the cardio-renal syndrome stephen l. rennyson md
TRANSCRIPT
The Cardio-Renal Syndrome
Stephen L. Rennyson MD
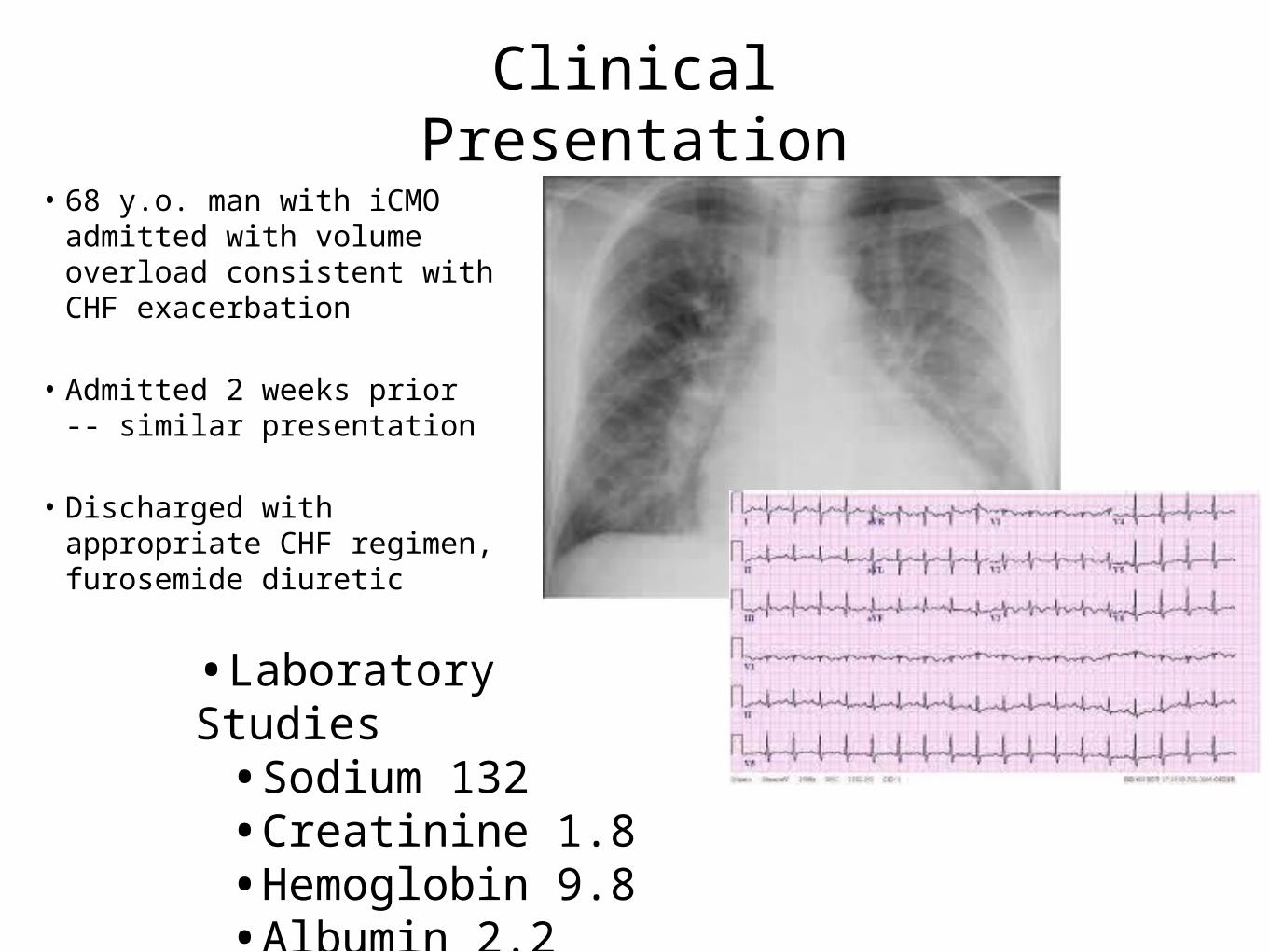
• 68 y.o. man with iCMO admitted with volume overload consistent with CHF exacerbation
• Admitted 2 weeks prior -- similar presentation
• Discharged with appropriate CHF regimen, furosemide diuretic
•Laboratory Studies•Sodium 132•Creatinine 1.8 •Hemoglobin 9.8•Albumin 2.2
Clinical Presentation

• Placed on BiPap in the ED, given 120 mg of iv Lasix, transferred to CICU . . . Started NTG gtt
• Initial success of 500 cc urine output
• Morning laboratory studies show creatinine rising
• Midnight dose of lasix produced little urine output
• Blood pressure falling . . .

Background
Pathophysiology
Management Options
Case
Cardio-Renal Syndrome

Congestive Heart Failure
• Epidemiology changing from acute management to managing the chronicity of cardiac dysfunction
• An indicence of 5 million persons
• Responsible for over 1 million yearly hospitalizations
• 280,000 deaths annually
Comorbid Conditions . . .Associated with a worse
prognosis
• Anemia (Hb < 10.0)
• Cirrhosis
• Peripheral Vascular Disease
• Hyponatremia (<135)
• Renal failure
N Engl J Med 2006; 355:260-269July 20, 2006
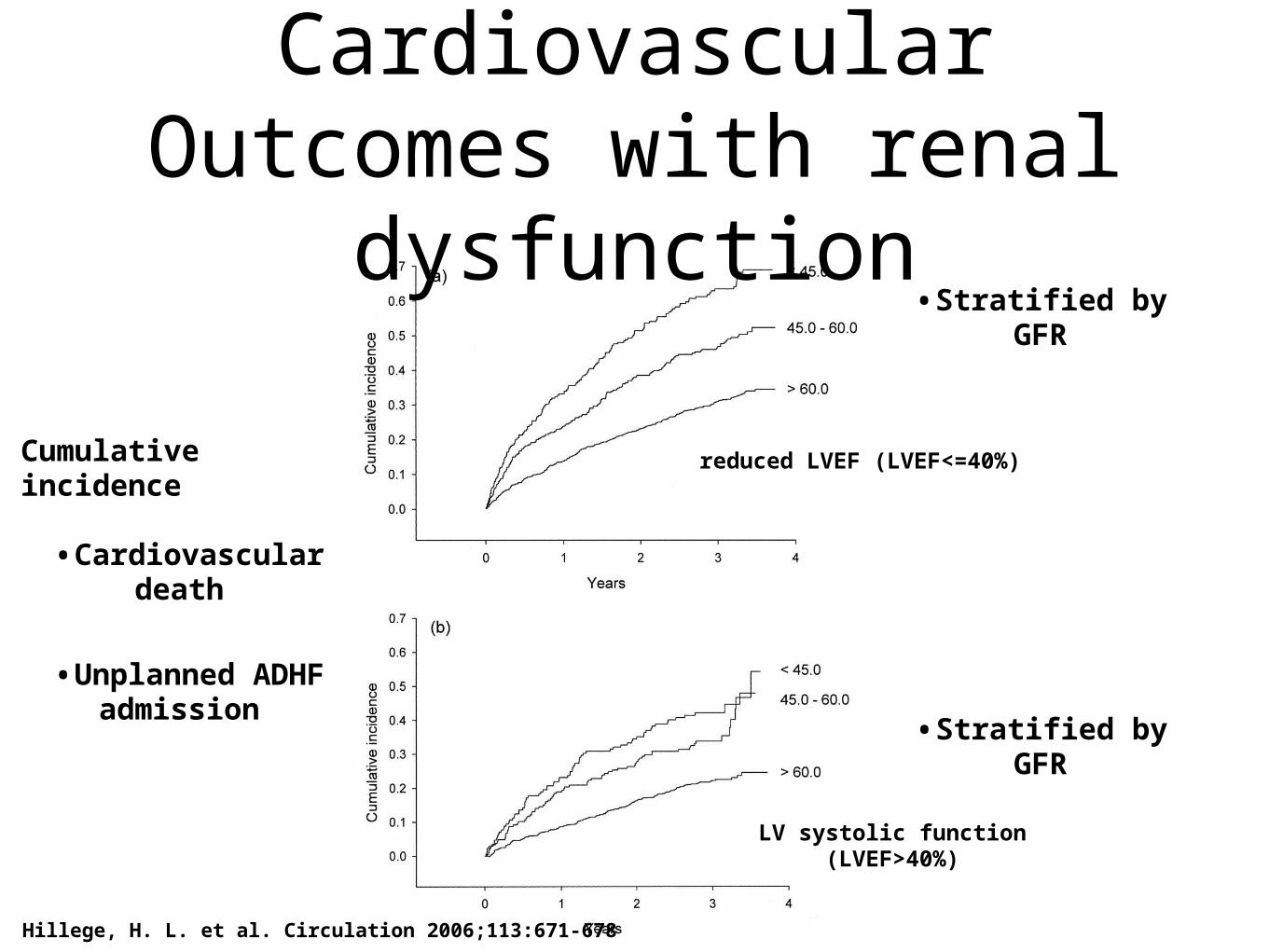
Hillege, H. L. et al. Circulation 2006;113:671-678
Cumulative incidence
•Cardiovascular death
•Unplanned ADHF admission
reduced LVEF (LVEF<=40%)
LV systolic function (LVEF>40%)
Cardiovascular Outcomes with renal
dysfunction•Stratified by GFR
•Stratified by GFR
ADHERE Registry•Registry of Acute Decompensated Heart Failure (ADHF)
•105,000 patient registry
•QOC study evaluating variations in CHF treatment
Best predictors of outcome:BUN
Creatinine

