testicular cancer - oncologypro.esmo.org · no testicular primary detectable 1-5 % of all gccs...
TRANSCRIPT

TESTICULAR CANCER
Dr Christoph OingThe Christie NHS Foundation TrustManchester, UK
The “most fascinating” cancer entity.

CONFLICT OF INTEREST DISCLOSURE Dr Christoph Oing
Personal financial interests• Honoraria speaker activity: Medac (2018), IPSEN (2017)Institutional financial interests• NoneNon-financial interests / Leadership role medical societies non-remunerated• Chairman “Junge DGHO” of the German Society of Hematology and Oncology
(DGHO)• ESMO YOC memberOther• Travel and conference attendance: IPSEN (2017)

PATHOPHYSIOLOGY
RISK CLASSIFICATION
TREATMENT
CASE DISCUSSION
TESTICULAR CANCERAgenda

EPIDEMIOLOGY & CLINICAL
PRESENTATION

TESTICULAR CANCERSigns and Symptoms
• Scrotal mass / swelling 74% Other NPL, Hydrocele, Spermatocele
• Scrotal pain 30% Inflammation, Torsion• Gynecomastia 10% Drugs, Liver disease• Infertility 5% Primary infertility• Organ-specific <5% Other medical conditions
(Jaundice, Dyspnea, neurol. Disorder, Fractures)
Signs & Symptoms Differential diagnosis

Most common solid malignancy among adolescents and men aged ≤ 40 years
Onset after puberty onset >75 years: spermatocytic tumours separate entity
TESTICULAR CANCER Age Distribution

TESTICULAR CANCERGeographical incidence

Established Risk Factors Relative risk Contralateral testicular cancer 24.8 - 27.6 Cryptorchidism / Maldescensus testis 3.5 - 17.1
Early orchidopexia important to decrease risk Positive family history 2.5 - 12.3
Highest risk if father or brother affected
Potential Risk Factors Relative risk Infertility 1.6 - 10.0 Atrophic testis <12mL 2.7 - 12.7 HIV 2.0 - 57.0
TESTICULAR CANCERRisk Factors

PATHOGENESIS

TESTICULAR CANCERHistopathology
WHO classification 2016

TESTICULAR CANCERHistology
YS
Bremmer et al., Der Pathologe 2014
GCNIS Pure Seminoma Mixed NSGCT
YS
CC
EC
EC
Courtesy of Dr Pedro Oliveira, The Christie NHS Foundation Trust. Histopathology Dept

TESTICULAR CANCERSubtype evolvement
Seminoma
Embryonal carcinoma
Choriocarcinoma
Yolk sac tumour
Teratoma
Embryonic Extra-embryonic
GCNIS
Non-seminoma40% 60%
Diffe
rent
iatio
n
Sensitivity

TESTICULAR CANCEROrigin of GCTs
Mediastinal
Retroperitoneal
Testicular
Cerebral / hypothalamic area
3 - 5%
95 - 97%

ORIGIN AND PROGNOSIS
0 12 24 360.0
0.2
0.4
0.6
0.8
1.0
med NS (N=228)retrop NS (N=226)
p < 0.001
Months
Prop
ortio
n su
rviv
ing
Bokemeyer et al., J Clin Oncol 2002
DIAGNOSTIC WORK-UP

Primary prevention
• No established primary prevention strategy
Secondary prevention
• Monthly self-examination recommended for every man
• Ultrasound of testes in brothers of patients and infertile men
TESTICULAR CANCERScreening

EXTRAGONADAL GCC
No testicular primary detectable
1-5 % of all GCCs
Arise from primordial germ cells on their developmental journey from the endodermal
layer to the genital ridge localised in the midline of the body
Histologically identical to testicular GCCs
Mediastinum Retroperitoneum Pituitary/hypothalamic region / CNS
10% of all retroperitoneal masses are extragonadal GCCs
Mediastinal GCCs have a dismal prognosis and often harbor TP53mut

