judgment of childrenwith ADHD seems to be influenced by their knowledge of ADHD characteristics.However, there are conflicting findings regarding the importance of years of teachingexperience and teachers’ general educational status in identifying children withADHD.
The degree to which the teachers’ original assessment is applicable is an importantissue because the early detection of children with ADHD from teachers can contribute
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4

272 M. Kypriotaki and G. Manolitsis
to the prevention of secondary disorders in a child and this can have serious implica-tions for the child’s overall development. Teacher assessments are often used to helpdetermine a diagnosis, the appropriate educational setting and therapies that wouldbenefit the student (Brown 1985, cited in Stevens, Quittner, and Abikoff 1998). Thus,teachers need to know the characteristics of ADHD so as to alleviate difficulties thatcome up (Harlacher, Roberts, and Merrell 2006). The aims of the present study wereto examine: (1) the validity of the initial teacher assessment in detecting primary-school children nominated as children with ADHD by their teachers; and (2) thefactors that influence teachers’ evaluations on a rating scale assessing ADHD, such aschild’s gender, the parents’ level of education, the child’s social and academic behav-iour in the classroom, the teacher–student relationship and the teachers’ cooperationwith the parents.
Method
Sample
The study sample comprised 420 primary-school children (7–12 years old) who wereinitially nominated as children with ADHD by 365 teachers. At first, 79 primaryschools (48 from urban and 31 from rural areas) from the island of Crete, Greece, wererandomly selected. Subsequently, teachers of every single class were asked to identifywhether any of the students in their classroom suffered from ADHD. All the studentsthat were initially identified by their teachers as children with ADHD participated inthe present study.
Materials
Teachers were asked to complete a standardised rating scale for the identification ofchildren with ADHD for each participant as well as a questionnaire assessingparticipants’ school behaviour and achievement inside the classroom.
ADHD rating scale-IV
This scale was constructed by DuPaul et al. (1998) and was standardised in Greece byKalantzi-Azizi, Aggeli, and Efstathiou (2005). The instrument is an 18-item, four-point scale ranging from never/rarely to sometimes, often and very often. Each itemdescribes a behaviour that is indicative of ADHD symptoms (e.g., he/she interrupts orannoys the others). Teachers were asked to respond with how frequently each partic-ipant manifested the behaviours listed on the scale. Cronbach’s alpha and Spearman–Brown split half reliability of the scale in the present sample was strong (0.87 and 0.83respectively).
Student behaviour questionnaire
This questionnaire was comprised of demographic items (the parents’ educationalbackground, the child’s age, gender, grade, number of siblings, birth order, number ofclassmates in his/her classroom) and seven other items on a five-point rating scale.Five of the seven items, ranging from excellent to very poor, assessed the student’sschool achievement, his/her relationship with classmates, his/her quality of behaviour
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4
European Journal of Special Needs Education 273
in group activities, the quality of relationship with his/her teacher, and the quality ofteachers’ cooperation with his/her parents. The other two items, ranging from alwaysto never, assessed the frequency of a student’s participation in group activities and thefrequency with which his/her classmates chose him/her as a teammate.
Procedure
The study was conducted between April and May of the 2007–08 school year.Questionnaires were distributed to the teachers of the randomly chosen primaryschools. Teachers were asked to fill in the questionnaires only for the students thatthey believed had ADHD. A total of 620 primary-school teachers were asked whetherthey believed that any of their students was an ADHD child; 120 responded that theydid not believe that any child of their class suffered from ADHD. Therefore, 500questionnaires were distributed and 420 were returned yielding a response rate of84%.
