the dynamic changes of circulating ocn+ cells versus insulinlike growth factor-i during primary...
TRANSCRIPT

Vol. 113 No. 6 June 2012
The dynamic changes of circulating OCN� cells versus insulinlikegrowth factor-I during primary healing of orthognathic surgeriesXi Yang, MSc,a,b Xiao-an Tao, PhD,c Jian-qiang Liang, BSc,b Yi-jun Huang, MSc,d and Xiao-ping Yang, MD,a
Guangzhou, ChinaSUN YAT-SEN UNIVERSITY AND HAIZHU DISTRICT STOMATOLOGICAL HOSPITAL
Objective. The objective of this study was to determine the dynamic changes of circulating osteocalcin� (OCN�) cells andinsulinlike growth factor-I (IGF-I) in peripheral blood during early primary repair of jaw bones in patients with orthognathicsurgery.Study design. The expression of bone-related genes was detected by RT-PCR in circulating OCN� cells. The numbers ofOCN� cells and serum level of IGF-I were determined by flow cytometry, immunocytochemical staining, and ELISA.Results. OCN� cells significantly increased in peripheral blood, and reached the peak at 1 to 2 weeks after surgery(P � .05). IGF-I in patients significantly decreased 1 week after surgery (P � .05), and then returned gradually to the normallevel. There was no significant correlation between the number of circulating OCN� cells and the level ofIGF-I (P � .05).Conclusions. These findings suggested that circulating OCN� cells, at least in part, could be mobilized in response to boneinjury, and contribute to bone repair in patients with orthognathic surgery. (Oral Surg Oral Med Oral Pathol Oral Radiol
2012;113:734-740)Over the past decades, several investigators have pro-vided evidence that cells with osteoblastic potential thatadhere to plastic are, indeed, present in the circulationin some species, but in exceedingly low numbers (lessthan 1/108) of peripheral blood mononuclear cells(PBMCs) in adult humans.1,2 Long et al.3,4 identified apopulation of cells in the bone marrow (BM) that hadosteogenic potential and were nonadherent and positivefor osteocalcin: bone-specific alkaline phosphatase.The concentration of cells with osteogenic potential inperipheral blood has been vastly underestimated owingto the use of assays that required adherence to plastic.Based on this hypothesis, a few studies have provedthat circulating cells with osteogenic potential actuallyexist, originating from BM, in peripheral blood, includ-ing circulating osteocalcin� (OCN�) cells, circulatingendothelial progenitor cells (EPCs), and circulatingbone marrow–derived osteogenic progenitor cells(MOPCs).5-7
Eghbali-Fatourechi et al.5 successfully identified thatcirculating nonadherent OCN� cells, which were de-
aDepartment of Oral and Maxillofacial Surgery, Guanghua School ofStomatology, Sun Yat-sen University, Guangzhou, China.bHaizhu District Stomatological Hospital, Guangzhou, China.cDepartment of Oral Medicine, Guanghua School of Stomatology,Sun Yat-sen University, Guangzhou, China.dDepartment of Pharmacology, Zhongshan School of Medicine, SunYat-sen University, Guangzhou, China.Received for publication Mar 6, 2011; returned for revision Apr 25,2011; accepted for publication May 19, 2011.© 2012 Elsevier Inc. All rights reserved.2212-4403/$ - see front matter
doi:10.1016/j.tripleo.2011.05.044734
tected in the peripheral blood of adult subjects (1%-2%of mononuclear cells), expressed osteoblastic genes,formed mineralized nodules in vitro, and formed bonein an in vivo transplantation assay. Furthermore, theyobserved that the percentage of cells positive for osteo-calcin increased markedly in 3 adults with recent frac-tures.5 Whereafter, Gössl et al.8 reported that a higherpercentage of EPCs expressed OCN in patients withcoronary atherosclerosis as compared with subjectswith normal endothelial functions and no structuralcoronary artery disease. Recently, Pal et al.9 observedthat circulating OCN� cells were involved in the onsetof aortic calcification and were related to the severity ofaortic calcification. All these reports indicated that cir-culating OCN� cells could function as osteoblasts andcould be supplied via the circulation for bone regener-ating and ectopic bone formation in vivo. However, thedynamic changes of circulating OCN� cells duringfracture healing have not been fully identified.5
Insulinlike growth factor-I (IGF-I), one of the mostabundant growth factors in bone matrix, has a clear rolein fracture healing by increasing cell proliferation andmatrix synthesis.10 Recent studies documented thatIGF-I induced mesenchymal stem cells into an osteo-genic lineage and directly stimulated cell migration ofhuman mesenchymal progenitor cells in vitro.11,12 Inaddition, systemically injected IGF-I–transduced mes-enchymal cells were able to return to and repopulate thebone marrow.13 These data suggested that IGF-I maycontribute to fracture healing by stimulating differenti-ation and migration of mesenchymal progenitor cells
with osteogenic potential.
