the 42nd shpa national conference medicines management 2016 · the 42nd shpa national conference...
TRANSCRIPT

A compilation of presentations discussing hospital pharmacy residencies, both in Australia and overseas
The 42nd SHPA National Conference
Medicines Management 2016
Session S5: Value, Vision, and Innovation
Table of Contents
• SHPA’s Andrew Matthews talks about about the SHPA Residency Program (slides 3- 31)
• Leanna Pugliese speaks about life inside a residency program, a perspective from the USA (slides 32 -55)
• Ruki Wijesinghe shares her perspective on setting up a residency program for pharmacists in Singapore (slides 56 - 71)
• Andrew Campbell speaks about ‘Residency – What’s in it for me?’: an early career pharmacist perspective (slides 72 -83)
• Russell Hill from Epic Pharmacy speaks about ‘Residency and how to get it’: a director of pharmacy perspective (slides 84 - 97)
Andrew MatthewsGeneral Manager Workforce TransformationThe Society of Hospital Pharmacists of AustraliaMM2016 18 November 2016
PHARMACIST RESIDENCY IN AUSTRALIA: Creating the SHPA Vision

Disclosure In relation to this presentation, I declare the following, real or
perceived conflicts of interest:
Andrew Matthews is an employee of The Society of Hospital Pharmacists of Australia
A conflict of interest is any situation in which a speaker or immediate family members have interests, and those may cause a conflict with the current presentation. Conflicts of interest do not preclude the delivery of the talk, but should be explicitly declared. These may include financial interests (eg. owning stocks of a related company, having received honoraria, consultancy fees), research interests (research support by grants or otherwise) or organisational interests

Learning objectives and pharmacist competency standards
Learning objectivesAfter this session, the participants will be able to:
• Describe the objectives and potential benefits of pharmacy residency programs
• Describe the individual components of education, teaching and training that make up a residency program
• Describe the competencies and characteristics of pharmacists participating in a program and supervising or delivering a program
• Describe the approaches to residency in different settings and countries
• Describe the requirements for successful implementation of a residency program in a hospital
Pharmacist competency standards* addressed include: 3.1, 3.2, 3.4, 8.3
*National competency standards framework for pharmacists in Australia, 2010
ASHP History of Accreditation• Pharmacy residencies date back to the 1930’s – called internships
– Were designed to train pharmacists in hospital pharmacy management
• ASHP’s first involvement was in 1948 with the development of standards for internships
In 1962, ASHP established an accreditation process and standards for residencies in hospital pharmacy• Term “internship” was replaced with “residency”
• During the early 1970’s, clinical practice residencies grew rapidly and accreditation standards for clinical pharmacy and specialized residencytraining were established
Acknowledgment: slides from Janet A. Silvester, Pharm.D., MBA, FASHP. Vice President, Accreditation Services Office, ASHP. Presented at SHPA Residency Symposium 2016

Why ASHP?• ASHP believed that residency training was a critical part of the
preparation for pharmacists to work in hospitals and health systems
• It was the right thing to do (mission > margin)
• ASHP subsidized the accreditation of residency training programs for about 45 years
• Now we have reached a critical mass of programs and the accreditation process pays for itself
Around the WorldExperience of Pharmacy Residency in the UK
Paul TonerDeputy Director of Pharmacy (Clinical Operations)
Royal Melbourne Hospital

AROUND THE WORLDPHARMACY RESIDENCY PROGRAMS IN CANADA
Dr Chris Freeman
@topherfreeman
Around the World …......
Sharing Singapore’s Experience
Ruki Wijesinghe, Pharm.D., BCPP.
Institute of Mental Health, Singapore
SHPA Residency Symposium
5th September 2016

www.shpa.org.au

www.shpa.org.au

www.shpa.org.au


Residency: by 2017…
Implementation of the first phase of a structured, formalised, supported and accredited national two-year residency program for pharmacists in
their foundation years.

