“the endoscopic advantage in transforaminal lumbar ... · “the endoscopic advantage in...
TRANSCRIPT

“The Endoscopic Advantage in Transforaminal Lumbar Interbody Fusion:
Facet Preservation and Visualized/Targeted Decompression and Endplate
Preparation”
James J. Yue, M.D.
Yale School of Medicine
Department of Orthopaedic Surgery
NASS 2016Solution ShowcaseBoston, MA

Disclosures
• Consultant: Wolf Spine, Aesculap Spine, Osseus Spine,
• Royalites: Aesculap Spine

Working Channel
Light Guide
Optics
Irrigation Channel
Full Endoscopic Surgery: Vertebris Scope (Wolf)
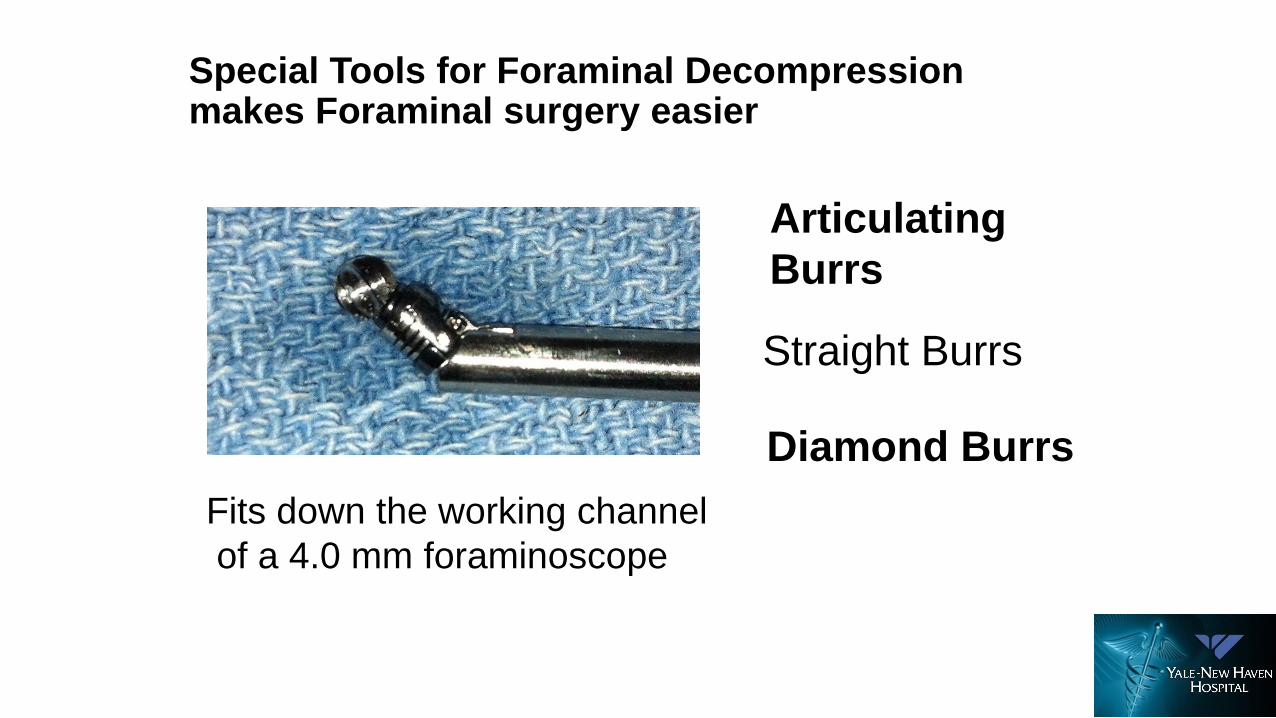
Special Tools for Foraminal Decompression makes Foraminal surgery easier
Articulating
Burrs
Diamond Burrs
Straight Burrs
Fits down the working channel
of a 4.0 mm foraminoscope
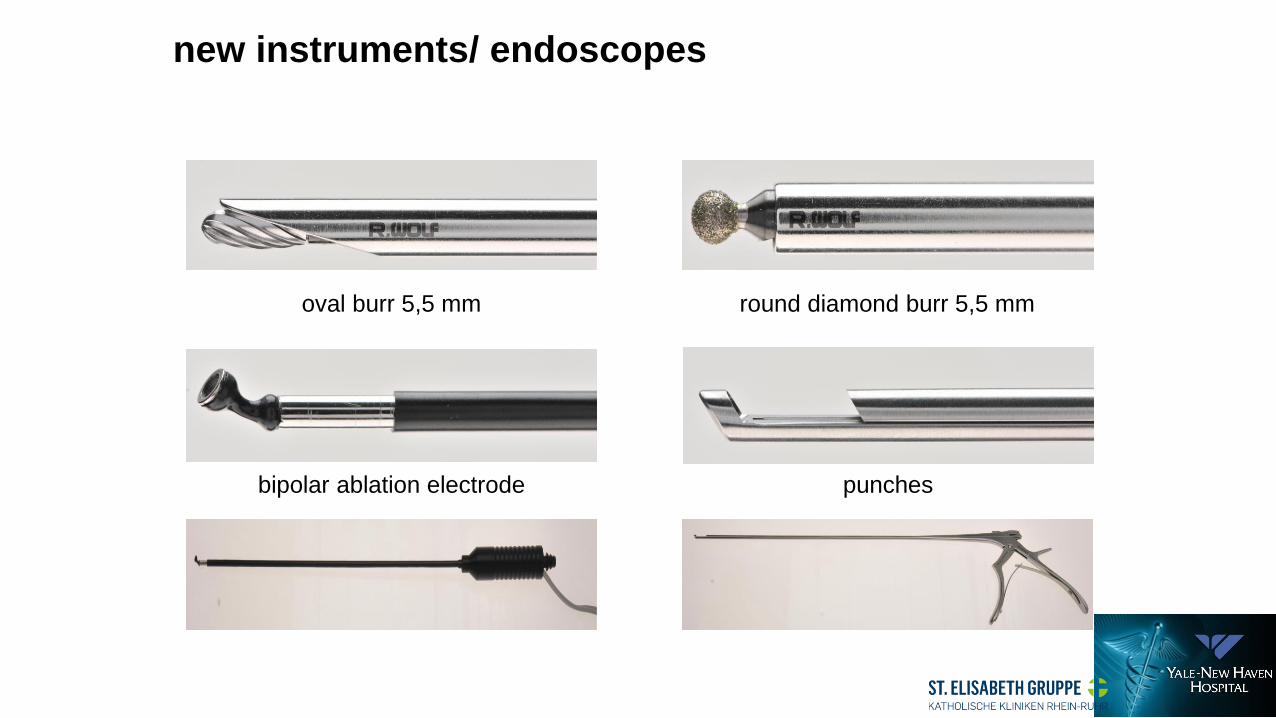
oval burr 5,5 mm round diamond burr 5,5 mm
bipolar ablation electrode punches
new instruments/ endoscopes
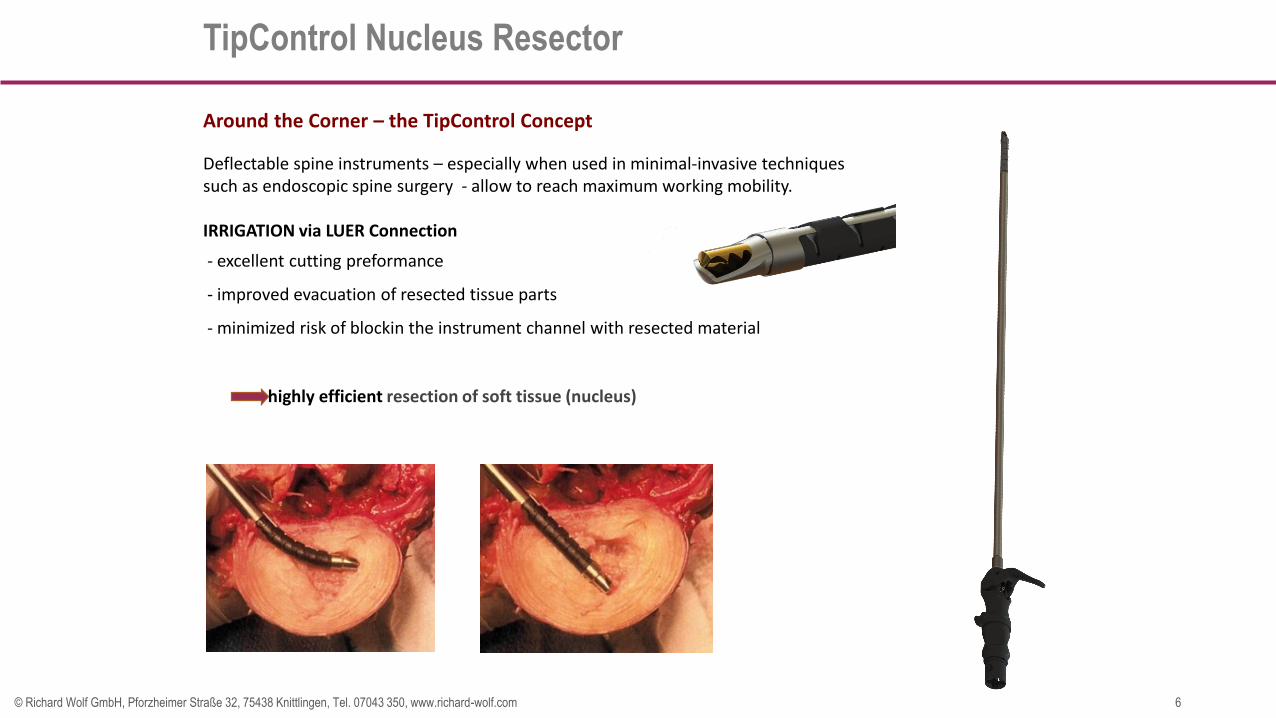
TipControl Nucleus Resector
6© Richard Wolf GmbH, Pforzheimer Straße 32, 75438 Knittlingen, Tel. 07043 350, www.richard-wolf.com
Around the Corner – the TipControl Concept
Deflectable spine instruments – especially when used in minimal-invasive techniquessuch as endoscopic spine surgery - allow to reach maximum working mobility.
IRRIGATION via LUER Connection
- excellent cutting preformance
- improved evacuation of resected tissue parts
- minimized risk of blockin the instrument channel with resected material
highly efficient resection of soft tissue (nucleus)
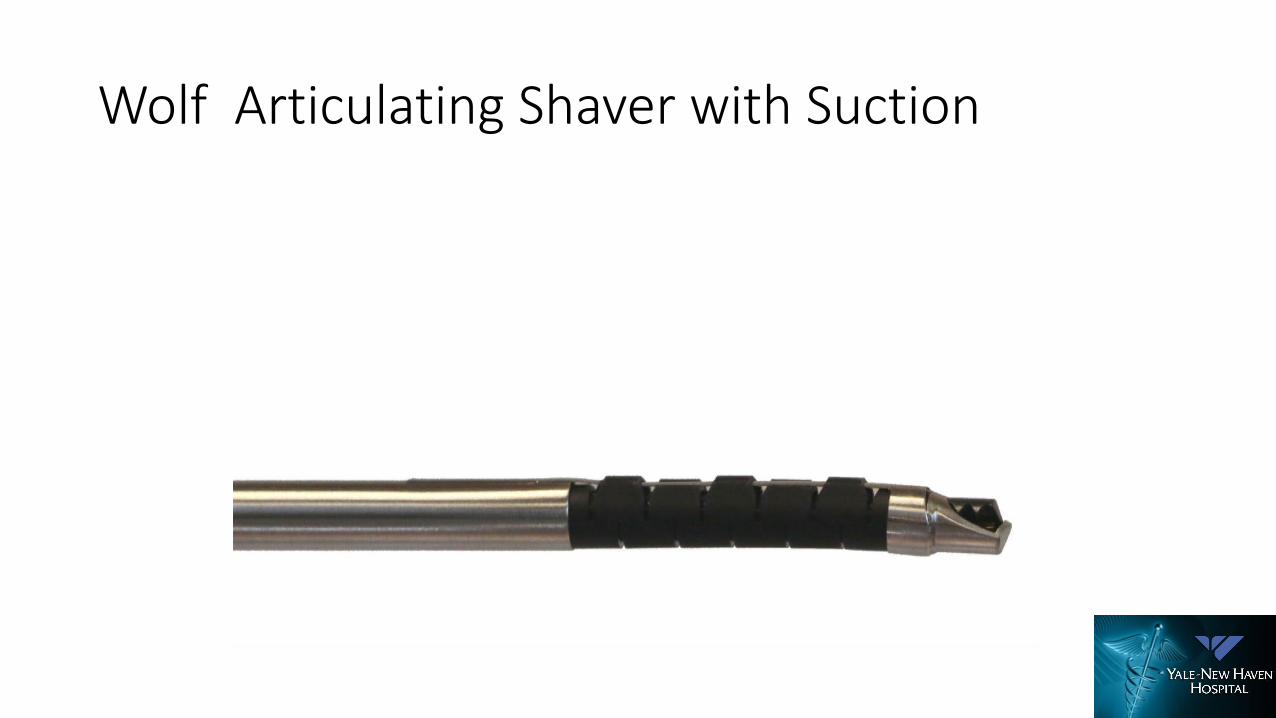
Wolf Articulating Shaver with Suction
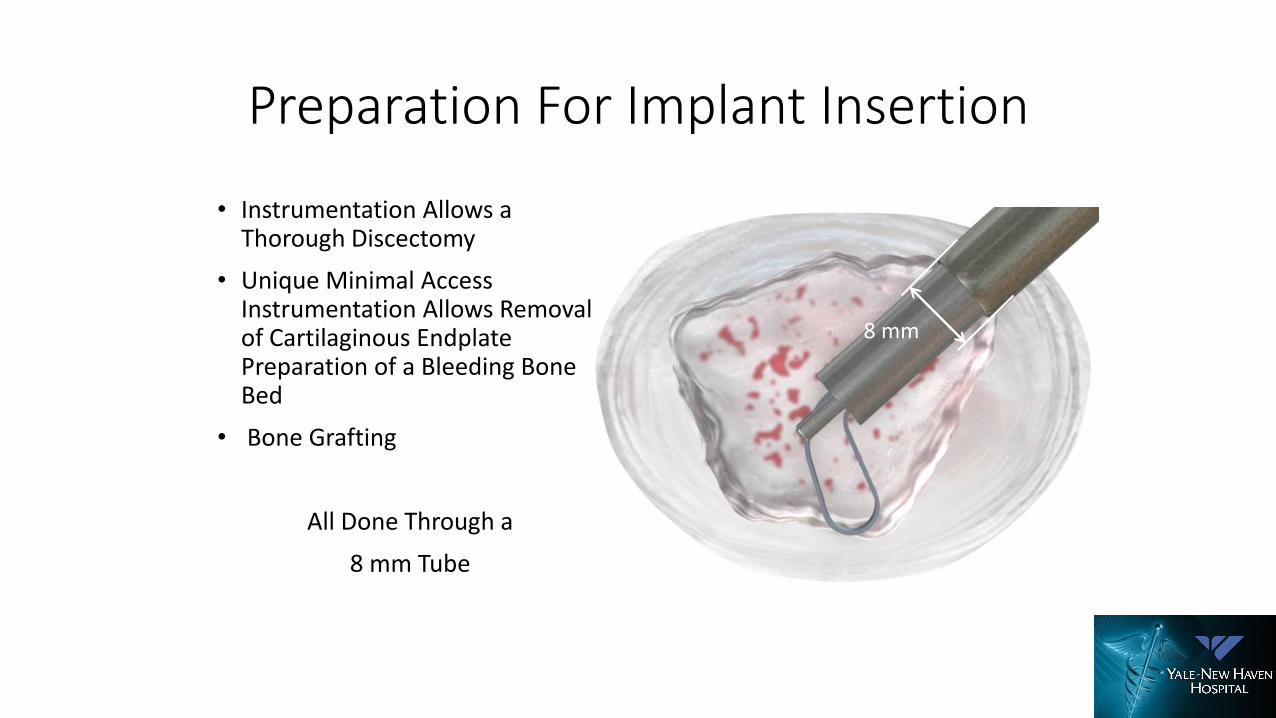
Preparation For Implant Insertion
• Instrumentation Allows a Thorough Discectomy
• Unique Minimal Access Instrumentation Allows Removal of Cartilaginous Endplate Preparation of a Bleeding Bone Bed
• Bone Grafting
All Done Through a
8 mm Tube
8 mm
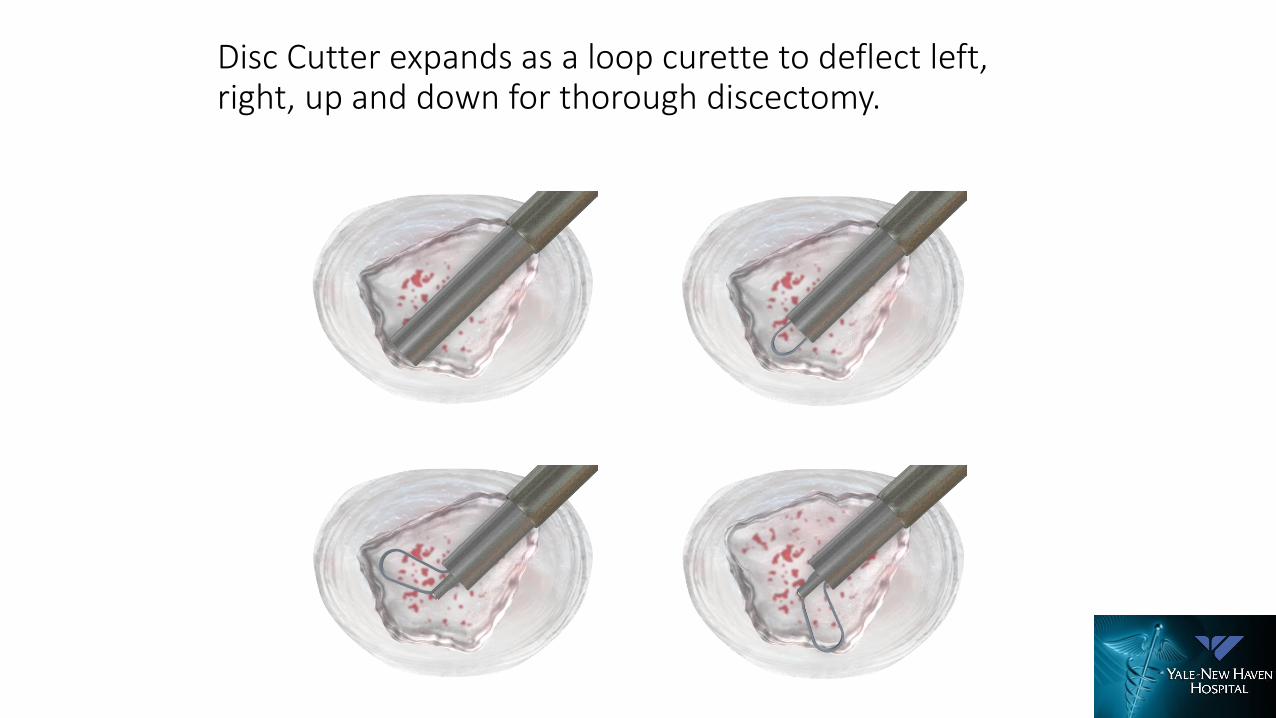
Disc Cutter expands as a loop curette to deflect left, right, up and down for thorough discectomy.
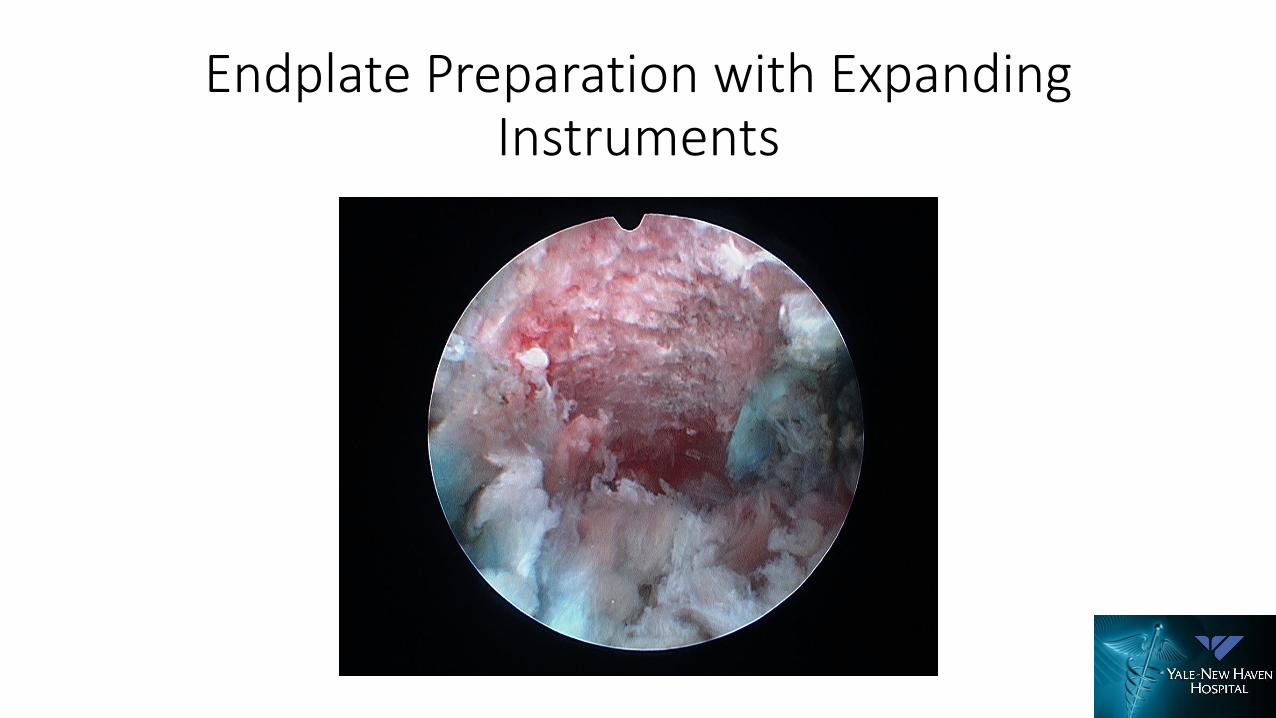
Endplate Preparation with Expanding Instruments

