the diagnosis of haemoglobinopathies from protein to - enerca
TRANSCRIPT

The diagnosis of haemoglobinopathies from protein to genome
Béatrice Gulbis, MD, PhD
Hôpital Erasme – Université Libre de Bruxelles
2
Objectives of laboratory tests
• Prevention • Screening for haemoglobinopathies > genetic counselling
• Diagnostic purposes: symptomatic patient • Chronic haemolytic anaemia
– Sickle cell disease and syndromes
– Thalassaemia or
– Unstable Hb variant
• Polycythaemia
– Hb variants of high oxygen affinity
• Cyanosis
– M Haemoglobin

3
Available tools?
History Physical examination
Laboratory
tests

Diagnosis of haemoglobinopathies
from protein to genome
First step
Clinical settings
4

5
Clinical settings
• Diagnosis of patients
(Healthy carriers)
• Family history (recessive vs dominant)
• Population at risk (origin, inbreeding)
• Symptoms/signs
• Acute and/or chronic
• Age at first symptoms/signs

6
Age at first onset
2 1 5’
3’ 16:
11: 3’
5’
Hb F
Hb A (95-98%)
Hb A2 (2-3.5%)
Haeme Haeme
Haeme Haeme
7
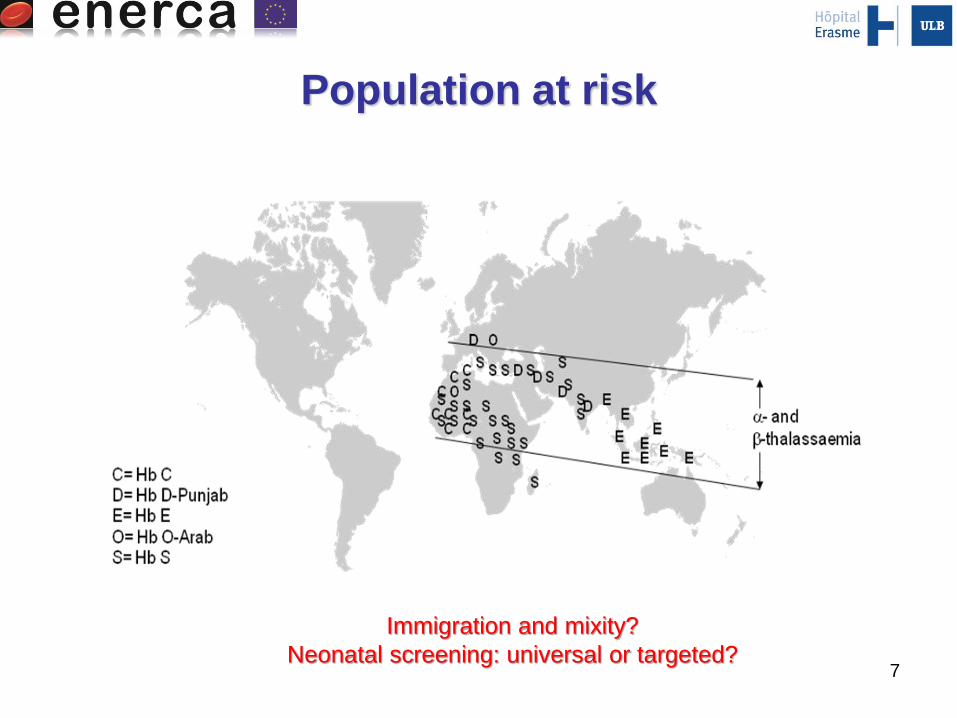
Population at risk
Immigration and mixity?
Neonatal screening: universal or targeted?

8
Physical exam(symptomatic patients)
Palor
Icterus
Splenomegaly
Hepatomegaly
Hb at high oxygen affinity Hb M Frequent …

Diagnosis of haemoglobinopathies
from protein to genome
First step
Clinical settings
Second step
First line laboratory
tests
9
10
Laboratory tests
• Complete blood count
• Blood smear
• Reticulocytes (absolute count, index)
• Indices of haemolysis
• Separation and quantitation of Hb fractions

11
Hb fractions
• Available methods
– Electrophoresis
– Chromatography
– Mass spectrometry
– Others

12
Hb fractions
• Each technique is based on a different
principle of separation of Hb fractions
Variable sensitivity and specificity

13
Hb fractions
Isoelectric focalisation
N
A F
S
C A2
No quantification

14
Hb fractions (quantification)
Automated capillary electrophoresis
Hb A Hb X (Z5 zone)

15
Hb fractions (quantification)
High performance chromatography
Hb A Hb X (S-window)

16
Hb fractions (quantification)
Chromatography: HbA1c methods
Hb X Hb X (S-window)

17
Hb fractions
Mass spectrometry
Trypsin
digest

18
Hb fractions
• Available methods
– Electrophoresis
– Chromatography
– Mass spectrometry
– Others

19
Presence of Hb S?
• Emmel test (sodium metabisulfite)
– One drop of blood and hypoxia generatted by 2% Na MB.
• Itano test (degree of solubility of Hb) – Hb S precipitates in the presence of Na dithionite – Phosphate
buffer

Characterization of the Hb variant: Why?
20
A
F
X
S
A
F
X
S
Hb S Korle-Bu
Asymptomatic Hb SD Punjab
Sickle cell disorder
"A2
window"
"D-window"

• Homozygous
– Hb SS
• Heterozygous
– Hb SC
– Hb SDPunjab
– Hb SOArab
– …
– Hb Sthalassemia
• Heterozygous
– Hb ASAntilles
21
Characterization of the Hb variant: Why?