STAGING & RISK ASSESSMENT

TNM / UICC STAGING
M1a med./cerv. LN or lung
M1b extr. pulm.
N1 < 2 cm(max. 5 LN)
N2 2 – 5 cmor > 5 LN
N3 > 5cm
T1 no vascular invasion
T2 vascular invasion
T3 invades sperm cord
T4 invades scrotum
Description of disease spread

RADIOLOGIC STAGING
Contrast-enhanced CT-scan of chest and abdomen
NO ROLE for 18F-FDG-PET imaging
Sensitivity and specificity not higher than for conventional CT-scan
MRI CNS only if brain mets suspected or choriocarcinoma with multiple
lung metastases and highly elevated HCG levels
Bone scan only if bone metastases suspected
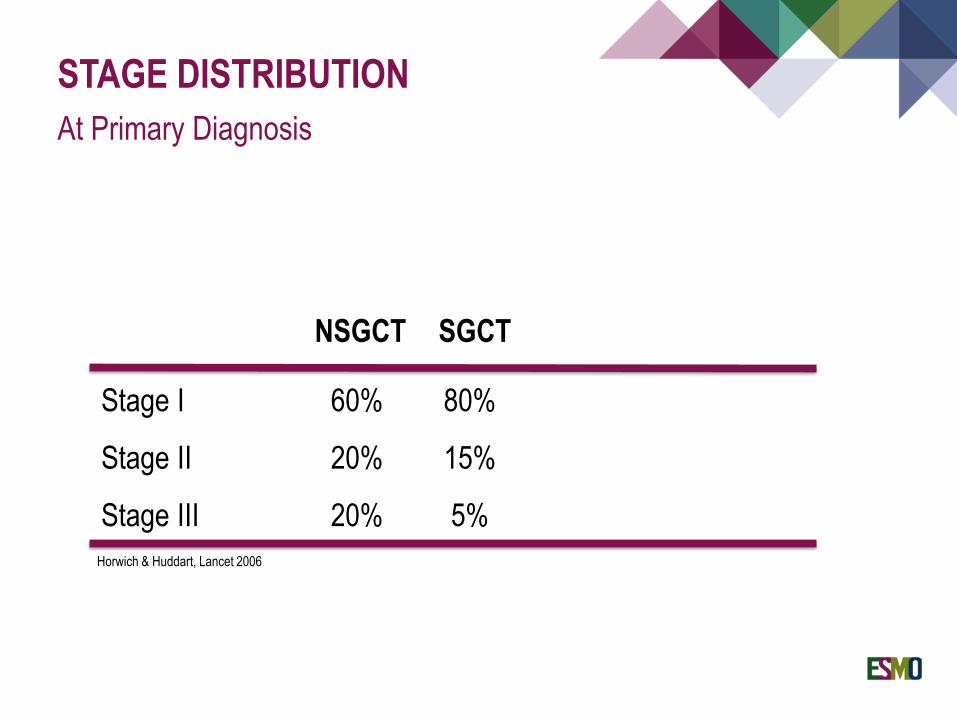
STAGE DISTRIBUTIONAt Primary Diagnosis
Stage I 60% 80%
Stage II 20% 15%
Stage III 20% 5%
SGCTNSGCT
Horwich & Huddart, Lancet 2006

THE S-FACTORTumor marker elevation
LDH [IU/L] HCG [IU/L] AFP [ng/mL]
S0 normal and < 5 and < 10
S1 < 1.5x ULN and < 5.000 and < 1.000
S2 1.5 – 10x ULN or 5.000 – 50.000 or 1.000-10.000
S3 > 10x ULN or > 50.000 or > 10.000
Prior to orchiectomy Day 5-6 post-surgery Half-life HCG 2-3 days
AFP 4-7 days During chemotherapy - prior every cycle
- don‘t take markers right after chemo