Special Tools for Foraminal Decompression
Laser & Catheter
Laser is very effective for resecting both soft tissue
and bony resection

ZEUS (AmendiaOLLIF)
Solid Bullet ImplantsExpandable implants
Rise Intra-LIF (Globus)
On Cage Joimax
Opti-Cage, Interventional Spine
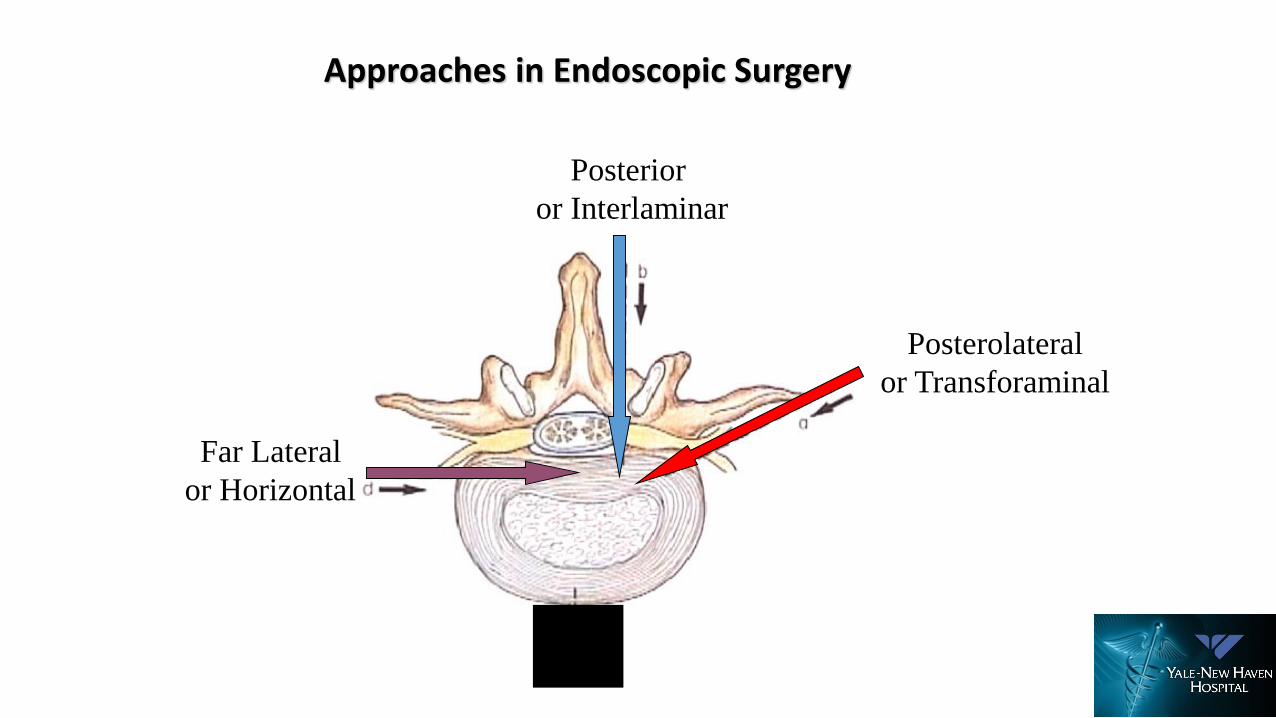
Posterior
or Interlaminar
Posterolateral
or Transforaminal
Far Lateral
or Horizontal
Approaches in Endoscopic Surgery

