“the culture of culturing”: update on national survey on
TRANSCRIPT

“The Culture of Culturing”: Update on National Survey on Blood Culture PracticesBRIEF PRESENTATION FOR THE NATIONAL CORPORATE IP NETWORK GROUP
APIC 43RD ANNUAL CONFERENCE
CHARLOTTE, NC JUNE 13, 2016
ROBERT GARCIA / BARBARA KRANZ

Update
Survey completion, 86 hospitals Blood Culture Survey Article Tables summarizing information Outline Urine culture article Editorial

Table 1: DemographicsHospital type (n=86) Responses Percent
Community 58 67.4
Teaching University affiliated 15 17.4
Children’s 3 3.5
Other 13 15.1
Census Region (n=86)
Northeast 12 14.0
South 9 10.5
Midwest 24 27.9
Other 5 5.8
Total beds (n=84)
<150 28 33.3
150-500 45 53.6
>500 11 13.1

Table 2: Blood Culture DataNo. Responses Percent
No. BCs drawn per year (n=82)>30,000 13 15.910,000-30,000 31 37.8<10,000 38 46.3
Does Microbiology Laboratory calculate a BC contamination rate? (n=85)
Yes 74 87.1No 11 12.9
Are BCC rates calculated for the following? (n=75)Each patient unit including the ED 54 72.0Each patient unit excluding the ED 2 2.7Only some patient units 6 8.0Other 13 17.3
What is the hospital’s overall BCC rate? (n=76)>5% 4 5.33-4.9% 7 9.2<3% 61 80.3Don’t know 4 5.3
If calculated, how often are BCC rates calculated by the Micro Lab? (n=75)
Monthly 54 72.0Quarterly 11 14.7Every 6 months 2 2.7Annually 6 8.0Other 2 2.7
Are BCC rates communicated to the IP Department? (n=75)
Yes 66 88.0No 9 12.0Are BCC rates communicated to each patient unit?Yes 41 53.2No 36 46.8

