the ards cognitive outcomes study (acos): … · for review only ards cognitive outcomes study...
TRANSCRIPT

For Review O
nly
THE ARDS COGNITIVE OUTCOMES STUDY (ACOS): LONG-
TERM NEUROPSYCHOLOGICAL FUNCTION IN ACUTE LUNG
INJURY
SURVIVORS
Journal: American Journal of Respiratory and Critical Care Medicine
Manuscript ID: Blue-201111-2025OC.R4
Manuscript Type: OC - Original Contribution
Date Submitted by the Author: 22-Mar-2012
Complete List of Authors: Mikkelsen, Mark; Hospital of the University of Pennsylvania, Pulmonary, Allergy, and Critical Care Division Christie, Jason; University of Pennsylvania, Pulmonary, Allergy, and Critical Care Division; University of Pennsylvania, Center for Clinical Epidemiology and Biostatistics Lanken, Paul; University of Pennsylvania, Pulmonary, Allergy, and Critical Care Division Biester, Rosette; University of Pennsylvania School of Medicine, Center for
Brain Injury and Repair Thompson, B; Massachusetts General Hospital, Department of Medicine, Pulmonary and Critical Care Unit Bellamy, Scarlett; University of Pennsylvania, Center for Clinical Epidemiology and Biostatistics Localio, A.; University of Pennsylvania, Center for Clinical Epidemiology and Biostatistics Demissie, Ejigayehu; University of Pennsylvania, Pulmonary, Allergy, and Critical Care Division; University of Pennsylvania, Center for Clinical Epidemiology and Biostatistics Hopkins, Ramona; Brigham Young University, Psychology Department and Neuroscience Center
Angus, Derek; University of Pittsburgh, Department of Critical Care Medicine
Keywords: acute respiratory distress syndrome, ARDS, cognitive function, critical illness
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 1
TITLE: THE ARDS COGNITIVE OUTCOMES STUDY (ACOS): LONG-TERM
NEUROPSYCHOLOGICAL FUNCTION IN ACUTE LUNG INJURY
SURVIVORS
Authors:
Mark E. Mikkelsen, M.D., M.S.1,2 *
Jason D. Christie, M.D., M.S.1,2 * Paul N. Lanken, M.D.1
Rosette C. Biester, Ph.D3
B. Taylor Thompson, M.D.4
Scarlett L. Bellamy, Sc.D.2
A. Russell Localio, Ph.D.2
Ejigayehu Demissie, M.S.N.1,2
Ramona O. Hopkins, Ph.D. 5, 6 Derek C. Angus, M.D., M.P.H. 7
* These authors contributed equally to this work
Institution: 1Pulmonary, Allergy, and Critical Care Division
Department of Medicine University of Pennsylvania School of Medicine
2Center for Clinical Epidemiology and Biostatistics University of Pennsylvania School of Medicine
3Department of Physical Medicine and Rehabilitation University of Pennsylvania School of Medicine Philadelphia Veterans Affairs Medical Center
4Pulmonary and Critical Care Unit, Department of Medicine Massachusetts General Hospital 5Department of Medicine, Pulmonary and Critical Care Division, Intermountain Medical Center 6 Psychology Department and Neuroscience Center, Brigham Young University 7CRISMA Center, Department of Critical Care Medicine and Department of Health Policy and Management University of Pittsburgh
Contributions Conception and Design: Angus, Biester, Christie, Hopkins, Lanken, Thompson Data Collection: Angus, Christie, Demissie, Hopkins, Lanken, Mikkelsen, Thompson
Page 1 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 2
Analysis and Interpretation of the Data: Angus, Bellamy, Biester, Christie, Hopkins, Localio, Mikkelsen, Thompson Drafting of the manuscript: Angus, Bellamy, Biester, Christie, Demissie, Hopkins, Lanken, Localio, Mikkelsen, Thompson Critical revision of the article for important intellectual content: Angus, Christie, Hopkins, Mikkelsen, Thompson Corresponding author: Mark E. Mikkelsen, M.D., M.S.C.E. Pulmonary, Allergy, and Critical Care Division Perelman School of Medicine, University of Pennsylvania 836 W. Gates Pavilion 3400 Spruce Street Philadelphia, PA 19104 e-mail: [email protected] Phone: (215) 615-5416 Abstract Word Count: 248 Body Text Word Count: 3500 This article has an online data supplement, which is accessible from this issue’s table of content online at www.atsjournals.org Funding: The study was supported in part by N01-HR-46058, N01-HR-46046-64, N01-HR-16146-54, and T32 HL07891 training grant, National Institutes of Health, National Heart, Lung and Blood Institute, Bethesda, MD. Disclosures: For each of the above authors, no financial or other potential conflicts of interest exist. Presented in part at the American Thoracic Society International Conference, May 2008, Toronto, Canada. Running Head: ARDS COGNITIVE OUTCOMES STUDY (ACOS) Descriptor: 4.2 ALI/ARDS: Diagnosis & Clinical Issues At a Glance Commentary: Scientific Knowledge on the Subject
Cognitive and psychiatric morbidities are prevalent, long-lasting, and potentially modifiable in survivors of critical illness. Whether neuropsychological function can be assessed in a multi-center trial is unknown. Furthermore, the frequency and risk factors for long-term neuropsychological impairment in ALI survivors have not been studied in a multi-center trial.
What This Study Adds to the Field
Page 2 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 3
We found that neuropsychological function in survivors from a multi-center
trial could be assessed using a validated telephone battery. Our findings demonstrated that a majority of ALI survivors experienced long-term cognitive and psychiatric morbidity, and we detected that hypoxemia is a risk factor for the development of long-term cognitive and psychiatric impairment.
Page 3 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 4
ABSTRACT
Rationale: Cognitive and psychiatric morbidity is common and potentially
modifiable following acute lung injury (ALI). However, practical measures of
neuropsychological function for use in multi-center trials are lacking.
Objectives: To determine whether a validated telephone-based
neuropsychological test battery is feasible in a multi-center trial. To determine the
frequency and risk factors for long-term neuropsychological impairment.
Methods: As an adjunct study to the ARDSNet Fluid and Catheter Treatment
Trial, we assessed neuropsychological function at 2 and 12 months post-hospital
discharge.
Measurements and Main Results: Of 406 eligible survivors, we approached
261 to participate and 213 consented. We tested 122 subjects at least once,
including 102 subjects at 12 months. Memory, verbal fluency and executive
function were impaired in 13% (12/92), 16% (15/96), and 49% (37/76) of long-
term survivors. Long-term cognitive impairment was present in 41 of the 75
(55%) survivors who completed cognitive testing. Depression, post-traumatic
stress disorder, or anxiety was present in 36% (37/102), 39% (40/102), and 62%
(63/102) of long-term survivors. Enrollment in a conservative fluid-management
strategy (p=0.005) was associated with cognitive impairment and lower partial
pressure of arterial oxygen during the trial was associated with cognitive (p=0.02)
and psychiatric impairment (p=0.02).
Conclusions: Neuropsychological function can be assessed by telephone in a
multi-center trial. Long-term neuropsychological impairment is common in ALI
Page 4 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 5
survivors. Hypoxemia is a risk factor for long-term neuropsychological
impairment. Fluid management strategy is a potential risk factor for long-term
cognitive impairment; however, given the select population studied and an
unclear mechanism, this finding requires confirmation.
Key words: acute respiratory distress syndrome; ARDS; cognitive function;
critical illness
Page 5 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 6
In the United States, 200,000 patients will develop acute lung injury (ALI)
each year (1). Advances in ALI management have decreased mortality to 25-
40% (1-4), resulting in an expanding population of survivors who have been
ravaged by their acute illness. Survivorship, it has been put forth, will be the
defining challenge of modern day critical care (5). Beyond the physical ailments
that survivors endure, neuropsychological impairment is increasingly recognized
as a prevalent, important, and potentially modifiable outcome among ALI
survivors (6-21) and critical illness in general (22-29).
Traditionally, neuropsychological (cognitive and psychiatric) function is
assessed in-person by an expert - a constraint that has limited the ability to study
the frequency and determinants of neuropsychological impairment in critically ill
populations and to measure the effects of an intervention on long-term
neuropsychological function. Neuropsychological function has not been studied
in survivors from a multi-center trial. Consequently, the generalizability of
observations from single center cohort studies is unknown. Furthermore,
evidence regarding the etiology of neuropsychological impairment in ALI
survivors is extremely limited.
As a practical approach to assess the neuropsychological function of
survivors from a multi-center trial, we developed a telephone battery of
standardized neuropsychological tests which could be administered by a non-
expert (10). We then validated the telephone battery against standard in-person
assessments (10, 30) and in ALI survivors specifically (10-11). Here, we
administered the battery to a subset of survivors from the Acute Respiratory
Page 6 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 7
Distress Syndrome Clinical Trials Network (ARDSNet) Fluid and Catheter
Treatment Trial (FACTT) (4, 31). FACTT tested the hypothesis that a
conservative fluid-management strategy targeted to lower intravascular
pressures as measured by either a pulmonary artery catheter (PAC) or central
venous catheter improves outcomes in ALI. Our goals were to determine whether
a telephone-based neuropsychological test battery was feasible in a multi-center
trial, to determine the frequency of long-term neuropsychological morbidity in
survivors from a multi-center trial, and to identify potential risk factors for the
development of long-term cognitive and psychiatric impairment. Results of this
study were previously reported in abstract form (32).
Materials and Methods
An expanded methods section is available in an online supplement. The
study was approved by the institutional review board of participating hospitals
and as a substudy of FACTT by the ARDSNet.
Study Design
The ARDS Cognitive Outcomes Study (ACOS) is a prospective, multi-
center cohort study of a subset of survivors from FACTT. FACTT enrolled
patients between June 2000 and October 2005. Between July 2002 and July
2003, FACTT was halted and new regulatory approval related to the study was
prohibited. The regulatory process for ACOS began prior to the halt and testing
was conducted between March 2003 and September 2006 in concert with the
Page 7 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 8
Economic Analysis of the Pulmonary-Artery Catheter (EA-PAC) study, a long-
term follow-up study of FACTT (33).
To be eligible for ACOS, subjects had to be enrolled in FACTT and EA-
PAC (33) and ACOS-specific regulatory approval had to be in place. FACTT
enrolled mechanically ventilated adult ALI patients (34). Subjects not consented
prior to discharge for ACOS were recruited via the telephone and through written
communication when telephone contact failed.
Neuropsychological Function and Quality of Life
We used a validated telephone battery of standardized
neuropsychological tests (10-11, 30). The telephone battery was administered
from the University of Pittsburgh to consenting, English-speaking subjects at 2
and 12 months post-hospital discharge. Subjects were not required to undergo 2
month testing to be tested at 12 months.
The instruments used to assess cognition, anxiety, depression, and post-
traumatic stress disorder (PTSD) symptoms are presented in Table E1 (35-42).
Quality of life (43) was assessed at 12 months as part of EA-PAC (33). We
focused our study on survivors tested at 12 months to assess long-term
neuropsychological function.
Data Analysis
The cognitive battery yielded scaled scores for each domain which were
normalized to allow for comparisons across tests and subjects (44-45). We report
Page 8 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 9
the median and interquartile range of results as percentiles. We defined
impairment in a single domain as a score > 2 standard deviations below the
population normative data (6-7, 9, 44-46). Cognitive impairment at the subject
level was defined as impairment in memory, verbal fluency, and/or executive
function in subjects who completed tests in each of these domains (6, 9, 10-11,
27).
We a priori hypothesized that long-term cognitive impairment would be
associated with duration of mechanical ventilation, either conservative or liberal
fluid-management strategy (4), hypotension (9), hypoxemia (6), PAC use (19, 47-
48), sepsis as the cause of ALI (49-50), and severity of illness (26). The pre-
specified potential confounding variables (6-12, 51-53) are detailed in the
supplement.
Psychiatric impairment was defined as impairment in any of the three
psychiatric measures (anxiety, depression, and PTSD) in subjects completing
each measure. We tested the following candidate risk factors for the
development of long-term psychiatric morbidity: age (18, 27-28), gender (18, 27-
29), race/ethnicity, level of education (19, 27), APACHE III scores, trial
interventions (fluid-management strategy, PAC), hypotension, hypoxemia (18,
27), any episode of hypoglycemia (glucose < 60 mg/dL) during the hospitalization
(20, 27), corticosteroid administration (54), ICU length of stay (17, 21, 27), and
duration of mechanical ventilation (17-18, 27).
Statistical Analysis
Page 9 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 10
Multivariable logistic regression was used to investigate the relationship
between candidate risk factors and long-term neuropsychological (cognitive or
psychiatric) impairment. We adjusted for each candidate risk factor and potential
covariates with an alpha level of significance <0.20 in univariate analyses (55).
To avoid over-fitting, adjustment was performed one covariate at-a-time (56). A
p-value of ≤ 0.05 was used to signify statistical significance.
The cognitive impairment risk factor analysis was limited to 75 survivors
who completed memory, verbal fluency, and executive function testing at 12
months. The Hayling Sentence Completion Test (HSCT) assesses executive
function with an error score and response latency component to produce an
overall score (35-36). The HSCT response times were not measured before
February, 2005 due to an error in the administration of the timing of the test. The
timing error resulted in 21 survivors tested at 12 months having incomplete
testing. In secondary analyses, 90 survivors who completed assessments in
memory, verbal fluency, and the error score of the HSCT at 12 months were
carried out.
We tested for associations between identified risk factors and memory,
verbal fluency, and executive function scores as continuous variables using
Spearman rank-correlation coefficients. Finally, we performed sensitivity
analyses to determine the effects of missing data on the observed associations.
Statistical analyses were performed using Stata 10.0 software (Stata Datacorp,
College Station, TX).
Page 10 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 11
Results
Enrollment
Of 1001 patients randomized in FACTT, 406 survivors were eligible for
ACOS (Figure 1, Figure E1 for enrollment by fluid-management strategy). Of 406
eligible survivors, we approached 261 to participate and 213 consented. Consent
rates did not differ by age, gender, race/ethnicity, or geographic region after
adjusting for mortality and excluding ineligible subjects in whom the time window
to be tested had elapsed (Table E2). Of 213 consenting subjects, 14 died prior to
initial testing, and we were able to contact and test 122 of 199 alive and
consenting subjects (61%) at least once. The 122 subjects were drawn from 28
hospitals and constitute the ACOS cohort.