Results
Accuracy of teachers’ identifications of students with ADHD
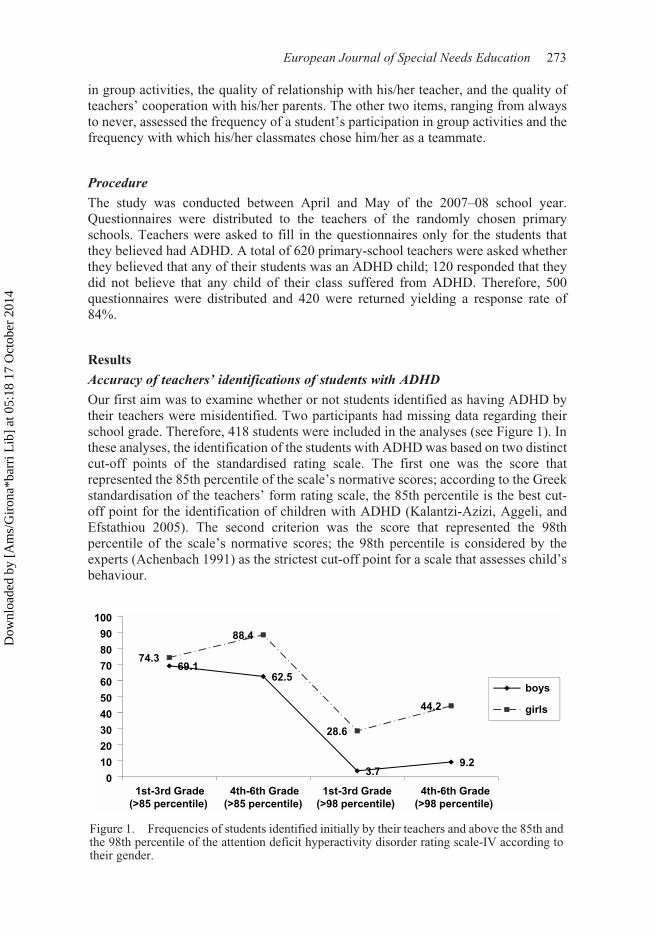
Our first aim was to examine whether or not students identified as having ADHD bytheir teachers were misidentified. Two participants had missing data regarding theirschool grade. Therefore, 418 students were included in the analyses (see Figure 1). Inthese analyses, the identification of the students with ADHD was based on two distinctcut-off points of the standardised rating scale. The first one was the score thatrepresented the 85th percentile of the scale’s normative scores; according to the Greekstandardisation of the teachers’ form rating scale, the 85th percentile is the best cut-off point for the identification of children with ADHD (Kalantzi-Azizi, Aggeli, andEfstathiou 2005). The second criterion was the score that represented the 98thpercentile of the scale’s normative scores; the 98th percentile is considered by theexperts (Achenbach 1991) as the strictest cut-off point for a scale that assesses child’sbehaviour.Figure 1. Frequencies of students identified initially by their teachers and above the 85th and the 98th percentile of the attention deficit and hyperactivity disorder rating scale-IV according to their gender.
Figure 1. Frequencies of students identified initially by their teachers and above the 85th andthe 98th percentile of the attention deficit hyperactivity disorder rating scale-IV according totheir gender.
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4

274 M. Kypriotaki and G. Manolitsis
Figure 1 shows that according to the normative criteria (above 85th or 98th percen-tile) of the ADHD rating scale-IV that teachers completed, girls were identified moreaccurately than boys as suffering from ADHD. The only case in which the frequencyof girls identified by both the teacher and the standardised scale did not differ signif-icantly (χ2(1) = 2.59, p = 0.11) from the respective frequency of boys was betweenfirst and third grade when the normative cut-off point of the scale was set at the 85thpercentile. For example, 69.1% of the boys and 74.3% of the girls attending Grades1–3 who were initially identified by their teachers as children with ADHD receivedscores in the scale above the 85th percentile according to the norms of the scale. Theremaining 30.9% of the boys and 25.7% of the girls attending Grades 1–3 who wereinitially identified by their teachers as children with ADHD could be characterised asmisidentifications because they did not get scores above the lowest cut-off point (85thpercentile) of the standardised scale. Among girls in Grades 4–8, 88.4% of thoseinitially identified by their teachers as having ADHD received scores above the 85thpercentile of the standardised scale. This was a significantly higher percentage thanthat of girls in Grades 1–3 (χ2(1) = 6.76, p < 0.01). The respective percentage of boys(62.5%) was significantly lower than that of girls (χ2(1) = 99.01, p < 0.001) in Grades4–6, but not significantly lower than the boys’ percentage in Grades 1–3 (χ2(1) = 3.15,p = 0.08).
In terms of the children who got scores above the strictest cut-off point of the stan-dardised scale (the 98% percentile) the percentages of both boys and girls were quitelow (see Figure 1). In this case, teachers accurately identified significantly more girlsthan boys at all grade levels (Grades 1–3: χ2(1) = 58.88, p < 0.001; Grades 4–6: χ2(1)= 75.39, p < 0.001).
These findings suggest that Greek teachers identified students as children withADHD at a higher frequency than the number of students that were identified by thestandardised rating scale. However, it seems that the frequency of false alarms basedonly on teachers’ initial identifications decreased largely from the initial school gradesto later ones.
Factors associated with teachers’ identifications of students with ADHD
It was examined whether teachers’ initial identifications of children with ADHD wereinfluenced by gender, grade level, parental education and whether teachers’ rating onthe ADHD scale was influenced by student-related variables (students’ schoolachievement, peer relations, students’ frequency of participation in group activities,quality of students’ involvement behaviour in group activities, peers acceptance,teacher–child relationship and teacher–parent cooperation).