TESTICULAR CANCERRisk assessment stage IIC / III
Prognosis 5-year OS Seminoma Non-seminoma
Good 90% Any primary location No non-pulmonary visceral
metastases Any marker level
Testis or primary extragonadal retroperitoneal tumor
No non-pulmonary visceral metastases Low markers AFP < 1,000 ng/ml HCG < 5,000 IU/l LDH < 1.5 x normal level
Intermediate 75%
Any primary location Presence of non-pulmonary
visceral metastases (liver, CNS, bone, intestinum)
Any marker level
Testis or primary extragonadal retroperitoneal tumor
No presence of non-pulmonary visceral metastases
Intermediate markers AFP 1,000-10,000 ng/ml HCG 5,000-50,000 IU/l LDH 1.5-10 x normal level
Poor 50% Does not exist
Primary mediastinal GCT with or without testis Primary retroperitoneal tumor Presence of non-pulmonary visceral
metastases (liver, CNS, bone intestinum) High markers AFP < 10,000 ng/ml HCG > 50,000 IU/l LDH > 10 x normal level
IGCCCG, J Clin Oncol 1997
90%
10%
56%
28%
16%

TESTICULAR CANCER… as times are changing
More recent retrospective series reported improved outcomes forall three risk groups
OS about 10-15% higher in contemporary intermediate and poorprognosis cohorts Fankhauser et al. Ann Oncol 2018 Seidel et al. Eur J Cancer 2018

TREATMENTSTAGE I

Seminoma(pT1-4 N0 M0)
CarboplatinAUC7 x1
Active Surveillance
RT para-aorticregion 20 Gy
• 80% overtreatment• Relapse risk
3-9%
• Recommended forall CS I SGCT
• Relapse risk10-15%
• SMN?
TESTICULAR CANCERStage I Seminoma

TESTICULAR CANCERStage I Seminoma
Active surveillance Radiation Carboplatin AUC 7 x1
Overall cure rate > 99% > 99% > 99%Relapse rate 15% 4-5% 5%Abdominal imagingrequired in FU Yes No Yes
% pts. unnecessarilyexposed to treatment 0% 85% 85%

TESTICULAR CANCERStage I Non-seminoma
Non-Seminoma(pT1-4 N0 M0)
BEP (1 cycle)
Active Surveillance
RPLND• Only expert centers• In-field relapses
• Relapse riskLVI neg 15-20%LVI pos 40-50%
• Recommendedfor LVI pos
• Relapse risk5%

TESTICULAR CANCERRisk factor stage I non-seminoma
MRC Prospective Surveillance Study 1984 - 1987
Relapse-free Rate by vascular invasion
Months from orchidectomy
168144120967248240
Rel
apse
-fre
e ra
te
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
Read et al., JCO 1992; 10:1762-8

TESTICULAR CANCERStage I Non-seminoma
Active surveillance RPLND BEP x 1 for LVI+Overall cure rate > 99% > 99% > 99%
Relapse rate15% low risk50% high risk
30% unselected10-15% 3-5%
Abdominal imagingrequired in FU Yes No Yes
% pts. unnecessarilyexposed totreatment
0%70%
85% low risk50% high risk
70%85% low risk50% high risk

