technique of pleural pneumonectomy in diffuse mesothelioma general thoracic surgery chapter 66
TRANSCRIPT

TECHNIQUE OF PLEURAL PNEUMONECTOMY IN
DIFFUSE MESOTHELIOMA
GENERAL THORACIC SURGERY
CHAPTER 66
Extrapleural pneumonectomy
• Improvement in operative mortality since 1970 ( 30% to 6% ) .
• Patient selection, preoperative preparation, intraoperative management, postoperative care with this extremely complex disease.

Staging
• Use the Butchart staging system— Surgical resection only appropriate for stage I disease.
• Brigham stage I and II as potentially respectable. Table 66-2.


Patient selection
• Karnofsky performance status higher than 70. • Normal liver and liver function, • ABG – Room air PCO2 less than 45 mmHg, PO2
more than 65 mmHg. • Lung function and ventilation–perfusion scan
normal. • Echocardiography, CT and MRI– For determine
the presence of transdiaphragmatic extention or mediastinal invasion.
Technique of right side extrapleural pneumonectomy
• Before thoracotomy, limited subcostal incision– Explore the possible transdiaphragmatic involvement. (May laparoscopic exploration). If peritoneal invasion, the thoracotomy should be terminated.
• Left lateral decubitus position, extended right posterolateral thoracotomy,
• N.G. tube.
Technique of right side extrapleural pneumonectomy
• Sixth ribs is excised. • Widely based extrapleural blunt and sharp
dissection. • Superiorly toward the apex and anterior
component. • Posterior latterly after adequate exposure of
anterior side which can provide safe view of mediastinal structure.