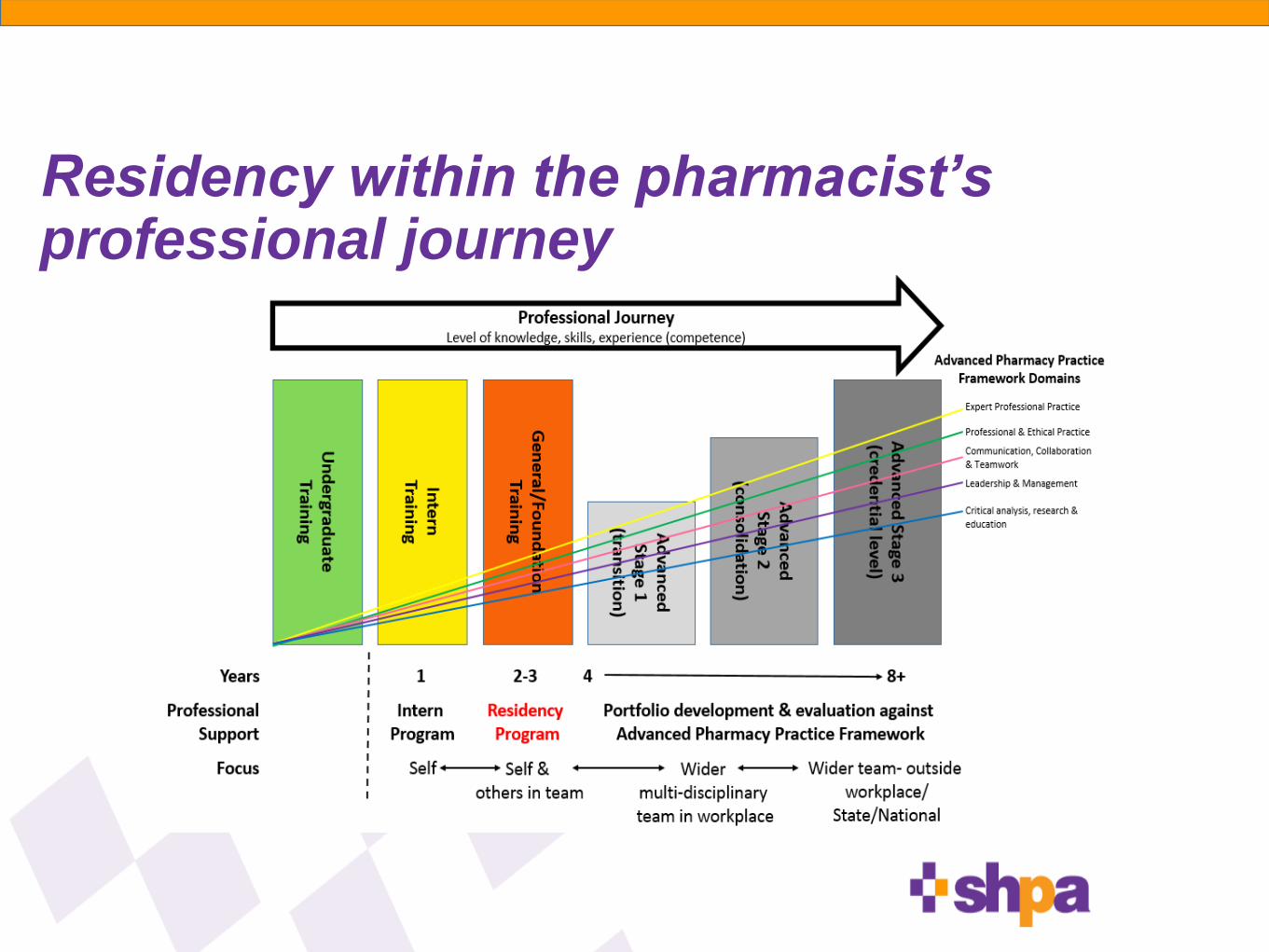
Residency within the pharmacist’s professional journey