TREATMENTADVANCED DISEASE
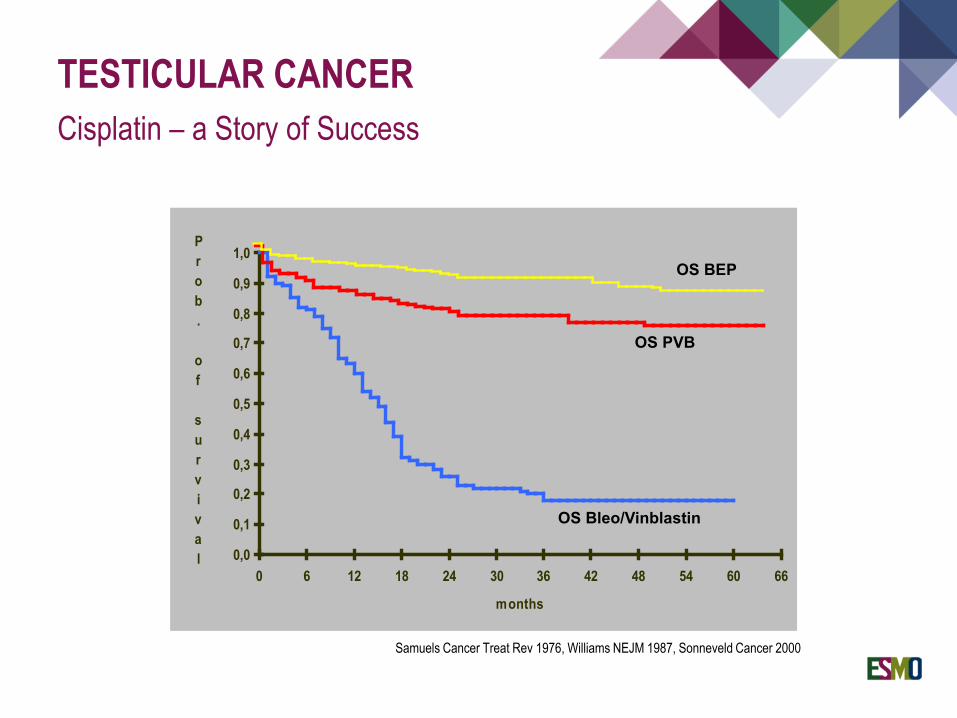
TESTICULAR CANCERCisplatin – a Story of Success
0,0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1,0
0 6 12 18 24 30 36 42 48 54 60 66
months
Prob. of survival
OS Bleo/Vinblastin
OS PVB
OS BEP
Samuels Cancer Treat Rev 1976, Williams NEJM 1987, Sonneveld Cancer 2000

TESTICULAR CANCERAdvanced Stages IIC / III
IGCCCG Risk Group 5 yr OS Treatment EBM Level
“good prognosis” 90 % 3 x BEP ( I B)SGCT & NSGCT [*alternatively 4 x EP] ( II A)“intermediate prognosis” 80 % 4 x BEP ( IV)SGCT & NSGCT [*alternatively 4 x VIP] ( I B)“poor prognosis” 50 % 4 x BEP ( I B)only NSGCT [*alternatively 4 x VIP] ( I B)
*only if Bleomycine not allowedOldenburg J et al., ESMO CPG Testicular Cancer, Ann Oncol 2015
BEP; Cisplatin, Etoposide, Bleomycine
EP; Cisplatin, Etoposide
VIP; Cisplatin, Etoposide, Ifosfamide

TESTICULAR CANCERImproving „poor risk“ outcomes
IGCCCG poor prognosis GCC
> 1 criterion: PMNSGCT CNS Metastases Liver Metastases Bone Metastases
None of the criteria
1 cycle standard doseBEP or VIP
Adequate marker declineNO adequate tumor
marker decline
3 more cycles of BEP or VIP
Recommendation:High-dose chemotherapy with 3 x HD-VIP + autolog. PBSCTAlsdorf, Oing et al., Exp Opin Pharmacother 2019