OOOO ORIGINAL ARTICLEVolume 113, Number 6 Yang et al. 735
Orthognathic surgery is an effective approach totreat various maxillofacial deformities, includingprognathism, retrognathism, asymmetries, and openbite. Since the first orthognathic surgical procedurewas reported by Simon Hullihen in the American Jour-nal of Dental Science, orthognathic surgeries havemade great improvement in past decades, includingbilateral ramus osteotomies, sagittal split osteotomy,bilateral split osteotomy, and intraoral vertical ramusosteotomy. Generally, orthognathic surgery was basedon anthropogenic jaw fracture. Although previous stud-ies proved that circulating nonadherent OCN� cellscould function as osteoblasts and be supplied via thecirculation for bone regenerating in vivo, the dynamicchanges of these cells during fracture healing have notbeen fully demonstrated. Therefore, we designed thissmall pilot study to determine the dynamic changes ofcirculating nonadherent OCN� cells and IGF-I, andexplore the correlation between the quantity of OCN�
cells and the level of IGF-I in peripheral blood duringearly primary repair of jaw bones in patients withorthognathic surgery.
MATERIAL AND METHODSStudy subjectsStudy subjects included 9 healthy adults (5 males and 4females, mean: 26.3 � 1.7 years) and 10 consecutivelyrecruited patients receiving orthognathic surgery (4males and 6 females, mean: 21.1 � 0.9 years). Periph-eral blood samples from these 9 healthy adults (50 mLeach) were used to analyze the expression of bone-related genes in circulating OCN� cells sorted by flu-orescence-activated cell-sorter. Blood samples obtainedfrom 10 surgery subjects (before and after operations)were detected by flow cytometry and immunohistochem-istry (IHC) to determine the dynamic changes of OCN�
cells in peripheral blood. All studies were approved bythe institutional review board at the Sun Yat-sen Uni-versity, and all subjects provided written informed con-sent. None of the subjects had history, symptoms,and/or signs of systematic infections, allergies, orsmoking in the preceding 3 months.
Flow cytometry and fluorescence-activated cellsorter analyses of OCN� cellsTo detect the dynamic changes of OCN� cells in pe-ripheral blood, blood samples were obtained from 9healthy adults and 10 patients before and after theoperations (1 week, 2 weeks, and 4 weeks postopera-tion). PBMCs were prepared from heparinized venousblood by density gradient centrifugation with lym-phoprep (AXIS-SHIELD Inc., Oslo, Norway). Then,cells were immediately processed for immunostaining
for detecting OCN� cells by flow cytometry as previ-ously described.5 Primary antibody was a goat poly-clonal antihuman osteocalcin antibody (Santa CruzBiotechnology, Inc., Santa Cruz, CA). Control isotypeantibodies were used at the same concentrations as theprimary antibodies. In brief, appropriate primary anti-body was added in 100-�L prepared cells and incu-bated for 30 minutes in the dark at 4°C. After that, cellswere washed and stained with fluorescein isothiocya-nate–conjugated Affinity Pure IgG f(ab=)2 fragmentdonkey antigoat antibody (Jackson ImmunoResearchLaboratories, Inc., West Grove, PA). The flow cytom-etry analyses of OCN� cells were done according to theprocedure that was described in a previous study.5 TheWINMDI 2.9 software (The Scripps Research Institute,La Jolla, CA) was used to quantify the fluorescencesignals and to set the logical electronic-gating param-eters. More than 50,000 PBMCs were acquired foranalyses of OCN� cells. For the reverse transcriptase–polymerase chain reaction (RT-PCR) analysis, mono-nuclear cells stained with the anti-osteocalcin antibodyand the corresponding secondary antibody were alsosorted by flow cytometry (EPICS ALTRA Flow Cyto-sorter, Beckman Coulter, Brea, CA) directly into agrowth medium consisting of MesenCult Basal Me-dium (Stemcell Technologies, Inc., Vancouver, Can-ada) supplemented with 10% fetal calf serum.
