the early phase of experimental acute renal failure
TRANSCRIPT

Pfl/igers Arch (i981) 392: 125- 133 Pflfigers Archiv
European Joumal of Physiology
�9 Springer-Verlag 1981
The Early Phase of Experimental Acute Renal Failure
VI. The Influence of Furosemide
June Mason, Hermann Kain, Johanna Welsch, and Jtirgen Schnermann with the technical assistance of Elizabeth Murdaugh, Paulo Faltay, Sigrid P~itz, and Maria Steff
Physiologisches Institut, Universitfit Mflnchen, PeUenkoferstrasse 12, D-8000 Mfinchen 2, Federal Republic of Germany
Abstract. Experiments were performed to determine whether furosemide, given in doses high enough to induce a strong diuresis and to inhibit the mechanism of tubuloglomerular feedback, offers any protection from acute renal failure induced by a nephrotoxin or ischaemia. Microperfusion of the loop of Henle revealed that a tubular furosemide con- centration of 5 - 10 -s mol - I-1 was necessary to fully inhibit the tubuloglomerular feedback response to a raised sodium chloride concentration at the macula densa. The infusion of furosemide systemically to achieve such concentrations in the tubule resulted in an improvement in renal function when given before or after the nephrotoxin but was without effect when given before or after ischaemia. Measurements of furosemide concentrations in the urine, however, confirmed that sufficient amounts were applied to inhibit the feedback mechanism. It is concluded from this and similar studies that furosemide is only beneficial in models of acute renal failure with an obstructive or nephrotoxic pathogenesis, in which it acts by flushing out the noxious material and not by inhibiting the mechanism of tubuloglomerular feedback.
Key words: Acute renal failure - Furosemide - Inulin clearance - Tubuloglomerular feedback
Introduction
The use of potent diuretics in the therapy of acute renal failure has been met with conflicting enthusiasm; although some investigators have claimed that furosemide in high doses improves renal function [3], or shortens the duration of renal insufficiency [9, 10], others have been unable to confirm any improvement [7, 14, 26, 37, 39]. An examination of the efficacy of furosemide treatment in experimental acute renal failure, in which the aetiology is clearly defined and renal function can be precisely measured, far from achieving any clarity, has led to equally conflicting views ; for each of the three major classes of acute renal failure - induced by ischaemia, nephrotoxins or haeme pigments - studies are available which report an improvement in renal function [2, 28, 38, 42, 51-53], no influence of furosemide [2, 20, 21, 27, 29, 4l, 54] and even a detrimental effect [2, 30]. However, inadequate attention to fluid substitution [21, 29], or to electrolyte replacement - particularly potassium replace-
Send offprint requests to J. Mason at the above address
ment [2, 20, 21, 27, 29, 41, 54] - may explain the lack of improvement with furosemide in many studies.
There are a number of reasons why treatment with furosemide might be anticipated to be beneficial during acute renal failure : the maintenance of a hefty flow of urine may prevent the accumulation of cellular debris within the tubules or the formation of pigment casts and circumvent obstruc- tion; the excretion of a larger portion of the filtrate may enhance the elimination of filtered toxins and substances which become noxious after prolonged contact with the tubular epithelium; furosemide may, by directly increasing renal blood flow, augment filtration rate; it could, by inhibiting the mechanism of tubuloglomerular feedback [58], prevent the decrease in filtration rate which would otherwise occur if deficient tubular reabsorption led to an increase in macula densa sodium chloride concentration [32]. Thus, relief or prevention of obstruction, accelerated excretion of toxins and a renal vasodilatation are all possible means by which furosemide could improve renal function in acute renal failure.
The present experiments were designed to determine whether the application of furosemide in doses high enough to both induce a maximal diuresis and to inhibit the mechanism oftubuloglomerular feedback hinders the impair- ment of renal function which follows renal damage, and whether it has any prophylactic properties. For this purpose, furosemide was given systemically just prior to or just after a neprotoxic or ischaemic insult, and renal function was monitored for several hours. The investigation was conducted on two experimental models, an ischaemic model, charac- terized neither by tubular obstruction [34] nor by tubular leakiness to inulin [40] and a uranyl nitrate model, similar to one reported to show mild signs of 0bstruction but no leakage to inulin [6], under conditions of rigorously maintained fluid and electrolyte balance. Thus, it was assumed that any alterations in inulin clearance would reflect changes in filtration rate of renal origin, any would be influenced only minimally by artefacts or variations in extracellular volume or composition.
Methods
Clearance Experiments and Experimental Models
The animals were anaesthetized with Inactin (Byk Gulden, Konstanz), 110- 120 rag- kg- 1, for the surgical preparation. Catheters were placed in the trachea, right jugular vein, right and left femoral arteries and urinary bladder. For the
0031-6768/81/0392/0125/$01.80

126
Fig. 1. Illustrates the method used to produce bilateral renal ischaemia. Each kidney was exposed through a flank incision, a portion of the renal artery freed from the vein and a length of wet catgut placed underneath it, as illustrated for the left kidney in the left panel. The animal was then placed in a prone position and the catgut streched tight across its back, as shown in the centre panel. The kidneys are easily accessible in this position, as depicted in the right panel, enabling the lack of blood flow to be confirmed at all times
determination of renal function 7 - 1 0 g. 100 ml- 1 polyfruc- tosan (Inutest, Linz, Austria) or 1 - 6 g C i . ml 1 3H inulin (New England Nuclear, Dreieich, FRG) dissolved in isotonic saline was administered through one of the jugular catheters as 0 .25-0.40ml.100g -1 prime initially, followed by a constant infusion of 0 . 3 - 0.6 ml. h- 1. 100 g- 1. Urine sam- ples were collected for 30rain periods from the bladder catheter and blood samples were taken at the mid-point of the urine collection from the femoral arterial catheter also used to monitor blood pressure. The application of furosemide was undertaken through the second femoral arterial catheter, whose tip had been advanced into the aorta, because it was shown in preliminary experiments to have adverse effects on blood pressure when given in high doses into the jugular vein. Fluid replacement during diuresis was achieved by infusing into the other jugular vein a modified Ringer's solution, shown in preliminary experiments to supply sufficient free water and potassium to maintain balance, which contained in mM-1-1 II5NaC1, 9 or 10 KC1, 26 NaHCO3 and 2CAC12, before dilution by 10 ~ with 5 g. 100 ml- 1 glucose, and which was equilibrated with 5 ~ CO2.
