technology diffusion, hospital variation, and racial disparities among elderly medicare...
TRANSCRIPT

Technology Diffusion, Hospital Technology Diffusion, Hospital Variation, and Racial Disparities Variation, and Racial Disparities Among Elderly Medicare Among Elderly Medicare Beneficiaries: 1989-2000Beneficiaries: 1989-2000
Peter W. Groeneveld, MD, MSPeter W. Groeneveld, MD, MS
Sara B. Laufer, MASara B. Laufer, MA
Alan M. Garber, MD, PhDAlan M. Garber, MD, PhD
CDEHA
Center on the Demography and Economics of Health
and Aging
Healthcare Disparities and Healthcare Disparities and Geographic VariationGeographic Variation
Racial disparities in medical procedure use may Racial disparities in medical procedure use may partially be explained by “small area” partially be explained by “small area” geographic differences in procedure availability.geographic differences in procedure availability.
Explained 95% of the difference in knee Explained 95% of the difference in knee replacement rates between white and latina replacement rates between white and latina women.*women.*
Within localities, there are large differences in Within localities, there are large differences in technology utilization rates among hospitals.technology utilization rates among hospitals.††
*Skinner J, et al. Racial, ethnic, and geographic disparities in rates of knee arthroplasty among Medicare patients. N Engl J Med 2003;349:1350-9.
†Selby JV, et al. Variation among hospitals in coronary-angiography practices and outcomes after myocardial infarction in a large health maintenance organization. N Engl J Med. 1996;335:1888-1896.

Research QuestionsResearch Questions
Do differences in major medical procedure Do differences in major medical procedure rates among hospitals help explain racial rates among hospitals help explain racial disparity in healthcare?disparity in healthcare?
Do hospitals with larger black inpatient Do hospitals with larger black inpatient populations provide more/less equal care?populations provide more/less equal care?
As medical technologies diffuse through As medical technologies diffuse through the marketplace, do racial disparities the marketplace, do racial disparities decrease?decrease?
SettingSetting
20% random selection of elderly 20% random selection of elderly Medicare beneficiaries Medicare beneficiaries hospitalized between 1989-2000.hospitalized between 1989-2000.
Medicare Provider Analysis and Medicare Provider Analysis and Review (MEDPAR) administrative Review (MEDPAR) administrative records.records.
Selection Criteria for Selection Criteria for ProceduresProcedures
Performed in sufficient volume among Performed in sufficient volume among the elderly throughout 1989-2000.the elderly throughout 1989-2000.
Substantial growth in volume and in Substantial growth in volume and in number of hospitals offering number of hospitals offering procedure during the 1990s.procedure during the 1990s.
Performed in inpatient setting.Performed in inpatient setting.
Influenced DRG assignment.Influenced DRG assignment.
Emerging Procedures and Emerging Procedures and Their Indicator DiagnosesTheir Indicator Diagnoses
Procedure Indicator Diagnoses (ICD-9)
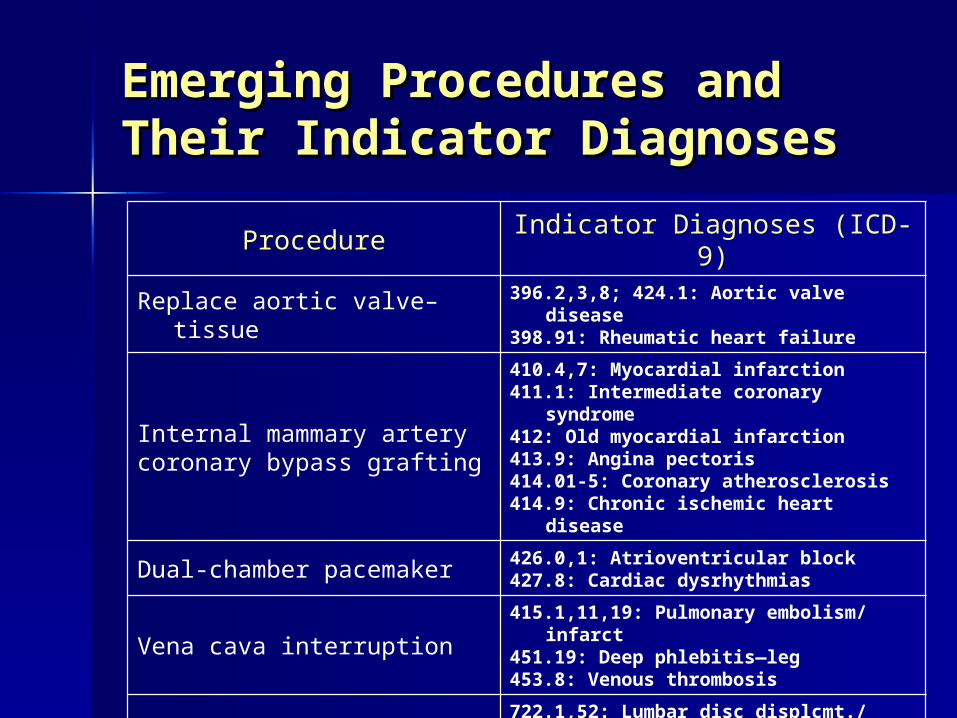
Replace aortic valve–tissue 396.2,3,8; 424.1: Aortic valve disease398.91: Rheumatic heart failure
Internal mammary arterycoronary bypass grafting
410.4,7: Myocardial infarction411.1: Intermediate coronary syndrome412: Old myocardial infarction413.9: Angina pectoris414.01-5: Coronary atherosclerosis414.9: Chronic ischemic heart disease
Dual-chamber pacemaker 426.0,1: Atrioventricular block427.8: Cardiac dysrhythmias
Vena cava interruption415.1,11,19: Pulmonary embolism/ infarct451.19: Deep phlebitis—leg453.8: Venous thrombosis
Lumbar/LS spinal fusion
722.1,52: Lumbar disc displcmt./ degenrtn724.00,02: Spinal stenosis737.30: Idiopathic scoliosis738.4: Spondylolisthesis