•Most Simplistic Description:
• Associated loss of renal function in the setting of advanced CHF
• CRS or RCS?
Cardio-Renal Syndrome
Subtypes• Type I, acute CRS
• Type II, chronic CRS
• Type III, acute renocardiac syndrome
• Type IV, chronic renocardiac syndrome
• Type V, secondary CRS -- sepsis, amyloidosis
Cardio-Renal Syndrome
• CHF patients at increased risk for CRS:
• Hypertension
• Diabetes
• Severe Vascular Disease
• Elderly

Background
Pathophysiology
Management
Conclusions
Cardio-Renal Syndrome
Pathophysiology
• Neurohormonal Factors:
• SNS, RAAS, AVP System
• Hemodynamics:
• Loss of Cardiac Output
• Transrenal perfusion pressure
• Intrarenal hemodynamics
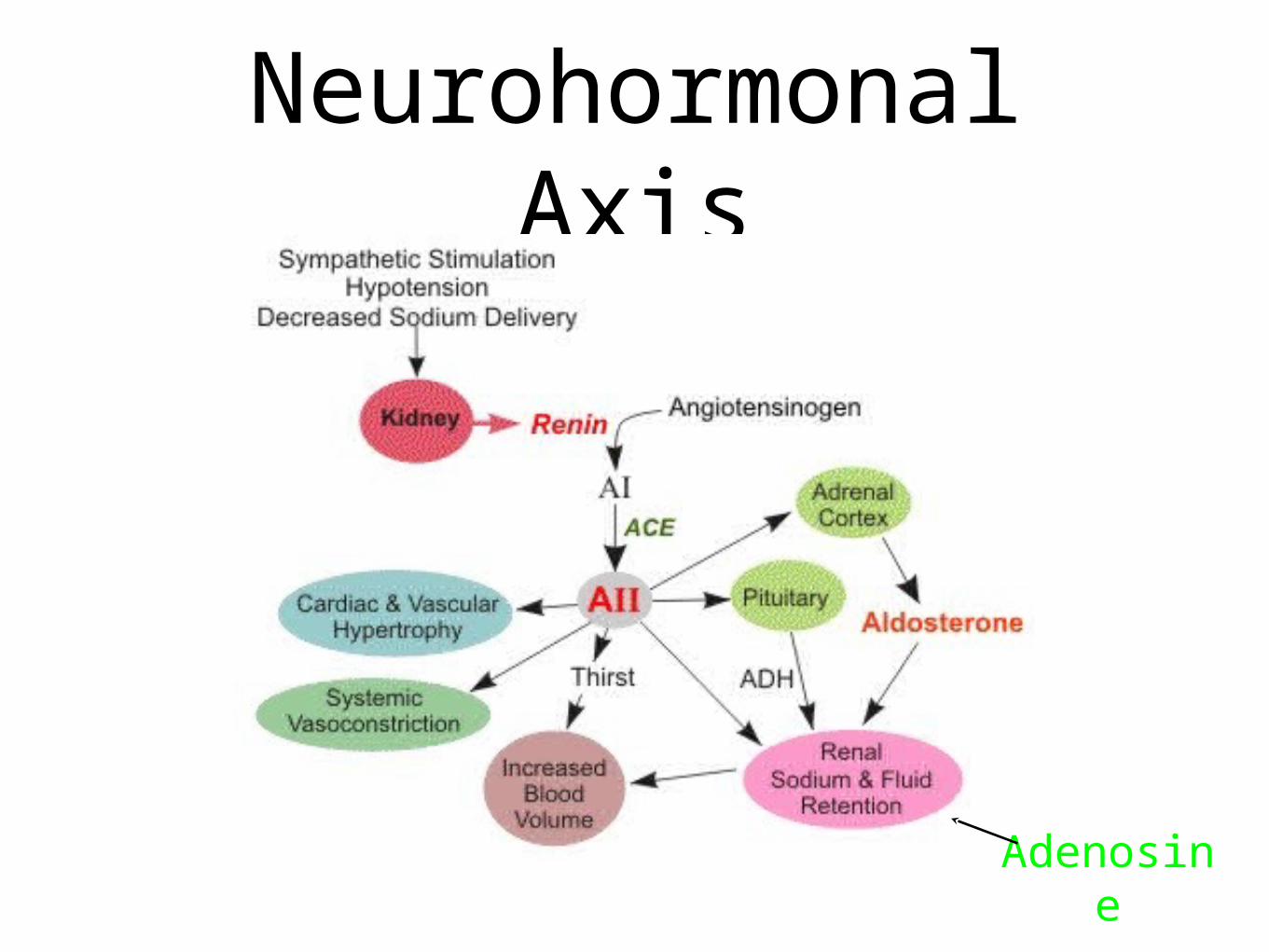
Neurohormonal Axis
Adenosine
CHF Hemodynamics• Systolic or Diastolic CHF
• Exacerbations -- Symptomatology seen objectively
• Elevated PCWP
• Elevations of INR, Alkaline Phosphatase
• Elevations of Creatinine
• Shift in paradigm
CVP and Renal Failure
• 2,557 patients underwent RHC
• Age 59 ± 15 years
• 57% were men
• Renal Function using estimated
Glomerular Filtration Rate (eGFR)
Damman, K. et al. J Am Coll Cardiol 2009;53:582-588

Damman, K. et al. J Am Coll Cardiol 2009;53:582-588
Curvilinear Relationship Between CVP and eGFR According to Different Cardiac Index Values
Central Venous Pressure
Solid line = cardiac index <2.5
dashed line = cardiac index 2.5 to 3.2
dotted line = cardiac index >3.2
p = 0.0217

CVP and Renal Failure
Damman, K. et al. J Am Coll Cardiol 2009;53:582-588
Kaplan-Meier Analysis of Event-Free Survival According to Tertiles of CVP