Characterization of the Hb variant: Why?
Influence of HbS polymerization
• Increase
– Hb C
– Hb D Punjab
– Hb O Arab
– ...
• Decrease
– Hb F
– Hb Korle-Bu
– Hb G Philadelphia
– ...
22

Quantify the variant: Why?
23
A
F S
S.M. (29/07/1996): Hb AS ?
S
56%
F
25%
A
13%
Hb fractions
1 • Separation and quantification of Hb fractions
2
• Presence of Hb variant
• Using a second method of different separation principle
3 • Give a conclusion
• Interpretation of the different techniques used
24

External Quality Control
• ENERCA recommendations
– Recommendations for preconceptional or
antenatal screening, prenatal diagnosis and
genetic counselling of haemoglobinopathies.
• European Molecular Genetics Quality
Network – Best practice (2002 and under
revision)
– Best Practice Guidelines for carrier
identification and prenatal diagnosis of
haemoglobinopathies -
http://www.emqn.org/emqn/Best+Practice
25

Diagnosis of haemoglobinopathies
from protein to genome
First step
Clinical settings
Second step
First line laboratory tests
Third step
Specialized tests
26

27
Laboratory tests
Additional tests
• Haemoglobinopathy
– Phenotype:
• Separation/quantification of Hb fractions
• Hb variant: characterization
• Blood smear: specific staining
• OxyHb: dissociation curve
• Hb M: absorption spectrum
– Genotype

Additional tests
• p50Hb variant
dissociative curve
p50 calculation http://www.ventworld.com/res
ources/oxydisso/oxydisso.htm
l
28

29
Additional tests
• Unstable Hb variant?
– Isopropanol test
Unstable Hb variant: Flocculation

30
Additional tests
• Presence of Hb H (alpha-thalassaemia)?
– Brilliant cresyl blue staining
31 31
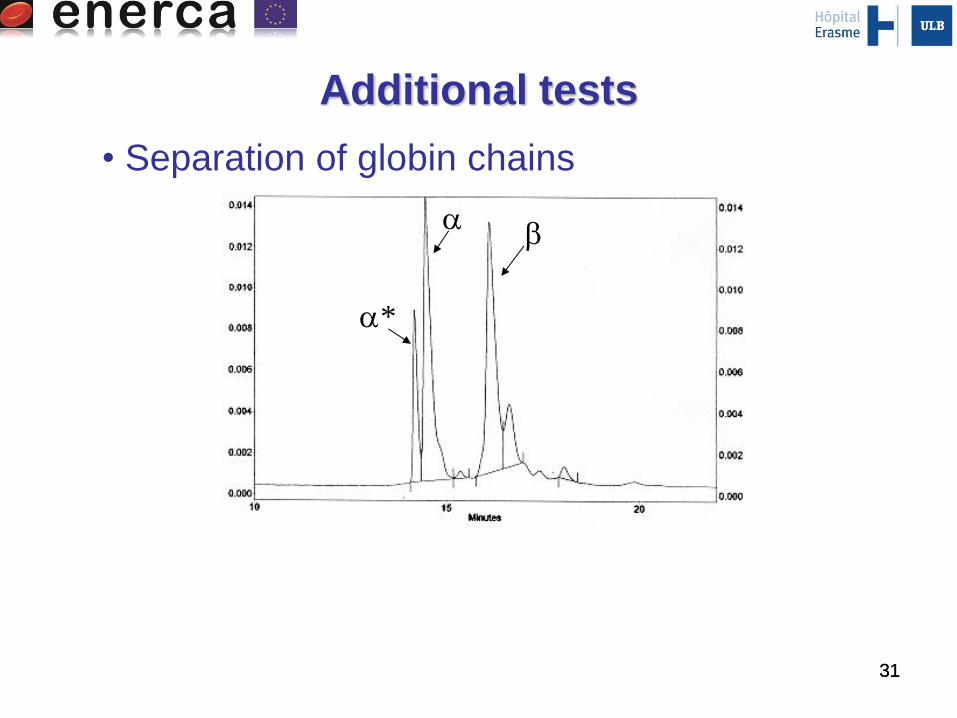
Additional tests
*
• Separation of globin chains

32
Laboratory tests
Additional tests
• Haemoglobinopathy
– Phenotype:
– Genotype

33
Molecular analysis
14.0 kb
10.3 kb
/ / -3.7
2
1
• Southern blot

34
Molecular analysis
• MLPA (Multiplex Ligation-dependent Probe Amplification)

35
Molecular analysis
• Sequencing

Next generation sequencing
36
- Gene panel sequencing
- Exomes
37
When to make the genotype?
• Diagnosis of
– -thalassaemia
– - thalassaemia (minor)
– Unusual Hb variant
– ALWAYS in the context of a prenatal
diagnosis

38
Home message
Based on the history and physical examination,
diagnostic approach in the laboratory:
Define the type of anemia and / or corpuscular
abnormality index
Establish the differential diagnosis
Achieve adequate complementary tests
Separation and quantification of Hb fractions are requested
At least two different principle of separation or identification
External quality control requested
Interpretation of the tests is helpful for the clinician
Be careful if based on a HbA1c method
Genotype is not always requested

Ackowledgment
• Belgian HematologicalSociety – Committee Red Blood Cells Disorders
www.bhs.be
• http://www.erasme.ulb.ac.be/files/files/Chimie/bilan_depistage_neonatal_hbpathies_2012.pdf
39