the efficacy and safety of a new ciprofloxacin suspension ... · suspension as a 10% solution...
TRANSCRIPT
RESPIRATORY MEDICINE (1999) 93, 252-261
The efficacy and safety of a new ciprofloxacin suspension compared with co-amoxiclav tablets in the treatment of acute exacerbations of chronic bronchitis
R. C. READ*, A. Kuss+, F. BERBISOUL*, N. KEARSLEY”, A. TORRE# AND R. KUBIN~
*Royal Hallamshire Hospital, Glossop Road, Sheffield, SIO 2]F, U.k, ’ Wesffalensfr. 24, 40472 Diisseldorf, Germany *61 rue Balard, 75015, Paris, France ‘Richmond Medical Cenfre, 462 Richmond Road, Sheffield, U.K. “Pulmonology Department, Co-ordinafor Insfifufe for Respiratory Diseases, Hospital Clinic, Villarroel 170, 08036 Barcelona, Spain TBayer Plc, Pharmaceufical Division, Strawberry Hill, Newbury, Berkshire RG14 l]A, U.K.
A multinational, multicentre, randomized, prospective, parallel-group study compared treatment with ciprofloxacin administered as an oral suspension (500 mg twice daily for 7 days) with co-amoxiclav tablets (625 mg three times daily for 7 days) in patients suffering from acute exacerbations of chronic bronchitis (AECB).
A total of 147 of 165 cases treated with ciprofloxacin (89.1%) and 146 of 162 cases treated with co-amoxiclav (90.1%) were classified as being clinical successes at the primary efficacy assessment 7 days after the end of therapy (assessed as reduced cough, improvement in dyspnoea, reduction in 24-h sputum volume or reduced purulence of sputum). Treatment equivalence was statistically confirmed; treatment difference: - l.O%, 95% CI - 6.6% and 4.5%.
Before treatment, 128 bacterial strains were isolated from 103 patients (60 ciprofloxacin and 68 co-amoxiclav). The most commonly isolated organism was Haemophilus influenzae (60 isolates), followed by Moraxella catarrhalis (12 isolates), Streptococcus pneumoniae (11 isolates) and Staphylococcus aureus (10 isolates). At day 14, 40 of 46 ciprofloxacin-treated patients (87.0%) and 46 of 55 co-amoxiclav-treated patients (83.6%) who were valid for bacteriological analysis were classified as being bacteriological successes (classed as eradication, eradication with colonization or presumed eradication; treatment difference: 3.3%, 95% CI - 8.3% and 14.9%).
The adverse event profile was comparable between treatment groups. Most adverse events considered possibly or probably related to study drug were related to the gastrointestinal system and were of mild or moderate severity: nausea (13% ciprofloxacin, 10.6% co-amoxiclav), flatulence (10.3% ciprofloxacin, 3.9% co-amoxiclav), abdominal pain (7.6% ciprofloxacin, 7.3% co-amoxiclav) and diarrhoea (4.3% ciprofloxacin, 6.7% co-amoxiclav).
We concluded that a 7-day course of ciprofloxacin suspension is equivalent to a 7-day course of co-amoxiclav tablets in terms of clinical and bacteriological efficacy and tolerability for the treatment of AECB. Thus, ciprofloxacin suspension may offer a suitable alternative treatment for AECB patients who have difficulty in swallowing, or who prefer liquid medications to tablets.
RESPIR. MED. (1999) 93, 252-261
Introduction
Acute exacerbations of chronic bronchitis (AECB) are generally characterized by increased cough, dyspnoea, and sputum production (1,2). The pathogen most often associ- ated with AECB is Haemophilus injfuenzae, accounting for more than 50% of all bacterial exacerbations (2-4). Other
Received 2 October 1998 and accepted in revised form 18 January 1999.
organisms associated with AECB include Moraxella catarrhalis, Streptococcus pneumoniae and Haemophilus parainjluenzae, with a smaller incidence of Klebsiella spp. and Pseudomonas spp. (l-3).
Most patients with AECB in primary care are treated with antibiotics, but there is increasing anxiety about the effectiveness of many of the currently used first-line antibiotics. Resistance to penicillins and cephalosporins continues to increase world-wide, especially amongst b-lactamase-producing bacteria such as H. injluenzae and
0954-6111/99/040252+ 10 $12.0010 0 1999 W. B. SAUNDERS COMPANY LTD

CIPROFLOXACIN COMPARED WITH CO-AMOXICLAV 253
AL catarrhalis, and the prevalence of S. pneumoniae strains resistant to penicillins and other antibiotics is also rising (5-7).
Ciprofloxacin is a 4-fluoroquinolone with a broad anti- bacterial spectrum against both Gram-negative and Gram- positive organisms. It does not have ideal activity against S. pneumoniae, but clinical studies on AECB have shown that ciprofloxacin is at least as effective as comparator antibiotics (8-16). The drug is 85% bioavailable after oral administration and has excellent tissue distribution (17,18). Ciprofloxacin, like other fluoroquinolones, acts by inter- action with DNA gyrase, a bacterial topoisomerase that is responsible for negative super-coiling of DNA within the bacterial cell ( 19).
The new ciprofloxacin oral suspension has comparable pharmacokinetics to the tablet formulation of the drug (data on file, Bayer AG, Wuppertal, Germany) and food has no significant effect on the absorption of this new formulation (data on file, Bayer AG, Wuppertal, Germany). Ease of administration of an oral medication is particularly important for patients for whom swallowing is difficult, such as the elderly, and patients with anatomical or dysfunctional problems.
The aim of this study was to compare the efficacy and tolerability of a ciprofloxacin oral suspension (500 mg twice daily for 7 days) with that of co-amoxiclav (625 mg three times daily for 7 days), an antibiotic of known therapeutic value in lower respiratory tract infections, in a large population who suffered AECB with a high likelihood of bacterial aetiology.
Methods
This was a randomized, prospective, open, parallel group, multinational comparative study carried out at 50 centres in four countries: France, Germany, Spain and the U.K. Independent ethics committees approved the study and patients gave written informed consent before participation in the study.
PATIENTS
Patients were randomized to treatment between 28 April 1995 and 7 May 1997. Patients were screened by their physician for eligibility to enter the study. In order to be eligible, they had to be diagnosed with chronic bronchitis, defined as a chronic cough productive of sputum for 3 consecutive months in 2 consecutive years, with an acute exacerbation indicated by the production of purulentl mucopurulent sputum and at least one of the following signs: increasing dyspnoea and/or increasing sputum vol- ume. Chest X-rays were performed on all randomized patients pre-treatment.