Target Oriented Endoscopic Surgery
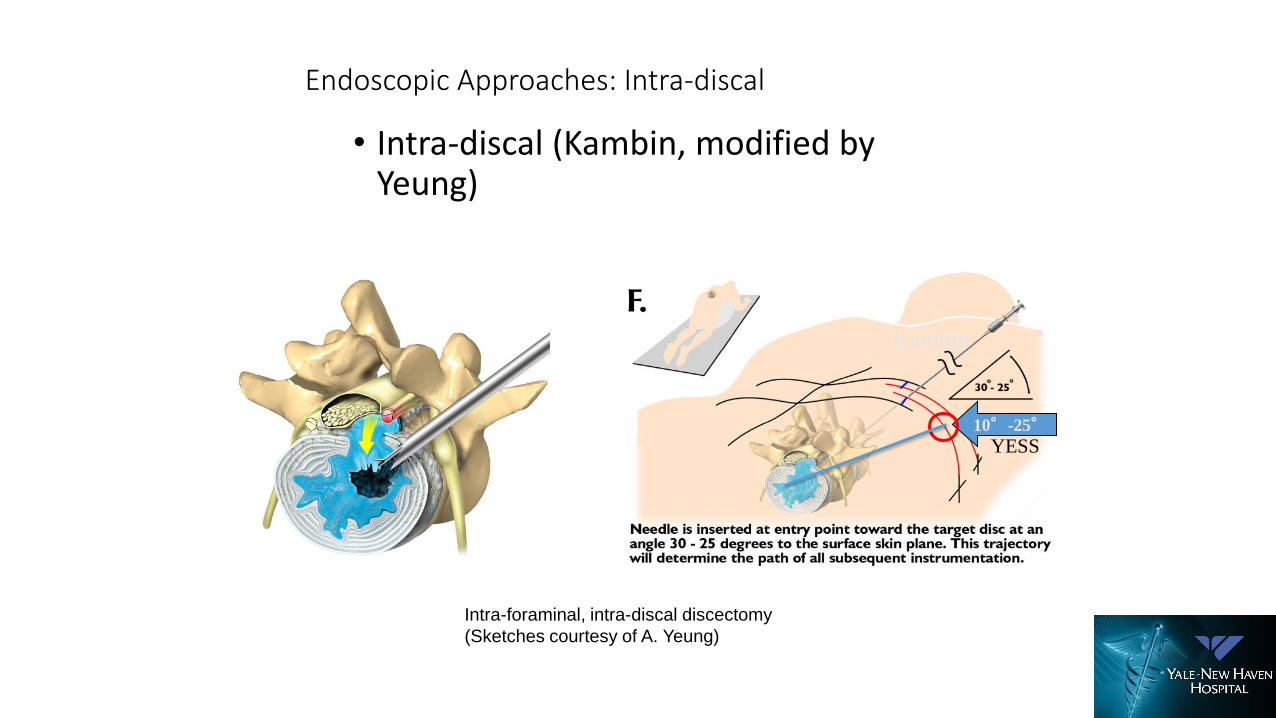
Endoscopic Approaches: Intra-discal
• Intra-discal (Kambin, modified by Yeung)
Intra-foraminal, intra-discal discectomy
(Sketches courtesy of A. Yeung)
10°-25°
Kambin
YESS
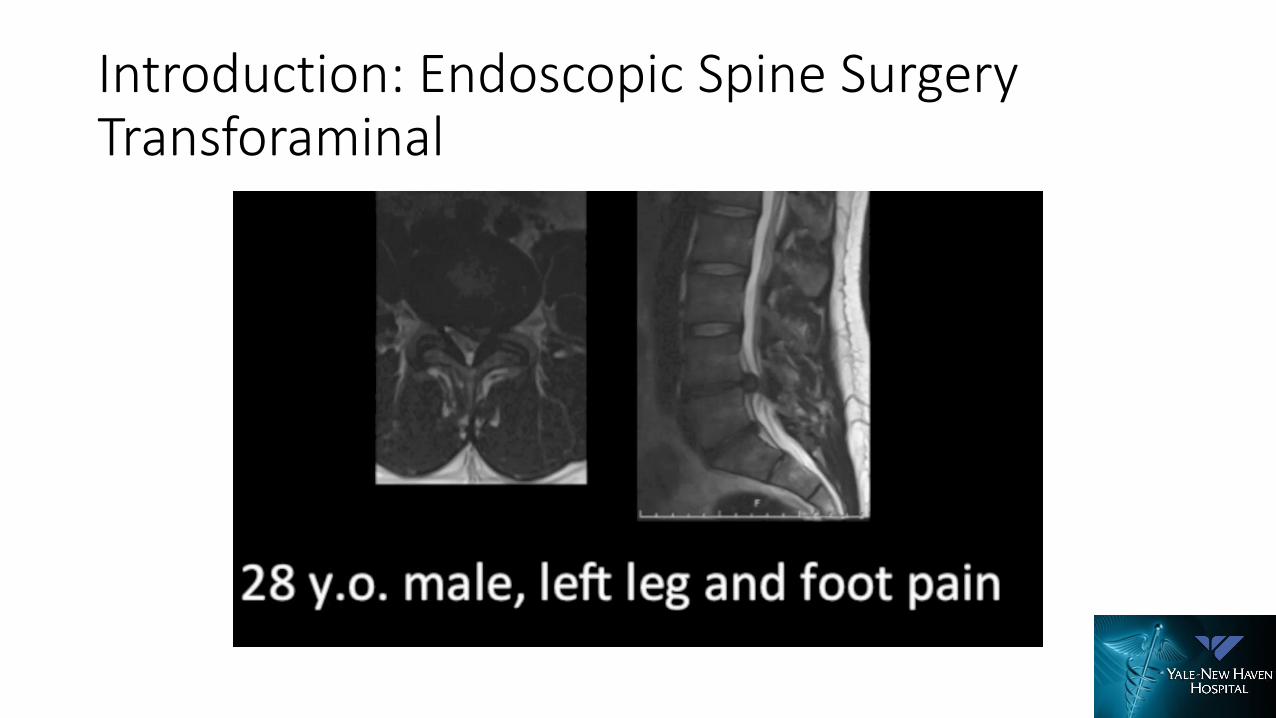
Introduction: Endoscopic Spine Surgery Transforaminal
Introduction: Endoscopic Surgery Interlaminar
Dr.R.Morgenstern, Centro Médico Teknon
Endoscopic Facet Sparing TransforaminalFusion• Endoscopic foraminal decompression preceding oblique lateral lumbar
interbody fusion to decrease the incidence of post operativedysaesthesia.
• Int J Spine Surg. 2014 Dec 1;8. doi: 10.14444/1019. eCollection 2014.
• Usefulness of an expandable interbody spacer for the treatment of foraminal stenosis in extremely collapsed disks: preliminary clinicalexperience with endoscopic posterolateral transforaminal approach. Morgenstern R, et al
• J Spinal Disord Tech. 2011 Dec;24(8):485-91. doi: 10.1097/BSD.0b013e3182064614.
Endoscopic Facet Sparing TransforaminalFusion: ASC• Wang, Michael Y., et al. "An analysis of the differences in the acute
hospitalization charges following minimally invasive versus open posterior lumbar interbody fusion: Clinical article." Journal of Neurosurgery: Spine 12.6 (2010): 694-699.
• Wang, Michael Y., et al Awake Endoscopic Fusion, American Association of Neurological Surgeons (AANS) 84th Annual Meeting. Abstract 601. Presented May 2, 2016.
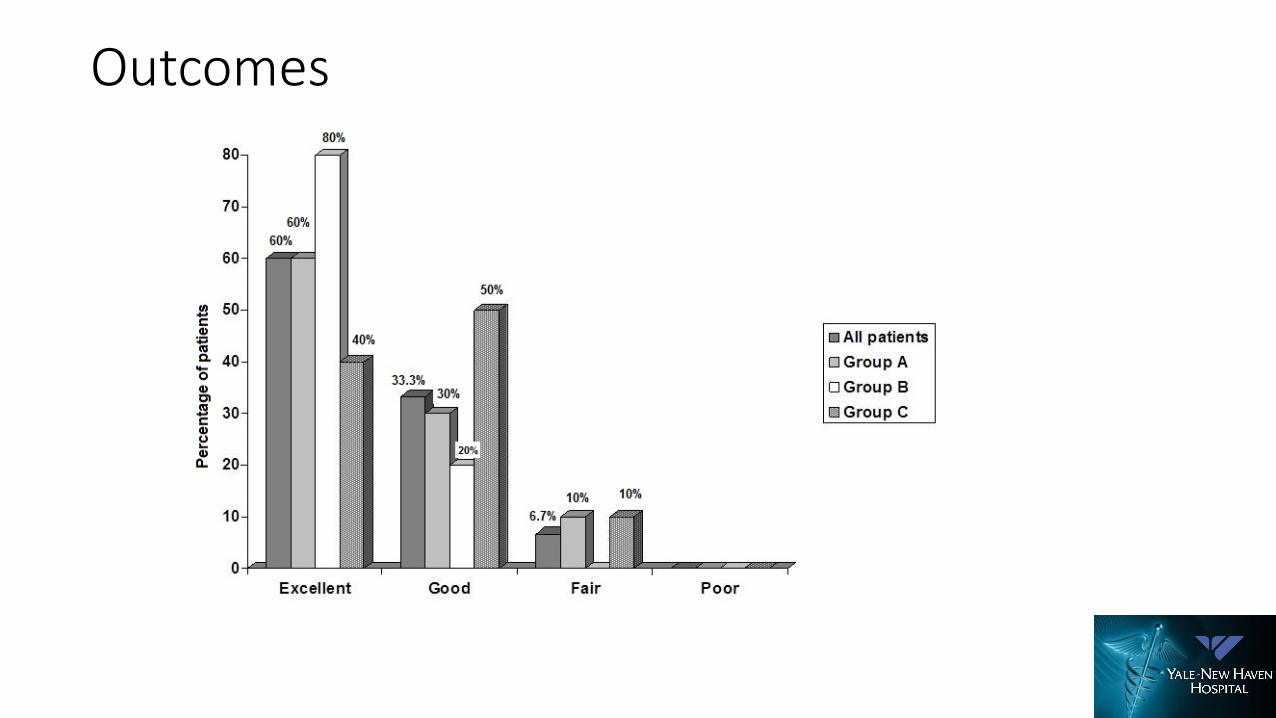
Outcomes
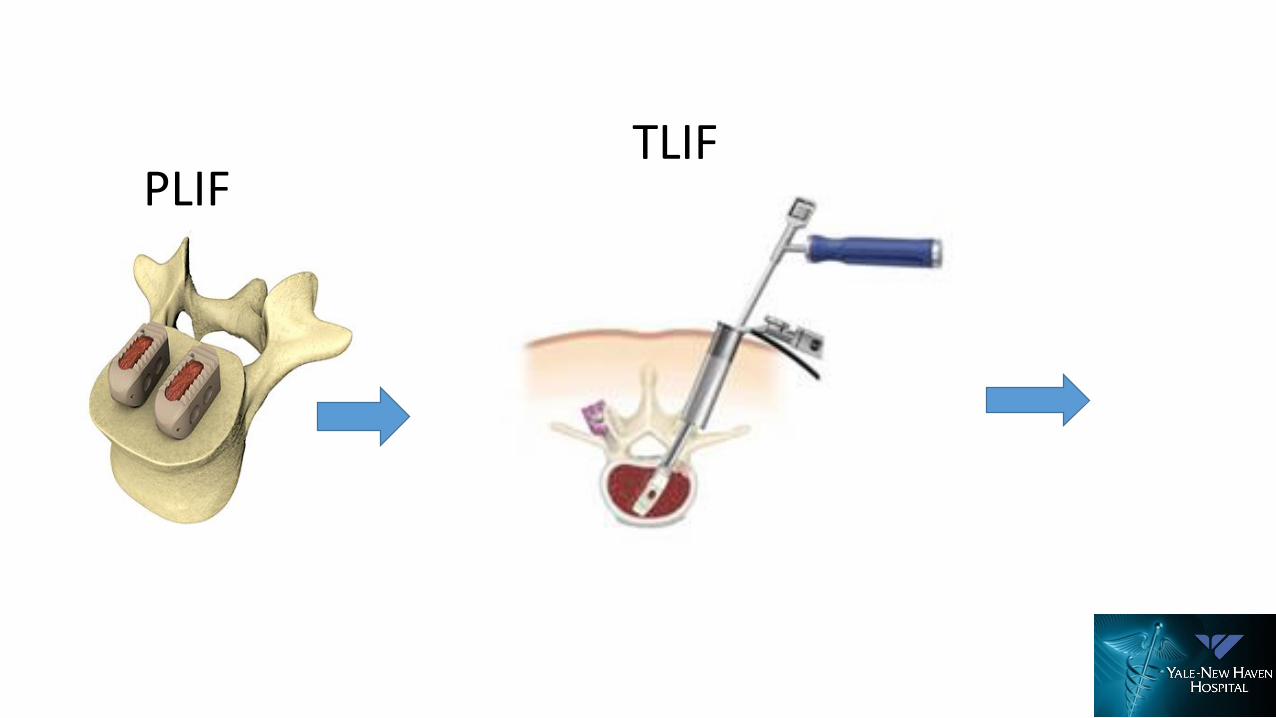
PLIFTLIF
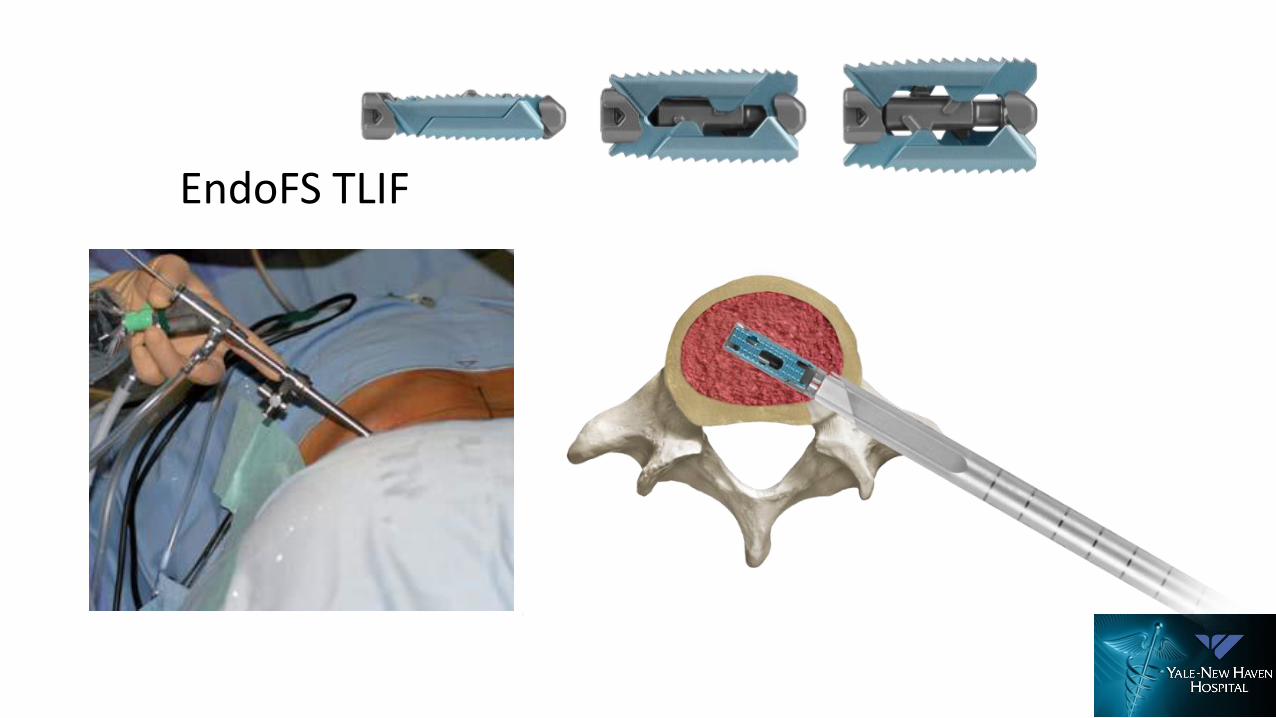
EndoFS TLIF
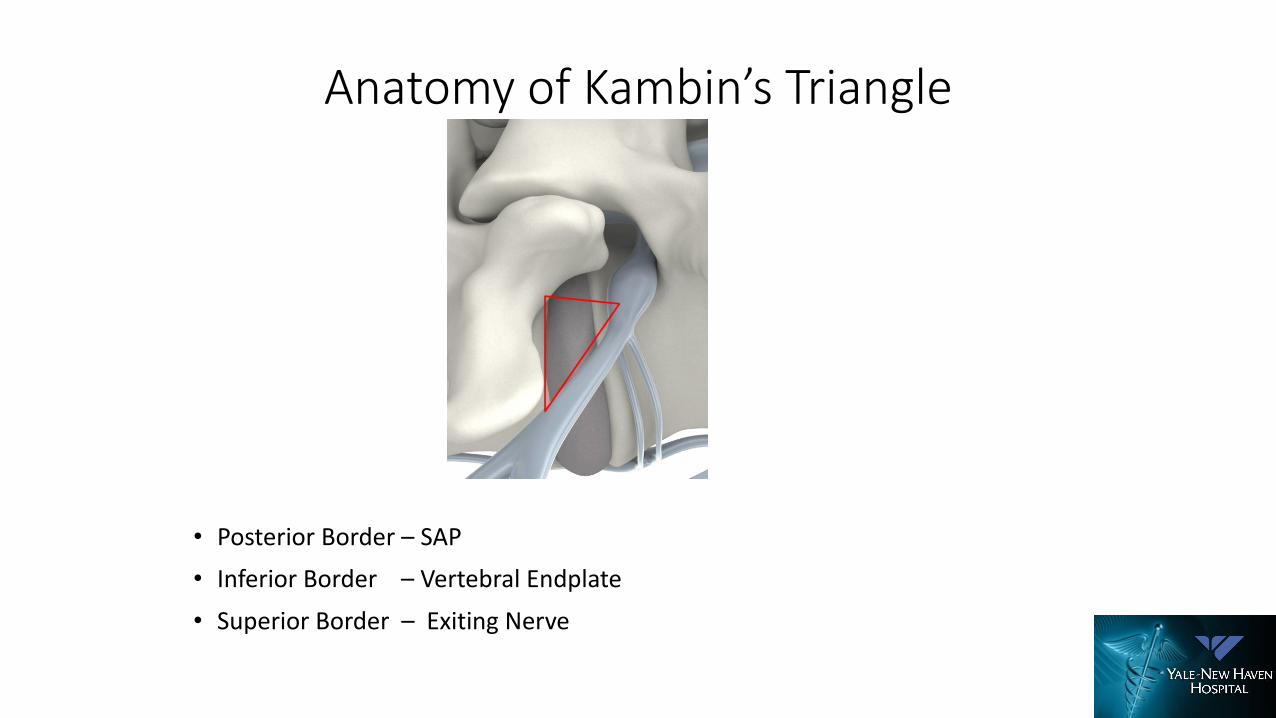
Anatomy of Kambin’s Triangle
• Posterior Border – SAP
• Inferior Border – Vertebral Endplate
• Superior Border – Exiting Nerve
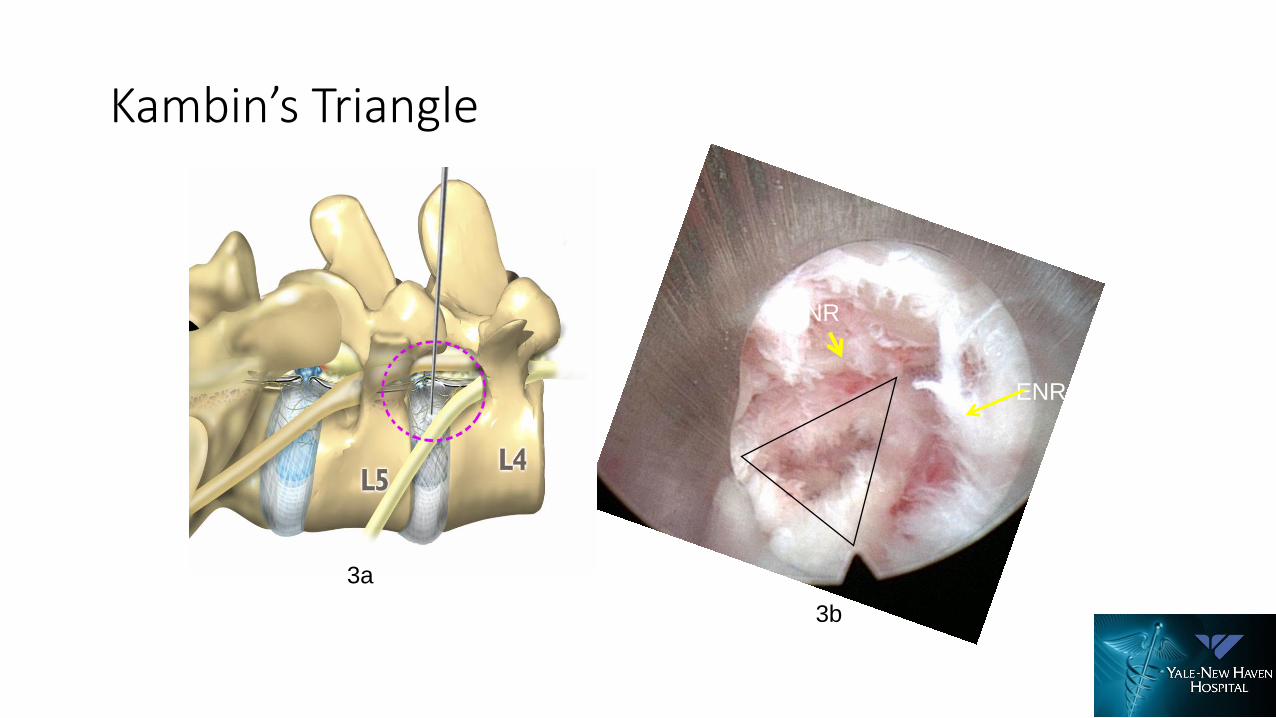
Kambin’s Triangle
ENR
TNR
3a
3b

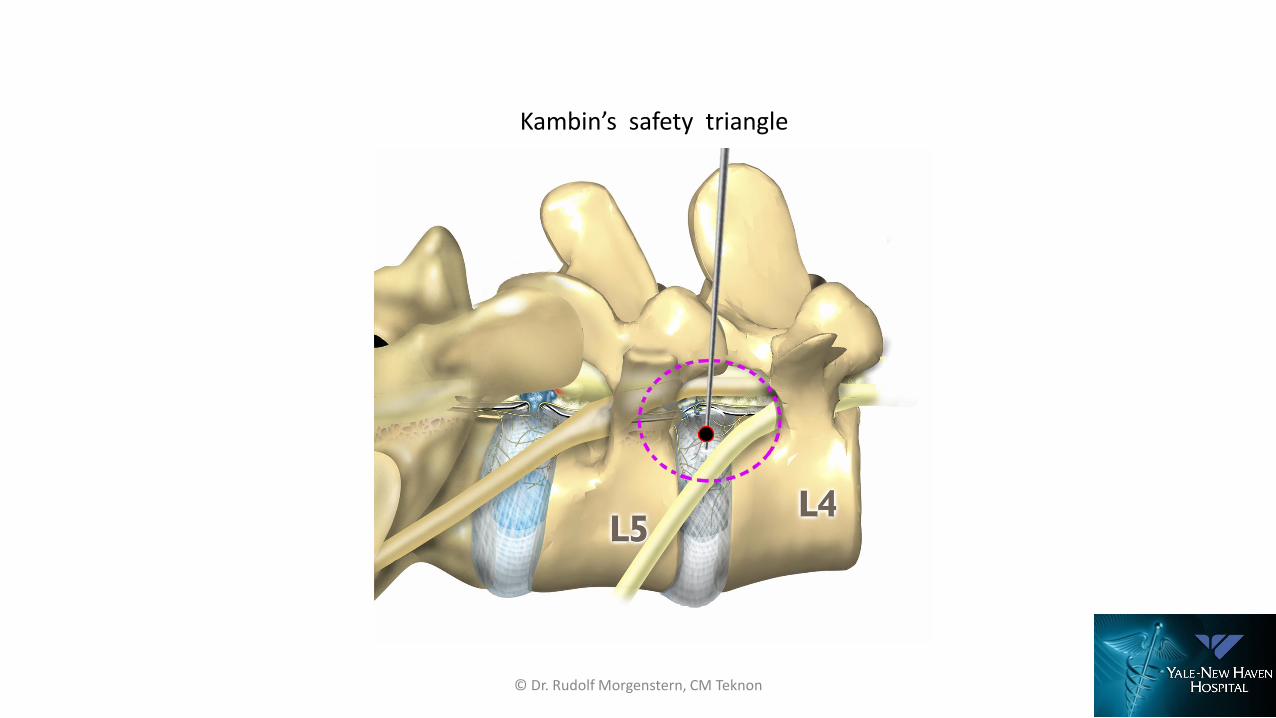
Kambin’s safety triangle
© Dr. Rudolf Morgenstern, CM Teknon, 2011
© Dr. Rudolf Morgenstern, CM Teknon
Kambin’s safety triangle
© Dr. Rudolf Morgenstern, CM Teknon