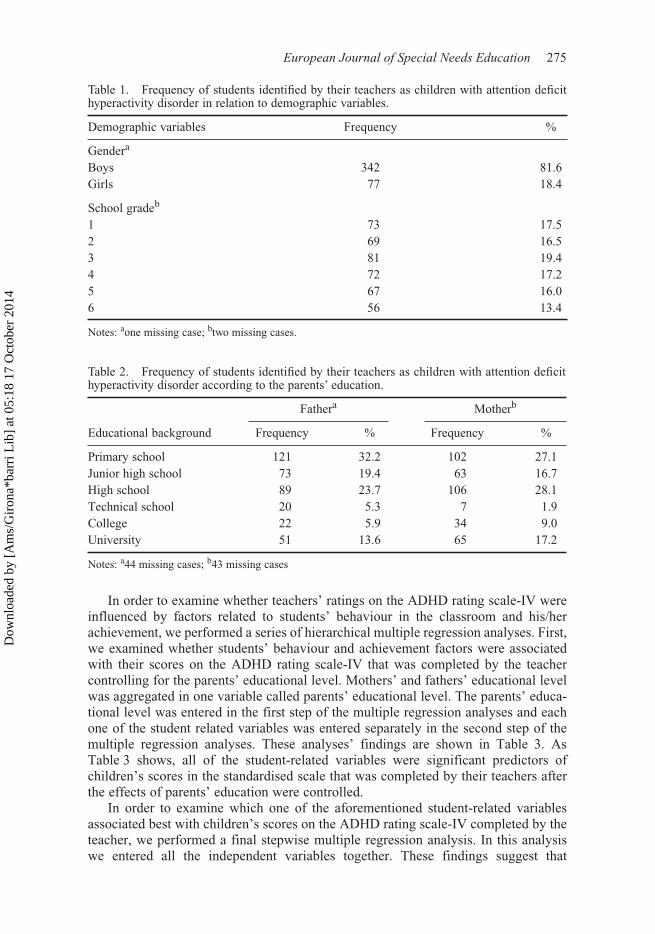
Teachers initially identified significantly more boys than girls (χ2(1) = 167.6 p <0.001) (see Table 1). Moreover, in the same table it is indicated that the frequency ofstudents that were initially identified by their teachers as children with ADHD wassimilar across the grades of the primary school (χ2(5) = 4.87, p > 0.05).
Parental educational background was a significant factor that influenced teach-ers’ initial identification of students with ADHD. Table 2 shows that the studentsthat were identified by their teachers as having ADHD differed both according totheir mothers’ (χ2(6) = 196.99, p < 0.001) and fathers’ (χ2(6) = 201.13, p < 0.001)educational background. In particular, more students identified as children withADHD had parents who only finished primary school than finished university orcollege.
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4
European Journal of Special Needs Education 275
In order to examine whether teachers’ ratings on the ADHD rating scale-IV wereinfluenced by factors related to students’ behaviour in the classroom and his/herachievement, we performed a series of hierarchical multiple regression analyses. First,we examined whether students’ behaviour and achievement factors were associatedwith their scores on the ADHD rating scale-IV that was completed by the teachercontrolling for the parents’ educational level. Mothers’ and fathers’ educational levelwas aggregated in one variable called parents’ educational level. The parents’ educa-tional level was entered in the first step of the multiple regression analyses and eachone of the student related variables was entered separately in the second step of themultiple regression analyses. These analyses’ findings are shown in Table 3. AsTable 3 shows, all of the student-related variables were significant predictors ofchildren’s scores in the standardised scale that was completed by their teachers afterthe effects of parents’ education were controlled.
In order to examine which one of the aforementioned student-related variablesassociated best with children’s scores on the ADHD rating scale-IV completed by theteacher, we performed a final stepwise multiple regression analysis. In this analysiswe entered all the independent variables together. These findings suggest that
Table 1. Frequency of students identified by their teachers as children with attention deficithyperactivity disorder in relation to demographic variables.
Demographic variables Frequency %
Gendera
Boys 342 81.6Girls 77 18.4
School gradeb
1 73 17.52 69 16.53 81 19.44 72 17.25 67 16.06 56 13.4
Notes: aone missing case; btwo missing cases.
Table 2. Frequency of students identified by their teachers as children with attention deficithyperactivity disorder according to the parents’ education.