RNA extraction and RT-PCR analysisTotal RNA was extracted from cells collected by fluo-rescence-activated cell sorting with TRIzolagent (Invit-rogen Life Technologies, Carlsbad, CA) according tothe manufacturer’s recommendations. The RNA purityand yield were measured by spectrophotometric absor-bance at 260 and 280 nm. The quality of the isolatedRNA samples was routinely confirmed by examiningthe integrity of 28S and 18S ribosomal RNA bands byelectrophoresis on agarose gels. Five hundred nano-grams of total RNA was reverse transcribed into com-plementary DNA (cDNA) with avian myelobastosisvirus (AMV) reverse transcriptase in a 10-�L reversetranscription system (Takara Bio, Inc., Kyoto, Japan).cDNA was synthesized from RNA samples of eachgroup at the same time to limit differences in theefficiency of the cDNA synthesis. Synthesized cDNAwas amplified by PCR using messenger RNA (mRNA)-specific primers to generate products corresponding tomRNA encoding human OCN, alkaline phosphatase(ALK), collagen type I alpha chain 1 (COL1A), and thehousekeeping gene glyceraldehyde-3-phosphate dehy-drogenase (GAPDH) using Takara RNA PCR Kit(AMV) Ver. 3.0 (Takara Bio, Inc.). The specific prim-ers were reported in previous studies.14 The mRNA-specific primer sequences, PCR product sizes, and op-
timized PCR conditions are presented in Table I.
CAGT
ORAL AND MAXILLOFACIAL SURGERY OOOO736 Yang et al. June 2012
Immunocytochemical stainingThe cytospins of PBMCs were prepared according tothe procedure described in a previous study with minorrevision.15 PBMCs isolated from peripheral blood werewashed twice with phosphate-buffered saline (PBS)and resuspended to a final concentration of 1 � 106
cells/mL. Cells were well mixed before being trans-ferred into cytofunnels for cytospin preparation. Then,the cytospin slides were fixed for 5 minutes in 2%paraformaldehyde (dissolved in pH 7.2 PBS) at roomtemperature and washed 3 times in PBS. Slides wereair-dried, wrapped in foil, and frozen at –80°C. Theimmunocytochemical method used in this study is de-scribed as follows. Briefly, endogenous peroxidase ac-tivity was quenched in 0.3% hydrogen peroxide in PBS
Fig. 1. RT-PCR analysis for expression of mRNA for bone-related genes in circulating OCN� cells collected by FACS.Current results provided clear evidence that the expression ofthe bone-related genes, including ALP (1), COLA1 (2), andOCN (3), was detected in circulating OCN� cells by RT-PCR. GAPDH (4) was used as internal control. Conditions forRT-PCR and the primers used are described in the Materialand Methods section.
