the effect of urine-derived stem cells expressing vegf loaded in collagen hydrogels on myogenesis...
TRANSCRIPT

lable at ScienceDirect
Biomaterials 34 (2013) 8617e8629
Contents lists avai
Biomaterials
journal homepage: www.elsevier .com/locate/biomater ia ls
The effect of urine-derived stem cells expressing VEGF loaded incollagen hydrogels on myogenesis and innervation following aftersubcutaneous implantation in nude mice
Guihua Liu a, Xisheng Wang a,b, Xiangzhou Sun c, Chunhua Deng c, Anthony Atala a,Yuanyuan Zhang a,*
aWake Forest Institute for Regenerative Medicine, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157, USAbDepartment of Urology, Affiliated Guanlan People Hospital, Guangdong Medical College, Shenzhen, GuangDong 518110, ChinacDepartment of Urology, First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, GuangDong 510080, China
a r t i c l e i n f o
Article history:Received 29 May 2013Accepted 21 July 2013Available online 9 August 2013
Keywords:Urine-derived stem cells (USCs)Cell therapyVascular endothelial growth factor (VEGF)Stress urinary incontinence (SUI)
* Corresponding author. Tel.: þ1 336 713 1189; fax:E-mail address: [email protected] (Y. Zhan
0142-9612/$ e see front matter � 2013 Elsevier Ltd.http://dx.doi.org/10.1016/j.biomaterials.2013.07.077
a b s t r a c t
Impairment of sphincter muscles or their neural and vascular support leads to stress urinary inconti-nence. The aim of this study was to determine the role of urine-derived stem cells (USCs) over-expressingvascular endothelial growth factor (VEGF) in collagen-I gel on angiogenesis, cell survival, cell growth,myogenic phenotype differentiation of the implanted cells and innervations following implantationin vivo. USCs were infected with adenovirus containing the human VEGF165 and green fluorescentprotein genes. A total of 5 � 106 cells, USCs alone, or plus endothelial cells or human skeletal myoblasts(as control) suspended in collagen-I gel were subcutaneously implanted into nude mice. Extensivevascularization and more implanted cells was noted in VEGF-expressing USCs groups compared to thenon-VEGF groups in vivo. Numbers of the cells displaying endothelial markers (CD 31 and von Wille-brand’s factor) and myogenic markers (myf-5, MyoD and desmin), and regenerated nerve fibers dis-playing neural markers (S-100, GFAP and neurofilament) significantly increased in the grafts of VEGF-expressing USCs. Improved angiogenesis by VEGF-expressing USCs enhanced grafted cell survival,recruited the resident cells and promoted myogenic phenotype differentiation of USCs and innervation.This approach has important clinical implications for the development of cell therapies for the correctionof stress urinary incontinence.
� 2013 Elsevier Ltd. All rights reserved.
1. Introduction
Autologous cells or mesenchymal stem cell injection therapy forstress urinary incontinence (SUI) has recently offered a promisingalternative for repair of urethral sphincter function. Major advan-tages of autologous cells are avoiding adverse events related to therejection of implanted allogenous tissues, and bypassing ethicalconcerns about use of embryonic stem cells [1]. Ear chondrocytes[2], muscle-derived progenitor cells [3], bone marrow-derivedmesenchymal stromal cells [4], and adipose-derived stem cells [5]are regarded as candidates for this therapy. However, harvesting
þ1 336 713 7290.g).
All rights reserved.
stem cells from these tissues causes potential complications such asdonor site morbidity. Moreover, local anesthesia or general anes-thesia is needed. To eliminate these complications and to generate alarge amount of cells with low medical costs, an autologous stemcell source obtained with non-invasive procedures would bedesirable.
Recently, we have successfully established a primary culturesystem to isolate and repopulate stem cells from urine, called urine-derived stem cells (USCs) [6e12]. These cells can grow up from asingle cell to a large amount of cells (1 � 1014 cells) at passage 14after 8 weeks [10]. After optimizing our methods, up to 140 USCclones/24 hour’s urine can be consistently obtained from each in-dividual [6]. In a previous report, 5 � 107 skeletal muscle-derivedstem cells in 4 ml of solution were required to treat SUI with anendoscopic injection [13]. Therefore, 3.7 � 108 cells generated fromone urine sample (containing 10e15 USC clones/200 ml urine) at

Table 1Research design.
Groups(G) Injections of cell e collagen-I gel Number of graft/number of animal
G1 USCs-GFP/VEGF-ECs 24/12G2 USCs-GFP/VEGF 24/12G3 USCs-GFP 22/11G4 Human myoblasts 10/5G5 Cell-free 10/5
G. Liu et al. / Biomaterials 34 (2013) 8617e86298618
low passage (<p4) within 3 weeks [10] is enough for use in cellinjection for SUI [12]. Additionally, these cells exhibit pericyte/mesenchymal stem cell markers and detectable levels of telome-rase. USCs also can give rise to mesoderm cell lineages, like oste-ocytes, chondrocytes, adipocytes, myocytes, and endothelial cells[14]. These cells can be obtained non-invasively at a low cost, us-ing a simple technology to harvest good-quality cells that can beexpanded to the required quantity [7]. To retain high rates of donorcell viability and function in vivo, angiogenic gene manipulation isfrequently used in cell-based therapy. Several studies have reportedthat both mesenchymal stem cells and differentiated cells thatexpress VEGF can improve cell survival, angiogenesis, and myo-genesis [15]. As mesenchymal stem cells possess angiogenic andanti-fibrotic effects, they are a good cell source for treatment of SUI.
The injectable hydrogels applied for tissue repair are classifiedinto synthetic and natural biomaterials, including (1) syntheticmaterials (i.e. Poly(organophosphazene) hydrogels); (2) the body’sown polymers (i.e. collagen gel, hyaluronic acid); (3) polymers innature (i.e. hydrated chitosan gels); (4) self-assembled peptides (i.e.peptide amphiphile system); and (5) new innovations and combi-nations (i.e. coating a poly lactic acid microcarrier with collagen)[16,17]. Collagen as a natural extracellular matrix proteins is widelydistributed in the human body [18]. As a hydrogel with high watercontent, collagen type I (collagen-I) gel is most commonly used as acell delivery vehicle in cell injection therapy because of its advan-tages in being biodegradable, non-cytotoxic, easily injectable andhighly versatile in tissue repair [19].