Compared to non-ACOS FACTT participants who survived 60-days
(N=609), the ACOS group was more likely to be female, more likely to be non-
Hispanic whites, less likely to have HIV/AIDS, and less likely to have pneumonia
as the cause of ALI (Table 1). The number of ACOS subjects enrolled from each
hospital ranged from 1 to 17 (median=3, interquartile range (IQR) 1-5).
By 12 months, 22 consenting subjects were deceased, 2 were
incarcerated, and 9 were deemed physically or mentally incapable of telephone-
based neuropsychological testing. Of the remaining 180 subjects who were alive
and able to be tested, 102 (57%) were tested at 12 months. These 102 long-term
survivors completed individual cognitive domain testing to various degrees (Table
E1), and 74% (75/102) completed testing in all cognitive domains. Long-term
survivors were tested on average 12 months post-hospital discharge (IQR 11 –
Page 11 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 12
13 months). None of these long-term survivors had a history of pre-existing
dementia.
Neuropsychological Test Battery Administration
The test battery required 45-60 minutes to complete. During the first
several tests, subject fatigue was noted to be significant when the battery was
administered during the same telephone call as the EAPAC questionnaire, which
required 15-20 minutes (33). Subsequently, the battery was administered during
a separate call. None of the initial tests were included in the primary analyses of
long-term cognitive impairment.
Using the separate testing session, survivors occasionally expressed
frustration and requested to end testing. Despite encouragement, explanation of
the reasons for the tests, and reassurance that the tests were meant to be
challenging, 8 long-term survivors declined to complete cognitive testing.
Baseline Characteristics and Effects of Fluid-Management Strategy
APACHE III score was higher (p=0.04) in the liberal-fluid strategy group
(Table E3). No other baseline characteristic differed between fluid-management
strategies. The ACOS patients in the conservative-strategy group received more
furosemide (p<0.001), resulting in a more negative seven-day cumulative fluid
balance (p=0.02), lower central venous pressures (p<0.001) and a trend towards
lower cardiac index (p=0.06) (Table E4). As in the larger FACTT study, in ACOS
the conservative fluid-management strategy resulted in shorter duration of
Page 12 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 13
mechanical ventilation (median difference of 2.5 days, p=0.04) and a trend to
shorter ICU stays (median difference of 3 ICU days, p=0.07).
Long-Term Cognitive Impairment and Psychiatric Morbidity
Cognitive function was below normal population mean scores in each
domain tested (Table E1). Cognitive impairment was observed in 41 of 75
survivors (55%) at 12 months. Using the error score of the HSCT to assess
executive function rather than the overall score, cognitive impairment was
observed in 54 of 90 survivors (60%).
Vocabulary and reasoning, domains hypothesized to be resilient to
acquired brain injury, were impaired in 3 of 98 survivors (3%). Among the
domains hypothesized to be susceptible to impairment following ALI, memory
was impaired in 12 of 92 (13%), verbal fluency in 15 of 96 (16%), and executive
function in 37 of 76 (49%) survivors at 12 months. Executive function was
impaired in 57 of 100 (57%) survivors when assessed using the error score of the
HSCT.
Symptoms of moderate or severe depression occurred in 37 of 102 (36%)
long-term survivors. PTSD screening was positive in 40 of 102 (39%) survivors.
Symptoms of moderate or severe anxiety occurred in 63 of 102 (62%) survivors.
Psychiatric symptoms were present in depression, anxiety, or PTSD in 67 of 102
(66%) survivors. Symptoms in two or more psychiatric domains occurred in 43 of
102 (42%) survivors. Cognitive impairment was significantly associated with the
presence of psychiatric symptoms (p=0.04) at 12 months. Specifically, cognitive
Page 13 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 14
impairment was associated with anxiety (p=0.04), but not depression (p=0.20) or
PTSD (p=0.33).
Long-Term Cognitive Impairment, Psychiatric Morbidity, and Quality of Life
Quality of life was low in ACOS survivors (median utility=0.67, IQR: 0.37,
0.90) at 12 months. There were no significant differences in quality of life
between cognitively impaired and non-impaired survivors (median utility in
impaired=0.66, IQR: 0.45, 0.9; non-impaired=0.69, IQR: 0.42, 0.82, p=0.85). In
survivors with psychiatric symptoms, quality of life was significantly worse
(median utility in 59 survivors with psychiatric symptoms=0.57, IQR: 0.26, 0.76;
utility in 35 survivors without symptoms=0.90, IQR: 0.53, 0.95, p<0.001).
Risk Factors for Long-Term Cognitive Impairment
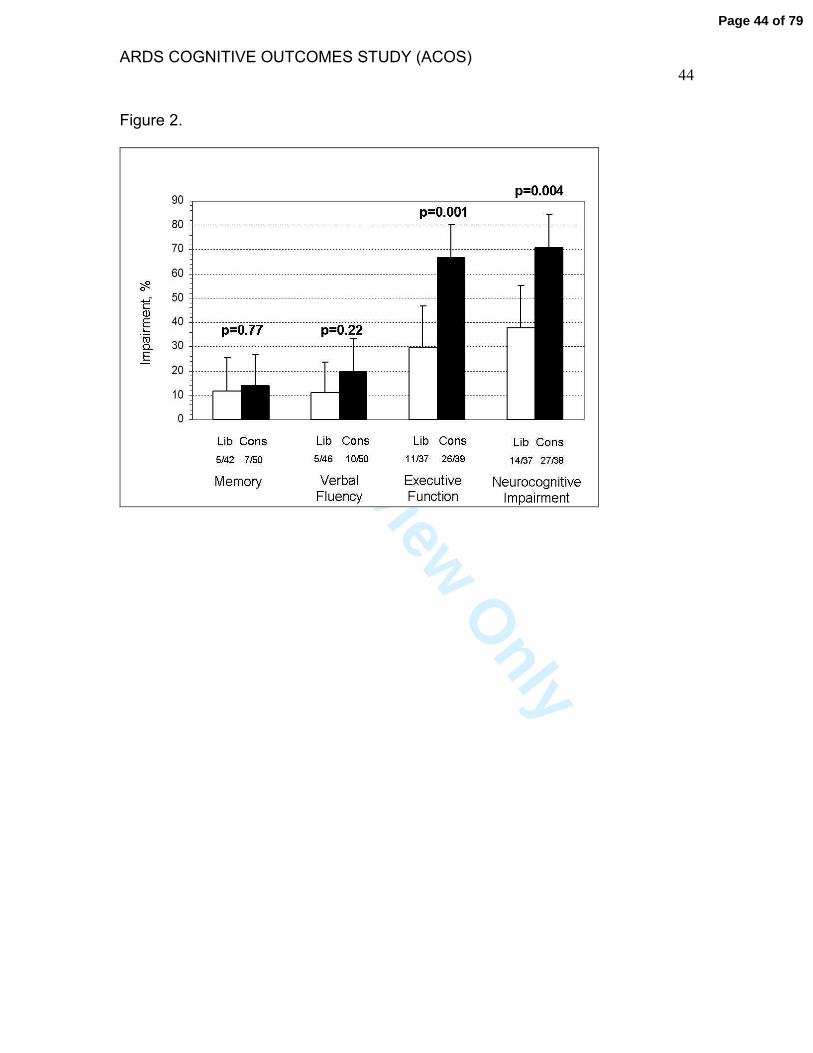
Lower partial pressure of arterial oxygen (PaO2) during FACTT was
associated with cognitive impairment at 12 months (p=0.02), as were enrollment
in the conservative fluid-management strategy (p=0.004) and lower central
venous pressure (p=0.04) (Table 2, E5, Figure 2). As detailed in the supplement,
lower PaO2 values (p=0.05), lower central venous pressures (p=0.02), and
enrollment in the conservative fluid-strategy group (p<0.001) correlated with
worse executive function. After adjustment for potential covariates, lower PaO2
and enrollment in the conservative fluid-management strategy were associated
independently with cognitive impairment at 12 months (Table 2 and Table E6).
Page 14 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 15
In secondary analyses, using the untimed error score of the HSCT for the
executive function assessment, the conservative fluid-management strategy
remained associated with cognitive impairment at 12 months (71% (34/48) vs.
48% (20/42) in liberal group, p=0.02). The association between PaO2 values and
cognitive impairment was no longer significant in these analyses (p=0.32). As
detailed in the supplement, we performed multiple sensitivity analyses to
determine the effects of missing data and incomplete cognitive testing. These
analyses may suggest that a relationship exists between hypoxemia and fluid-
management strategy and long-term cognitive impairment.
Risk Factors for Long-Term Psychiatric Morbidity
Survivors with psychiatric morbidity at 12 months had lower PaO2 values
(p=0.02), lower systolic blood pressures (p=0.05), and were more likely to have
had an episode of hypoglycemia (p=0.03) (Table 3). As detailed in the
supplement, lower PaO2 values (p=0.05), lower systolic blood pressures
(p=0.04), and an episode of hypoglycemia (p=0.01), were associated with
anxiety. After adjustment for potential covariates, lower PaO2 was associated
independently with long-term psychiatric morbidity.
Discussion
We found that neuropsychological function in survivors from a multi-center
trial can be assessed using a validated telephone battery. Similar to previous
investigations, we found a majority of ALI survivors experience long-term
Page 15 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 16
cognitive and psychiatric morbidity. Furthermore, our findings demonstrate a
relationship between cognitive impairment, psychiatric symptoms, and adverse
quality of life in long-term survivors. Finally, we confirmed prior associations that
hypoxemia is a potential risk factor for the development of long-term cognitive
and psychiatric impairment.
We found that neuropsychological function can be assessed over the
telephone in a multi-center trial. This has the potential to be an important
development for future critical care trials, as neuropsychological impairment is
increasingly recognized as a common, long-lasting, and potentially modifiable
outcome. However, our experience highlights potential limitations of measuring
neuropsychological function in multi-center trials.
First, attrition was significant. Attrition is a recognized barrier to conducting
long-term outcomes studies in critical care trials (24-25, 57-59), due in part to the
mortality experienced by critically ill patients. After accounting for mortal losses,
the requirement that subjects be enrolled in EA-PAC, and the delay in study
initiation, only 406 of the 1001 subjects randomized in FACTT were alive and
eligible for ACOS.
However, as 12% of eligible survivors declined and 36% were unable to
be contacted to obtain consent for ACOS after discharge, the opportunity to
increase subject participation in future studies exists. Potential solutions to
increase consent rate in future studies include: enrolling subjects prospectively
and prioritizing in-person consent prior to discharge, and employing multiple
strategies and repeated attempts to contact potential subjects (60-61).
Page 16 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 17
Furthermore, as 12% of subjects who consented to long-term neuropsychological
assessment subsequently declined and 25% were lost to follow-up, the
opportunity to improve retention also exists. Although it is unclear why subjects
declined to be tested, potential explanations include that subjects were asked to
complete multiple follow-up interviews as part of EA-PAC and ACOS and
neuropsychological assessments were lengthy. Finally, subjects completed
cognitive testing via the telephone to varying degrees. Fatigue and/or frustration
appeared to play a role, as did an error in test administration. Future studies will
need to balance the merits of administering a more comprehensive battery with
the potential burden imposed upon study participants.
Potential solutions to improve retention and test completion in future
studies include: increasing the flexibility of scheduling by centralizing test
administration in different time-zones to minimize potential conflicts with work
and/or healthcare visits, increasing the number of trained staff to administer the
neuropsychological battery and identifying and employing the most effective
strategies to ensure test completion, selecting an intermediate testing timepoint
(e.g., 3 months) which minimizes mortal losses yet ensures adequate time for
survivors to transition through the healthcare system to home (24-25, 62-63),
using a shorter test battery (64) or limiting the domains to be assessed (62), and
using multiple strategies in a systematic fashion to retain participants (60-61).
Through the effective use of many of these strategies, more recent studies are
demonstrating the ability to recruit and retain ALI survivors successfully (61, 65-
66). Finally, compared to non-participants, ACOS subjects were more likely to
Page 17 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 18
be female and white; as such, our findings may not generalize to other
populations.
In conclusion, we found that we were able to assess long-term
neuropsychological function in survivors from a multi-center trial using a
telephone battery. However, we encountered significant challenges in regards to
recruitment, retention, and test completion. We acknowledge that these
challenges pose a potential threat to the internal and external validity of such an
approach. To improve the performance of this practical approach in future
studies, we have highlighted potential solutions to improve recruitment, retain
study participants, and ensure complete neuropsychological assessments.
The ALI subjects in our study had long-term cognitive and psychiatric
morbidity consistent with prior studies where data was obtained in-person (6-9,
24-25). Coupled with our prior work (10-11, 30), our findings validate that many
ALI survivors experience clinically important long-term cognitive impairment.
Approximately half of our ALI survivors had executive dysfunction. While
cognitive impairment was not associated with decreased quality of life in ALI
survivors enrolled in ACOS, the evidence supports that cognitive impairment has
a considerable adverse impact on individuals and society (6-21, 67-68).
ALI survivors enrolled in ACOS experienced anxiety, depression, and
PTSD symptoms. The presence of long-term psychiatric symptoms, and
symptoms of anxiety in particular, was found to be associated with lower PaO2
values and hypoglycemia during the hospitalization. Our findings validate the
recent work of Hopkins et al, wherein hypoxemia was associated with anxiety at
Page 18 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 19
1 year in ARDS survivors (18), augment the recent work of Dowdy et al which
found that hypoglycemia was associated with depression at 3 months (20), and
support the notion that psychiatric symptoms may result from brain injury
sustained during the hospitalization. We found that psychiatric morbidity was
associated with cognitive impairment and significantly worse quality of life.
Because cognitive impairment may lead to development of psychiatric symptoms
(18), and psychiatric symptoms may lead to impaired physical function (66), our
findings support the idea that cognitive impairment, psychiatric symptoms, and
quality of life are inter-related and impact upon each other in survivors of critical
illness.
We found that hypoxemia is a potential risk factor for the development of
long-term cognitive impairment. Consistent with the work of Hopkins and
colleagues (6), we found lower PaO2 values were associated with cognitive
impairment in general and executive dysfunction specifically. Enrollment in the
conservative fluid-management strategy was identified as a potential risk factor
for the development of long-term cognitive impairment and executive dysfunction.
To potentially explain this finding, we demonstrated that within the ACOS
population lower central venous pressures, the explicit target of the conservative
fluid-management strategy, were associated with cognitive impairment and
executive dysfunction. However, there was no indirect evidence for reduced
cerebral perfusion (e.g., cardiac index, systolic blood pressure) as the mediator
for the observed association, thus it is unclear how conservative fluid
management may have caused cognitive impairment. Given the highly selected
Page 19 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 20
population that enrolled in and completed ACOS testing, it is unclear if this
finding generalizes to the entire FACTT cohort. This finding will need to be
validated.
