the acetabulum, hip joint and proximal femur trauma mi zucker, md
TRANSCRIPT
The ACETABULUM, HIP JOINT and Proximal FEMUR
TRAUMA
MI Zucker, MD
A dr Z Lecture
• On injuries of the “Hip”.
First:
The Acetabulum and the Hip Joint
The ACETABULUM and HIP JOINT
Now, injuries of:
• ACETABULUM
• HIP JOINT
(Later: injuries of the proximal femur, also called the” hip”).
Radiography
• Pelvis AP
• Judet views: 45 degree obliques
• CT
• (MRI: not often needed)
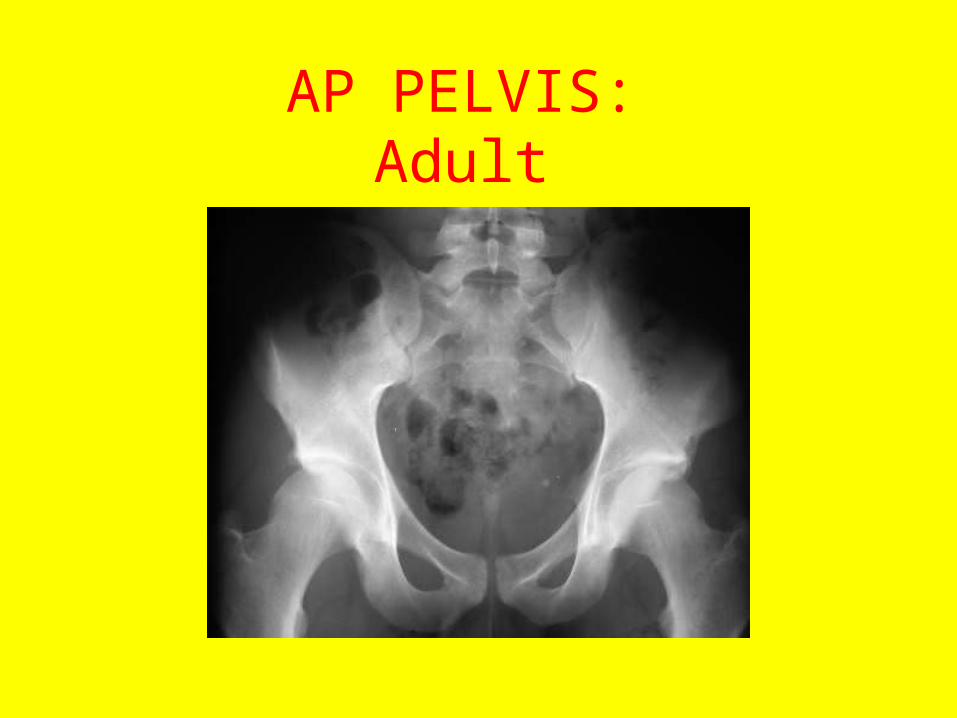
AP PELVIS: Adult
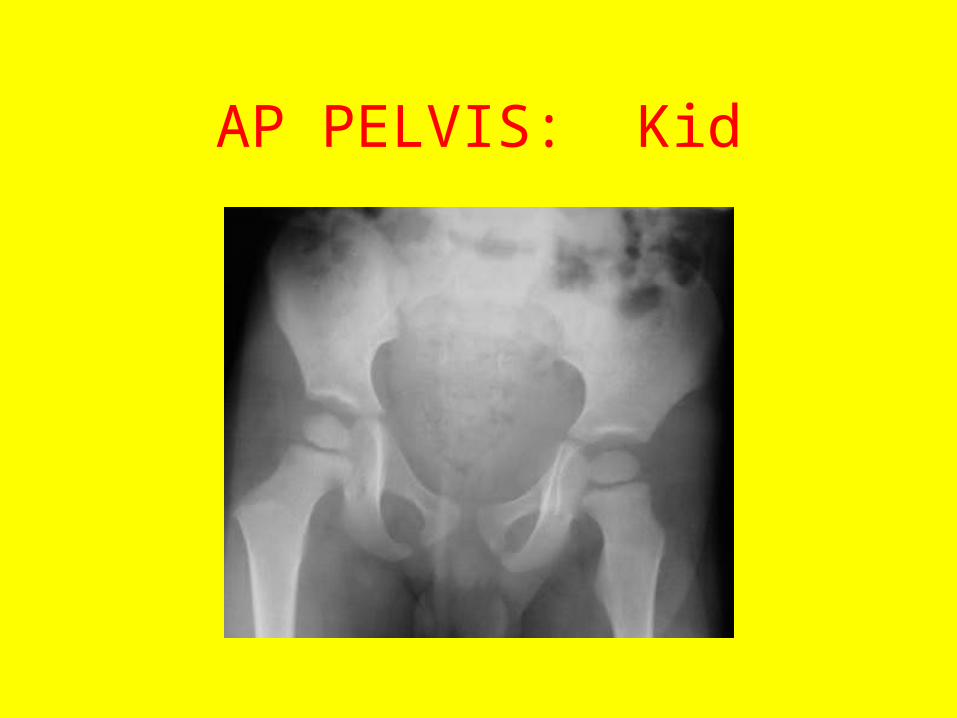
AP PELVIS: Kid
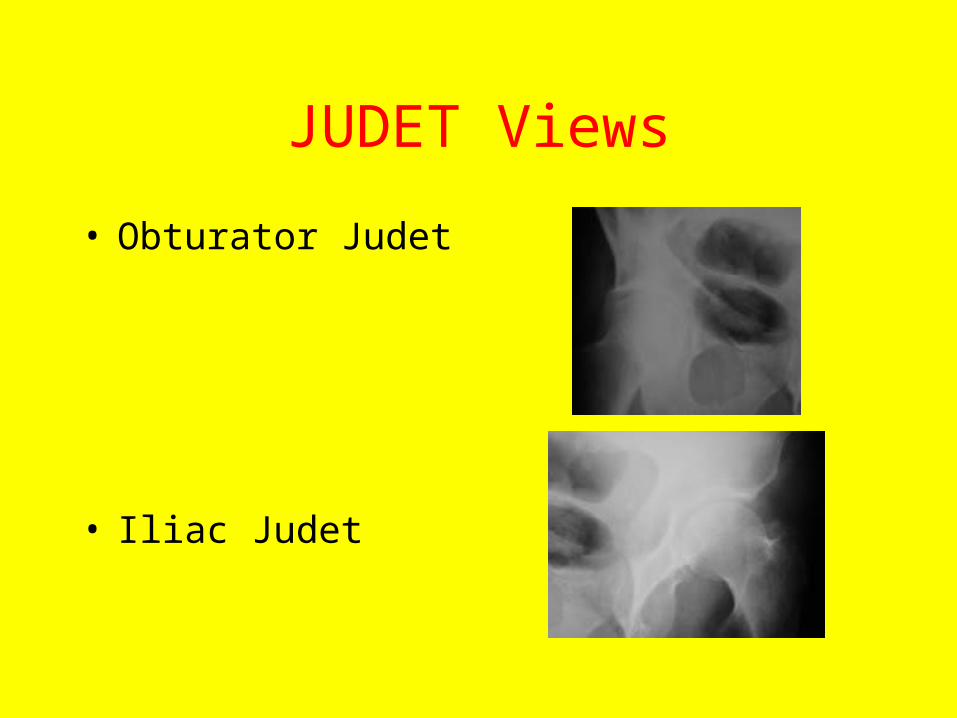
JUDET Views
• Obturator Judet
• Iliac Judet
Anatomy of the Acetabulum
The SIX Lines:
• Iliopubic (iliopectineal)
• Ilioischial
• Tear drop (“U”)
• Dome (roof)
• Anterior wall
• Posterior wall
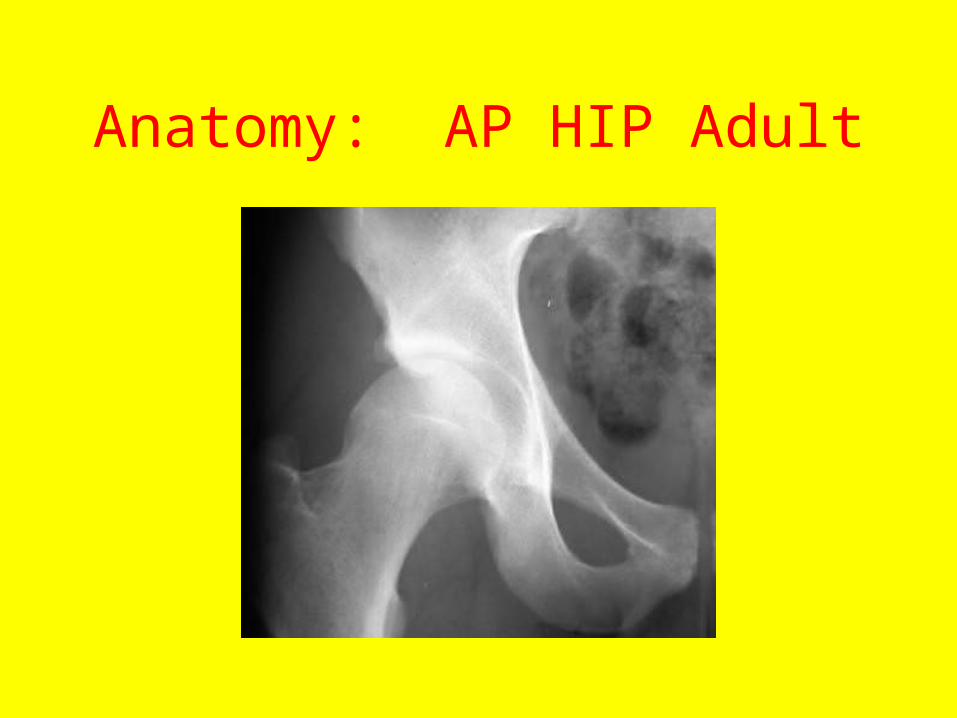
Anatomy: AP HIP Adult
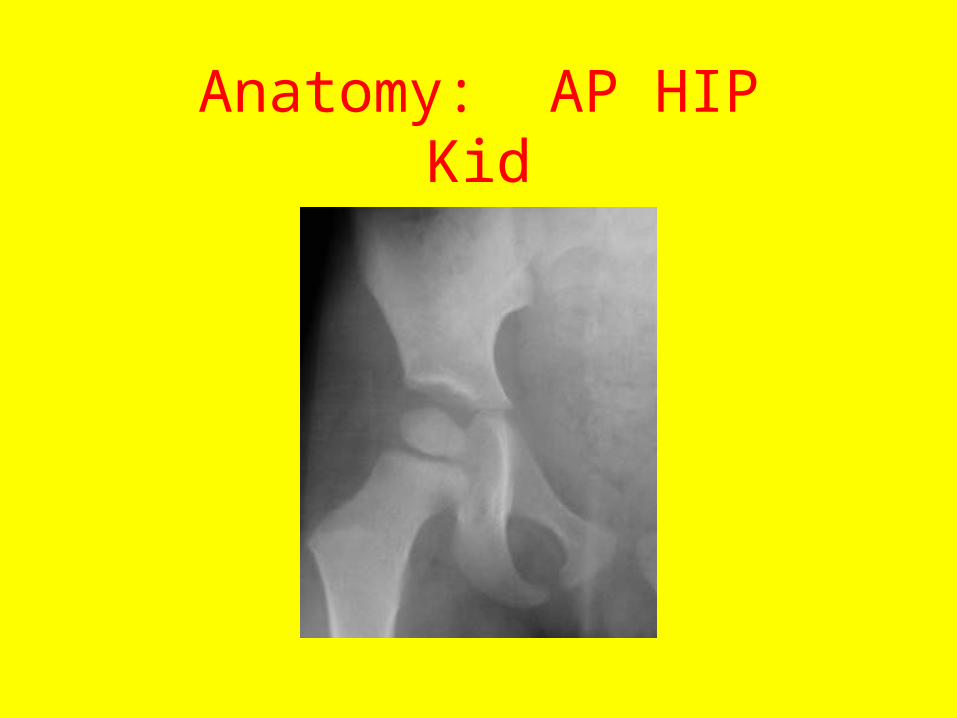
Anatomy: AP HIPKid

Anatomy: Obturator Judet
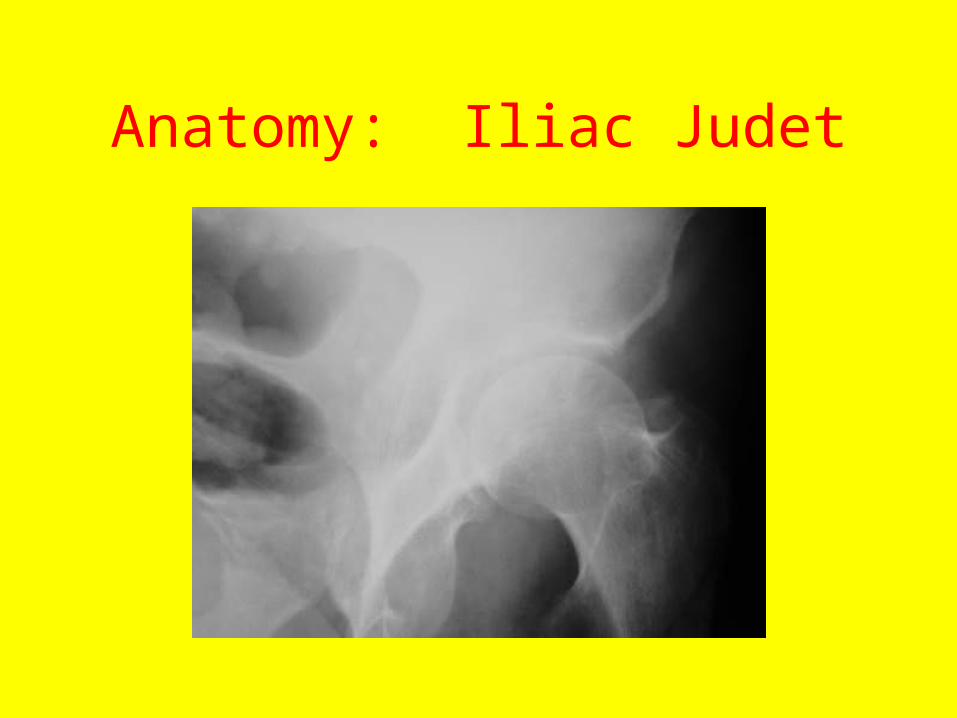
Anatomy: Iliac Judet
Acetabulum Fractures
• The classification of Letournel and Judet is standard.