Renal Hemodynamics• Transrenal perfusion pressure
• TRPP = MAP - CVP
• CVP influenced:
• PAP -- Oxygenation, Valve Dysfunction, CO
• Volume Status
• MAP -- Perfusion Pressure
• Cardiac Output
• Systemic Vascular Resistance
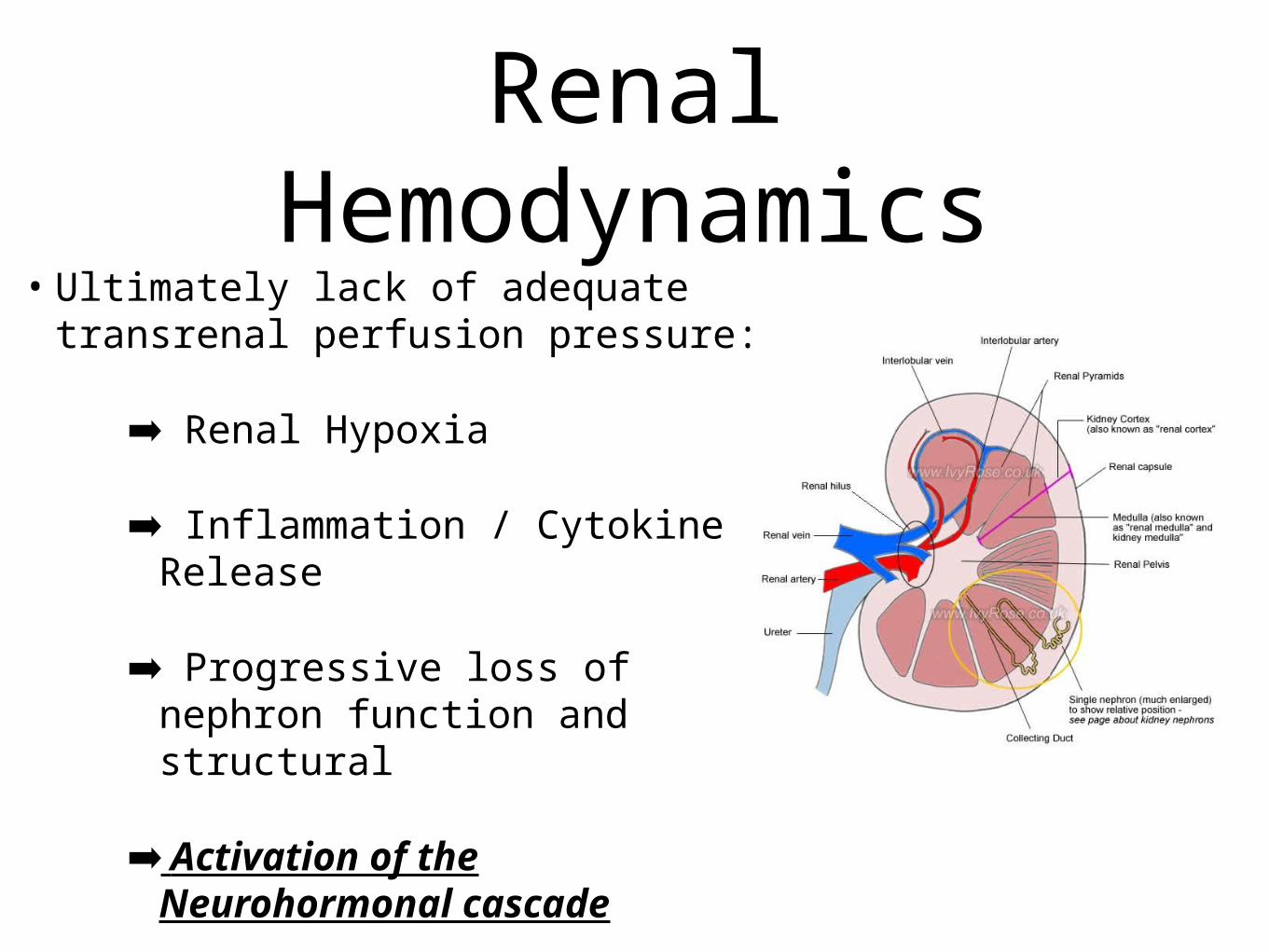
• Ultimately lack of adequate transrenal perfusion pressure:
➡ Renal Hypoxia
➡ Inflammation / Cytokine Release
➡ Progressive loss of nephron function and structural
➡ Activation of the Neurohormonal cascade
Renal Hemodynamics

Background
Pathophysiology
Management Options
Case
Cardio-Renal Syndrome

The Cardio-Renal Syndrome
• Treatment Goals
• Same goals as ADHF
• Removal of Volume
• Optimizing Hemodynamics
• Complicated by chronic renal failure and acutely worsening renal function
Removal of Volume
• Loop Diuretics
• Brain Naturetic Peptide
• Arginine Vasopressin Antatonism
• Adenosine Antagonism
• Ultrafiltration

Loop Diuretics
• Goal --> Deplete extracellular fluid volume
• Balanced refilling interstitium to intravascular compartment
• Reality --> Contraction of circulating volume --> Activation of neurohormonal response