© Dr. Rudolf Morgenstern, CM Teknon
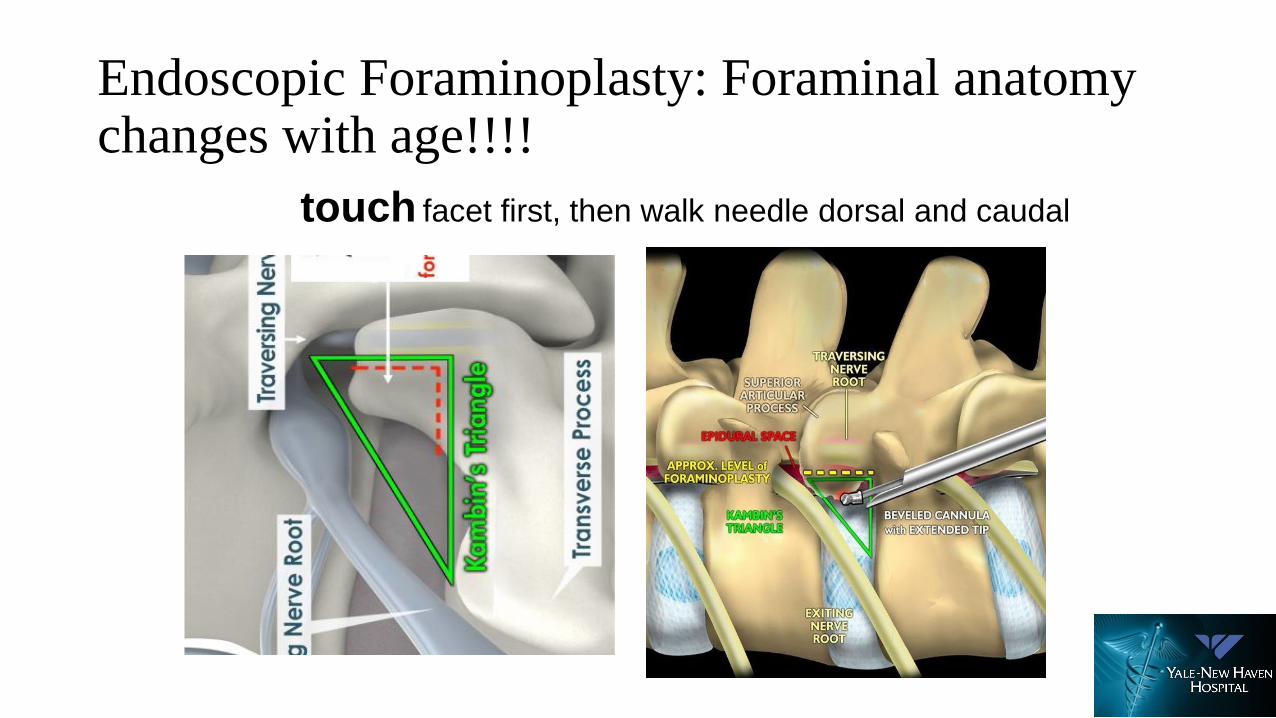
Endoscopic Foraminoplasty: Foraminal anatomy changes with age!!!!
touch facet first, then walk needle dorsal and caudal
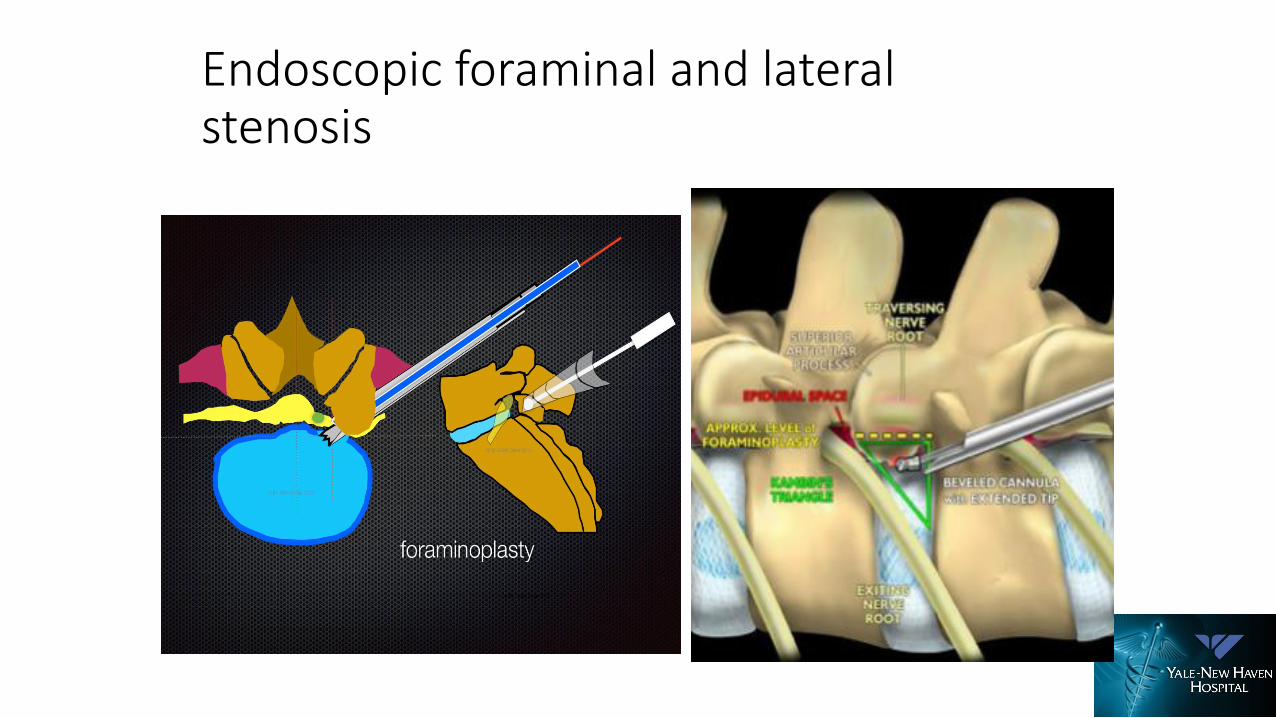
Endoscopic foraminal and lateral stenosis
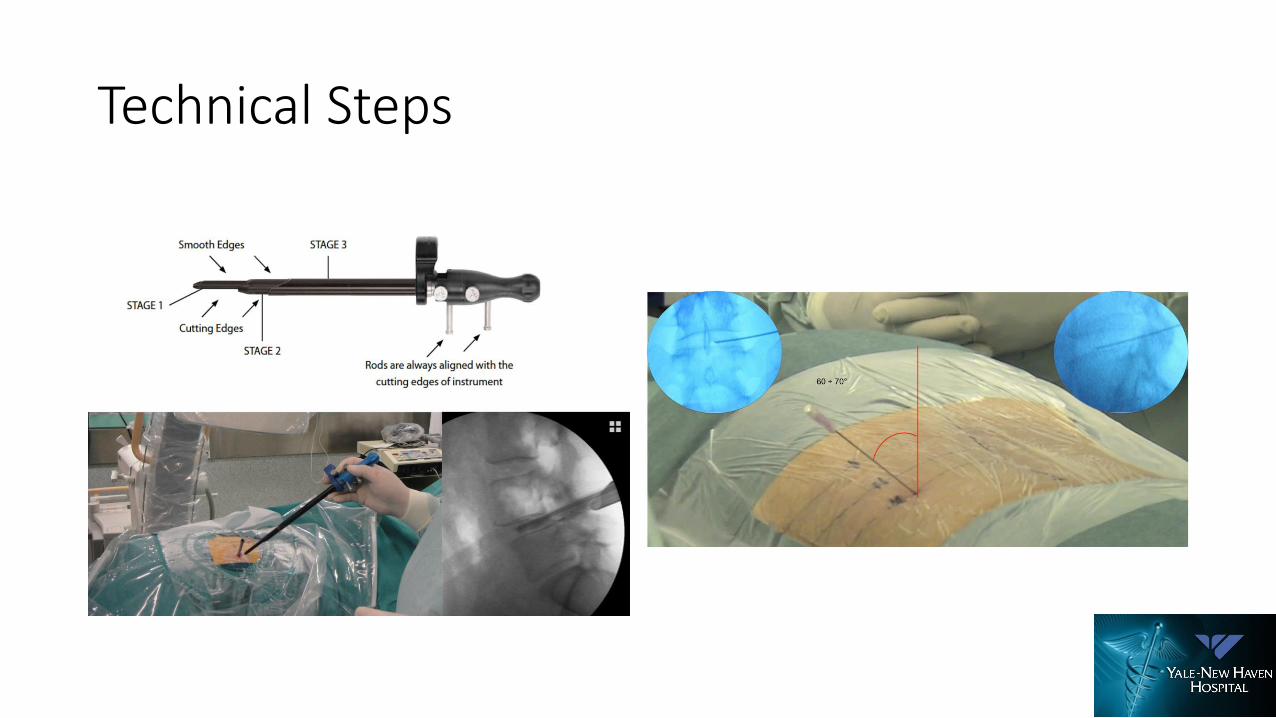
Technical Steps
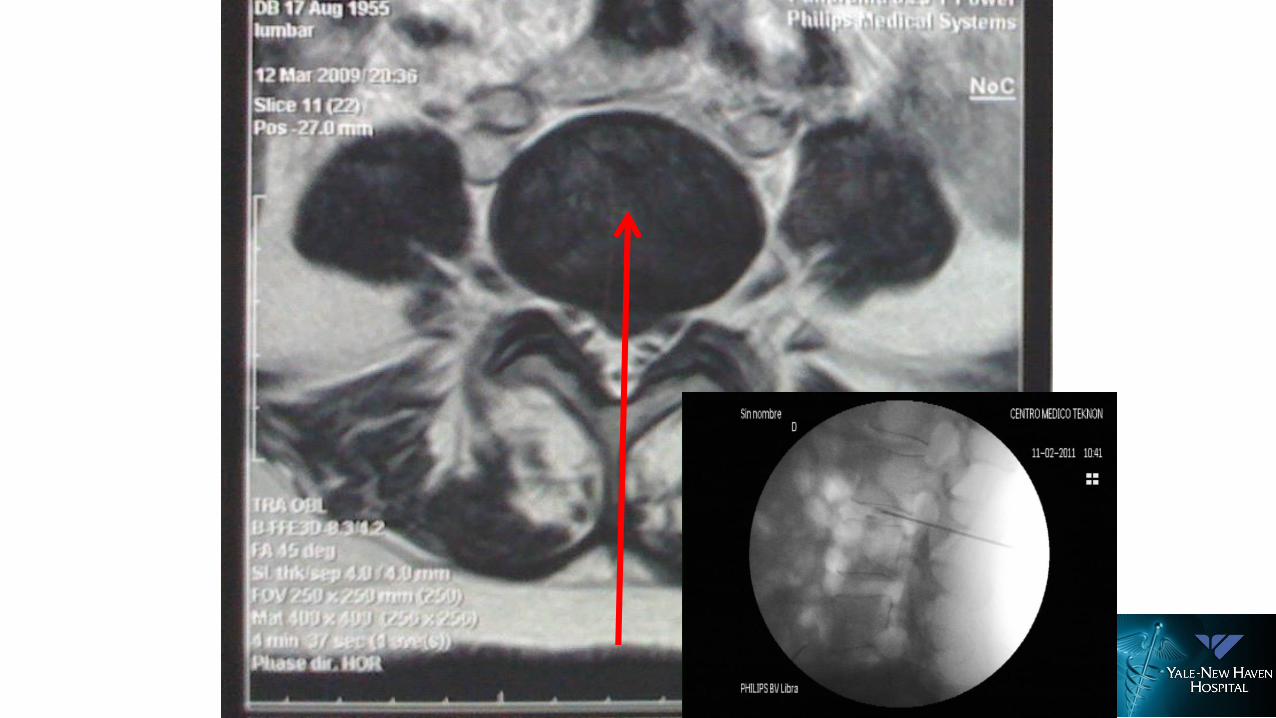
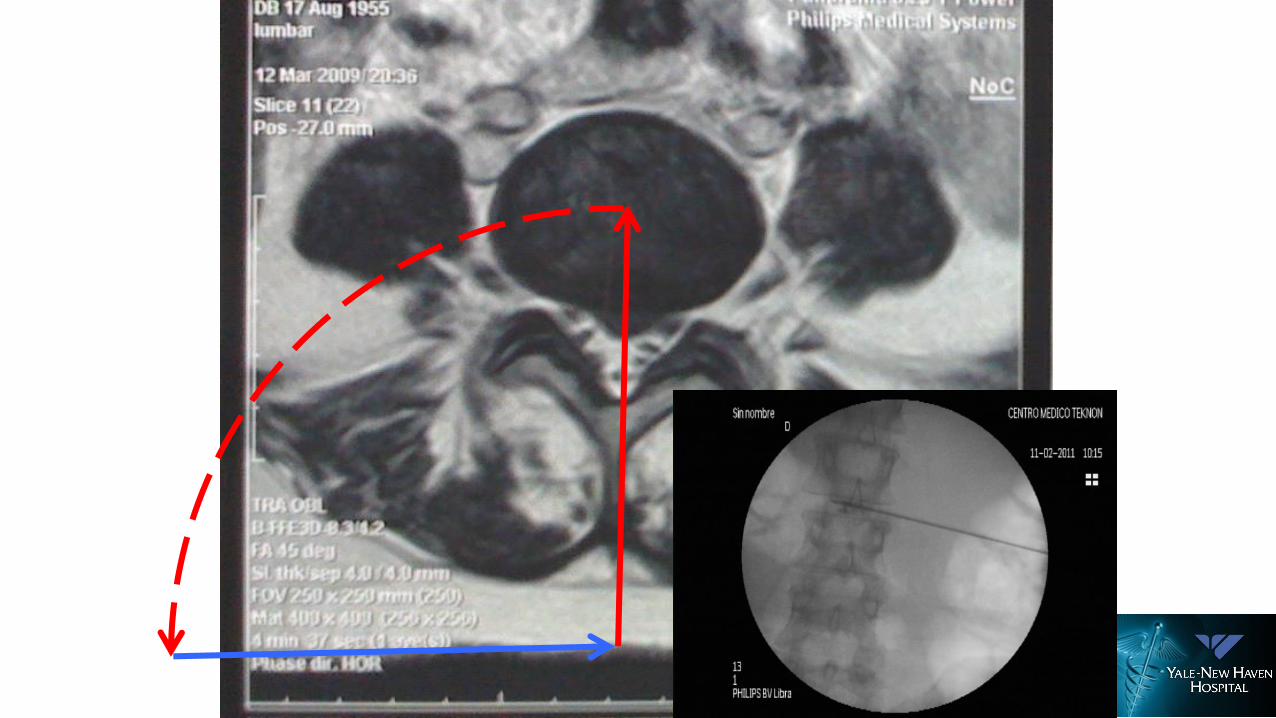
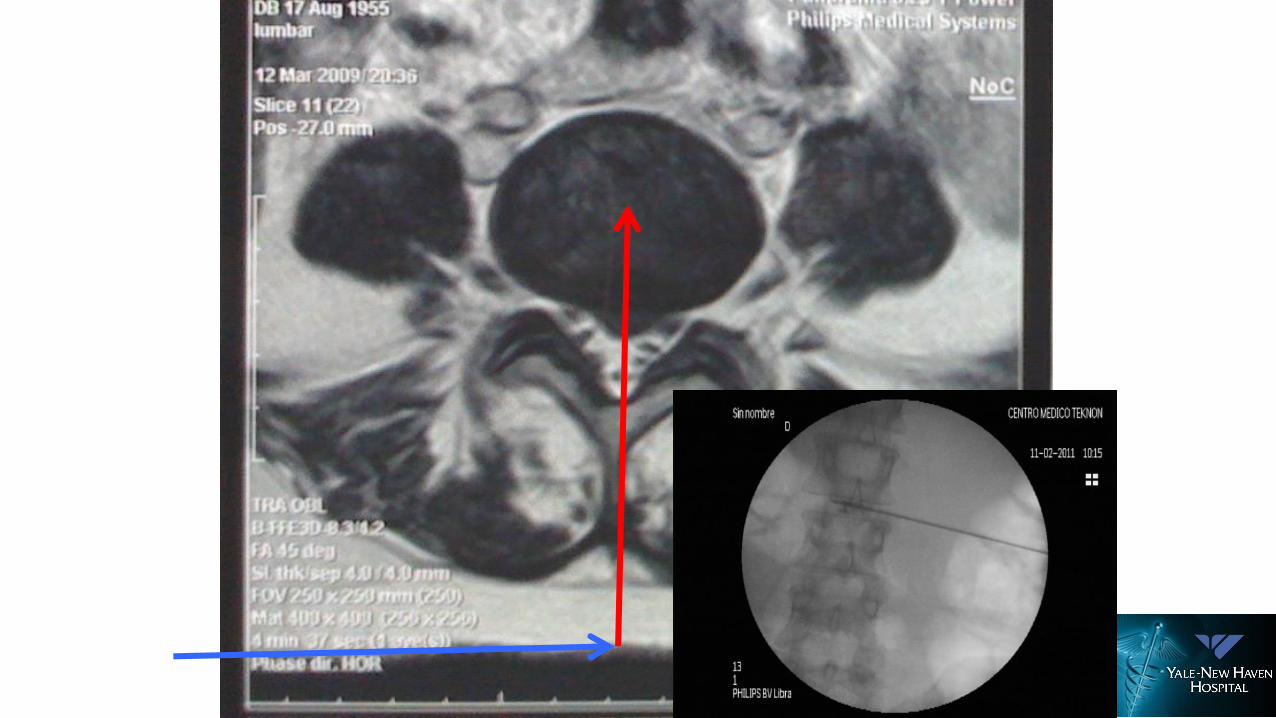
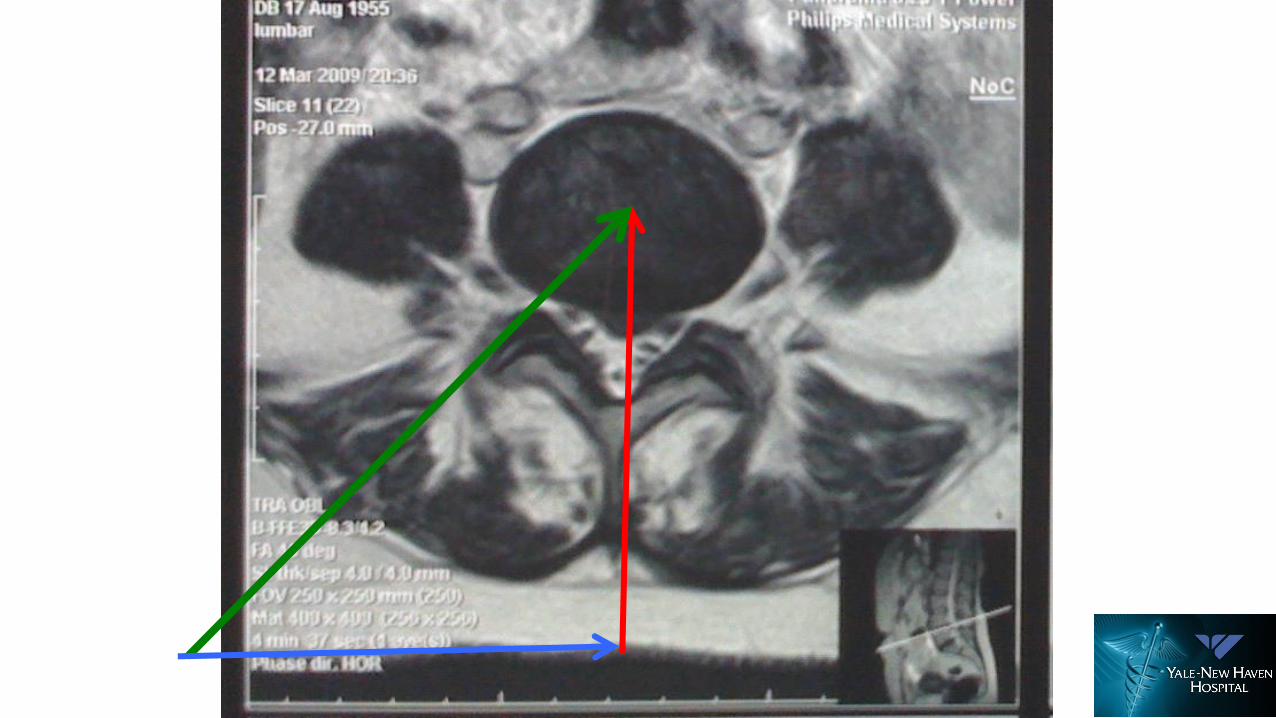
Needle Placement:
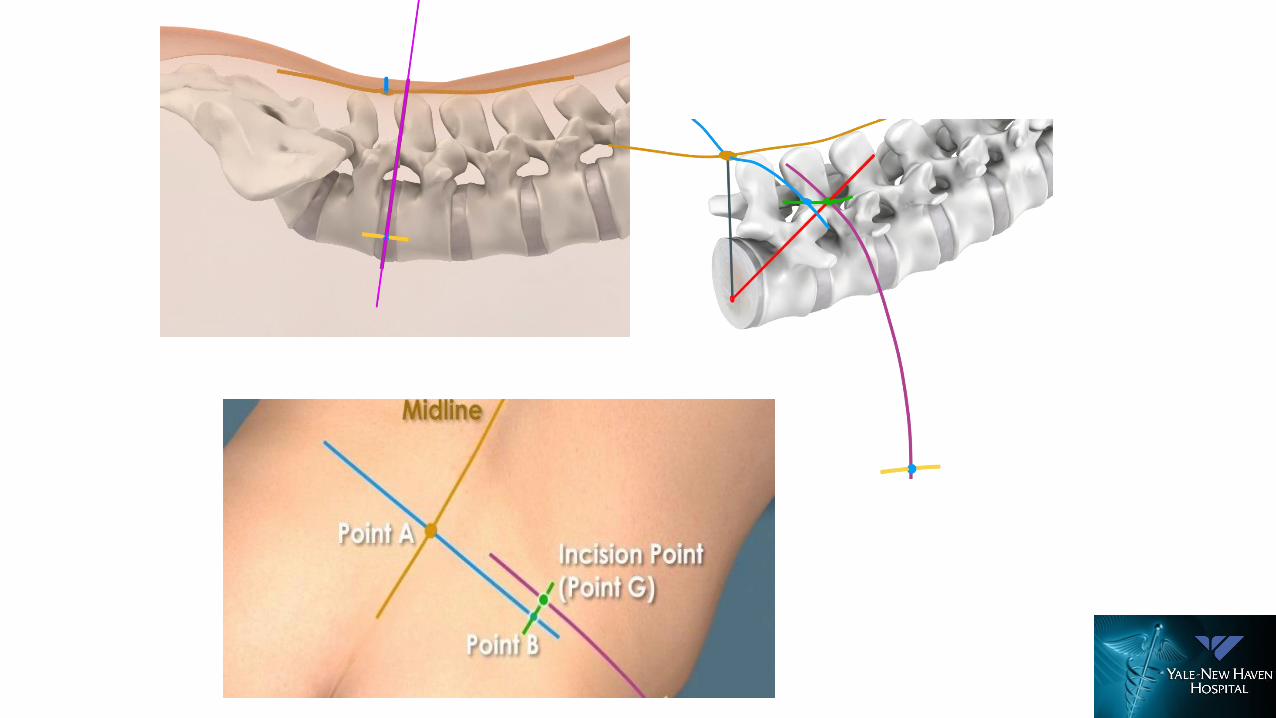