• But rather than discussing it, we will just describe the major fractures.
Acetabulum Injuries: Mechanisms
• Major force: MVA, fall from a height. Force directed up one leg, or anteriorly or laterally to hip.
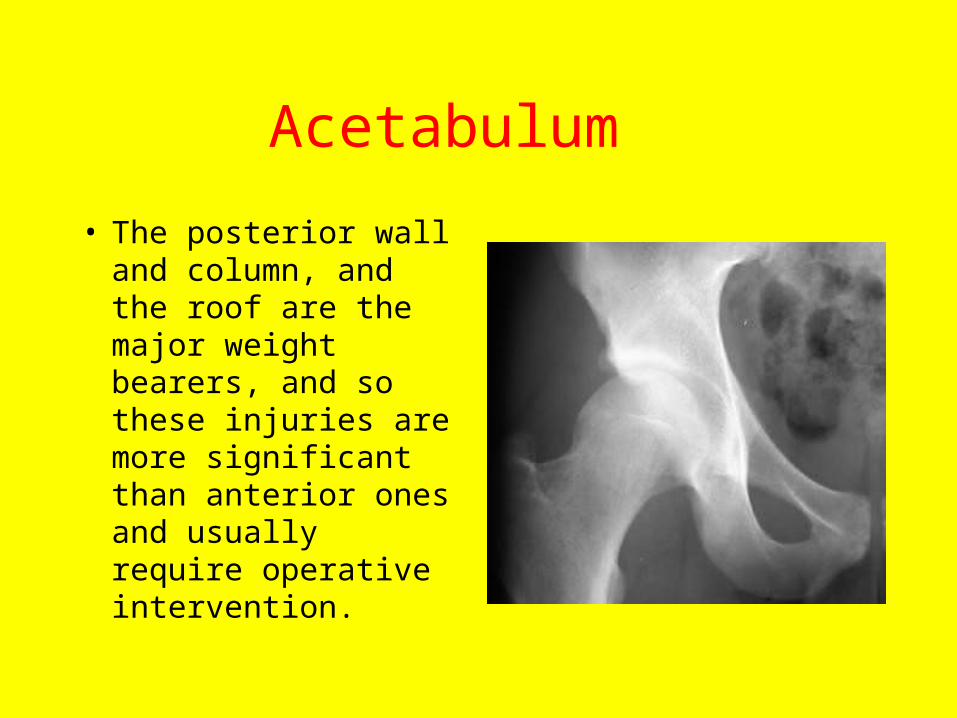
Acetabulum
• The posterior wall and column, and the roof are the major weight bearers, and so these injuries are more significant than anterior ones and usually require operative intervention.
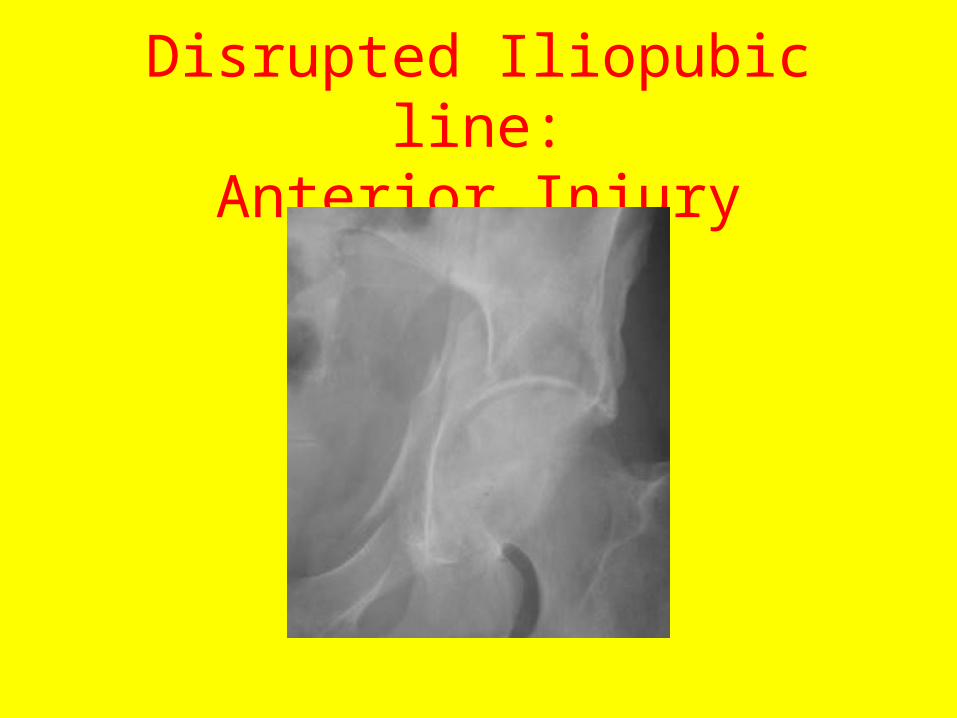
Disrupted Iliopubic line:Anterior Injury
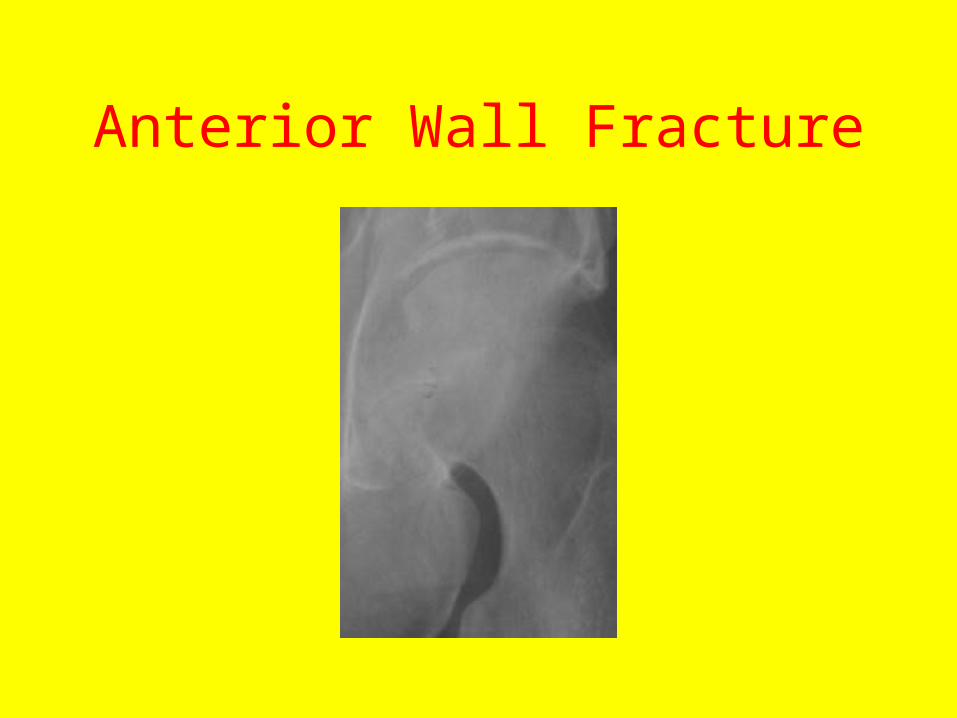
Anterior Wall Fracture
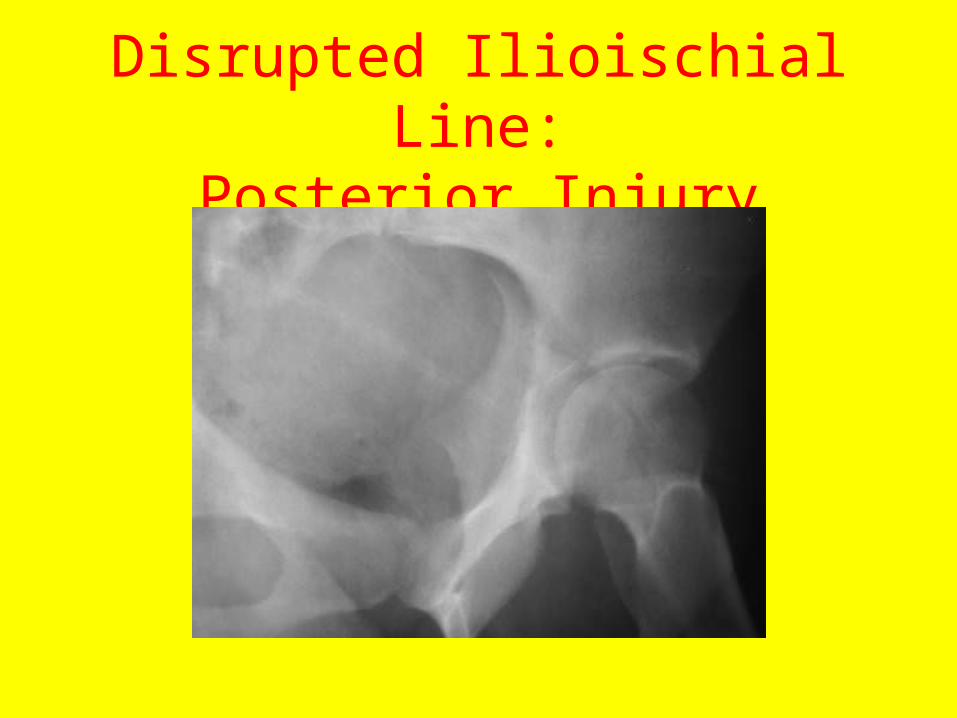
Disrupted Ilioischial Line:Posterior Injury