Loop Diuretics
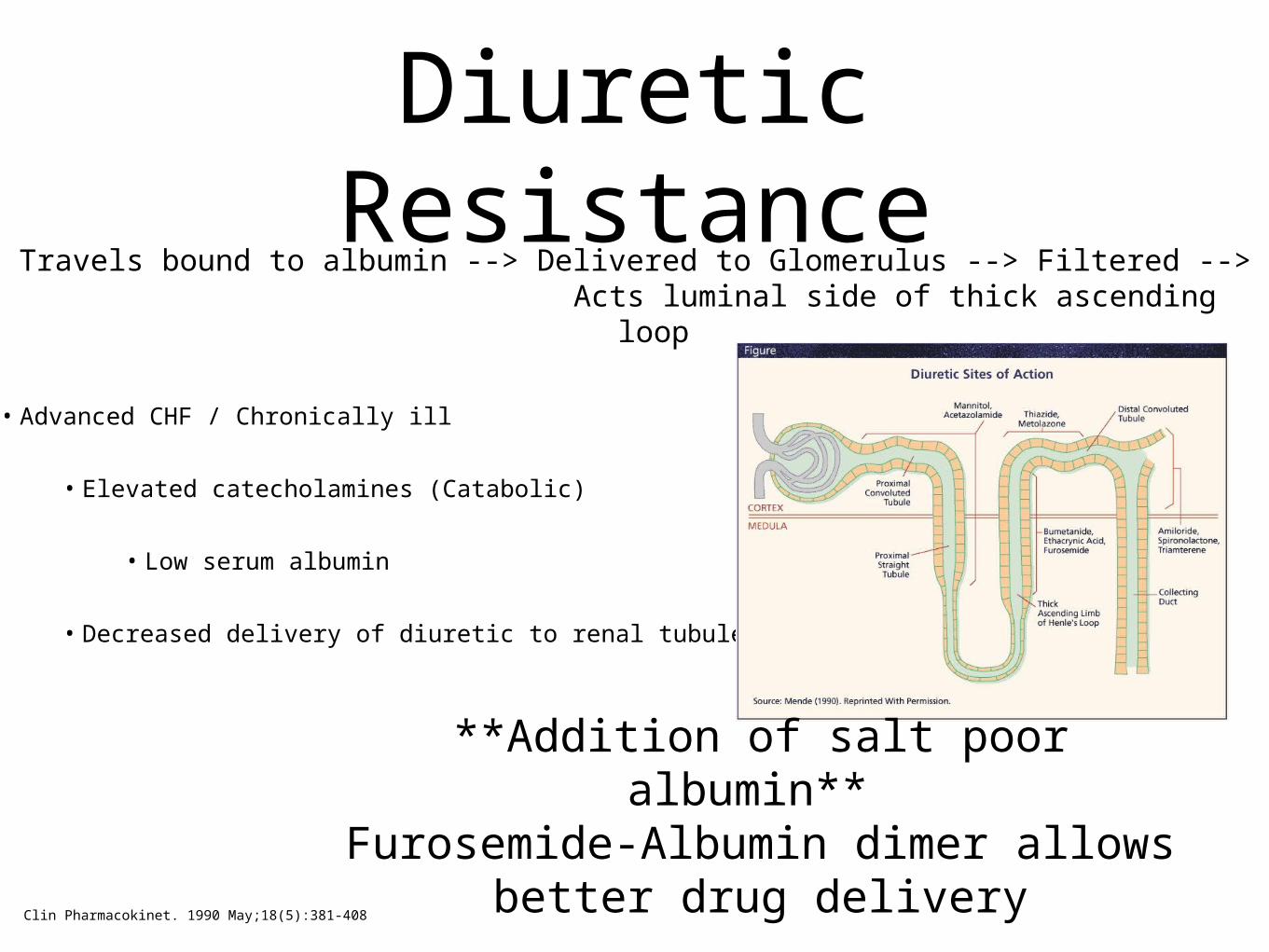
• Furosemide
• Blockage of the thick ascending loop Na/ K/ 2 Cl pump
• Acts intraluminally
• Travels Bound to albumin
• High Na delivered to distal tubules
Chronic use -> cellular hypertrophy -> increased Na reabsorption -> Failure of diuresis
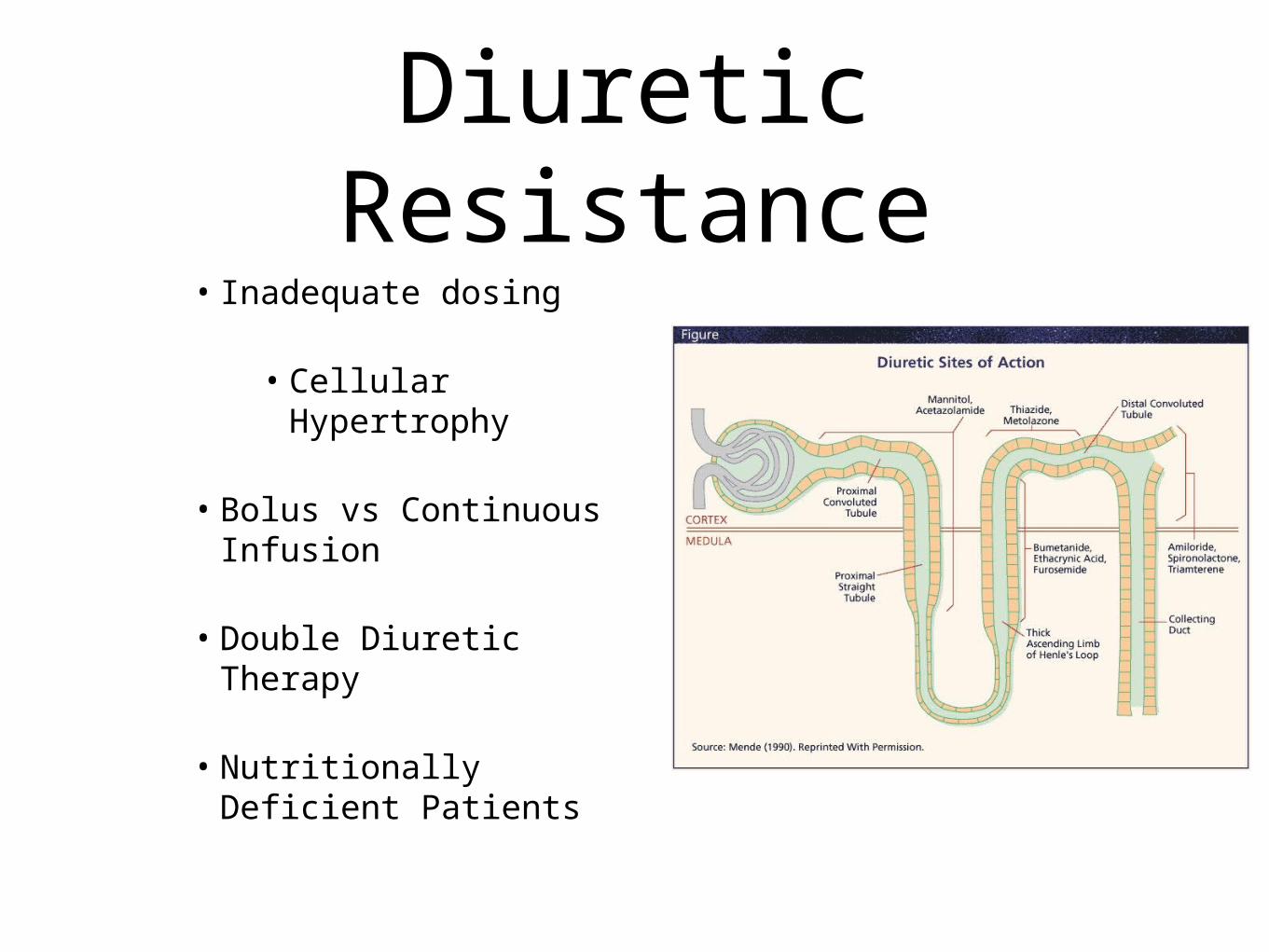
Diuretic Resistance• Inadequate dosing
• Cellular Hypertrophy
• Bolus vs Continuous Infusion
• Double Diuretic Therapy
• Nutritionally Deficient Patients
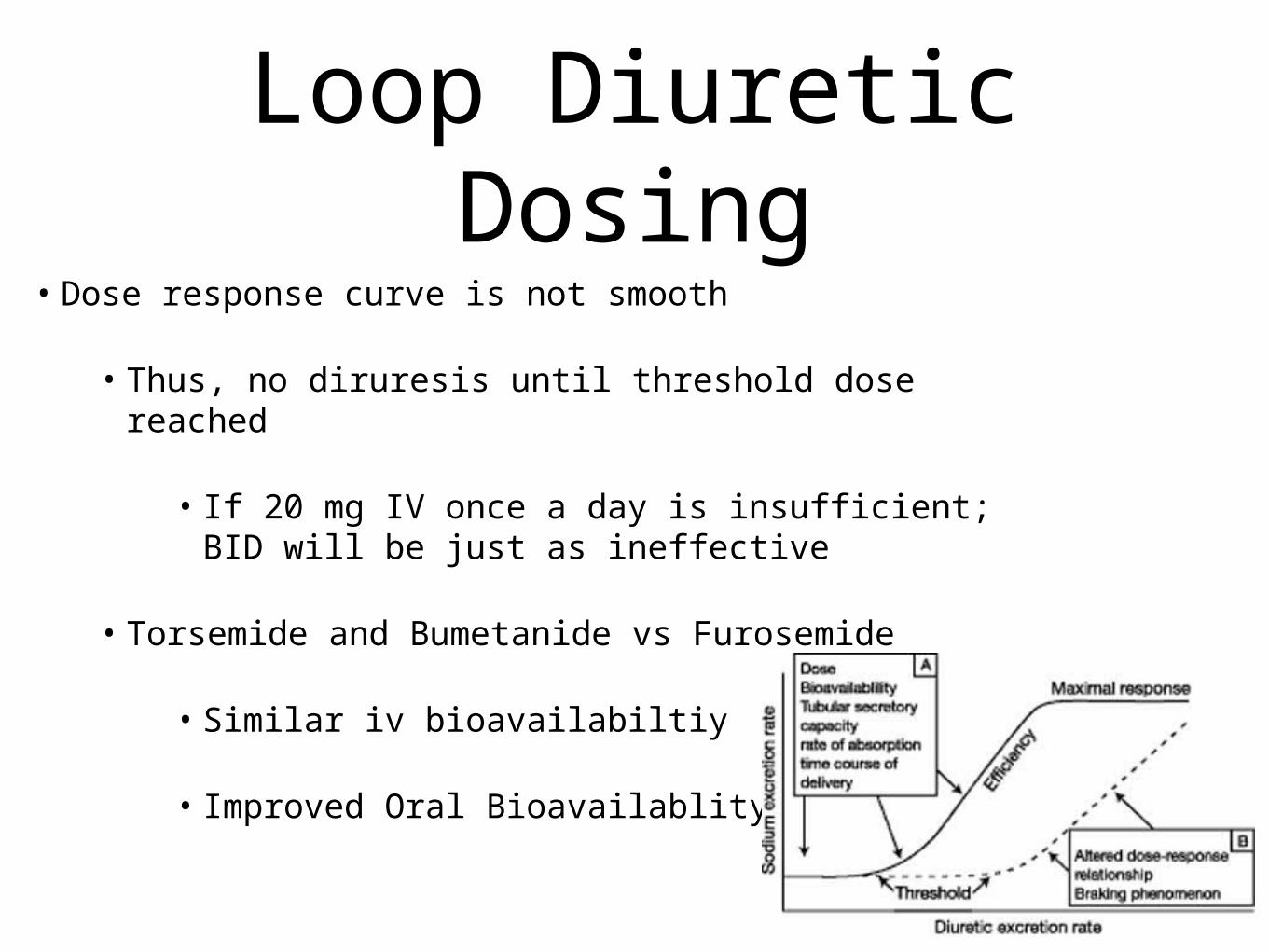
Loop Diuretic Dosing
• Dose response curve is not smooth
• Thus, no diruresis until threshold dose reached
• If 20 mg IV once a day is insufficient; BID will be just as ineffective
• Torsemide and Bumetanide vs Furosemide
• Similar iv bioavailabiltiy
• Improved Oral Bioavailablity
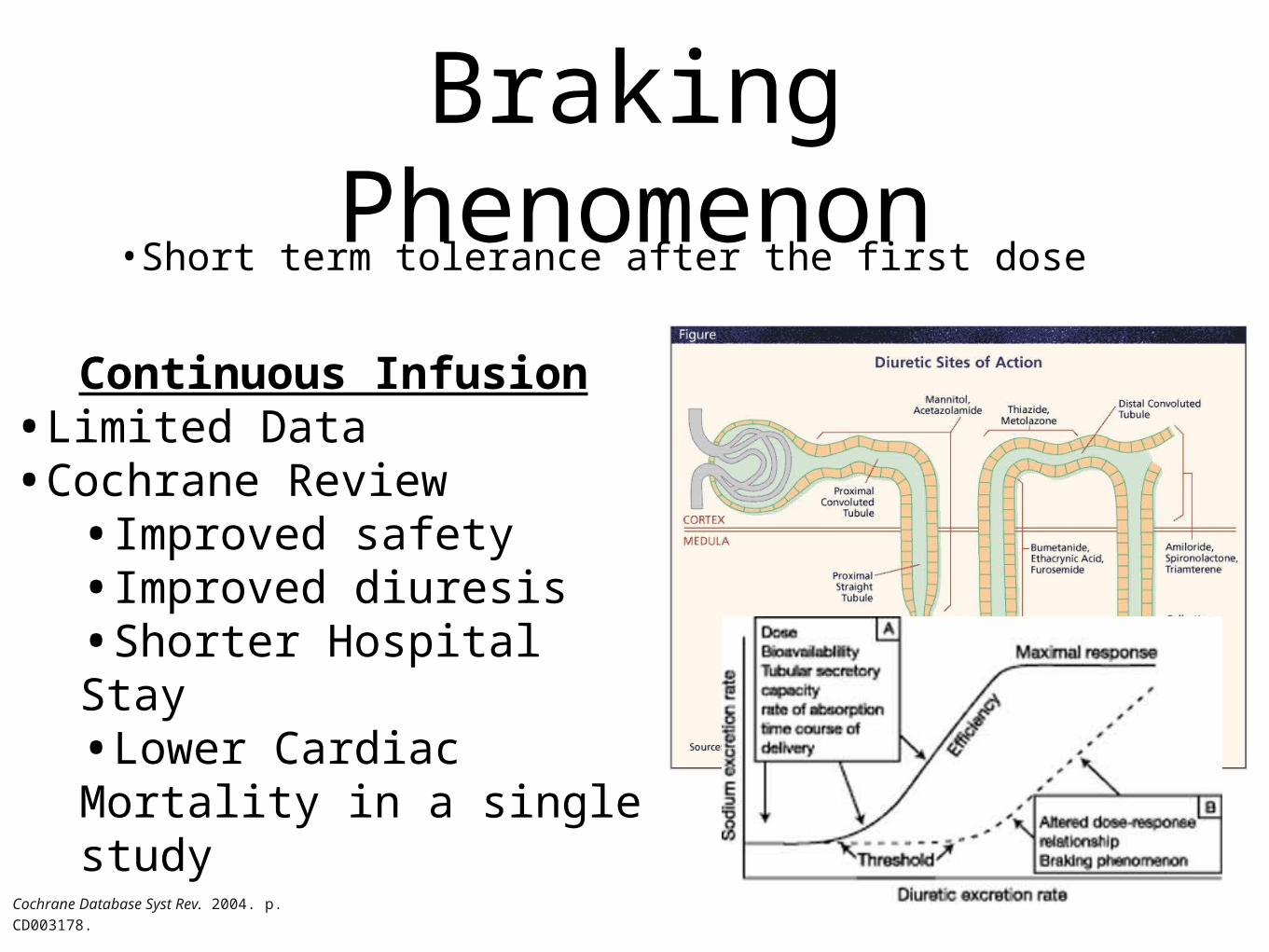
Braking Phenomenon
•Short term tolerance after the first dose
Continuous Infusion•Limited Data •Cochrane Review
•Improved safety•Improved diuresis•Shorter Hospital Stay•Lower Cardiac Mortality in a single study
Cochrane Database Syst Rev. 2004. p. CD003178.