Hospitalization with indicator Hospitalization with indicator diagnosis, 1989-2000.diagnosis, 1989-2000.
Linked to subsequent hospitalizations Linked to subsequent hospitalizations within 90 day period. within 90 day period.
Outcomes:Outcomes: – Procedure within 90 days of admission Procedure within 90 days of admission oror
– Death prior to 90 days without procedure Death prior to 90 days without procedure oror
– Survive 90 days without procedure.Survive 90 days without procedure.
Cohort Formation / Cohort Formation / OutcomesOutcomes
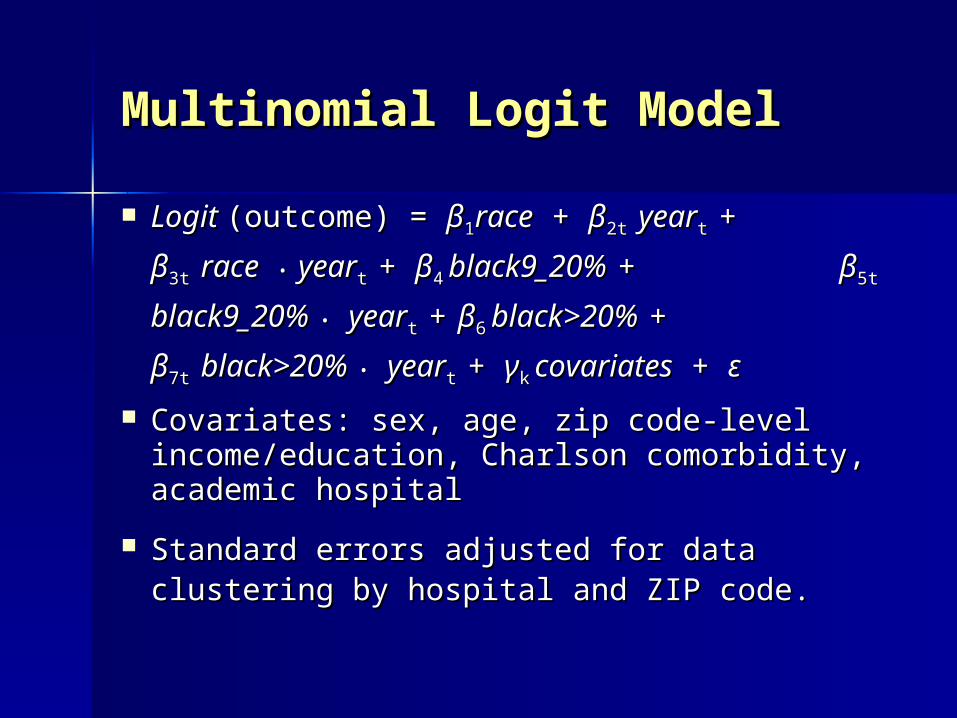
Multinomial Logit ModelMultinomial Logit Model
Logit Logit (outcome) = (outcome) = ββ11racerace + + ββ2t 2t yearyeart t + + ββ3t 3t
racerace • • yearyeart t + + ββ44 black9_20%black9_20% ++ ββ5t 5t
black9_20%black9_20% •• yearyeart t ++ ββ66 black>20%black>20% ++
ββ7t 7t black>20%black>20% •• yearyeart t + + γγkk covariatescovariates + + εε