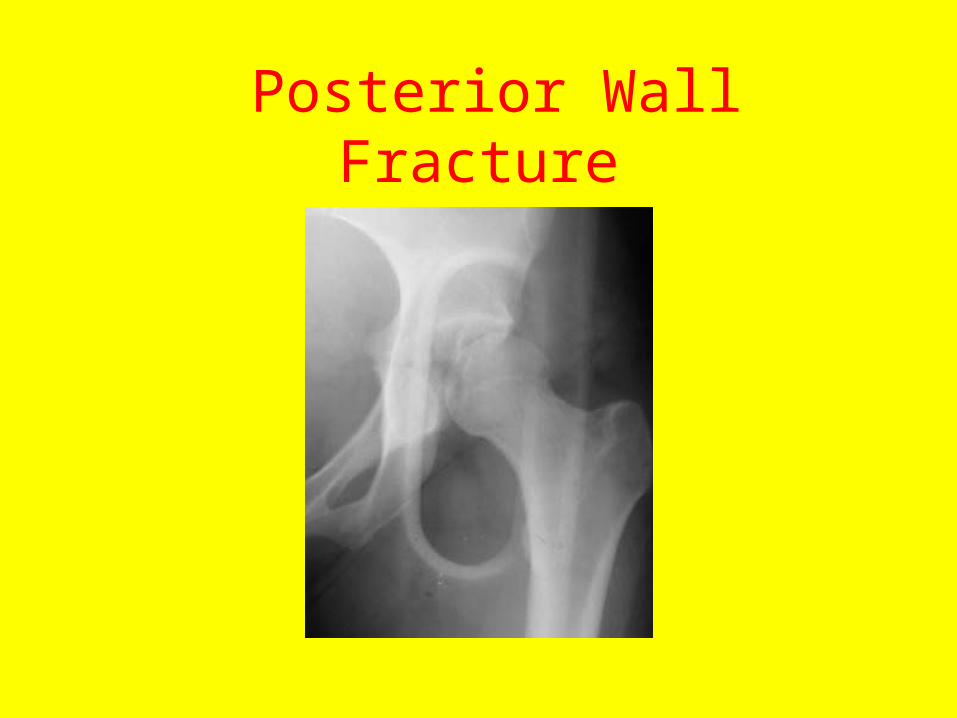
Posterior Wall Fracture
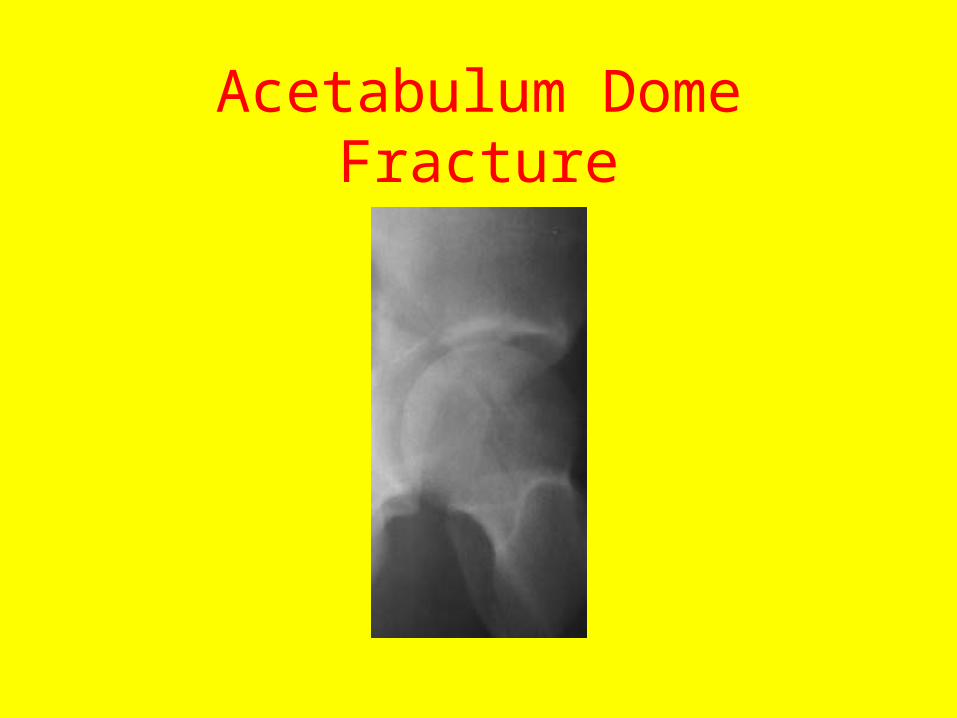
Acetabulum Dome Fracture
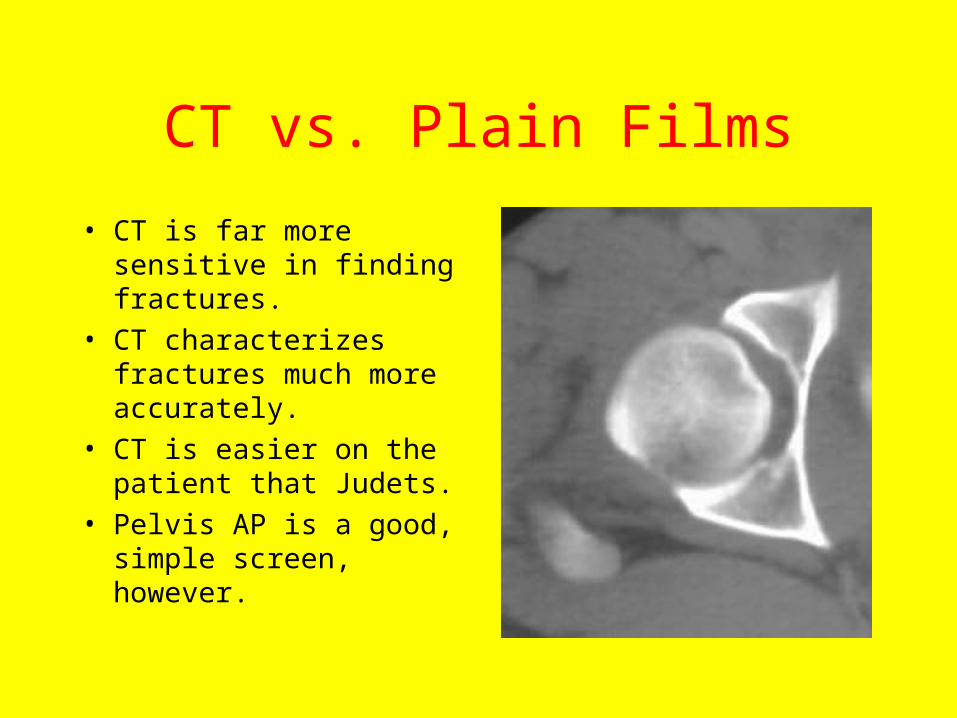
CT vs. Plain Films
• CT is far more sensitive in finding fractures.
• CT characterizes fractures much more accurately.
• CT is easier on the patient that Judets.
• Pelvis AP is a good, simple screen, however.
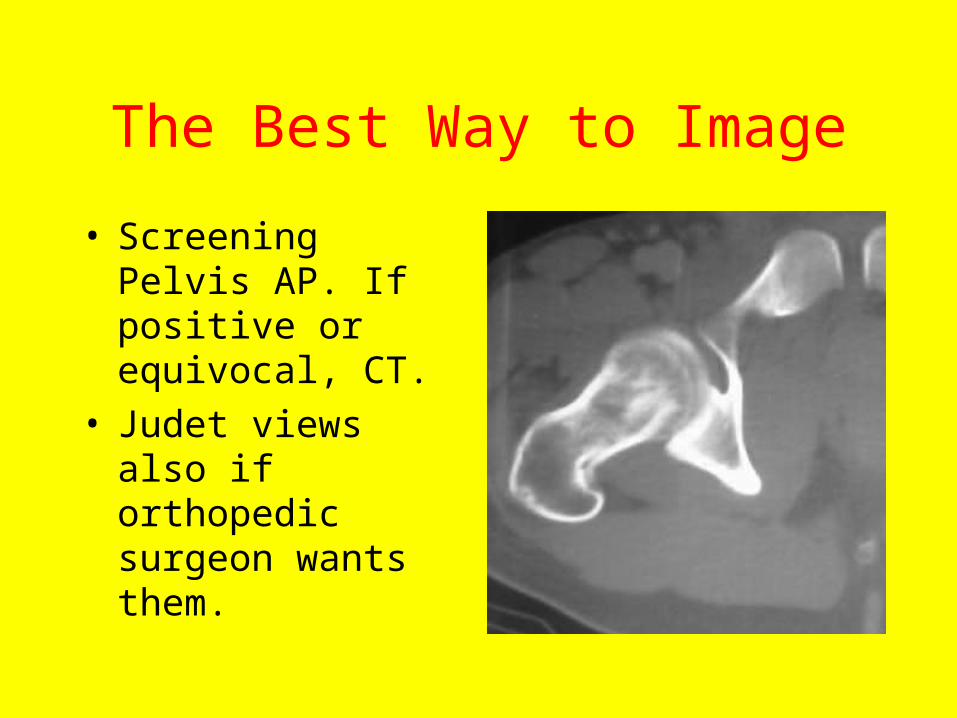
The Best Way to Image
• Screening Pelvis AP. If positive or equivocal, CT.
• Judet views also if orthopedic surgeon wants them.
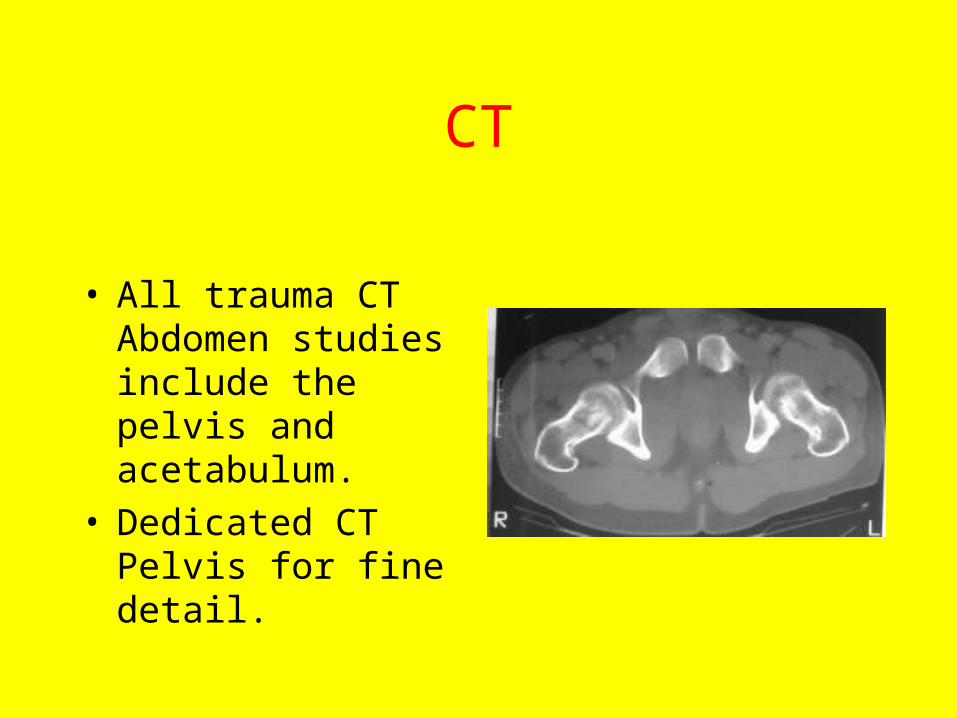
CT
• All trauma CT Abdomen studies include the pelvis and acetabulum.
• Dedicated CT Pelvis for fine detail.