Improving local blood circulation, promoting muscle tissue en-gineering, and recovering peripheral nerve function are threecritical criteria for correction of urethra sphincter muscle defects,particularly with sever scarred tissues or lack of blood supply in theneighboring tissue of urethral sphincter. Our hypothesis for thisstudy is that VEGF-expressing USCs plus endothelial cells incollagen-I gel can contribute to a better outcome in all three ele-ments. The objective of this study was to systematically evaluateangiogenesis in VEGF-expressing USCs in collagen-I hydrogel andits effect on the myogenic differentiation and neo-innervation inquantification fashion and to determine whether improved revas-cularization could improve injection therapy for potential in thecorrection of SUI.
2. Materials and methods
2.1. Ethical approval
Protocols for human urine collection, umbilical cord, and human skeletal musclesamples used in this study were approved by the Wake Forest University HealthSciences Institutional Review Board. Written informed consents have been obtainedand were approved by Wake Forest University institutional review board. Experi-ments using nude mice were approved by the Wake Forest University Health Sci-ences Institutional Animal Care and Use Committee.
2.2. USCs isolation and expansion
Twenty-two voided urine samples (100e400 ml/sample) were collected fromfive healthy individuals (male, 25e40 years old). Each fresh urine specimen wasimmediately transferred to the laboratory for isolation and culture as reportedpreviously [7]. Briefly, urine samples were centrifuged at 500 � g for 5 min and thesupernatant was removed. The cell pellet was gently resuspended in mixed mediacomposed of embryo fibroblast medium (EFM) and keratinocyte serum-free me-dium (KSFM) (1:1 ratio) [7] and plated in 24-well plates (p0). Individual single USCsappeared 3e5 days after initially plated and reached a confluence of 70e80%, 3e4days late. The cells were trypsinized, and transferred into 6-well dishes (p1). Finally,cell cultures were transferred to a 100 mm culture dish (p2) for expansion. For mostexperiments, USCs at p3e4 were used.
2.3. Human umbilical cord endothelial cell culture
Human umbilical vein endothelial cells (HUVEC) were isolated by brief perfusionof enzyme solution into umbilical cord veins [20]. HUVECs were then cultured on
fibronectin-coated plates (Millipore, Billerica, MA) using Endothelial GrowthMedium-2 (EGM2) (Lonza Biologics, Portsmouth, NH) containing 2% fetal bovineserum (FBS) and supplements, including VEGF (2 ng/ml), epidermal growth factor,hydrocortisone, GA-1000 (gentamicin, amphotericin-b), fetal bovine serum, basicfibroblast growth factor, insulin-like growth factor, ascorbic acid, and heparin atmanufacturer concentrations at 37 �C in a 5% CO2 cell incubator.
2.4. Human skeletal myoblast culture
Human myoblasts were isolated from chopped skeletal muscle tissue(1 mm � 1 mm) by incubation in 10 ml of Collagenase-II (0.1% w/v)-Dispase (4 mg/ml) solution prepared in DMEM for 1 h at 37�C with constant shaking (60 rpm). Theliberated cells were collected (400� g) andwashed with DMEMmedium containing10% horse serum and plated into a 6-well tissue culture dish. Two hours after, thesupernatant from the dish was transferred to another well and the process repeated.Five days after culture, the media was changed to SkGM2 (Lonza Biologics, Ports-mouth, NH) containing 10% FBS at 37 �C in a 5% CO2 cell incubator.
2.5. Infection of cells with adenoviral vectors
The recombinant E1-deleted adenoviral vector encoding green fluorescentprotein (GFP) and human VEGF165 under the cytomegalovirus promoter (Ad-GFP/VEGF) was obtained from the Harvard Human Gene Therapy Initiative (Boston,MA). Multiplicity of infection was optimized by using the virus at different di-lutions as we have described previously [12]. USCs were seeded in a 6-well plateat 2000/cm2, and infected with the adenoviral vector expressing VEGF (Ad-GFP/VEGF) at multiplicities of infection (MOI) from 50 to 1000. The MOI that generatedmaximum transfected efficiency with minimum cellular toxicity was chosen forfurther experiments.
2.6. Angiogenic growth factors secreted by USCs
To measure angiogenic trophic factors secreted by USCs before VEGF genetransfection, totally 5�105 USCs at passage 2 were seeded at 6-well plates and wereincubated with serum-free DMEM under normal condition (5% CO2, 37�C) for 24 h.The conditioned medium was analyzed by human angiogenesis array kit (R&DSystems) according to the manufacturer’s instructions. Briefly, the membrane con-taining 55 angiogenesis-related antibodies was blocked with bovine serum albuminfor 1 h on a rocking platform at room temperature. Membrane was then incubatedwith culture supernatants from USCs, along with detection antibody cocktail over-night on a rocking platform at 4 �C. Themembranewas incubated with streptavidin-horseradish peroxidase conjugate antibody and developed on X-ray film followingexposure to chemiluminescent reagents. Pixel density was produced by QuantityOne software� and was normalized to the mean pixel density from reference spotsof its own membrane.
2.7. Enzyme-linked immunosorbent assay
To evaluate VEGF secreted by gene-modified USCs, culture media of VEGF-expressing USCs were replaced every 2 days and aspirated at Days 1, 5, 10, 15, 20,25 and 30 for VEGF assays by enzyme-linked immunosorbent assay (ELISA) ac-cording to the manufacturer’s instructions (R&D Systems, Minneapolis, MN). Briefly,VEGF standards were also used simultaneously for generating a standard curve.Media samples were diluted (100e1000 folds) before use to remainwithin the rangeof the standard. Finally, after color development, the microplate was read at 450 nm(Molecular Devices, Spectramax-M5) to calculate VEGF concentrations.
2.8. In vivo implantation
For preparation of cell injection, USCs (p3) from 5 donors were trypsinized and4 � 106 cells were seeded in a 15 cm2 dish, respectively. To infect cells with Ad-GFP/VEGF, adenovirus was added into 5 ml of DMEM high glucose (serum free) culturemedia and incubated for 2 h at 37 �C in a 5% CO2 incubator. After the virus-containing medium was removed, the USCs were incubated in normal culture me-dium for another 14e18 h before collecting for injection.