Our study sample size limits the generalizability of our findings and is a
major limitation. We also acknowledge the potential for uncontrolled confounding
as our sample size limited our ability to adjust for potential covariates
simultaneously, we were unable to adjust for sedation or delirium (25, 69), and
we did not screen for pre-existing dementia formally (70) or pre-existing
psychiatric disease. There exists the potential for informative censoring, and
although some subjects were determined to be incapable of telephone-based
neuropsychological testing, we did not assess formally for hearing loss before
testing. Although furosemide has been associated with hearing loss, there was
no association between furosemide dose administered and cognitive impairment
(Table E5). We used conservative criteria to define cognitive impairment and
limited the probability of a Type I error (46); however, our multiple comparisons
could result in falsely-rejecting the null hypothesis. If we used a Bonferroni
correction factor, only the conservative fluid-management strategy would remain
associated with cognitive impairment. Regardless, our risk factor assessment
requires confirmation. Finally, depression, anxiety, and PTSD were identified
using self-report measures, which may overdiagnose these disorders. These
psychiatric instruments, while reliable and valid, are not the gold standard for
clinical diagnosis.
Page 20 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 21
In conclusion, we found that neuropsychological function can be assessed
in a multi-center trial, but it was challenging and opportunities to improve the
performance of this strategy exist. Our findings validate that cognitive and
psychiatric morbidity are common in ALI survivors, findings that have significant
implications for these patients long-term functioning. Executive dysfunction,
specifically, was a common morbidity. We found evidence that hypoxemia is a
risk factor for long-term cognitive and psychiatric impairment and a signal that
fluid management strategy is a potential risk factor for long-term cognitive
impairment. Further studies are necessary to confirm this latter observation given
the select population studied and an unclear mechanism. Future clinical trials in
critically ill populations should include assessment of long-term outcomes,
including neuropsychological outcomes. We will need to be cautious in our
interpretation of such studies and acknowledge that confirmatory studies may be
required. Nevertheless, to improve the lives of critically ill survivors, we should
assess both the short- and long-term effects of an intervention.
Page 21 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 22
Acknowledgments
We thank the subjects for their participation in follow-up interviews and their
family members for their support to better understand long-term
neuropsychological effects of critical illness. We acknowledge the contributions of
Gilles Clermont, Lan Kong, and Kim Fusko of the University of Pittsburgh for
project and data management and for recruiting, coordinating and conducting
interviews and to investigators and study coordinators at participating ARDS
Clinical Trials Network sites for recruitment, data collection, and support.
Page 22 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 23
References
1.) Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, Neff M, Stern
EJ, Hudson LD. Incidence and outcomes of acute lung injury. N Engl J Med
2005; 353:1685-93
2.) The Acute Respiratory Distress Syndrome Network. Ventilation with lower
tidal volumes as compared with traditional tidal volumes for acute lung injury and
the acute respiratory distress syndrome. N Engl J Med 2000; 342: 1301-1308
3.) The Acute Respiratory Distress Syndrome Network. High versus lower
positive end-expiratory pressures in patients with the acute respiratory distress
syndrome. N Engl J Med 2004; 351: 327-336
4.) The National Heart, Lung, and Blood Institute Acute Respiratory Distress
Syndrome (ARDS) Clinical Trials Network. Comparison of two fluid management
strategies in acute lung injury. N Engl J Med 2006; 354(24): 2564-75
5.) Iwashyna TJ. Survivorship will be the defining challenge of critical care in the
21st century. Ann Intern Med 2010; 153(3): 204-205
6.) Hopkins R, Weaver L, Pope D, Orme J, Bigler E, Larson-Lohr V.
Neuropsychological sequelae and impaired health status in survivors of severe
acute respiratory distress syndrome. Am J Respir Crit Care Med 1999; 160:50-6
7.) Hopkins RO, Weaver LK, Chan KJ, Orme JF. Quality of life, emotional, and
cognitive function following acute respiratory distress syndrome. J Int
Neuropsychol Soc 2004; 10:1005-1017
8.) Rothenhausler HB, Ehrentraut S, Stoll C, Schelling G, Kapfhammer HP. The
relationship between cognitive performance and employment and health status in
Page 23 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 24
long-term survivors of the acute respiratory distress syndrome: results of an
exploratory study. Gen Hosp Psychiatry 2001; 23:90-96
9.) Hopkins RO, Weaver LK, Collingridge D, Parkinson RB, Chan KJ, Orme JF.
Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory
distress syndrome. Am J Respir Crit Care Med 2005; 171:340-347
10.) Christie JD, Biester R, Taichman DB, Shull WH, Hansen-Flaschen J, Shea
JA, Hopkins RO. Formation and validation of a telephone battery to assess
cognitive function in acute respiratory distress syndrome survivors. J Crit Care
2006; 21:125-132
11.) Mikkelsen ME, Shull WH, Biester RC, Taichman DB, Lynch S, Demissie
E, Hansen-Flaschen J, Christie JD. Cognitive, mood and quality of life
impairments in a select population of ARDS survivors. Respirology 2009; 14: 76-
82
12.) Herridge MS, Cheung AM, Tansey CM, Matte-Martyn A, Diaz-Granados
N, Al-Saidi F, Cooper AB, Guest CB, Mazer CD, Mehta S, Stewart TE, Barr A,
Cook D, Slutsky AS, for the Canadian Critical Care Trials Group. One-year
outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med
2003; 348:683-93
13.) Herridge MS, Tansey CM, Matté A, Tomlinson G, Diaz-Granados N,
Cooper A, Guest CB, Mazer CD, Mehta S, Stewart TE, Kudlow P, Cook D,
Slutsky AS, Cheung AM, for the Canadian Critical Care Trials Group. Functional
disability 5 years after acute respiratory distress syndrome. N Engl J Med 2011;
364: 1293-1304
Page 24 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 25
14.) Adhikari NK, McAndrews MP, Tansey CM, Matté A, Pinto R, Cheung AM,
Diaz-Granados N, Barr A, Herridge MS. Self-reported symptoms of depression
and memory dysfunction in survivors of ARDS. Chest 2009; 135(3): 678-87
15.) Adhikari NK, Tansey CM, McAndrews MP, Matté A, Pinto R, Cheung AM,
Diaz-Granados N, Herridge MS. Self-reported depressive symptoms and
memory complaints in survivors five years after ARDS. Chest 2011; 140(6):
1484-93
16.) Davydow DS, Desai SV, Needham DM, Bienvenu OJ. Psychiatric
morbidity in survivors of the acute respiratory distress syndrome: a systematic
review. Psychosom Med 2008; 70: 512-519
17.) Nelson BJ, Weinert CR, Burly CL, Marinelli WA, Gross CR. Intensive care
unit drug use and subsequent quality of life in acute lung injury patients. Crit Care
Med 2000; 28(11): 3626-30
18.) Hopkins RO, Key CW, Suchyta DO, Weaver LK, Orme JF. Risk factors for
depression and anxiety in survivors of acute respiratory distress syndrome. Gen
Hosp Psych 2010; 32: 147-155
19.) Dowdy DW, Bienvenu OJ, Dinglas V, Mendez-Tellez PA, Sevransky J,
Shanholtz C, Needham DM. Are intensive care factors associated with
depressive symptoms six months after acute lung injury? Crit Care Med 2009;
37: 1702-1707
20.) Dowdy DW, Dinglas V, Mendez-Tellez PA, Bienvenu OJ, Sevransky J,
Dennison CR, Shanholtz C, Needham DM. Intensive care unit hypoglycemia
Page 25 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 26
predicts depression during early recovery from acute lung injury. Crit Care Med
2008; 36: 2726-2733
21.) Kapfhammer HP, Rothenhausler HB, Krauseneck T, Stoll C, Schelling G.
Posttraumatic stress disorder and health-related quality of life in long-term
survivors of acute respiratory distress syndrome. Am J Psych 2004; 161(1): 45-
52
22.) Ehlenbach WJ, Hough CL, Crane PK, et al. Association between acute
care and critical illness hospitalization and cognitive function in older adults.
JAMA 2010; 303(8): 763-770
23.) Iwashyna TJ, Ely EW, Smith DM, et al. Long-term cognitive impairment
and functional disability among survivors of severe sepsis. JAMA
2010;304(16):1787-1794
24.) Jackson JC, Girard TD, Gordon SM, Thompson JL, Shintani AK,
Thomason JWW, Pun BT, Canonico AE, Dunn JG, Bernard GR, Dittus RS, Ely
EW. Long-term cognitive and psychological outcomes in the awakening and
breathing controlled trial. Am J Respir Crit Care Med 2010; 182: 183-191
25.) Girard TD, Jackson JC, Pandharipande PP, Pun BT, Thompson JL,
Shintani AK, Gordon SM, Canonico AE, Dittus RS, Bernard GR, Ely EW.
Delirium as a predictor of long-term cognitive impairment in survivors of critical
illness. Crit Care Med 2010; 38(7): 1513-20
26.) Jones C, Griffiths RD, Slater T, Benjamin KS, Wilson S. Significant
cognitive dysfunction in non-delirious patients identified during and persisting
following critical illness. Intensive Care Med 2006; 32: 923-926
Page 26 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 27
27.) Desai S, Lawa TJ, Needham DM. Long-term complications of critical care.
Crit Care Med 2011; 39(2): 371-379
28.) Davydow DS, Gifford JM, Desai SV, Needham DM, Bienvenu OJ.
Posttraumatic stress disorder in general intensive care unit survivors: a
systematic review. Gen Hosp Psych 2008; 30: 421-434
29.) Davydow DS, Gifford JM, Desai SV, Bienvenu OJ, Needham DM.
Depression in general intensive care unit survivors: a systematic review. Int Care
Med 2009; 35: 796-809
30.) Taichman DB, Christie J, Biester R, Mortensen J, White J, Kaplan S,
Hansen-Flaschen J, Palevsky HI, Elliott CG, Hopkins RO. Validation of a brief
telephone battery for cognitive assessment of patients with pulmonary arterial
hypertension. Respir Res 2005; 6: 39
31.) The National Heart, Lung, and Blood Institute Acute Respiratory Distress
Syndrome (ARDS) Clinical Trials Network. Pulmonary-artery versus central
venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:
2213-24
32.) Mikkelsen ME, Lanken PN, Biester R, Gallop R, Bellamy S, Localio AR,
Hopkins RO, Angus DC, Christie JD for the ARDSNet. Conservative fluid
strategy is associated with neurocognitive deficits in survivors of acute lung injury
[abstract]. Am J Respir Crit Care Med 2008; 177: A819
33.) Clermont G, Kong L, Weissfeld LA, Lave JR, Rubenfeld GD, Roberts MS,
Connors AF, Bernard GR, Thompson BT, Wheeler AP, Angus DC. The effect of
Page 27 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 28
pulmonary artery catheter use on costs and long-term outcomes of acute lung
injury. PLoS ONE 2011; 6(7): e22512
34.) Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M,
Legall JR, Morris A, Spragg R. The American-European consensus conference
on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial
coordination. Am J Respir Crit Care Med 1994; 149: 818–824
35.) Burgess PW, Shallice T. The Hayling and Brixton Tests. London, England:
Thames Valley Test Company Limited, 2007
36.) Sukantarat KT, Burgess PW, Williamson RC, Brett SJ. Prolonged
cognitive dysfunction in survivors of critical illness. Anaesthesia 2005; 60, 847-
853
37.) Biggs JT, Wylie LT, Ziegler VE. Validity of the Zung self-rating depression
scale. British J Psych 1978; 132: 381-385
38.) Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring
clinical anxiety: psychometric properties. J Cons Clin Psychol 1998; 56:893-7
39.) Weisaeth L. Torture of a Norwegian ship’s crew: the torture, stress
reactions and psychiatric aftereffects. Acta Psychiatr Scand Suppl 1989; 355: 63-
72
40.) Wechsler D, ed. Wechsler Adult Intelligence Scale, Third edition. San
Antonio: The Psychological Corporation; 1997
41.) Wechsler D. Wechsler Memory Scale. San Antonio: The Psychology
Corporation, 1997
Page 28 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 29
42.) Lezak MD. Neuropsychological Assessment. New York: Oxford University
Press, 1995
43.) Torrance GW, Feeny DH, Furlong WJ, Barr RD, Zhang Y, Wang Q. Multi-
attribute preference functions for a comprehensive health status classification
system: Health utilities index Mark 2. Medical Care 1996; 34(7): 702-722
44.) Heaton RK, Grant I, Matthews CG. Comprehensive norms for an
expanded Halstead-Reitan Battery: demographic corrections, research findings
and clinical applications. Psychological Assessment Resources, Inc., Odessa,
1991
45.) Heaton RK. Comprehensive norms for an expanded Halstead-Reitan
Battery: A supplement for the WAIS-R. Psychological Assessment Resources,
Inc., Odessa, 1994
46.) Ingraham LJ, Aiken CB. An empirical approach to determining criteria for
abnormality in test batteries with multiple measures. Neuropsychology 1996;
10:120-124
47.) Doblar DD, Hinckle JC, Fay ML, Condon BF. Air embolism associated with
pulmonary artery catheter introducer kit. Anesthesiology 1982; 56: 307-309
48.) Boyd KD, Thomas SJ, Boyd AD. A prospective study of complications of
pulmonary artery catheterizations in 500 consecutive patients. Chest 1983; 84:
245-249
49.) Reichenberg A, Yirmiya R, Schuld A, Kraus T, Haack M, Morag A,
Pollmächer T. Cytokine-associated emotional and cognitive disturbances in
humans. Arch Gen Psychiatry 2001; 58: 445-452
Page 29 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 30
50.) Patarca-Montero R, Antoni M, Fletcher MA, Klimas NG. Cytokine and
other immunologic markers in chronic fatigue syndrome and their relation to
neuropsychological factors. Appl Neuropsychol 2001; 8: 51-64
51.) Ngandu T, von Strauss E, Helkala EL, Winblad B, Nissinen A, Tuomilehto
J, Soininen H, Kivipelto M. Education and dementia: what lies behind the
association? Neurology 2007; 69: 1442-1450
52.) Richards PM, Ruff RM. Motivational effects on neuropsychological
functioning: comparison of depressed versus nondepressed individuals. J
Consult Clin Psychol 1989; 57: 396-402
53.) Buckelew SP, Hannay HJ. Relationships among anxiety, defensiveness,
sex, task difficulty and performance on various neuropsychological tasks.