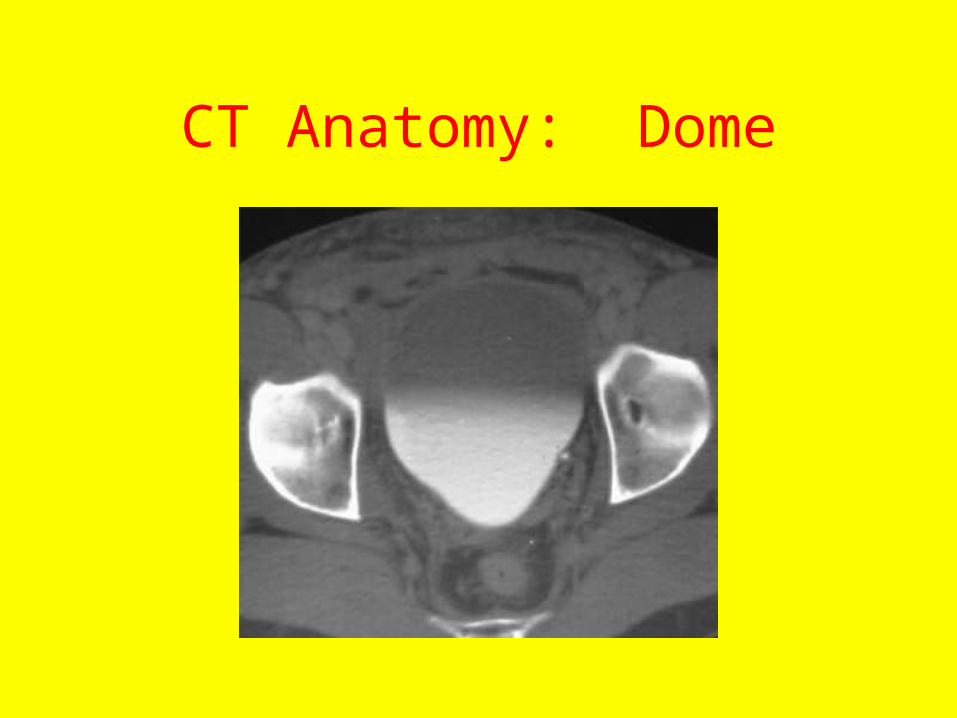
CT Anatomy: Dome
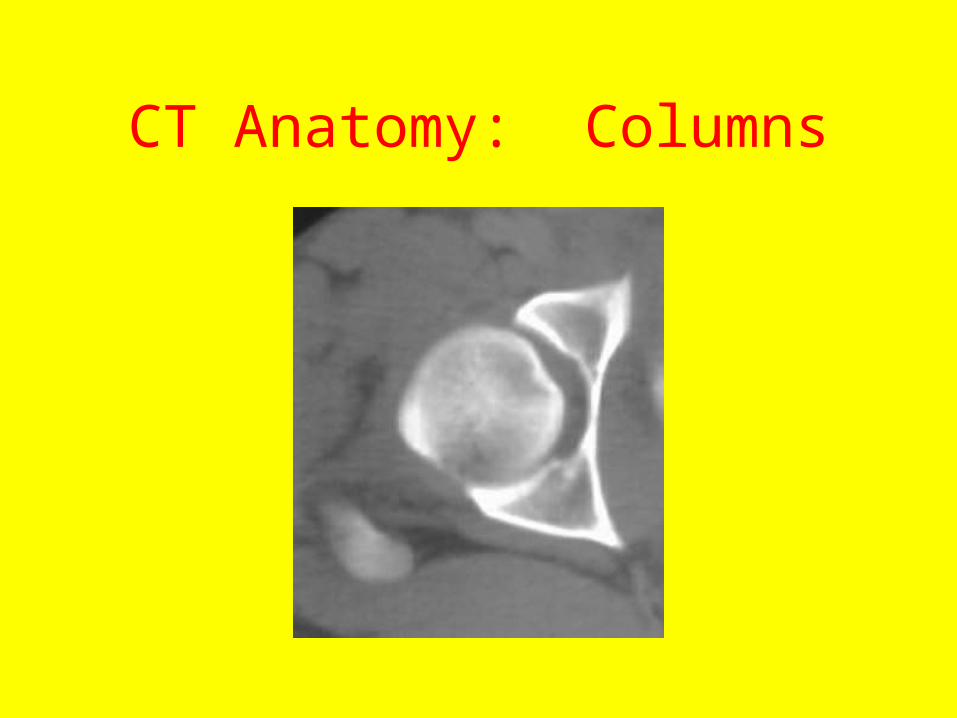
CT Anatomy: Columns
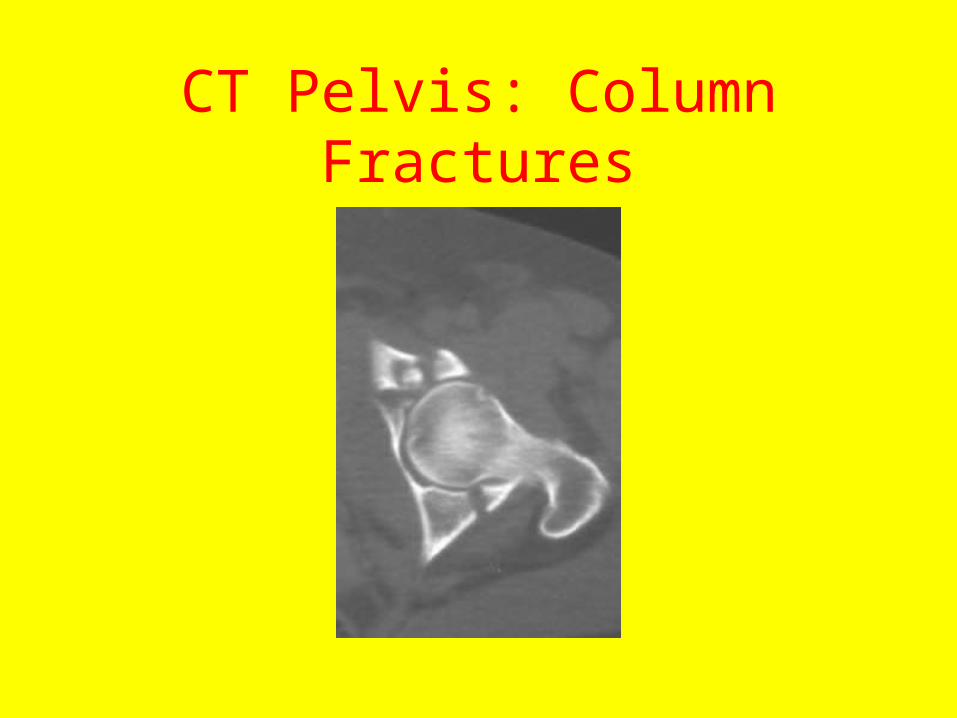
CT Pelvis: Column Fractures
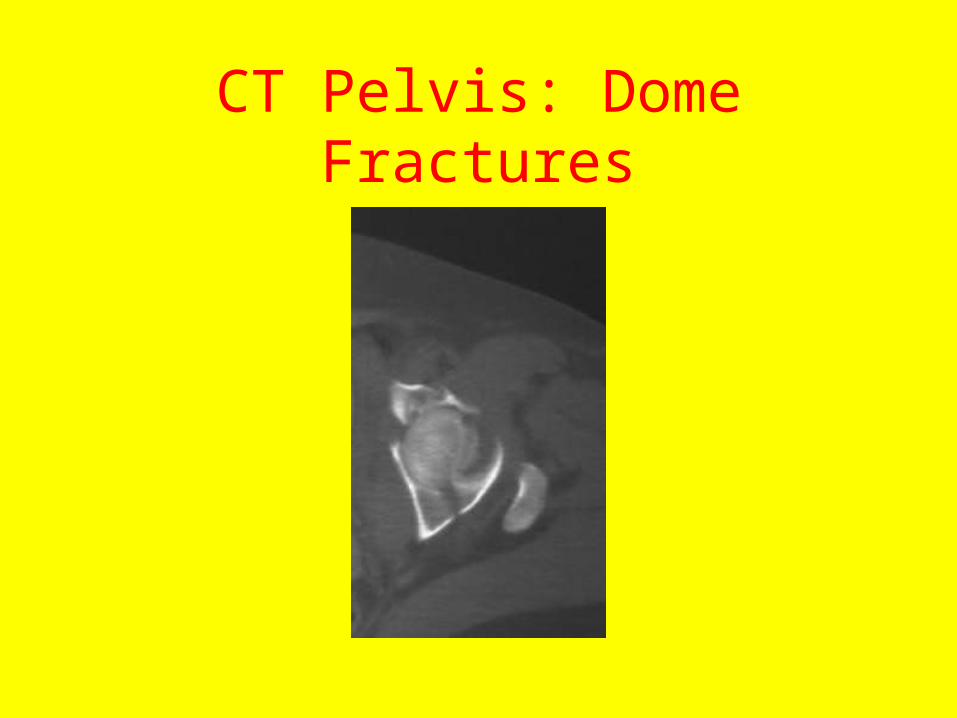
CT Pelvis: Dome Fractures
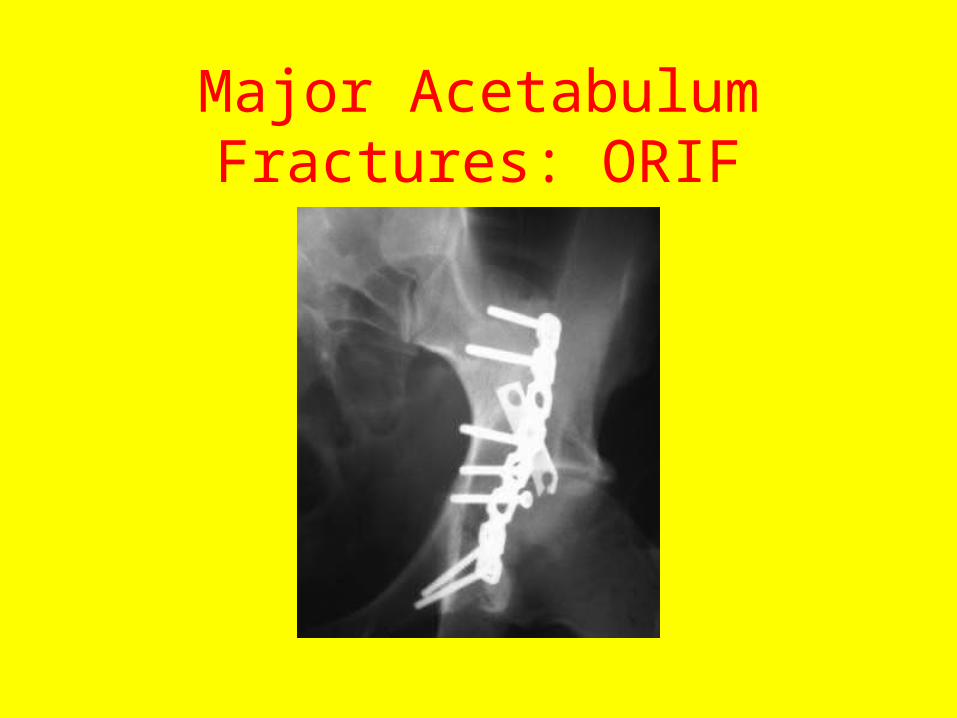
Major Acetabulum Fractures: ORIF
Dislocations of the Hip
• Posterior Dislocations: 90%
• Anterior Dislocations: 10%
• “Central dislocations” are really displaced fractures of the medial acetabulum wall with medial displacement of the femur head.