Experiments were performed under three conditions of renal function, the control state, after uranyl nitrate or following bilateral ischaemia. Control kidneys were either unmanipulated or were sham treated to have undergone the same procedures as the other two groups. Uranyl nitrate, 7.5mg.m1-1, was given as a single dose of 15mg.kg -1, injected over a period of 5 rain into the aorta through the femoral arterial catheter also used for furosemide adminis- tration. Bilateral renal ischaemia was induced by exposing first the left and then the right kidney through a small flank incision, dissecting the renal artery free from the vein, and looping a length of softened catgut around the artery. Fourty- five minutes of warm ischaemia was achieved in the prone position by placing artery clamps on the free ends of the catgut and hanging then across the back of the animal. With this procedure, by which the taughtened catgut interrupts flow to the kidney by making a kink in the renal artery, removal of the oil-soaked covering pads allows both kidneys to be inspected periodically during ischaemia. The method is illustrated in Fig. 1.
Renal function was monitored for up to 6 h after anaes- thesia in 12 groups of male, Sprague-Dawley rats of compara- ble weights, ranging from 190- 310 g. Measurements of renal
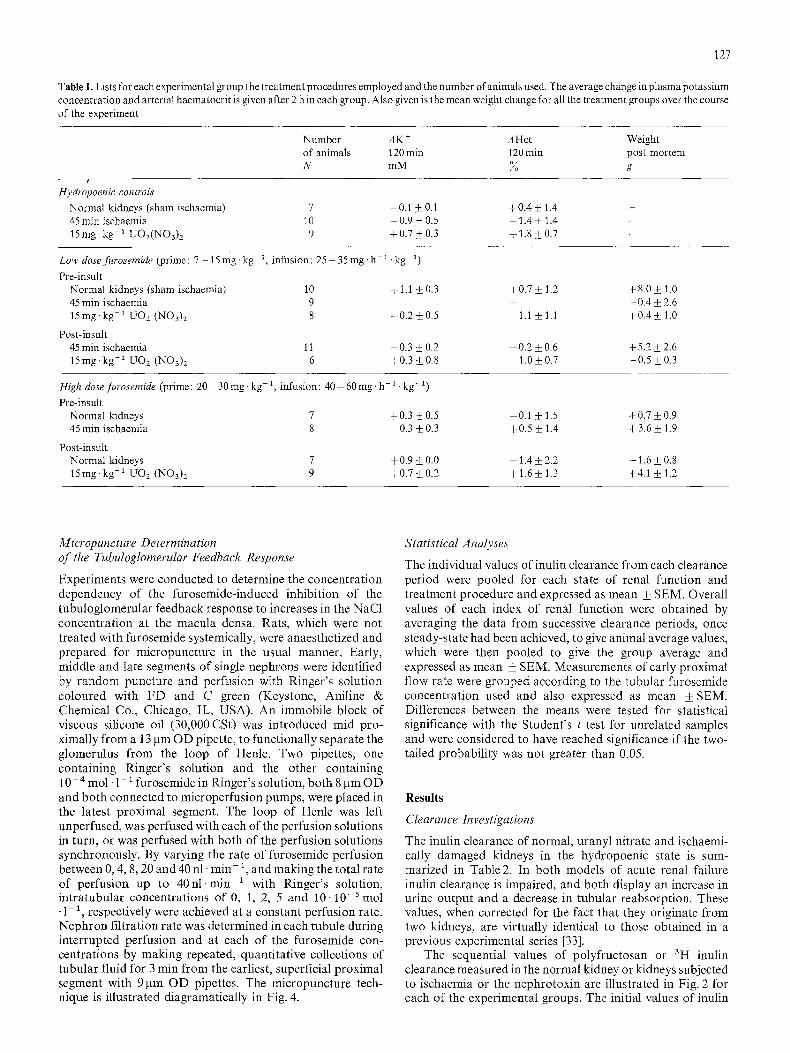
function were obtained during hydropoenia, during "low dose" furosemide or during "high dose" furosemide. Hydropoenic controls received only the 3H inulin infusion plus any additional saline needed after uranyl nitrate or ischaemia to replace urinary losses. Furosemide (Hoechst, Frankfurt, FRG), first made isotonic by the addition of NaCI, was diluted further and given as a priming dose followed by a constant infusion either before the damaging agent, "pre-insult", or after it, "post-insult". For "low dose", furosemide was diluted to 33 ~ to give the priming dose of 7 - 15mg.kg -1 and to 66~ to infuse 2 5 - 3 0 m g . h - l . k g -1. For "high dose" furosemide was left undiluted to give the priming dose of 2 0 - 3 0 m g . k g - ~ , followed by 4 0 - 60 mg. h- 1. kg- 1 infusion. Thus, in both groups the priming dose was contained in a volume of 0 .3 - 0.6 ml. 100 g-1 and the infusion involved an additional volume load of 0 .25- 0.40 ml. h- 1 �9 100 g- ~. Fluid replacement with Ringer's so- lution was matched to urinary output at 5rain intervals. Plasma potassium concentration and haematocrit, measured in each arterial blood sample, were used to assess the adequacy of the fluid and electrolyte replacement and the weight of the animals post-mortem was used to determine the final state of fluid balance. The treatment procedures em- ployed in each of the 12 groups of animals and the number of animals in each group are listed in Table 1, together with the changes in plasma potassium concentration and haematocrit at 2 h, and the increment in body weight post-mortem.
Analytical Procedures
In control animals, the polyfructosan concentration in urine or plasma was measured colourimetrically using the anthrone method [191. Since furosemide behaves as a chromogen in this reaction, renal function was determined with 3H inulin in the remaining groups. The 3H activity in urine and plasma was assessed by counting 20 gl samples in Aquasol (New England Nuclear, Boston, MA, USA) for 20min using a well-type scintillation counter (Beckman Instruments, Munich, FRG). Plasma potassium concentration was determined flame photometrically (Instrumentation Laboratory, Hersel, FRG). Furosemide concentration in urine was measured colourimetrically using the diazo-reaction, after first remov- ing the furfuryl group by heating with HC1 [22].