Percept Mot Skills 1986; 63: 711-718
54.) Schelling G, Stoll C, Kapfhammer HP, Rothenhausler HB, Krauseneck T,
Durst K, Haller M, Briegel J. The effect of stress doses of hydrocortisone during
septic shock on posttraumatic stress disorder and health-related quality of life in
survivors. Crit Care Med 1999; 27: 2678-2683
55.) Maldonado G, Greenland S. Simulation study of confounder-selection
strategies. Amer J of Epid 1993; 138: 923-936
56.) Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation
study of the number of events per variable in logistic regression analysis. J Clin
Epidemiol 1996; 49: 1373-1379
57.) Rubenfeld GD. Improving clinical trials of long-term outcomes. Crit Care
Med 2009; 37: S112-S116
Page 30 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 31
58.) Kress JP, Gehlbach B, Lacy M, Pliskin N, Pohlman AS, Hall JB. The long-
term psychological effects of daily sedative interruption on critically ill patients.
Am J Respir Crit Care Med 2003; 168: 1457-1461
59.) Strom T, Stylsvig M, Toft P. Long-term psychological effects of a no-
sedation protocol in critically ill patients. Critical Care 2011; 15:R293
60.) Robinson KA, Dennison CR, Wayman DM, Pronovost PJ, Needham DM.
Systematic review identified number of strategies important to retaining study
participants. J Clin Epidemiol 2007; 60(8): 757-765
61.) Chen KF, Colantuoni E, Siddiqi F, Dinglas VD, Sepulveda KA, Fan E,
Pronovost PJ, Needham DM. Repeated attempts using different strategies are
important for timely contact with study participants. J Clin Epidemiol 2011; 64:
1144-1151
62.) Jackson J, Ely EW, Morey MC, Anderson VM, Siebert CS, Denne LB,
Clune J, Archer KR, Torres R, Janz D, Schiro E, Jones J, Shintani A, Levine B,
Pun BT, Thompson J, Brummel NE, Hoenig H. Cognitive and physical
rehabilitation of intensive care unit survivors: results of the RETURN randomized
controlled pilot investigation. Crit Care Med 2012; 40: 000-000
63.) Unroe M, Kahn JM, Carson SS, Govert JA, Martinu T, Sathy SJ, Clay AS,
Chia J, Gray A, Tulsky JA, Cox CE. One-year trajectories of care and resource
utilization for recipients of prolonged mechanical ventilation: a cohort study. Ann
Intern Med 2010; 153: 167-175
64.) Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V,
Collin I, Cummings JL, Chertkow H. The Montreal Cognitive Assessment, MoCA:
Page 31 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 32
a brief screening tool for mild cognitive impairment. J Amer Ger Soc 2005; 53:
695-699
65.) National Heart, Lung, and Blood Institute; Johns Hopkins University.
Evaluating health outcomes and quality of life after acute lung injury among
participants of the ALTA, OMEGA, and EDEN (ARDS Network) studies (The
ALTOS Study). In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library
of Medicine (US). 2000-2012. Available from: http://clinicaltrials.gov/show/
NCT00719446 NLM Identifier: NCT00719446
66.) Bienvenu OJ, Colantuoni E, Mendez-Tellez PA, Dinglas VD, Shanholtz C,
Husain N, Dennison CR, Herridge MS, Pronovost PJ, Needham DM. Depressive
symptoms and impaired physical function after acute lung injury: a 2-year
longitudinal study. Am J Respir Crit Care Med 2012; 185: 517-524
67.) Rozzini L, Chilovi BV, Trabucchi M, Padovani A, Marson D, Griffith R.
Impaired financial abilities in mild cognitive impairment: A direct assessment
approach. Neurology 2003; 60: 2021
68.) Jonsson L, Lindgren P, Wimo A, Jonsson B, Winblad B. Costs of mini
mental state examination-related cognitive impairment. Pharmacoeconomics
1999; 16: 409-416
69.) Van den Boogard M, Schoonhoven L, Evers AW, van der Hoeven JG, van
Achterberg TV, Pickkers P. Delirium in critically ill patients: impact on long-term
health-related quality of life and cognitive functioning. Crit Care Med 2012; 40(1):
112-118
Page 32 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 33
70.) Pisani MA, Inouye SK, McNicoll L, Redlich CA. Screening for preexisting
cognitive impairment in older intensive care unit patients: use of proxy
assessment. J Am Geriatr Soc 2003; 51: 689-693
Page 33 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 34
Figure 1. Enrollment and outcomes. Abbreviations: ACOS=ARDS Cognitive Outcomes Study. Figure 2. Long-term cognitive impairment according to fluid management strategy. Impairment in a domain was defined as a score > 2 SD below the population norm. Cognitive impairment was defined as impairment in memory, verbal fluency, and/or executive function in the 75 survivors completing testing in each of these cognitive domains. Memory, verbal fluency, or executive function was assessed in 92, 96, and 76 subjects, respectively. Proportions of impaired subjects are specified by domain, according to fluid-management strategy. Error bars reflect upper bound of 95% confidence interval. Lib=liberal fluid strategy, Cons=conservative fluid strategy.
Page 34 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 35
Table 1. Comparison of baseline characteristics between FACTT 60-day survivors not enrolled in ACOS and ACOS participants.
FACTT Survivors
Not Enrolled in ACOS (N=609)
ACOS Cohort
(N=122)
p-value
Variable
Age (yr) 47 (37 – 57) 49 (40 – 58) 0.23
Male sex (%) 54 43 0.04
Race or ethnic group (%) White non-Hispanic Black non-Hispanic Hispanic Other
64 21 7 8
86 11 3 0
<0.001
Primary Lung Injury (%) Pneumonia Sepsis Aspiration Trauma Multiple transfusions Other
49 20 16 9 1 5
36 25 16 8 2
13
0.005
Co-existing conditions (%) None Diabetes HIV infection or AIDS Cirrhosis Solid tumors Leukemia Lymphoma Immunosuppression
71 16 7 3 1 2 0 6
75 18 0 2 1 1 2 7
0.39 0.65 0.001 0.78 1.00 1.00 0.13 0.84
APACHE III score, mean (SD) 85 (66 – 105) 85 (63 – 102) 0.32
Medical ICU
65 56 0.06
Glasgow Coma Scale 8 (6 – 12) 8 (4 – 11) 0.38
Mean arterial pressure, mm Hg 76 (68 – 87) 77 (67 – 85) 0.49
Vasopressor use, (%) 34 33 0.81
PaO2:FiO2 122 (83 – 168) 122 (86 – 165) 0.73
Conservative strategy (%) 51 55 0.38
Pulmonary artery catheter (%) 51 52 0.70
Definition of abbreviation: ACOS=ARDSNet Cognitive Outcomes Study; AIDS=acquired immunodeficiency virus; APACHE III= Acute Physiologic and Chronic Health Evaluation III scores; HIV=human immunodeficiency virus; PaO2:FiO2=ratio of partial pressure of arterial oxygen to fraction of inspired oxygen. Values expressed as a percentage or median (interquartile range).
Page 35 of 79

For Review Only
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 36
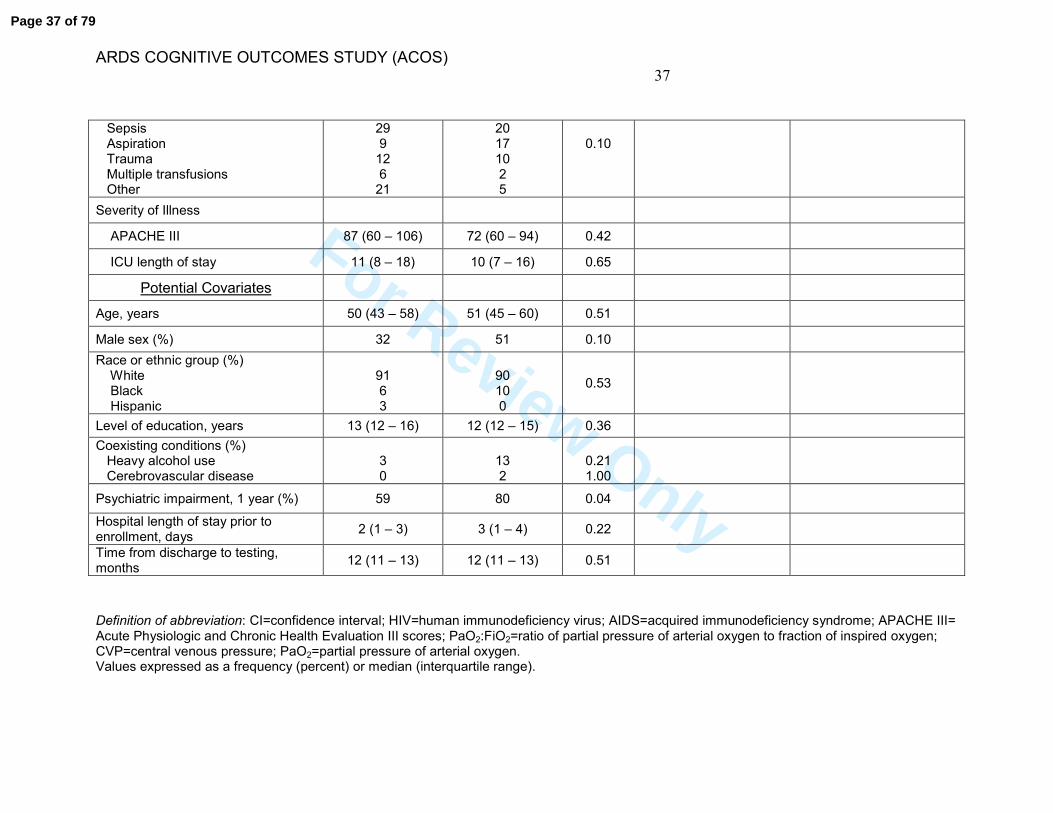
Table 2. Associations with long-term cognitive impairment in ALI survivors. Cognitive impairment at the subject level was defined as impairment in memory, verbal fluency, and/or executive function in the 75 subjects who completed tests in each of these domains at the 12-month follow-up.
Long-Term Cognitive Impairment
Not Impaired
(n=34) Impaired (n=41)
p-value Unadjusted Odds
Ratio (95% CI) Adjusted Odds Ratio
(95% CI) ‡
Candidate Risk Factors
Duration of mechanical ventilation 8 (4 – 11) 6 (4 – 9) 0.43
Conservative fluid-management strategy (%)
32 66 0.004 4.03 (1.53 – 10.59) 3.35 (1.16 – 9.70) –
5.46 (1.92 – 15.53)
Hypotension (hemodynamic data on-study) *
Systolic Blood Pressure (mm Hg) 108 (102 – 113) 104 (96 – 112) 0.32
Cardiac index (liters/min/m2)
† 4.5 (3.8 – 5.3) 4.5 (3.7 – 5.0) 0.49
Shock * (%) 32 29 0.77
Vasopressor use 26 24 0.84
Hypoxemia (respiratory variables on-study)
PaO2 86 (70 – 98) 71 (67 – 80) 0.02 1.56 (1.09 – 2.24) §
1.51 (1.01 – 2.26) –
1.68 (1.14 – 2.49) §
PaO2:FiO2 152 (132 – 192) 157 (133 – 190) 0.63
Oxygenation index 7.38 (4.55 –
10.42) 7.67 (5.97 –
10.02) 0.57
Oxygen saturation (%) 95.1 (93.3 – 96.8) 94.2 (92.6 – 95.8) 0.10
Pulmonary artery catheter (%) 53 61 0.48
Primary lung injury (%) Pneumonia
24
46
Page 36 of 79
For Review Only
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 37
Sepsis Aspiration Trauma Multiple transfusions Other
29 9
12 6
21
20 17 10 2 5
0.10
Severity of Illness
APACHE III 87 (60 – 106) 72 (60 – 94) 0.42
ICU length of stay 11 (8 – 18) 10 (7 – 16) 0.65
Potential Covariates
Age, years 50 (43 – 58) 51 (45 – 60) 0.51
Male sex (%) 32 51 0.10
Race or ethnic group (%) White Black Hispanic
91 6 3
90 10 0
0.53
Level of education, years
13 (12 – 16) 12 (12 – 15) 0.36
Coexisting conditions (%) Heavy alcohol use Cerebrovascular disease
3 0
13 2
0.21 1.00
Psychiatric impairment, 1 year (%) 59 80 0.04
Hospital length of stay prior to enrollment, days
2 (1 – 3) 3 (1 – 4) 0.22
Time from discharge to testing, months
12 (11 – 13) 12 (11 – 13) 0.51
Definition of abbreviation: CI=confidence interval; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome; APACHE III= Acute Physiologic and Chronic Health Evaluation III scores; PaO2:FiO2=ratio of partial pressure of arterial oxygen to fraction of inspired oxygen; CVP=central venous pressure; PaO2=partial pressure of arterial oxygen. Values expressed as a frequency (percent) or median (interquartile range).
Page 37 of 79
For Review Only
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 38
On-study variables were summarized at the subject level as means to account for influential observations. With the exception of systolic blood pressure, in which the worst values over the preceding 24 hours were recorded to derive the cardiovascular component of the Brussels organ failure score, values were measured and recorded daily (measure closest to 8 am) during the study. * Shock defined as mean arterial pressure < 60 or vasoactive agent use (assignment to FACTT protocol cells 1 or 2) at any time during FACTT (4). †
Cardiac index was measured in 39 survivors (20 in the liberal-strategy group and 19 in the conservative-strategy group). ‡ Potential covariates were included in the multivariable logistic regression models one covariate at-a-time. The adjusted odds ratios presented represent the range of odds ratios observed in multivariable logistic regression models. For additional details, please see Table E6 in the on-line supplement. § For each 10-unit decrease in PaO2, odds ratio for the development of cognitive impairment increased by 1.56.
Page 38 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 39
Table 3. Associations with long-term psychiatric morbidity in ALI survivors. Psychiatric morbidity was defined as present if symptoms of anxiety, depression, or post-traumatic stress disorder were identified at the 12-month follow-up.