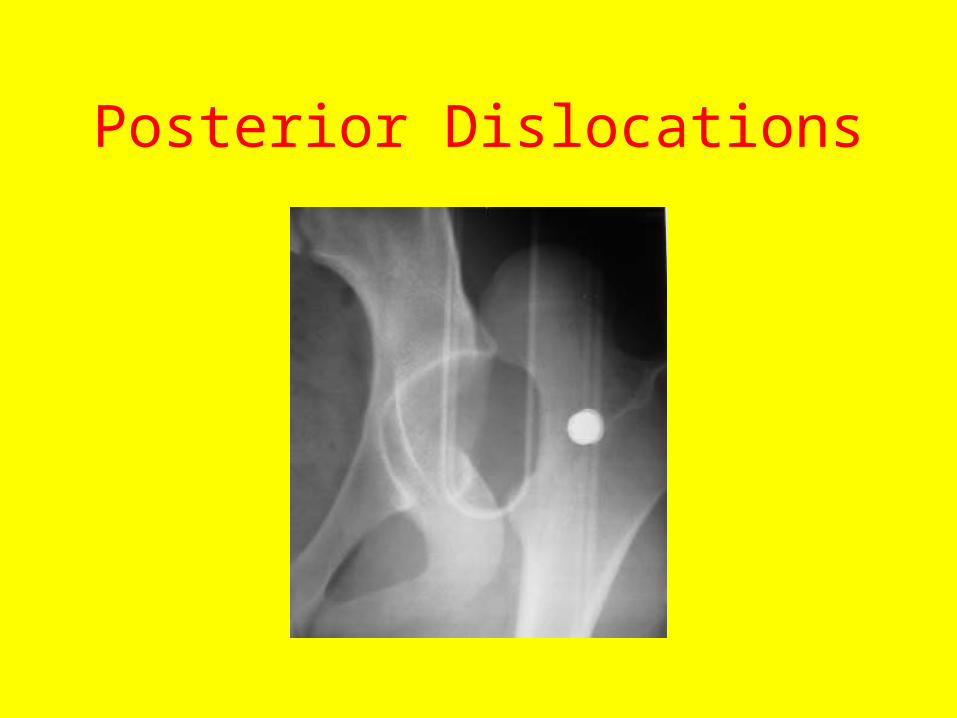
Posterior Dislocations
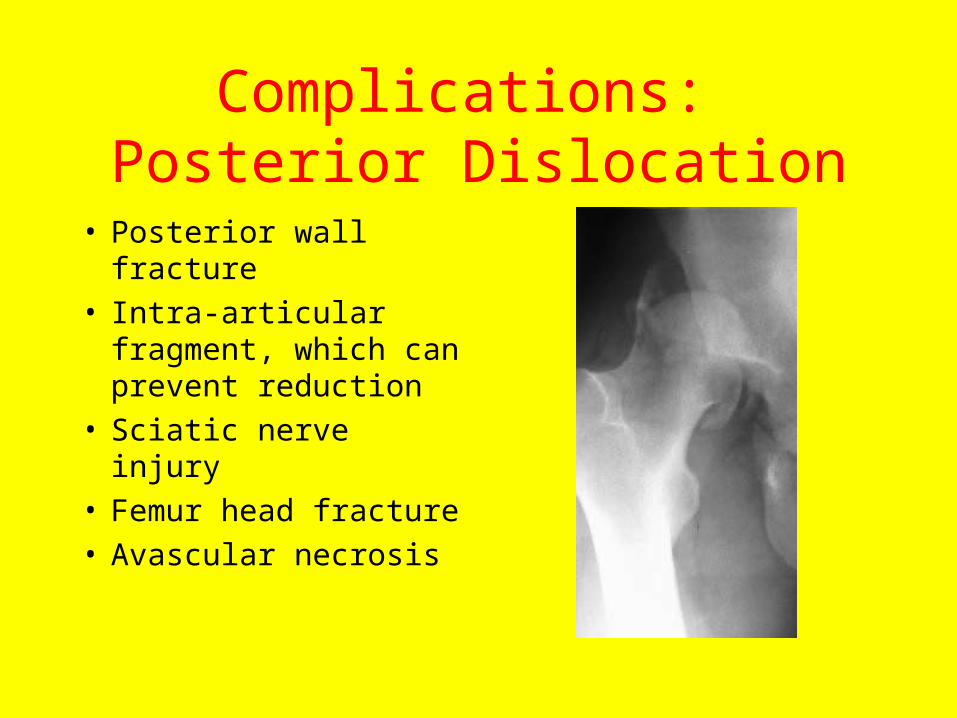
Complications: Posterior Dislocation
• Posterior wall fracture• Intra-articular
fragment, which can prevent reduction
• Sciatic nerve injury• Femur head fracture• Avascular necrosis
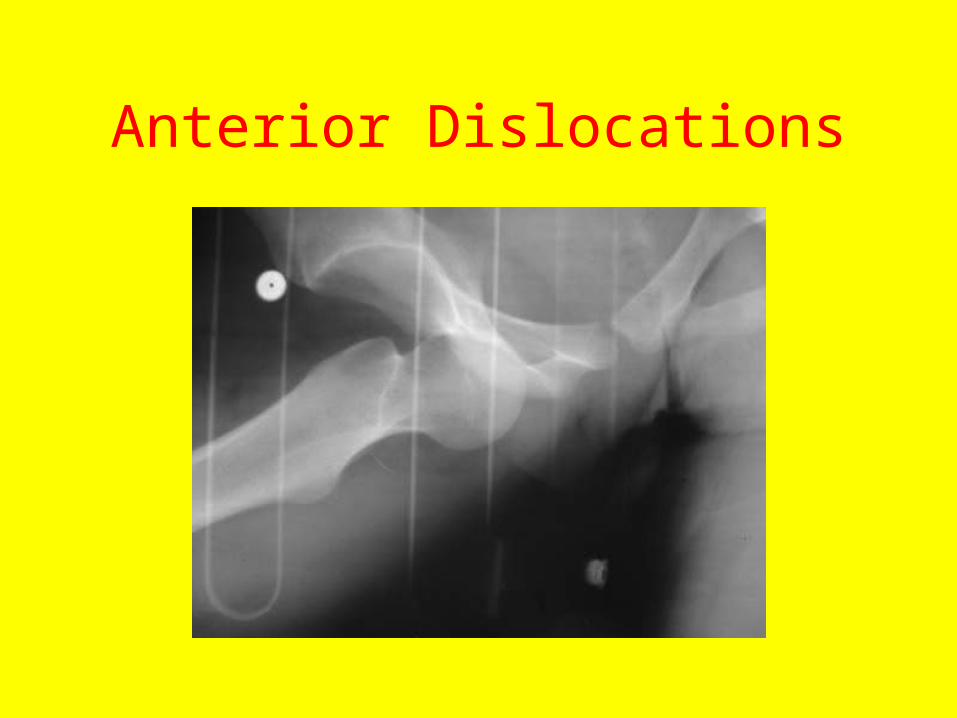
Anterior Dislocations
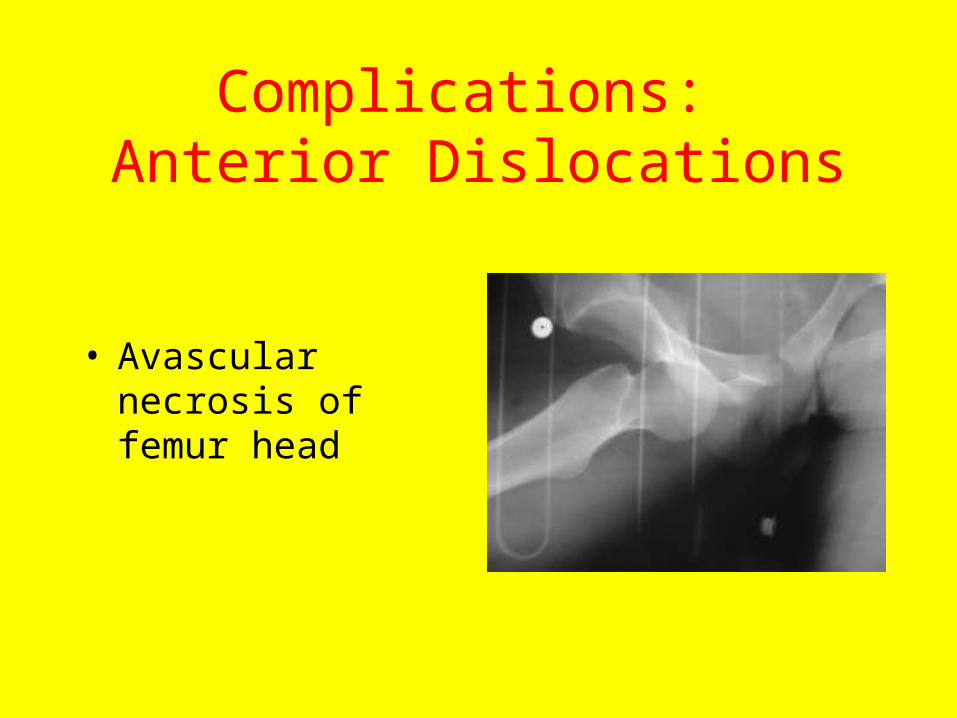
Complications: Anterior Dislocations
• Avascular necrosis of femur head
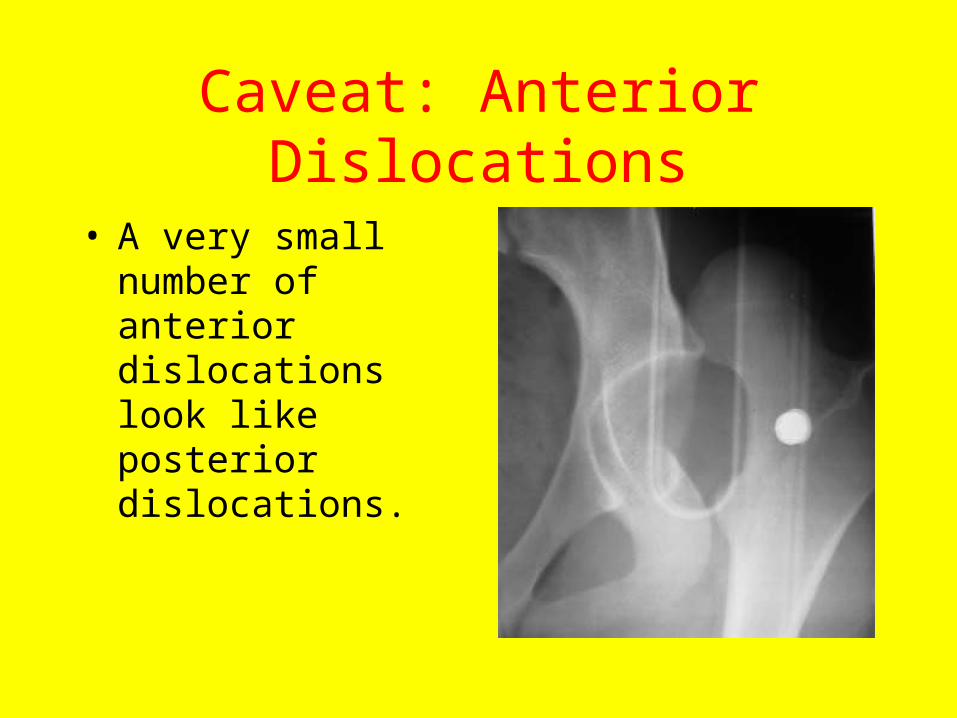
Caveat: Anterior Dislocations
• A very small number of anterior dislocations look like posterior dislocations.
And now….
• The PROXIMAL FEMUR
• Also called the “HIP”
The Proximal FEMUR
Often called the “Hip” it includes the :
• Head of femur
• Neck of femur
• Intertrochanteric femur
• Greater and lesser trochanters
• Subtrochanteric femur shaft
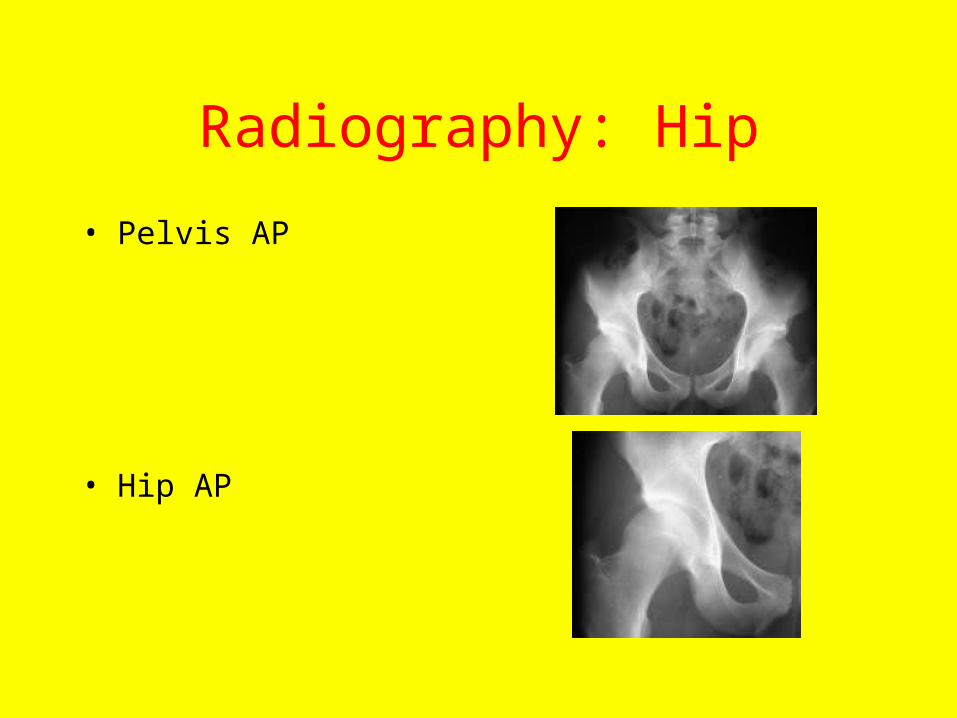
Radiography: Hip
• Pelvis AP
• Hip AP
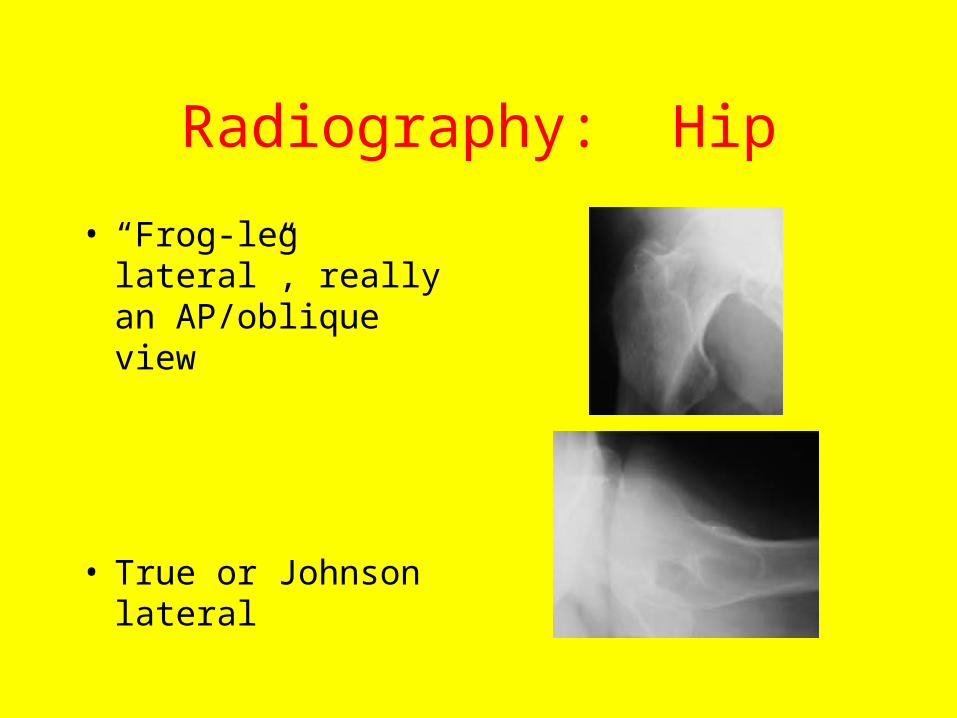
Radiography: Hip
• “Frog-leg lateral”, really an AP/oblique view
• True or Johnson lateral
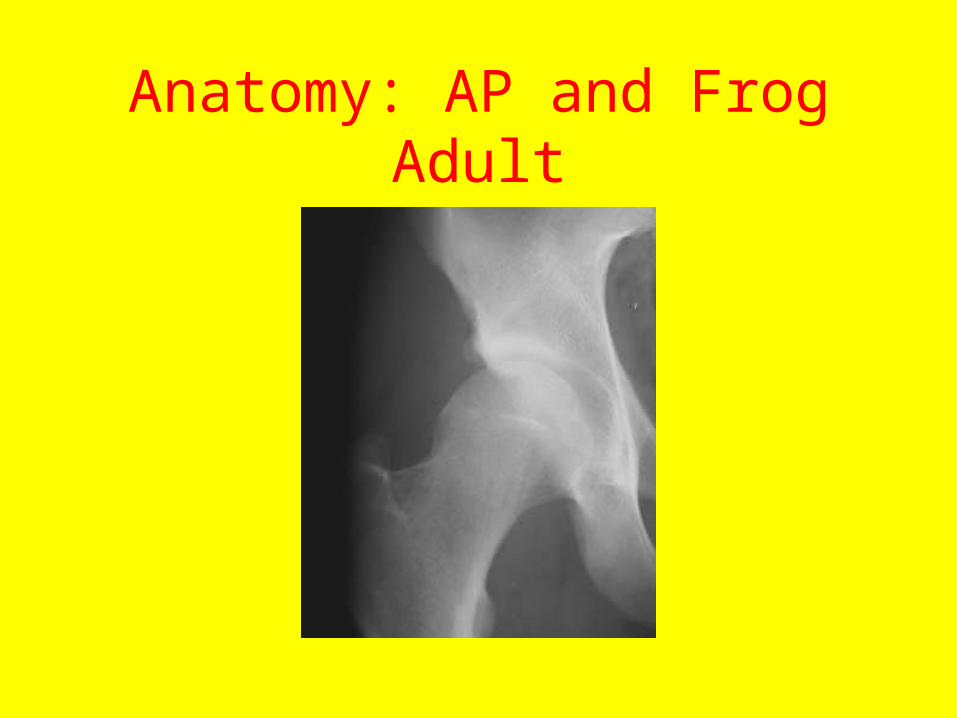
Anatomy: AP and Frog Adult
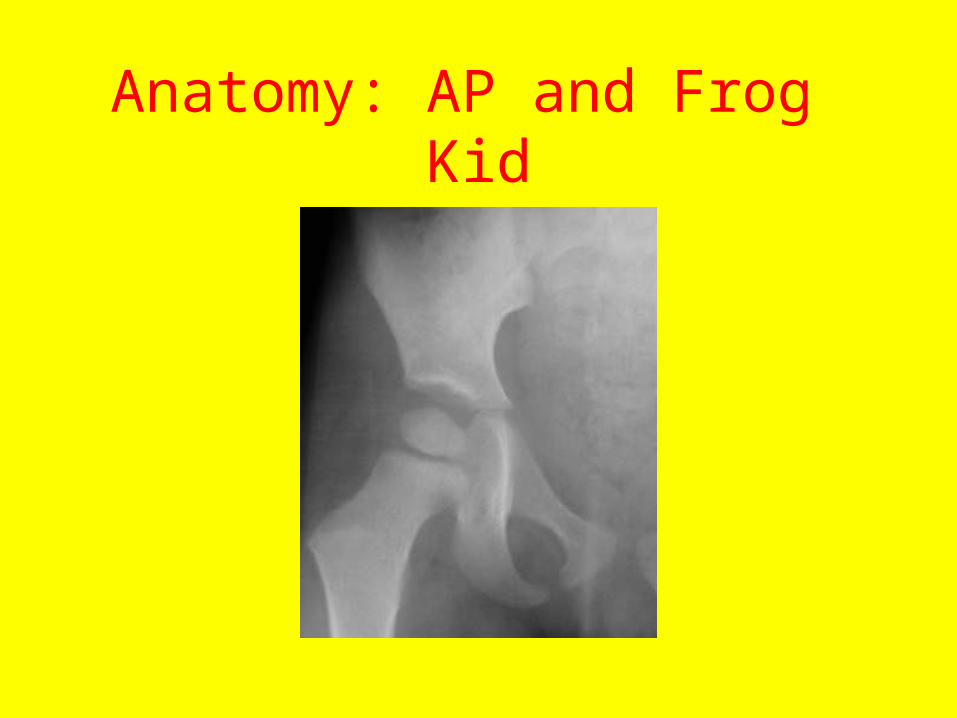
Anatomy: AP and Frog Kid
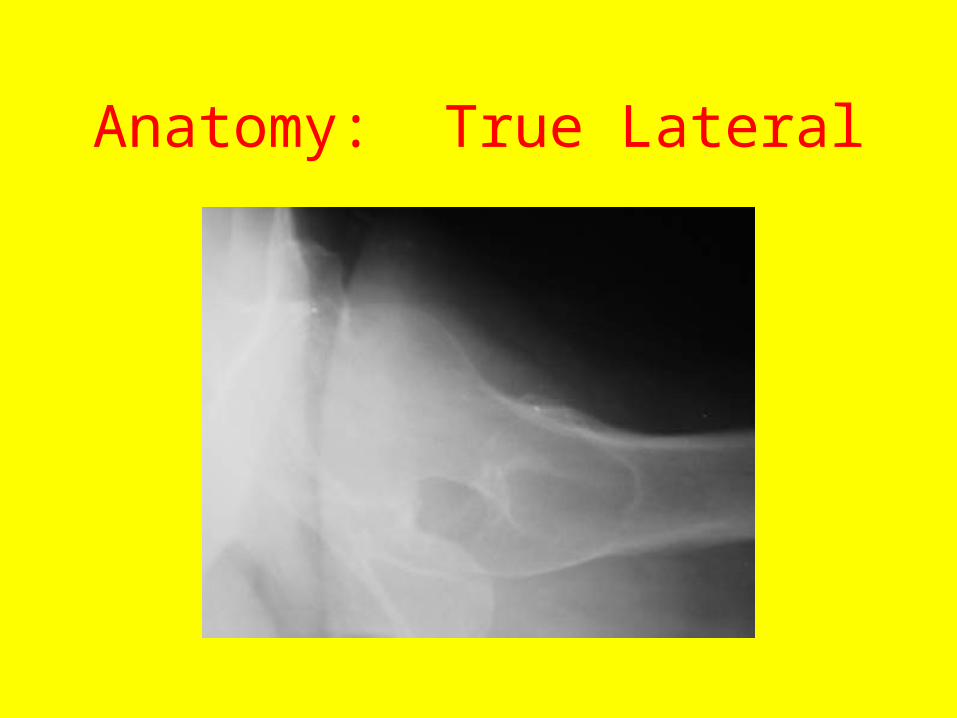
Anatomy: True Lateral
Role of MRI, CT and Bone Scan
• CT: Not much of a role, as not sensitive enough for subtle fractures in axial projection, and reformats not good enough, but improving with MDCT.