Technique of right side extrapleural pneumonectomy
• Brachial triangle is exposed carefully– To avoid avulsion of subclavian artery and vein
• Protected internal mammary artery.
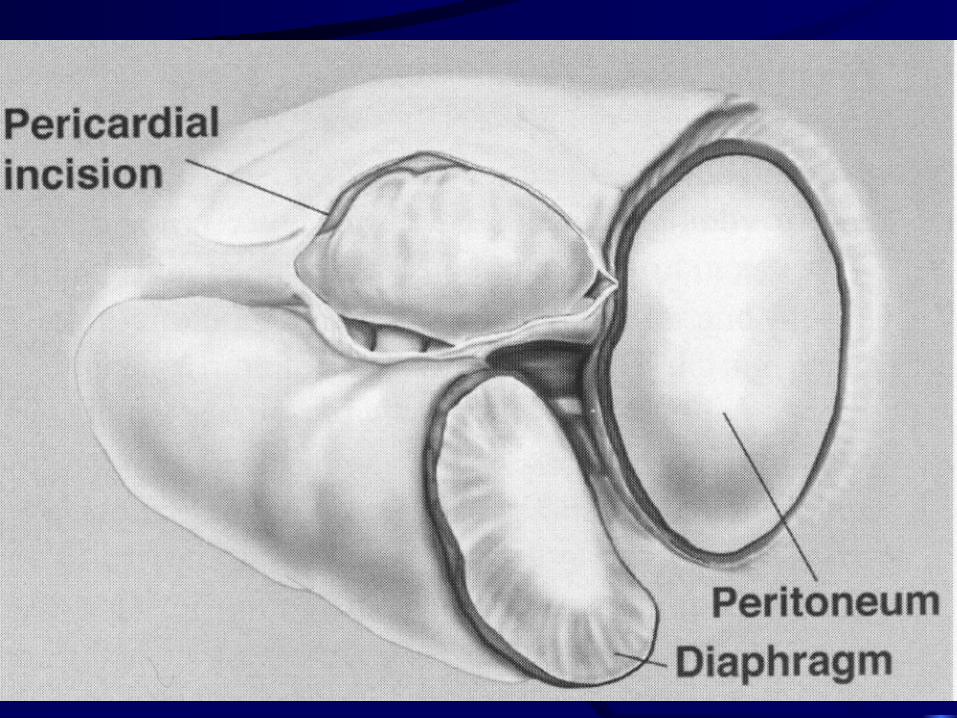
• Open pericardium with resection posterior to hilum.
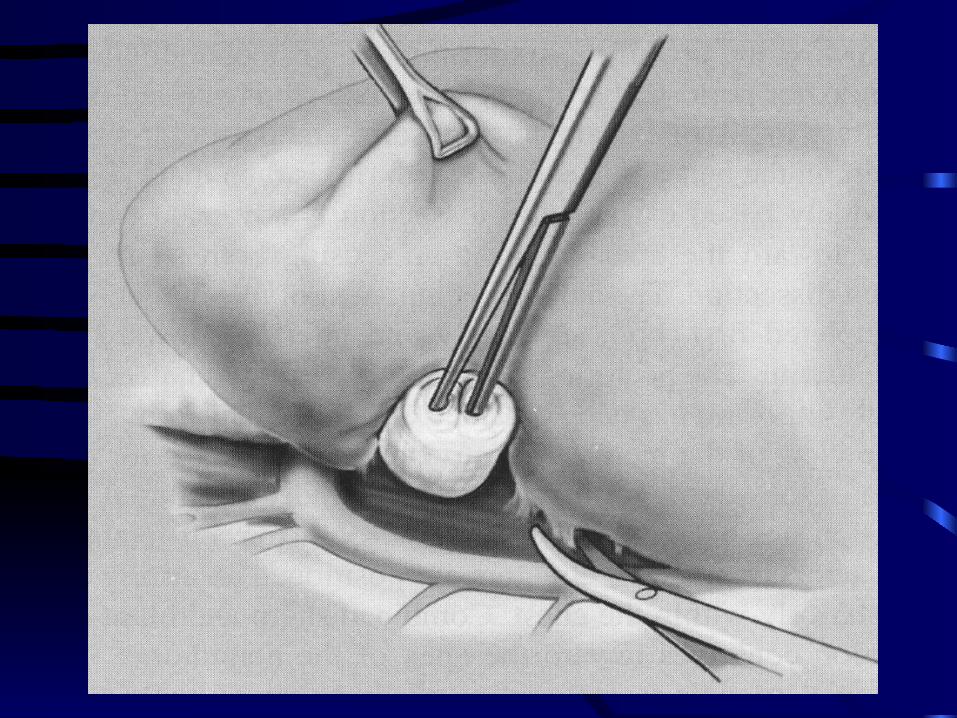
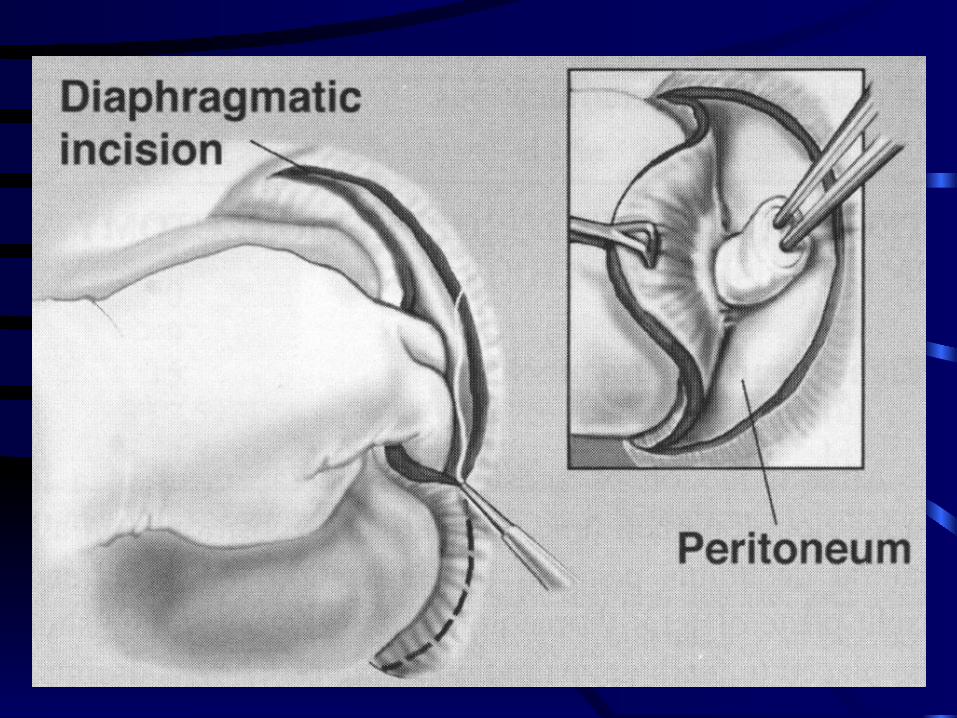
• Diaphragm is dissected off the peritoneum by blunt dissection using sponge stick.