Table 3: Policy (part 1)No. Responses Percent
Does your hospital have defined clinical indications for BCs?
Yes 43 50.6No 42 49.4Does your hospital have defined clinical indications for follow-up BCs?
Yes 29 33.7No 57 66.3Does your hospital have a checklist to support adherence to established BC protocol?
Yes 31 36.0No 55 64.0Does your hospital use a dedicated phlebotomy team exclusively for drawing blood cultures?
For all units 15 17.6Only for specific units 14 16.5Not at all 56 65.9Does your protocol require drawing BCs before administration of antibiotics?
Yes 71 82.6No 15 17.4Does your hospital protocol emphasize preference of collection of BC via venipuncture rather than CVAD?
Yes 77 89.5No 9 10.5Does your hospital select a different venipuncture site for each BC set?
Yes 79 91.9No 7 8.1For suspected CRBSI does your hospital draw a set from catheter paired with a set obtained from a peripheral vein site?
Yes 59 68.6No 27 31.4Does your protocol require hand hygiene with soap and water or sanitizer prior to donning gloves for BC draw?
Yes 82 95.3No 4 4.7Does your hospital use a BC collection kit?Yes, a commercially available kit 23 26.7Yes, a kit packaged in-house 24 27.9No 39 45.3
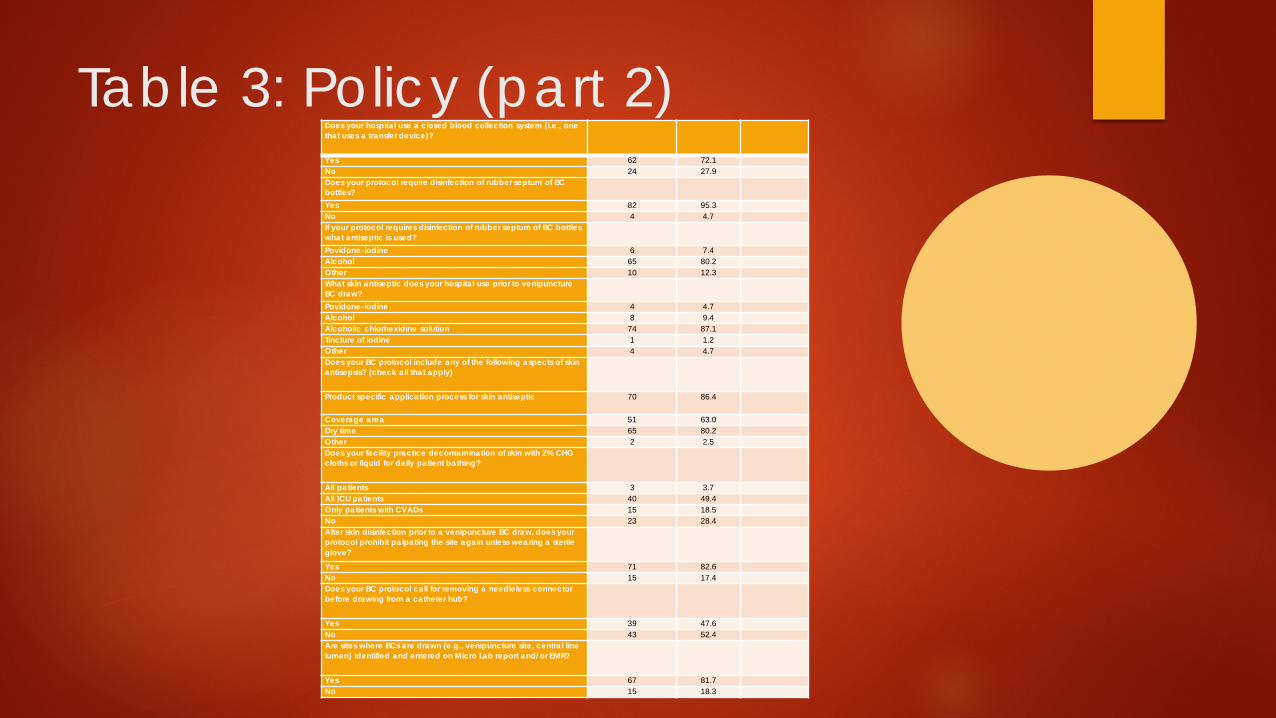
Table 3: Policy (part 2)Does your hospital use a closed blood collection system (i.e., one that uses a transfer device)?
Yes 62 72.1No 24 27.9Does your protocol require disinfection of rubber septum of BC bottles?Yes 82 95.3No 4 4.7If your protocol requires disinfection of rubber septum of BC bottles what antiseptic is used?Povidone-iodine 6 7.4Alcohol 65 80.2Other 10 12.3What skin antiseptic does your hospital use prior to venipuncture BC draw?Povidone-iodine 4 4.7Alcohol 8 9.4Alcoholic chlorhexidine solution 74 87.1Tincture of iodine 1 1.2Other 4 4.7Does your BC protocol include any of the following aspects of skin antisepsis? (check all that apply)
Product specific application process for skin antiseptic 70 86.4
Coverage area 51 63.0Dry time 65 80.2Other 2 2.5Does your facility practice decontamination of skin with 2% CHG cloths or liquid for daily patient bathing?
All patients 3 3.7All ICU patients 40 49.4Only patients with CVADs 15 18.5No 23 28.4After skin disinfection prior to a venipuncture BC draw, does your protocol prohibit palpating the site again unless wearing a sterile glove?Yes 71 82.6No 15 17.4Does your BC protocol call for removing a needleless connector before drawing from a catheter hub?
Yes 39 47.6No 43 52.4Are sites where BCs are drawn (e.g., venipuncture site, central line lumen) identified and entered on Micro Lab report and/or EMR?
Yes 67 81.7No 15 18.3
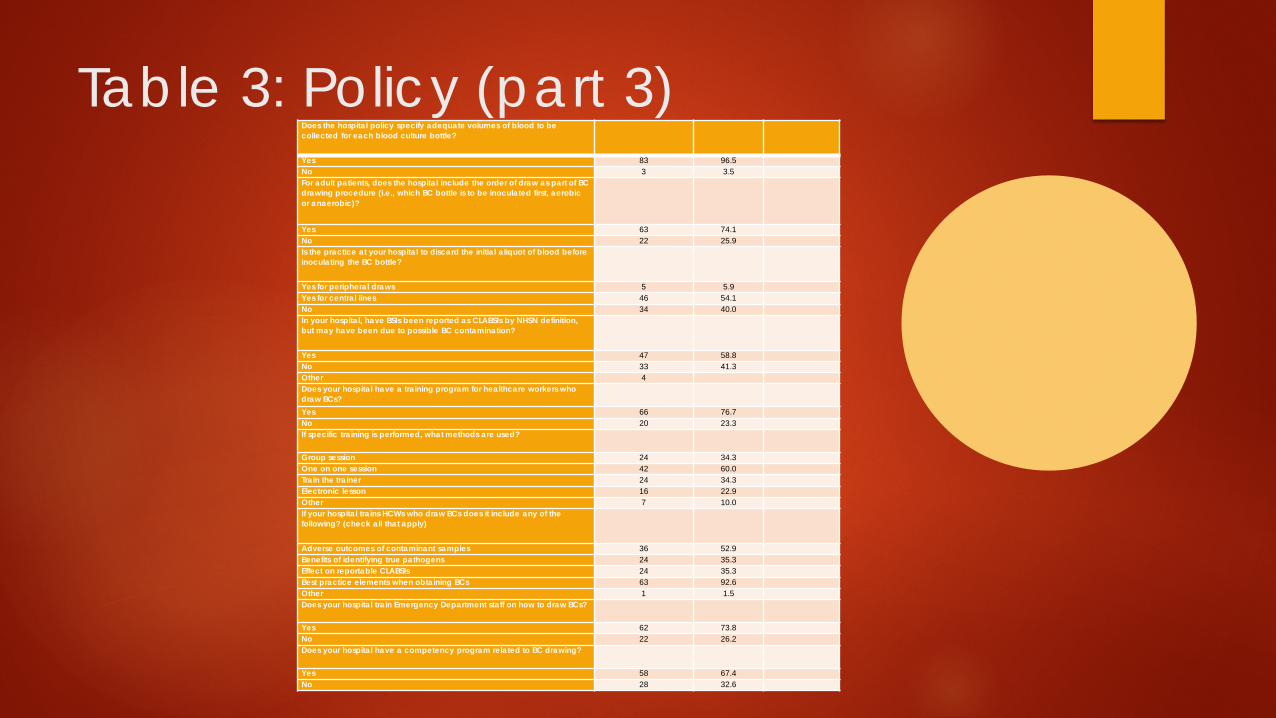
Table 3: Policy (part 3)Does the hospital policy specify adequate volumes of blood to be collected for each blood culture bottle?
Yes 83 96.5No 3 3.5For adult patients, does the hospital include the order of draw as part of BC drawing procedure (i.e., which BC bottle is to be inoculated first, aerobic or anaerobic)?