Why?
•Ever-changing healthcare systempharmacy workforce must evolve
need enhanced capacity, capability and flexibility
•SHPA Future Summit feedbackSupport for developing models of clinical fellowships and residency-type
programs to develop pharmacists to be able to perform expanded practice
roles
•Lack of existing formal or structured experiential training
programs Potential barrier to strengthening and expansion of pharmacists’ roles and
scopes of practice
Existing programs variable or ad-hoc
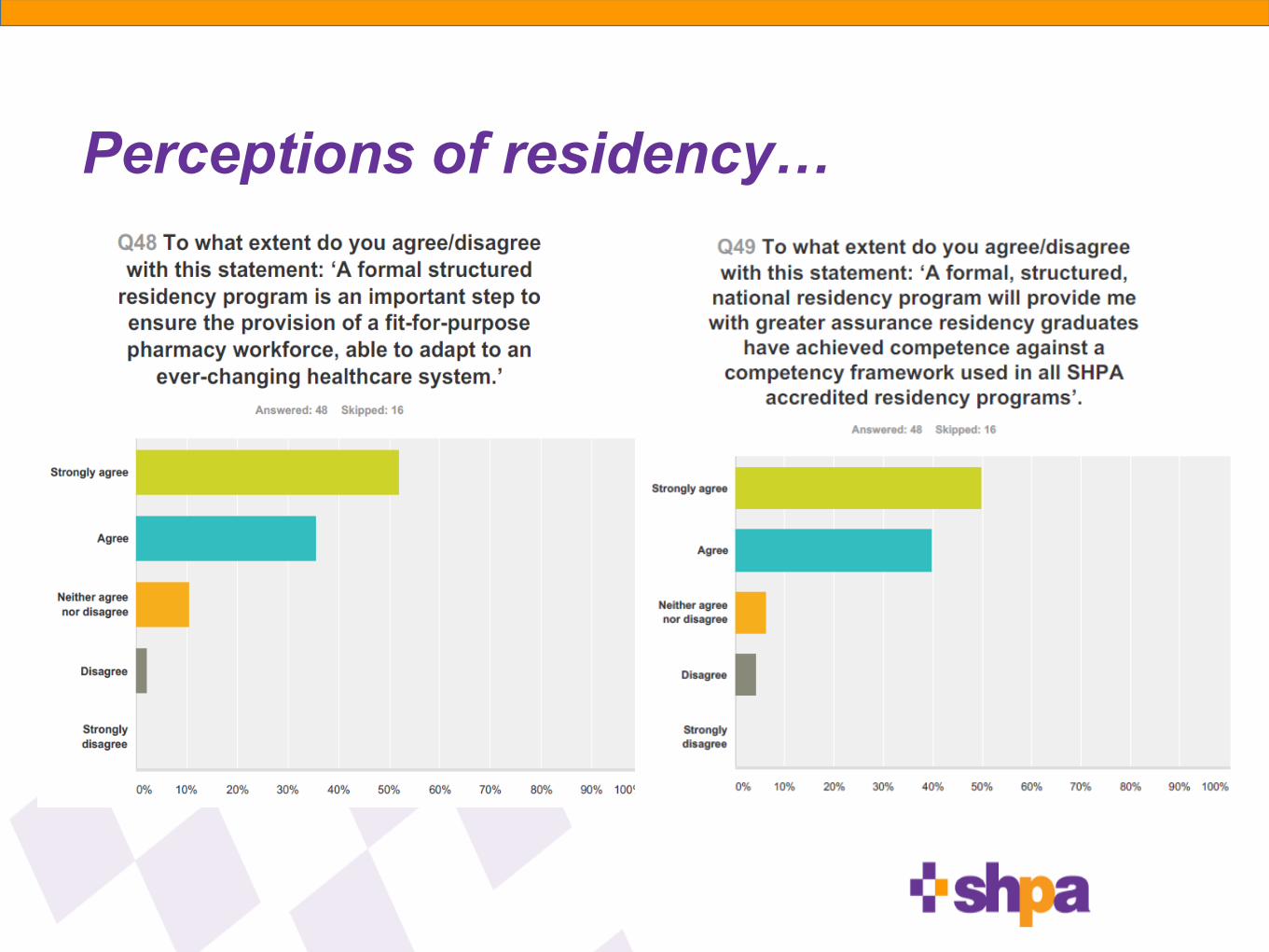
Perceptions of residency…
Objectives and key principles
www.shpa.org.au

Accreditation Standards
The Standards cover 4 Domains:
•Resident- Program relationship
•Capacity and experience of department and staff
•Range of pharmacy services and ability to deliver the residency curriculum
•Commitment to professional development
www.shpa.org.au

Accreditation
•residency sites will exhibit a culture that demonstrates a commitment to education and training for staff.
•the breadth of practice based experiences may be achieved through a combination of home site and rotation site practice.
•the Accreditation Standards provide the requirements for a residency program site to achieve, in order for a residency program to be accredited by SHPA.