G. Liu et al. / Biomaterials 34 (2013) 8617e8629 8619
Five groups were designated, as listed in Table 1. USCs at p3 and endothelial cellsand human myoblasts at p5 were used for cell injection into 45 male athymic mice(21e27 g, Harlan Laboratories, Indianapolis, IN). Based on our previous experiment[12], a total of 5 � 106 cells, USCs alone, or plus endothelial cells (USCs: endothelialcells, 4:1) or human skeletal myoblasts as a positive control were embedded in0.5 ml collagen-I gel (2 mg/ml, Becton Dickinson, Franklin Lakes, NJ); the cell-collagen gel was injected subcutaneously into two sites per animal on the rightand left flanks.
2.9. Histologic and immunocytochemical analysis
The weights and gross appearances with capillary distribution of the graftswere assessed at 28 days when mice were sacrificed. The implanted tissue sam-ples were fixed in 10% neutral buffered formalin, dehydrated, and embedded inparaffin. A 5-mm section was cut and mounted using anti-fade mounting media(Vector Laboratories, Burlingame, CA). For visualization of cell density, anti-GFPstaining and 40 , 6-diamidino-2-phenylindole (DAPI) staining were performed.Masson’s Trichrome staining was used to measure the ratio of cells and collagenin the graft tissue.
To specifically identify endothelial cell, muscle cell and nerve fiber markerswithin graft tissues, immunofluorescent staining was performed using the asso-ciated antibodies listed in Table 2. As the tissue samples were not immediatelyprocessed due to technical reasons, GFP expression in the implanted cells wasfaded and barely observed under immunofluorescence microscopy 3 months afterpreserved at �80 �C. Therefore, we used anti-GFP (FITC conjugated) antibodycombined with endothelial-, muscle-specific and nerve fiber-specific markers andDAPI staining to monitor the fate and differentiation of USCs implanted intoathymic mice. The slides were visualized under a fluorescent microscope (Leica-DM 4000B, Germany) and the images recorded for the analysis. For semi-quantitation of new nerve fibers and sections stained with Masson’s Trichromewere evaluated by two independent and blinded observers using 200� magnifi-cation images captured by the microscope (Leica-DM 4000B, Germany). For semi-quantitation of implanted GFP labeled human cells, immunofluorescent stainingfor endothelial and myogenic-specific markers, the average total number of tar-geted cells was counted in 10 fields under 400� magnification and presented asthe percentage of positive cells/total cells in the implants. G1 (USCs/Ad-VEGF plusendothelial cells) was used as a standard for the other four groups whencomparing results by group.
2.10. Real-time quantitative PCR
The mRNA was extracted from the implanted grafts using an RNA isolation kit(5 PRIME, Gaithersburg, MD) according to the manufacturer’s instructions. Five mgof RNA was converted to cDNA in a reaction containing random primers, nucleo-tides, and reverse transcriptase enzyme using a high-capacity cDNA reverse tran-scription kit (Invitrogen, Carlsbad, CA). One-tenth of the cDNA was then used forreal-time analysis along with Taqman Universal PCR master mix and Taqmangene expression probes (vWF, Hs00169795_m1; CD31, Hs01065279_m1; Desmin,Hs01090875; Myf-5, Hs00224610; MyoD, Hs00159528_m1; GAPDH, NM_002046.3;
Table 2Antibodies used in this study.
Antibody Cell markers Host Dilution Company
CD31 Endothelialcells
Goat 1:100 Santa Cruz SC-1506
vWF Endothelialcells
Rabbit 1:200 Dako A0086
desmin Skeletalmuscle cells
Goat 1:100 Santa Cruz SC-7559
myf-5 Skeletalmuscle cells
Goat 1:100 Santa Cruz SC-302
MyoD Skeletalmuscle cells
Rabbit 1:100 Santa Cruz SC-304
S-100 Peripheralnerve
Rabbit 1:100 Abcam ab868
GFAP Schwanncells
Rabbit 1:1000 Abcam ab7779
NF Peripheralnerve
Rabbit 1:1000 Abcam ab8135
Anti-GFP (FITC) Cell label Goat 1:250 Abcam ab6662Anti-Goat
(Alexa Fluor 594)Secondaryantibody
Rabbit 1:400 Invitrogen A21223
Anti-Rabbit(Alexa Fluor 594)
Secondaryantibody
Goat 1:400 Invitrogen A11072
GFAP, Glial fibrillary acidic protein; NF, neurofilament; GFP, Green fluorescentprotein; vWF, von Willebrand factor.
Applied Biosystems, Foster City, CA) according to the manufacturer’s instructionsusing a 7300 real-time PCR system and their reagents (Applied Biosystems).HUVECs and hSKMCs were used as positive control for endothelial and myogenicmarkers respectively.
2.11. Statistical analyses
Values are expressed as mean � standard deviation (SD). p Values �0.05 wereconsidered as statistically significant. Comparisons of weight, GFP/DAPI ratio, semi-quantitation for the immunofluorescent staining of endothelial and myogenicmarkers, nerve numbers, and real-time PCR analysis between the groups wereperformed by using one-way ANOVA followed by a StudenteNewmaneKeuls posthoc test for multiple comparisons when appropriate.
3. Results
3.1. Angiogenesis trophic factors secreted by USCs in vitro and VEGFlevels in culture medium of gene-modified USCs
Twenty-five angiogenesis-related proteins, such as VEGF, Angio-genin, Ang-1, Endoglin, Endothelin-1,MMP-9, CXCL4 and othersweredetected in the supernatant of human USCs (Fig. 1A) by humanangiogenesis array kit.
By 24 h after infection, gene-modified USCs produced 30.73 �1.89 ng/ml VEGF in the supernatant measured by ELISA analysis.Additionally, the in vitro VEGF secretion by VEGF-expressing USCsin the culture medium peaked on day 15 post-infection (Fig. 1B),after which the VEGF levels rapidly declined by day 25. As theratio of GFP labeling observed by using immunofluorescent mi-croscope, USCs infected with Ad-VEGF at an MOI of 200 showedmaximum infection efficiency (approximately 98%); increasingthe MOI above 200 led to cell toxicity but could not increaseinfection efficiency.