Patients were excluded from study participation because of known allergy to the study antibiotics, pregnancy and lactation, significant renal or hepatic impairment, concomi- tant serious illness, recent antibiotic therapy and recent participation in another clinical trial.
ANTIBIOTIC THERAPY
Patients were randomized to receive either ciprofloxacin suspension as a 10% solution (equivalent to 500 mg) bid for 7 days or oral co-amoxiclav 625 tablets (500 mg amoxicillin, 125 mg clavulanate) tid for 7 days. Medications were allowed to be taken either before or after meals. The study drugs were administered in an open, non-blind fashion.
CLINICAL AND BACTERIOLOGICAL EVALUATIONS
Patients were assessed pre-therapy (day 0), at the end of treatment (day 7) and 7 days after treatment had ended (day 14). They were contacted at monthly intervals there- after for 6 months. The investigators could withdraw patients from the study at any time if adverse events occurred or if the study drug was judged to be ineffective.
Clinical assessments were based on reduced cough, improvement in dyspnoea, reduction in 24-h sputum vol- ume or reduced purulence of sputum, all of which were graded according to predefined scales.
Sputum samples for culture were collected before treat- ment, on days 7 and 14, when available at the end of therapy, and if treatment failure occurred. The number of samples obtained at each time point was as follows: 327 at visit l/day 0 (165 ciprofloxacin and 162 co-amoxiclav), 293 at visit 2/day 7 (147 ciprofloxacin and 146 co-amoxiclav), and 241 at visit 3/day 14 (113 ciprofloxacin and 128 co-amoxiclav). At first exacerbation, a total of 82 sputum samples was collected (44 ciprofloxacin and 38 co-amoxiclav). The quality of sputum was assessed accord- ing to published recommendations (20). Recent data suggest that only sputum samples with 225 polymorpho- nuclear granulocytes (PMNs) per x 100 microscopic field should be included to increase the likelihood that cultured organisms were indeed ‘causative’ of AECB (21). However, review of the samples showed that there was no difference in the growth patterns of organisms between samples with PMN 225 per x 100 field and samples with ~25 PMN per x 100 field. Therefore, all samples were analysed as one
population. Assessments were also made of clinical signs and symp-
toms (wheeze, malaise, dyspnoea, cough and exercise intolerance).
The clinical response at day 14, 7 days after termination of antibiotic therapy, was the primary efficacy variable and was assessed as: (i) cure (resolution of signs and symptoms), (ii) improvement (subjective improvement of symptoms), (iii) failure (no resolution of signs and symptoms), (iv) relapse (at day 14 only, an initial resolution of signs and symptoms during study drug administration but subsequent worsening of signs and symptoms) or (v) indeterminate (not evaluable). Clinical success was defined as cure or improvement at days 7 and 14. Patients who did not have clinical improvement, or whose condition worsened by day 7, were deemed treatment failures. Secondary assessments were clinical response at day 7, and time to subsequent exacerbation in patients considered clinically cured at day 14.

254 R. c. REA!~ ET AL.
TABLE 1. Reasons for withdrawal during treatment
Reason for withdrawal
Ciprofloxacin 500 mg twice daily
(n= 185)
Patients (n (%)
Co-amoxiclav 625 mg three times daily
(n= 179) Overall (n=364)
Adverse event 2 (1) 1 (0.5) 3 (1) Consent withdrawn 1 (0.5) 0 1 (0.25) Lost to follow-up 0 2 (1) 2 (0.5) Non-compliance 1 (0.5) 0 1 (0.25)
Total 4 (2) 3 (2) 7 (2)
Minimum inhibitory concentrations (MICs) of anti- biotics for the isolated organisms were determined using E-test strips (AB Biodisk, Sweden).
SAFETY EVALUATIONS
Blood and urine samples were collected before treatment and at the end of treatment (day 7) for clinical chem- istry, haematology and urinalysis. Adverse events were coded using COSTART terms and were assessed for frequency, duration, severity, outcome and relationship to study drug.
STATISTICAL ANALYSIS
It was calculated that 332 valid patients would be needed for a power to show equivalence of 80% where the true difference between treatments was 0%, and for a signiti- cance level of 5% where the true difference between treat- ments was 10%. It was anticipated that 440 patients would need to have been recruited to obtain 332 valid patients. However, interim analysis showed that fewer patients were needed and recruitment was prematurely terminated after 364 patients had been entered. From these 364 patients, 327 valid patients were obtained, which was sufficient to main- tain the power of the study and allow the primary objective of the study to be met.
The clinical response at days 14 (primary assessment) and 7 (secondary assessment) was analysed using 95% confidence intervals (CI) from the exact test for the com- mon odds ratio, after homogeneity of the odds ratio between treatment centres had been assessed using the Zelen test. The bacteriological response was analysed in the same way.
The time to the next exacerbation was analysed using the Kaplan-Meier estimate of freedom from signs and symp- toms. Equivalence of exacerbation-free profiles between ciprofloxacin and co-amoxiclav treatments was assessed using the log-rank, Breslow and Tarone-Ware tests: The 95% confidence intervals of the treatment differences were calculated for each analysis.
Results
A total of 364 patients was randomized to treatment, of whom 185 (510/) were randomized to receive ciprofloxacin and 179 (49%) to receive co-amoxiclav. All but one of the patients were included in the safety analyses; this patient did not receive study medication. A further 36 patients were excluded from the valid for efficacy population and thus, 327 (90%) patients were considered evaluable for efficacy (165 ciprofloxacin and 162 co-amoxiclav). A total of seven patients withdrew during the 7-day treatment period, three of whom were withdrawn due to adverse events (Table 1). The demographic characteristics of the two treatment groups valid for efficacy were very similar (Table 2). Over 66% of patients in both treatment groups were either current or previously active smokers. Many patients received concomitant medication, the most frequently used being (percentage of patients): salbutamol (29%) beclom- ethasone (22%), theophylline (15%), prednisolone (14%) and ipratropium (10%). A total of 103/327 (31%) patients had valid bacteriological data at day 7 and 1021327 (31%) were considered bacteriologically evaluable at day 14, i.e. their bacteriological evaluation was not either ‘missing’ or ‘indeterminate’, and they had provided a bacteriologically positive pretreatment sputum sample.