Fathera Motherb
Educational background Frequency % Frequency %
Primary school 121 32.2 102 27.1Junior high school 73 19.4 63 16.7High school 89 23.7 106 28.1Technical school 20 5.3 7 1.9College 22 5.9 34 9.0University 51 13.6 65 17.2
Notes: a44 missing cases; b43 missing cases
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4

276 M. Kypriotaki and G. Manolitsis
teachers’ judgments about students’ peer relations and teacher–student relationshipwere the best student-related predictors of children’s scores on the ADHD ratingscale-IV (Table 4).
According to these findings, children’s gender and parental education backgroundwere significant factors that influence teachers’ initial judgment regarding the childrenwho were characterised by him/her as having ADHD. Moreover, teachers tended torate higher the children who did not get along well with their peers or their teachers.
Discussion
Findings from this study suggest that teachers detect far more students with ADHDthan the number expected from the results based on the ADHD rating scale. Inparticular, if we take into consideration the stricter criterion of the 98th percentile,then the frequency of false alarms on behalf of the teacher rises significantly, espe-cially in relation to boys (see Figure 1). This is probably because of limited teacherknowledge of ADHD as well as the different way the symptoms manifest themselvesin boys and girls. For example, symptoms such as aggressive behaviour or motoractivity, which usually characterise boys, obviously make them stand a greater chanceof being considered as students with ADHD, because they disturb the peace in theclassroom. The present study’s findings are in line with previous studies (Glass andWegar 2001; Havey et al. 2005) and signal how important it is for teachers to learnmore about ADHD. Besides, previous studies have shown that teachers tend to‘exaggerate’ ADHD symptoms (Amador-Campos et al. 2006) and ‘identify’symptoms that are not characteristic of the disorder (Pilling 2000).
Table 3. Results of hierarchical multiple regression analyses for the prediction ofparticipants’ scores on attention deficit hyperactivity disorder rating scale-IV.
Variable’s order ∆R2 β
1. Parents’ education 0.01 0.012. School achievement 0.05 0.06**2. Peer relations 0.11 0.12**2. Frequency of student’s participation in group activities 0.06 0.07**2. Quality of student’s behaviour in group activities 0.03 0.04*2. Frequency that his/her classmates choose him/her as a teammate 0.08 0.09**2. Quality of teacher–student relationship 0.06 0.07**2. Quality of teacher–parent cooperation 0.02 0.03*
Notes: *p < 0.01; **p < 0.001.
Table 4. Results of the stepwise multiple regression analysis for the prediction ofparticipants’ scores on attention deficit hyperactivity disorder rating scale-IV when all thesignificant independent variables entered in the model.
Variable’s order ∆R2 β
1. Peer relations 0.09 0.09**2. Quality of teacher–student relationship 0.02 0.11*
Notes: *p < 0.01; **p < 0.001.
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4
European Journal of Special Needs Education 277
Another interesting finding was that teachers seem to be more accurate in identi-fying girls than boys, according to the criteria of the ADHD rating scale (over the 85thand the 98th percentile). It is possible that teachers appear more accurate in identifyinggirls because many problems related to ADHD in boys (e.g., aggressive behaviour) arealso characteristic of other disorders and, therefore, classified under other disorders,such as ODD or conduct disorder. Indeed, teachers are likely to assess only the severecases of ADHD in girls and that is the reason why they seem to be more accurate, asfar as girls are concerned. There was no significant difference between the frequencyof boys and girls in Grades 1–3 that were assessed by teachers as having ADHD andreached above the 85th percentile (see Figure 1).
Additionally, teachers identified significantly more boys than girls as ADHDstudents. This can be because of the different way the symptoms are manifested inboys and girls respectively (Abikoff et al. 2002), as well as to the fact that ADHD ismore frequent in boys than in girls. As a result, ADHD symptoms in girls could oftenbe overlooked by teachers because girls with ADHD do not cause as many disruptionsin the classroom as boys. In other words, when an ADHD child exhibits aggressivebehaviour the teacher more easily notices the rest of his/her deviant behaviour, whilein the case of girls, who are not as disruptive in the classroom, their ADHD goesunnoticed.
The findings of the present study are in line with the findings of other studieswhich have shown that teachers tend to identify more boys than girls, irrespective ofthe type of symptoms that the child manifested (Sciutto, Nolfi, and Bluhm 2004).Moreover, other findings have shown that clinicians tend to diagnose boys more oftenthan girls with ADHD (Gardner et al. 2002), or that both parents and teachers attributegreater problems with attention span, impulse control, and motor activity to boys thanto girls (DuPaul 1991).