TESTICULAR CANCERResidual seminoma
Advanced SEM
Chemotherapy
Residues < 3cm Residues ≥ 3cm
Follow-up 18F-FDG-PET-CT
PET - PET +
W W Surgery RTxOing et al., Nuclear Oncology, 1st Ed., 2014
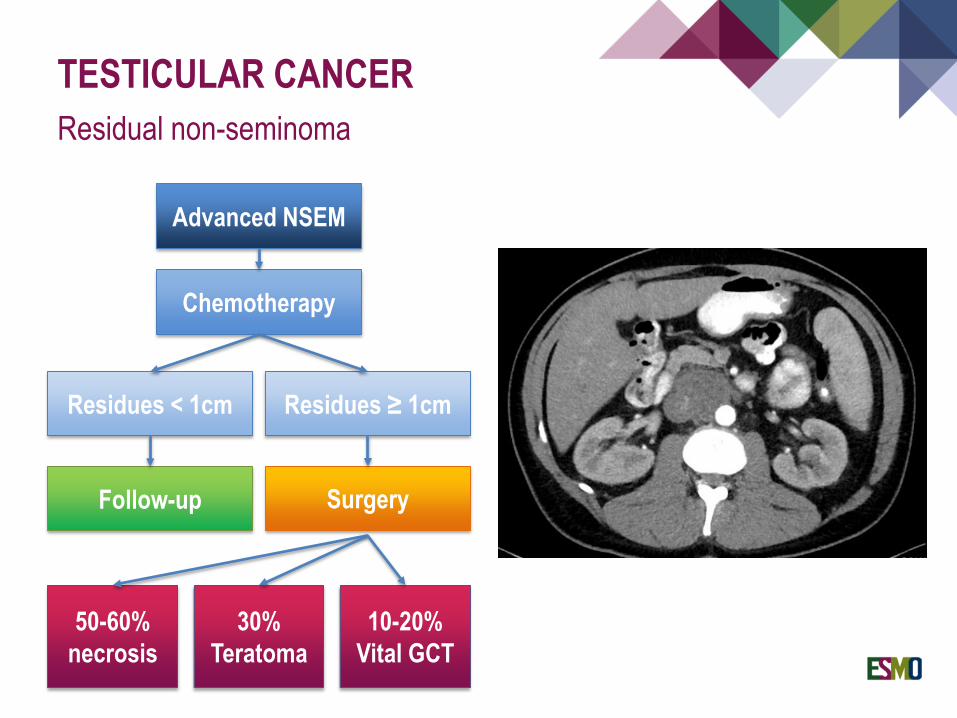
TESTICULAR CANCERResidual non-seminoma
Advanced NSEM
Chemotherapy
Residues < 1cm Residues ≥ 1cm
Follow-up Surgery
50-60%necrosis
30%Teratoma
10-20%Vital GCT

TESTICULAR CANCERThe teratoma issues
Growing teratoma syndrome
Teratomas completelytreatment resistant
Only surgery curative Secondary malignant
transformation withdismal prognosis Courtesy of Dr Pedro Oliveira, The Christie NHS Foundation Trust.
Histopathology Dept

TREATMENT@1ST RELAPSE

TESTICULAR CANCERTiming of relapse
Ko et al., J Clin Oncol 2016
Most relapses occur duringthe first 2 yrs after EOT
Most relapses detecteddue to symptoms
< 5% of relapses duringthird year or later
Late relapses confer dismal prognosis
Surgical approachespreferred for late relapsesif technically feasible

