the effects of brief incarcerations on jail diversion outcomes for people with serious mental...
TRANSCRIPT
The Effects of Brief Incarcerations on Jail Diversion Outcomes for People with
Serious Mental Illness
Presenter: Allison Gilbert Robertson, Ph.D., M.P.H.Duke University School of Medicine
Department of Psychiatry & Behavioral [email protected]
Academic and Health Policy Conference on Correctional Health
Chicago, ILMarch 22, 2013
Sponsor and Collaborators• Duke University Medical Center
– Allison Gilbert Robertson, PhD, MPH (PI)– Marvin Swartz, MD (Co-PI)
• Connecticut Dept. of Mental Health and Addiction Services (DMHAS)/UConn SSW– Hsiu-Ju Lin, PhD – Linda Frisman, PhD
• University of South Florida– John Petrila, JD, LLM
This work was funded by Public Health Law Research, a national program of the Robert
Wood Johnson Foundation.
Jail diversion• Court-based jail diversion programs: a growing
policy response to problem of CJ involvement among adults with SMI– ~560 diversion programs are currently operating in 47 states
• Various program models—MH court structure, others use alternative approaches
• Common criteria include:– SMI diagnosis– Many exclude felony or violent offenders– Indication that mental illness was a contributing factor in referral
offense, determination of “suitability”– Willingness to comply with court-arranged treatment plan
Jail diversion: what we know now
• Generally, significant reductions in recidivism are evident– But improvements are modest
• Evidence lacking on which program components predict successful diversion– Access to treatment services. . . ?– A legal mechanism that uniquely engages
participants and promotes their success. . . ?

CT’s jail diversion program• CT one of two states with an innovative, statewide jail
diversion program
• Community MH clinicians based in courts – Work with court personnel to identify and divert eligible adults
SMI
• Reports that some judges opt to first put some individuals in jail for a few days to enhance motivation for entering treatment and avoiding a jail sentence
- Enhance motivation - Ineffective, inappropriate - Good set up for Tx - Traumatizing
