the aids institute the impact of essential health benefits on people living with hiv/aids carl...
TRANSCRIPT
The AIDS Institute
The Impact of Essential Health Benefits
on People Living with HIV/AIDS
Carl SchmidDeputy Executive Director
ADAP Advocacy Association Annual ConferenceWashington DC
July 8, 2013
The AIDS Institute
Outline
• Essential Health Benefits• Overview• Private plans• Expanded Medicaid• Current Status• Implementation
The AIDS Institute
• Established by ACA as core services health plans required to cover beginning 2014
• Applies to: • Plans in the individual and small group
markets (inside and outside the Exchanges/Marketplaces)• “grandfathered” plans exempt
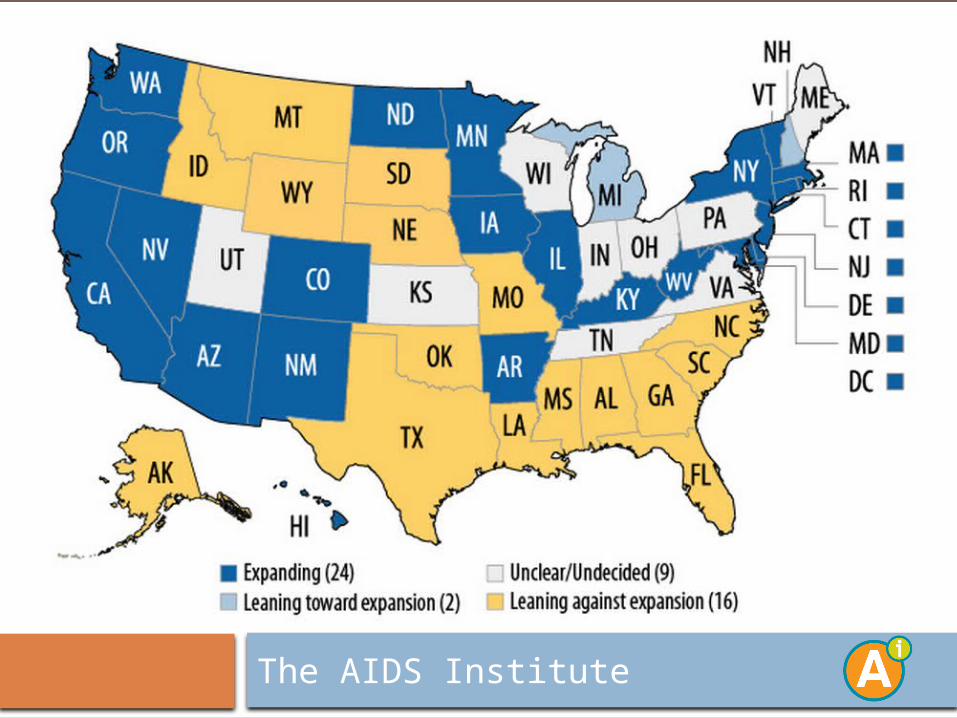
• Medicaid Expansion plans (Alternative Benefit Plans)
• Basic Health Plans• Estimated to impact 68 million people
Essential Health Benefits
The AIDS Institute
Essentials Health Benefits (EHB)Law outlines 10 broad categories of services that
must be covered, leaves to Secretary of HHS to define:
• Ambulatory patient services
• Emergency services • Hospitalization • Maternity and newborn
care • Mental health and
substance use• Prescription drugs
• Rehabilitative and habilitative services
• Laboratory services • Preventive/wellness
services; chronic disease management
• Pediatric services, including oral and vision care
The AIDS Institute
• CCIIO released bulletin outlining approach for defining EHB
(December 2011)• We expected Secretary to explicitly define the 10
categories• Instead, a benchmark approach
• States chose benchmark from:• 3 largest small group plans in the state• 3 largest state employee plans in the state• 3 largest federal employee plans• Largest HMO in the state’s commercial
market• Default: Largest small group plan in the
state
EHB & the Private Market
The AIDS Institute
• Drug benefit: • Only one drug in each class covered by
benchmark• Would be unworkable for certain conditions,
such as HIV that require a full formulary• Strong patient community opposition
• Concerns with:• Benchmark approach• Drug benefit
EHB & the Private Market
The AIDS Institute
• Released February 2013• Maintains commitment to benchmark approach• Moves away from one drug per class:
• Proposes the greater of: • 1) One drug per US Pharmacopeia (USP)
category & class; or • 2) Same number of drugs in each category &
class as benchmark• Much better than initial proposal
EHB Final Rule: Private Plans
The AIDS Institute
The AIDS Institute
• Plans in a significant majority of states will have to cover all medicines in two of the HIV/AIDS classes
• Plans in 48 states (including DC) will be required to cover all Protease Inhibitors
• Plans in 7 states would be permitted to cover fewer than 75% of therapies in the class of “other ARVs” (or antiretrovirals with different mechanisms of action that are currently not classified based on the USP classification system).