Psychiatric Morbidity
Not Present
(n=35) Present (n=67)
p-value
Baseline characteristics
Age, years 51 (38 – 64) 50 (44 – 57) 0.58
Male sex (%) 40 45 0.64
Race or ethnic group (%) White Black Hispanic
94 6 0
81 15 4
0.19
Level of education, years 14 (12 – 16) 12 (12 – 15) 0.15
Medical ICU (%) 49 58 0.44
APACHE III
88 (63 – 108) 77 (60 – 99) 0.31
Conservative strategy (%) 46 60 0.18
Pulmonary artery catheter (%) 57 52 0.64
On-study variables *
Hemodynamic variables†
Systolic Blood Pressure (mm Hg) 111 (102 – 116) 104 (98 – 111) 0.05
Shock (%) 37 30 0.46
Respiratory variables
PaO2 ‡ 86 (72 – 98) 72 (68 – 90) 0.02
Metabolic variables
Glucose (mg/dL) 123 (107 – 140) 119 (109 – 136) 0.99
Hypoglycemia‡, < 60 mg/dL (%) 0 13 0.03
Hyperglycemia‡, > 180 mg/dL (%) 34 30 0.65
Corticosteroid therapy §
Corticosteroids (mg of
Methylprednisolone, cumulative) 0 (0 – 60) 0 (0 – 140) 0.58
Corticosteroids received (%) 29 33 0.66
ICU length of stay (days) 11 (7 – 20) 12 (8 – 16) 0.92
Duration of mechanical ventilation (days)
7 (4 – 15) 7 (4 – 10) 0.94
Definition of abbreviation: ICU=intensive care unit; APACHE III= Acute Physiologic and Chronic Health Evaluation III scores; PaO2=partial pressure of arterial oxygen.
Page 39 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 40
Values expressed as a frequency (percent) or median (interquartile range).
* On-study variables were summarized at the subject level as means to account for influential
observations. With the exception of systolic blood pressure, in which the worst values over the preceding 24 hours were recorded to derive the cardiovascular component of the Brussels organ failure score, values were measured and recorded daily (measure closest to 8 am) during the study. †
Shock defined as mean arterial pressure < 60 or vasoactive agent use (assignment to FACTT protocol cells 1 or 2) at any time during FACTT (4). The association between systolic blood pressure and psychiatric impairment was non-significant after adjustment for potential covariates (p=0.14). ‡
For each 10-unit decrease in PaO2, odds ratio for the development of psychiatric morbidity
increased by 1.35 (95% confidence interval 1.02, 1.78) and the association remained after adjustment for potential covariates. Hypo- and hyperglycemia were defined as any episode of serum glucose < 60 mg/dL or > 180 mg/dL, respectively, during the hospitalization. We were unable to adjust for potential covariates in the association between hypoglycemia and psychiatric morbidity as psychiatric symptoms were present in each subject who had a hypoglycemia episode. §
Corticosteroid therapy was neither associated with PTSD (11 of 32 subjects (34%) who received corticosteroids experienced symptoms of PTSD compared with 29 of 70 subjects (41%) who did not receive corticosteroids, p=0.50), nor was corticosteroid therapy associated with psychiatric morbidity in the subgroup of 27 sepsis-associated ALI subjects (6 of 12 subjects (50%) who received corticosteroids experienced long-term psychiatric morbidity compared to 11 of 15 subjects (73%) who did not receive corticosteroids, p=0.26).
Page 40 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 41
Figure 1.
Page 41 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 42
Consented to long-term follow-up for EA-PAC
N=655
Tested at 12 months ‡
N=102
Subjects randomized in FACTT N=1001
Consented to ACOS N=213
Causes outside of investigator control: Deceased: N=22 Incarcerated: N=2 Incapable
†: N=9
Causes which may be potentially remediable by future investigators: Declined: N=25 Lost to follow-up
†: N=53
Total: N=111
Ineligible: N=227 * Declined: N=119 Total: N=346
Completed Testing in All Domains
N=75
Causes outside of investigator control: Deceased: N=194 Ineligible
†: N=55
Total: N=249
Causes which may be potentially remediable by future investigators: Declined: N=48 Unable to be contacted: N=145 Total: N=193
Survivors eligible for ACOS N=406
Page 42 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 43
* Of 1001 FACTT subjects who underwent randomization, 227 were ineligible for long-term
follow-up as part of EA-PAC as no regulatory approval was in place and 119 declined consent (33). †
Subjects were categorized as ineligible if the time window to be tested had elapsed due to the regulatory halt, as incapable if self-determined or determined by a surrogate to be physically or mentally incapable of telephone-based neuropsychological testing, and as lost to follow-up if consent was obtained but the subject was not tested. Of 53 subjects categorized as lost to follow-up, no contact information was available for 1 subject, no telephone service was available for 1 subject, no explanation was provided for 1 subject, and the remaining 50 subjects were recorded as “lost to follow-up.” ‡
Of 52 subjects tested at 2 months, 32 were re-tested at 12 months. The reasons for 20 subjects being tested at 2 months but not at 12 months were that 11 patients were lost to follow-up, 5 declined, 3 died, and 1 was incarcerated. Subjects were not required to undergo testing at 2 months to be tested at 12 months.
Page 43 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS) 44
Figure 2.
Page 44 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
1
TITLE: THE ARDS COGNITIVE OUTCOMES STUDY (ACOS): LONG-
TERM NEUROPSYCHOLOGICAL FUNCTION IN ACUTE LUNG INJURY
SURVIVORS
Authors:
Mark E. Mikkelsen, M.D., M.S.1,2 *
Jason D. Christie, M.D., M.S.1,2 * Paul N. Lanken, M.D.1
Rosette C. Biester, Ph.D3
B. Taylor Thompson, M.D.4
Scarlett L. Bellamy, Sc.D.2
A. Russell Localio, Ph.D.2
Ejigayehu Demissie, M.S.N.1,2
Ramona O. Hopkins, Ph.D. 5, 6 Derek C. Angus, M.D., M.P.H. 7
* These authors contributed equally to this work
Institution: 1Pulmonary, Allergy, and Critical Care Division
Department of Medicine University of Pennsylvania School of Medicine
2Center for Clinical Epidemiology and Biostatistics University of Pennsylvania School of Medicine
3Department of Physical Medicine and Rehabilitation University of Pennsylvania School of Medicine Philadelphia Veterans Affairs Medical Center
4Pulmonary and Critical Care Unit, Department of Medicine Massachusetts General Hospital 5Department of Medicine, Pulmonary and Critical Care Division, Intermountain Medical Center 6 Psychology Department and Neuroscience Center, Brigham Young University 7CRISMA Center, Department of Critical Care Medicine and Department of Health Policy and Management University of Pittsburgh
Running Head: ARDS COGNITIVE OUTCOMES STUDY (ACOS) Descriptor: 4.2 ALI/ARDS: Diagnosis & Clinical Issues
Page 45 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
2
Online Data Supplement
Methods
The study was reviewed and approved by the Institutional Review Boards
of each participating hospital. It was also approved by the Natural History and
Steering Committees of the NIH National Heart, Lung, and Blood Institute
(NHLBI) Acute Respiratory Distress Syndrome Clinical Trials Network
(ARDSNet) in 2002.
Study Design
The ARDS Cognitive Outcomes Study (ACOS) is a prospective, multi-
center cohort study of survivors from the ARDSNet Fluid and Catheter Treatment
Trial (FACTT). FACTT enrolled patients from 38 North American hospitals
between June 2000 and October 2005. Between July 2002 and July 2003,
FACTT was halted and new regulatory approval related to the study was
prohibited. ACOS was coordinated and executed by investigators at the
University of Pennsylvania and University of Pittsburgh. The regulatory process
for ACOS began prior to the halt and testing was conducted between March
2003 and September 2006 in concert with the Economic Analysis of the
Pulmonary-Artery Catheter (EA-PAC) study as a planned long-term assessment
of neuropsychological function in FACTT survivors (E1). As a consequence of
the regulatory halt of FACTT, ACOS ran partially concurrent with FACTT.
Subjects gave informed consent for the telephone administration of
neuropsychological tests.
Page 46 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
3
Study Patients
To be eligible for ACOS, subjects had to be enrolled in FACTT and EA-
PAC (E1) and ACOS-specific regulatory approval had to be in place. FACTT
enrolled mechanically ventilated adults who met the American-European
Consensus Conference criteria for ALI (E2). In FACTT, subjects were assigned
at random to a conservative or liberal fluid management strategy (E3), and either
a central venous catheter or PAC (E4) in a two-by-two factorial design. Baseline
characteristics, including the presence of pre-existing dementia and site of
enrollment, and medical data were collected prospectively as part of FACTT. We
categorized the geographic region within the continental United States into one of
five categories (Northeast, South, Southwest, Midwest, and West) based on the
site of enrollment, consistent with prior studies (E5). On-study data, including
hemodynamic, respiratory, renal and metabolic variables, were collected and
recorded daily by the ARDS Network data coordinating center, as were
cumulative fluid balance, organ-failure-free day assessments, ICU length of stay,
and duration of mechanical ventilation (E3).
Cognitive and Psychiatric Function
A validated telephone battery of standardized neuropsychological tests
was administered to consenting, English-speaking subjects at 2 and 12 months
post-hospital discharge. Subjects were not required to undergo 2 month testing
to be tested at 12 months. The test administration call center was centralized at
the University of Pittsburgh. The telephone battery was administered using a
Page 47 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
4
detailed standardized script by two non-neuropsychologists at the University of
Pittsburgh who were blinded to group randomization. These two investigators
received formal training from neuropsychologists and were evaluated for
competence during the pilot interview stage prior to administering tests to
subjects. The details of formation and validation of the battery used in this study
have been presented previously (E6-8).
The following cognitive domains were assessed: vocabulary, reasoning,
memory, verbal fluency and executive function. Executive function is a set of
cognitive abilities that enable individuals to engage in purposeful, goal-directed
behaviors, cognitive flexibility, abstract thinking, initiate behavior and are
necessary for effective daily functioning. Memory, verbal fluency, and executive
function were hypothesized to be domains susceptible to impairment in ALI
survivors based on previous investigations in this population (E6, E8-E10).
Anxiety, depression, and post-traumatic stress disorder (PTSD) symptoms were
assessed using standardized measures (E11-14). Neuropsychological tests were
reviewed, scored, and standardized by neuropsychologists at the University of
Pennsylvania. Instruments used to assess each neuropsychological domain are
presented in Table E1 (E11-18). To minimize the effect of order presentation, the
tests were administered in random sequence (E6-E8).
Data Analysis
The cognitive battery yielded scaled scores for each domain which were
normalized to allow for comparisons across tests and subjects (E19-20). We
Page 48 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
5
report the median and interquartile range of results as percentiles. We defined
impairment in a single domain as a score > 2 SD below the population normative
data (E9-10, 21-22), a conservative definition of cognitive impairment that
represents significant deficits outside the normal range of cognitive function.
Cognitive impairment at the subject level was defined as impairment in memory,
verbal fluency, and/or executive function in subjects who completed tests in each
of these domains. We used the most conservative criteria to define impairment in
a single domain and limited our cognitive assessment a priori to three domains
shown to be affected in ALI survivors in previous studies (E6, E8-10) to minimize
the probability of a Type I error to an acceptable alpha level of < 0.05 (E22).
The Beck Anxiety Inventory and the Zung Self-Rating Depression Scale
are scored as none, mild, moderate and severe (E11-13). Patients with moderate
or severe anxiety or depression were classified as impaired similar to previous
studies (E6, E8, E21). The modified Post-traumatic Stress Syndrome 10-
Questions Inventory (PTSS-10) is scored as normal or impaired (E14).
Psychiatric impairment was defined as impairment in any, or multiple, of the three
psychiatric measures (anxiety, depression, and PTSD) in subjects completing
tests in each of these domains. We focused our study on survivors tested at
approximately 12 months post-discharge to assess long-term neuropsychological
function.
Based on prior studies, we a priori hypothesized that cognitive impairment
would be associated with duration of mechanical ventilation, either conservative
or liberal fluid-management strategy (E3), hypotension (E10), hypoxemia (E9),
Page 49 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
6
PAC use (E4, E23), sepsis as the primary cause of lung injury (E24-25), and
severity of illness (E26). PAC use was considered as a candidate risk factor
given its association with arrhythmias and the potential risk of paradoxical air
and/or microthrombotic embolism given the prevalence of moderate-to-large
patient foramen ovale shunting in patients with ARDS (E23, E27-E28). There
was no standardized delirium assessment in FACTT (E3-4) to permit adjusting
for duration of delirium, which was recently shown to be associated with long-
term cognitive impairment (E29-30). The pre-specified potential confounding
variables included: age, gender, race, history of heavy alcohol use or
cerebrovascular disease, level of education, the presence of concomitant
psychiatric impairment, hospital length of stay prior to enrollment, and the time to
testing (E6, E8-10, E21, E31-33).
We used baseline measures and daily measurements during the study
(“on-study” data) to explore our hypotheses. On-study data from FACTT were
summarized at the subject level as means to account for influential observations.
We used hemodynamic values (systolic blood pressure (SBP), vasopressor use,
cardiac index) and protocol assignment to shock cells from FACTT (E3-E4) to
explore the potential causative role of hypotension (E10) and central venous
pressure (CVP) to explore the potential role of fluid-management strategy.
Respiratory values (partial pressure of arterial oxygen, PaO2, partial pressure of
arterial oxygen to fraction of inspired oxygen, PaO2:FiO2, oxygenation index, and
oxygen saturation) were assessed to explore the potential causative role of
hypoxemia (E9). We used Acute Physiologic and Chronic Health Evaluation
Page 50 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
7
(APACHE) III scores and intensive care unit (ICU) length of stay for severity of
illness measures.
With the exception of the shock assessment, which was measured as
often as every 4 hours, and SBP and PaO2:FiO2, in which the worst values over
the preceding 24 hours were recorded to derive the Brussels organ failure score,
values were measured and recorded daily (measure closest to 8 am) during the
study.
In addition, serum sodium, bicarbonate, blood urea nitrogen, creatinine,
glucose (E34), organ-failure-free (cardiovascular, central nervous system, and
renal) days (E35), and cumulative furosemide and corticosteroid dose given their
potential anticholinergic activity (E36-37), were assessed in exploratory analyses
(see Table E5).
Based on prior studies and/or plausibility, we tested the following
candidate risk factors for the development of psychiatric morbidity: age (E38-
E40), gender (E38-41), race/ethnicity, level of education (E39, E42), APACHE III,
the trial interventions (fluid-management strategy, PAC), hypotension, hypoxemia
(E38-39), any episode of hypoglycemia during the hospitalization (E43),
corticosteroid administration (E43), ICU length of stay (E45-E46), and duration of
mechanical ventilation (E38, E45).