Approach


NEUROMONITORING

CONFIDENTIAL: For Internal Use Only, Not for Distribution
Procedure Overview
1) Needle Insertion
CONFIDENTIAL: For Internal Use Only, Not for Distribution
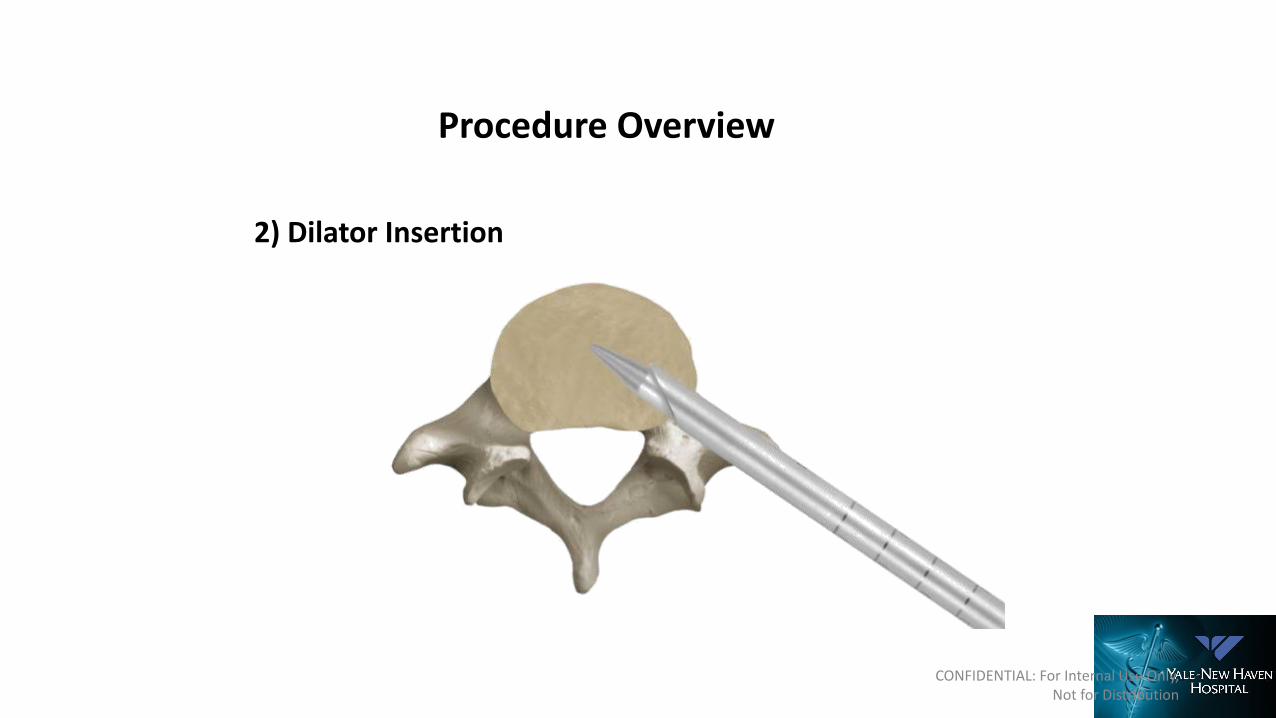
Procedure Overview
2) Dilator Insertion
CONFIDENTIAL: For Internal Use Only, Not for Distribution
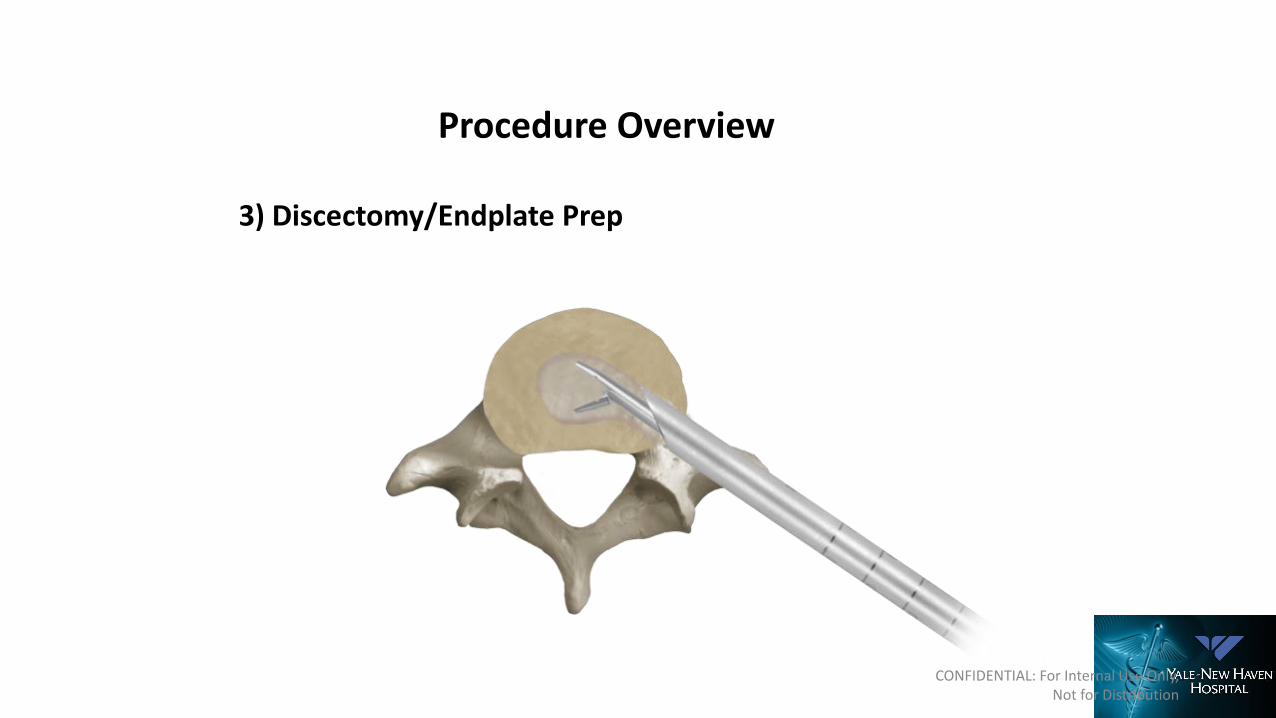
Procedure Overview
3) Discectomy/Endplate Prep

Description
CONFIDENTIAL: For Internal Use Only, Not for Distribution
Width: 8mm width only
Lengths: 22, 26, 30, 34mm
Expansion Range: 7-14mm
Lordosis: 4°
Implant information is available in the Technique Guide
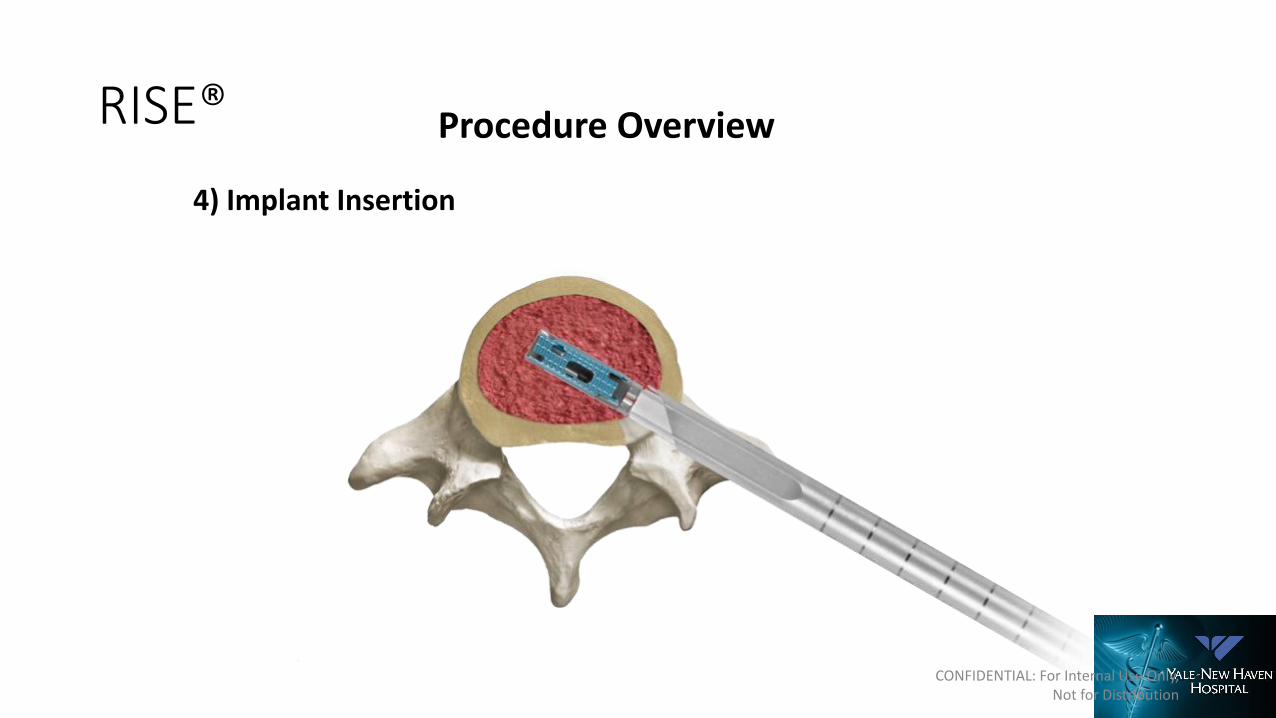
RISE®IntraLIF™ Implant Overview
RISE®
CONFIDENTIAL: For Internal Use Only, Not for Distribution
Procedure Overview
4) Implant Insertion

Foraminoplasty may be needed to enter space
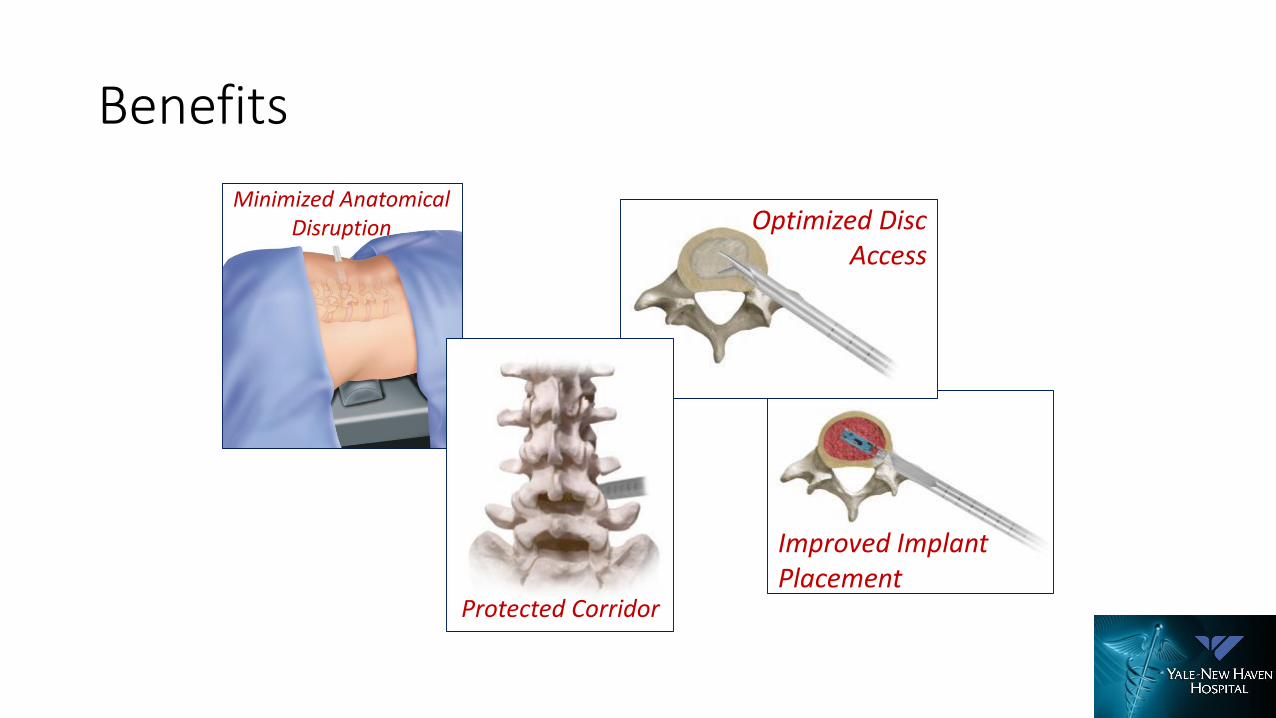
Benefits
Minimized Anatomical Disruption
Improved Implant Placement
Optimized Disc Access
Protected Corridor