Technique of right side extrapleural pneumonectomy
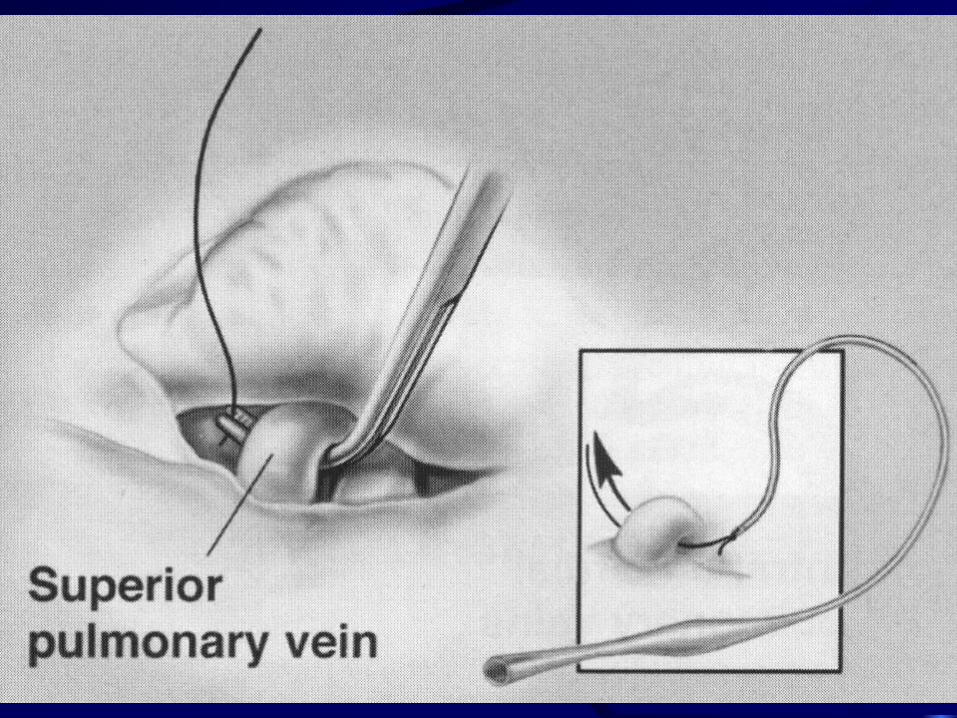
• Ligated the right main pulmonary artery, superior and interior pulmonary vein, right main stem bronchus.
• Pericardial fat-pad– Cover the cutting end of bronchus.
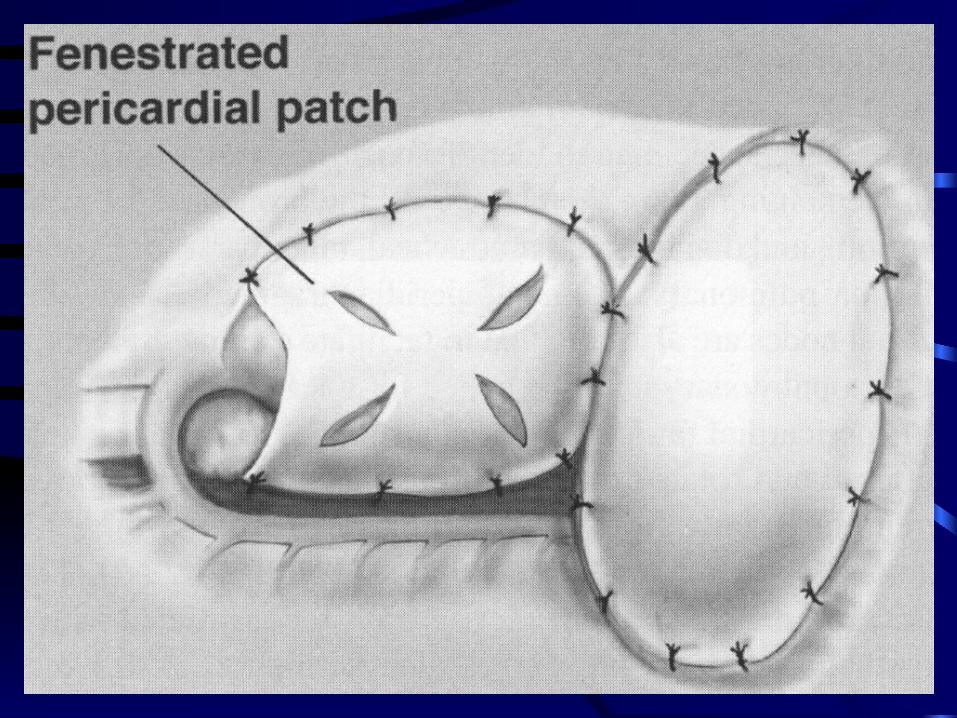
• Radical lymph node dissection. • Right side pericardium is reconstructed by
prothetic patch to prevent cardiac herniation. • Diaphragm reconstructed by prosthetic
impermeable patch.

Technique of left side extrapleural pneumonectomy
• Dissection is less difficult. • Dissection the posteromedial aspect – Should
entering correct plane in preaortic region – To prevent avulsion intercostals vessels.
• Assessment of aorta is critical step on left side pleuropneumonectomy.
• Protect esophagus. • Pericardium is NOT routinely reconstructed–
Because of risk of cardiac herniation is low.
Technique of extrapleural pneumonectomy
• Hemostasis— Intra-operative blood loss 750 for right side and 500 for left side.
• Use argon beam coagulator and electrocautery for the numerous small vessels in extrapleural plane.

Postoperative management
• Control pain.
• Minimize intravascular volume change ( 1-L, 24hour fluid restriction for 3-5 days ) .
• DVT prophylaxis.
• Bed rest 48 hours– To facilitate mediastinal stability.

Result
• Mortality 3.8% ( 1999 ) .
• 2-year survival – 38%.
• 5-year survival – 15%.