Table I. Specific primers for RT-PCR with expected fGene GenBank no. Primer sequence (5=–
ALP NM_000478 Sense: CCAACGTGGCTAAGAAAntisense: CATCTCGTTGTCTG
COL-1 NM_000088 Sense: CGGCAAGGTGTTGTGCAntisense: CACGGAAATTCCTC
OCN NM_199173 Sense: GGTGCAGCCTTTGTGTAntisense: GTCAGCCAACTCGT
GAPDH NM_002046 Sense: CATGGAGAAGGCTGGGAntisense: CACTGACACGTTGG
for 15 minutes at 37°C. Nonspecific binding was
blocked by incubating the slides for 10 minutes innormal goat serum, and subsequently with the primaryanti-OCN antibody (clone: SCV-19, dilution: 1:100,Santa Cruz Biotechnology, Inc.) at room temperaturefor 1 hour. Detection was carried out using the relevantbiotin-conjugated secondary antibody, followed bystreptavidin-peroxidase complex (Lab Vision, Co., Fre-mont, CA) for 15 minutes at room temperature. Allstages were separated by PBS washes, and the finalproduct was visualized by a diaminobenzidine (DAB)substrate kit for 5 minutes. The sections were thencounterstained with hematoxylin. Control isotype anti-body was substituted for the primary antibody as anegative control. Isotype antibody was used at the sameconcentrations as the primary antibodies.
Two investigators determined the number of OCN�
cells in all slides independently. OCN� cells werecounted in the 10 consecutive areas at �400 magnifi-cation by light microscopy. The percentage of positiveimmunoreactive cells was determined by the number ofpositive cells (yellow cells) on total cell count of thestudied cell type identified by hematoxylin staining(blue and yellow cells).
Enzyme-linked immunosorbent assay analysisfor IGF-IThe concentrations of IGF-I in serum of patientswere determined using an enzyme-linked immu-nosorbent assay (ELISA) kit (Boster, Inc., Wuhan,China), according to the manufacturer’s protocol. Inbrief, the 96-well plates were coated with 0.1 mL/well of capture antibody and incubated at 4°C over-night. Then, 0.2 mL/well assay diluents were addedto block nonspecific reaction at room temperature for2 hours. After that, 0.1 mL/well of samples andstandard were added to appropriate wells, and two-fold serial dilutions of standard were performed tomake the standard curve. Then, the plates weresealed and incubated at room temperature for 2hours. After washing plates, 0.1 mL/well of the de-tection antibody was added and the plates were in-cubated at room temperature for 1 hour again. Then,0.1 mL/well of avidin-horseradish peroxidase was
nt size and optimal annealing temperatureAnnealing temperature, °C Fragment, base pair
CC58 434
TG58 339
CGTCC
62 159
GG62 415
ragme3=)
TGTCAGTAGATGCGGT
CCAAGCACAGCTC
added into each well and incubated at room temper-

OOOO ORIGINAL ARTICLEVolume 113, Number 6 Yang et al. 737
ature for 30 minutes. Substrate solution was thenadded, plates were incubated for 15 minutes, and thereaction was terminated by the addition of stop so-lution. Finally, the concentration of cytokines wascalculated from the colorimetric optical density,which was read at 450 nm. The measurement of totalprotein and ELISA analysis were done in duplicate,and the data were calculated from mean of 2 tests foreach sample.
Statistical analysisAll calculations were performed using the SPSS statis-
Fig. 2. Flow cytometric analyses of OCN� cells in periphprevalence of circulating OCN� cells in peripheral bloodcontrol; B, preoperation; C, 1 week postoperation; D, 2 weekcolor at www.ooooe.net.
tical software package (SPSS 11.0 for Windows, SPSS,
Inc., Chicago, IL). Results were expressed as mean �SD. All data were analyzed by paired t test. A P valueless than .05 was considered to be statistically signifi-cant.
RESULTSThe proportion of circulating OCN� cells were 3.32% �0.86% of PBMCs of young Chinese adults. The expres-sions of the bone-related genes, including OCN, ALP, andCOL-1 (collagen type 1) were detected in circulatingOCN� cells by RT-PCR (Fig. 1). In addition, the propor-tion of circulating OCN� cells is negatively correlated
ood of patients before and after orthognathic surgery. Thegnificantly increased after orthognathic surgery. A, Isotypeoperation; E, 4 weeks postoperation. Images are available in
eral blwas sis post
with the age of the patients (R � –0.691, P � .039).