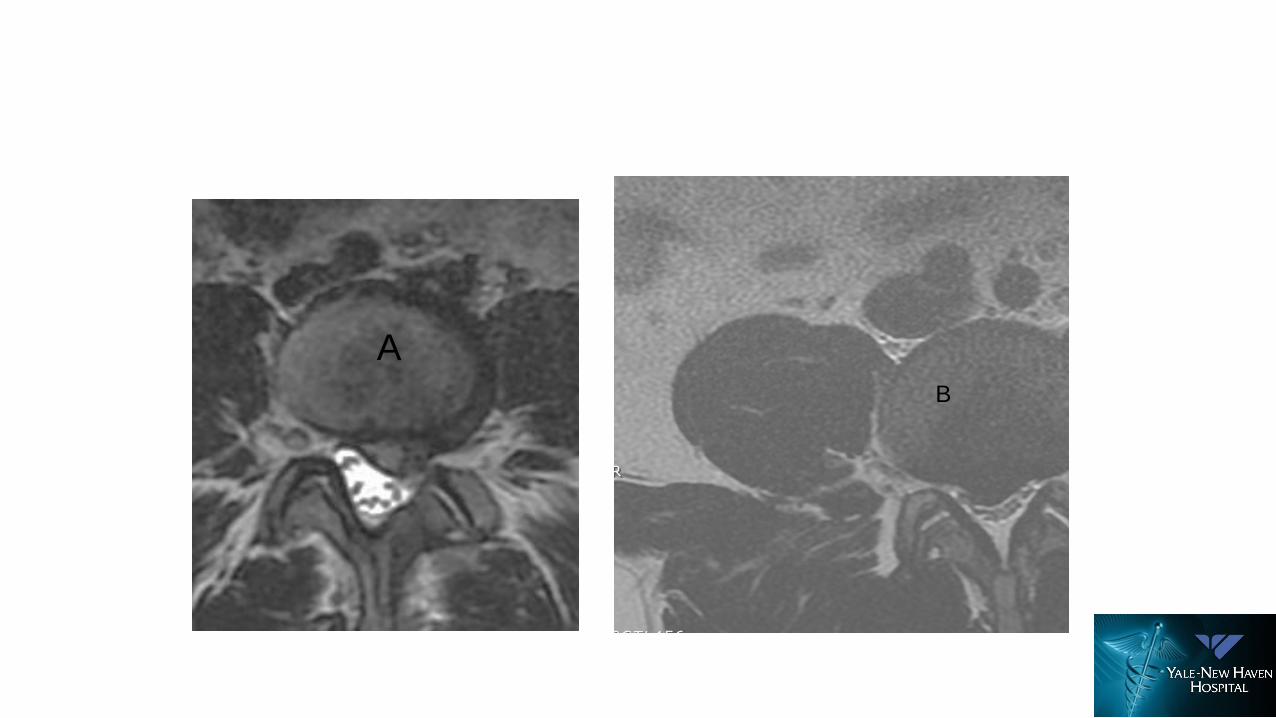
L1-L2 Disc
Most vulnerable for abdominal organ injury using extreme lateral approach
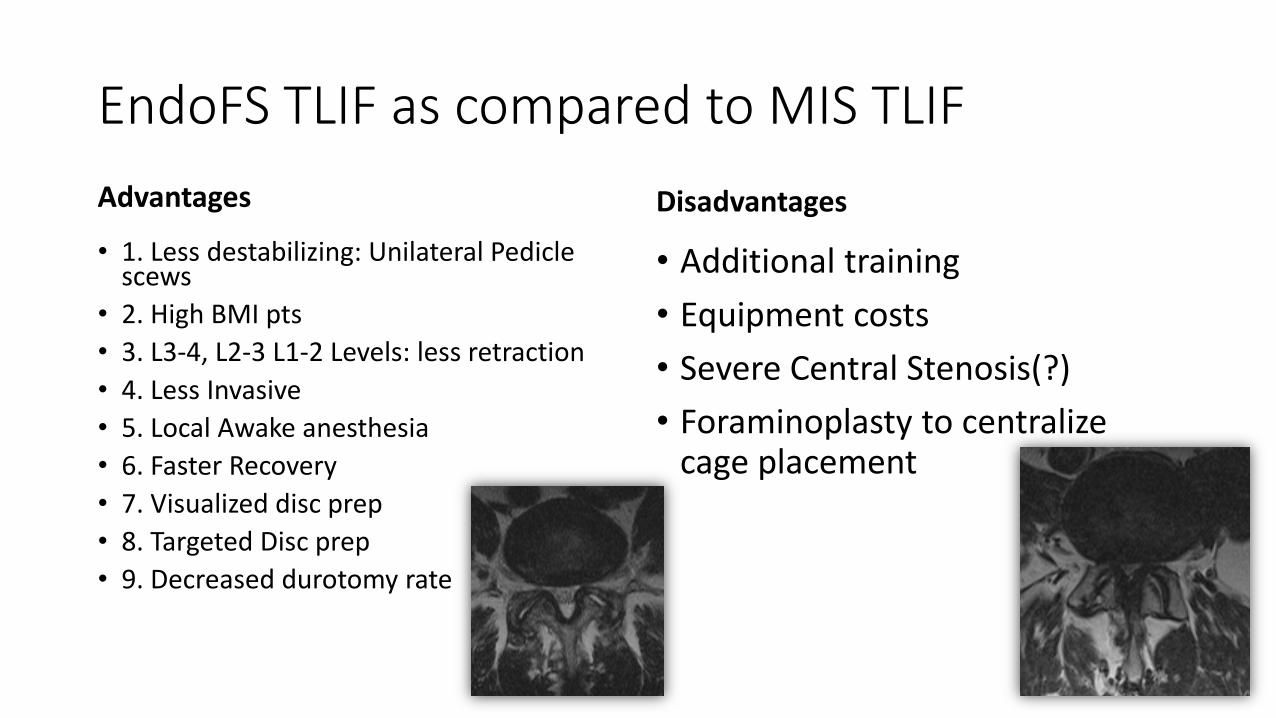
EndoFS TLIF as compared to MIS TLIF
Advantages
• 1. Less destabilizing: Unilateral Pedicle scews
• 2. High BMI pts
• 3. L3-4, L2-3 L1-2 Levels: less retraction
• 4. Less Invasive
• 5. Local Awake anesthesia
• 6. Faster Recovery
• 7. Visualized disc prep
• 8. Targeted Disc prep
• 9. Decreased durotomy rate
Disadvantages
• Additional training
• Equipment costs
• Severe Central Stenosis(?)
• Foraminoplasty to centralize cage placement

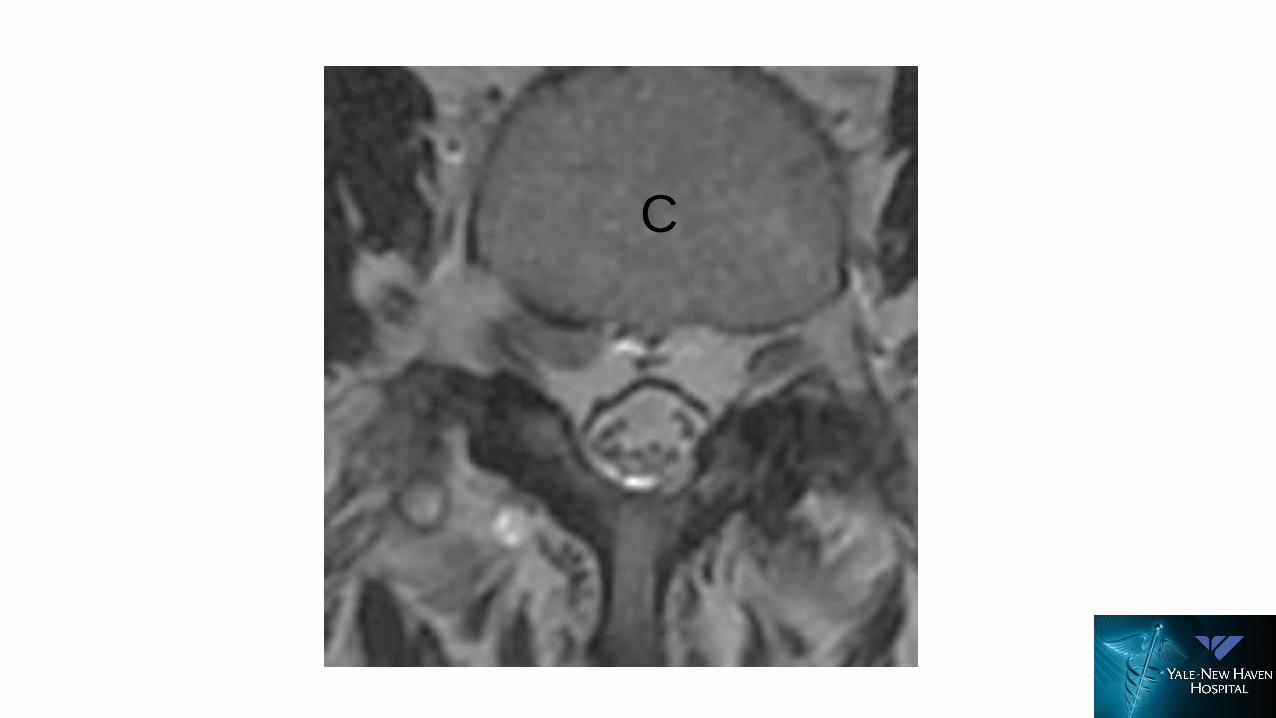
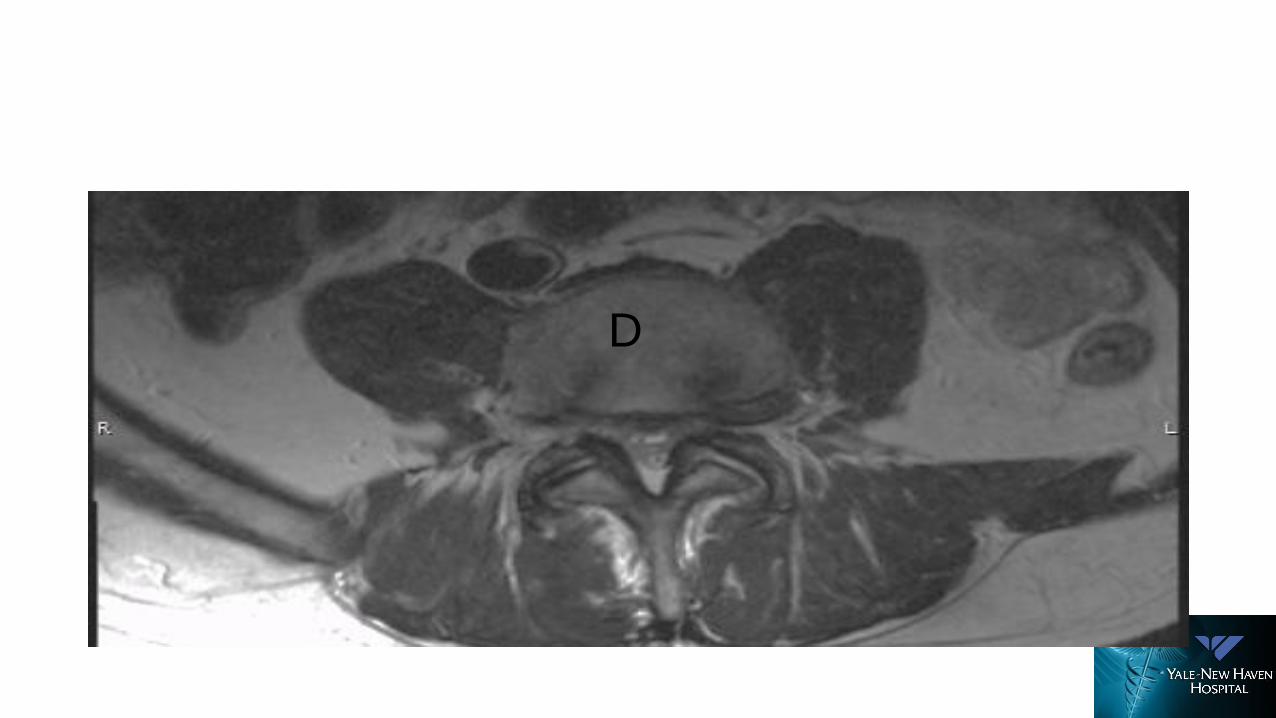
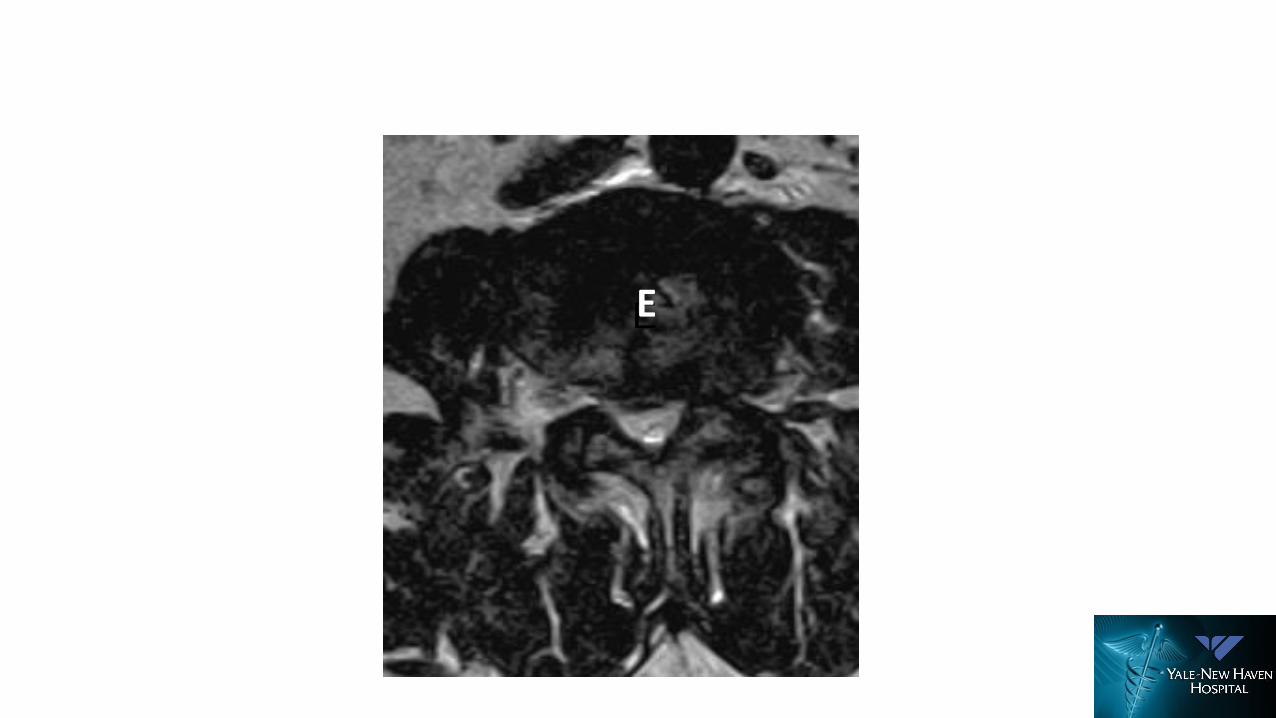
Big, Small, Narrow, Wide: Endoscopic Surgery The Neutralizer
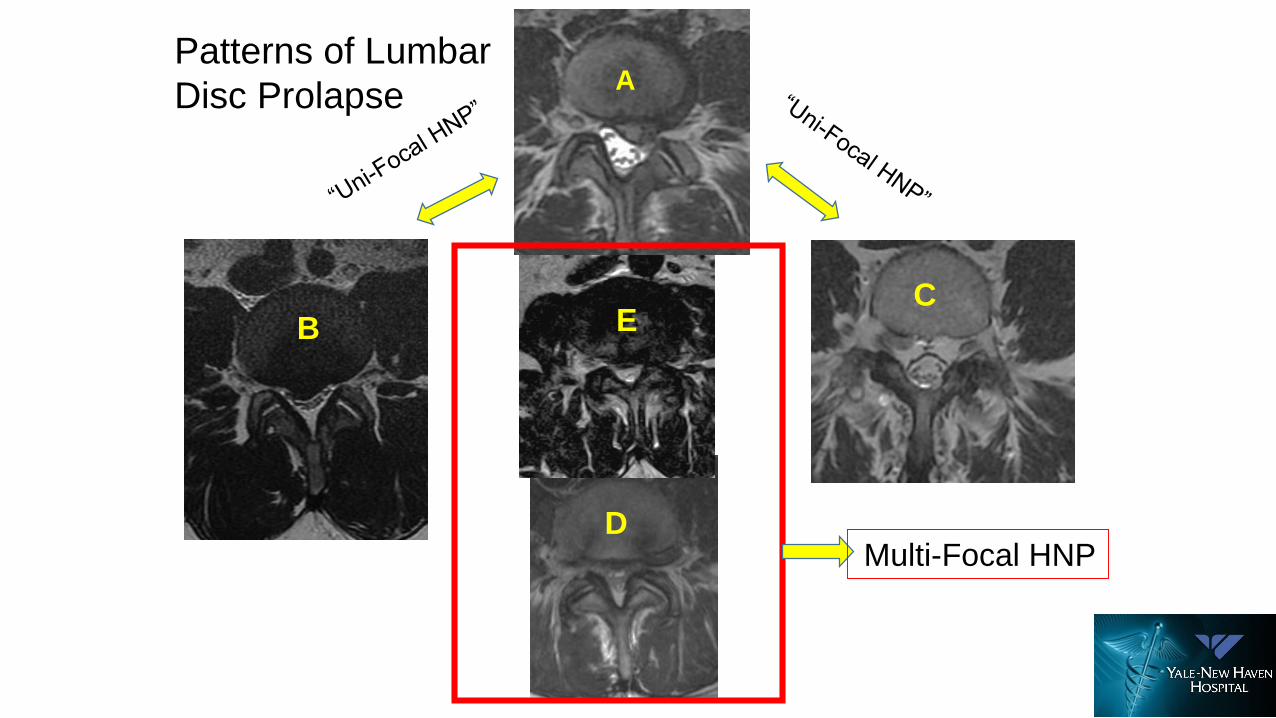
A
C
D
E
Patterns of Lumbar
Disc Prolapse
Multi-Focal HNP
B EB
AB
C
D
EEE