– Detox– Stabilization
Therapeutic jurisprudence
Counter-therapeutic and -productive
- or -

Research QuestionsCompared to immediate diversion, to what
extent do brief jail stays before initiating diversion improve outcomes by. . .
1) further reducing use of crisis-driven health
care (i.e., hospitalization and ED visits)?
2) further reducing recidivism (subsequent arrest and incarceration)?
Study DesignPart 1: Observational study of effect of pre-
diversion brief incarcerations• Quasi-experimental study of administrative records from
public behavioral health and CJ systems for adults with SMI who participated in a statewide jail diversion program in Connecticut during FYs 2006 & 2007
Part 2: Diversion observations and personnel interviews
• Observations of jail diversion proceedings in CT courts • Informal interviews with key jail diversion and court
personnel

Study MeasuresDependent variables• Psychotropic medication adherence
– Medication possession ratio
• Targeted outpatient service use
• Hospitalizations for MH or substance abuse treatment
• ED visits
• Rearrest
• (Re)incarceration

Study MeasuresDependent variables• Psychotropic medication adherence
– Medication possession ratio
• Targeted outpatient service use
• Hospitalizations for MH or substance abuse treatment
• ED visits
• Rearrest
• (Re)incarceration
Study MeasuresDependent variables• Psychotropic medication adherence
– Medication possession ratio
• Targeted outpatient service use
• Hospitalizations for MH or substance abuse treatment
• ED visits
• Rearrest
• (Re)incarceration

Study Measures
Independent variables
• Study group variable: “Jail first” - any v. no brief incarceration before diversion
• Clinical diagnoses & demographics
• Pre-diversion OP service use
• Pre-diversion psychotropic medication adherence
• Recent offending history
Analysis • Propensity-score matching to identify a balanced
comparison group
• Multivariable models to estimate effect of jail first on probability and level of recidivism and crisis-driven service use– Generalized Estimating Equations (GEE) for binary
outcomes – Mixed-effects, mixed-distribution models for count