3.2. Gross appearance and analysis of implanted grafts
Because measurements of the graft sizes or volumes are unre-liable in soft tissues (Fig. 2A), we measured the weight of implantsat 28 days after transplantation. The weights of implanted grafts inUSCs expressing VEGF with endothelial cells (G1) and or withoutendothelial cells (G2) groups significantly increased compared tothose in the other three groups (Fig. 2B). No significant differencewas seen inweights between G1 and G2, but USCs alone (G3) graftsweighed more than in humanmyoblast cell (G4) and gel alone (G5)injection groups (Fig. 2B). Moreover, the degree of adhesion andcapillary formation on grafts in G1 and G2 remarkably increasedcompared to other groups, indicating more angiogenesis occurredin both groups. Importantly, no tumors or ectopic osteogenic tis-sue formed in any groups following 28 days of subcutaneousimplantation.
3.3. Histology, immunocytochemistry and real-time PCR analysis
Masson’s Trichrome staining indicates the ratio of cells (Red)and collagen (Blue) within the graft tissue. More cells including theimplanted cells and resident cells survived in G1 and G2, the rationof cells and collagenwas higher than other three groups (i.e. G3e5)(Fig. 2A). The ratio of USCs expressing GFP antibody was signifi-cantly more in G1 and G2 compared to other groups on day 28.However, there was no significant difference between G1 and G2.Additionally, G3 showedmore GFP labeling than G4 and G5 (Fig. 2C,Table 3).
3.3.1. Neo-angiogenesisTotal number of cells expressing endothelial cell markers (CD31
and von Willebrand’s factor) significantly increased in G1 and G2confirmed by Immunofluorescent staining and hemi-quantitative

Fig. 1. Angiogenesis trophic factors secreted by USCs in vitro and VEGF levels in culture medium of gene-modified USCs. (A) Angiogenesis trophic factors secreted by USCs in vitro.(i) Twenty-five angiogenesis-related proteins were detected in the supernatant of human USCs by human angiogenesis array kit. (ii) Quantitative pixel density was produced byQuantity One software� and was normalized to the mean pixel density from reference spots of its own membrane. (B) ELISA for over-expressed VEGF analysis. USCs infected withAd-VEGF/GFP were cultured for 30 days and the spent media was collected at regular intervals for VEGF analysis. VEGF levels reached a peak on day 15 post-infection, whichgradually decreased with time.
G. Liu et al. / Biomaterials 34 (2013) 8617e86298620

Fig. 2. Characterization of the implanted grafts after 4 weeks in vivo. (A) Gross morphology (top row) of the implants (marked by white arrows) after 4 weeks in vivo showingdetails of vascularization and implant size. Neovascularization of grafts was observed in G1 (USCs-VEGF þ ECs) and G2 (USCs-VEGF) compared to the poor vascularization of the G5grafts (gel alone). Masson’s trichrome staining (middle and lower row) on the grafts depicts cells (red) to be more abundant in G1 and G2. Scale bar ¼ 50 mm. (B) Implanted grafts inG1 and G2 were significantly heavier than the groups G3 (USCs alone), G4 (human myoblast injection) or G5. G3 also weighed more than G4 and G5, *p < 0.05, **p < 0.01. (C) (i)Implanted cells were detected in vivo by immunofluorescent labeling using anti-GFP antibody, stained in green (white arrows) with DAPI (blue) stained nucleus. (ii) The ratio of GFPto total cell nuclei in the implanted grafts showed that more cells expressed human nuclear marker in G1 and G2, indicating increased survival of the implanted cells, *p < 0.05,**p < 0.01. Scale bar ¼ 50 mm. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
G. Liu et al. / Biomaterials 34 (2013) 8617e8629 8621
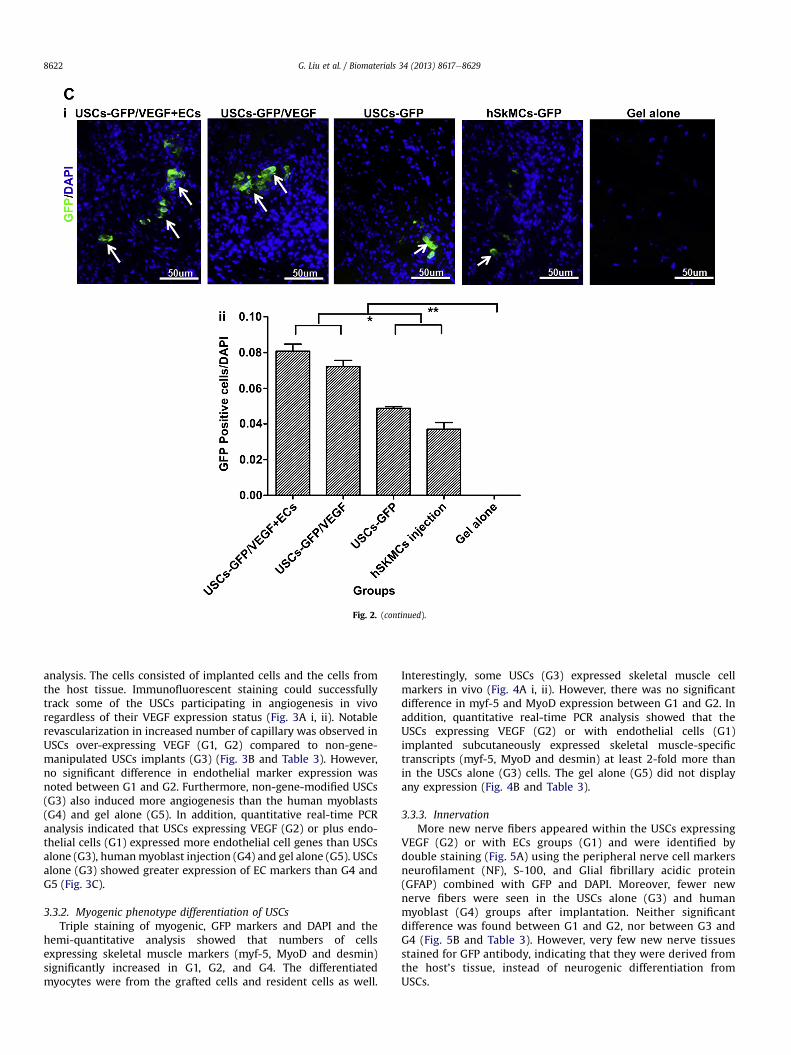
Fig. 2. (continued).