• MRI: BIG role! We will discuss it later.
• Bone scan: Obsolete. Too many early false negatives in osteoporotic patients.
Hip Fractures
• Head: A complication of acetabulum fractures or dislocations
• NECK• INTERTROCHANTERIC• Isolated greater or lesser trochanter• Subtrochanter shaft
Hip Fractures
• Femur neck and intertrochanteric fractures occur mainly in elderly people with osteoporosis who sustain a ground level fall.
• They can occur in normal people with major force.
• Femur neck stress fractures are also occasionally seen in athletic people.
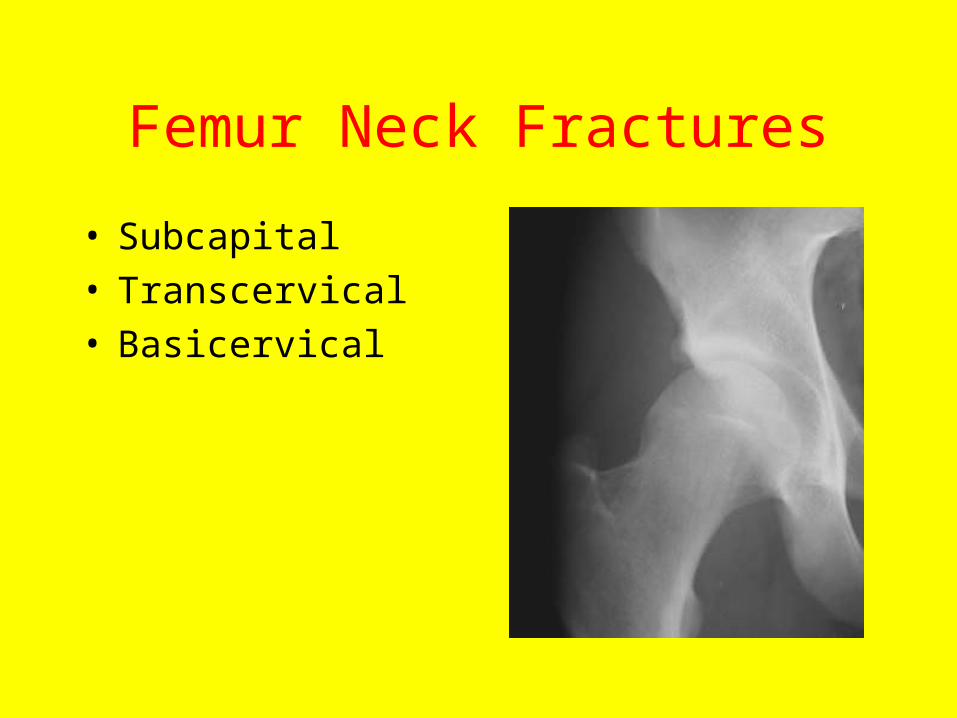
Femur Neck Fractures
• Subcapital• Transcervical• Basicervical
Classification: Femur Neck Fractures
GARDEN:
• I: Impacted or incomplete
• II: Complete, but nondisplaced
• III: Partially displaced
• IV: Completely displaced
Femur Neck Fractures: Management
• Garden I and II’s don’t disrupt blood supply to femur head, so need only mechanical stabilization.
• Garden III and IV’s disrupt blood supply in 30%-50%.
Femur Neck Fractures: Management
• Garden III and IV’s in an elderly or chronically ill patient: Hemiarthroplasty. You don’t want to operate again on these patients if AVN occurs.
• But in a younger healthy patient, might try pinning and do hemiathroplasty later if AVN occurs, because hip prostheses need replacement every 10-12 years.