ORAL AND MAXILLOFACIAL SURGERY OOOO738 Yang et al. June 2012
These findings were consistent with those of Eghbali-Fatourechi et al.5
Fig. 2 shows the proportions of circulating OCN�
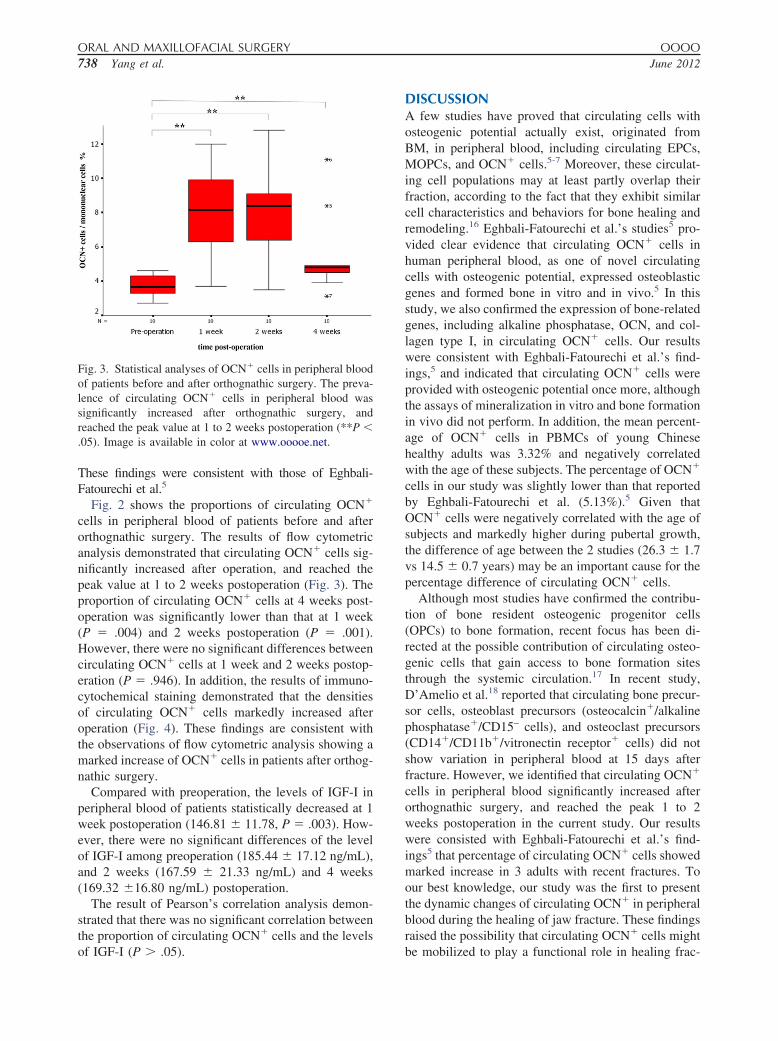
cells in peripheral blood of patients before and afterorthognathic surgery. The results of flow cytometricanalysis demonstrated that circulating OCN� cells sig-nificantly increased after operation, and reached thepeak value at 1 to 2 weeks postoperation (Fig. 3). Theproportion of circulating OCN� cells at 4 weeks post-operation was significantly lower than that at 1 week(P � .004) and 2 weeks postoperation (P � .001).However, there were no significant differences betweencirculating OCN� cells at 1 week and 2 weeks postop-eration (P � .946). In addition, the results of immuno-cytochemical staining demonstrated that the densitiesof circulating OCN� cells markedly increased afteroperation (Fig. 4). These findings are consistent withthe observations of flow cytometric analysis showing amarked increase of OCN� cells in patients after orthog-nathic surgery.
Compared with preoperation, the levels of IGF-I inperipheral blood of patients statistically decreased at 1week postoperation (146.81 � 11.78, P � .003). How-ever, there were no significant differences of the levelof IGF-I among preoperation (185.44 � 17.12 ng/mL),and 2 weeks (167.59 � 21.33 ng/mL) and 4 weeks(169.32 �16.80 ng/mL) postoperation.