CLINICAL RESPONSE
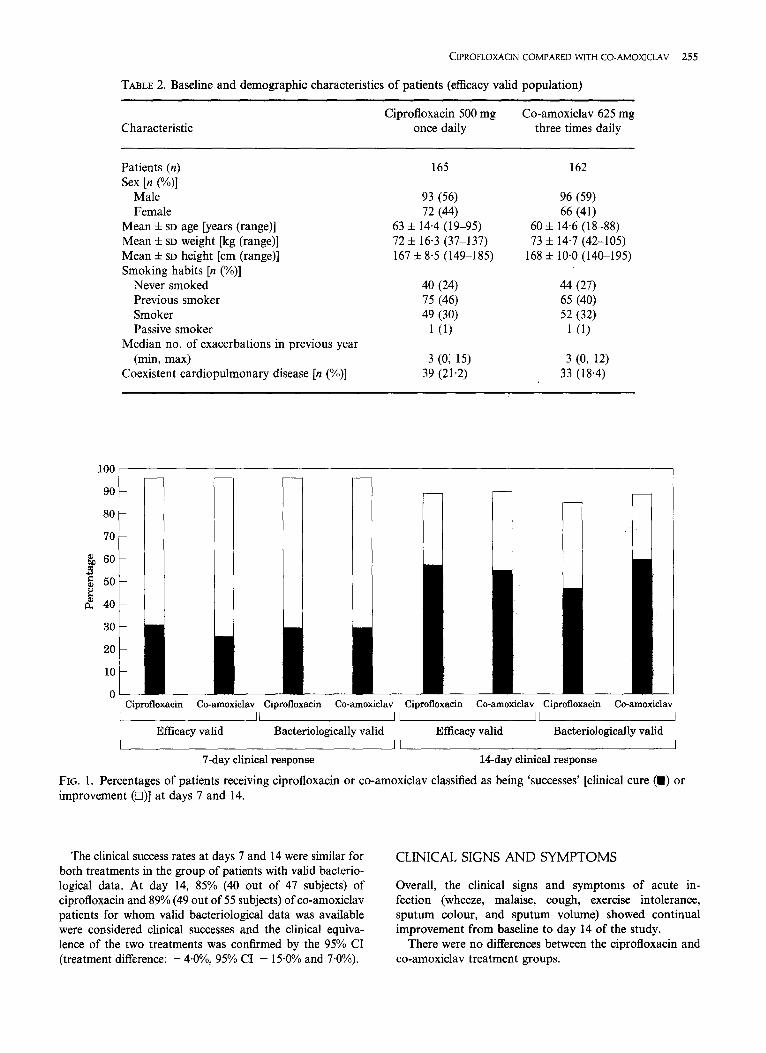
The clinical response of patients at day 7 (end of treatment) and day 14 is summarized in Fig. 1. At day 7, of the 327 clinically evaluable patients, 96% of both ciprofloxacin- (159 of 165 subjects) and co-amoxiclav-treated (156 of 162 subjects) patients were considered clinical successes (cured or improved). The clinical equivalence of the two treat- ments was confirmed by the 95% CI (treatment difference: O*l%, 95% CI - 3.4% and 3.5%). This clinical success rate was maintained to day 14, 7 days after termination of treatment: 89% (147 of 165 subjects) of ciprofloxacin and 90% (146 of 162 subjects) of co-amoxiclav-treated patients were still considered clinical successes. The clinical equiva- lence of the two treatments was again confirmed by the 95% CI (treatment difference: - l.O%, 95% CI - 6.6% and 4.5%). 1- L
CIPROFLOXACIN COMPARED WITH CO-AMOXICLAV 255
TABLE 2. Baseline and demographic characteristics of patients (efficacy valid population)
Characteristic Ciprofloxacin 500 mg Co-amoxiclav 625 mg
once daily three times daily
Patients (n) Sex [n (“/)I
Male Female
Mean f SD age [years (range)] Mean & SD weight [kg (range)] Mean f SD height [cm (range)] Smoking habits [n (%)I
Never smoked Previous smoker Smoker Passive smoker
Median no. of exacerbations in previous year (min, max)
Coexistent cardiopulmonary disease [n (%)]
165
93 (56) 72 (44)
63 f 14.4 (19-95) 72 h 16.3 (37-137) 167 f 8.5 (1499185)
40 (24) 75 (46) 49 (30)
1 (1)
3 (0; 15) 39 (21.2)
162
96 (59) 66 (41)
60 f 14.6 (18-88) 73 f 14.7 (42-105)
168 f 10.0 (140-195)
44 (27) 65 (40) 52 (32).
1 (1)
3 a 12) 33 (18.4) ,.
80
Q 60 B !j 50 z
d 40
1
Ciprofloxacin Co-amoxiclav Ciprofloxacin Co-amoxiclav Ciprofloxacin Co-amoxiclav Ciprofloxacin Co-amoxiclav -w-i
Efficacy valid Bacteriologically valid Efficacy valid Bacteriologically valid I I I I
7-day clinical response 14-day clinical response
FIG. 1. Percentages of patients receiving ciprofloxacin or co-amoxiclav classified as being ‘successes’ [clinical cure (H) or improvement (O)] at days 7 and 14.
The clinical success rates at days 7 and 14 were similar for both treatments in the group of patients with valid bacterio- logical data. At day 14, 85% (40 out of 47 subjects) of ciprofloxacin and 89% (49 out of 55 subjects) of co-amoxiclav patients for whom valid bacteriological data was available were considered clinical successes and the clinical equiva- lence of the two treatments was confirmed by the 95% CI (treatment difference: - 4*0%, 95% CI - 15.0% and 7.0%).
CLINICAL SIGNS AND SYMPTOMS
Overall, the clinical signs and symptoms of acute in- fection (wheeze, malaise, cough, exercise intolerance, sputum colour, and sputum volume) showed continual improvement from baseline to day 14 of the study.
There were no differences between the ciprofloxacin and co-amoxiclav treatment groups.

256 R. c. %W ET AL.
TABLE 3. Bacteriological response at days 7 and 14 in patients with valid bacteriological data
, Ciprofloxacin 500 mg Co-amoxiclav 625 mg Day and response once daily three times daily
Day 7 succ4?ss [n (%)]
Eradication Presumed eradication Eradication/colonization
Failure [n (%)] Persistence Persistence/colonization Recurrence Eradicationlre-infection Indeterminate
’ Day 14 success [n (“!)I
Eradication Presumed eradication Eradication/colonization
Failure [n (%)] Persistence Persistence/colonization Recurrence Eradicationlre-infection Indeterminate
40 (85) 46 (84) 30 (63) 32 (58) 4 (8) 6 (11) 6 (13) 8 (15) 7 (15) 9 (16) 7 (15) 7 (12) 0 1 (2) 0 0 0 1 (2) 1 (2) 0
40 (87) 46 (84) 14 (30) 15 (28) 2 (4) 4 (7)
24 (51) 27 (49) 6 (13) 9 (16) 5 (11) 3 (5) 0 l(2) 0 2 (4) 1 (2) 3 (5) 1, (2) 0
Before the start of treatment, 128 organisms were found in 103 patients. The bacteriological response shown in this table is based on these patients.