The DOSE TrialDiuretic Optimization Strategies Evaluation
DOSE Trial•308 patients with ADHF•Low vs High Dose Furosemide•Continuous vs a12 hour dosing
•Overall no significant difference among all groups
•Patients symptoms•Creatinine•High Dose group had a greater diuresis with transient increases in creatinineN Engl J Med. 2011 Mar 3;364(9):797-805.

Diuretic Resistance
• Loop + Thiazide
• Chlorothiazide 250 mg vs 500 mg IV / Metolazone 5-10 mg PO
• Very Effective -- Weight loss and edema resolution
• Double Sodium Excretion
• CAUTION: Hyponatremia, Hypotension, Worsening renal function
Chronic use -> cellular hypertrophy -> increased Na reabsorption -> Failure of diuresis
Double Diuretic Therapy or Sequential Nephron Blockade
J Am Coll Cardiol, 2010; 56:1527-1534, doi:10.1016/j.jacc.2010.06.034
Diuretic Resistance
• Advanced CHF / Chronically ill
• Elevated catecholamines (Catabolic)
• Low serum albumin
• Decreased delivery of diuretic to renal tubules
Travels bound to albumin --> Delivered to Glomerulus --> Filtered --> Acts luminal side of thick ascending loop
Clin Pharmacokinet. 1990 May;18(5):381-408
**Addition of salt poor albumin** Furosemide-Albumin dimer allows
better drug delivery
Brain Natriuretic Peptide
LV volume overload --> Cardiac Myocytes secrete BNP precursor --> Converted to proBNP --> ProBNP cleaved into:
• C-terminal BNP (biologically active)
• Decrease in SVR and CVP
• Increase natriuresis
• N-terminal BNP or NT-proBNP (biologically inactive)
Nesiritide (Natrecor)•New to market in 2001
•Actions in ADHF
•PCWP reduced within 15 minutes of administration
•Resultant decreases in PA and RA pressure
•Reduced SVRI
•Resultant increase in CO
•Enhances loop diuretic effects
•Modest intrinsic natriuretic and diuretic effects
•No tachyphylaxis
•Blocks loop diuretic effects of aldosterone up-regulationCleve Clin J Med. 2002 Mar;69(3):252-6. Review Clin Cardiol. 2010 Jun;33(6):330-6