The result of Pearson’s correlation analysis demon-strated that there was no significant correlation betweenthe proportion of circulating OCN� cells and the levels
Fig. 3. Statistical analyses of OCN� cells in peripheral bloodof patients before and after orthognathic surgery. The preva-lence of circulating OCN� cells in peripheral blood wassignificantly increased after orthognathic surgery, andreached the peak value at 1 to 2 weeks postoperation (**P �.05). Image is available in color at www.ooooe.net.
of IGF-I (P � .05).
DISCUSSIONA few studies have proved that circulating cells withosteogenic potential actually exist, originated fromBM, in peripheral blood, including circulating EPCs,MOPCs, and OCN� cells.5-7 Moreover, these circulat-ing cell populations may at least partly overlap theirfraction, according to the fact that they exhibit similarcell characteristics and behaviors for bone healing andremodeling.16 Eghbali-Fatourechi et al.’s studies5 pro-vided clear evidence that circulating OCN� cells inhuman peripheral blood, as one of novel circulatingcells with osteogenic potential, expressed osteoblasticgenes and formed bone in vitro and in vivo.5 In thisstudy, we also confirmed the expression of bone-relatedgenes, including alkaline phosphatase, OCN, and col-lagen type I, in circulating OCN� cells. Our resultswere consistent with Eghbali-Fatourechi et al.’s find-ings,5 and indicated that circulating OCN� cells wereprovided with osteogenic potential once more, althoughthe assays of mineralization in vitro and bone formationin vivo did not perform. In addition, the mean percent-age of OCN� cells in PBMCs of young Chinesehealthy adults was 3.32% and negatively correlatedwith the age of these subjects. The percentage of OCN�
cells in our study was slightly lower than that reportedby Eghbali-Fatourechi et al. (5.13%).5 Given thatOCN� cells were negatively correlated with the age ofsubjects and markedly higher during pubertal growth,the difference of age between the 2 studies (26.3 � 1.7vs 14.5 � 0.7 years) may be an important cause for thepercentage difference of circulating OCN� cells.
Although most studies have confirmed the contribu-tion of bone resident osteogenic progenitor cells(OPCs) to bone formation, recent focus has been di-rected at the possible contribution of circulating osteo-genic cells that gain access to bone formation sitesthrough the systemic circulation.17 In recent study,D’Amelio et al.18 reported that circulating bone precur-sor cells, osteoblast precursors (osteocalcin�/alkalinephosphatase�/CD15– cells), and osteoclast precursors(CD14�/CD11b�/vitronectin receptor� cells) did notshow variation in peripheral blood at 15 days afterfracture. However, we identified that circulating OCN�
cells in peripheral blood significantly increased afterorthognathic surgery, and reached the peak 1 to 2weeks postoperation in the current study. Our resultswere consisted with Eghbali-Fatourechi et al.’s find-ings5 that percentage of circulating OCN� cells showedmarked increase in 3 adults with recent fractures. Toour best knowledge, our study was the first to presentthe dynamic changes of circulating OCN� in peripheralblood during the healing of jaw fracture. These findingsraised the possibility that circulating OCN� cells might
be mobilized to play a functional role in healing frac-
OOOO ORIGINAL ARTICLEVolume 113, Number 6 Yang et al. 739
tures in portions of the peripheral skeleton not adjacentto red marrow in patients with orthognathic surgery.Certainly, we realize that the sample size in this studywas not large enough. In addition, the severity of frac-ture was not considered in our study.