The grade of students initially identified by teachers as children with ADHD wasalso examined to determine whether it influenced teachers’ judgement. The presentfindings showed that the detection of students with ADHD by their teachers did notdifferentiate according to the grade that students attended. Theoretically, it could beanticipated that the frequency of students with ADHD would be diminished in thelater primary-school grades, if in earlier grades students were detected and followedan effective psychoeducational treatment. This finding might reveal that even olderchildren suffer from ADHD, because they have never been addressed so as to receiveproper support.
Findings from the present study also suggest that teacher referral is influenced byparental education. This finding agrees with other research (Sauver et al. 2004) thathas shown that lower levels of parental education are associated with an increased riskfor ADHD. This may be because of the fact that teachers believe that the parents whohave a lower level of education cannot offer their children the appropriate conditions,circumstances or run the required psychoeducational interventions, so as to lessen themanifestation of the symptoms (Sauver et al. 2004).
Another interesting finding is that a child’s scores on the ADHD scale were influ-enced by teachers’ judgment of the relationship the child has with his/her classmates.In other words, it is more likely for a student to be assessed as suffering from ADHDby the teacher scale when the teacher believes that this student does not get along wellwith his/her classmates. This may be related to the fact that the majority of childrenwith ADHD do not get along well with their peers and their relationships are mainlydriven by rejection, isolation, lack of popularity, or difficulties in the apprehension of
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4

278 M. Kypriotaki and G. Manolitsis
social messages (Bacchini, Affuso, and Trotta 2008; Bagwell et al. 2001; Greshamet al. 1998; Hinshaw and Melnick 1995); besides, the ADHD symptoms themselvesmake relationships with peers challenging (Mrug, Hoza, and Gerdes 2001).
Furthermore, findings from this study suggest that it is more likely that a studentwill be thought as suffering from ADHD (teacher rating scale) if the teacher believesthat the student does not get along well with his/her own teacher. The present findingsextend the literature examining the association of teacher–student interactions withstudents’ disruptive behaviour. Hughes, Cavell and Jackson (1999) revealed that poorteacher–student relationships predicted increased levels of aggression in a sample ofsecond and third graders nominated by teachers as aggressive children. The presentstudy extends the previous findings as it is shown that the quality of teacher–studentrelationships predicted increased levels of rating in a scale for the assessment ofADHD in a sample of primary-school children nominated by teachers as children withADHD. Maybe these disturbed teacher–student relationships stem from a lack ofattention span or an increased motor activity or impulsive behaviour in the classroom;a repertoire that makes learning processes difficult. However, it is possible forteachers to attribute negative qualities to some students based on their own disturbedrelationships with them, a tendency that does not protect these students against beingcategorised as ADHD students.
In conclusion, findings from the present study suggest that: (1) teachers assess farmore students as children with ADHD than the number based on the ratings from thestandardised Greek version of the ADHD rating scale-IV; (2) teachers identify moreboys than girls as having ADHD, but their assessment of girls seems more valid thanthat of boys; (3) teachers assess more easily as students with ADHD those childrenwho come from parents that have a low educational level; (4) teachers’ inferencesfrom the relationship of a student with his/her peers and the relationship of the samestudent with his/her own teacher are the strongest predictors of the total score that thestudent will get on the ADHD rating scale; and (5) school achievement is not a strongpredictor of the score that the student will get on the ADHD rating scale.
The present findings contribute to the literature that underline teachers’ importantrole in the identification of children with special educational needs. In addition, theconceptualisation of ADHD by teachers is also influenced by social context factors.For example, proximal and distal social context attitudes towards ADHD and lack ofcourses on special education during pre-service teachers’ training may favour a stress-ful environment for students with ADHD and their classmates and their teachers. Thenew trend in educating children with special educational needs necessitates the appro-priate training of teachers of mainstream classrooms in order to be able to identifyaccurately and early their students’ difficulties.
The present study also has certain limitations. One limitation is that our resultsrefer to students that have initially been assessed by teachers as suffering from ADHD.They cannot be generalised to a population that has not received the same initialassessment by the teachers. This means that the present study did not take into consid-eration the children that may have ADHD, but have not yet been diagnosed as such bytheir teachers. Additionally, these results only refer to the teacher assessment andthere are no similar results for parent assessment. It should be noted that the results ofthe present study come from the answers of teachers who work in public schools inCrete, the largest island in southern Greece with 500,000 inhabitants. A recommenda-tion for future research is to conduct a replication study on a national level. Finally,the supplementary completion of the Greek version of the ADHD rating scale-IV by
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4
European Journal of Special Needs Education 279
parents (parent version) would contribute to cross-validation of the children identifiedas suffering from ADHD.