127
Table 1, Lists for each experimental group the treatment procedures employed and the number of animals used. The average change in plasma potassium concentration and arterial haematocrit is given after 2 h in each group. Also given is the mean weight change for all the treatment groups over the course of the experiment
Number A K + A Hct Weight of animals 120 min 120 min post nmrtern N mM ~ g
i
Hydropoenic controls Normal kidneys (sham ischaemia) 7 0.1 • 0.1 +0.4 • 1.4 - 45 rain ischaemia 10 - 0.9 • 0.5 - 1.4 • 1.4 - 15 rag- kg- 1 U O 2 ( N O 3 ) 2 9 +0.7 • 0.3 + 1.8 • 0.7
Low dose furosemide (prime : 7 - t 5 mg. kg 1, infusion: 25 - 35 mg. h- 1. kg 1)
Pre-insult Normal kidneys (sham ischaemia) 10 + 1.1 • 0.3 + 0.7 _+ 1.2 45 min ischaemia 9 - 15mg.kg-1 UO2 (NO3)2 8 +0.2 • 0.5 - i .1 • 1.1
Post-insult 45 min ischaemia 11 - 0.3 + 0.2 - 0.2 • 0.6 15mg-kg -1 UO2 (NO3)2 6 +0.3 • 0.8 -1.0•
+8.0• -0.4• +0.4•
+5.2• -0.5•
High dosefurosemide (prime: 20 30mg-kg -1, infusion: 40-60mg.h -1 .kg -1)
Pre-insnlt Normal kidneys 7 +0.3 • 0.5 -0.1 • 1.5 45 rain ischaemia 8 0.3 • 0.3 +0.5 • 1.4
Post-insult Normal kidneys 7 + 0.9 • 0.0 -1.4 _+ 2.2 15mg.kg -1 UO2 (NO3)2 9 +0.7• +1.6 • 1.3
+0.7• +3.6•
-1.6• +4A•
Micropuncture Determination of the Tubuloglomerular Feedback Response
Experiments were conducted to determine the concentration dependency of the furosemide-induced inhibition of the tubuloglomerular feedback response to increases in the NaC1 concentration at the macula densa. Rats, which were not treated with fnrosemide systemically, were anaesthetized and prepared for micropuncture in the usual manner. Early, middle and late segments of single nephrons were identified by random puncture and perfusion with Ringer's solution coloured with FD and C green (Keystone, Aniline & Chemical Co., Chicago, IL, USA). An immobile block of viscous silicone oil (30,000CSt) was introduced mid pro- ximally from a 13 ~m OD pipette, to functionally separate the glomerulus from the loop of Henle. Two pipettes, one containing Ringer's solution and the other containing 10- 4 mol- 1 - 1 furosemide in Ringer's solution, both 8 gm OD and both connected to microperfusion pumps, were placed in the latest proximal segment. The loop of Henle was left unperfused, was perfused with each of the perfusion solutions in turn, or was perfused with both of the perfusion solutions synchronously. By varying the rate of furosemide perfusion between 0, 4, 8, 20 and 40 nl. ra in- 1, and making the total rate of perfusion up to 4 0 n l . m i n -1 with Ringer's solution, intratubular concentrations of 0, 1, 2, 5 and 10 .10-Stool �9 1- 1, respectively were achieved at a constant perfusion rate. Nephron filtration rate was determined in each tubule during interrupted perfusion and at each of the furosemide con- centrations by making repeated, quantitative collections of tubular fluid for 3 min from the earliest, superficial proximal segment with 9 ~tm OD pipettes. The micropuncture tech- nique is illustrated diagramatically in Fig. 4.
Statistical Analyses
The individual values of inulin clearance from each clearance period were pooled for each state of renal function and treatment procedure and expressed as mean _+ SEM. Overall values of each index of renal function were obtained by averaging the data from successive clearance periods, once steady-state had been achieved, to give animal average values, which were then pooled to give the group average and expressed as mean _+ SEM. Measurements of early proximal flow rate were grouped according to the tubular furosemide concentration used and also expressed as mean + SEM. Differences between the means were tested for statistical significance with the Student's t test for unrelated samples and were considered to have reached significance if the two- tailed probability was not greater than 0.05.
Results
Clearance Investigations
The inulin clearance of normal, uranyl nitrate and ischaemi- cally damaged kidneys in the hydropoenic state is sum- marized in Table 2. In both models of acute renal failure inulin clearance is impaired, and both display an increase in urine output and a decrease in tubular reabsorption. These values, when corrected for the fact that they originate from two kidneys, are virtually identical to those obtained in a previous experimental series [33].
The sequential values of polyfructosan or 3H inulin clearance measured in the normal kidney or kidneys subjected to ischaemia or the nephrotoxin are illustrated in Fig. 2 for each of the experimental groups�9 The initial values of inulin

128
Table2. Summarises the functional characteristics of the normal, uranyl nitrate and ischaemic kidneys in the h.ydropoenic state. The values of polyfructosan or inulin clearance, Cp or C~N, urine to plasma concentration ratio, U/Pp or U/P[~, and urine flow rate, V, are given as mean _+ SEM. The asterisks denote those values which are significantly different from the corresponding control values in the normal kidney
Normal kidneys (sham ischaemia)
15mg-kg -~ U02 (~NT03) 2 45 rain ischaemia
Cp or Cm (ml .min -~ �9 lOOg -1) 0.80+ 0.07 0.51 +0.05* 0.15+0.23" U/Pp or U/P~ 313 +_24 31 _+5* 32 _+8* V(gl-min-l.100g -~) 2.9 +_ 0.4 18.4 _+2.8* 9.1 _+2.8* n (number of animals) 7 9 10
CIN or Cp [ ml/min/1OOg ]
1.0 ~
0.8-
0.6-
0.~-
0.2-
0
CONTROLS
~ X / ~ SHAM 'SCHAEMIA
! UNAN L,, ,A
ISCHAEMIA
ISCHAEMIA 0 60 120 180
PRE- INSULT F LOW DOSE FUROSEMIDE
- I ~ ' ~--~w. URANYL NIINAIE
~_...... SHAM ISCHAEMIA
ISCHAEM[A
ISCHAEMIA f
6 60 12o 1~o
POST-INSULT LOW DOSE FUROSEHIDE
F t ISCHAEMIA 45min /
o 60 1~o ~8o 2Zo
CIN orCp [ ml/min/lOOg ]
1.0-
0.8-
0.6-
0.4-
0.2-
CONTROLS
: t \ / ~ \ SHAM ,SCHAE..