Intraop
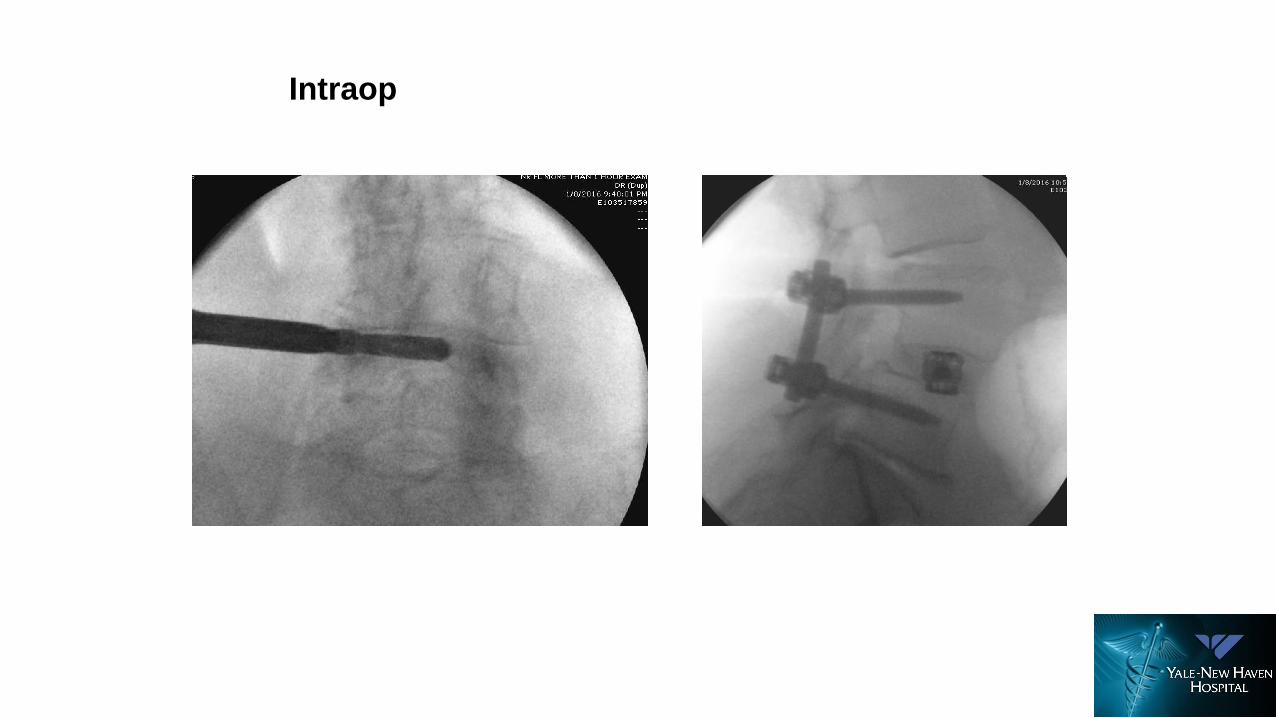
Intraop
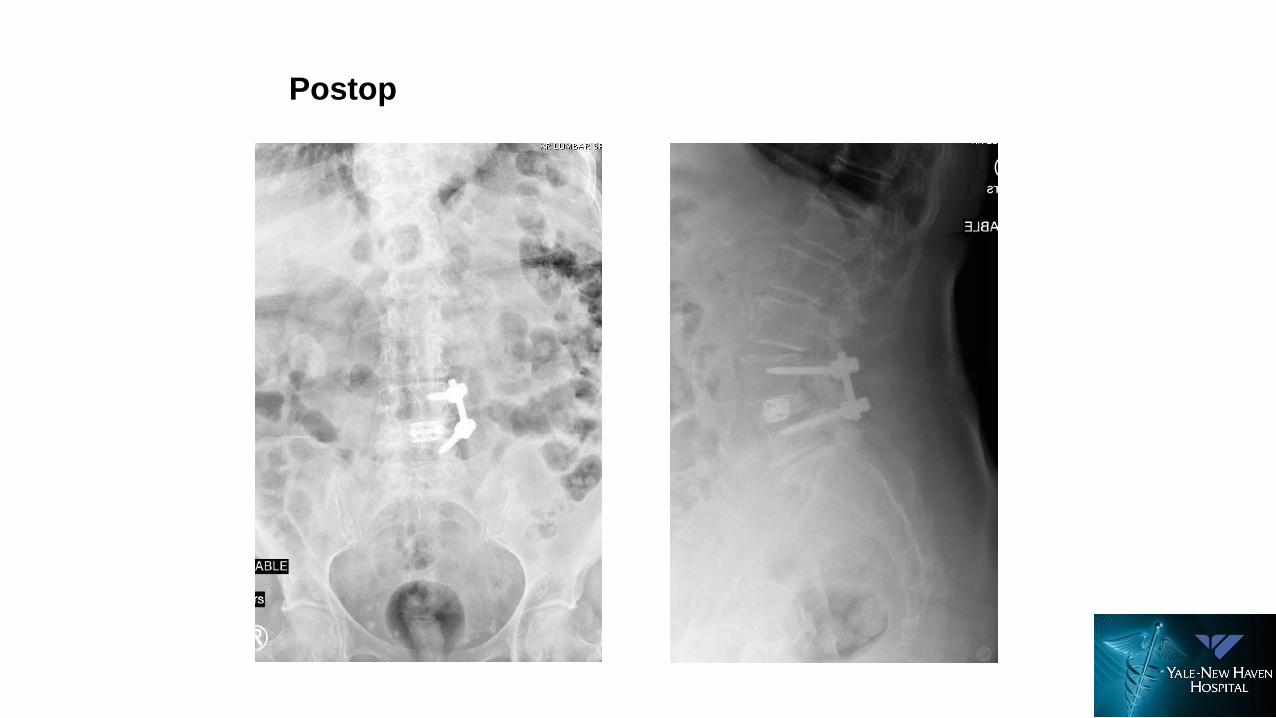
Postop
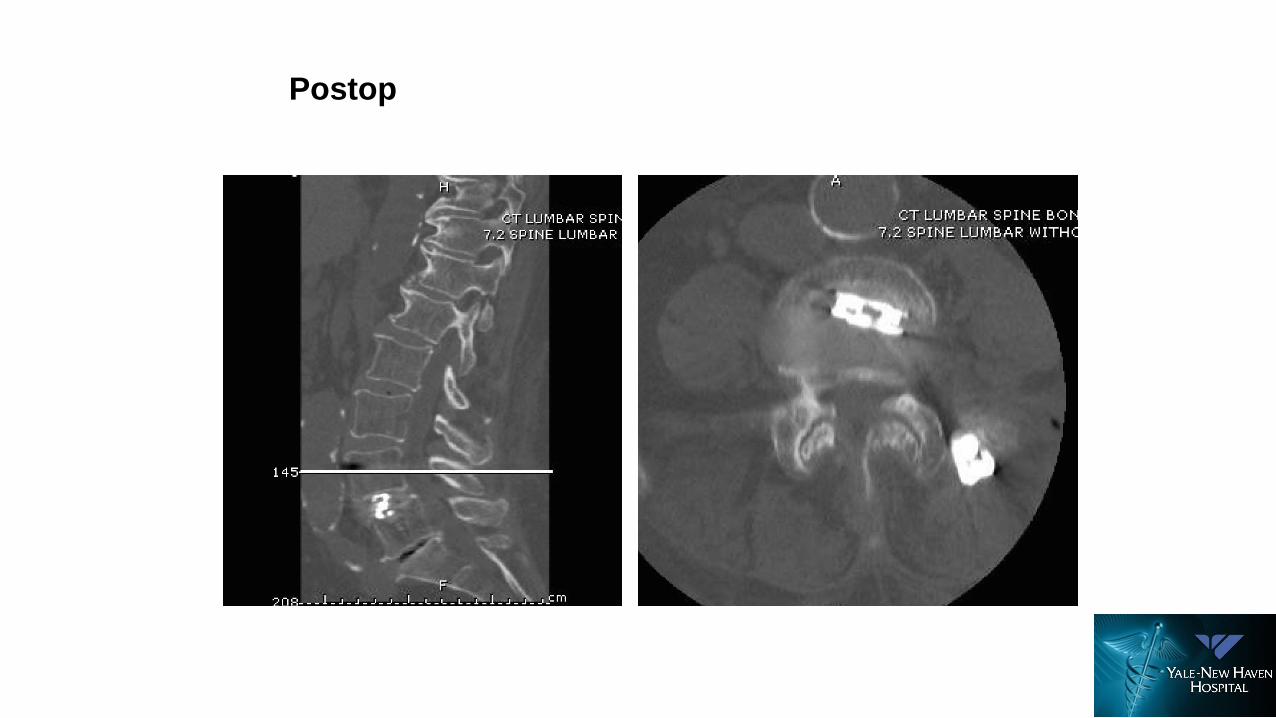
Postop
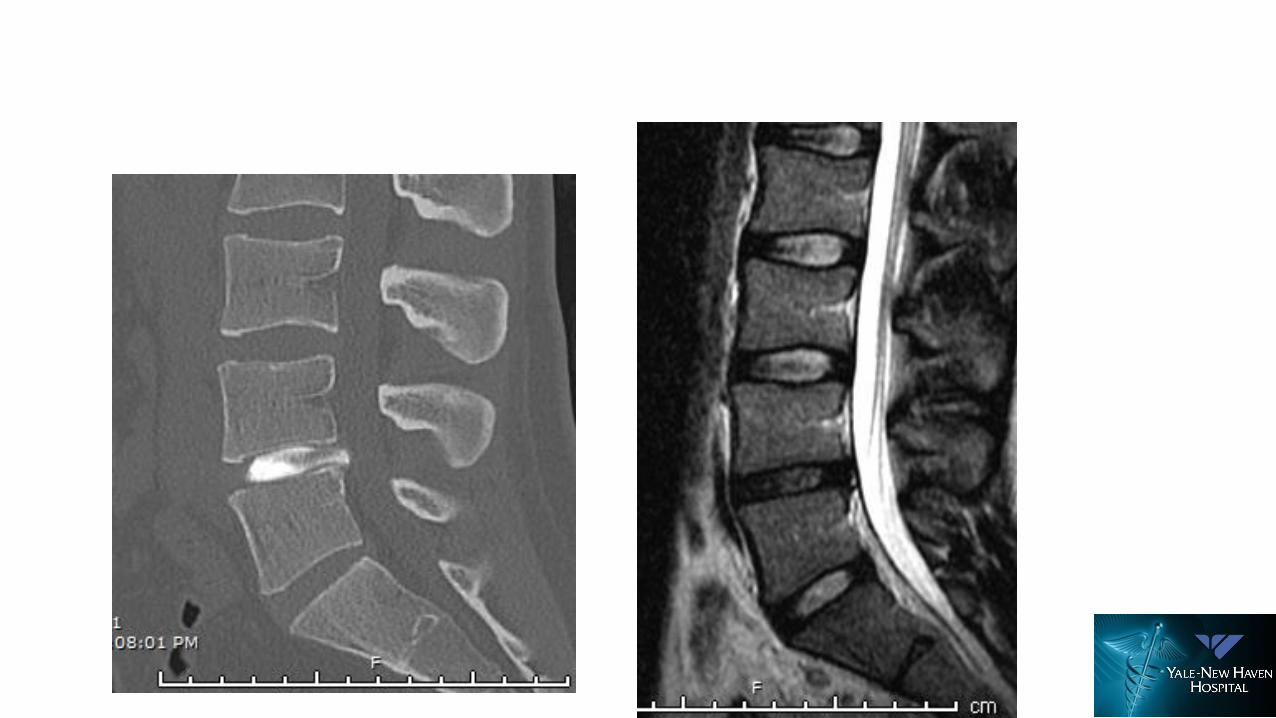
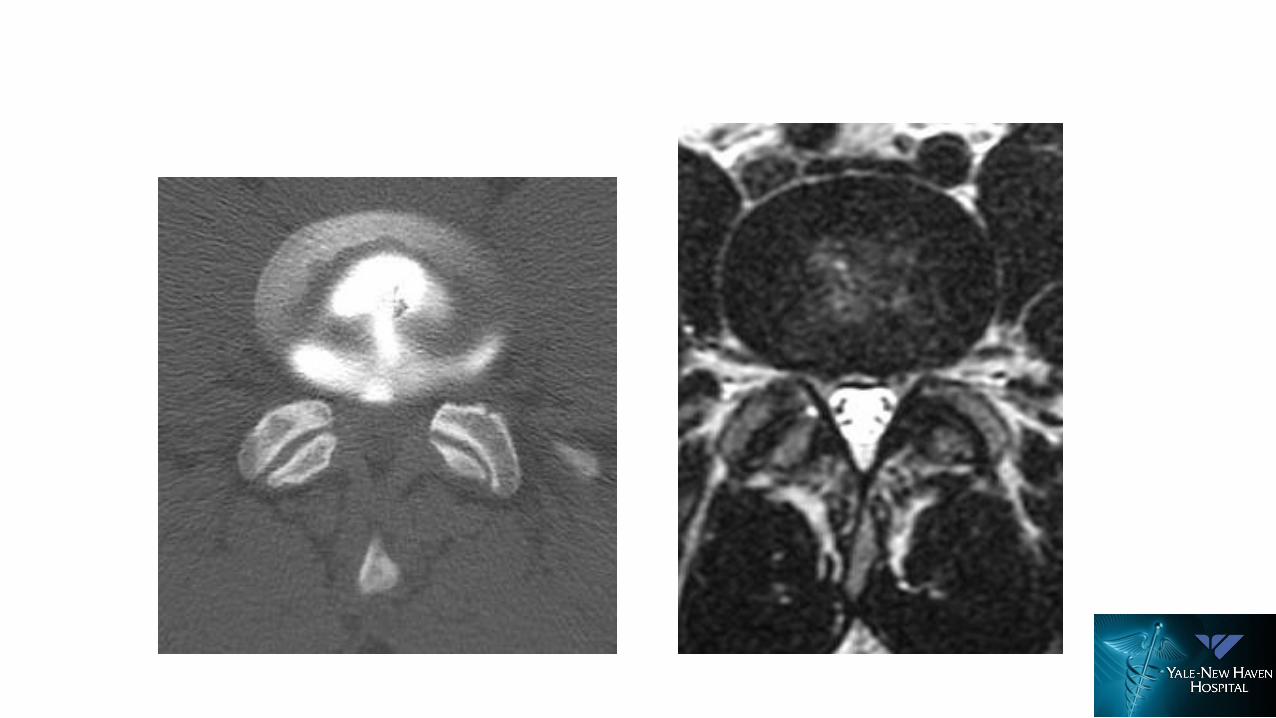
Case
• Police Officer
• WC case
• 25 yo male
• BMI 24
• Significant hx of diverticulitis
• LBP 8/10
• Right leg pain 6/10
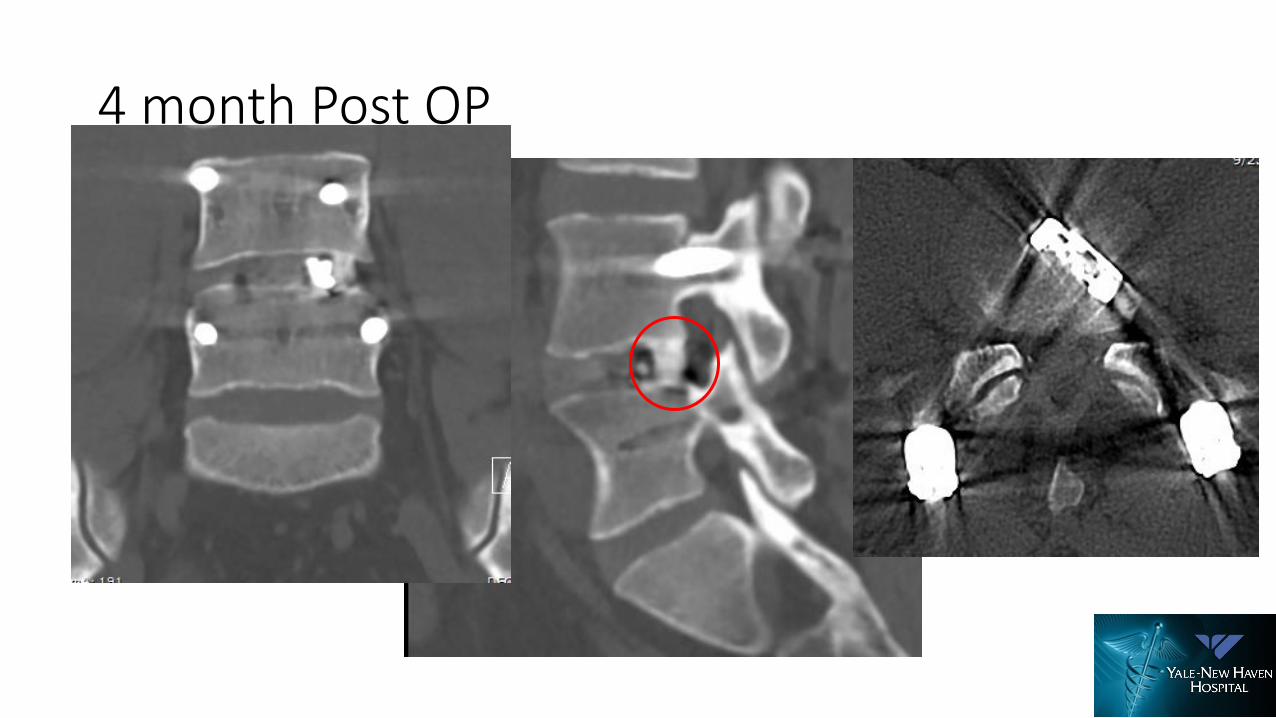
4 month Post OP