variables with many zeros– Structural Equation Models for mediation analysis

Clinical and demographic characteristics after propensity matching
Age (mean) 34.71 years
SexMale 58.8%Female 41.2%
RaceWhite 47.5%African American 27.5%Hispanic 22.1%Other 2.9%
Primary diagnosisSchizophrenia 49.5%Bipolar 50.5%
Dual diagnosis 79.3%
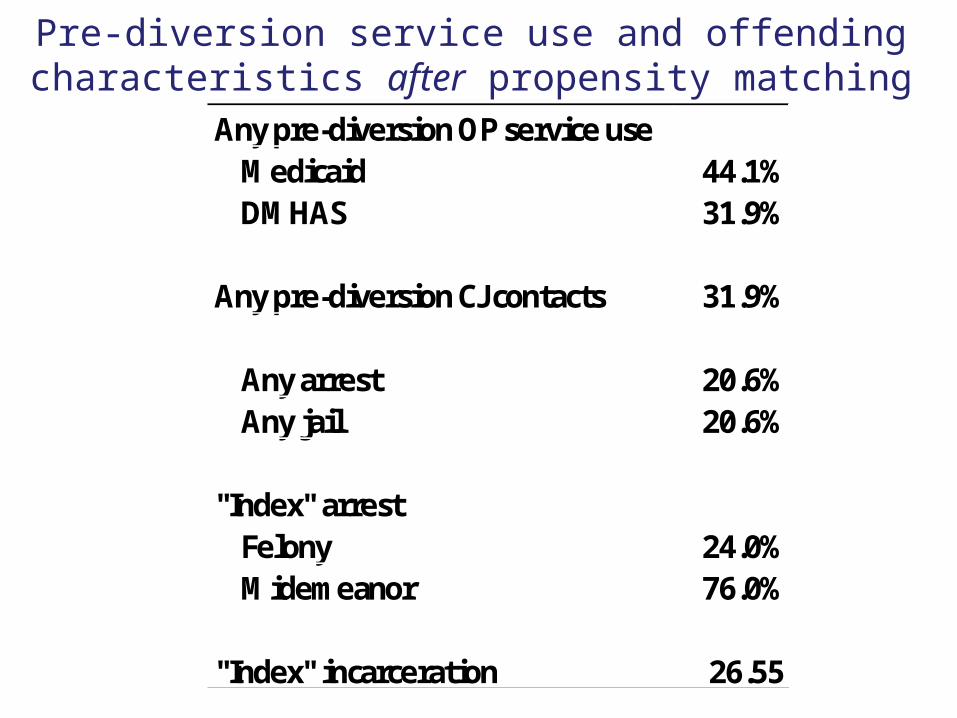
Pre-diversion service use and offending characteristics after propensity matching
Any pre-diversion OP service useMedicaid 44.1%DMHAS 31.9%
Any pre-diversion CJ contacts 31.9%
Any arrest 20.6%Any jail 20.6%
"Index" arrestFelony 24.0%Midemeanor 76.0%
"Index" incarceration 26.55
Regression results
Independent variables Coeff Coeff Coeff Coeff
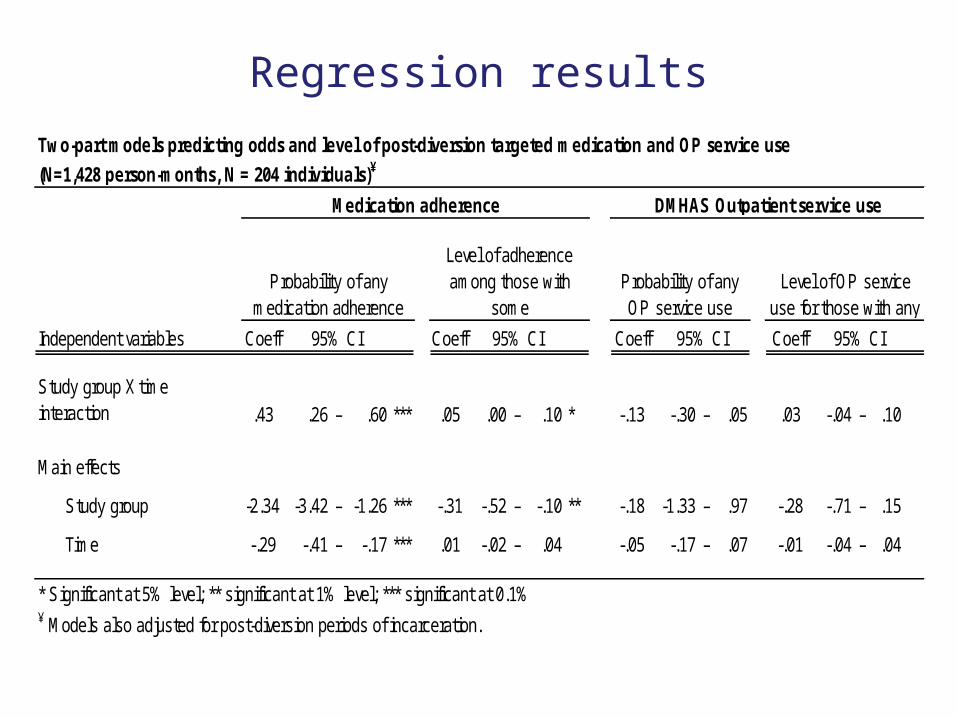
.43 .26 – .60 *** .05 .00 – .10 * -.13 -.30 – .05 .03 -.04 – .10
Main effects
Study group -2.34 -3.42 – -1.26 *** -.31 -.52 – -.10 ** -.18 -1.33 – .97 -.28 -.71 – .15
Time -.29 -.41 – -.17 *** .01 -.02 – .04 -.05 -.17 – .07 -.01 -.04 – .04DMHAS OP service use .10 .07 – .13 *** .01 .00 .02 *** -- -- -- -- -- --* Significant at 5% level; ** significant at 1% level; *** significant at 0.1%¥ Models also adjusted for post-diversion periods of incarceration.
95% CI 95% CI 95% CI 95% CI
Study group X time interaction
Two-part models predicting odds and level of post-diversion targeted medication and OP service use
(N=1,428 person-months, N = 204 individuals)¥
Medication adherence DMHAS Outpatient service use
Probability of any medication adherence
Level of adherence among those with
someProbability of any OP service use
Level of OP service use for those with any
Regression results
Independent variables Coeff Coeff Coeff Coeff
.43 .26 – .60 *** .05 .00 – .10 * -.13 -.30 – .05 .03 -.04 – .10
Main effects
Study group -2.34 -3.42 – -1.26 *** -.31 -.52 – -.10 ** -.18 -1.33 – .97 -.28 -.71 – .15
Time -.29 -.41 – -.17 *** .01 -.02 – .04 -.05 -.17 – .07 -.01 -.04 – .04DMHAS OP service use .10 .07 – .13 *** .01 .00 .02 *** -- -- -- -- -- --* Significant at 5% level; ** significant at 1% level; *** significant at 0.1%¥ Models also adjusted for post-diversion periods of incarceration.