Comparisons between groups were made using Student’s t-test or
Wilcoxon’s rank-sum test for continuous variables and the chi-squared statistic or
Fisher’s exact test for categorical variables. In the presence of a significant
association, continuous measurements were categorized based on the
Page 51 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
8
distribution into quartiles to assess for dose-response effects. Quality of life was
assessed at 12 months post-discharge as part of the EA-PAC study (E1). Quality
of life was measured using the Health Utilities Index Mark 2 (E47).
Statistical Analysis:
Multivariable logistic regression was used to investigate the relationship
between candidate risk factors and long-term neuropsychological impairment
(cognitive impairment and psychiatric morbidity). We adjusted for each candidate
risk factor and potential covariates with an alpha level of significance < 0.20 in
univariate analyses (E48). Age and level of education were forced into the final
cognitive models to account for potential differences in pre-morbid cognitive
impairment. Time to testing and race were forced into the final cognitive models
to account for potential time and survival biases. To avoid over-fitting the model,
adjustment for potential confounding was performed one covariate at-a-time
(E49). Multivariable logistic regression was also used to investigate the
relationship between sociodemographic factors and consent to participate in a
study of long-term neuropsychological function. For all analyses, associations
were reported as an OR with 95% confidence intervals (CI). A standard two-
tailed p-value of ≤ 0.05 was used to signify statistical significance. Statistical
analyses were performed using Stata 10.0 software (Stata Datacorp, College
Station, TX).
The primary analysis was limited to 75 survivors who completed testing in
all three cognitive domains of interest at 12 months: memory, verbal fluency, and
Page 52 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
9
executive function. The Hayling Sentence Completion Test (HSCT) assesses
executive function with an error score and response latency component to
produce an overall score. The response times for the HSCT were not measured
before February, 2005 due to an error in the administration of the timing of the
test. This error effected 21 of 102 survivors (8 randomized to the liberal-strategy
group and 13 to the conservative-strategy group) at 12 months. In secondary
analyses, 90 survivors who completed assessments in memory, verbal fluency,
and the error score of the HSCT at 12 months were carried out.
Sensitivity Analyses:
We performed multiple sensitivity analyses to determine the effects of
missing data on the observed association between fluid-management strategy
and long-term cognitive impairment. To assess the potential effects of morbidity
and mortality post-consent, we assumed that all 31 subjects who died post-
consent or were classified as incapable to have the tests administered were
impaired. To assess the potential effects of loss to follow-up post-consent, we
first assumed that all 50 survivors reported as lost to follow-up were impaired,
then we assumed that all 50 survivors reported as lost to follow-up were not
impaired, and finally we assumed that impairment in those lost to follow-up was
similar to the 55% incidence observed for the full cohort. To assess the potential
effects of the 25 survivors who refused testing, we performed separate analyses
using these same three assumptions. Finally, to gauge the potential effects of
incomplete cognitive assessments on the associations identified in the primary
Page 53 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
10
analysis, we assumed that all 27 survivors without a complete cognitive
assessment were impaired, and then assumed that survivors without a complete
cognitive assessment were not impaired. To minimize the assumptions of the
latter scenario, survivors were categorized as impaired if the subject was
impaired in a tested domain.
Results
Association between Risk Factors and Cognitive Domain Performance:
Lower PaO2 values correlated with worse executive function (rho=0.24,
p=0.05), but not verbal fluency (rho=0.16, p=0.14) or memory (rho=0.14, p=0.20).
Similarly, lower central venous pressures correlated with worse executive
function (rho=0.28, p=0.02), but not verbal fluency (rho= -0.07, p=0.47) or
memory (rho=0.14, p=0.20). Enrollment in the conservative fluid-strategy group
correlated with worse executive function (rho= -0.39, p<0.001), but not verbal
fluency (rho= -0.01, p=0.89) or memory (rho= -0.12, p=0.25).
Association between Risk Factors and Anxiety, Depression, and PTSD:
Lower PaO2 values were associated with anxiety (p=0.05), as were lower systolic
blood pressures (p=0.04). Neither lower PaO2 values, nor lower systolic blood
pressures, were found to be associated with depression or PTSD. An episode of
hypoglycemia was associated with anxiety at 12 months (p=0.01), but not
depression (p=0.28), or PTSD (p=0.31).
Page 54 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
11
Sensitivity Analyses:
Given the potential bias due to the effects of dropouts, we performed
several sensitivity analyses. Under the assumption that all 31 subjects who
consented for ACOS but died before testing (N=22) or were classified as
incapable of test performance (N=9) were impaired (Figure 1), the association
between conservative fluid-management strategy and long-term cognitive
impairment remained significant (N=106, OR=3.48, 95% CI: 1.48, 8.16, p=0.004).
The association also persisted if we assumed that the 50 survivors lost to follow-
up post-consent were all impaired (N=125, OR=2.92, 95% CI: 1.28, 6.61,
p=0.01), were all not impaired (N=125, OR=2.45, 95% CI: 1.14, 5.28, p=0.02), or
were impaired to a similar degree (55% incidence) as the overall cohort of long-
term survivors (N=125, OR=2.24, 95%CI: 1.10, 4.59, p=0.03). The association
also persisted if we assumed that the 25 patients who refused after initially
consenting were all impaired (N=100, OR=2.51, 95% CI: 1.05, 5.97, p=0.04),
were all not impaired (N=100, OR=3.76, 95% CI: 1.62, 8.72, p=0.002), or were
impaired to a similar degree (55% incidence) as the overall cohort of long-term
survivors (N=100, OR=2.78, 95% CI: 1.23, 6.31, p=0.01).
Assuming that survivors with an incomplete cognitive assessment were
not impaired, we found the association between the conservative fluid
management strategy and long-term cognitive impairment remained (N=102,
OR=2.76, 95% CI: 1.22, 6.21, p=0.014); as did the association between lower
PaO2 values and long-term cognitive impairment (N=93, OR=1.36, 95% CI: 1.03,
1.81, p=0.033). Under the assumption that survivors with an incomplete cognitive
Page 55 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
12
assessment were impaired, we observed an association similar to the unadjusted
association between the conservative-strategy group and long-term cognitive
impairment (N=102, OR=4.09, 95% CI: 1.70, 9.83, p=0.002). The association
between lower PaO2 values and long-term cognitive impairment was no longer
significant (N=93, OR=1.26, 95% CI: 0.95, 1.66, p=0.10).
Page 56 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
13
References
E1) Clermont G, Kong L, Weissfeld LA, Lave JR, Rubenfeld GD, Robertss MS,
Connors AF, Bernard GR, Thompson BT, Wheeler AP, Angus DC. The effect of
pulmonary artery catheter use on costs and long-term outcomes of acute lung
injury. PLoS ONE 2011; 6(7): e22512.
E2) Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M,
Legall JR, Morris A, Spragg R. The American-European consensus conference
on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial
coordination. Am J Respir Crit Care Med 1994; 149: 818–824
E3) The National Heart, Lung, and Blood Institute Acute Respiratory Distress
Syndrome (ARDS) Clinical Trials Network. Comparison of two fluid management
strategies in acute lung injury. N Engl J Med 2006; 354(24): 2564-75
E4) The National Heart, Lung, and Blood Institute Acute Respiratory Distress
Syndrome (ARDS) Clinical Trials Network. Pulmonary-artery versus central
venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:
2213-24
E5) Chan PS, Nichol G, Krumholz HM, Spertus JA, Jones PG, Peterson ED,
Rathore SS, Nallamothu BK, for the American Heart Association National
Registry of Cardiopulmonary Resuscitation (NRCPR) Investigators. Racial
differences in survivors after in-hospital cardiac arrest. JAMA 2009; 302(11):
1195-1201
E6) Christie JD, Biester R, Taichman DB, Shull WH, Hansen-Flaschen J, Shea
JA, Hopkins RO. Formation and validation of a telephone battery to assess
Page 57 of 79
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
14
cognitive function in acute respiratory distress syndrome survivors. J Crit Care
2006; 21:125-132
E7) Taichman DB, Christie J, Biester R, Mortensen J, White J, Kaplan S,
Hansen-Flaschen J, Palevsky HI, Elliott CG, Hopkins RO. Validation of a brief
telephone battery for cognitive assessment of patients with pulmonary arterial
hypertension. Respir Res 2005; 6: 39
E8) Mikkelsen ME, Shull WH, Biester RC, Taichman DB, Lynch S, Demissie E,
Hansen-Flaschen J, Christie JD. Cognitive, mood and quality of life impairments
in a select population of ARDS survivors. Respirology 2009; 14: 76-82
E9) Hopkins R, Weaver L, Pope D, Orme J, Bigler E, Larson-Lohr V.
Neuropsychological sequelae and impaired health status in survivors of severe
acute respiratory distress syndrome. Am J Respir Crit Care Med 1999; 160:50-6
E10) Hopkins RO, Weaver LK, Collingridge D, Parkinson RB, Chan KJ, Orme
JF. Two-year cognitive, emotional, and quality-of-life outcomes in acute
respiratory distress syndrome. Am J Respir Crit Care Med 2005; 171:340-347
E11) Zung WK. A self-rating depression scale. Arch Gen Psych 1965; 12:63-70
E12) Biggs JT, Wylie LT, Ziegler VE. Validity of the Zung self-rating depression
scale. British J Psych 1978; 132: 381-385
E13) Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical
anxiety: psychometric properties. J Cons Clin Psychol 1998; 56:893-7
E14) Weisaeth L. Torture of a Norwegian ship’s crew: the torture, stress
reactions and psychiatric aftereffects. Acta Psychiatr Scand Suppl 1989; 355: 63-
72
Page 58 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
15
E15) Wechsler D, ed. Wechsler Adult Intelligence Scale, Third edition. San
Antonio: The Psychological Corporation; 1997
E16) Wechsler D. Wechsler Memory Scale. San Antonio: The Psychology
Corporation, 1997
E17) Lezak MD. Neuropsychological Assessment. New York: Oxford University
Press, 1995
E18) Burgess PW, Shallice T. The Hayling and Brixton Tests. London, England:
Thames Valley Test Company Limited, 2007
E19) Heaton RK, Grant I, Matthews CG. Comprehensive norms for an
expanded Halstead-Reitan Battery: demographic corrections, research findings
and clinical applications. Psychological Assessment Resources, Inc., Odessa,
1991
E20) Heaton RK. Comprehensive norms for an expanded Halstead-Reitan
Battery: A supplement for the WAIS-R. Psychological Assessment Resources,
Inc., Odessa, 1994
E21) Hopkins RO, Weaver LK, Chan KJ, Orme JF. Quality of life, emotional, and
cognitive function following acute respiratory distress syndrome. J Int
Neuropsychol Soc 2004; 10:1005-1017
E22) Ingraham LJ, Aiken CB. An empirical approach to determining criteria for
abnormality in test batteries with multiple measures. Neuropsychology 1996;
10:120-124
Page 59 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
16
E23) Boyd KD, Thomas SJ, Boyd AD. A prospective study of complications of
pulmonary artery catheterizations in 500 consecutive patients. Chest 1983; 84:
245-249
E24) Reichenberg A, Yirmiya R, Schuld A, Kraus T, Haack M, Morag A,
Pollmächer T. Cytokine-associated emotional and cognitive disturbances in
humans. Arch Gen Psychiatry 2001; 58: 445-452
E25) Patarca-Montero R, Antoni M, Fletcher MA, Klimas NG. Cytokine and other
immunologic markers in chronic fatigue syndrome and their relation to
neuropsychological factors. Appl Neuropsychol 2001; 8: 51-64
E26) Jones C, Griffiths RD, Slater T, Benjamin KS, Wilson S. Significant
cognitive dysfunction in non-delirious patients identified during and persisting
following critical illness. Intensive Care Med 2006; 32: 923-926
E27) Doblar DD, Hinckle JC, Fay ML, Condon BF. Air embolism associated with
pulmonary artery catheter introducer kit. Anesthesiology 1982; 56: 307-309
E28) Mekontso Dessap A, Boissier F, Leon R, Carreira S, Campo FR, Lemaire
F, Brochard L. Prevalence and prognosis of shunting across patient foramen
ovale during acute respiratory distress syndrome. Crit Care Med 2010; 38(9):
1786-92
E29) Girard TD, Jackson JC, Pandharipande PP, Pun BT, Thompson JL,
Shintani AK, Gordon SM, Canonico AE, Dittus RS, Bernard GR, Ely EW.
Delirium as a predictor of long-term cognitive impairment in survivors of critical
illness. Crit Care Med 2010; 38(7): 1513-20
Page 60 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
17
E30) Van den Boogard M, Schoonhoven L, Evers AW, van der Hoeven JG, van
Achterberg TV, Pickkers P. Delirium in critically ill patients: impact on long-term
health-related quality of life and cognitive functioning. Crit Care Med 2012; 40(1):
112-118
E31) Ngandu T, von Strauss E, Helkala EL, Winblad B, Nissinen A, Tuomilehto
J, Soininen H, Kivipelto M. Education and dementia: what lies behind the
association ? Neurology 2007; 69: 1442-1450
E32) Richards PM, Ruff RM. Motivational effects on neuropsychological
functioning: comparison of depressed versus nondepressed individuals. J
Consult Clin Psychol 1989; 57: 396-402
E33) Buckelew SP, Hannay HJ. Relationships among anxiety, defensiveness,
sex, task difficulty and performance on various neuropsychological tasks.
Percept Mot Skills 1986; 63: 711-718
E34) Hopkins RO, Suchyta MR, Snow GL, Jephson A, Weaver LK, Orme JF.
Blood glucose dysregulation and cognitive outcomes in ARDS survivors. Brain Inj
2010; 24(12): 1478-84
E35) Schoenfeld DA, Bernard GR. Statistical evaluation of ventilator-free days as
an efficacy measure in clinical trials of treatments for acute respiratory distress
syndrome. Crit Care Med 2002; 30: 1772-1777
E36) Milbrandt EB, Angus DC. Bench-to-bedside review: Critical-illness
associated cognitive dysfunction – mechanisms, markers, and emerging
therapeutics. Critical Care 2006; 10: 238
Page 61 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
18
E37) Mulsant BH, Pollock BG, Kirshner M, Shen C, Dodge H, Ganguli M. Serum
anticholinergic activity in a community-based sample of older adults: relationship
with cognitive performance. Arch Gen Psychiatry 2003; 60: 198 – 203
E38) Hopkins RO, Key CW, Suchyta DO, Weaver LK, Orme JF. Risk factors for
depression and anxiety in survivors of acute respiratory distress syndrome. Gen
Hosp Psych 2010; 32: 147-155
E39) Desai S, Lawa TJ, Needham DM. Long-term complications of critical care.