• ARV coverage in NM and WI especially concerning, other states with poor hepatitis drug coverage
EHB Final Rule: Private Plans
The AIDS Institute
• FL selected its largest small group product• Blue Cross and Blue Shield of Florida (PPO):
BlueOptions 5462
• Benchmark antiretroviral and hepatitis drug coverage by class (out of all FDA approved): • Total HIV/AIDS Drugs (28/35)
• Non-nucleoside Reverse Transcriptase Inhibitors (5/6)
• Nucleoside & Nucleotide Reverse Transcriptase Inhibitors (11/12)
• Protease Inhibitors (9/11)• Anti-HIV Agents, Other (3/6)
• Anti-hepatitis Agents (12)
State Example: Florida
The AIDS Institute
• Did not address what to do with new drugs coming to market during plan year
• Concerns about using USP system to classify drugs:
• Updated only every 3 years• Combination products not recognized• Very broad
• Requires that plans have procedures to allow access to clinically appropriate drugs not covered by the health plan• But no guidance on specific requirements
• Contains language allowing insurers to “appropriately utilizing reasonable medical management technique(s)”
Problems with EHB: Private Plans
The AIDS Institute
• Proposed Rule - January 2013• Utilizes benchmark process • Must contain all 10 benefit categories• Applies to all enrolled through Medicaid
Expansion• States permitted to adopt separate benchmarks
for special populations• “Medically frail” can enroll in traditional Medicaid
Medicaid
The AIDS Institute
EHB Proposed Rule: Medicaid
The AIDS Institute
• Two step process: • State selects alternative benefit plan (ABP)
from existing Medicaid benchmark:• Standard FEHBP BCBS • State employee plan• Largest commercial HMO plan in the state• A Secretary approved plan (including
traditional Medicaid)• If ABP not a EHB option in private market, state
selects a private EHB to backfill benefits missing from benchmark
EHB Proposed Rule: Medicaid
The AIDS Institute
• Drug benefit• Must cover all drugs made by companies
participating in Medicaid drug rebate program• States may incentivize use of generics and
adopt utilization management techniques, including quantity limits
• Allows differential cost-sharing for preferred vs. non drugs • Proposed co-pays: $8 for each non-preferred
drug/$4 preferred• Can deter usage/adherence
EHB Proposed Rule: Medicaid
The AIDS Institute
• Waiting on Medicaid EHB final rule• Coverage begins January 1• Do not know what benchmark states will use
• CMS and states reviewing adequacy of private plans• Will not know what drugs covered until
October 1• Will see an uneven coverage from state to state• Patient costs also unknown
Current Status
The AIDS Institute
• Enrollment for private plans begins October 1• Beneficiary should review plan for
• Drug adequacy and costs• Use of quantity limits, tiers, prior authorizations,
etc.
• Appeals process for medical necessity purposes• If not working for patients with HIV/AIDS can
appeal to CMS to change process or legislation• CMS committed to this process for first two years
• HIV/AIDS Community needs to monitor• Ryan White Program can provide coverage
completion services
Implementation
The AIDS Institute
ResourcesRules and Guidance• EHB Final Rule (Private Plans):
http://www.gpo.gov/fdsys/pkg/FR-2013-02-25/pdf/2013-04084.pdf• EHB Proposed rule (Medicaid):
https://www.federalregister.gov/articles/2013/01/22/2013-00659/medicaid-childrens-health-insurance-programs-and-exchanges-essential-health-benefits-in-alternative
Essential Health Benefits Coalition Responses to Rulemaking:• Proposed Rule (Private Plans):
http://www.theaidsinstitute.org/sites/default/files/attachments/coalition%20comments%20on%20nprm%20ehb%20FINAL.pdf
• Proposed Rule (Medicaid):http://www.theaidsinstitute.org/sites/default/files/attachments/coalition%20comments%20on%20nprm%20ehb%20medicaid%20FINAL.pdf
Other• State benchmark EHB coverage summaries (incl. drug):
http://www.cms.gov/CCIIO/Resources/Data-Resources/ehb.html• Where states stand with benchmark selection:
http://kff.org/health-reform/state-indicator/ehb-benchmark-plans/