95% CI 95% CI 95% CI 95% CI
Study group X time interaction
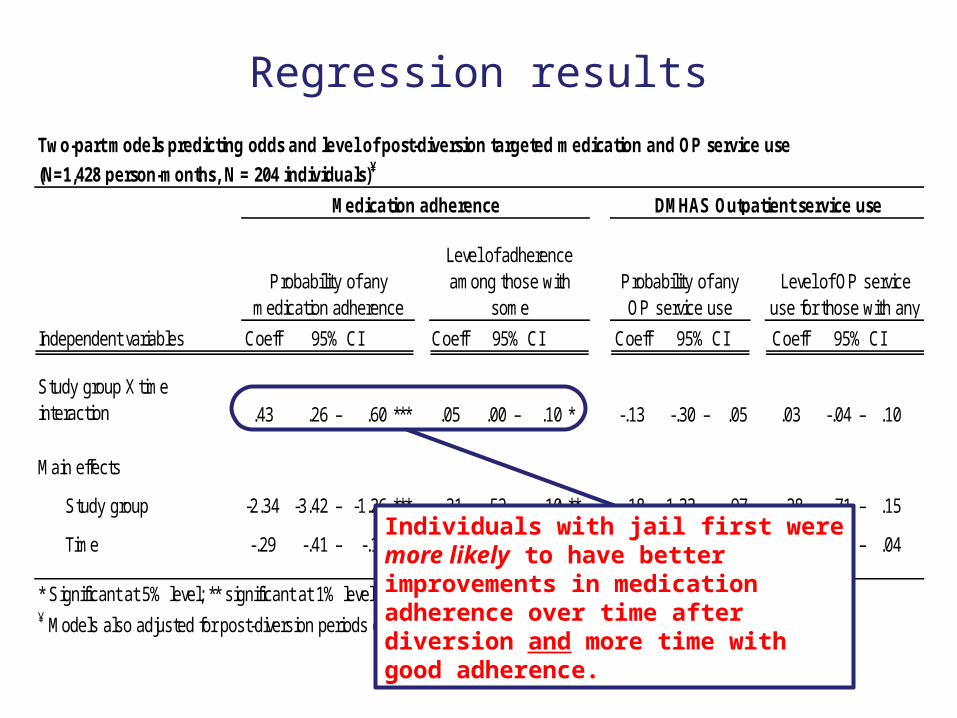
Two-part models predicting odds and level of post-diversion targeted medication and OP service use
(N=1,428 person-months, N = 204 individuals)¥
Medication adherence DMHAS Outpatient service use
Probability of any medication adherence
Level of adherence among those with
someProbability of any OP service use
Level of OP service use for those with any
Individuals with jail first were more likely to have better improvements in medication adherence over time after diversion and more time with good adherence.
Regression results
Independent variables Coeff Coeff Coeff Coeff
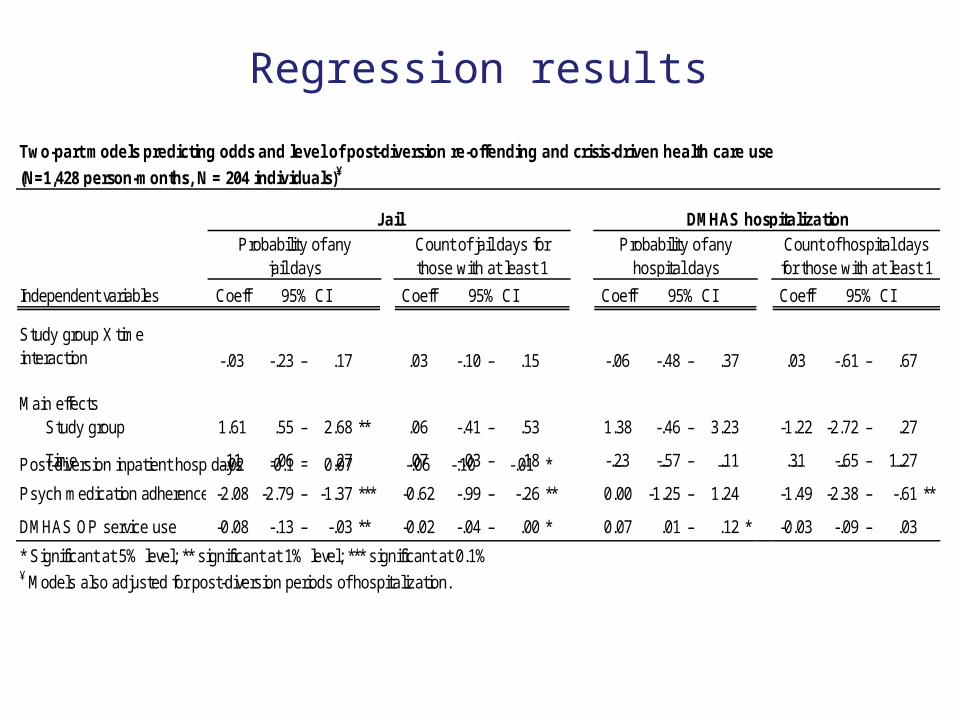
-.03 -.23 – .17 .03 -.10 – .15 -.06 -.48 – .37 .03 -.61 – .67
Main effectsStudy group 1.61 .55 – 2.68 ** .06 -.41 – .53 1.38 -.46 – 3.23 -1.22 -2.72 – .27
Time .11 -.06 – .27 .07 -.03 – .18 -.23 -.57 – .11 .31 -.65 – 1.27Post-diversion inpatient hosp days-.02 -0.1 – 0.07 -.06 -.10 -.01 * -- -- -- -- -- --
Psych medication adherence -2.08 -2.79 – -1.37 *** -0.62 -.99 – -.26 ** 0.00 -1.25 – 1.24 -1.49 -2.38 – -.61 **
DMHAS OP service use -0.08 -.13 – -.03 ** -0.02 -.04 – .00 * 0.07 .01 – .12 * -0.03 -.09 – .03
* Significant at 5% level; ** significant at 1% level; *** significant at 0.1%¥ Models also adjusted for post-diversion periods of hospitalization.
Two-part models predicting odds and level of post-diversion re-offending and crisis-driven health care use
(N=1,428 person-months, N = 204 individuals)¥
Study group X time interaction
DMHAS hospitalizationProbability of any
hospital daysCount of hospital days for those with at least 1
95% CI 95% CI
Probability of any jail days
Count of jail days for those with at least 1
95% CI 95% CI
Jail

Regression results
Independent variables Coeff Coeff Coeff Coeff
-.03 -.23 – .17 .03 -.10 – .15 -.06 -.48 – .37 .03 -.61 – .67