ISCHAEMIA
PRE-INSULT HIGH DOSE FUROSEMIDE
ISCHAEMIA
45ram / [ ' ~ t ~ ' " - - ~ - ' ~ - ISCHAEMLA/'5m'n / ~ ' ~ " ISCHAEMIA, r . . , ,
60 ' 12o ' 18o 60 12o
POST-INSULT F HIGH DOSE FUROSEMIDE
" ~ NORMAL KIDNEY
&\ F
, , , _ t UN,N,L N,,A,E
o 6 ' 18o 6 ' r;o ' 18o 3o TIME [rain]
Fig. 2. Depicts the sequential values of polyfructosan or inulin clearance obtained from normal and damaged kidneys without furosemide, the controls, or when furosemide was given before or after the damaging agent, pre-insult or post-insult. The control groups are shown twice, once for comparison with the low dose furosemide in the upper pannel and once for comparison with the high dose furosemide in the lower pannel. The closed symbols indicate those values obtained during hydropoenia and the open symbols denote those values obtained with furosemide. The data are presented as mean _+ SEM
clearance in the sham-operated, ischaemia or uranyl nitrate groups, which were obtained after dissection of the renal artery or insertion of the aortic catheter but before ischaemia or uranyl nitrate, were little different from those of normal kidneys, indicating a minimal influence of these procedures on renal function. The application of furosemide per se appeared to have no influence on inulin clearance, as is evident in the normal kidneys in both high dose furosemide groups and from the uranyl nitrate kidneys before the toxin in the low dose furosemide group. However, there was a significant fall in inulin clearance upon low dose furosemide
administration in the sham-ischaemia group, which was not evident in the sham-operated animals not given furosemide, indicating that the combination of extensive surgery and furosemide has some deleterious effects on renal function. Following ischaemia, no difference in renal function com- pared to the controls was apparent after any of the treatment procedures. With uranyl nitrate, however, the inulin clear- ance seemed less depressed compared to the controls in the pre-insult low dose group and showed immediate improve- ment in the post-insult low dose group, even though no effect was apparent in the post-insult high dose group.

Cp or ClN [ml.min'+. 100g -1 ]
U/Pp Or
U/PIN
[,u[ .rain -i. I00g-I ]
HYDROPOENIC LOW DOSE FUROSEMIDE HIGH DOSE FUROSEMIDE CONTROLS Pre-lnsult Post -Insult Pre-lnsult Post -Insult
0.8 I*)
0.6
0./~
0.2
o ~ ~
1 0 - - - +t ++
Fig. 3 Shows in the upper portion the values of polyfructosan or inulin clearance, Cp or CIN, the middle portion the urine to plasma inulin concentration ratio, U/Pp or U/P~N, and in the lower portion the urine flow rate, V. The values were obtained by pooling the average value in each animal to calculate the mean + SEM for each group. The animal average was calculated using all clearance periods in the normal and post-ischaemic kidneys but using only the fourth and subsequent periods after uranyl nitrate, when steady-state conditions had been achieved. The asterisks denote those values of polyfructosan or inulin clearance which are statistically different from those of the corresponding hydropoenic controls
129
The average values of renal function, obtained by pooling the mean values from each animal once steady-state had been achieved, are depicted in Fig. 3. It is apparent that the normal kidneys of the high dose furosemide groups had marginally higher values of inulin clearance than the sham-operated animals. After ischaemia, the inulin clearance was unaltered compared to the controls in all groups. Following unranyl nitrate, inulin clearance was elevated by low dose furosemide given pre- or post-insult, but uninfluenced by high dose furosemide. The urine to plasma inulin concentration ratios fell after furosemide to values of under 10 in normal kidneys and to values as low as 2 after ischaemia or uranyl nitrate. The rate of urine flow rose enormously with low dose furosemide,
and did not increase further at the higher dosage, except in the case of the normal kidneys.
Micropuncture Investigation
The results of the experiments to determine the dependency of the mechanism of tubuloglomerutar feedback upon the tubular furosemide concentration are illustrated in Fig. 4, together with the micropuncture technique employed. Nephron filtration rate, as given by the rate of fluid delivery to the earliest superficial proximal segment, fell upon late proximal perfusion of the loop of Henle at 40 nl . ra in- ~ to 52 ~ of its initial value. The inclusion of furosemide in the
I0 ~'M/I RINGER'S FUROSENIDE SOLUTION
/
EARLY PROXIMAL FLOW RATE [nt.min-1.100g -I] '+-I\+ 8-
6-
NO RINGER'S O.l,lO-4M/l 0.2.10"4M/1 0.5,I0-4M/I IO'l'M/l NO PERFUSION PERFUSION FUROSEMIOE FUROSEMIDE FUROSEMIDE FUROSEMIDE PERFUSION 13.4--1.2 7.0~0.9 6.8-*0.9 9.9=0 9 12.8--1.1 12,7-'1.1 12.9~1.2
Fig. 4. Illustrates on the left the micropuncture technique employed and on the right the experimental results, given as mean + SEM. The loop of Henle was perfused orthogradely at 40nl-rain-1 with mixtures of Ringer's solution and 10-+mo1.1-1 furosemide in a random sequence to give the concentrations indicated. Early proximal flow rate was determined in each nephron before perfusion, at each furosemide concentration and after finishing perfusion. The difference in early proximal flow rate between the initial no perfusion and Ringer's perfusion value represents the full feedback response, which was unaltered with 10- 5 mol. 1 1 furosemide. At 5.10 5 tool- 1- a furosemide and above the feedback response was fully inhibited. After rinsing the tubule the pre-perfusion value was reobtained. The asterisks denote those values which are statistically indistinguishable from the initial no perfusion state