Accreditation
• 32 applications received
• covering 57 hospitals
• likely intake of >130 residents
• detailed evaluation of residency program applications against SHPA Accreditation Standards for pharmacy residency programs
• 24 residency programs accredited
www.shpa.org.au/accredited-sites

Across all applications, there were many
excellent examples of innovative experiential
learning ideas, and sound evidence of
detailed structures already in place with
many skilled staff ready to coordinate and
support a future residency program

Snapshot of applications
• Residency Program accreditation applications by AIHW Hospital Peer Group

Snapshot of applications
• Residency Program accreditation applications by State/Territory

Snapshot of applications
• Residency Program accreditation applications by AIHW Hospital Peer Group remoteness measure

Sites promoting their accreditation

Thank you
@APharm68
www.shpa.org.au
www.shpa.org.au/hospital-pharmacy-residency

➤ End of Andrew Matthews’ presentation
➤ Go back to Table of Contents

BORN IN THE USA - A USA RESIDENCY EXPERIENCE
Inside a Residency Program: Surviving and Thriving
Leanna Pugliese Pharm.D.Investigational Medicines Pharmacist
Calvary Mater Newcastle

Disclosure
In relation to this presentation, I declare the following real, or perceived conflicts of interest:
NIL
A conflict of interest is any situation in which a speaker or immediate family members have interests, and those may cause a conflict with the current presentation. Conflicts of interest do not preclude the delivery of the talk, but should be explicitly declared. These may include financial interests (eg. owning stocks of a related company, having received honoraria, consultancy fees), research interests (research support by grants or otherwise) or organizational interests

➤ Describe the objectives and potential benefits of pharmacy residency programs
➤ Describe the individual components of education, teaching, and training that make up a residency program
➤ Describe the competencies and characteristics of pharmacists participating in a program and supervising or delivering a program
➤ Describe the approaches to residency in different settings in countries
➤ Describe the requirements for successful implementation of a residency program in a hospital

➤ Post graduates in the US can pursue further training with either a clinical focus(residency program) or a research focus (fellowship training)
➤ Presently in the US there are 3 different types of PGY-1 residencies:
➤ Pharmacy Practice (Hospital)
➤ Community
➤ Managed Care
➤ A PGY-1 residency is equivalent to THREE years working as a clinical pharmacist
➤ Grow exponentially in clinical skills and gain experience in teaching, research, pharmacy operations, and medication use policy and evaluation
WHY DO A POST GRADUATE (PGY-1) RESIDENCY??

THE PATH TO RESIDENCY
➤ Throughout Pharmacy School
➤ Build your CV and demonstrate time management skills
➤ Leadership activities
➤ Work experience
➤ Research experience
➤ Rotations

Tucson, Arizona


THE PATH TO RESIDENCY
➤ Admission to a PGY-1 residency will usually require the following…
➤ Cover letter
➤ Curriculum vitae
➤ Three professional letters of recommendation (preceptors, professors, employers)
➤ Official transcript from accredited School of Pharmacy
➤ Personal interview
➤ Employment application process
YOU MADE IT! THE RESIDENCY
➤ Must be a licensed pharmacist
➤ Year long program
➤ 10 rotations, mandatory & electives
➤ Longitudinal rotations
➤ Evaluations post rotation w preceptor & resident as well as quarterly (reciprocal)
➤ Paid (Stipend) + Benefits
➤ Mandatory on-call
➤ Must be ACLS, BLS, and First Aid certified
➤ Must complete a major “writing project” or similar
➤ Develop skill set writing a paper for publication