Main effectsStudy group 1.61 .55 – 2.68 ** .06 -.41 – .53 1.38 -.46 – 3.23 -1.22 -2.72 – .27
Time .11 -.06 – .27 .07 -.03 – .18 -.23 -.57 – .11 .31 -.65 – 1.27Post-diversion inpatient hosp days-.02 -0.1 – 0.07 -.06 -.10 -.01 * -- -- -- -- -- --
Psych medication adherence -2.08 -2.79 – -1.37 *** -0.62 -.99 – -.26 ** 0.00 -1.25 – 1.24 -1.49 -2.38 – -.61 **
DMHAS OP service use -0.08 -.13 – -.03 ** -0.02 -.04 – .00 * 0.07 .01 – .12 * -0.03 -.09 – .03
* Significant at 5% level; ** significant at 1% level; *** significant at 0.1%¥ Models also adjusted for post-diversion periods of hospitalization.
Two-part models predicting odds and level of post-diversion re-offending and crisis-driven health care use
(N=1,428 person-months, N = 204 individuals)¥
Study group X time interaction
DMHAS hospitalizationProbability of any
hospital daysCount of hospital days for those with at least 1
95% CI 95% CI
Probability of any jail days
Count of jail days for those with at least 1
95% CI 95% CI
Jail
No differences in probability or level of post-diversion incarceration or psych hospitalization between study groups.

Regression results
Independent variables Coeff Coeff Coeff Coeff
-.03 -.23 – .17 .03 -.10 – .15 -.06 -.48 – .37 .03 -.61 – .67
Main effectsStudy group 1.61 .55 – 2.68 ** .06 -.41 – .53 1.38 -.46 – 3.23 -1.22 -2.72 – .27
Time .11 -.06 – .27 .07 -.03 – .18 -.23 -.57 – .11 .31 -.65 – 1.27Post-diversion inpatient hosp days-.02 -0.1 – 0.07 -.06 -.10 -.01 * -- -- -- -- -- --
Psych medication adherence -2.08 -2.79 – -1.37 *** -0.62 -.99 – -.26 ** 0.00 -1.25 – 1.24 -1.49 -2.38 – -.61 **
DMHAS OP service use -0.08 -.13 – -.03 ** -0.02 -.04 – .00 * 0.07 .01 – .12 * -0.03 -.09 – .03
* Significant at 5% level; ** significant at 1% level; *** significant at 0.1%¥ Models also adjusted for post-diversion periods of hospitalization.