TESTICULAR CANCERIPFSG Score – Prognosis @1st relapse
Internsational Prognostic Factors Study Group, J Clin Oncol 2010
RISK FACTORS AT RELAPSE
Extragonadal Primary Non-seminoma No CR / PR after 1st-line Relapse within 12mos Extrapulmonary Mets High AFP / HCG 2nd or further Relapse
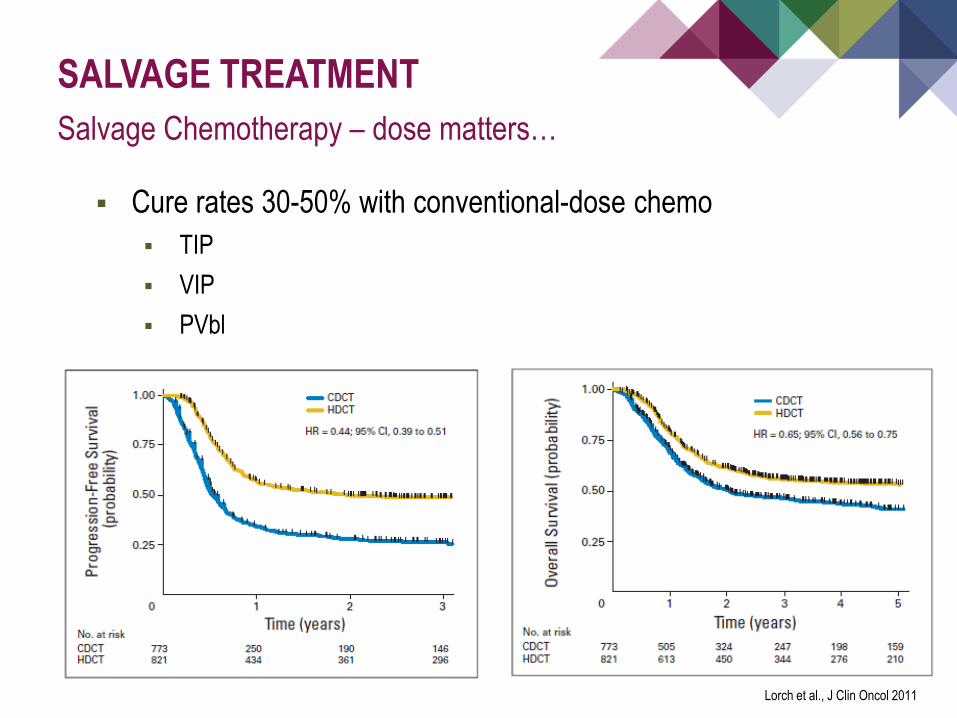
SALVAGE TREATMENTSalvage Chemotherapy – dose matters…
Lorch et al., J Clin Oncol 2011
Cure rates 30-50% with conventional-dose chemo TIP VIP PVbl

TESTICULAR CANCERTIGER Phase III trial

REFRACTORY DISEASELimited Treatment Options
Most active agents
Gemcitabine (oral Etoposide) Oxaliplatin (Temozolomide) Paclitaxel (Irinotecan)
ORR Mono 10-15% Doublet 30-35% Triplet 50%

R/R GERM CELL CANCERSNovel targeted therapies
Many agents investigated TKI (Sunitinib, Pazopanib, Imatinib)
mTORi (Everolimus)
Immune-Checkpoint-Inhibitors (Pembro, Tremelimumab/Durvalumab)
Anitbody-Drug-Conjugates (Brentuximab-vedotin)
No relevant activity in unselected phase II trials!

SURVIVORSHIP CARE

SURVIVORSHIP CAREA Field of Growing Importance
Cancer Registry of Norway, pers. communication

LONG-TERM TOXICITYSide Effects of GCC Treatment
Kier et al., JAMA Oncol 2016
Secondary Neoplasms Leukemia Lung, Bladder,
Sarcoma Pancreas, Stomach
Cardiovascular Events Metabolic Syndrome Neurotoxixcity Pneumonitis, Fibrosis Chronic Kidney Failure Fatigue Hypogonadism / Infertility

TAKE HOME MESSAGE
Most common solid malignancy among men aged ≤ 40 years Extraordinary cure rates >90% over all stages GCNIS as malignant precursor Pure seminoma (SGCT) vs Non-seminoma (NSGCT) AFP and HCG as prognostic and predictive biomarkers
Active surveillance after orchiectomy preferred in CS I seminoma Active surveillance also for CS I non-seminoma
Alternatively 1x BEP in high-risk patients (LVI+) SGCT CS IIA: Radiotherapy 30-36Gy preferred over chemo NSGCT CS IIA/B: Chemo preferred over RPLND
Localised Disease Stages

TAKE HOME MESSAGE
Advanced stages CS IIC-III: IGCCCG risk-stratification Good risk: 3x BEP or 4x EP OS >90% Intermediate/poor risk: 4x BEP or 4x VIP OS 60-90% Consider high-dose VIP + autoSCT for selected cases
NSGCT residues > 1cm have to be surgically removed Salvage treatment still curative
4x TIP, VIP, VeIP conventional options Higher cure rates with HD-Carbo/Eto TIGER trial
Secondary tumors, metabolic syndrome, peripheral neuropathy, renal impairment and infertility important survivorship issues
Advanced Disease & Relapse

EMUC 2019… if you haven‘t been to Vienna!