ReferencesAbikoff, H.B., P.S. Jensen, L.E. Arnold, B. Hoza, L. Hechtman, S. Pollack, D. Martin, J. et al.
2002. Observed classroom behavior of children with ADHD: Relationship to gender andcomorbidity. Journal of Abnormal Child Psychology 30: 349–59.
Achenbach, Thomas M. 1991. Manual for the child behavior checklist/4–18 and 1991 profile.Burlington, VT: University of Vermont, Department of Psychiatry.
American Psychiatric Association. 2000. Diagnostic and statistical manual of mentaldisorders. 4th ed. Washington, DC: American Psychiatric Association.
Amador-Campos, J.A., M. Forns-Santacana, J. Guárdia-Olmos, and M. Peró-Cebollero. 2006.DSM-IV Attention deficit hyperactivity disorder symptoms: Agreement between infor-mants in prevalence and factor structure at different ages. Journal of Psychopathology andBehavioral Assessment 28, no. 1: 23–32.
Atkins, M.S., W.E. Pelham, and M.H. Licht. 1985. A comparison of objective classroommeasures and teacher ratings of attention deficit disorder. Journal of Abnormal ChildPsychology 13, no. 1: 155–67.
Bacchini, D., G. Affuso, and T. Trotta. 2008. Temperament, ADHD and peer relations amongschoolchildren: The mediating role of school bullying. Aggressive Behavior 34: 447–59.
Bagwell, C.L., M.E. Schmidt, A.F. Newcomb, and W.M. Bukowski. 2001. Friendship andpeer rejection as predictors of adult adjustment. In The role of friendship in psychologicaladjustment, ed. D.W. Nangle, and C.A. Erdley, 25–49. San Francisco, CA: Jossey-Bass.
Barkley, Russell A. 1998. Attention deficit hyperactivity disorder: A handbook for diagnosisand treatment. New York: Guilford Press.
Baum, S.M., and F.R. Olenchak. 2002. The alphabet children: GT, ADHD, and more.Exceptionalist 10, no. 2: 77–91.
Biederman, J., S.V. Faraone, M.C. Monuteaux, and J.R. Grossbard. 2004. How informativeare parent reports of attention-deficit/hyperactivity disorder symptoms for assessingoutcome in clinical trials of long-acting treatments? A pooled analysis of parents’ andteachers’ reports. Pediatrics 113, no. 6: 1667–71.
Brandau, H., and M. Pretis. 2004. Early identification and systemic educational interventionfor young children with attention-deficit/hyperactivity disorder. European Journal ofSpecial Needs Education 19, no. 1: 17–31.
Concannon, P.E., and Y.P. Tang. 2005. Management of attention deficit hyperactivity disor-der: a parental perspective. Journal of Pediatrics and Child Health 41: 625–30.
De Nijs, P.F., R.F. Ferdinand, E.I. De Bruin, M.C.J. Dekker, C.M. Van Duijn, and F.C.Verhulst. 2004. Attention-deficit/hyperactivity disorder (ADHD): Parents’ judgmentabout school, teachers’ judgment about home. European Child and Adolescent Psychiatry13, no. 5: 315–20.
Döpfner, Manfred, Stephanie Schürmann, and Jan Fröhlich. 1998. Therapieprogramm fürKinder mit hyperkinetischem und oppositionellem Problemverhalten THOP. Weinheim,Germany: Beltz.
DuPaul, G.J. 1991. Parent and teacher ratings of ADHD symptoms: Psychometricproperties in a community – based sample. Journal of Clinical Child Psychology 20, no.3: 245–53.
DuPaul, George J., Thomas J. Power, Arthur D. Anastopoulos, and Robert Reid. 1998. ADHDrating scale-IV: Checklists, norms, and clinical interpretation. New York: Guilford Press.
Gardner, W., K.A. Pajer, K.J. Kelleher, S.H. Scholle, and R.C. Wasserman. 2002. Child sexdifferences in primary care clinicians’ mental health care of children and adolescents.Archives of Pediatrics and Adolescent Medicine 156: 454–9.
Ghanizadeh, A., M.J. Bahredar, and S.R. Moeini. 2006. Knowledge and attitudes towardsattention deficit hyperactivity disorder among elementary school teachers. PatientEducation and Counseling 63: 84–8.
Glass, C.S., and K. Wegar. 2001. Teacher perceptions of the incidence and management ofattention deficit hyperactivity disorder. Education 121, no. 2: 412–20.