BACTERIQLOGICAL RESPONSE BY PATIENT
At day 7, the bacteriological success ‘rates (eradication, presumed eradication, or eradication with colonization) for bacteriologically evaluable patients was 85% (40 of 47 subjects) for patients treated with ciprofloxacin and 84% (46 of 55 subjects) for patients treated with co-amoxiclav. Treatment equivalence was confirmed (treatment difference: 1.5%, 95% CI - 10.4% and 13.3%). Similar bacteriological success rates at day 14 were also observed for patients treated with ciprofloxacin (40 of 46 patients; 87%) or co-amoxiclav (46 of 55 patients; 84%). Equivalence of the treatments was again confirmed by the 95% CI (treatment difference: 3.3%, 95% CI - 8.3% and 14.9%). Results are shown in Table 3.
BACTERIOLOGICAL RESPONSE FOR INDIVIDUAL PATHOGENS
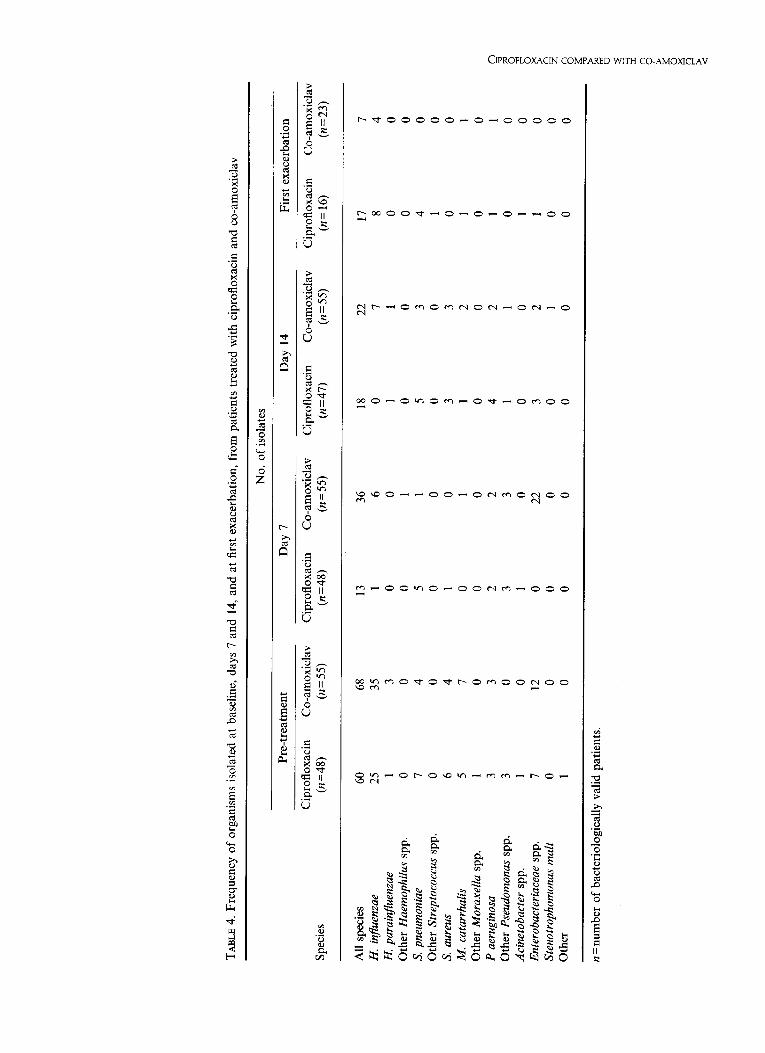
At baseline, 128 organisms were isolated from 103 patients (31%): 60 from the ciprofloxacin group and 68 from the co-amoxiclav group. The frequency of isolation of indi- vidual micro-organisms at baseline, day 7, day 14 and fist exacerbation is shown in Table 4. Ciprofloxacin had a higher bacteriological success rate than co-amoxiclav for H. injuenzae, the most frequently isolated organism (601128, 47%).
The number of S. pneumoniue isolates was low (combined 1 l/128, 9%; ciprofloxacin 7/60, 11.7%; co-amoxiclav 4/68, 5.9%); hence, it was difficult to compare the anti- pneumococcal bacteriological efficacy of the two treatment groups. The bacteriological efficacy for other organisms isolated was generally similar between the ciprofloxacin and co-amoxiclav treatment groups. There was a difference for the Enterobacteriaceae, where the isolation rates were simi- lar at baseline, but by day 7 all 22 isolates were from the co-amoxiclav treatment group, suggesting superinfection by members of this group. The presence of micro-organisms in sputum correlated poorly with treatment failure. A total of 49 organisms were isolated at day 7 and 40 at day 14, but only five patients with organisms at day 7 and 11 with organisms at day 14 were considered clinical failures.