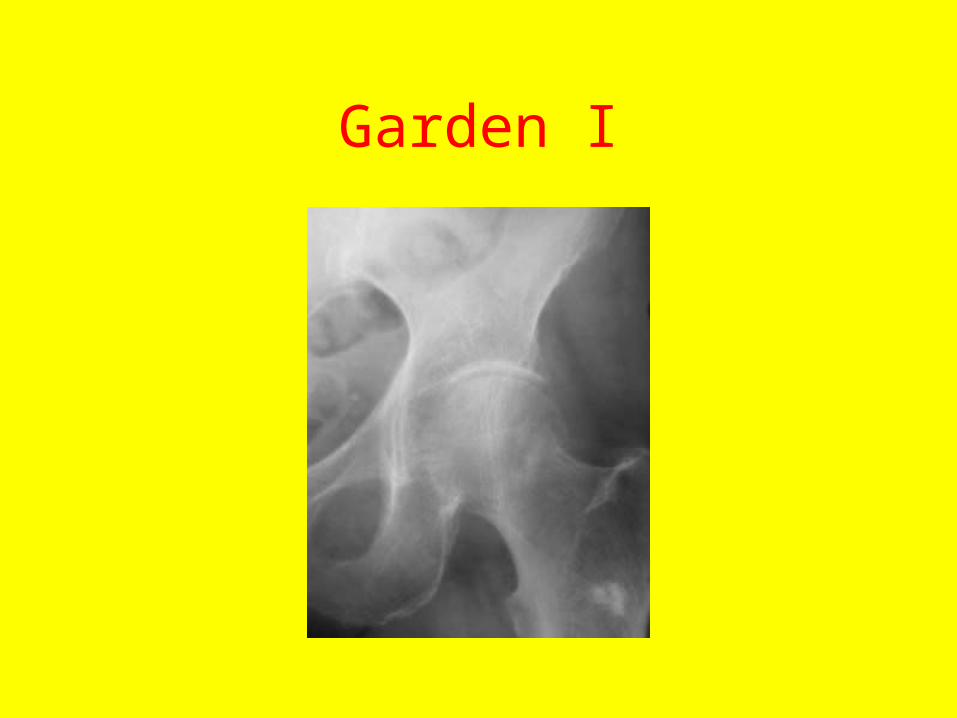
Garden I

Garden II

Garden III

Garden IV

Less common mechanisms
• Stress fracture, marathon runner.

Treatment, Garden I-II: Pins

Treatment, Garden III-IV: Hemiarthroplasty
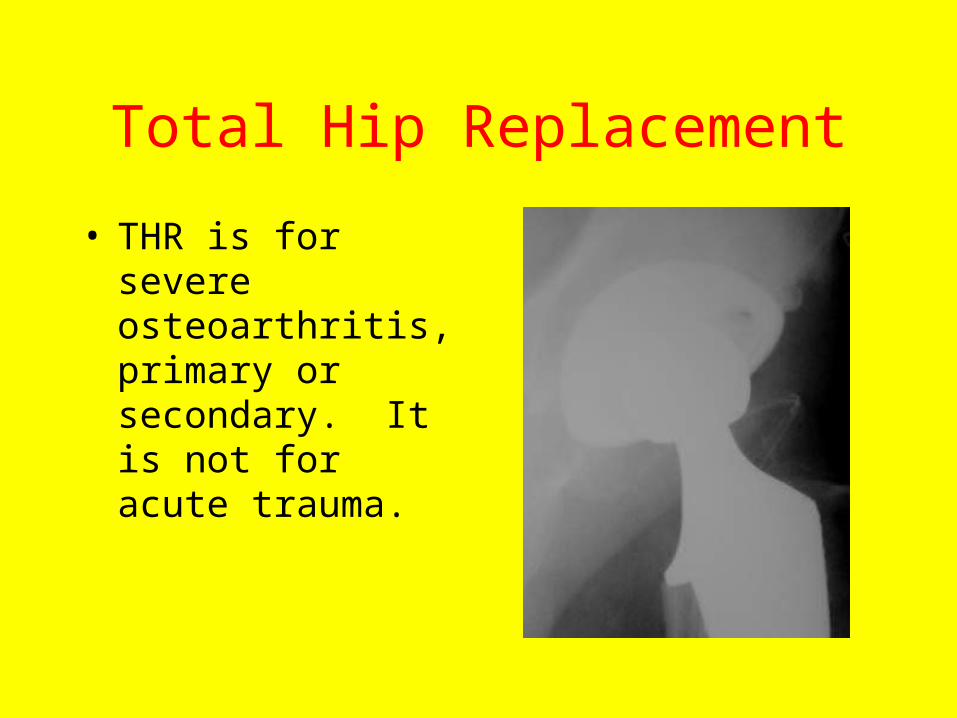
Total Hip Replacement
• THR is for severe osteoarthritis, primary or secondary. It is not for acute trauma.
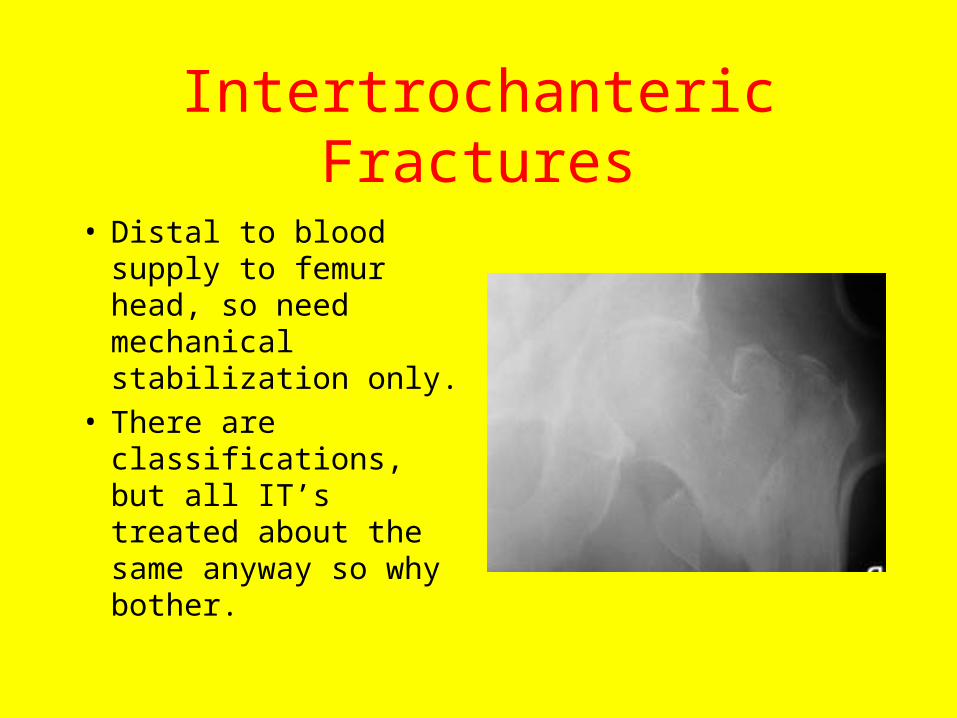
Intertrochanteric Fractures
• Distal to blood supply to femur head, so need mechanical stabilization only.
• There are classifications, but all IT’s treated about the same anyway so why bother.
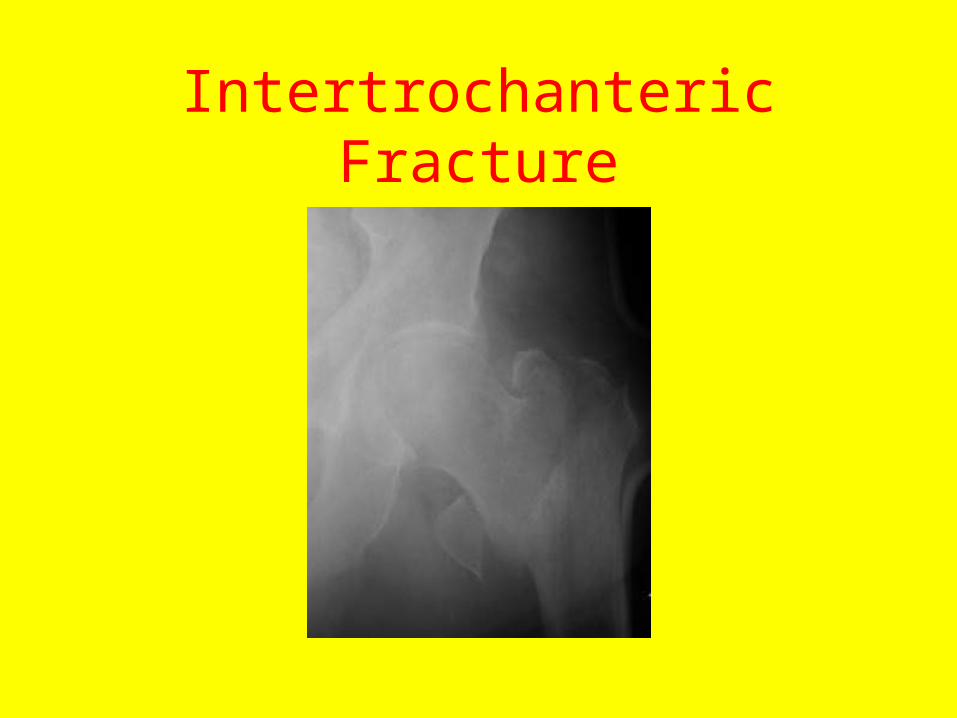
Intertrochanteric Fracture

Treatment: Dynamic Compression Screw
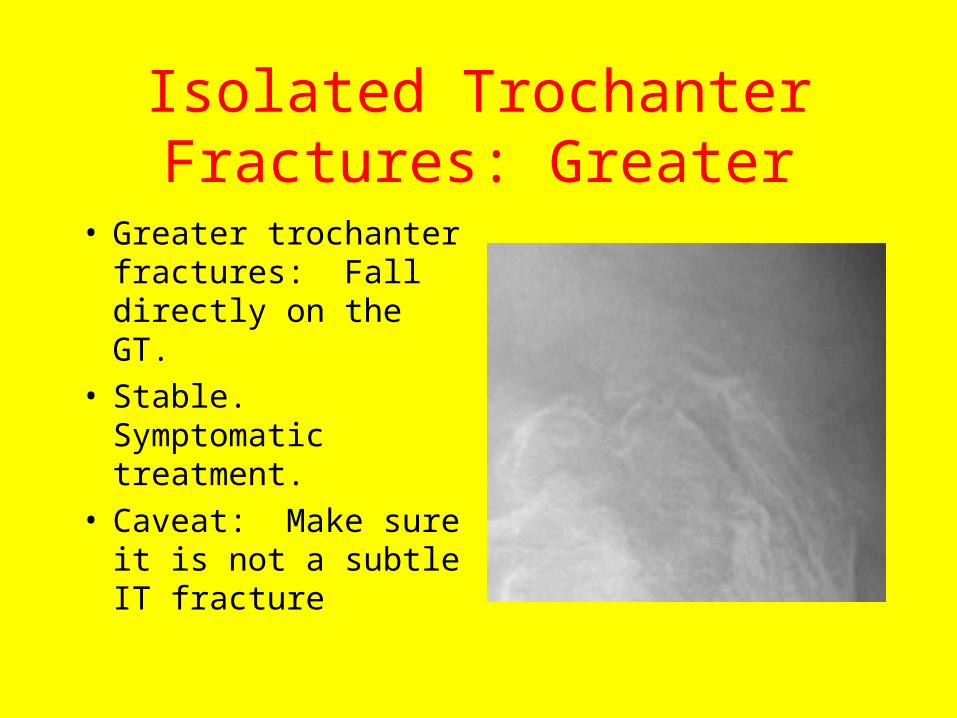
Isolated Trochanter Fractures: Greater
• Greater trochanter fractures: Fall directly on the GT.
• Stable. Symptomatic treatment.
• Caveat: Make sure it is not a subtle IT fracture
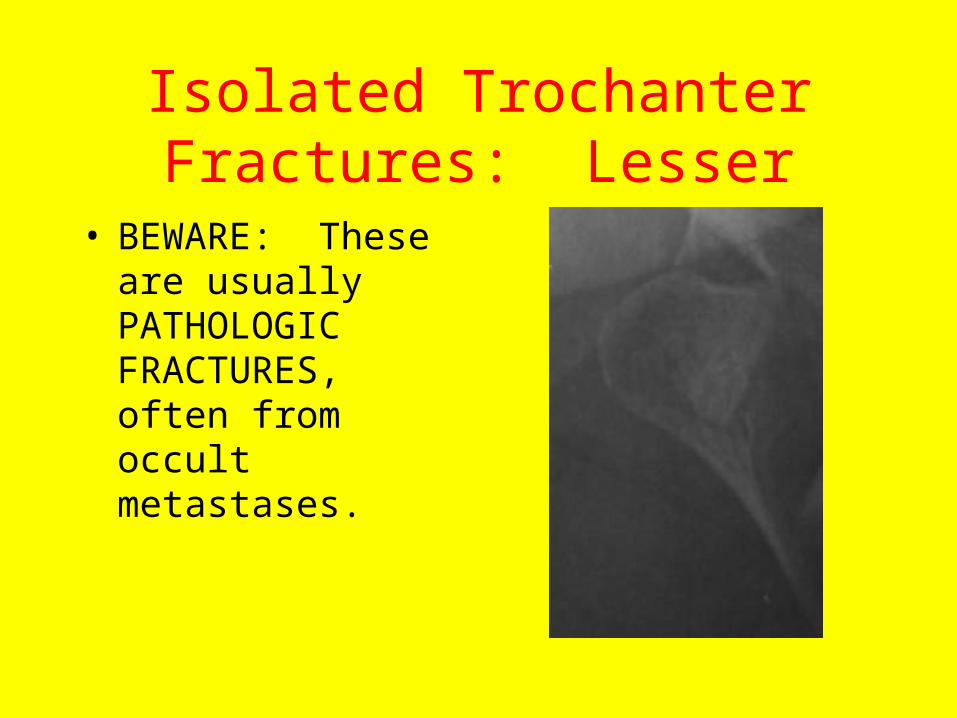
Isolated Trochanter Fractures: Lesser
• BEWARE: These are usually PATHOLOGIC FRACTURES, often from occult metastases.