Covariates: sex, age, zip code-level Covariates: sex, age, zip code-level income/education, Charlson comorbidity, income/education, Charlson comorbidity, academic hospitalacademic hospital
Standard errors adjusted for data clustering Standard errors adjusted for data clustering by hospital and ZIP code.by hospital and ZIP code.
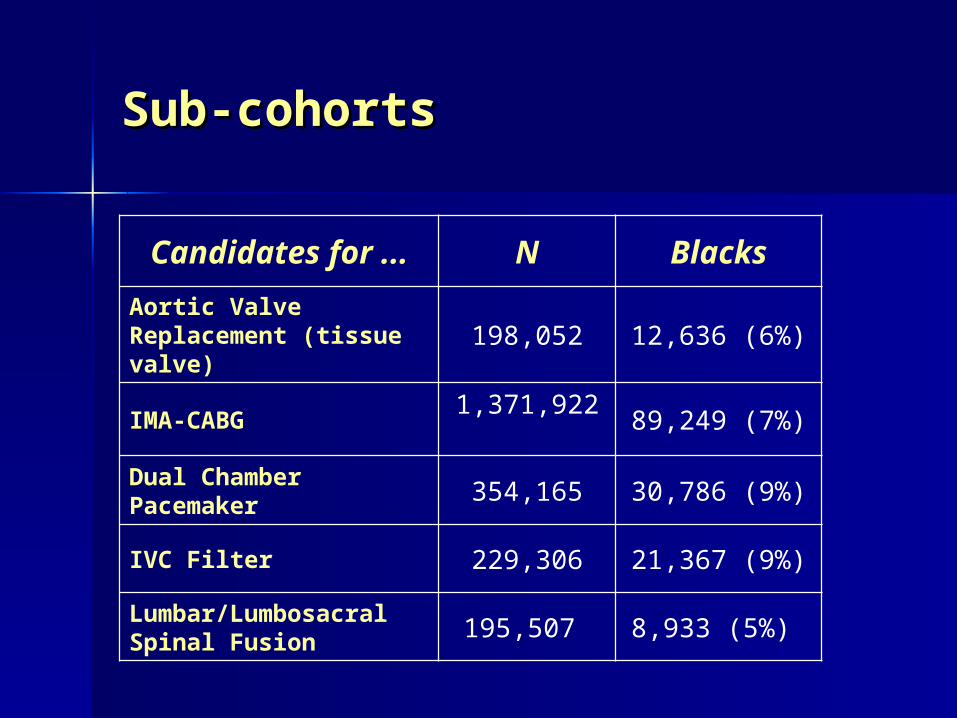
Sub-cohortsSub-cohorts
Candidates for ... N Blacks
Aortic Valve Replacement (tissue valve) 198,052 12,636 (6%)
IMA-CABG 1,371,922 89,249 (7%)
Dual Chamber Pacemaker 354,165 30,786 (9%)
IVC Filter 229,306 21,367 (9%)
Lumbar/Lumbosacral Spinal Fusion 195,507 8,933 (5%)
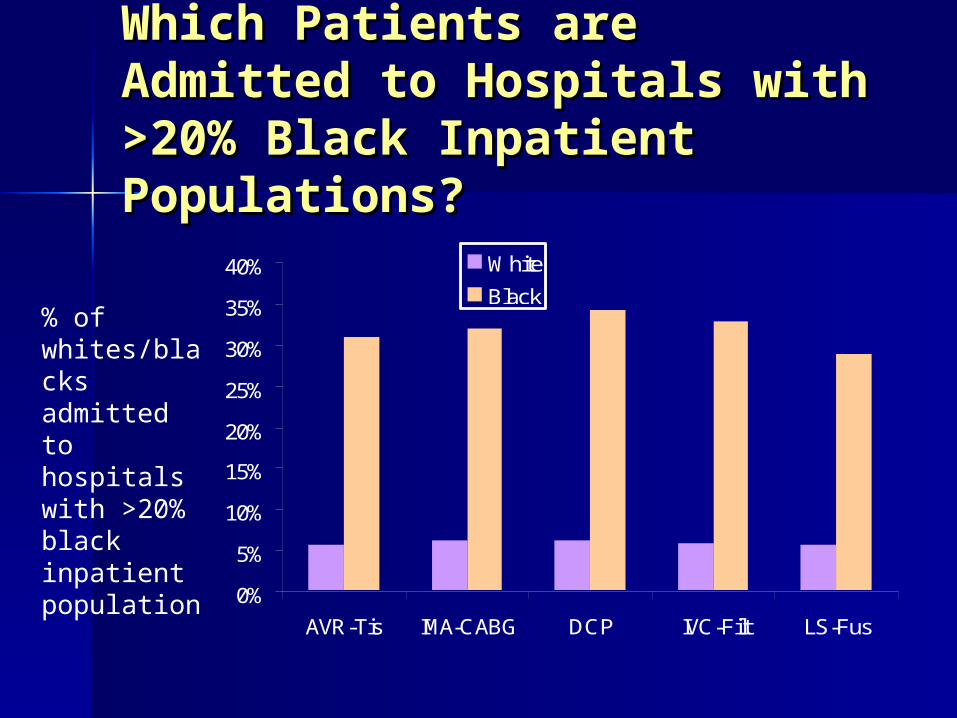
Which Patients are Which Patients are Admitted to Hospitals with Admitted to Hospitals with >20% Black Inpatient >20% Black Inpatient Populations?Populations?
0%
5%
10%
15%
20%
25%