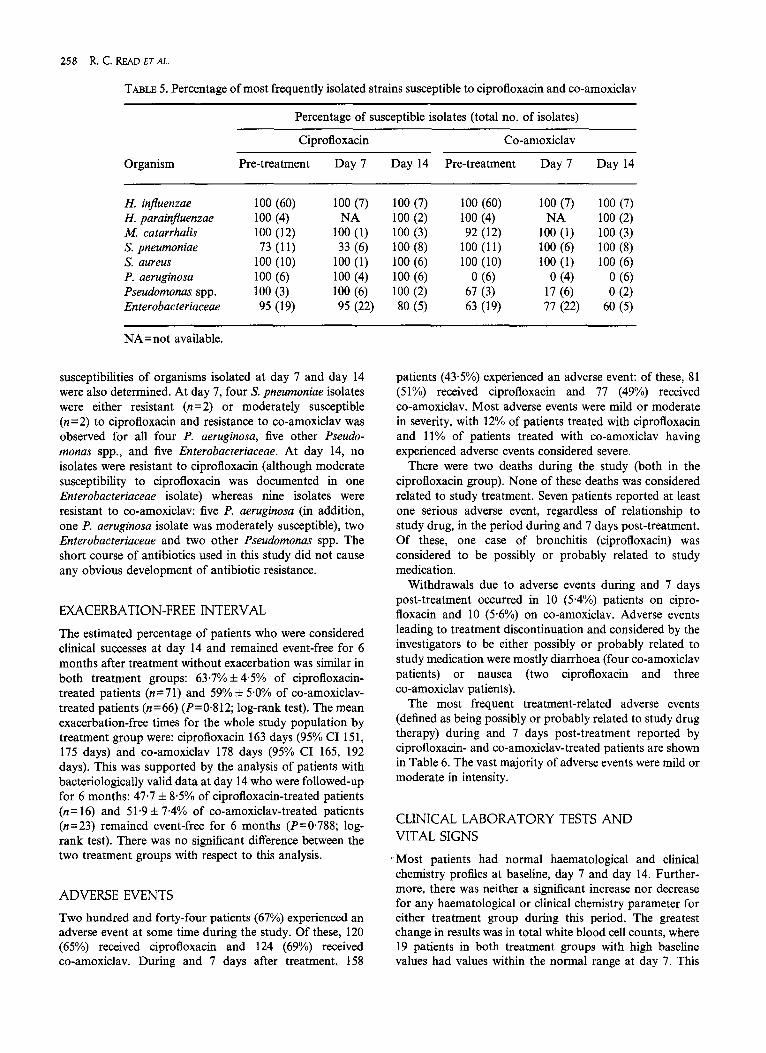
All isolates of H. influenzae and H. parainjluenzae were susceptible to both study drugs (Table 5). Of the 11 pneumococci isolated, all were susceptible to co-amoxiclav and eight were fully (MIC 2 1 mg 1 - ‘), and three moder- ately (MIC ~1 to <4), susceptible to ciprofloxacin. All of the organisms isolated at baseline were susceptible or moderately susceptible to ciprofloxacin except the Entero- bacteriuceue, where 5% of organisms were resistant. Of the organisms isolated from all patients, resistance rates against co-amoxiclav were 100% for P. aeruginosa, 33% for other Pseudomonas spp. and 16% for the Enterobacteriaceae (21% of the latter showed moderate susceptibility). The antibiotic
TABL
E 4.
Fre
quen
cy o
f or
gani
sms
isol
ated
at
base
line,
day
s 7
and
14, a
nd a
t fir
st e
xace
rbat
ion,
fro
m p
atie
nts
treat
ed w
ith c
ipro
floxa
cin
and
co-a
mox
icla
v
No.
of
isol
ates
Spec
ies
Pre-
treat
men
t D
ay 7
Cip
roflo
xaci
n C
o-am
oxic
lav
Cip
roflo
xaci
n C
o-am
oxic
lav
(n=4
8)
(n=5
5)
(n=4
8)
(n=5
5)
Day
14
Cip
roflo
xaci
n C
o-am
oxic
lav
(n=4
7)
(n=5
5)
Firs
t ex
acer
batio
n
Cip
roflo
xaci
n C
o-am
oxic
lav
(n=
16)
(n=2
3)
All
spec
ies
60
68
13
36
18
22
17
H. i
nfue
nzae
25
35
1
6 0
7 8
H. p
arain
fluen
zae
1 3
0 0
1 1
0 O
ther
Hae
mop
hilus
sp
p.
0 0
0 1
0 0
0 S.
pne
umon
iae
7 4
5 1
5 3
4 O
ther
Stre
ptoc
occu
s sp
p.
0 0
0 0
0 0
1 S.
aur
eus
6 4
1 0
3 3
0 M
. ca
tarrh
alis
5 7
0 1
1 2
1 O
ther
Mor
axell
a sp
p.
1 0
0 0
0 0
0 P
aeru
ginos
a 3
3 2
2 4
2 1
Oth
er P
seud
omon
as
spp.
3
0 3
3 1
1 0
Acin
etob
acte
r sp
p.
1 0
1 0
0 0
1 En
tero
bacte
riace
ae
spp.
7
12
0 22
3
2 1
Sten
otro
phom
onas
m
alt
0 0
0 0
0 1
0 O
ther
1
0 0
0 0
0 0
7 4 0 0 0 0 0 1 0 1 0 0 0 0 0
n = n
umbe
r of
bac
terio
logi
cally
val
id p
atie
nts.
258 R. c. READ ET AL.
TABLE 5. Percentage of most frequently isolated strains susceptible to ciprofloxacin and co-amoxiclav
Organism
Percentage of susceptible isolates (total no. of isolates)
Ciprofloxacin Co-amoxiclav
Pre-treatment Day 7 Day 14 Pre-treatment Day 7 Day 14
H. infuenzae 100 (60) 100 (7) 100 (7) 100 (60) 100 (7) 100 (7) H. parainfZuenzae 100 (4) 100 (2) 100 (4) NA 100 (2) M. catarrhalis 100 (12)
lOZ1) 100 (3) 92 (12) 100 (1) 100 (3)
S. pneumoniae 73 (11) 33 (6) 100 (8) 100 (11) 100 (6) 100 (8) S. aureus 100 (10) 100 (1) 100 (6) 100 (10) 100 (1) 100 (6) P. aeruginosa 100 (6) 100 (4) 100 (6) 0 (6) 0 (4) 0 (6) Pseudomonas spp. 100 (3) 100 (6) 100 (2) 67 (3) 17 (6) 0 (2) Enterobacteriaceae 95 (19) 95 (22) 80 (5) 63 (19) 77 (22) 60 (5)
NA = not available.
susceptibilities of organisms isolated at day 7 and day 14 were also determined. At day 7, four S. pneumoniae isolates were either resistant (n=2) or moderately susceptible (n=2) to ciprofloxacin and resistance to co-amoxiclav was observed for all four P. aeruginosa, five other Pseudo- monas spp., and five Enterobacteriaceae. At day 14, no isolates were resistant to ciprofloxacin (although moderate susceptibility to ciprofloxacin was documented in one Enterobacteriaceae isolate) whereas nine isolates were resistant to co-amoxiclav: five P. aeruginosa (in addition, one P. aeruginosa isolate was moderately susceptible), two Enterobacteriaceae and two other Pseudomonas spp. The short course of antibiotics used in this study did not cause any obvious development of antibiotic resistance.