Crit Care Med 2011; 39(2): 371-379
E40) Davydow DS, Gifford JM, Desai SV, Needham DM, Bienvenu OJ.
Posttraumatic stress disorder in general intensive care unit survivors: a
systematic review. Gen Hosp Psych 2008; 30: 421-434
E41) Davydow DS, Gifford JM, Desai SV, Bienvenu OJ, Needham DM.
Depression in general intensive care unit survivors: a systematic review. Int Care
Med 2009; 35: 796-809
E42) Dowdy DW, Bienvenu OJ, Dinglas V, Mendez-Tellez PA, Sevransky J,
Shanholtz C, Needham DM. Are intensive care factors associated with
depressive symptoms six months after acute lung injury? Crit Care Med 2009;
37: 1702-1707
E43) Dowdy DW, Dinglas V, Mendez-Tellez PA, Bienvenu OJ, Sevransky J,
Dennison CR, Shanholtz C, Needham DM. Intensive care unit hypoglycemia
predicts depression during early recovery from acute lung injury. Crit Care Med
2008; 36: 2726-2733
Page 62 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
19
E44) Schelling G, Stoll C, Kapfhammer HP, Rothenhausler HB, Krauseneck T,
Durst K, Haller M, Briegel J. The effect of stress doses of hydrocortisone during
septic shock on posttraumatic stress disorder and health-related quality of life in
survivors. Crit Care Med 1999; 27: 2678-2683
E45) Nelson BJ, Weinert CR, Burly CL, Marinelli WA, Gross CR. Intensive care
unit drug use and subsequent quality of life in acute lung injury patients. Crit Care
Med 2000; 28(11): 3626-30
E46) Kapfhammer HP, Rothenhausler HB, Krauseneck T, Stoll C, Schelling G.
Posttraumatic stress disorder and health-related quality of life in long-term
survivors of acute respiratory distress syndrome. Am J Psych 2004; 161(1): 45-
52
E47) Torrance GW, Feeny DH, Furlong WJ, Barr RD, Zhang Y, Wang Q. Multi-
attribute preference functions for a comprehensive health status classification
system: Health utilities index Mark 2. Medical Care 1996; 34(7): 702-722
E48) Maldonado G, Greenland S. Simulation study of confounder-selection
strategies. Amer J of Epid 1993; 138:923-936
E49) Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation
study of the number of events per variable in logistic regression analysis. J Clin
Epidemiol 1996; 49: 1373-1379
Page 63 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
20
Figure E1. Enrollment and outcomes by fluid-management strategy.
Abbreviations: ACOS=ARDS Cognitive Outcomes Study
Page 64 of 79

For Review Only
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
21
Table E1. Outcomes measured in the neuropsychological test battery and cognitive domain performance at 12 months. Cognitive domains are listed by increasing prevalence of impairment in the 102 long-term ALI survivors.
Cognitive Domain
Instrument
No.
Percentile
Vocabulary *
WAIS-III: Vocabulary E14 98 25 (9 – 50)
Reasoning *
WAIS – III: Similarities E14 98 37 (16 – 63)
Memory † WMS – III: Logical Memory I E15
92 37 (5 – 63)
Verbal Fluency †
Controlled Oral Word Association Test E16
96 19 (4 – 34)
Executive Functioning †
Hayling Sentence Completion Test
(HSCT) E17 76 5 (<1 – 25)
Psychiatric Domain
Instrument
Anxiety
Beck Anxiety Inventory E12 102
Depression
Zung Self-Rating Depression Scale E10-E11 102
Post-traumatic stress disorder
Post-traumatic Stress Syndrome 10-Questions Inventory E13
102
Definition of abbreviation: HSCT=Hayling Sentence Completion Test; WAIS-III=Wechsler Adult Intelligence Scale-III; WMS-III: Wechsler Memory Scale-III. * Domain a priori hypothesized to be resilient to effects of acute lung injury. †
Domain a priori hypothesized to be susceptible to effects of acute lung injury. ‡
The error score of the HSCT was completed in 100 long-term survivors.
Page 65 of 79

For Review Only
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
22
Individual cognitive domain performance expressed as percentiles based on normative data.
Page 66 of 79

For Review Only
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
23
Table E2. Patient characteristics and consent to participate in a study to assess long-term neuropsychological outcomes.
Variable* Consent Rate † p-value Adjusted Odds Ratio
(95% CI) ‡
p-value
Age, years (%) Age < 39 Age 40 – 48 Age 49 – 59 Age ≥ 60
47/156 (30) 65/162 (40) 58/166 (35) 43/171 (25)
0.02
Reference
1.59 (0.93 – 2.69) 1.28 (0.75 – 2.18) 1.23 (0.70 – 2.19)
Reference
0.09 0.37 0.47
Gender (%) Female sex Male sex
114/308 (37) 99/347 (28)
0.02
Reference 0.75 (0.52 – 1.11)
Reference
0.15
Race or ethnic group (%) White non-Hispanic Black non-Hispanic Hispanic § Other §
166/446 (37) 34/136 (25) 12/60 (20)
1/13 (8)
0.001
Reference
0.73 (0.44 – 1.22) 0.55 (0.26 – 1.13)
Reference 0.23 0.10
United States geographic region (%) Northeast Southeast Southwest Midwest West
49/128 (38) 70/192 (36) 22/124 (18) 32/83 (38)
40/128 (31)
0.001
Reference 1.78 (0.90 – 3.55) 0.64 (0.32 – 1.25) 1.28 (0.74 – 2.21) 1.62 (0.90 – 2.93)
Reference
0.10 0.19 0.37 0.11
* Sociodemographic and hospital-level information in those 655 subjects who consented to long-term follow-up as part of EA-PAC (E1). Age was categorized into quartiles based on the observed distribution. † Of 442 subjects who consented to EA-PAC, but not ACOS, 194 died between EA-PAC consent and completion of long-term follow-up, 55 were
ineligible as the time window to be tested had elapsed due to the regulatory halt, 48 declined, and the remaining 145 were categorized as “not consented.”
‡ Adjusted for each variable and whether patient died during long-term follow-up after excluding the 55 ineligible subjects.
§ Hispanic and other race/ethnicity were collapsed into one group in the multivariable logistic regression model.
Page 67 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
24
Table E3. Characteristics of long-term survivors with complete cognitive testing, by fluid-management strategy.
Liberal (N=37)
Conservative (N=38)
p-value
Age, years 53 (43 – 60) 50 (47 – 56) 0.75
Male sex (%) 43 42 0.92
Race or ethnic group (%) White non-Hispanic Black non-Hispanic Hispanic
92 8 0
89 8 3
1.00
Level of education, years
12 (12 – 16) 12 (12 – 16) 0.43
Time from enrollment to testing, months
13 (12 – 13) 12 (12 – 14) 0.64
Time from discharge to testing, months
12 (11 – 13) 12 (11 – 13) 0.97
Previously Tested 24 37 0.24
Primary lung injury (%) Pneumonia Sepsis Aspiration Trauma Multiple transfusions Other
30 30 11 5 5
19
42 18 16 16 3 5
0.20
Coexisting conditions (%)*
Diabetes HIV infection or AIDS Cirrhosis Solid tumors Leukemia Lymphoma Immunosuppression
16 0 5 0 0 5 8
19 0 3 3 3 0 11
0.76
– 1.00 1.00 1.00 0.49 1.00
Medical ICU (%) 59 53 0.87
APACHE III †
90 (64 – 107) 65 (58 – 89) 0.04
Glasgow Coma Scale 7 (3 – 11) 8 (7 – 11) 0.44
Mean arterial pressure, mm Hg
* 74 (66 – 84) 77 (65 – 86) 0.68
Met shock criteria at baseline (%) 46 39 0.57
Vasopressor use at baseline (%) 43 32 0.30
Pre-randomization fluid balance, mL
†
1869 (522 – 5564)
1261 (450 – 3744)
0.29
PaO2:FiO2 ‡ 120 (87 – 162) 124 (80 – 180) 0.61
Page 68 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
25
PaO2
¶ 80 (67 – 105) 82 (67 – 97) 0.81
Pulmonary artery catheter (%) 62 53 0.40
Definition of abbreviation: HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome; ICU=intensive care unit; APACHE III= Acute Physiologic and Chronic Health Evaluation III scores; PaO2:FiO2=ratio of partial pressure of arterial oxygen to fraction of inspired oxygen. Values expressed as a percentage or median (interquartile range). * Measured in 74 survivors;
† measured in 73 survivors;
‡ measured in 71 survivors;
¶ measured in
72 survivors. Shock at baseline present if mean arterial pressure < 60 at baseline or vasoactive agent administered.
Page 69 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
26
Table E4. On-study physiologic variables and outcomes of long-term survivors with complete cognitive testing, by fluid-management strategy.
Fluid-Management Strategy
Liberal
(N=37)
Conservative
(N=38) p-value
Hemodynamic variables
Systolic Blood Pressure (mm Hg) * 108 (102 – 114) 102 (96 – 112) 0.11
Cardiac index (liters/min/m2)
† 4.8 (4.2 – 5.5) 4.2 (3.3 – 4.7) 0.06
CVP (mm Hg) 12.0 (10.4 – 13.8) 9.4 (6.6 – 11) <0.001
CVP < 8 mm Hg (1st quartile) (%)
CVP 8 – 12 mm Hg
CVP > 12 mm Hg (4th quartile)
16
43
40
37
50
13
0.015
Shock ‡
(%)
Vasopressor use (%)
Ineffective circulation (%)
27
19
16
34
32
8
0.50
0.21
0.31
Fluid balance (cumulative over 7 days,
mL) 1659
(-4236 – 6244) -2706
(-7970 – -336) 0.02
Respiratory variables
PaO2:FiO2 158 (128 – 191) 156 (133 – 191) 0.60
Oxygenation index 7.50 (5.11 – 10.3) 7.30 (5.16 – 10.05) 0.94
PaO2 79 (70 – 97) 72 (68 – 84) 0.14
PaCO2 43 (35 – 46) 42 (36 – 48) 0.59
PEEP 7 (6.2 – 8.4) 6.9 (5 – 8) 0.39
Oxygen saturation (%) 95 (92.8 – 96.6) 94.5 (92.7 – 96) 0.54
pH 7.41 (7.37 – 7.44) 7.44 (7.40 – 7.45) 0.01
ICU length of stay (days) 12 (9 – 18) 9 (7 – 13) 0.07
Duration of mechanical ventilation
(days) 8.5 (4.5 – 12) 6 (4 – 9) 0.04
Glasgow coma scale ‡ 11 (11 – 12) 12 (10 – 14) 0.59
Renal and metabolic variables
Sodium 140 (139 – 143) 142 (139 – 144) 0.32
Blood urea nitrogen (mg/dL) 17.8 (15.7 – 31.6) 22.4 (17.0 – 32.8) 0.32
Creatinine (mg/dl) 0.98 (0.77 – 1.16) 0.92 (0.68 – 1.24) 0.63
Bicarbonate (mmol/L) 25.8 (24.0 – 28.9) 27.4 (23.0 – 32.2) 0.15
Glucose (mg/dL) 118 (110 – 144) 121 (108 – 134) 0.44
Page 70 of 79
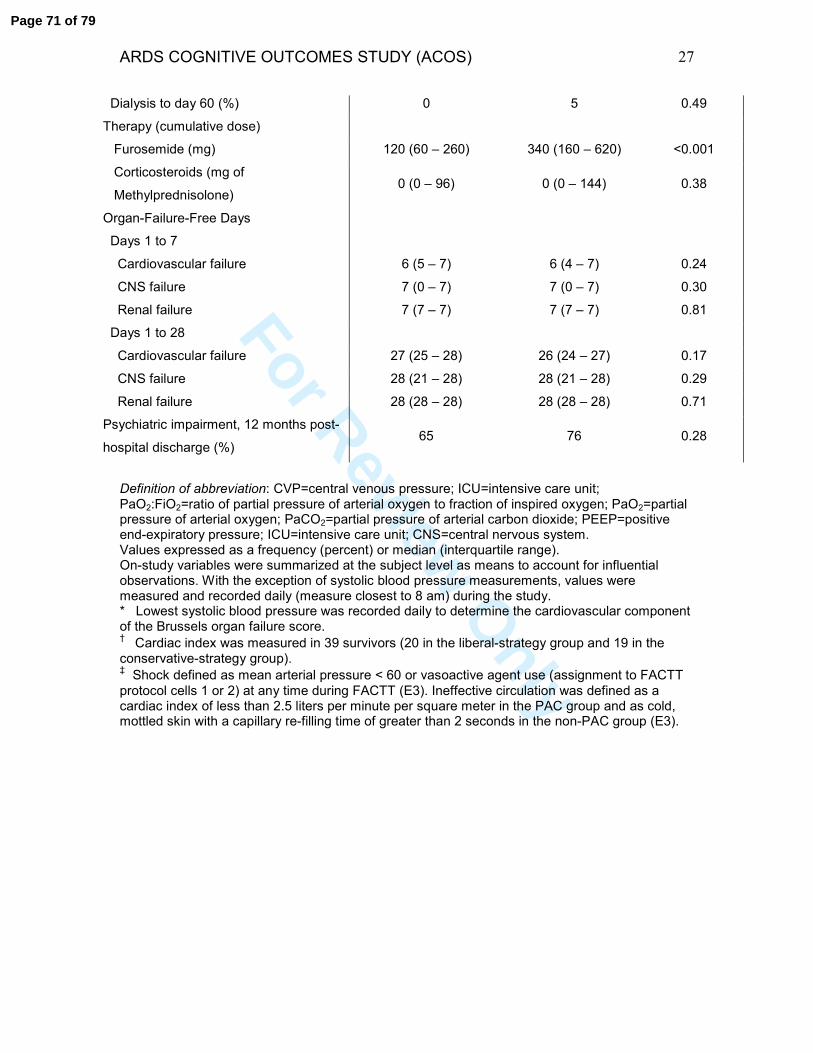
For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
27
Dialysis to day 60 (%) 0 5 0.49
Therapy (cumulative dose)
Furosemide (mg) 120 (60 – 260) 340 (160 – 620) <0.001
Corticosteroids (mg of
Methylprednisolone) 0 (0 – 96) 0 (0 – 144) 0.38
Organ-Failure-Free Days
Days 1 to 7
Cardiovascular failure 6 (5 – 7) 6 (4 – 7) 0.24
CNS failure 7 (0 – 7) 7 (0 – 7) 0.30
Renal failure 7 (7 – 7) 7 (7 – 7) 0.81
Days 1 to 28
Cardiovascular failure 27 (25 – 28) 26 (24 – 27) 0.17
CNS failure 28 (21 – 28) 28 (21 – 28) 0.29
Renal failure 28 (28 – 28) 28 (28 – 28) 0.71
Psychiatric impairment, 12 months post-
hospital discharge (%) 65 76 0.28
Definition of abbreviation: CVP=central venous pressure; ICU=intensive care unit; PaO2:FiO2=ratio of partial pressure of arterial oxygen to fraction of inspired oxygen; PaO2=partial pressure of arterial oxygen; PaCO2=partial pressure of arterial carbon dioxide; PEEP=positive end-expiratory pressure; ICU=intensive care unit; CNS=central nervous system. Values expressed as a frequency (percent) or median (interquartile range). On-study variables were summarized at the subject level as means to account for influential observations. With the exception of systolic blood pressure measurements, values were measured and recorded daily (measure closest to 8 am) during the study. * Lowest systolic blood pressure was recorded daily to determine the cardiovascular component of the Brussels organ failure score. †
Cardiac index was measured in 39 survivors (20 in the liberal-strategy group and 19 in the conservative-strategy group). ‡
Shock defined as mean arterial pressure < 60 or vasoactive agent use (assignment to FACTT
protocol cells 1 or 2) at any time during FACTT (E3). Ineffective circulation was defined as a cardiac index of less than 2.5 liters per minute per square meter in the PAC group and as cold, mottled skin with a capillary re-filling time of greater than 2 seconds in the non-PAC group (E3).