G. Liu et al. / Biomaterials 34 (2013) 8617e86298622
analysis. The cells consisted of implanted cells and the cells fromthe host tissue. Immunofluorescent staining could successfullytrack some of the USCs participating in angiogenesis in vivoregardless of their VEGF expression status (Fig. 3A i, ii). Notablerevascularization in increased number of capillary was observed inUSCs over-expressing VEGF (G1, G2) compared to non-gene-manipulated USCs implants (G3) (Fig. 3B and Table 3). However,no significant difference in endothelial marker expression wasnoted between G1 and G2. Furthermore, non-gene-modified USCs(G3) also induced more angiogenesis than the human myoblasts(G4) and gel alone (G5). In addition, quantitative real-time PCRanalysis indicated that USCs expressing VEGF (G2) or plus endo-thelial cells (G1) expressed more endothelial cell genes than USCsalone (G3), humanmyoblast injection (G4) and gel alone (G5). USCsalone (G3) showed greater expression of EC markers than G4 andG5 (Fig. 3C).
3.3.2. Myogenic phenotype differentiation of USCsTriple staining of myogenic, GFP markers and DAPI and the
hemi-quantitative analysis showed that numbers of cellsexpressing skeletal muscle markers (myf-5, MyoD and desmin)significantly increased in G1, G2, and G4. The differentiatedmyocytes were from the grafted cells and resident cells as well.
Interestingly, some USCs (G3) expressed skeletal muscle cellmarkers in vivo (Fig. 4A i, ii). However, there was no significantdifference in myf-5 and MyoD expression between G1 and G2. Inaddition, quantitative real-time PCR analysis showed that theUSCs expressing VEGF (G2) or with endothelial cells (G1)implanted subcutaneously expressed skeletal muscle-specifictranscripts (myf-5, MyoD and desmin) at least 2-fold more thanin the USCs alone (G3) cells. The gel alone (G5) did not displayany expression (Fig. 4B and Table 3).
3.3.3. InnervationMore new nerve fibers appeared within the USCs expressing
VEGF (G2) or with ECs groups (G1) and were identified bydouble staining (Fig. 5A) using the peripheral nerve cell markersneurofilament (NF), S-100, and Glial fibrillary acidic protein(GFAP) combined with GFP and DAPI. Moreover, fewer newnerve fibers were seen in the USCs alone (G3) and humanmyoblast (G4) groups after implantation. Neither significantdifference was found between G1 and G2, nor between G3 andG4 (Fig. 5B and Table 3). However, very few new nerve tissuesstained for GFP antibody, indicating that they were derived fromthe host’s tissue, instead of neurogenic differentiation fromUSCs.

Table 3Summary of USC-gel subcutaneous injection in vivo for 28 days.
Groups 1 2 3 4 5
USCs-GFP/VEGF-ECsþ gel
USCs-GFP/VEGF þ gel
USCs/GFPþgel
Humanmyoblastsþ gel
Gelalone
Gross measurementGraft size 4þ 3þw4þ 3þ 2þw3þ 3þBlood supply 4þ 3þ 2þ þ �
Cell densityDAPI staining 4þ 3þw4þ 2þ 2þ þGFP staining 4þ 3þw4þ þw2þ þ �
AngiogenesisTrichorome
observation4þ 3þw4þ 2þ þ �
CD 31 4þ 3þ þw2þ �wþ �vWF 4þ 3þw4þ 2þ þ �
Muscle tissue engineeringMyoD 4þ 3þw4þ 2þ 4þ �desmin 4þ 3þ 2þ 4þ �myf-5 4þ 3þw4þ þw2þ 4þ �
Nerve regenerationS-100 4þ 3þw4þ þw2þ þ �GFAP 4þ 4þ þ þ �NF 4þ 3þw4þ þ þw2þ �
�, No targeted cell or capillary; þ, 1e25% of G1 changes; 2þ, 25e50% of G1 changes;3þ, 50e75% of G1 changes; 4þ, G1 changes as standard.
G. Liu et al. / Biomaterials 34 (2013) 8617e8629 8623
4. Discussion
Our previous study demonstrated that progenitor/stem cells canbe isolated from voided urine via a simply, safe, low-cost and non-invasive method [7]. USCs possess stem cell characteristics withhighly proliferative capacity because of they display telomeraseactivity [14]. In addition, these cells have multi-potent differenti-ation potential, particularly USCs able to give rise functionalendothelial cells and myocytes. Based on our previous in vivo studyon angiogenic gene-manipulated USCs [12], we further demon-strate, in the present study, that angiogenesis induced by VEGFgene-modified USCs significantly promoted myogenic phenotypedifferentiation of USCs and innervation in vivo, as assessed withtarget cell-specific markers at gene and protein levels. VEGF-expressing USCs in collagen-I gel retained graft size and increasedthe number of cells that survived and recruited more resident cellsafter implantation. In addition, collagen-I gel as a cell friendlybiodegradable biomaterial showed better retention of cells andeasy preparation for the stem cell therapy for potential in treatmentof SUI.
Three types of tissues around the urethra (i.e. muscle, vesselsand peripheral nerve) are associated with urinary continence, andare all potential objectives for stem cell therapies. The sphinctermuscle unit of the urethra contains both internal and externalsphincter muscles. The internal sphincter is the extension of thedetrusor muscle and is made of smooth muscle; thus, it is underinvoluntary or autonomic control, and is the primary muscle forstopping the release of urine. The external sphincter is made ofskeletal muscle which under the voluntary control of the somaticnervous system. The goal of treating SUI is to recover the defect ofboth skeletal and smooth muscles, and neurons in the urethralproximal segment [21]. Bulk injection and pharmacotherapy donot address those goals. The concept of using autologous stemcells for SUI is different from that of using bulking materials. Asmesenchymal stem cells have the potential to give rise to muscle
cells and possess angiogenic and anti-fibrotic effects, variouskinds of mesenchymal stem cells (including skeletal muscle pro-genitor cells, bone marrow stem cells, and adipose stem cells),have been used to treat low-grade SUI, with promising results.However, angiogenic gene-modified mesenchymal stem cellssignificantly improved the function of local tissues scarred due toischemia [22]. In this study, we designed VEGF-expressing USCsfor the potential treatment of moderate- or higher-grade SUIwhere the sphincter tissue is characterized as having a poorblood supply, extensive scarring tissue, weak muscular and nervefunction.