Two-part models predicting odds and level of post-diversion re-offending and crisis-driven health care use
(N=1,428 person-months, N = 204 individuals)¥
Study group X time interaction
DMHAS hospitalizationProbability of any
hospital daysCount of hospital days for those with at least 1
95% CI 95% CI
Probability of any jail days
Count of jail days for those with at least 1
95% CI 95% CI
Jail
People with good medication adherence were less likely to go to jail after diversion; and among those who did, those with good medication adherence were incarcerated for fewer days.

Regression results
Independent variables Coeff Coeff Coeff Coeff
-.03 -.23 – .17 .03 -.10 – .15 -.06 -.48 – .37 .03 -.61 – .67
Main effectsStudy group 1.61 .55 – 2.68 ** .06 -.41 – .53 1.38 -.46 – 3.23 -1.22 -2.72 – .27
Time .11 -.06 – .27 .07 -.03 – .18 -.23 -.57 – .11 .31 -.65 – 1.27Post-diversion inpatient hosp days-.02 -0.1 – 0.07 -.06 -.10 -.01 * -- -- -- -- -- --
Psych medication adherence -2.08 -2.79 – -1.37 *** -0.62 -.99 – -.26 ** 0.00 -1.25 – 1.24 -1.49 -2.38 – -.61 **
DMHAS OP service use -0.08 -.13 – -.03 ** -0.02 -.04 – .00 * 0.07 .01 – .12 * -0.03 -.09 – .03