Page 71 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
28
Table E5. Associations with long-term cognitive impairment in ALI survivors. Cognitive impairment at the subject level was defined as impairment in memory, verbal fluency, and/or executive function in the 75 subjects who completed tests in each of these domains.
Cognitive Impairment
Not Impaired
(n=34) Impaired (n=41)
p-value
Baseline characteristics
Age, years 50 (43 – 58) 51 (45 – 60) 0.51
Male sex (%) 32 51 0.10
Race or ethnic group (%) White Black Hispanic
91 6 3
90 10 0
0.53
Level of education, years
13 (12 – 16) 12 (12 – 15) 0.36
Hospital length of stay prior to enrollment, days
2 (1 – 3) 3 (1 – 4) 0.22
ARDS at enrollment 88 90 1.00
Primary lung injury (%) Pneumonia Sepsis Aspiration Trauma Multiple transfusions Other
24 29 9 12 6 21
46 20 17 10 2 5
0.10
Coexisting conditions (%) Diabetes HIV infection or AIDS Cirrhosis Solid tumors Leukemia Lymphoma Immunosuppression Heavy alcohol use Cerebrovascular disease
18 0 0 0 3 6 9 3 0
17 0 7 2 0 0
10 13 2
1.00
– 0.25 1.00 0.45 0.20 1.00 0.21 1.00
Medical ICU (%) 59 54 0.56
APACHE III
87 (60 – 106) 72 (60 – 94) 0.42
Glasgow Coma Scale 8 (6 – 9) 8 (6 – 11) 0.39
Mean arterial pressure, mm Hg
80 (72 – 87) 72 (62 – 84) 0.12
Met shock criteria * (%) 44 41 0.82
Vasopressor use (%) 44 32 0.27
Pre-randomization fluid balance, mL
2109 (450 – 5189)
1437 (679 – 3744)
0.44
Page 72 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
29
PaO2:FiO2 122 (76 – 170) 126 (87 – 166) 0.75
PaO2 81 (66 – 104) 81 (67 – 99) 0.97
Conservative strategy (%) 32 66 0.004
Pulmonary artery catheter (%) 53 61 0.48
On-study variables
Hemodynamic variables
Systolic Blood Pressure (mm Hg) † 108 (102 – 113) 104 (96 – 112) 0.32
Cardiac index (liters/min/m2)
‡ 4.5 (3.8 – 5.3) 4.5 (3.7 – 5.0) 0.49
CVP (mm Hg) 11.0 (8.7 – 12.7) 9.7 (6.6 – 12.0) 0.038
CVP < 8 mm Hg (1st quartile) (%)
CVP 8 – 12 mm Hg CVP > 12 mm Hg (4
th quartile)
12 53 35
39 41.5 19.5
0.02
Shock * (%) Vasopressor use Ineffective circulation *
32 26 9
29 24 15
0.77 0.84 0.50
Fluid balance (cumulative over 7 days, mL)
-2352 (-5236 – 3598)
-503 (-4236 – 5698)
0.24
Respiratory variables
PaO2:FiO2§ 152 (132 – 192) 157 (133 – 190) 0.63
Oxygenation index 7.38 (4.55 – 10.42) 7.67 (5.97 – 10.02) 0.57
PaO2 86 (70 – 98) 71 (67 – 80) 0.02
PaO2 < 68 (1st quartile) (%)
PaO2 68 – 93 PaO2 > 93 (4
th quartile)
13 50 37
27 65 8
0.014
PaCO2 43 (36 – 47) 42 (35 – 48) 0.96
PEEP 7 (5 – 9) 7 (6 – 7.8) 0.84
Oxygen saturation (%) 95.1 (93.3 – 96.8) 94.2 (92.6 – 95.8) 0.10
pH 7.42 (7.38 – 7.44) 7.43 (7.40 – 7.45) 0.27
ICU length of stay (days) 11 (8 – 18) 10 (7 – 16) 0.65
Duration of mechanical ventilation (days)
8 (4 – 11) 6 (4 – 9) 0.43
Glasgow coma scale 11 (11 – 13) 12 (11 – 14) 0.66
Renal and metabolic variables
Sodium 141 (139 – 144) 142 (139 – 144) 0.49
Blood urea nitrogen (mg/dL) 20.6 (15.7 – 32.8) 19.8 (15.7 – 31.6) 0.94
Creatinine (mg/dl) 0.98 (0.69 – 1.24) 0.86 (0.70 – 1.14) 0.36
Bicarbonate (mmol/L) 26.6 (24.1 – 29.6) 25.9 (23.0 – 30.4) 0.95
Glucose (mg/dL) 124 (110 – 138) 118 (108 – 135) 0.74
Hypoglycemia, < 60 mg/dL (%) 6 12 0.45
Hyperglycemia, > 180 mg/dL (%) 26 37 0.35
Page 73 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
30
Dialysis to day 60 (%) 0 5 0.50
Therapy (cumulative dose)
Furosemide (mg) 200 (120 – 420) 200 (80 – 440) 0.62
Corticosteroids (mg of Methylprednisolone)
0 (0 – 144) 0 (0 – 136) 0.80
Organ-Failure-Free Days
Days 1 to 7
Cardiovascular failure 6 (5 – 7) 6 (4 – 7) 0.98
CNS failure 7 (0 – 7) 7 (0 – 7) 0.82
Renal failure 7 (7 – 7) 7 (7 – 7) 0.25
Days 1 to 28
Cardiovascular failure 26 (24 – 28) 27 (24 – 27) 0.97
CNS failure 28 (21 – 28) 28 (21 – 28) 0.59
Renal failure 28 (28 – 28) 28 (28 – 28) 0.79
Time from enrollment to testing, months
13 (12 – 13) 12 (12 – 14) 0.53
Time from discharge to testing, months
12 (11 – 13) 12 (11 – 13) 0.51
Previously Tested (%) 38 24 0.20 Neuropsychiatric impairment, 1 year (%)
59 80 0.04
Definition of abbreviation: HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome;ARDS=acute respiratory distress syndrome (PaO2:FiO2 ≤ 200); ICU=intensive care unit; APACHE III= Acute Physiologic and Chronic Health Evaluation III scores; PaO2:FiO2=ratio of partial pressure of arterial oxygen to fraction of inspired oxygen; CVP=central venous pressure; ICU=intensive care unit; PaO2=partial pressure of arterial oxygen; PaCO2=partial pressure of arterial carbon dioxide; PEEP=positive end-expiratory pressure; ICU=intensive care unit; CNS=central nervous system. Values expressed as a frequency (percent) or median (interquartile range). On-study variables were summarized at the subject level as means to account for influential observations. With the exception of systolic blood pressure measurements, values were measured and recorded daily (measure closest to 8 am) during the study. Hypo- and hyperglycemia were defined as any episode of serum glucose < 60 mg/dL or > 180 mg/dL, respectively, during the hospitalization. * Shock defined as mean arterial pressure < 60 or vasoactive agent use (assignment to FACTT protocol cells 1 or 2) at any time during FACTT (E3). Ineffective circulation was defined as a cardiac index of less than 2.5 liters per minute per square meter in the PAC group and as cold, mottled skin with a capillary re-filling time of greater than 2 seconds in the non-PAC group (E4). †
Lowest systolic blood pressure was recorded daily to determine the cardiovascular component of the Brussels organ failure score. ‡
Cardiac index was measured in 39 survivors (20 in the liberal-strategy group and 19 in the conservative-strategy group). §
Using mean PaO2:FiO2 on-study to categorize subjects as ALI or ARDS, 77% met criteria for
ARDS (PaO2:FiO2 ≤ 200), 23% met criteria for ALI, and there was no association with cognitive impairment (p=0.82).
Page 74 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
31
Table E6. Association between identified candidate risk factors and long-term cognitive impairment, adjusted for each potential covariate, one covariate at-a-time.* Cognitive impairment at the subject level was defined as impairment in memory, verbal fluency, and/or executive function in the 75 subjects who completed tests in each of these domains.
Hypoxemia Logistic Regression Model
Total N in Model
Odds Ratio (95% CI) p-value
PaO2 (base model) † ‡ § 67 1.56 (1.09 – 2.24) 0.015 Adjusted for: Age
67 1.57 (1.08 – 2.28) 0.017
Gender 67 1.53 (1.07 – 2.20) 0.021 Race 67 1.52 (1.05 – 2.19) 0.026 Level of education 67 1.57 (1.09 – 2.25) 0.015 Time to testing 67 1.56 (1.09 – 2.24) 0.015 Psychiatric impairment 67 1.49 (1.03 – 2.16) 0.033 Mean arterial pressure (baseline) 66 1.51 (1.05 – 2.18) 0.028 Vasopressor use (baseline) 67 1.57 (1.06 – 2.32) 0.023 Vasopressor use ‡ 67 1.68 (1.14 – 2.49) 0.009 Central venous pressure ‡ 67 1.60 (1.11 – 2.32) 0.012 Primary lung injury 67 1.51 (1.01 – 2.26) 0.043 Conservative fluid-management 67 1.48 (1.02 – 2.15) 0.037
Fluid-Management Logistic Regression Model
Total N in Model
Odds Ratio (95% CI) p-value
Conservative fluid-management strategy (base model)
75 4.03 (1.53 – 10.59) 0.005
Adjusted for: Age
75 4.15 (1.56 – 11.00) 0.004
Gender 75 4.36 (1.60 – 11.85) 0.004 Race 75 4.47 (1.66 – 12.01) 0.003 History of heavy alcohol use † 72 5.46 (1.92 – 15.53) 0.001 History of cerebrovascular disease † 73 4.78 (1.77 – 12.91) 0.002 Level of education 75 4.45 (1.64 – 12.07) 0.003 Time to testing 75 4.00 (1.52 – 10.53) 0.005 Psychiatric impairment 75 3.84 (1.43 – 10.31) 0.008 Mean arterial pressure (baseline) † 74 4.88 (1.76 – 13.58) 0.002 Vasopressor use (baseline) 75 3.89 (1.47 – 10.28) 0.006 Vasopressor use ‡ 75 4.28 (1.59 – 11.51) 0.004 Central venous pressure ‡ 75 3.40 (1.21 – 9.58) 0.021 Primary lung injury 75 3.51 (1.24 – 9.94) 0.018 PaO2
† ‡ 67 3.35 (1.16 – 9.70) 0.026
* Potential covariates were included in the multivariable logistic regression models if the variable was found to be associated with cognitive impairment in the univariate analyses (p<0.20) and to assess whether inclusion of the potential covariate altered the odds ratio for the candidate risk factor by > 10%. Age, race, level of education, and time from enrollment to testing were forced into the models. See methods for details. † History of heavy alcohol use was missing in 3 survivors; history of cerebrovascular disease was missing in 2 survivors; baseline mean arterial pressure missing in 1 survivor. On-study PaO2 measurements were missing in 8 survivors.
Page 75 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
32
‡ On-study values. Daily measurements on-study were summarized, at the subject level, as means. § For each 10-unit decrease in partial pressure of oxygen in arterial blood (PaO2), odds ratio for the development of cognitive impairment increases by 1.56 in the base model.
Page 76 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
33
Figure E1.
Page 77 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
34
Conservative Fluid-Management Strategy
N=503
Consented to long-term follow-up for EA-PAC
N=322
Consented to long-term follow-up for EA-PAC
N=333
Tested at 12 months §
N=56 Tested at 12 months
§
N=46
Liberal Fluid-Management Strategy N=498
Consented to ACOS N=102
Consented to ACOS N=111
Deceased: N=13 Incarcerated: N=1 Incapable
†: N=5
Declined: N=9 Missing: N=1 Lost to follow-up
†: N=26
Total: N=55‡
Deceased: N=91 Ineligible
†: N=31
Declined: N=26 Unable to be contacted: N=74 Total: N=222
Completed Testing in All Domains
N=37
Completed Testing in All Domains
N=38
Deceased: N=9 Incarcerated: N=1 Incapable
†: N=4
No contact information: N=1 No telephone service: N=1 Declined: N=16 Lost to follow-up
†: N=24
Total: N=56‡
Deceased: N=103 Ineligible
†: N=24
Declined: N=22 Unable to be contacted: N=71 Total: N=220
Page 78 of 79

For Review O
nly
ARDS COGNITIVE OUTCOMES STUDY (ACOS)
35
* Of 1001 FACTT subjects who underwent randomization, 227 were ineligible for long-term
follow-up as part of EA-PAC as no regulatory approval was in place and 119 refused consent (21). †
Subjects were categorized as ineligible if the time window to be tested had elapsed due to the regulatory halt, as incapable if self-determined or determined by a surrogate to be physically or mentally incapable of telephone-based neuropsychological testing, and as lost to follow-up if consent was obtained but the subject was not tested. ‡
Reasons for not being testing, in those who consented, are categorized initially as causes outside of investigator control and then as causes which may be potentially remediable by future investigators. §
Of 52 subjects tested at 2 months (20 from liberal arm and 32 from conservative arm), 32 were re-tested at 12 months. Subjects were not required to undergo testing at 2 months to be tested at 12 months.
Page 79 of 79