An adequate blood supply is crucial for survival of cells in celltherapy, particularly in the core of the implants [23,24]. VEGF is aclassic growth factor that promotes angiogenesis and maintainsvascularity via its specific mitogenic and anti-apoptotic effects onendothelial cells through the receptors VEGFR-1 and VEGFR-2[25,26]. Mesenchymal stem cells possess angiogenic capacity dueto their paracrine function and production of VEGF in response tooxidative stress or injuries [27]. Bonemarrowmesenchymal stromalcells over-expressing VEGF significantly promoted postischemicmyocardial angiogenesis, reduced infarct size, and enhanced func-tional recovery compared to unmodified cells in a rodent model[28]. In the present study, we demonstrated that USCs could secreteangiogenic growth factors into the culture medium in vitro. Withno adding an exogenous angiogenic factor, the implanted USCsalone improved neo-angiogenesis and myogenesis compared tocell-free controls in vivo by increasing levels of genes and proteinsof endothelial and myogenic markers and more neo vessel for-mations. Moreover, angiogenic gene modification of USCs remark-ably strengthened the angiogenic effects of USCs by increasingneovascularization.
A combination of VEGF gene-modified cells and endothelialcells significantly enhanced revascularization, muscle regenerationand tissue repair [29]. In the current study, VEGF expression plusendothelial cells promotes outcomes in cell survival, cell recruit-ment, myogenesis, innervation and neovascularization that aresimilar to USCs expressing VEGF without endothelial cells. Itmight be because USCs are able to differentiate endothelial cellsand also secrete angiogenic trophic factors. Replacing endothelialcells with USCs could make stem cell therapy more feasible andsimple. Therefore, USCs with pro-angiogenic growth factoradministration could considerably improve revascularization, thecell survival rate and invite more cells from the around tissues toparticipate into tissue repair when used in stem cell therapies intreatment of SUI.
As there are limited opportunities for endogenous myogenicrepair around the urethra after sphincter injuries, stem celltherapies might offer an alternative, less invasive approach fortreatment of SUI. Several clinical trials demonstrated that cellinjection therapy into the mid-urethra restored damaged con-tractile function of the striated muscles and rhabdosphincter[30,31]. Besides multi-potent differentiation capability, mesen-chymal stem cells possess angiogenic, anti-fibrotic, and immunemodulation properties [15]. In the present study, we de-monstrated that USCs can give rise to muscle phenotype cellsand endothelial cells on their own without pre-induction andpromoted angiogenesis in vivo as assessed using immuno-fluorescence staining. Analyses by real-time PCR consistentlydemonstrated myogenic phenotype differentiation and angio-genic effects of USCs compared to human skeletal muscles orcell-free implants. USCs expressed skeletal muscle cell markers(i.e. MyoD, desmin, myf-5, myogenin and myosin) when theywere induced in vitro (data not shown).
In this study, although USCs were not purposefully induced toSkMCs or SMCs in vitro by adding myogenic differentiation

G. Liu et al. / Biomaterials 34 (2013) 8617e86298624
growth factors, USCs on their own gave rise to muscle cellsexpressing skeletal and smooth muscle cell markers after sub-cutaneous implantation. Additionally, myogenic marker expres-sion significantly increased in USCs expressing VEGF groupscompared to non-VEGF USCs groups. Parts of the cells expressingmyogenic markers also displayed GFP, indicating that somedifferentiated cells arose from the implanted human USCs and the
Fig. 3. Immunofluorescent staining and quantitative PCR analysis for endothelial-specific mweeks in vivo. G1 (USCs-VEGF þ ECs), G2 (USCs-VEGF) and G3 (USCs alone) were subjecte(vWF) (top row) and CD31 (bottom row) with GFP. Specific staining (shown by arrows) appeanalysis of immunofluorescent staining for endothelial-specific markers revealed that G1Masson’s trichrome staining revealed VEGF-induced capillary formation in the implanted grain vivo. Little to no revascularization was observed with injection of human myoblasts or gelall five groups using endothelial-specific primers (CD31, vWF). Significantly higher expressiVEGF) than in G3 (USCs alone). However, there was no expression of any specific transcriptinterpretation of the references to colour in this figure legend, the reader is referred to the
remaining cells were recruited from host. When USCs expressingVEGF along with endothelial cells were used, more vesselsformed and more cells expressing muscle markers were observed.This is in agreement with another study, which has demonstratedVEGF would promote differentiation of MSCs into mature muscletissues in vivo [32]. Our data suggest that myogenic phenotypedifferentiation of USCs and muscle tissue engineering in vivo
arkers in vivo. (A) Implants of the different USCs (p3) groups were harvested after 4d to immunofluorescent staining (i) using endothelial markers: von Willebrand factorars red with GFP in green and blue (DAPI). Scale bar ¼ 50 mm. (ii) The hemi-quantitativeand G2 significant improved the angiogenesis than the G3. *p < 0.05, **p < 0.01. (B)ft (arrows). Injection of USCs alone could also promote capillary formation after 28 daysalone. Scale bar ¼ 50 mm. (C) Quantitative real-time PCR was performed on total RNA foron of CD31 and vWF transcripts was observed in G1 (USCs-VEGF þ ECs) and G2 (USCs-seen in G4 (human myoblast injection) and G5 (Gel alone). *p < 0.05, **p < 0.01. (Forweb version of this article.)

Fig. 3. (continued).
G. Liu et al. / Biomaterials 34 (2013) 8617e8629 8625
might function via an indirect effect of angiogenesis that pro-motes muscle cell differentiation [33]. Although the exactmechanistic of myogenic and endothelial differentiation USCs isunknown, three possibilities might occur without pre-conditionalinduction. First, as USCs at p3e4 were already cultured in themedia with 5% FBS for a few weeks, numerous growth factors
(such as myogenic growth factors, i.e. HGF, IGF, PDGF and TGF,and endothelial growth factors, i.e. VEGF) in the serum mightplay role in inducing USCs into different cell lineages as wepreviously reported [7]; Second, as the USCs were adjacent toskeletal muscle tissue after subcutaneously implanted, the hostmuscle tissue might guide USCs to continuously give rise to

Fig. 4. Immunofluorescent staining and quantitative PCR for skeletal myogenic-specific markers in vivo. (A) Implants of different treatment groups of USCs (p3) wereharvested after 4 weeks in vivo. G1 (USCs-VEGF þ ECs), G3 (USCs alone) and G4 (human myoblast injection) were subjected to immunofluorescent staining (i) using skeletalmyogenic markers (myf-5: top row, MyoD: middle row and desmin: bottom row) and GFP. Specific staining (depicted by white arrows) appears red (myf-5, MyoD anddesmin), green (GFP) and blue (nuclei counterstained with DAPI). Scale bar ¼ 25 mm. (ii) The hemi-quantitative analysis of immunofluorescent staining for myogenic-specific markers showed that G1 significant improved the myogenic than the G3 but still lower than G4. *p < 0.05, **p < 0.01. (B) Quantitative real-time PCR per-formed on total RNA for all five groups using myogenic-specific primers (myf-5, MyoD and desmin). Significant higher expression of MyoD, desmin, and myf-5 transcriptswas observed in G1 (USCs-VEGF þ EC) and G2 (USCs-VEGF) than in G3 (USCs alone) but lower than in G4 (human myoblast injection, positive control). However, there wasno expression of any specific transcripts in G5 (Gel alone). *p < 0.05, **p < 0.01. (For interpretation of the references to colour in this figure legend, the reader is referred tothe web version of this article.)