* Significant at 5% level; ** significant at 1% level; *** significant at 0.1%¥ Models also adjusted for post-diversion periods of hospitalization.
Two-part models predicting odds and level of post-diversion re-offending and crisis-driven health care use
(N=1,428 person-months, N = 204 individuals)¥
Study group X time interaction
DMHAS hospitalizationProbability of any
hospital daysCount of hospital days for those with at least 1
95% CI 95% CI
Probability of any jail days
Count of jail days for those with at least 1
95% CI 95% CI
Jail
Among people with at least one DMHAS hospital day after diversion, those with good medication adherence were hospitalized for fewer days than those with poor adherence.
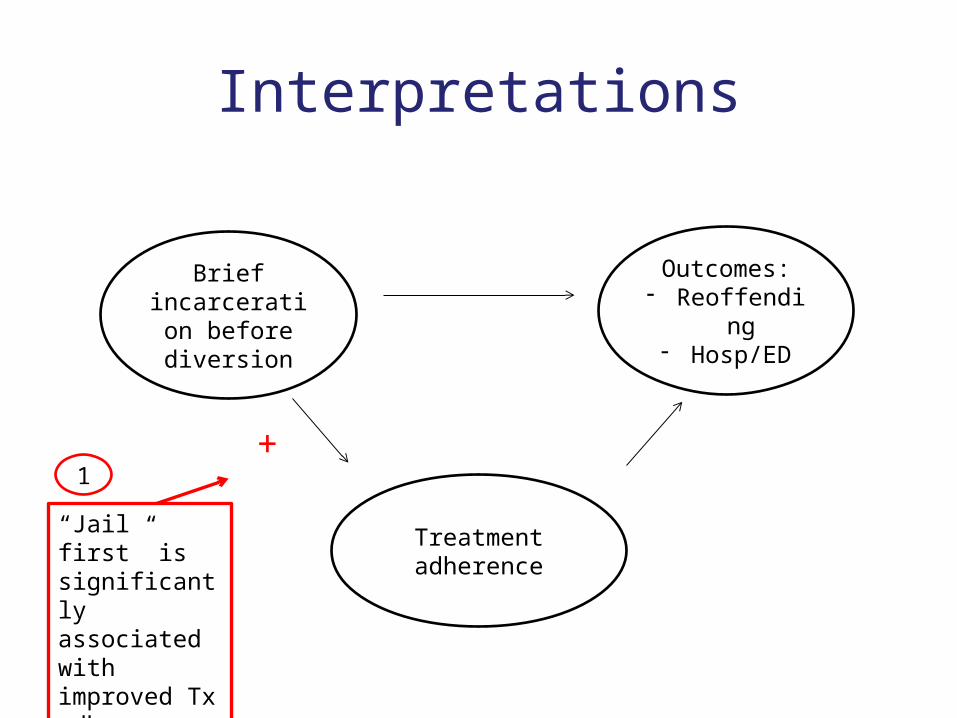
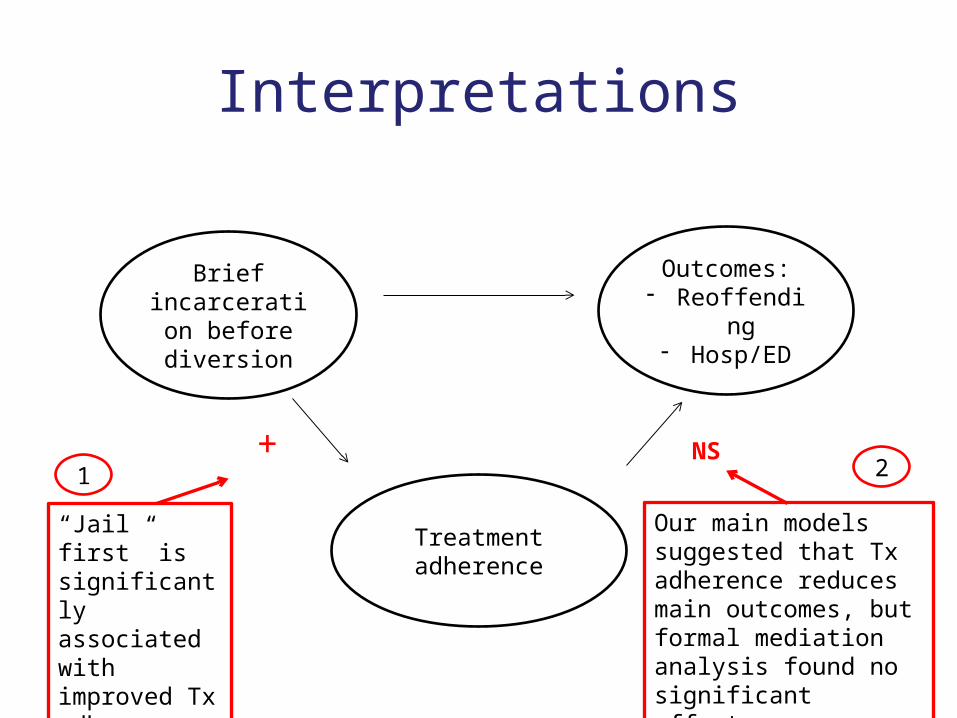
Interpretations
Brief incarceration
before diversion
Treatment adherence
Outcomes:- Reoffending- Hosp/ED
+
“Jail first” is significantly associated with improved Tx adherence.
1
Interpretations
Brief incarceration
before diversion
Treatment adherence
Outcomes:- Reoffending- Hosp/ED
+
“Jail first” is significantly associated with improved Tx adherence.
NS
Our main models suggested that Tx adherence reduces main outcomes, but formal mediation analysis found no significant effect.