ASCEND-HF• Over 7000 patients with ADHF -- standard
therapy
• Nesiritide infusion 24 hrs - 7 days vs placebo
• Primary End points:
• CHF mortality and readmission (30 days)
• Self reported Dyspnea at 6 and 24 hours
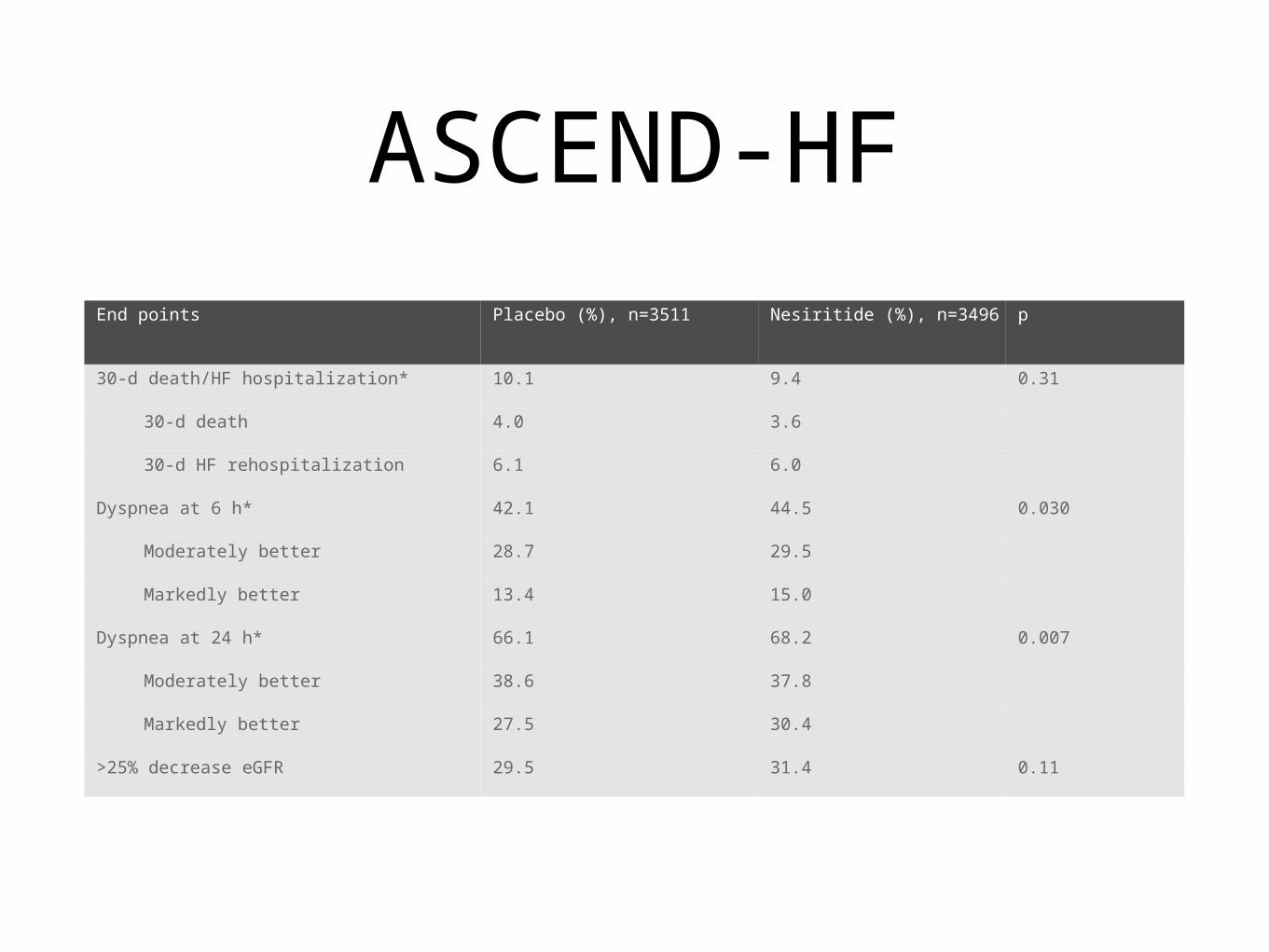
ASCEND-HFEnd points Placebo (%), n=3511 Nesiritide (%), n=3496 p
30-d death/HF hospitalization* 10.1 9.4 0.31
30-d death 4.0 3.6
30-d HF rehospitalization 6.1 6.0
Dyspnea at 6 h* 42.1 44.5 0.030
Moderately better 28.7 29.5
Markedly better 13.4 15.0
Dyspnea at 24 h* 66.1 68.2 0.007
Moderately better 38.6 37.8
Markedly better 27.5 30.4
>25% decrease eGFR 29.5 31.4 0.11
ASCEND-HF• Role of Natrecor:
• Resolved Concerns:
• Worsening mortality
• Worsening renal function
• No significant benefit compared to standard therapy
• Improved Dyspnea Score ($500.00/day)

Arginine Vasopressin
• Arginine vasopressin (AVP), secreted by posterior pituitary
• V1 Vascular receptor
• V2 Renal receptor Proportional to the severity of HF
Contributes to fluid retention and hyponatremia
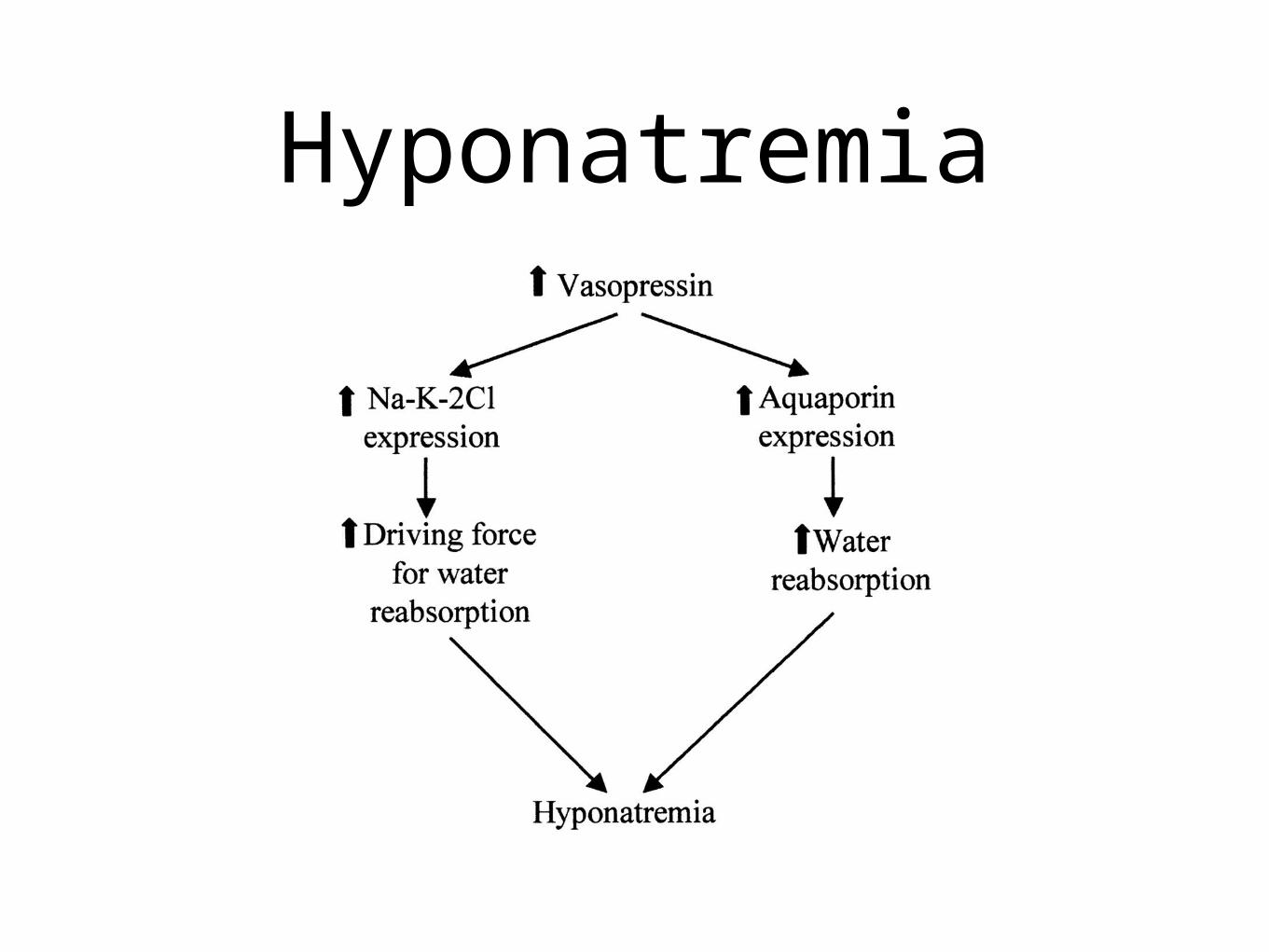
Hyponatremia

ACTIV Trial• Initial trial for Tolvaptan -- AVP antagonist
• 319 patients with systolic dysfunction (<40%) admitted with exacerbation
• Tolvaptan vs Placebo/ Standard Treatment
• Greater loss of body weight
• Greater urine output at 24 hours
• Increase in serum sodium
JAMA. 2004 Apr 28;291(16):1963-71.