G. Liu et al. / Biomaterials 34 (2013) 8617e86298626

Fig. 4. (continued).
G. Liu et al. / Biomaterials 34 (2013) 8617e8629 8627
muscle-lineage cells in vivo; Third, VEGF secreted from VEGFgenetically-modified USCs might prompt both myogenic and en-dothelial differentiation.
The current study further confirmed our previous observation[11] that USCs expressing VEGF enhance nerve regeneration. Morenerve regeneration occurred in the grafts of USCs expressing VEGFwith or without endothelial cells, compared to the other expressiongroups. Because these regenerated nerve cells had few GFP stain-ing, the nerve fibers most likely originate from the host peripheralnerve due to improved angiogenesis, instead of differentiation fromthe implanted USCs. Obviously, nerve regeneration could helprecover muscle sphincter function and correct SUI.
Histopathologically, chronic SUI also can be classified into mild,moderate and severe according to sphincter muscle damage,amount scarring tissue formation, vascularization, and never fiberdensity. In severe SUI, there appear more sphincter muscle dam-age, heavier scar tissue, fewer blood supply, lack of nerve existing[34,35]. MSCs alone are able to achieve satisfying outcome incertain cases with mild or even moderate SUI in clinical setting[36]. However, USCs combined with pro-angiogenic growth factorsvia gene transfection or nano-particular slow releasing system [9]appear more suitable for cases with severe SUI. Importantly, notumor tissue or ectopic bone tissue were found 4 weeks afterimplantation. A longer-term follow-up of the outcome with USCs

Fig. 5. Immunofluorescent staining and semi-quantitation of native nerve regeneration. USCs with or without VEGF expression were subcutaneously injected into nude mice andanalyzed after 28 days. (A) Cross-sections of G1 (USCs/VEGF-GFP þ EC) and G3 (USCs/GFP) implants displayed regenerated peripheral nerve. Staining with GFP (green), nuclearcounterstain DAPI (blue), and nerve cell antibodies (red) e Glial Fibrillary Acidic Protein (GFAP) (left row), S-100 (middle row) and Neurofilament (NF) (right row) e show increasednative nerve regeneration with implants containing USCs expressing VEGF as compared to the non-VEGF group. Scale bar ¼ 50 mm. (B) VEGF containing groups showed asignificantly increased number of nerve fibers, hence promoting regeneration of peripheral nerve. *p < 0.05, **p < 0.01. (For interpretation of the references to colour in this figurelegend, the reader is referred to the web version of this article.)
G. Liu et al. / Biomaterials 34 (2013) 8617e86298628
combined with pro-angiogenic growth factor administration hasbeen further preformed in our ongoing study.
5. Conclusions
Myogenic repair with stem cell therapy aims to rebuild thecontractile function of the striated muscles and rhabdosphincter tocorrect SUI. USCs can differentiate into endothelial and muscle-lineage cells that might promote revascularization and muscleregeneration, via either myogenic phenotype differentiation of
stem cells or paracrine function of stem cells. Our study demon-strated that the angiogenic potential of USCs in collagen-I hydrogelappreciably increased cell viability, resident cell recruitment,myogenic regeneration, and innervation via angiogenic effects, thistreatment might be indicated the potential in treatment of patientswith moderate to severe SUI.
Disclosure statement
No conflicts of interest exist.

G. Liu et al. / Biomaterials 34 (2013) 8617e8629 8629
Acknowledgements
The authors would like to thank Ms. Karen Klein (ResearchSupport Core, Wake Forest School of Medicine) for her editorialassistance with this manuscript.
References
[1] Dissaranan C, Cruz MA, Couri BM, Goldman HB, Damaser MS. Stem celltherapy for incontinence: where are we now? what is the realistic potential?Curr Urol Rep 2011;12:336e44.
[2] Bent AE, Tutrone RT, McLennan MT, Lloyd LK, Kennelly MJ, Badlani G. Treat-ment of intrinsic sphincter deficiency using autologous ear chondrocytes as abulking agent. Neurourol Urodyn 2001;20:157e65.
[3] Yokoyama T, Pruchnic R, Lee JY, Chuang YC, Jumon H, Yoshimura N, et al.Autologous primary muscle-derived cells transfer into the lower urinary tract.Tissue Eng 2001;7:395e404.
[4] Gunetti M, Tomasi S, Giammo A, Boido M, Rustichelli D, Mareschi K, et al.Myogenic potential of whole bone marrow mesenchymal stem cells in vitroand in vivo for usage in urinary incontinence. PLoS One 2012;7:e45538.
[5] Lin G, Wang G, Banie L, Ning H, Shindel AW, Fandel TM, et al. Treatment ofstress urinary incontinence with adipose tissue-derived stem cells. Cyto-therapy 2010;12:88e95.
[6] Lang R, Liu G, Shi Y, Bharadwaj S, Leng X, Zhou X, et al. Self-renewal anddifferentiation capacity of urine-derived stem cells after urine preservation for24 hours. PLoS One 2013;8:e53980.
[7] Zhang Y, McNeill E, Tian H, Soker S, Andersson KE, Yoo JJ, et al. Urine derivedcells are a potential source for urological tissue reconstruction. J Urol2008;180:2226e33.
[8] Bodin A, Bharadwaj S, Wu S, Gatenholm P, Atala A, Zhang Y. Tissue-engineeredconduit using urine-derived stem cells seeded bacterial cellulose polymer inurinary reconstruction and diversion. Biomaterials 2010;31:8889e901.