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4
280 M. Kypriotaki and G. Manolitsis
Gresham, F.M., D.L. MacMillan, K.M. Bocian, S.L. Ward, and S.R. Forness. 1998. Comorbid-ity of hyperactivity-impulsivity-inattention and conduct problems: Risk factors in social,affective, and academic domains. Journal of Abnormal Child Psychology 26: 393–406.
Harlacher, J.E., N.E. Roberts, and K.W. Merrell. 2006. Classwide interventions for studentswith ADHD. A summary of teacher options beneficial for the whole class. TeachingExceptional Children 39, no. 2: 6–12.
Havey, J.M., J.M. Olson, C. McCormick, and G.L. Cates. 2005. Teachers’ perceptions of theincidence and management of attention-deficit hyperactivity disorder. Applied Neuropsy-chology 12, no. 2: 120–27.
Hinshaw, S.P., and S.M. Melnick. 1995. Peer relationships in boys with attention-deficithyperactivity disorder with and without comorbid aggression. Development and Psycho-pathology 7: 627–47.
Hughes, J.N., T.A. Cavell, and T. Jackson. 1999. Influence of the teacher–student relationshipon childhood conduct problems: A prospective study. Journal of Clinical ChildPsychology 28, no. 2: 173–84.
Jerome, L., M. Gordon, and P. Hustler. 1994. A comparison of American and Canadianteachers’ knowledge and attitudes towards attention deficit hyperactivity disorder. Cana-dian Journal of Psychiatry 39: 563–7.
Kalantzi-Azizi, Anastasia, Katerina Aggeli, and George Efstathiou. 2005. Helleniki klimakaaksiologisis tis DEP-Y-IV, klimaka gia goneis, klimaka gia ekpaideutikous, Stathmisi tisADHD rating scale-IV [Greek version of ADHD-IV rating scale, scale for parents, scalefor teachers. Standardization of ADHD rating scale-IV]. Athens, Greece: HellenikaGrammata.
Kalantzi-Azizi, A., and E. Karademas. 2004. Diaspasi prosoxis kai adynamia elenhou tonparopmiseon: Apo ton aprosekto mathiti os ti diataraxi elleimatikis prosoxis-hyperkini-tikotita [ADHD and lack of control of impulsiveness: From the inattentive student toattention deficit hyperactivity disorder]. In Adaptation in school, prevention and treatmentof difficulties, ed. A. Kalantzi-Azizi and M. Zafiropoulou, 223–53. Athens, Greece:Hellenika Grammata.
Kasten, E.F., D.L. Coury, and T.E. Heron. 1992. Educators’ knowledge and attitudes regard-ing stimulants in the treatment of attention deficit hyperactivity disorder. Developmentaland Behavioral Pediatrics 13, no. 3: 215–19.
Kerns, K.A., K. Eso, and J. Thomson. 1999. Investigation of a direct intervention for improv-ing attention in young children with ADHD. Developmental Neuropsychology 16, no. 2:273–95.
Kos, J.M., A.L. Richdale, and D.A. Hay. 2006. Children with attention deficit hyperactivitydisorder and their teachers: A review of the literature. International Journal of Disability,Development and Education 53, no. 2: 147–160.
Kos, J.M., A.L. Richdale, and M.S. Jackson. 2004. Knowledge, about attention-deficit/hyper-activity disorder: A comparison of in-service and preservice teachers. Psychology in theSchools 41, no. 5: 517–26.
Kypriotaki, M. 2004. Diataraxes sygentrosis prosoxis, Tropoi stiriksis kai antimetopisis, sigh-rones antilipsis [Attention deficit disorder-support and treatment: contemporary aspects].Heraklion, Greece: Author.
Kypriotakis, A. 2001. Mia Paidagogiki, Ena Sxoleio gia Ola ta Paidia, Sygxrones antilipseisagogis kai ekpaidefsis ton paidion me empodia sti zoi kai sti mathisi [One kind of peda-gogy, one kind of school for all children: Contemporary aspects of education and trainingfor children with difficulties in life and learning]. Athens, Greece: Ellinika Grammata.
Lauth, G.W., B.G. Heubeck, and K. Mackowiak. 2006. Observation of children with atten-tion-deficit hyperactivity (ADHD) problems in three natural classroom contexts. BritishJournal of Educational Psychology 76: 385–404.
LeFever, G.B., M.S. Villers, A.L. Morrow, and E.S. Vaughn. 2002. Parental perceptions ofadverse educational outcomes among children diagnosed and treated for ADHD: A callfor improved school/provider collaboration. Psychology in the Schools 39, no. 1: 63–71.