30%
35%
40%
AVR-Tis IMA-CABG DCP IVC-Filt LS-Fus
White
Black% of whites/blacks admitted to hospitals with >20% black inpatient population
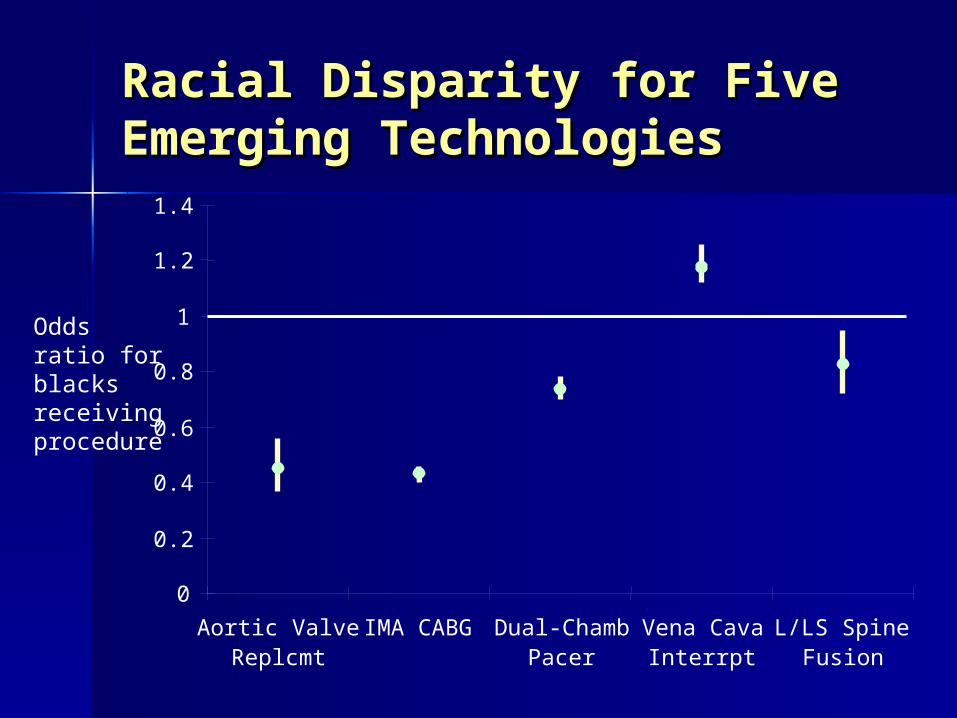
Racial Disparity for Five Racial Disparity for Five Emerging TechnologiesEmerging Technologies
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Aortic ValveReplcmt
IMA CABG Dual-ChambPacer
Vena CavaInterrpt
L/LS SpineFusion
Odds ratio for blacks receiving procedure
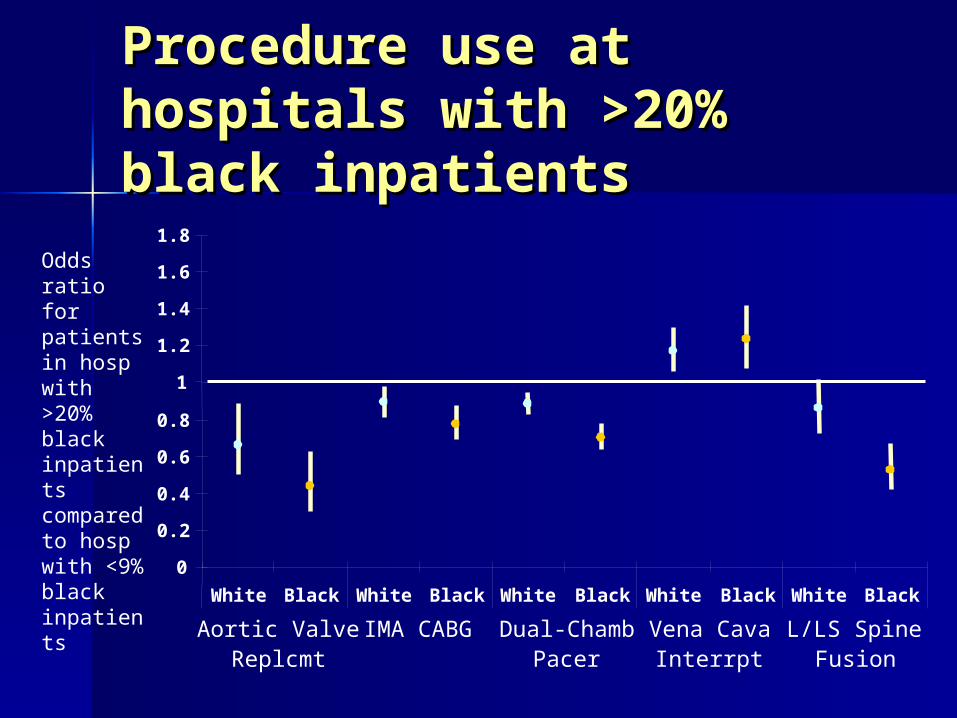
Procedure use at Procedure use at hospitals with >20% hospitals with >20% black inpatientsblack inpatients
Odds ratio for patients in hosp with >20% black inpatients compared to hosp with <9% black inpatients
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
0
White Black White Black White Black White Black White Black
Aortic ValveReplcmt
IMA CABG Dual-ChambPacer
Vena CavaInterrpt
L/LS SpineFusion