EVEREST Trial• Efficacy of Vasopressin Antagonism in HF Outcome Study With
Tolvaptan
• Over 4000 patients in two separate study groups
• EF < 40%
• Tolvaptan (30mg) vs Placebo in combination with standard HF thearpy
• Treatment time up to 7 days
JAMA. 2007 Mar 28;297(12):1332-43. Epub 2007 Mar 25

Tolvaptan(n=2072)
% of patients
Placebo(n=2061)
% of patients
Baseline Meds
Diuretics 97.1 96.6
ACEi / ARB 84.3 84.1
β-blocker 70.8 69.6
Aldo blocker 53.6 54.7
IV inotrope 4.0 4.3
Nesiritide 4.2 5.1
Baseline HF Characteristics
Dyspnea 90.9 91.1
Edema 79.3 79.3
JVD ≥ 10 cm H2O 27.0 26.9
Serum Na+ <134 mEq/L 7.9 8.0

EVEREST Trial
JAMA. 2007 Mar 28;297(12):1332-43. Epub 2007 Mar 25

EVEREST Trial
JAMA. 2007 Mar 28;297(12):1332-43. Epub 2007 Mar 25

EVEREST Trial
JAMA. 2007 Mar 28;297(12):1332-43. Epub 2007 Mar 25
EVEREST Trial
• No change over 24 month follow up:
• All Cause Mortality
• Cardiovascular Mortality
• Heart Failure Hospitalization
JAMA. 2007 Mar 28;297(12):1332-43. Epub 2007 Mar 25
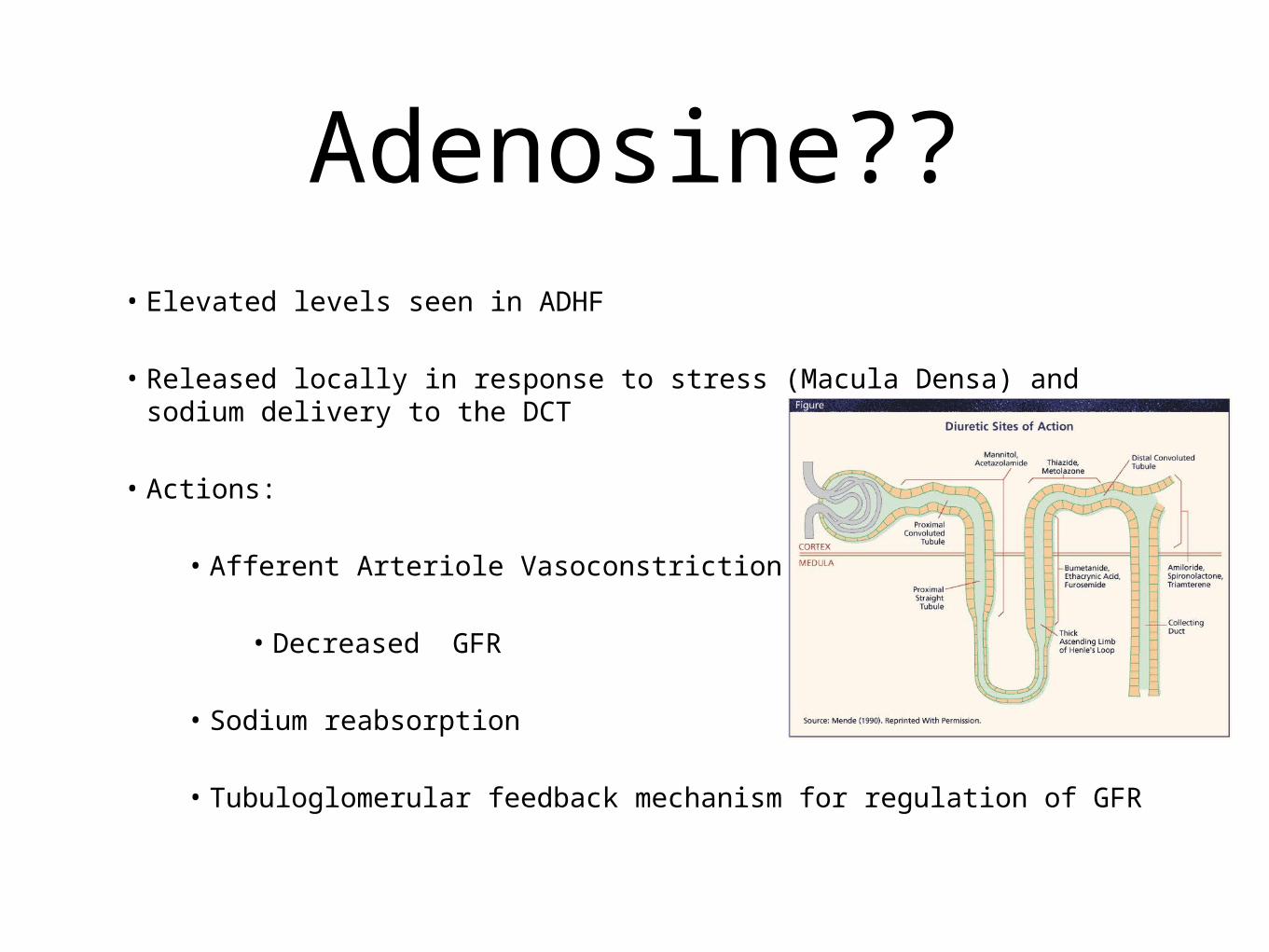
• Elevated levels seen in ADHF
• Released locally in response to stress (Macula Densa) and sodium delivery to the DCT
• Actions:
• Afferent Arteriole Vasoconstriction
• Decreased GFR
• Sodium reabsorption
• Tubuloglomerular feedback mechanism for regulation of GFR
Adenosine??
Adenosine
• Tubuloglomerular Feedback
• Acute delivery of sodium to the distal tubules (Lasix)
• Adenosine further released from the macula densa
• Further renal dysfunction
Br J Pharmacol. 2003 August 2; 139(8): 1383–1388.

Adenosine Antagonism
BG9719
• 63 patients with ADHF
• Compared Groups
• Lasix Alone
• Adenosine Antagonist Alone
• Combination thearpy
Circulation. 2002;105:1348-1353

Adenosine
Circulation. 2002;105:1348-1353
Ultrafiltration• The removal of isotonic volume across a
semipermeable membrane
• Hemodialysis -- Removal of volume and solutes using a concentration gradient
• UF does not decrease sodium presentation to the macula densa
• Avoids neurohormonally mediated sodium and water reabsorption
Ultrafiltration
• Advantages
• Low Flow Catheters -- Simple PICC line
• Veno-Venous filtration
• No ICU monitoring needed