130
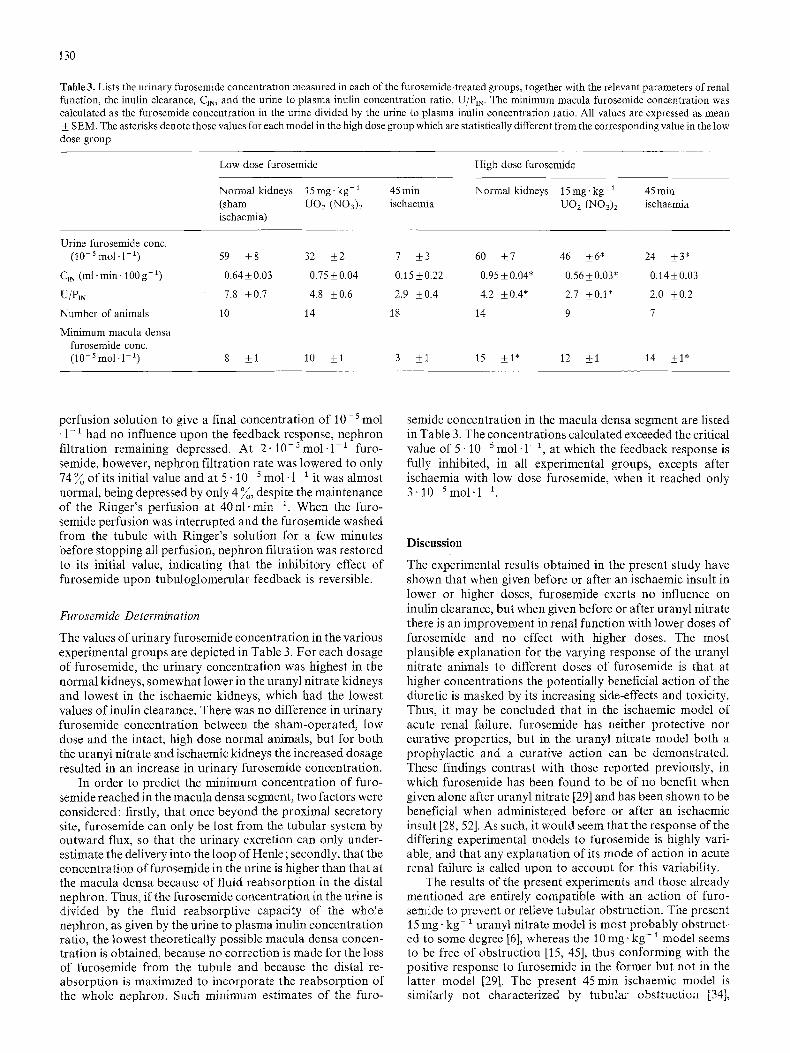
Table 3. Lists the urinary furosemide concentration measured in each of the furosemide-treated groups, together with the relevant parameters of renal function, the inulin clearance, CIN, and the urine to plasma inulin concentration ratio, U/PIN. The minimum macula furosemide concentration was calculated as the furosemide concentration in the urine divided by the urine to plasma inulin concentration ratio. All values are expressed as mean -+ SEM. The asterisks denote those values for each model in the high dose group which are statistically different from the corresponding value in the low dose group
Low dose furosemide High dose furosemide
Normal kidneys 15 mg- kg- 1 45 min Normal kidneys 15 rag- kg- ~ 45 rain (sham UO2 (NO3)2 ischaemia UO2 (NO3)2 ischaemia ischaemia)
Urine furosemide conc. (I0-5 mol.1 -~ ) 59 _+8 32 +2 7 +_3 60 +_7 46 +_6* 24 _+3*
CIN (ml .rain. 100g -1) 0.64+0.03 0 .75_+0 .04 0 .15+_0 .22 0.95_+0.04* 0.56+0.03* 0.14+-0.03
U/PIN 7.8 +0.7 4.8 +0.6 2.9 +_0.4 4.2 +0.4* 2.7 +0.1" 2.0 +0.2
Number of animals l 0 14 18 14 9 7
Minimum macula densa furosemide conc. (10 s mol.l-1) 8 +1 10 +_1 3 -+l 15 +_l* 12 +_1 14 _+1"
perfusion solution to give a final concentrat ion of 10-s mol �9 1- a had no influence upon the feedback response, nephron filtration remaining depressed. At 2- 10-5 mol . 1-1 furo- semide, however, nephron filtration rate was lowered to only 74 ~ of its initial value and at 5 . 1 0 - 5 tool. 1- a it was almost normal, being depressed by only 4 ~ , despite the maintenance of the Ringer 's perfusion at 40 h i - m i n - 1 . When the furo- semide perfusion was interrupted and the furosemide washed from the tubule with Ringer 's solution for a few minutes before stopping all perfusion, nephron filtration was restored to its initial value, indicating that the inhibitory effect of furosemide upon tubuloglomerular feedback is reversible.
Furosemide Determ&ation
The values of urinary furosemide concentration in the various experimental groups are depicted in Table 3. For each dosage of furosemide, the urinary concentration was highest in the normal kidneys, somewhat lower in the uranyl nitrate kidneys and lowest in the ischaemic kidneys, which had the lowest values of inulin clearance. There was no difference in ur inary furosemide concentrat ion between the sham-operated, low dose and the intact, high dose normal animals, but for both the uranyt nitrate and ischaemic kidneys the increased dosage resulted in an increase in urinary furosemide concentration.
In order to predict the minimum concentrat ion of furo- semide reached in the macula densa segment, two factors were considered: firstly, that once beyond the proximal secretory site, furosemide can only be lost from the tubular system by outward flux, so that the urinary excretion can only under- estimate the delivery into the loop of Henle; secondly, that the concentration of furosemide in the urine is higher than that at the macula densa because of fluid reabsorpt ion in the distal nephron. Thus, if the furosemide concentrat ion in the urine is divided by the fluid reabsorptive capacity of the whole nephron, as given by the urine to plasma inulin concentrat ion ratio, the lowest theoretically possible macula densa concen- t rat ion is obtained, because no correction is made for the loss of furosemide from the tubule and because the distal re- absorpt ion is maximized to incorporate the reabsorpt ion of the whole nephron. Such minimum estimates of the furo-
semide concentration in the macula densa segment are listed in Table 3. The concentrations calculated exceeded the critical value of 5 .10 5 mol . 1-1, at which the feedback response is fully inhibited, in all experimental groups, excepts after ischaemia with low dose furosemide, when it reached only 3. J0-5 mol .1 -1
Discussion
The experimental results obtained in the present study have shown that when given before or after an ischaemic insult in lower or higher doses, furosemide exerts no influence on inulin clearance, but when given before or after uranyl nitrate there is an improvement in renal function with lower doses of furosemide and no effect with higher doses. The most plausible explanation for the varying response of the uranyl nitrate animals to different doses of furosemide is that at higher concentrations the potentially beneficial action of the diuretic is masked by its increasing side-effects and toxicity. Thus, it may be concluded that in the ischaemic model of acute renal failure, furosemide has neither protective nor curative properties, but in the uranyl nitrate model both a prophylact ic and a curative action can be demonstrated. These findings contrast with those reported previously, in which furosemide has been found to be of no benefit when given alone after uranyl nitrate [29] and has been shown to be beneficial when administered before or after an ischaemic insult [28, 52]. As such, it would seem that the response of the differing experimental models to furosemide is highly vari- able, and that any explanation of its mode of action in acute renal failure is called upon to account for this variability.