Puget Sound Area/Seattle, Washington

MULTICARE HEALTH SYSTEM (MHS)
➤ Comprised of Tacoma General Hospital and Mary Bridge Paediatric Hospital
➤ 437-bed acute care tertiary hospital, 82-Paediatric beds
➤ Adult & Paediatric Trauma (level II)/Emergency Services
➤ Regional Heart Institute recognized as a centre of excellence
➤ Medical, Cardiac, Neuro Intensive Care units
➤ Physician order entry, electronic health record, barcode & carousels (central rx), electronic dispensing cabinets, smart pumps
➤ 24/7 Pharmacy service
THE RESIDENCY
➤ MHS Core Objectives
➤ Develop the resident’s competence in providing patient care
➤ Competence in practice management
➤ Require the resident to complete an appropriate major project
➤ Program Goals
➤ Perform in a clinically oriented hospital or ambulatory clinic position
➤ Be prepared to be highly successful in advanced training such as PGY2 residency
➤ Perform in an introductory supervisory or management position
➤ Meet standards for hire within the MHS pharmacy system
THE RESIDENCY
Role of the Preceptor
➤ Take part in the development of the goals, objectives, and activities prior to beginning of each resident training experience
➤ Attempt to cover, through informal clinical conferences, each main area of clinical pharmacy practice associated with their specialty
➤ Focus on any of the resident's areas of special interest and growth
➤ Attempt to allow the resident as much "hands on" experience as possible in dealing with patients, medical staff, and nursing staff
➤ Required to complete a summative evaluation of the resident's performance at the end of each learning experience, and submit the document to the program director

THE RESIDENCY
➤ Clinical pharmacy services include patient monitoring, education of medical house-staff, drug use evaluation and clinical research activities
➤ Pharmacokinetic Services
➤ Anticoagulation Services
➤ Parenteral Nutrition Services
➤ Cardiac Arrest Team Participation
➤ Congestive Heart Failure Clinic Staffing
➤ Decentralised Pharmacist role
➤ Do not have primary dispensing responsibilities

MY RESIDENCY EXPERIENCE - ROTATIONS
Adult Medical/Surgical & Adult Critical Care
➤ Ward round
➤ Collaborative practice agreement(s), ie. cancer pain management
➤ Chemo orders
➤ Antiemetics per pharmacy
➤ All vanc/aminoglycosides per pharmacy
➤ TPN per pharmacy
➤ Anticoagulation per pharmacy
➤ Diabetes Management and Education
➤ Attend all codes
➤ Orders

MY RESIDENCY EXPERIENCE- ROTATIONS
Family Practice Medicine/HIV
➤ Anticoagulation clinic
➤ Pharmacist run w collaborative practice agreement
➤ Onsite for medication management, compliance issues, patient care
➤ Cholesterol/DM management
➤ HIV medication management
➤ Staff education

MY RESIDENCY EXPERIENCE- ROTATIONS
Adult Ambulatory Haematology/Oncology
➤ Satellite clinic w hood space
➤ Oversee compounding of all clinic/inpatient adult chemo
➤ Morning report
➤ Check all chemo orders
➤ Antiemetics per pharmacy
➤ Coordinate compassionate access programs w physician/patient

MY RESIDENCY EXPERIENCE- ROTATIONS
Paediatrics
➤ Paediatric Intensive Care (PICU) - 24 beds
➤ Ward rounds
➤ Methadone/midazolam weaning protocols
➤ Orders
➤ Patient/Staff education
➤ Paediatric Acute Care - 58 med/surg beds
➤ Inpatient chemo
➤ Neonatal Intensive Care (NICU)
➤ Check/review all TPNS
➤ Paediatric Outpatient Haem/Onc Clinic
➤ Review & compounding of chemo orders
➤ Outpatient dispensing

MY RESIDENCY EXPERIENCELongitudinal Rotations
➤ Major Project
➤ Pharmacy Management
➤ Weekly meetings w Director
➤ Participation on at least one clinical hospital committee
➤ Surgical Care Improvement Project (SCIP)
➤ Journal club
➤ P&T Committee (monthly)
➤ One MUE and at least 3 drug monographs presented
➤ Congestive Heart Failure Clinic staffing
➤ Drug Information
➤ 2 formal DI response submissions for each rotation
➤ Proficiency in literature searches, citations, and graded sources of literature
➤ Staffing
➤ Weekends, at least once monthly up to every other weekend
➤ Assignment to a decentralized area towards end of year when resident is independently responsible for all services in that area
MY RESIDENCY EXPERIENCE- MAJOR PROJECT
Febrile Neutropenia Protocol and Guideline Development
➤ Literature review on febrile neutropenia guidelines
➤ Retrospective chart review with all ICD 9 codes relating to “febrile neutropenia”
➤ Analysis on appropriateness of antibiotics used in FN
➤ Inpatient vs outpatient
➤ Approval from pertinent treating physicians
➤ Forms committee approval
➤ Staff education
➤ Presentation at Western States Conference