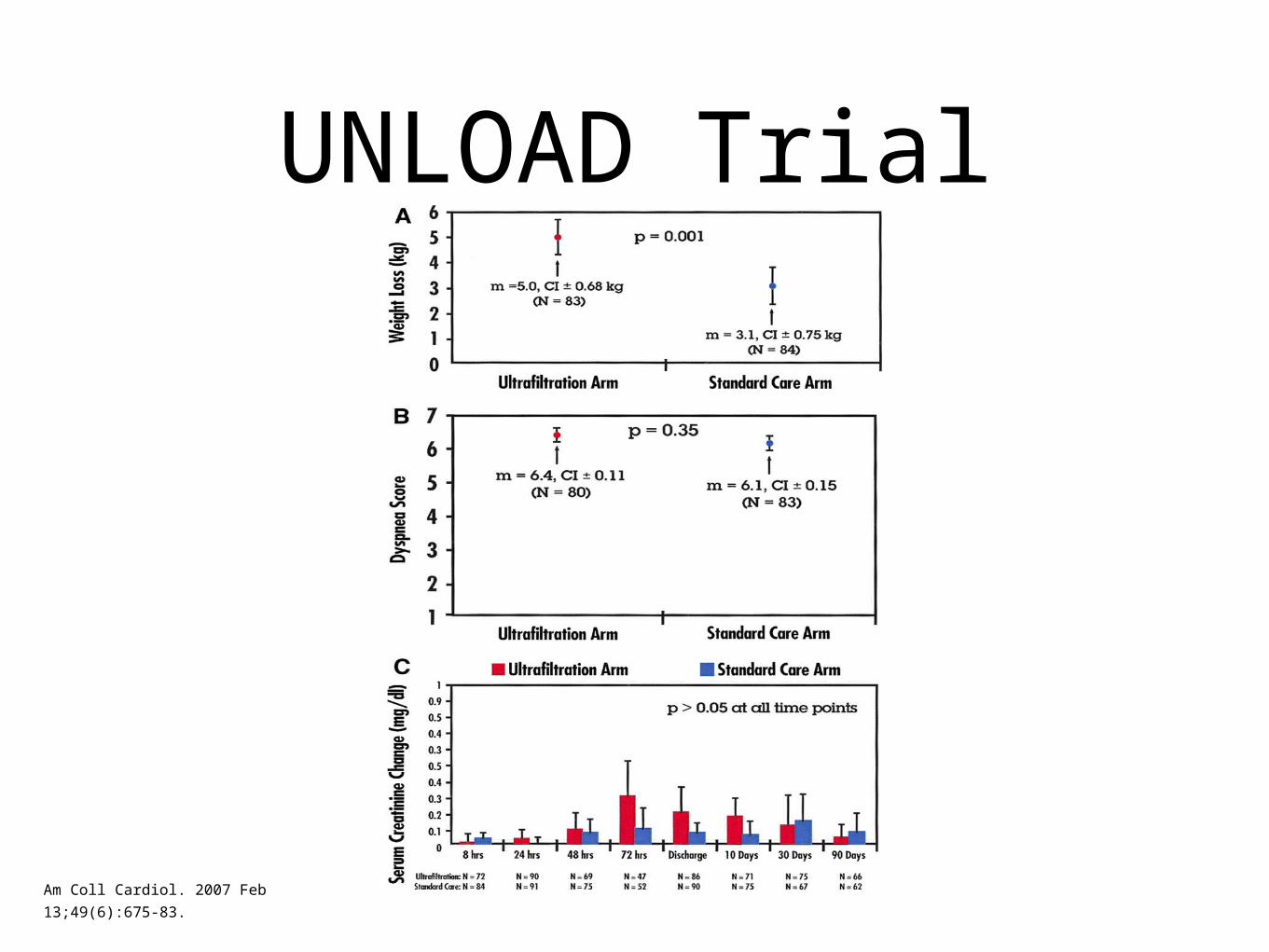
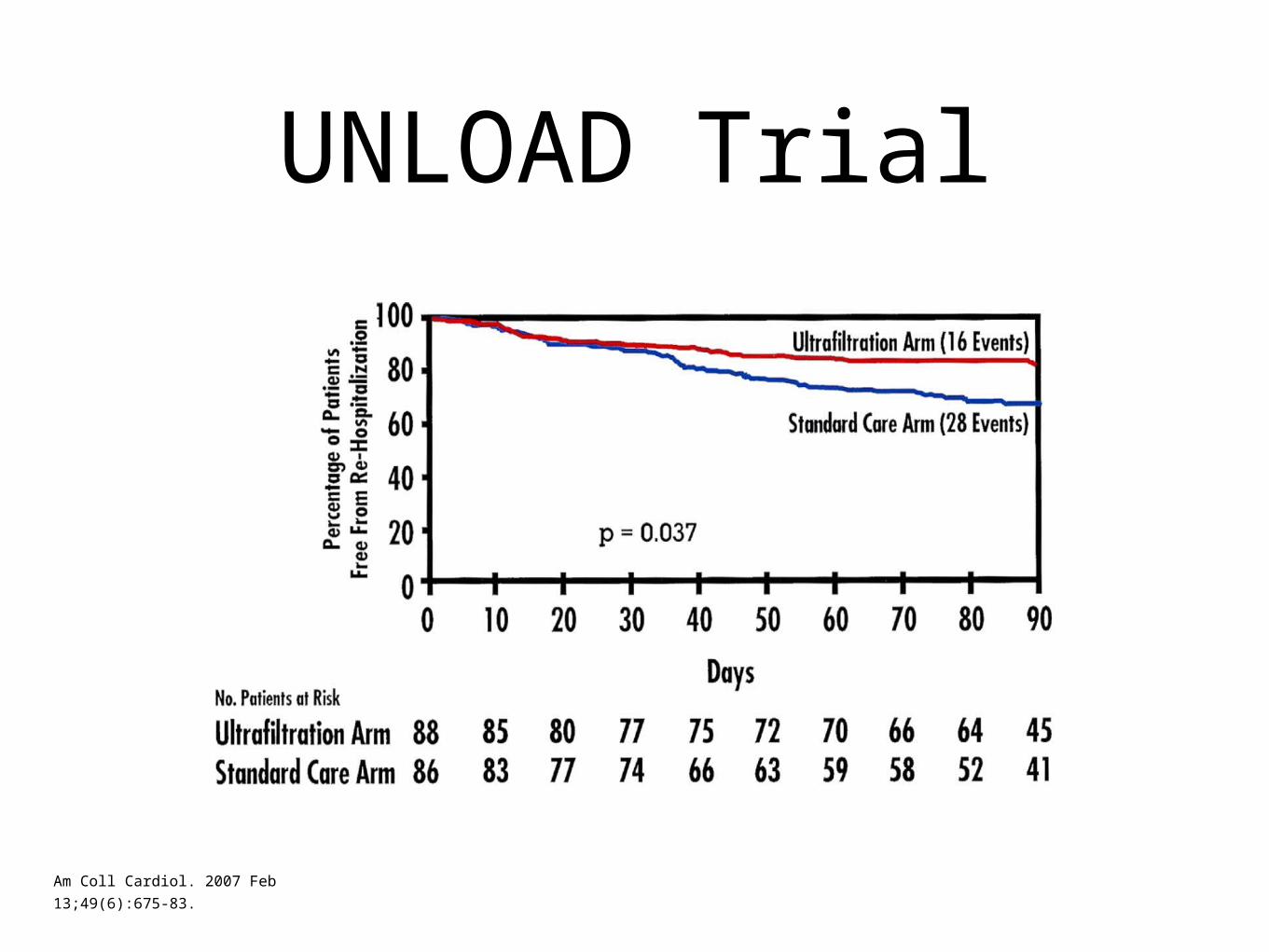
UNLOAD Trial
• 200 Patients with ADHF
• Randomized:
• Conventional IV Diuresis
• UF up to 500cc/hr
Am Coll Cardiol. 2007 Feb 13;49(6):675-83.
UNLOAD Trial• Hypotension during 48 h after randomization:
• Similar UF (4 of 100) 4% vs. Standard (3 of 100) 3%
• Net fluid loss 48 h after randomization:
• UF 4.6 ± 2.6 L
• Standard-care 3.3 ± 2.6 L (p = 0.001)
Am Coll Cardiol. 2007 Feb 13;49(6):675-83.
UNLOAD Trial
Am Coll Cardiol. 2007 Feb 13;49(6):675-83.
UNLOAD Trial
Am Coll Cardiol. 2007 Feb 13;49(6):675-83.

• 68 y.o. man with iCMO admitted with volume overload consistent with CHF exacerbation
• Diuresis poor
• Creatinine Rising
•Laboratory Studies•Sodium 132•Creatinine 1.8 •Hemoglobin 9.8•Albumin 2.2
Clinical Presentation

• Goals:
• Improve symptoms
• Limit further activation of the neurohormonal cascase
• Little has been done to improve mortality
TRPP = MAP - CVP
• The Cardio-Renal Syndrome is a worst case scenario for the CHF patient
•Mortality is clearly worsened
•Management is difficult:– Many options; nothing improves mortality
– Promising new therapies -- Adenosine . . .
– Each readmission for ADHF increases mortality thus optimization (Ultrafiltration) may play a larger role
Conclusions