The results of the present experiments and those already mentioned are entirely compatible with an action of furo- semide to prevent or relieve tubular obstruction. The present 15 mg- k g - 1 uranyl nitrate model is most probably obstruct- ed to some degree [6], whereas the 10mg. kg-1 model seems to be free of obstruction [15, 45], thus conforming with the positive response to furosemide in the former but not in the latter model [29]. The present 45 min ischaemic model is similarly not characterized by tubular obstruction [34],

/31
whereas the 60 or 90 min ischaemic model is reported to be severely obstructed [1, 47 - 49, 52], which is in accord with the beneficial effect produced by furosemide in the latter [28, 52] but not in the former model. Furthermore, the improvement in renal function seen in the mercuric chloride model [2, 51], which often displays an obstructive component [16, 34], in noradrenalin-induced acute renal failure [53], which seems also to be obstructed [8, 12] and in methaemoglobin renal failure [38], which is undoubtedly obstructed [34, 44], is also consistent with this hypothesis.
Alternatively, the results of the present investigation can be interpreted to indicate the action of furosemide to enhance the excretion of toxic substances. Since ischaemic injury, which is manifest as a derangement of cellular architecture and metabolism, is not an excretable entity, it need not be influenced by furosemide, but uranium ions, which are believed not to penetrate the cell but to bind to the luminal surface [43], may simply be eliminated from the kidney faster during a diuresis. This suggestion derives support from the recent finding that the protection of renal function by saline diuresis following intoxication with mercuric ions, which do penetrate the cell [55], was associated with a decrease in the mercury content of the renal cortex and an increase in the excretion of mercury in the urine [25]. Consequently, the improvement in renal function reported with furosemide after mercuric chloride [2, 51], may also be caused by this means.
An action of furosemide to directly increase renal blood flow, although well documented for the normal kidney [5, 23, 31, 46] could hardly account for the increase in renal function seen in the uranyl nitrate model and its absence in the ischaemic model. Furthermore, except for noradrenaline- induced acute renal failure, in which PG E2 or bradykinin not surprisingly improve renal function [35, 42], all efforts to increase blood flow in acute renal failure kidneys pharma- cologically - with dopamine [29] or PG E2 [35] in uranyl nitrate renal failure, or with PG A1 in ischaemic [13], glycerol or uranyl nitrate induced acute renal failure [11] - failed to enhance renal function. Thus it seems safe to conclude that any vasodilatatory effect that furosemide may have in acute renal failure kidneys is not associated with an improvement in renal function.
Finally, an action of furosemide to enhance filtration rate by inhibiting the mechanism of tubuloglomerular feedback is difficult to resolve with the present experimental findings. It could be argued that furosemide fails to augment filtration rate in the low dose ischaemic group because insufficient furosemide reaches the tubular system to be effective (an estimated 3 .10- s mol. 1-1 at the macula densa) and that at higher doses, when effective tubular concentrations are reached, noxious systemic effects mask this action. If this were the case, furosemide would be only theoretically beneficial in this model and of no realistic therapeutic value, for the necessary condition of higher tubular concentrations at lower systemic doses is not realisable. It is difficult to compare the results of these experiments with those of others, in which there is no information regarding the concentrations of furosemide achieved either in urine or plasma. However, if the present data are taken as a guide-line, in which 2 5 - 3 5 m g . h - i . k g -~ was not sufficient to guarantee full in- hibition of tubuloglomerular feedback in the 45min isch- aemic model with 20 ~ residual filtration rate, it is evident that in all investigations except for one [2], the furosemide given was either too little or too infrequent to sustain the concentrations required. Thus, in these studies it is the effect
of furosemide as a diuretic and not as an inhibitor of tubuloglomerular feedback which has been investigated. In the one study employing adequately high doses of furosemide to inhibit tubuloglomerular feedback [2], the interpretation of the results is made difficult because pre-renal influences cannot be excluded and because protection was only demon- strated after very low doses of mercuric chloride and was not apparent after the more commonly employed higher dose.
Consequently, a careful analysis of the present data and a critical assessment of the other reports in the literature, seem to lead to the conclusion that furosemide will improve renal function by relieving or preventing obstruction and possibly enhancing the excretion of nephrotoxic substances in those models of acute renal failure with an obstructive or nephro- toxic component but an action to either increase renal blood flow directly or inhibit tubulogtomerular feedback pharma- cologically remains unproven, and seems unlikely. Thus, the beneficial effects of furosemide would appear to be directly attributable to its ability to induce a diuresis, rather than to any specific property of the substance itself. If this is so, it must be expected that all diuretics display the same beneficial features. A variety of osmotic agents have been shown to alleviate the symptoms of acute renal failure in the un- doubtedly obstructed methaemoglobin model [50], and con- siderable improvements in renal function have been obtained with mannitol diuresis in noradrenalin-induced renal failure [8, 12, 42], after 60min ischaemia [17, 18, 24, 47], following mercuric chloride [51] or after glycerol [56], which seem to be either obstructed or toxic in nature, or both. Similarly, supplying saline as the sole source of drinking fluid, with or without concomitant DOCA administration, produced a sodium excretion-related protection from uranyl nitrate and mercuric chloride induced renal failure, which was inde- pendent of renal renin content [4]. Thus, providing the diuretic does not possess the additional characteristics of reducing renal blood flow, as does chlorothiazide or ben- zolamide [42], any type of diuretic seems to improve renal function in models of acute renal failure whose pathogenesis features tubular obstruction or nephrotoxicity or both. That the degree of protection afforded correlates well with the rate of urine flow or solute excretion prior to the insult [4, 8, 12, 50, 51], is hardly surprising because this describes the effective- ness of the diuretic agent to produce a diuresis. Furthermore, it is intuitively obvious that a solute diuresis, by augmenting tubular flow through most of the nephron, will be more effective in rinsing the nephron than a water diuresis, which increases tubular flow only through the most distal part of the nephron, and explains the lack of protection reported in glucose-drinking or diabetes insipidus rats challenged with glycerol [36, 56].