Heretofore, the exact mechanisms of circulating cellswith osteogenic potential contributing to fracture heal-ing and bone remodeling are unclear. In the studiesreported by Eghbali-Fatourechi et al.,19 37% circulatingOCN� cells expressed the hematopoietic/endothelialmarker CD34, which suggested significant overlap be-tween circulating cells expressing OCN and those ex-pressing the hematopoietic/endothelial marker CD34.This finding had been independently confirmed by Ma-tsumoto et al.20 and Gössl and colleagues,8 who iden-tified that part of circulating CD34� cells expressed theOCN, mRNA, and protein. In addition, when infusedinto immunocompromised rats following femur frac-tures, circulating CD34� cells could localize to thefracture site and differentiate into endothelial cells, aswell as osteoblasts, and enhance fracture healing.8,20
Based on these findings, we presume that circulatinghuman OCN� cells may participate in fracture healing
Fig. 4. Immunocytochemical staining for OCN� cells in perresults of immunocytochemical analysis indicated that the fresubjects after orthognathic surgery. A, Preoperation; B, 1 wetion. Images are available in color at www.ooooe.net.
of patients with orthognathic surgery by contributing
both to vasculogenesis and osteogenesis, although fur-ther work is needed to test this hypothesis.
Recent studies documented that IGF-I induced dif-ferentiation of mesenchymal stem cells into an osteo-genic lineage, and stimulated directed cell migration ofhuman mesenchymal progenitor cells in vitro.11,12
More importantly, systemically administered mesen-chymal stromal cells transduced with IGF-I localizedpreferentially to a fracture site and accelerated fracturehealing in vivo.13 These data suggested that IGF-I maycontribute to fracture healing by stimulating differenti-ation and migration of mesenchymal progenitor cellswith osteogenic potential. In our study, however, therewere no significant correlations between the proportionof circulating OCN� cells and IGF-I levels in patientswith orthognathic surgery throughout the study period.The results indicated that mobilization of circulatingOCN� cells was not a result of IGF-I in patients withorthognathic surgery. Recently, Otsuru et al.21 demon-strated that circulating OPCs were recruited to thebone-forming site by the CXCR4/stromal cell–derivedfactor-1 pathway (SDF-1). Considering that the circu-lating cell populations with osteogenic potential, in-
blood of patients before and after orthognathic surgery. Theof peripheral OCN� cells demonstrated marked increase in
toperation; C, 2 weeks postoperation; D, 4 weeks postopera-
ipheralquencyek pos
cluding circulating OCN� cells, EPCs, and MOPCs,

ORAL AND MAXILLOFACIAL SURGERY OOOO740 Yang et al. June 2012
may overlap their fraction,16 it seems possible that theCXCR4/SDF-1 pathway may also play an importantrole in mobilization and recruitment of circulatingOCN� cells in patients with orthognathic surgery. Therelated study is in progress in our laboratory.
In sum, our findings collectively suggest that circu-lating OCN� osteoblast-lineage cells, at least in part,can be mobilized in response to bone injury, and con-tribute to bone repair during the early stage of fracturehealing in patients with orthognathic surgery. Cer-tainly, the exact mechanism for mobilization and re-cruitment of circulating OCN� cells needs to be deter-mined in further studies.
We thank all volunteers for their cooperation in currentstudy.
REFERENCES1. Zvaifler NJ, Marinova-Mutafchieva L, Adams G, Edwards CJ,
Moss J, Burger JA, et al. Mesenchymal precursor cells in theblood of normal individuals. Arthritis Res 2000;2:477-88.
2. Kuznetsov SA, Mankani MH, Gronthos S, Satomura K, BiancoP, Robey PG. Circulating skeletal stem cells. J Cell Biol2001;153:1133-40.
3. Long MW, Williams JL, Mann KG. Expression of human bone-related proteins in the hematopoietic microenvironment. J ClinInvest 1990;86:1387-95.
4. Long MW, Robinson JA, Ashcraft EA, Mann KG. Regulation ofhuman bone marrow-derived osteoprogenitor cells by osteogenicgrowth factors. J Clin Invest 1995;95:881-7.
5. Eghbali-Fatourechi GZ, Lamsam J, Fraser D, Nagel D, RiggsBL, Khosla S. Circulating osteoblast-lineage cells in humans.N Engl J Med 2005;352:1959-66.
6. Lee DY, Cho TJ, Kim JA, Lee HR, Yoo WJ, Chung CY, et al.Mobilization of endothelial progenitor cells in fracture healingand distraction osteogenesis. Bone 2008;42:932-41.