Western States Conference
May the odds be ever in your favour…

WESTERN STATES
➤ Four day annual conference
➤ Provides pharmacy residents an opportunity to make brief, formal presentations on their residency projects or ongoing research in a relaxed yet professional setting
➤ Discuss clinical or administrative case experiences while engaging in open forum discussions and meeting leaders in the field of pharmacy practice
➤ Networking with colleagues
➤ Network with industry exhibitors
➤ Broaden relationships with those outside of the hospital setting
The residents of today are the leading practitioners and educators of tomorrow


➤ End of Leanna Pugliese’s presentation
➤ Go back to Table of Contents

Building a Residency Program:
Making it Work
Ruki Wijesinghe, Pharm.D., BCPP.
Medicines Management 2016 – 42nd SHPA National Conference18th November 2016, Perth, Australia
DISCLOSURE
In relation to this presentation, I declare that I have
no real or perceived conflicts of interest

LEARNING OBJECTIVES
After this session, the participants will be able to:
1. Describe the objectives and potential benefits of pharmacy residency programs
2. Describe the individual components of education, teaching and training that make up a residency program
3. Describe the competencies and characteristics of pharmacists participating in a program and supervising or delivering a program
4. Describe the approaches to residency in different settings and countries
5. Describe the requirements for successful implementation of a residency program in a hospital

OVERVIEW
2020 vision
Funding & Training
‘Specialist’ pharmacist development pathway
PGY1
Preceptor development & competencies
Challenges

VISION FOR THE FUTURE
ACCP & ASHP calls for residency training to be
the minimum standard for providing direct patient
care by 2020
Advocate that clinical pharmacists be board
certified
1. Murphy JE, Nappi JM, Bosso JA et al. American College of Clinical Pharmacy’s vision of the future: postgraduate pharmacy
residency training as a prerequisite for direct patient care practice. Pharmacotherapy. 2006; 26:722-33
2. American Society of Health-System Pharmacists. ASHP long-range vision for the pharmacy work force in hospitals and health
systems. Am J Health-Syst Pharm. 2007; 64:1320-30

PROJECTED NUMBERS FOR RESIDENCY
TRAINING BY 2020
Based on:
Transition from 4-yr BSc to Pharm.D.
Residency positions needed (consider at least 75% will
enter direct patient care roles)
Annual growth in the # of residency positions
Need rapid establishment of new sites to meet the 2020 goal
Pharmacist work force in 2020: Implications of requiring residency training for practice Thomas J. Johnson Am J Health-Syst
Pharm. 2008; 65:166-70

FUNDING & TRAINING
MOH scholarships (2008 – 2012)
35 US residency training
Established local residencies
‘Grandfatherd-in’ specialist pharmacists
43 Pharm.D. or masters
3-5 year bond (service period)
Eligible to apply for a residency
Part-funded by the employer (hospital)
ASHP Pharmacy Preceptors Conference
Preceptor development
International Pharmaceutical Federation (FIP). Advanced Practice and Specialisation in Pharmacy: Global Report 2015. The Hague:
International Pharmaceutical Federation; 2015.

SINGAPORE PHARMACY “SPECIALISTS”Career Pathway Framework 2009
Professional, Clinical or Research track
Pharmacists Registration Act 2007
Made provisions for accreditation and registration of ‘specialists’
Established Pharmacy Specialists Accreditation Board
Maintain the register of specialists (oncology, cardiology, infectious disease, psychiatry, geriatrics)
Developed Accreditation Standards
Accredit training programs (residency) to develop specialists
Review the need for new specialties
https://www.moh.gov.sg/content/moh_web/healthprofessionalsportal/pharmacists/career_practice/pharmacy_specialist_training_accreditation.html
International Pharmaceutical Federation (FIP). Advanced Practice and Specialisation in Pharmacy: Global Report 2015. The Hague: International
Pharmaceutical Federation; 2015