Comparison of Disparities at Comparison of Disparities at Hospitals with >20% or <9% Hospitals with >20% or <9% Black InpatientsBlack Inpatients
p=0.01
p=0.005
p<0.001
p<0.001
p=0.78
0.2
Black<9%
Black>20%
Black<9%
Black>20%
Black<9%
Black>20%
Black<9%
Black>20%
Black<9%
Black>20%
Aortic ValveReplcmt
IMA CABG Dual-ChambPacer
Vena CavaInterrpt
L/LS SpineFusion
0.4
0.6
0.8
1
1.2
1.4Odds ratio for blacks compared to whites in hosps with <9% black inpatients and hosps with >20% black inpatients

ConclusionsConclusions
Hospitals with larger black inpatient Hospitals with larger black inpatient populations had generally lower populations had generally lower procedure rates for their patients.procedure rates for their patients.
These hospitals also had greater levels These hospitals also had greater levels of racial disparity.of racial disparity.
Substantial racial disparities persisted Substantial racial disparities persisted in the use of several emerging medical in the use of several emerging medical technologies during the 1990s.technologies during the 1990s.

LimitationsLimitations
Administrative data were Administrative data were insufficiently detailed to determine insufficiently detailed to determine who met definitive procedural who met definitive procedural criteria.criteria.
Possible that systematic differences Possible that systematic differences exist between the accuracy and exist between the accuracy and detail of MEDPAR records for whites detail of MEDPAR records for whites and blacks.and blacks.

ImplicationsImplications
The quality and innovativeness of care The quality and innovativeness of care provided by hospitals with >20% black provided by hospitals with >20% black inpatient populations is critical to the inpatient populations is critical to the provision of more equal healthcare.provision of more equal healthcare.
Policy initiatives to improve racial Policy initiatives to improve racial disparities in healthcare should disparities in healthcare should concentrate on the mediating role of concentrate on the mediating role of these hospitals.these hospitals.

END

Procedure Rate Growth: Procedure Rate Growth: 1989-19991989-1999
0
5
10
15
20
25
30
35
AVR-Tissue
IMA-CABG Dual Pacer IVC Filter LumbarFusion
1989
1999Procedures per 10,000 elderly Medicare Beneficiaries

CovariatesCovariates
Race (black or white).Race (black or white).
Sex, age, ZIP-code-level race-specific Sex, age, ZIP-code-level race-specific income/education, urban location.income/education, urban location.
Charlson comorbidity index.Charlson comorbidity index.
Black inpatient population (%) of Black inpatient population (%) of center in which patient hospitalized.center in which patient hospitalized.