In summary, it may be stated that furosemide improves renal function in the uranyl nitrate but not in the ischaemic model in the present study. These results, together with those of similar investigations reported in the literature, are best explained by an action of furosemide in models with an obstructive or nephrotoxic component to wash out the obstructive or nephrotoxic material. Examination of the literature reveals a protective effect for such models of acute renal failure subjected to any form of solute diuresis. As such, the failure of the 45min ischaemic model to respond to furosemide in the present study and to saline diuresis in a previous study [33], is compatible with the original contention that this model is not obstructed [34]. The conclusion that solute diuresis per se is protective in many forms of acute renal

132
fai lure s t rong ly s u p p o r t s the sugges t ion [4, 33, 51] t h a t the p r o t e c t i o n f r o m acute rena l fa i lure i n d u c e d by glycerol, d i c h r o m a t e , u r a n y l n i t r a t e or mercu r i c sal ts o b s e r v e d in s a l ine -d r ink ing an ima l s (for references see [3 3]) is a t t r i b u t a b l e to the diuresis a n d no t to the s upp r e s s i on o f renin , as was p rev ious ly supposed . F u r t h e r m o r e , the fal lacy o f a s s u m i n g t h a t inc reased u r ine o u t p u t ind ica tes i m p r o v e d rena l f u n c t i o n is d e m o n s t r a t e d by the 45 m i n i schaemic m o d e l in the p re sen t s tudy a n d the u r a n y l n i t r a t e [29] a n d mercu r i c ch lor ide mode l s [54] in o t h e r inves t iga t ions , w h i c h all fai led to show a rise in f i l t r a t ion ra te w i th f u r o s e m i d e b u t all u n d e r w e n t a diuresis.
Acknowledgements. This investigation was supported by the Deutsche Forschungsgemeinsehaft.
A preliminary report of the experimental data has been presented previously at the following meetings : II European Colloquium on Renal Physiology, BalatonfiJred 1977; IV Congress of the Iranian Society of Physiology and Pharmacology, Shiraz 1977; VII International Congress of Nephrology, Montreal 1978.
References
1. Arendshorst WJ, Finn WF, Gottschalk CW (1975) Pathogenesis of acute renal failure following temporary renal ischemia in the rat. Circ Res 37:558-568
2. Bailey RR, Natale R, Turnbull DI, Linton AL (1973) Protective effect of furosemide in acute tubular necrosis and acute renal failure. Clin Sci Mol Med 4 5 : 1 - 1 7
3. Beaufils F, de Myttenaere S, Rohan J, Chapman A (1972) Effets du furos4mide chez les malades en insuffisance r6nale aigufi. Nouv Presse Med 16 : 1073-1078
4. Bidani A, Churchill P, Fleischmann L (1979) Sodium-chloride- induced protection in nephrotoxic acute renal failure: independence from renin. Kidney Int 16:481-490
5. Birtch AG, Zakheim RM, Jones LG, Barger AC (1967) Redistribution of renal blood flow produced by furosemide and ethacrynic acid. Circ Res 21 : 869-- 878
6. BIantz RC (1975) The mechanism of acute renal faiIme after uranyt nitrate. J Clin Invest 55:621-635
7. Borirakchanyavat B, Vongsthongsri M, Sitprija V (1978) Furose- mide and acute renal failure. Postgrad Med J 54 :30-32
8. Burke TJ, Cronin RE, Duchin KL, Peterson LN, Schrier RW (1980) Ischemia and tubule obstruction during acute renal failure in dogs: mannitol in protection. Am J Physiol 238:F305-F314
9. Cantarovich F, Galli C, Benedetti L, Chena C, Castro If, Correa C, Perez-Loredo J, Fernandez JC, Locatelli A, Tizado J (1973) High dose furosemide in established acute renal failure. Br Med J 4: 449 - 450
10. Cantarovich F, Locatelli A, Fernandez JC, Loredo JP (1971) Furosemide in high doses in the treatment of acute renal failure. Postgrad Med J april Suppl: 13 - 17
11. Cioffi RF, O'Connell B, Shalhoub RJ (1975) Effect ofprostaglandin A 1 on acute renal failure in the rat. Nephron 15:29-34
12. Cronin RE, Erickson AM, de Torrente A, McDonald KM, Schrier RW (1978) Norepinephrine-induced acute renal failure : a reversible ischemic model of acute renal failure. Kidney Int 14:187-190
13. Eliahou HE, Iaina A, Solomon S, Gavendo S (1977) Alleviation of anoxic experimental acute renal failure in rats by fl-adrenergic blockade. Nephron 19 : 158-166
14. Epstein M, Schneider NS, Befeler B (1975) Effect of intrarenal furosemide on renal function and intrarenal hemodynamics in acute renal failure. Am J Med 58:510-516
15. Flamenbaum W, Huddleston ML, McNeil JS, Hamburger RJ (1974) Uranyl nitrate-induced acute renal failure in the rat: micropuncture and renal hemodynamic studies. Kidney Int 6:408-418
16. Flamenbaum W, McDonald FD, DiBona GF, Oken DE (1971) Micropuncture study of renal tubular factors in low dose mercury poisoning. Nephron 8 : 221 - 234
17. Flores J, DiBona DR, Beck CH, Leaf A (1972) The role of cell swelling in ischemic renal damage and the protective effect of hypertonic solute. J Clin Invest 51 : 118-126
18. Frega NS, DiBona DR, LeafA (1976) Ischemic renal injury. Kidney Int 10:(Suppl 6) S17 -$25
19. Fiihr J, Kaczmarczyk J, Kriittgen CD (1955) Eine einfache Methode zur Inulinbestimmung ffir Nieren-Clearance-Untersuchung bei Stoffwechselgesunden und Diabetikern. Klin Wochenschr 33 : 729 - 730
20. Green RD, Boyer D, Halasz NA, Collins GM (1979) Pharmaco- logical protection of rabbit kidneys from normothermic ischemia. Transplantation 28 : 131 - 134
21. Greven J, Klein H (1976) Renal effects of furosemide in glycerol induced acute renal failure in the rat. Pfltigers Arch 365:81-87
22. H/iussler A, Hajdu P (1964) Untersuchungen mit dem Salidiureticum 4-chlor-N-(furylmethyl)-5 sulfamyl-anthranilsfiure. II. Arzneimittel- Forschung 14: 710 - 713
23. Hook JB, Blatt AH, Brody MJ, Williamson HE (1966) Effects of several saluretic-diuretic agents on renal hemodynamics. J Pharma- col Exp Ther 154: 667 - 673
24. Kashgarian M, Siegel NJ, Ries AL, DiMeola HJ, Hayslett JP (1976) Hemodynamic aspects in development and recovery phases of experimental postischemic acute renal failure. Kidney Int 10:(Suppl 6) 160-168