1 2
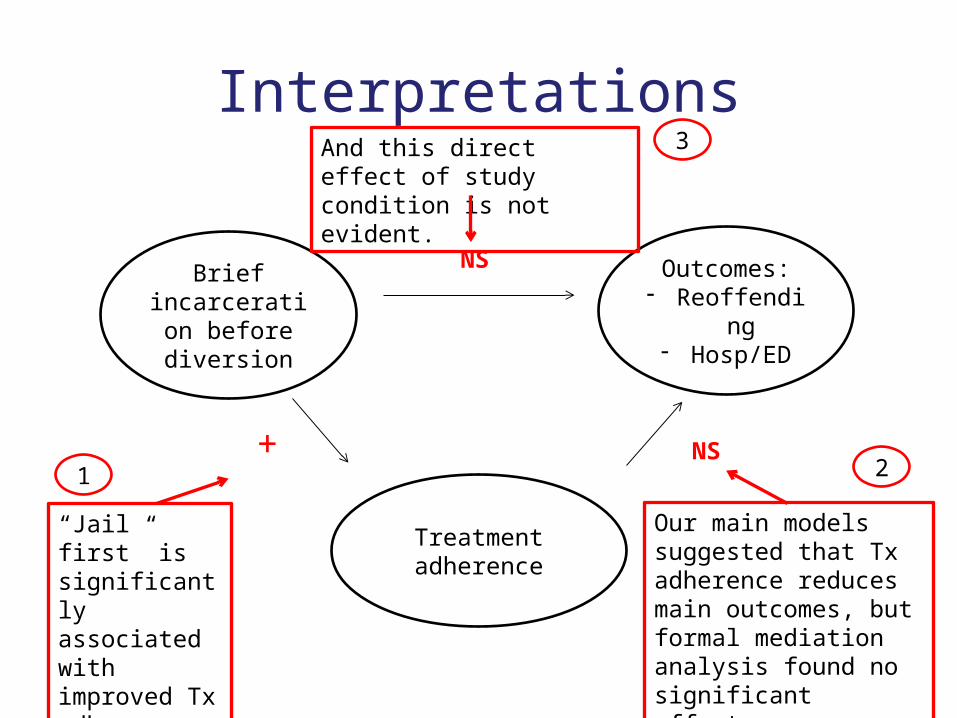
Interpretations
Brief incarceration
before diversion
Treatment adherence
Outcomes:- Reoffending- Hosp/ED
+
“Jail first” is significantly associated with improved Tx adherence.
NS
Our main models suggested that Tx adherence reduces main outcomes, but formal mediation analysis found no significant effect.
And this direct effect of study condition is not evident.
NS
1 2
3
Summary and next steps
• Explore moderator analyses – Estimating effects of jail before diversion on
specific sub-groups (e.g., dual Dx, felony index arrest)
• Future research – Examine role of Tx adherence more closely
• How/why jail first improve Tx adherence• Why that doesn’t translate to improved health and
public safety outcomes
Thank you!

Extra slides

CT site visit and interviews• Semi-structured interviews with key players in
jail diversion program– Judge, bail commissioners, public defender, PD social
worker, court coordinator, jail diversion clinicians
• Key themes emerged– Where goal is to divert clients at arraignment, public
safety comes first– “Frequent fliers” among most likely to get some pre-
diversion jail time; many perceived to be willingly making bad choices
– Need for detox, general stabilization in combination with lack of Tx slots also often means jail time first
Propensity Score Method
• Step 1:– Case control match with local greedy algorithm
• Is a local matching algorithm, i.e., making optimal matching decisions at each step without attempting to make the best overall global matching decision
• Once a match is made, the match is not reconsidered• Study group cases are ordered and sequentially matched to the nearest unmatched
control group cases• If more than one unmatched control matches to a case, the control is random selected• 92 cases matched
• Step 2:– Distance score within same quintile
• For 10 un-matched cases, distance scores were computed between treated cases unmatched control cases with the same quintile
• Unmatched control case with smallest absolute distance is selected• All 102 matched, and all covariates were balanced between study and control groups

Latent Growth Curve Analysis
Study group
Baseline- CJ
Slope- CJ
Baseline - Rx
Slope- Rx
-0.205** 0.031**
-2.086
0.368
0.082
-1.075*
0.210