7. Otsuru S, Tamai K, Yamazaki T, Yoshikawa H, Kaneda Y. Bonemarrow-derived osteoblast progenitor cells in circulating bloodcontribute to ectopic bone formation in mice. Biochem BiophysRes Commun 2007;354:453-8.
8. Gössl M, Mödder UI, Atkinson EJ, Lerman A, Khosla S. Osteo-calcin expression by circulating endothelial progenitor cells inpatients with coronary atherosclerosis. J Am Coll Cardiol2008;52:1314-25.
9. Pal SN, Rush C, Parr A, Van Campenhout A, Golledge J.Osteocalcin positive mononuclear cells are associated with theseverity of aortic calcification. Atherosclerosis 2010;210:88-93.
10. Tran GT, Pagkalos J, Tsiridis E, Narvani AA, Heliotis M, Man-
talaris A, et al. Growth hormone: does it have a therapeutic rolein fracture healing? Expert Opin Investig Drugs 2009;18:887-911.
11. Koch H, Jadlowiec JA, Campbell PG. Insulin-like growth fac-tor-I induces early osteoblast gene expression in human mesen-chymal stem cells. Stem Cells Dev 2005;14:621-31.
12. Fiedler J, Brill C, Blum WF, Brenner RE. IGF-I and IGF-IIstimulate directed cell migration of bone-marrow-derived humanmesenchymal progenitor cells. Biochem Biophys Res Commun2006;345:1177-83.
13. Shen FH, Visger JM, Balian G, Hurwitz SR, Diduch DR. Sys-temically administered mesenchymal stromal cells transducedwith insulin-like growth factor-I localize to a fracture site andpotentiate healing. J Orthop Trauma 2002;16:651-9.
14. Truong LH, Kuliwaba JS, Tsangari H, Fazzalari NL. Differentialgene expression of bone anabolic factors and trabecular bonearchitectural changes in the proximal femoral shaft of primaryhip osteoarthritis patients. Arthritis Res Ther 2006;8:R188.
15. St-Laurent J, Boulay ME, Prince P, Bissonnette E, Boulet LP.Comparison of cell fixation methods of induced sputum speci-mens: an immunocytochemical analysis. J Immunol Methods2006;308:36-42.
16. Matsumoto T, Kuroda R, Mifune Y, Kawamoto A, Shoji T,Miwa M, et al. Circulating endothelial/skeletal progenitor cellsfor bone regeneration and healing. Bone 2008;43:434-9.
17. Khosla S, Eghbali-Fatourechi GZ. Circulating cells with osteo-genic potential. Ann N Y Acad Sci 2006;1068:489-97.
18. D’Amelio P, Cristofaro MA, Grimaldi A, Ravazzoli M, PluvianoF, Grosso E, et al. The role of circulating bone cell precursors infracture healing. Calcif Tissue Int 2010;86:463-9.
19. Eghbali-Fatourechi GZ, Mödder UI, Charatcharoenwitthaya N,Sanyal A, Undale AH, Clowes JA, et al. Characterization ofcirculating osteoblast lineage cells in humans. Bone 2007;40:1370-77.
20. Matsumoto T, Kawamoto A, Kuroda R, Ishikawa M, Mifune Y,Iwasaki H, et al. Therapeutic potential of vasculogenesis andosteogenesis promoted by peripheral blood CD34-positive cellsfor functional bone healing. Am J Pathol 2006;169:1440-57.
21. Otsuru S, Tamai K, Yamazaki T, Yoshikawa H, Kaneda Y.Circulating bone marrow-derived osteoblast progenitor cells arerecruited to the bone-forming site by the CXCR4/stromal cell-derived factor-1 pathway. Stem Cells 2008;26:223-34.
Reprint requests:
Xiao-ping Yang, MDDepartment of Oral and Maxillofacial SurgeryGuanghua School of StomatologySun Yat-sen University56 Linyuanxi RoadGuangzhou, 510060, China
[email protected]