[9] Liu G, Pareta RA, Wu R, Shi Y, Zhou X, Liu H, et al. Skeletal myogenic differ-entiation of urine-derived stem cells and angiogenesis using microbeadsloaded with growth factors. Biomaterials 2013;34:1311e26.
[10] Bharadwaj S, Liu G, Shi Y, Markert C, Andersson KE, Atala A, et al. Charac-terization of urine-derived stem cells obtained from upper urinary tract foruse in cell-based urological tissue engineering. Tissue Eng Part A 2011;17:2123e32.
[11] Wu S, Liu Y, Bharadwaj S, Atala A, Zhang Y. Human urine-derived stem cellsseeded in a modified 3D porous small intestinal submucosa scaffold for ure-thral tissue engineering. Biomaterials 2011;32:1317e26.
[12] Wu S, Wang Z, Bharadwaj S, Hodges SJ, Atala A, Zhang Y. Implantation ofautologous urine derived stem cells expressing vascular endothelial growthfactor for potential use in genitourinary reconstruction. J Urol 2011;186:640e7.
[13] Smaldone MC, Chen ML, Chancellor MB. Stem cell therapy for urethralsphincter regeneration. Minerva Urol Nefrol 2009;61:27e40.
[14] Bharadwaj S, Liu G, Shi Y, Wu R, Yang B, He T, et al. Multi-potential differ-entiation of human urine-derived stem cells: potential for therapeutic ap-plications in urology. Stem Cells 2013. http://dx.doi.org/10.1002/stem. 1424[Epub ahead of print].
[15] Djouad F, Bouffi C, Ghannam S, Noel D, Jorgensen C. Mesenchymal stem cells:innovative therapeutic tools for rheumatic diseases. Nat Rev Rheumatol2009;5:392e9.
[16] Hilborn J. In vivo injectable gels for tissue repair. Wiley Interdiscip RevNanomed Nanobiotechnol 2011. http://dx.doi.org/10.1002/wnan.91 [Epubahead of print].
[17] Gutowska A, Jeong B, Jasionowski M. Injectable gels for tissue engineering.Anat Rec 2001;263:342e9.
[18] Puetzer JL, Bonassar LJ. High density type I collagen gels for tissue engineeringof whole Menisci. Acta Biomater 2013;9:7787e95.
[19] Wallace DG, Rosenblatt J. Collagen gel systems for sustained delivery andtissue engineering. Adv Drug Deliv Rev 2003;55:1631e49.
[20] Lang I, Schweizer A, Hiden U, Ghaffari-Tabrizi N, Hagendorfer G, Bilban M,et al. Human fetal placental endothelial cells have a mature arterial and ajuvenile venous phenotype with adipogenic and osteogenic differentiationpotential. Differentiation 2008;76:1031e43.
[21] Stangel-Wojcikiewicz K, Malgorzata S, Nikolavsky D, Chancellor MB. Cellulartherapy for treatment of stress urinary incontinence. Curr Stem Cell Res Ther2010;5:57e62.
[22] Das H, George JC, Joseph M, Das M, Abdulhameed N, Blitz A, et al. Stem celltherapy with overexpressed VEGF and PDGF genes improves cardiac functionin a rat infarct model. PLoS One 2009;4:e7325.
[23] Shudo Y, Miyagawa S, Fukushima S, Saito A, Shimizu T, Okano T, et al. Novelregenerative therapy using cell-sheet covered with omentum flap delivers ahuge number of cells in a porcine myocardial infarction model. J ThoracCardiovasc Surg 2011;142:1188e96.
[24] Lindvall O, Kokaia Z, Martinez-Serrano A. Stem cell therapy for humanneurodegenerative disorders-how to make it work. Nat Med 2004;10(Suppl.):S42e50.
[25] Kang SK, Kang KS, Jee MK, Kim BS. Vascular endothelial growth factor/kinaseinsult domain receptor (KDR)/fetal liver kinase 1 (FLK1)-mediated skin-epithelial progenitor cells reprogramming. Tissue Eng Part A 2010;16:2687e97.
[26] Imoukhuede PI, Popel AS. Expression of VEGF receptors on endothelial cells inmouse skeletal muscle. PLoS One 2012;7:e44791.
[27] Wang M, Crisostomo PR, Herring C, Meldrum KK, Meldrum DR. Human pro-genitor cells from bone marrow or adipose tissue produce VEGF, HGF, andIGF-I in response to TNF by a p38 MAPK-dependent mechanism. Am J PhysiolRegul Integr Comp Physiol 2006;291:R880e4.
[28] Wang Y, Haider HK, Ahmad N, Xu M, Ge R, Ashraf M. Combining pharmaco-logical mobilization with intramyocardial delivery of bone marrow cells over-expressing VEGF is more effective for cardiac repair. J Mol Cell Cardiol2006;40:736e45.
[29] Nomi M, Miyake H, Sugita Y, Fujisawa M, Soker S. Role of growth factors andendothelial cells in therapeutic angiogenesis and tissue engineering. CurrStem Cell Res Ther 2006;1:333e43.
[30] Becker C, Jakse G. Stem cells for regeneration of urological structures. Eur Urol2007;51:1217e28.
[31] Mitterberger M, Pinggera GM, Marksteiner R, Margreiter E, Fussenegger M,Frauscher F, et al. Adult stem cell therapy of female stress urinary inconti-nence. Eur Urol 2008;53:169e75.
[32] Kim MH, Hong HN, Hong JP, Park CJ, Kwon SW, Kim SH, et al. The effect ofVEGF on the myogenic differentiation of adipose tissue derived stem cellswithin thermosensitive hydrogel matrices. Biomaterials 2010;31:1213e8.
[33] Youssif M, Shiina H, Urakami S, Gleason C, Nunes L, Igawa M, et al. Effectof vascular endothelial growth factor on regeneration of bladder acel-lular matrix graft: histologic and functional evaluation. Urology 2005;66:201e7.
[34] O’Sullivan R, Karantanis E, Stevermuer TL, Allen W, Moore KH. Definition ofmild, moderate and severe incontinence on the 24-hour pad test. BJOG2004;111:859e62.
[35] Gunasekaran K. Stress urinary incontinence e an overview. J Indian MedAssoc 2011;109:721e2.
[36] Stangel-Wojcikiewicz K, Majka M, Basta A, Stec M, Pabian W, Piwowar M,et al. Adult stem cells therapy for urine incontinence in women. Ginekol Pol2010;81:378e81.