EXACERBATION-FREE INTERVAL
The estimated percentage of patients who were considered clinical successes at day 14 and remained event-free for 6 months after treatment without exacerbation was similar in both treatment groups: 63.7% f 4.5% of ciprofloxacin- treated patients (n=71) and 59% f 5.0% of co-amoxiclav- treated patients (n=66) (P=O*812; log-rank test). The mean exacerbation-free times for the whole study population by treatment group were: ciprofloxacin 163 days (95% CI 15 1, 175 days) and co-amoxiclav 178 days (95% CI 165, 192 days). This was supported by the analysis of patients with bacteriologically valid data at day 14 who were followed-up for 6 months: 47.7 f 8.5% of ciprofloxacin-treated patients (n= 16) and 51.9 f 7.4% of co-amoxiclav-treated patients (n=23) remained event-free for 6 months (P=O.788; log- rank test). There was no significant difference between the two treatment groups with respect to this analysis.
ADVERSE EVENTS
Two hundred and forty-four patients (67%) experienced an adverse event at some time during the study. Of these, 120 (65%) received ciprofloxacin and 124 (69%) received co-amoxiclav. During and 7 days after treatment, 158
patients (43.5%) experienced an adverse event: of these, 81 (510/) received ciprofloxacin and 77 (49%) received co-amoxiclav. Most adverse events were mild or moderate in severity, with 12% of patients treated with ciprofloxacin and 11% of patients treated with co-amoxiclav having experienced adverse events considered severe.
There were two deaths during the study (both in the ciprofloxacin group). None of these deaths was considered related to study treatment. Seven patients reported at least one serious adverse event, regardless of relationship to study drug, in the period during and 7 days post-treatment. Of these, one case of bronchitis (ciprofloxacin) was considered to be possibly or probably related to study medication.
Withdrawals due to adverse events during and 7 days post-treatment occurred in 10 (5.4%) patients on cipro- floxacin and 10 (5.6%) on co-amoxiclav. Adverse events leading to treatment discontinuation and considered by the investigators to be either possibly or probably related to study medication were mostly diarrhoea (four co-amoxiclav patients) or nausea (two ciprofloxacin and three co-amoxiclav patients).
The most frequent treatment-related adverse events (defined as being possibly or probably related to study drug therapy) during and 7 days post-treatment reported by ciprofloxacin- and co-amoxiclav-treated patients are shown in Table 6. The vast majority of adverse events were mild or moderate in intensity.
CLINICAL LABORATORY TESTS AND VITAL SIGNS
Most patients had normal haematological and clinical chemistry profiles at baseline, day 7 and day 14. Further- more, there was neither a significant increase nor decrease for any haematological or clinical chemistry parameter for either treatment group during this period. The greatest change in results was in total white blood cell counts, where 19 patients in both treatment groups with high baseline values had values within the normal range at day 7. This

CIPROFLOXACIN COMPARED WITH CO-AMOXICLAV 259
TABLE 6. Most frequent (occurring in at least 2% of study population) adverse events possibly or probably related to ciprofloxacin or co-amoxiclav treatment during and 7 days post-treatment
Adverse events during and 7 days post-treatment
Adverse event Ciprofloxacin Co-amoxiclav
(n= 184) (n= 179)
Nausea 24 (13.0%) 19 (10.6%) Flatulence 19 (10.3%) 7 (3.9%) Abdominal pain 14 (7.6%) 13 (7.3%) Diarrhoea 8 (4.3%) 12 (6.7%) Vomiting 9 (4.9%) 9 (50%) Dyspepsia 7 (3.8%) 3 (1.7%)
shift was expected, and confirms the total white blood cell count as a good indicator of acute infection.
No clinically relevant changes occurred in systolic and diastolic blood pressure or heart rate from baseline to day 14.
Discussion
Ciprofloxacin oral suspension has been developed to improve ease of antibiotic administration for those patients who find swallowing difficult, for example the elderly, and those with anatomical or dysfunctional swallowing prob- lems. Some patients who do not have such difficulties also prefer liquid medications to tablets. Previous studies have shown that this oral formulation has similar pharmaco- kinetics to the ciprofloxacin tablet (data on file, Bayer AG, Wuppertal, Germany), and that food has no significant effect on its absorption (data on file, Bayer AG, Wuppertal, Germany). This study was performed to assess the efficacy and safety of ciprofloxacin oral suspension compared with co-amoxiclav, a /?-lactam antibiotic considered as ‘gold standard’ in the treatment of AECB (22-31).
The results of this study showed that a 7-day course of ciprofloxacin 500 mg oral suspension given twice daily was clinically equivalent to co-amoxiclav 625 mg tablets admin- istered three times daily. Both antibiotics produced high clinical success rates (96% for both drugs) at the end of treatment. This was maintained at 7 days post-treatment (day 14), with 89% of ciprofloxacin and 90% of co-amoxiclav patients still considered clinical successes. These findings are in agreement with previously reported clinical response rates between 80% and 95% for the treatment of AECB with ciprofloxacin (32-34).
The organism most frequently isolated before treatment was H. infuenzae and the ciprofloxacin suspension was more effective than co-amoxiclav in eradicating this species. The numbers of H. infruenzae isolated in the ciprofloxacin group were 25 at pre-treatment, 1 at day 7 and 0 at day 14. The respective figures for co-amoxiclav were 35, 6 and 7. A
comparatively high number of H. influenzae were isolated from patients in the co-amoxiclav treatment group, although all of these isolates were susceptible to co-amoxiclav at all visits when tested using the E-test for antibiotic susceptibility. However, results for the MIC and minimum bactericidal concentration (MBC) of an anti- biotic represent the net antibiotic effect over a fixed incubation period, and notable discrepancies between the bacteriological response - assessed by in vitro susceptibility testing-and the clinical response are common. Thus, in order to determine whether or not an organism is susceptible to an antibiotic, one needs to understand the pharmacokinetics of the drug (35).
A number of pharmacokinetic surrogate relationships have been used to try to predict the outcome of antibiotic treatment (36), and the best predictor for /3-lactams, macrolides and /3-lactamlclavam combinations - such as co-amoxiclav- was the time that the plasma antibiotic concentration remained above the MIC for a particular organism (T>MIC) (37,38). In the case of co-amoxiclav, T>MIC,, for H. injluenzae was about 40% of the time for each dosage interval when the antibiotic was administered at a dose of either 875 mg bid or 500 mg tid (39). It has been shown that to approach maximum bacterial killing, cepha- losporin T>MIC needs to be for 60-70% of the dose period (40-43) whereas a bacteriostatic effect occurred when T>MIC was 40% of the dose period. Perhaps this could explain the persistence of H. ir$uenzae isolates in the co-amoxiclav treatment arm in this study. Conversely, ciprofloxacin - like other fluoroquinolones - exhibits concentration-dependent killing of bacteria (44,45), which could explain the lack of persistence of H. influenzae in the ciprofloxacin treatment group.