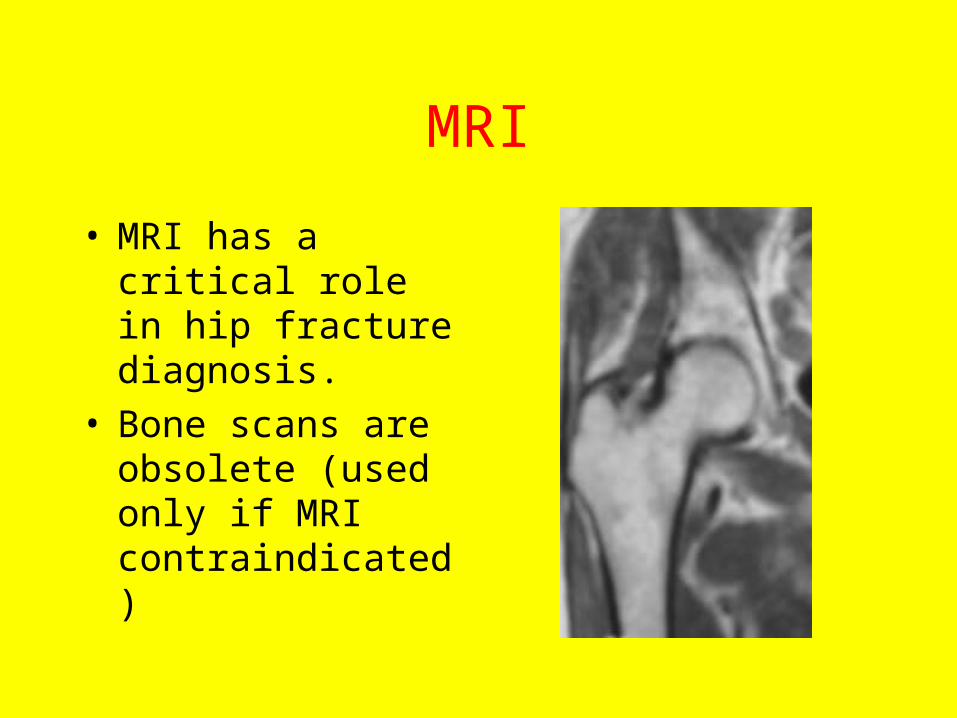
MRI
• MRI has a critical role in hip fracture diagnosis.
• Bone scans are obsolete (used only if MRI contraindicated)
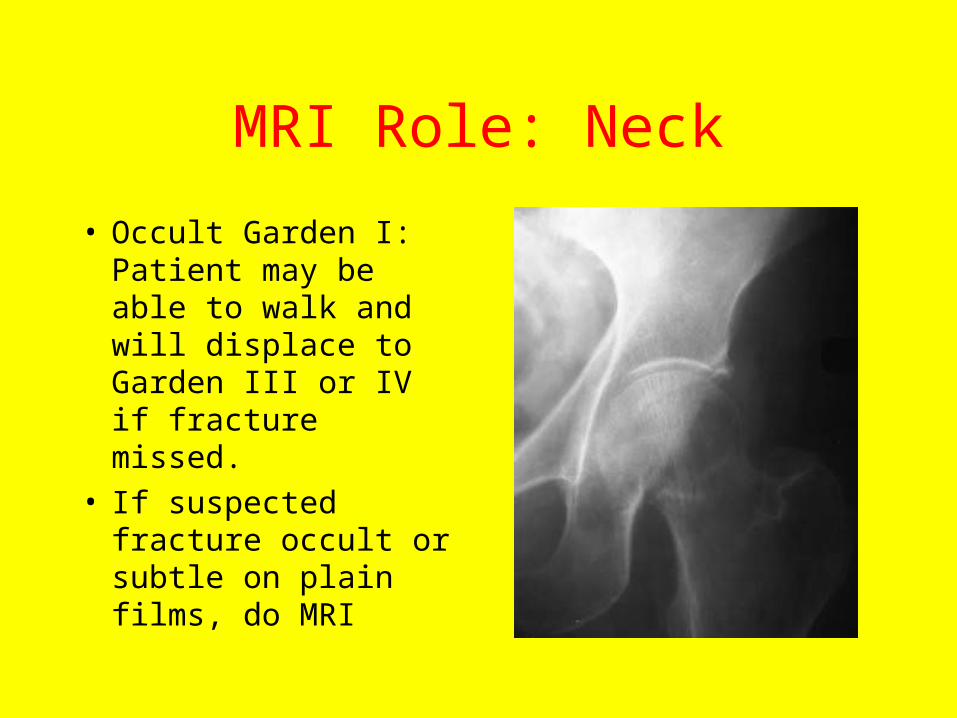
MRI Role: Neck
• Occult Garden I: Patient may be able to walk and will displace to Garden III or IV if fracture missed.
• If suspected fracture occult or subtle on plain films, do MRI
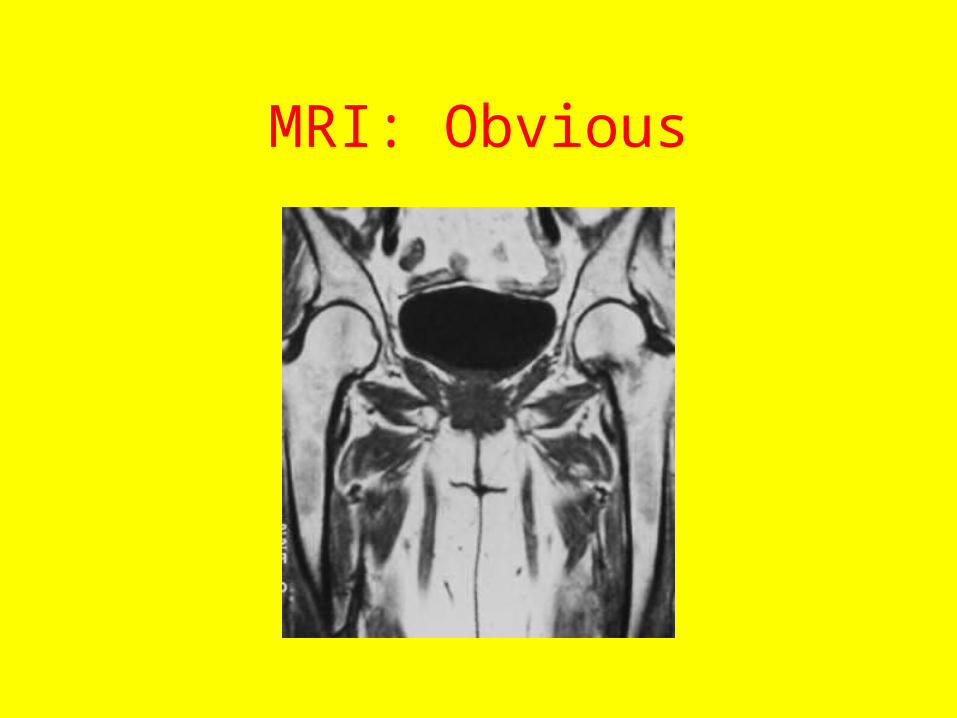
MRI: Obvious
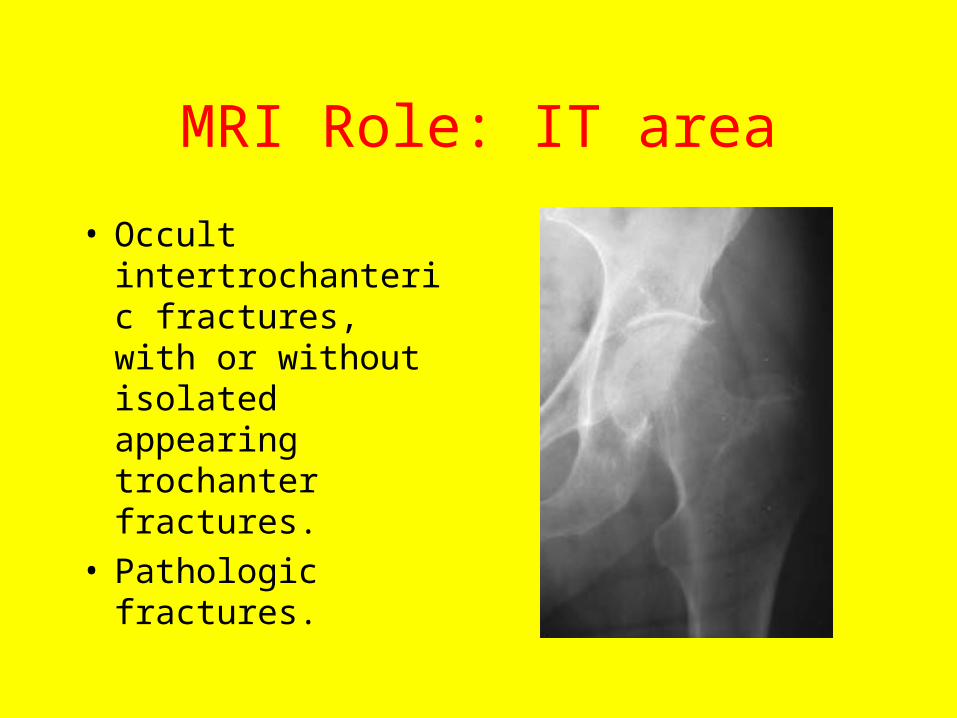
MRI Role: IT area
• Occult intertrochanteric fractures, with or without isolated appearing trochanter fractures.
• Pathologic fractures.

MRI: Obvious IT Fracture
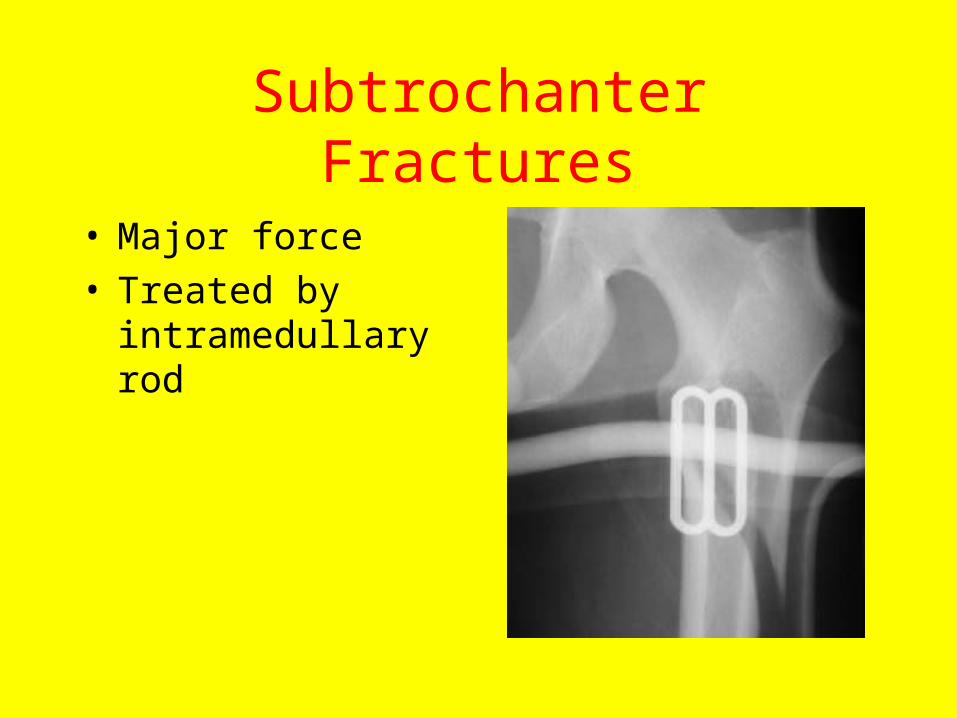
Subtrochanter Fractures
• Major force• Treated by
intramedullary rod

GOODBYE
• Copyright 2004
MI Zucker