SPECIALIST DEVELOPMENT PATHWAY
International Pharmaceutical Federation (FIP). Advanced Practice and Specialisation in Pharmacy: Global Report 2015. The Hague: International
Pharmaceutical Federation; 2015.
Post BSc Year 1
Pre-registration - practising certificate
Year 2-3
Work experience
Year
4-5Master in Clinical Pharmacy or (after 2020) Pharm.D.
Year 6 PGY1 (mandatory after 2020), BCPS
Year 7 PGY2, Board certification in speciality
Year 8 Post-residency practice
Year 9 Specialist registration - practising certificate
PGY1 – 12 MONTHS
6 core rotations
Infectious disease, general medicine, critical care, ambulatory care, medication safety & informatics, management & leadership
4-6 weeks each
Longitudinal residency project & manuscript
1 selective core + 3 elective rotations
[Cardiology, nutrition, renal] + [geriatric, hematology, oncology, neurology, pediatrics]
4-5 weeks each
Training sites: major tertiary hospitals (NUH, SGH, TTSH)
Evaluation: formative + summative for each rotation
RESIDENCY PRECEPTOR DEVELOPMENT
Identify potential staff to be groomed as preceptors
Plan for post-graduate education for identified staff
Teaching Cert / Workshops / Diploma / MHPEd
Funding, hire backfill
Provide clinical practice opportunities (manage or
develop new clinical services) – Clozapine Clinic
Allow protected time for teaching
ACCPs Clinical Practice and Preceptorship Program in collaboration with
NUS held the initial 3-day workshop in May 2014 for pharmacy educators
of 10 hospitals in Singapore
RESIDENCY PRECEPTOR COMPETENCIES
Teaching record (awards, student evaluations)
‘Model’ practitioner (board certification, specialist)
Contribution to practice (QI projects, research supervision)
Committee appointments (local, national)
Publications or conference presentations
Peer reviewer of manuscripts /conference papers
Member of professional organizations (active contribution)

OVERCOMING CHALLENGES
Standardization of portfolio evaluation process
Timeframe for adequate portfolio development
Involvement of pharmacy managers to disseminate information
Communication, marketing & promotion
Application submission via pharmacy managers
‘Scope’ of resident / specialist practice
Collaboration with physicians to deliver care as a ‘team’

➤ End of Rukmalee Wijesinghe’s presentation
➤ Go back to Table of Contents

RESIDENCY:WHAT’S IN IT FOR ME?
Andy Campbell
Pharmacist
Sir Charles Gairdner Hospital

SIR CHARLESGAIRDNER
HOSPITAL
➤
➤
➤
➤
➤
➤
~ 6 0 0 bed tertiary hospital
Major teaching centre; strong
links with all universities in
WA
Part of QEII
WA’s largest cancer centre
Principle site for neurosurgery
and liver transplants
Home of Nobel Laureate
Barry Marshall

PHARMACY DEPT
➤
➤
➤
Approx. 60 pharmacists and 30
support staff
Inpatient, outpatient
dispensaries and aseptic
manufacturing service (ASU)
Clinical service to all major
wards 5 days a week
➤
➤
➤
Inpatient dispensary, ASU
and roaming pharmacist on
weekends/holidays
Outpatient cancer and CF clinic
Clinical trials

➤
➤
6 interns per year
Rotations through:
➤
➤
➤
➤
➤
➤
Inpatient and outpatient
dispensaries
Intern-run Satellite
dispensary
ASU
Clinical rotations
CoNeCT
Projects
INTERN PROGRAM

Post-grad?
What opportunities exist?
How do I get where I want to be?
I need experience… but how?
Workplace culture? Mentors?
Where do I want to be in 5 years?
Where will pharmacy be in 5years?
INTERNSHIP DONE. NOW WHAT?
I got asked to fill in on this ward and I’ve been here eversince!
Here’s a purple pen… good luck!
LOOKING TO THOSE AROUND US

Does my workplace culture support personal professional development?
What types of support are available? How likely is it that I’ll get a shot?
Is there someone I can talk to?
LOOKING TO THOSE AROUND US

LOOKING TO THOSE AROUND US

Medical colleagues Nursing colleagues
LOOKING TO THOSE AROUND US
PHARMACIST RESIDENCY: THE MISSING LINK?