Yes 63 74.1No 22 25.9Is the practice at your hospital to discard the initial aliquot of blood before inoculating the BC bottle?
Yes for peripheral draws 5 5.9Yes for central lines 46 54.1No 34 40.0In your hospital, have BSIs been reported as CLABSIs by NHSN definition, but may have been due to possible BC contamination?
Yes 47 58.8No 33 41.3Other 4Does your hospital have a training program for healthcare workers who draw BCs?Yes 66 76.7No 20 23.3If specific training is performed, what methods are used?
Group session 24 34.3One on one session 42 60.0Train the trainer 24 34.3Electronic lesson 16 22.9Other 7 10.0If your hospital trains HCWs who draw BCs does it include any of the following? (check all that apply)
Adverse outcomes of contaminant samples 36 52.9Benefits of identifying true pathogens 24 35.3Effect on reportable CLABSIs 24 35.3Best practice elements when obtaining BCs 63 92.6Other 1 1.5Does your hospital train Emergency Department staff on how to draw BCs?
Yes 62 73.8No 22 26.2Does your hospital have a competency program related to BC drawing?
Yes 58 67.4No 28 32.6
Article Outline
The following may be supported by CLSI, ASM, CDC, ENA, NHS, IDSA Results indicating alignment with best practices
BC contamination rates reported to the IP department Drawing BCs prior to administration of antibiotics – ref 40 Policy indicating venipuncture drawing rather than CVAD – refs 44,52-60 Policy indicating different venipuncture site for each BC set - CLSI Policy indicating hand hygiene prior to donning gloves – ref 67 Disinfection of rubber septum of BC bottles – disinfectant used, ref 10,50 Antiseptic for venipuncture - aspects of antiseptics, ref see article Identification of BC draw sites – see article Tan 4 Policy specifies adequate volumes of blood – question did not specify adults vs
pediatrics, ref 50, 117-123 Training program for personnel who draw BCs – training methods; content; ED training;
see article Tab 4

Article Outline Results indicating need for modification or improvement in practice
Calculation of a BC contamination rate – ref 10
Calculation of a BC contamination rate by patient units – ref 10
Current BC contamination rate - CLSI
BC contamination rates communicated to each patient unit – ref CLSI, 10
Defined clinical indications for BCs – refs 47,51
Defined clinical indications for follow-up BCs - refs 47,51
Checklist to support adherence to established BC protocol – ref 153, article
Dedicated phlebotomy teams – ref see article Tab 4
Drawing paired sets from CVAD and venipuncture when CRBSI suspected – ref 63,64 (IDSA)
Use of a BC collection kit – ref AJIC 2015 article, ref 68-78
Use of a closed blood culture collection system - NHS
Decolonization of skin – ref 105-109
Use of sterile gloves – ref 111
BC draw through a needleless connector – 40, 115 (update: new INS Standards)
Order of draw – ref 125,126
Discarding initial aliquot – ref 131-134
Competency program – ref 148
Identification of BC rates by person drawing specimen – ref see article
Possible false-positive CLABSI reporting – see article, ref 153 **J. Boyce**
Thank you……Questions?