Co-amoxiclav appeared to be more effective than cipro- floxacin in eradicating S. pneumoniae; however, the number of Streptococcus spp. isolated pre-treatment was small, making it difficult to compare the anti-pneumococcal bacteriological efficacy of the two treatment groups. The numbers of S. pneumoniae isolated in the ciprofloxacin group were seven at pre-treatment, five at day 7 and five at day 14. The corresponding figures for co-amoxiclav were four, one and three. In contrast, co-amoxiclav-treated patients appeared to be more susceptible to superinfection by Enterobacteriaceae following antibiotic treatment than were ciprofloxacin-treated patients. Pre-treatment isolation rates of the Enterobacteriaceae were seven (ciprofloxacin) and 12 (co-amoxiclav), but at day 7 all 22 cases of Entero- bacteriaceae isolated were in the co-amoxiclav group. At day 14, the isolation rates were three (ciprofloxacin) and two (co-amoxiclav).
No differences between ciprofloxacin and co-amoxiclav treatments were observed for time to next exacerbation. Thus, it would appear unlikely that short antibiotic treat- ment regimens can influence the course of a chronic disease that is associated with significant epithelial cell damage.
The frequency of adverse events in this study was as expected in this group of patients and comparable between the treatment groups. Most drug-related adverse events were gastrointestinal in nature, with no relevant qualitative differences between the two treatments.
260 R.C. READ ET AL
In conclusion, ciprofloxacin suspension was clinically equivalent to the widely used first-line treatment of co-amoxiclav tablets, and there were no differences between the safety profiles of the two antibiotics. Based on the results of this study, together with other published data, we would suggest that ciprofloxacin oral suspension offers an alternative treatment of choice for AECB patients, especially those who have difficulties in swallowing, or who prefer liquid medications to tablets.
Acknowledgement
This study was supported Bayer AG.
References
by an educational grant from
1.
2.
3.
4.
5.
6.
I.
8.
9.
10.
11.
Ball P. Epidemiology and treatment of chronic bron- chitis and its exacerbations. Chest 1995; 1OS: 43S-52s. Orr PH, Scherer K, Macdonald A, Moffatt ME. Randomized, placebo-controlled trials of antibiotics for acute bronchitis: a critical review of the literature. J Fam Pratt 1993; 36: 507-512. Johnson JA. Pathogenesis of bacterial infections of the respiratory tract. Br J Biomed Sci 1995; 52: 157-161. Mulder J, Goslings WRO, Vaan der Plas MC, Lopes Cardozo P. Studies on the treatment with antibacterial drugs of acute and chronic purulent bronchitis caused by Haemophilus injluenzae. Acta Med Stand 1952; 142: 3249. Baquero F, Loza E. Antibiotic resistance of micro- organisms involved in ear, nose and throat infections. Pediatr Infect Dis 1994; 18: S9-S14. Jorgensen JH, Doern GV, Maher LA, Howell AW, Redding JS. Antimicrobial resistance among respirat- ory isolates of Haemophilus injluenzae, Moraxella catarrhalis and Streptococcus pneumoniae in the United States. Antimicrob Agents Chemother 1990; 34: 2075- 2080. Kayser FH, Morenzoni G, Santanam P. The Second European Study on the frequency of antimicrobial resistance in Haemophilus injluenzae. Eur J Clin Microbial Infect Dis 1990; 9: 810-817. Kobayashi H, Takamure H, Takeda H et al. Compara- tive clinical study of ciprofloxacin and cefaclor in the treatment of respiratory tract infections. Chemother (Tokyo) 1986; 34: 101 l-1037. Chodosh S, Tuck J, Stottmeier KD, Pizzuto D. Com- parison of ciprofloxacin with ampicillin in acute infec- tious exacerbations of chronic bronchitis. Am J Med 1989; 87 (Suppl. 5A): 107-l 12. Schmidt EW, Zimmermann I, Ritzerfeld W, Voss E, Ulmer WT. Controlled prospective study of oral amoxycillinlclavulanate vs ciprofloxacin in acute exacerbations of chronic bronchitis. J Antimicrob Chemother 1989; 24 (Suppl. B): 185-193. Basran GS, Joseph J, Abbas AMA, Hughes C, Tillotoson G. Treatment of acute exacerbations of
12.
13.
14.
15
16.
17.
18.
19.
20.
21.
22.
23.
24.
chronic obstructive airways disease - a comparison of amoxycillin and ciprofloxacin. J Antimicrob Chemother 1990; 26 (Suppl. F): 19-24. Cazzola M, Vinciguerra A, Beghi GF et al. Compara- tive evaluation of the clinical and microbiological effi- cacy of co-amoxiclav vs cefixime or ciprofloxacin in bacterial exacerbation of chronic bronchitis. J Chem- other 1995; 7: 432-441. Chodosh S, Echols R, Kowalsky S, Painter B, Valalik E. A prospective, randomized, double-blind, compara- tive study of ciprofloxacin and cefuroxime axetil for the treatment of acute exacerbations of chronic bronchitis. Ann Meet Infect Dis Sot Am, 1995; Washington DC, USA. Al66 (Abstract). Chodosh S, Schreurs AJM, Shan M, Moesker HL, Kowalsky S, The Bronchitis Study Group. The efficacy of oral ciprofloxacin vs clarithromycin for the treat- ment of acute bacterial exacerbations of chronic bronchitis. Clin Infect Dis 1996; 23: 913. (Abstract). Anzueto A, Niederman MS, Haverstock DC, Tillotson G, The Bronchitis Study Group. Efficacy of cipro- floxacin and clarithromycin in acute bacterial exacer- bations of complicated chronic bronchitis: interim analysis. Clin Therapeut 1997; 19: 55-67. The Canadian Ciprofloxacin Health Economic Study Group, Grossman R, Mukherjee J et al. A l-year community-based health economic study of cipro- floxacin vs usual antibiotic treatment in acute ex- acerbations of chronic bronchitis. Chest 1998; 113: 131-141. Bergan T, Thorsteinsson SB, Solberg S, Bjornskau L, Kolstad IM, Johnsen S. Pharmacokinetics of cipro- floxacin: intravenous and increasing oral doses. Am J Med 1987; 82 (Suppl. 4A): 97-102. Bergogne-BCrCzin E. Pharmacokinetics of fluoro- quinolones in the respiratory tissues and fluids. Quin Bull 1993; lo: l-5. Hooper DC, Wolfson JS. Mechanisms of quinolone action and bacterial killing. In: Hooper DC, Wolfson JC, eds. Quinolone Antimicrobial Agents. Washington DC: American Society for Microbiology, 1993, 53-75. NCCLS. Performance standards for antimicrobial sus- ceptibility testing. Wayne, USA: National Committee for Clinical Laboratory Standards; 1990. Document MlOO-S6. Baquero F, Alvarez M-E, Canton R. Bacteriological diagnosis of respiratory tract infections. Clin Microbial Infect 1996; 1: SlO-S15. Aigner K, Schindl R, Mittermayer H. Augmentin in acute exacerbations of chronic bronchitis. J Int Med Res 1984; 12: 321-326. McGhie D, Kerfoot P, Talbot DJ. A comparative study of Miraxid (pivmecillinam plus pivampicillin) and Augmentin (amoxycillin plus clavulanic acid) in the treatment of lower respiratory tract infections in general practice. J Znt Med Res 1986; 14: 254-260. Maesen FP, Davies BI, Baur C. Amoxycillin/ clavulanate in acute purulent exacerbations of chronic bronchitis. J Antimicrob Chemother 1987; 19: 373-383.