PHARMACIST RESIDENCY: EMPOWERING THE ECP

➤ End of Andrew Campbell’s presentation
➤ Go back to Table of Contents

The Director’s Chair:Residency and how to get it
Russell Hill

Disclosure In relation to this presentation, I declare the following, real
or perceived conflicts of interest:
A conflict of interest is any situation in which a speaker or immediate family members have interests, and those may cause a conflict with the current presentation. Conflicts of interest do not preclude the delivery of the talk, but should be explicitly declared. These may include financial interests (eg. owning stocks of a related company, having received honoraria, consultancy fees), research interests (research support by grants or otherwise) or organisational interests
None to Declare

Learning objectives and pharmacist competency standards
Learning objectivesAfter this session, the participants will be able to:
• Describe the objectives and potential benefits of pharmacy residency programs
• Describe the individual components of education, teaching and training that make up a residency program
• Describe the competencies and characteristics of pharmacists participating in a program and supervising or delivering a program
• Describe the approaches to residency in different settings and countries
• Describe the requirements for successful implementation of a residency program in a hospital
Pharmacist competency standards* addressed include: 3.1, 3.2, 3.4, 8.3
*National competency standards framework for pharmacists in Australia, 2010

Residency and how to get it?
• Epic Pharmacy awarded provisional accreditation
• Overview of decision making processo Emotional, Rational, Financial
• Our Residency Program
• Private sector challenges
• Future
Background
• Private sector organisationo Private and public sector hospital pharmacy
services
o Servicing 45 hospitals across 6 states and territories
• Small to large tertiary teaching hospital
o Oncology/cancer care focus
o Employ 327 pharmacists and 314 technicians
Why? – the emotional
• “Felt” intuitively makes sense!
• Keen to support developments which progress the profession
• Experienced the success following introduction of the UK STEP program
• Promote private sector hospital pharmacy
• Excitement, energy and a “buzz” around the concept
• Prepared to take a leap of faitho Limited information available at time of application

Why ?– the rational
• Recognition as being committed to developing the profession
• Develop a learning organisational culture with clinical focus
• Improve the quality of our junior pharmacists o Improve patient care
• Formalise and standardise our current trainingo Critical review of existing training
Why? The financial
Costs
• Some unknowns
• Cost of participating in inter-state training (ex WA)
• Clinical pharmacy educator/coordinator role
• Potential salary implications
• ClinCat training
Benefit• Intangible v absolute• Better value from existing
positions• Increased staff engagement
and enablement• Support “new to hospital”
pharmacists and associated risks
• Reduced staff turnover

Our Program
• 738 bed tertiary private teaching hospital that provides intern training and links to local universities
• Initially existing staff (2) will participate (no increase in head count)
• Establish contracted resident positions through
o Natural attrition
o Review of intern posts
• Initially all rotations at the primary hospital
o Future scope to capitalize on the Icon Group Network
• Restructure our rostering to fit in with residency program
• Broad leadership group

Structure
• Keep it simple, easy to implement in the first instanceo Rotation 1- Operations (6 months)
o Rotation 2- Surgical
• 3 months orthopaedics
• 3 months general surgery
o Rotation 3 –Medical
• 3 months general medicine (including respiratory)
• 3 months cardiology
o Rotation 4 – Elective (6 months)
• Oncology/haematology
• Psychiatry
• Care of the elderly

Private Sector Challenges
• Dispensing load as result of dependency on PBS supply models
• Pharmacist to bed ratios may differ
• Challenges around working with multidisciplinary teams
• Different applications of performance evaluation tools
• No defined clinical pharmacy educator position

The Future
• Participate and evaluate
• “Tweak” pharmacy operations so residency becomes seamless
• Leverage benefits across the wider Icon Group
• Specialty residencies

Conclusion
• Private health care is a significant component of the Australian Healthcare landscape
• All patients (public and private) o entitled to receive best care possible
o Access highest standard of pharmacy services
• Congratulate SHPA on the program and adopting a whole sector perspective
• Encourage everyone to get involved!
➤ End of Russell Hill’s presentation
➤ Go back to Table of Contents