Mrug, S., B. Hoza, and A.C. Gerdes. 2001. Children with attention-deficit/hyperactivitydisorder: peer relationships and peer-oriented interventions. In The role of friendship inpsychological adjustment, ed. D.W. Nangle and C.A. Erdley, 51–77. San Francisco, CA:Jossey-Bass.
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4
European Journal of Special Needs Education 281
Nowacek, E.J., and N. Mamlin. 2007. General education teachers and students with ADHD:What modifications are made? Preventing School Failure 51, no. 3: 28–35.
Pelham, W.E, G.A. Fabiano, and G.M. Massetti. 2005. Evidence-based assessment of atten-tion deficit hyperactivity disorder in children and adolescents. Journal of Clinical Childand Adolescent Psychology 34, no. 3: 449–76.
Pilling, B.A. 2000. Teacher competency in identifying ADHD and other childhood mentalhealth disorders: Some possible explanations for ADHD misdiagnosis. PhD diss.,Brigham Young University; Dissertation Abstracts International 61: 2777.
Pisecco, S., C. Huzinec, and D. Curtis. 2001. The effect of child characteristics on teachers’acceptability of classroom-based behavioral strategies and psychostimulant medication forthe treatment of ADHD. Journal of Clinical Psychology 30, no. 3: 413–21.
Reuner, G., and A. Oberle. 2000. ADS und was sonst noch. In ADS: Verstehen-akzeptieren-helfen, ed. T. Fitzner and W. Stark, 139–149. Weinheim, Germany: Beltz.
Rinn, A.N., and J.M. Nelson. 2009. Preservice teachers’ perceptions of behaviors characteris-tic of ADHD and giftedness. Roeper Review 31: 18–26.
Robbins, C.A. 2005. ADHD couple and family relationships: Enhancing communication andunderstanding through imago relationship therapy. JCLP/In Session 61, no. 5: 565–77.
Sauver, J.L., W.J. Barbaresi, S.K. Katusic, R.C. Colligan, A.L. Weaver, and S.J. Jacobsen.2004. Early life risk factors for attention-deficit/hyperactivity disorder: A population-based cohort study. Mayo Foundation for Medical Education and Research 79, no. 9:1124–31.
Sciutto, M.J., M.D. Terjesen, and A.S. Bender Frank. 2000. Teachers’ knowledge and misper-ceptions of attention-deficit/hyperactivity disorder. Psychology in the Schools 37, no. 2:115–22.
Sciutto, M.J., C.J. Nolfi, and C. Bluhm. 2004. Effects of child gender and symptom type onreferrals for ADHD by elementary school teachers. Journal of Emotional and BehavioralDisorders 12, no. 4: 247–53.
Sherman, J., C. Rasmussen, and L. Baydala. 2008. The impact of teacher factors on achieve-ment and behavioural outcomes of children with attention deficit/hyperactivity disorder(ADHD): A review of the literature. Educational Research 50, no. 4: 347–60.
Snider, V.E., T. Busch, and L. Arrowood. 2003. Teacher knowledge of stimulant medicationand ADHD. Remedial and Special Education 24, no. 1: 46–56.
Spencer, T., J., Biederman, M. Harding, D. O’Donnell, T. Wilens, S. Faraone, B. Coffey, andD. Geller. 1998. Disentangling the overlap between Tourette’s disorder and ADHD.Journal of Child Psychology and Psychiatry 39, no. 7: 1037–44.
Stevens, J., A.L. Quittner, and H. Abikoff. 1998. Factors influencing elementary schoolteachers’ ratings of ADHD and ODD behaviors. Journal of Clinical Child Psychology 27,no. 4: 406–14.
Stormont, M., and M.S. Stebbins. 2005. Preschool teachers’ knowledge, opinions, and educa-tional experiences with attention deficit/hyperactivity disorder. Teacher Education andSpecial Education 28, no. 1: 52–61.
Yang, K.N., and J. Schaller. 1997. Teachers’ ratings of attention-deficit hyperactivity disorderand decisions for referral for services in Taiwan. Journal of Child and Family Studies 6,no. 2: 249–61.
Vereb, R.L., and J.C. DiPerna. 2004. Teachers’ knowledge of ADHD, treatments for ADHD,and treatment acceptability: An initial investigation. School Psychology Review 33, no. 3:421–8.
Dow
nloa
ded
by [
Am
s/G
iron
a*ba
rri L
ib]
at 0
5:18
17
Oct
ober
201
4