CIPROFLOXACIN COMPARED WITH CO-AMOXICLAV 261
25. Periti P, Novelli A, Schildwachter G, Schmidt-Gayk H, Ryo Y, Zuck P. Efficacy and tolerance of cefpodoxime proxetil compared with co-amoxiclav in the treatment of exacerbations of chronic bronchitis. J Antimicrob Chemother 1990; 26 (Suppl. E): 63-69.
26. Rademaker CM, Sips AP, Beumer HM et al. A double-blind comparison of low-dose ofloxacin and amoxycillin/clavulanic acid in acute exacerbations of chronic bronchitis. J Antimicrob Chemother 1990; 26 (Suppl. D): 75-81.
27. Legnani D, Lombard0 VM, Negretto GG, Beghi G, Caratozzolo 0. Comparative clinical and micro- biological study of amoxycillin-clavulanic acid and ciprofloxacin in acute purulent exacerbations of chronic bronchitis. J Hosp Infect 1992; 22 (Suppl. A): 69-74.
28. Beghi G, Berni F, Carratu L et al. Efficacy and tolerability of azithromycin versus amoxicillin/ clavulanic acid in acute purulent exacerbations of chronic bronchitis. J Chemother 1995; 7: 146152.
29. Behler PG, Boge K, Bohning W, Gams W, Gartner- Toth M, Wettengel R. Amoxicillin/clavulanic acid vs cefetamet pivoxil in the treatment of acute exacerbation of chronic bronchitis (AECB) in adults. J Chemother 1995; 7 (Suppl. 1): 1620.
30. Aubier MA. Comparison of ceftibuten versus amoxicillinlclavulanate in the treatment of acute exacerbations of chronic bronchitis. Chemother 1997; 43: 297-302.
31. Hoepelman IM, Mollers MJ, van Schie MH et al. A short (3-day) course of azithromycin tablets versus a IO-day course of amoxycillin-clavulanic acid (co- amoxiclav) in the treatment of adults with lower respir- atory tract infections and effect on long-term outcome. Int J Antimicrob Agents 1997; 9: 141-146.
32. Ball AP. Evidence for the efficacy of ciprofloxacin in lower respiratory tract infections. Rev Contemp Pharmacother 1992; 3: 1333142.
33. Ball AP, Tillotson GS. Lower respiratory tract infec- tion therapy - the role of ciprofloxacin. J Int Med Res 1995; 23: 315-327.
34. Chodosh S, Lakshminarayan S, Swarz H, Breisch S. Efficacy and safety of a IO-day course of 400 or 600 milligrams of grepafloxacin once daily for treatment of acute bacterial exacerbations of chronic bronchitis:
comparison with a lo-day course of 500 milligrams of ciprofloxacin twice daily. Antimicrob Agents Chemother 1998; 42: 114120.
35. Cazzola M, Matera MG. Interrelationship between pharmacokinetics and pharmacodynamics in choosing the appropriate antibiotic and the dosage regimen for treating acute exacerbations of chronic bronchitis. Respir Med 1998; 92: 895-901.
36. Nix DE, Schentag JJ. Role of pharmacokinetics and pharmacodynamics in the design of dosage schedules for 12-h cefotaxime alone and in combination with other antibiotics. Diagn Microbial Infect Dis 1995; 22: 71-76.
37. Vogelman B, Craig WA. Kinetics of antimicrobial activity. J Pediatr 1986; 108: 8355840.
38. Craig WA, Ebert SC. Killing and regrowth of bacteria in vitro: a review. Stand J Infect Dis 1991; 74 (Suppl.): 63-70.
39. Drusano GL, Craig WA. Relevance of pharmaco- kinetics and pharmacodynamics in the selection of antibiotics for respiratory tract infections. J Chemother 1997; 9 (Suppl. 3): 3844.
40. Craig WA. Interrelationship between pharmacokinetics and pharmacodynamics in determining dosage regi- mens for broad-spectrum cephalosporins. Diugn Micro- biol Znfect Dis 1995; 22: 89-96.
41. Vogelman B, Gudmundsson S, Leggett J, Turnidge J, Ebert S, Craig WA. Correlation of antimicrobial phar- macokinetic parameters with therapeutic efficacy in an animal model. J Znfect Dis 1988; 157: 831-847.
42. Leggett JE, Fantin B, Ebert S et al. Comparative antibiotic dose-effect relations at several dosing inter- vals in murine pneumonitis and thigh-infection models. J Infect Dis 1989; 159: 281-292.
43. Craig WA. The pharmacokinetics of cefpirome: ration- ale for a twelve-hour dosing regimen. Stand J Infect Dis 1993; 91 (Suppl.): 3340.
44. Smith JT. Awakening the slumbering potential of the 4-quinolone antibacterials. Pharm J 1984; 233: 299-305.
45. Chin N, Neu HC. Ciprofloxacin, a quinolone carboxy- lit acid compound active against aerobic and anaerobic bacteria. Antimicrob Agents Chemother 1984; 25: 319- 326.