25. Kirschbaum BB, Sprinkle FM, Oken DE (1980) Renal function and mercury level in rats with mercuric chloride nephrotoxicity. Nephron 26 :28-34
26. Kleinknecht D, Ganeval D, Gonzales-Duque LA, Fermanian J (1976) Furosemide in acute oliguric renal failure. A controlled trial. Nephron 17 : 51 - 58
27. K611ing B, Greven J (1978) Untersuchungen zur Wirksamkeit von Furosemid bei experimentellem akuten Nierenversagen. Res Exp Med 173:89-93
28. Kramer HJ, Schuurmann J, Wassermann C, Dusing R (1980) Prostaglandin-independent protection by furosemide from oliguric ischemic renal failure in conscious rats. Kidney Int 17: 455 - 464
29. Lindner A, Cutler RE, Goodman WG (1979) Synergism of do- pamine plus furosemide in preventing acute renal failure in the dog. Kidney Int 16:158-166
30. Lopez-Nova J, Rodicio-Diaz JL, Hernando-Avendano L (1977) Negative effect of frusemide pretreatment in glyceroi induced acute renal failure. Biomedicine 26:117-122
31. Ludens JH, Hook JB, Brody MJ, Williamson HE (1968) Enhancement of renal blood flow by furosemide. J Pharmacot Exp Ther 163 : 456 - 460
32. Mason J, Gutsche HU, Moore L, M~iller-Suur R (1979) The early phase of experimental acute renal failure. IV. The diluting ability of the short loops of Henle. Pfl/igers Arch 379:11-18
33. Mason J, Kain H, Shiigai T, Welsch J (1979) The early phase of experimental acute renal failure. V. The influence of suppressing the renin-angiotensin system. Pfliigers Arch 380:233 - 243
34. Mason J, Olbricht C, Takabatake T, Thurau K (1977) The early phase of experimental acute renal failure. I. Intratubular pressure and obstruction. Pfliigers Arch 370:155 - 163
35. Mauk RH, Patak RV, Fadem SZ, Lifschitz MD, Stein JH (1977) Effect of prostaglandin E administration in a nephrotoxic and vasoconstrictor model of acute renal failure. Kidney Int 12:122- 130
36. McDonald FD, Thiel G. Wilson DR, DiBona GF, Oken DE (1969) The prevention of acute renal failure in the rat by long-term saline loading: a possible role of the renin-angiotensin axis. Proc Soc 131:610-614
37. Minuth AN, Terrell JB, Suki WN (1976) Acute renal failure: a study of the course and prognosis of 104 patients and of the role of furosemide. Am J Med Sci 271:317-324
38. Montoreano R, Mouzet MT, Cunarro J, Ruiz-Guinazu A (1971) Prevention of the initial oliguria of acute renal failure by the administration of furosemide. Postgrad Med J april Suppl : 7 - 1 0
39. Muth RG (1973) Furosemide in acute renal failure. In: Proceeding, Co~ference on acute renal failure. DHEW publ. no. (NIH)74--608, U.S. Goverment Printing Office, Washington DC, pp 245-264

133
40. Olbricht C, Mason J, Takabatake T, Hohlbrugger G, Thurau K (1977) The early phase of experimental acute renal failure. II. Tubular leakage and the reliability of glomerular markers. Pfliigers Arch 372:251-258
41. Papadimitriou M, Milionis A, Sakellariou G, Metaxas P (i978) Effect of furosemide on acute ischaemic renal failure in the dog. Nephron 20 : 157-161
42. Patak RV0 Fadem SF, Lifschitz MD, Stein JH (1979) Study of factors which modify the development of norepinephrine-induced acute renal failure in the dog. Kidney Int 15:227-237
43. Rothstein A (1970) A reappraisal of the action of uranyl ion on cell membranes. In: Maniloff J, Colman F, MilIer F (eds) Effects of metals on cells, subcellular elements and macromolecules, C.C. Thomas, Springfield, Ill, p 365
44. Ruiz-Guinazu A, Coelho JB, Paz RA (1967) Methemoglobin- induced acute renal failure in the rat. Nephron 4:257-275
45. Stein JH, Gottschall J, Osgood RW, Ferris TF (1975) Patho- physiology of a nephrotoxic model of acute renal failure. Kidney Int 8 :27-41
46. Stein JH, Mauk RC, Boonjarern S, Ferris TF (1972) Differences in the effect of furosemide and chlorothiazide on the distribution of renal autoregulation. J Lab Clin Med 79:995-1003
47. Tanner GA, Sloan KL, Sophasan S (1973) Effects of renal artery occlusion on kidney function in the rat. Kidney Int 4: 377-389
48. Tanner GA, Sophasan S (1976) Kidney pressures after temporary renal artery occlusion in the rat. Am J Physiol 230 : 1173 - 1181
49. Tanner GA, Steinhausen M (1976) Tubular obstruction in ischemia- induced acute renal failure in the rat. Kidney Int 10 : (SuppI 6) S 65 - $73
50. Teschan PE, Lawson NL (1966) Studies in acute renal failure. Prevention by osmotic diuresis, and observations on the effect of plasma and extracellular volume expansion. Nephron 3:1 - 16
51. Thiel G, Brunner, F, Wunderlich P, Huguenin M, Bienko, B, Torhorst J, Peters-Haefeli L, Kirchertz E J, Peters G (1976) Protection of rat kidneys against HgC12 induced acute renal failure by induction of high urine flow without renin suppression. Kidney Int 10:(Suppl 6) S191 - $ 2 0 0
52. Thiei G, De Rougement D, Torhorst J, Kaufmann A, Peters-Haefeii L, Brunner FP (1980) Importance of tubular obstruction and its prevention in ischemic acute renal failure in the rat. In: Leaf A, Giebisch G, Bolis L, Gorini S (eds) Renal pathology - recent advances. Raven Press, New York
53. de Torrelite A, Miller PD, Cronin RE, Paulsen PE, Erickson AL, Schrier RW (1978) Effects of furosemide and acetylcholine in norepinephrine-induced acute renal failure. Am J Physio1235 : 131 - 136
54. Ufferman RC, Jaenike JR, Freeman RB, Pabico PE (1975) Effects of furosemide on low dose mercuric chloride acute renal failure in the rat. Kidney Int 8 : 362- 367
55. Webb JL (1966) Enzyme and metabolic inhibitors, II. Academic Press, New York, p 1237
56. Wilson DR, Thiel G, Arce ML, Oken DE (1967) Glycerol induced hemoglobinuric acute renal failure in the rat. III. Micropuncture study of the effects of mannitol and isotonic saline on individual nephron fnnction. Nephron 4:337-355
57. Wilson DR, Thiel G, Arce ML, Oken DE (1969) The role of the concentration mechanism in the development of acute renal failure: micropuncture studies using diabetes insipidus rats. Nephron 6:128-139
58. Wright FS, Schnermann J (1974) Interference with feedback control of glomerular filtration rate by furosemide, triflocin and cyanide. J Clin Invest 53 : 1695 - 1708
Received April 27/Accepted October 7, 1981