Case
• Female
• 76 years old
• Spondylolisthesis L4-L5 grade II
• Central stenosis L4-L5
• Right foraminal stenosis L4-L5
• Pre-op : VAS = 8 ; ODI = 38
• Post-op : VAS = 0 ; ODI = 17
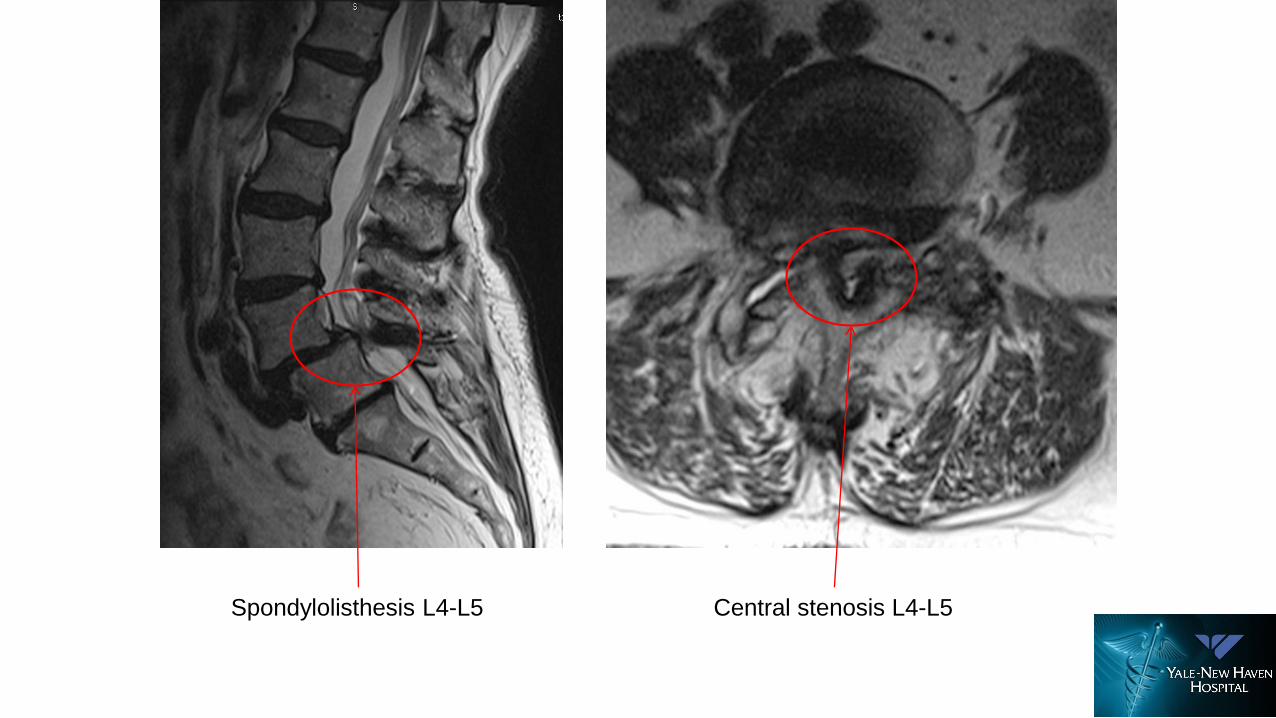
Central stenosis L4-L5Spondylolisthesis L4-L5
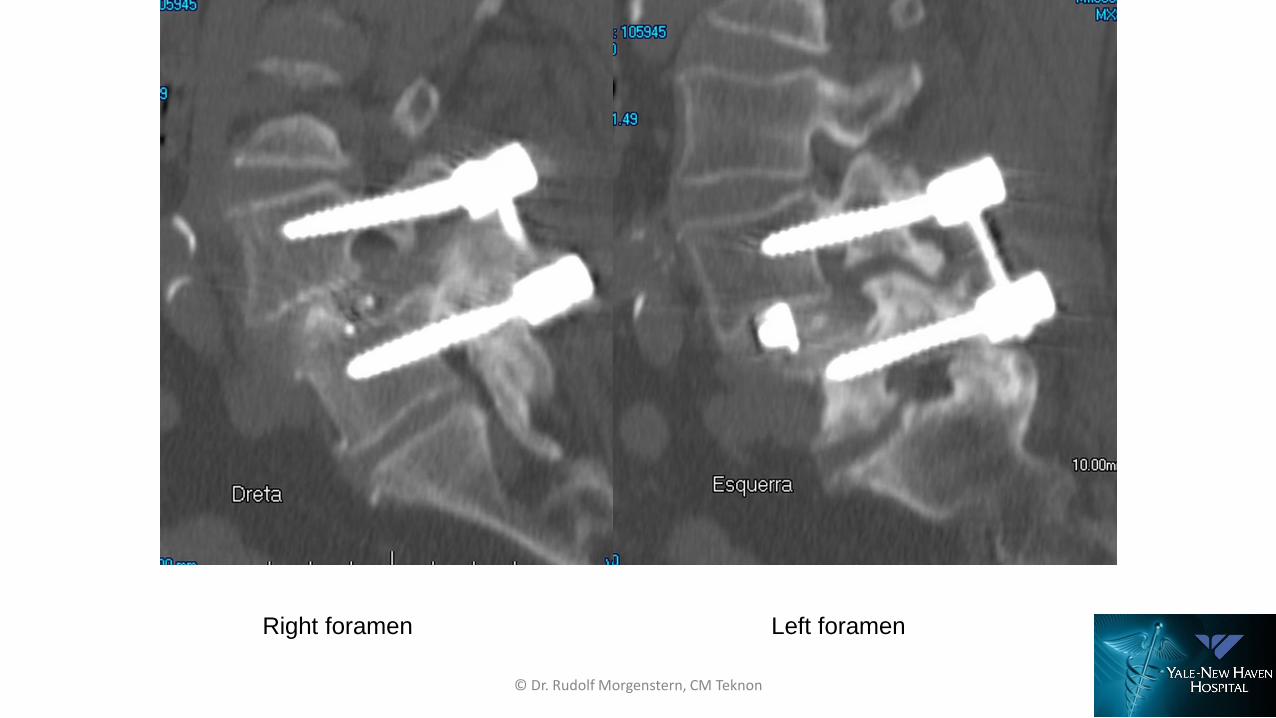
Right foramen Left foramen
© Dr. Rudolf Morgenstern, CM Teknon
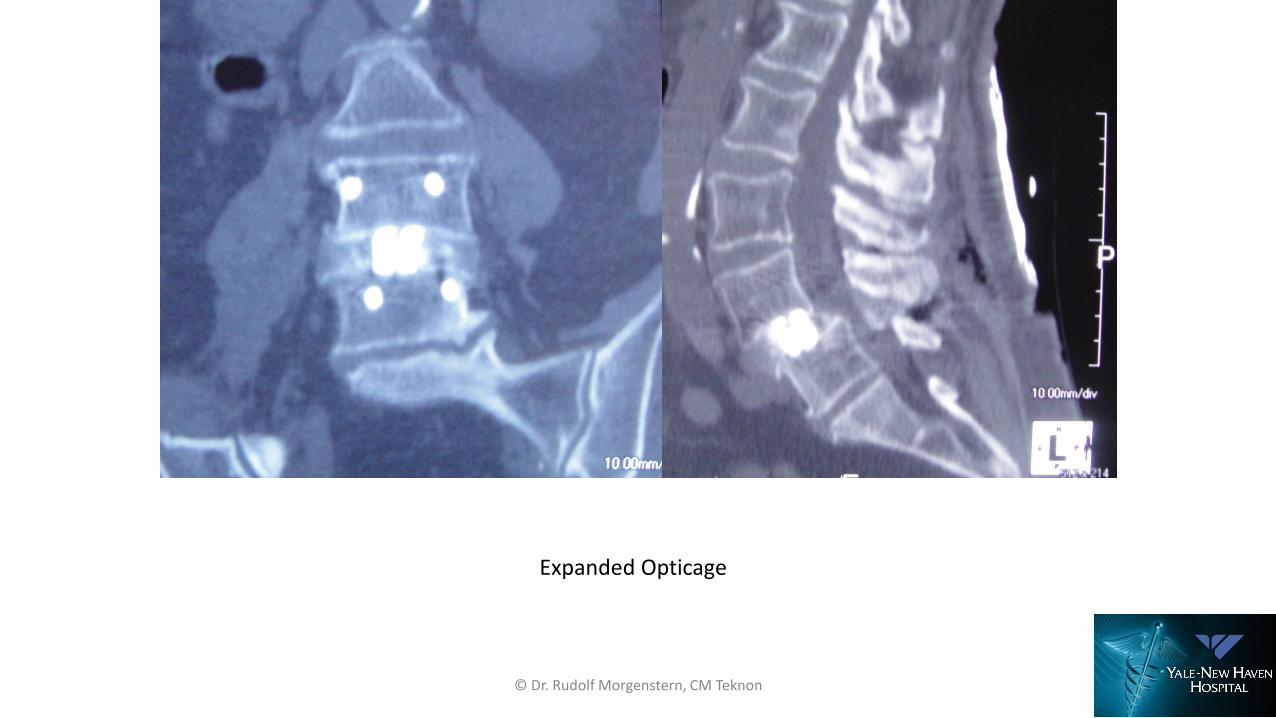
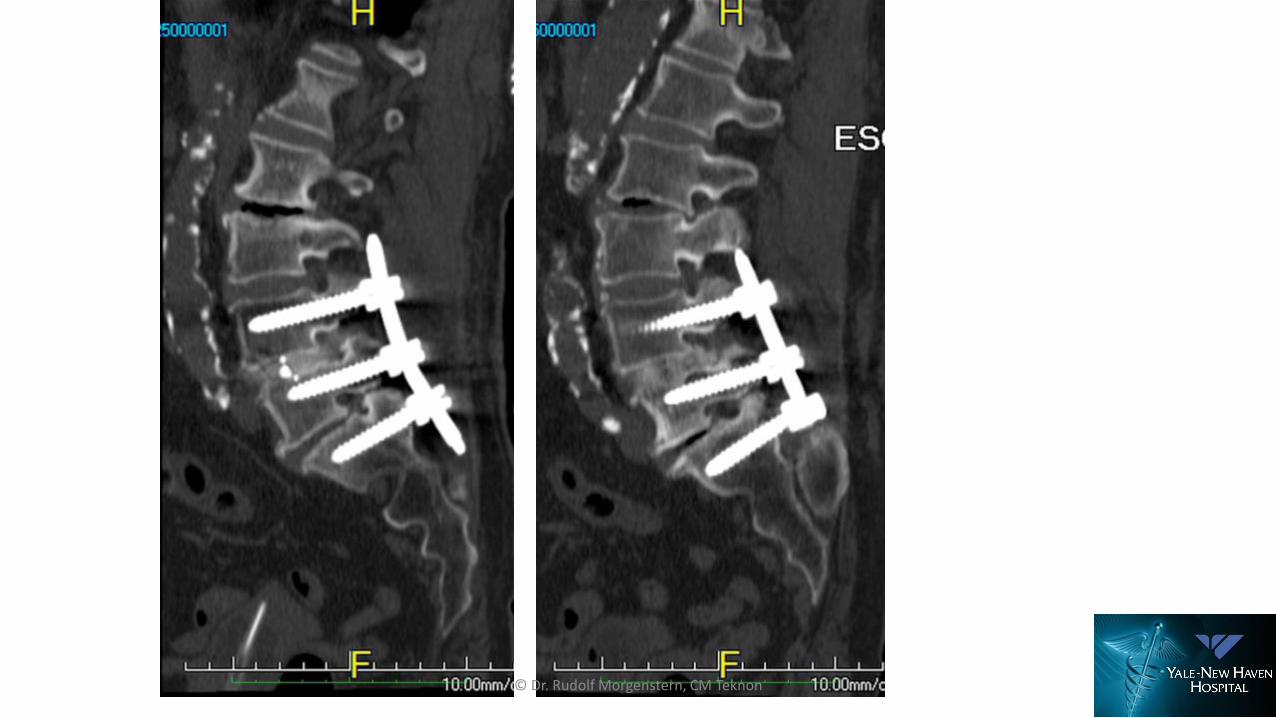
Expanded Opticage
© Dr. Rudolf Morgenstern, CM Teknon
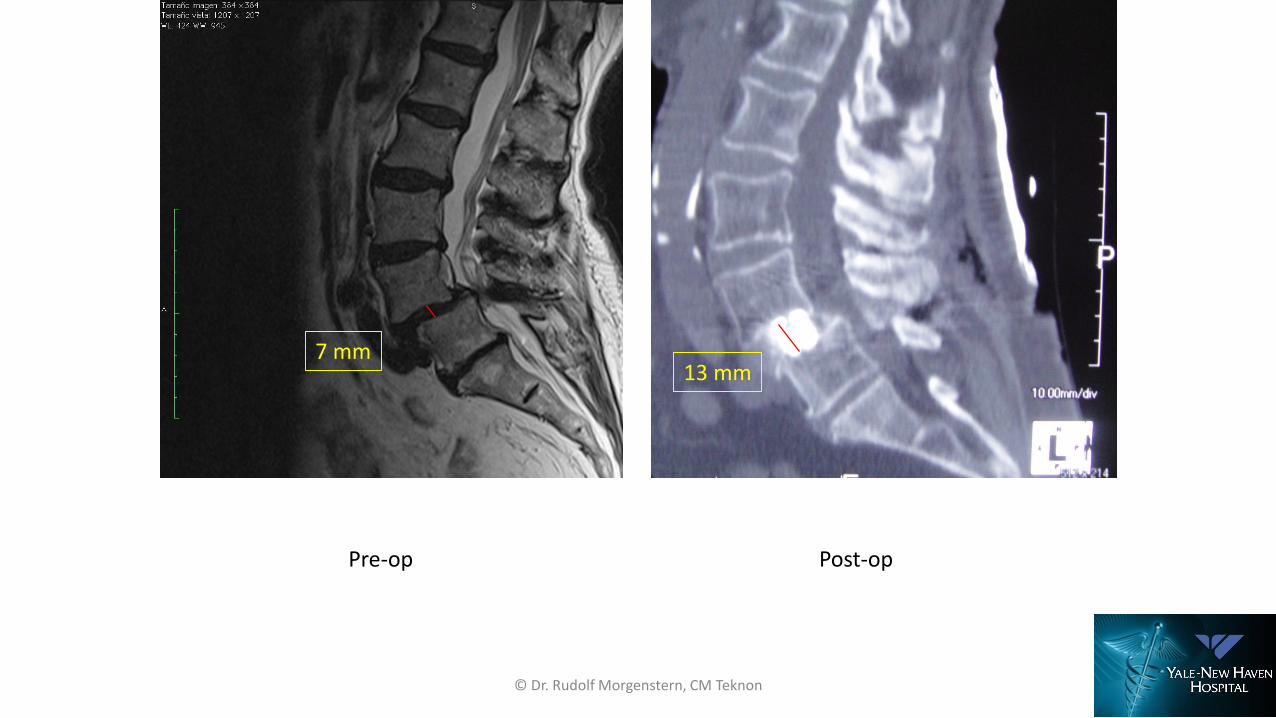
7 mm13 mm
Pre-op Post-op
© Dr. Rudolf Morgenstern, CM Teknon
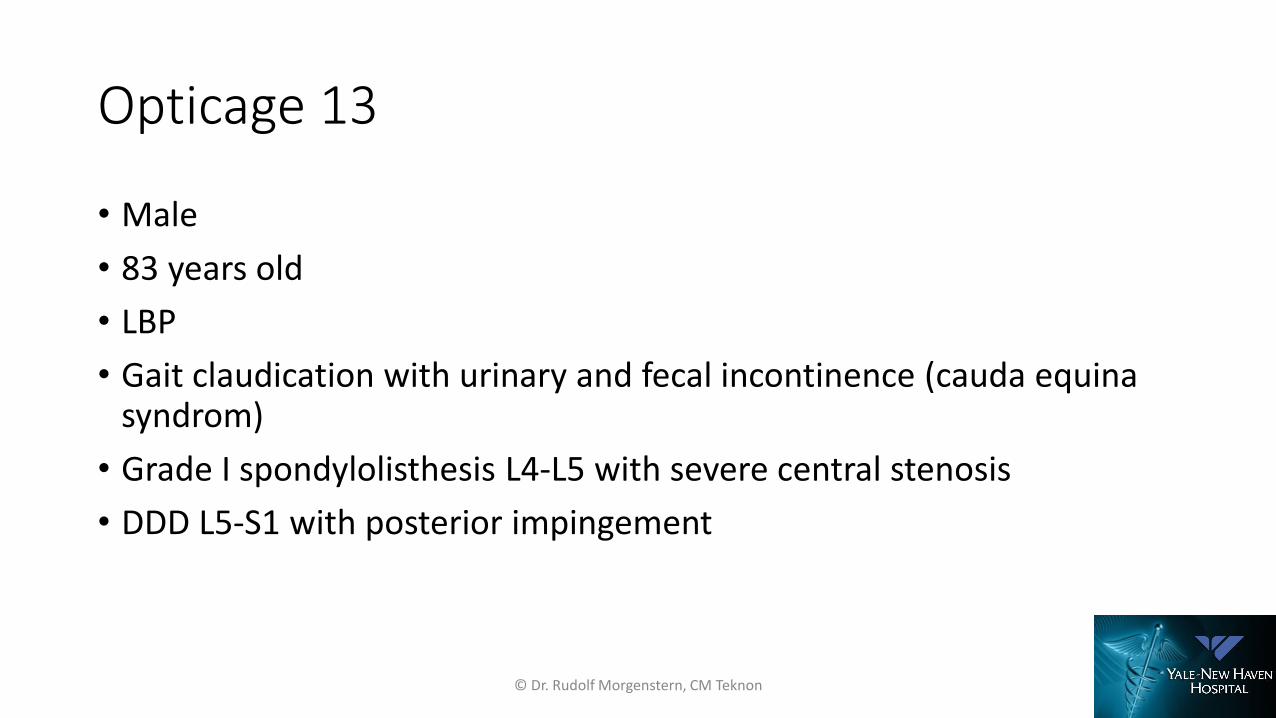
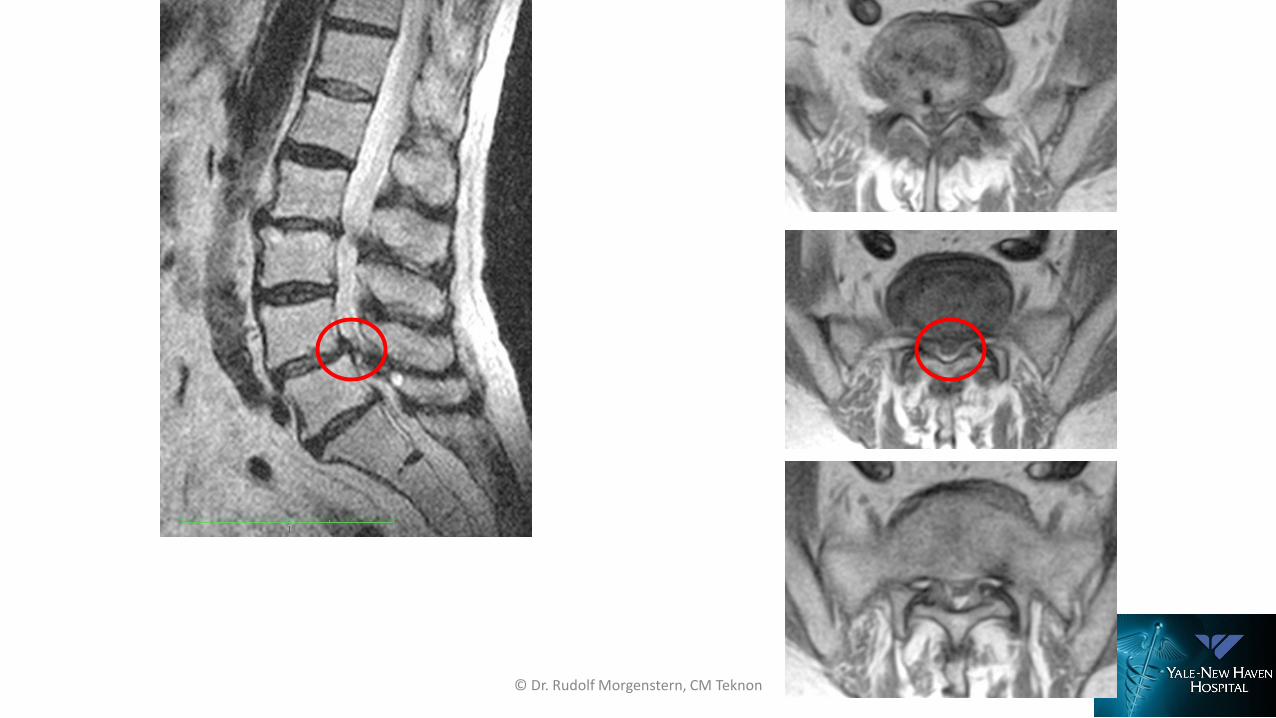
Opticage 13
• Male
• 83 years old
• LBP
• Gait claudication with urinary and fecal incontinence (cauda equina syndrom)
• Grade I spondylolisthesis L4-L5 with severe central stenosis
• DDD L5-S1 with posterior impingement
© Dr. Rudolf Morgenstern, CM Teknon
© Dr. Rudolf Morgenstern, CM Teknon
© Dr. Rudolf Morgenstern, CM Teknon
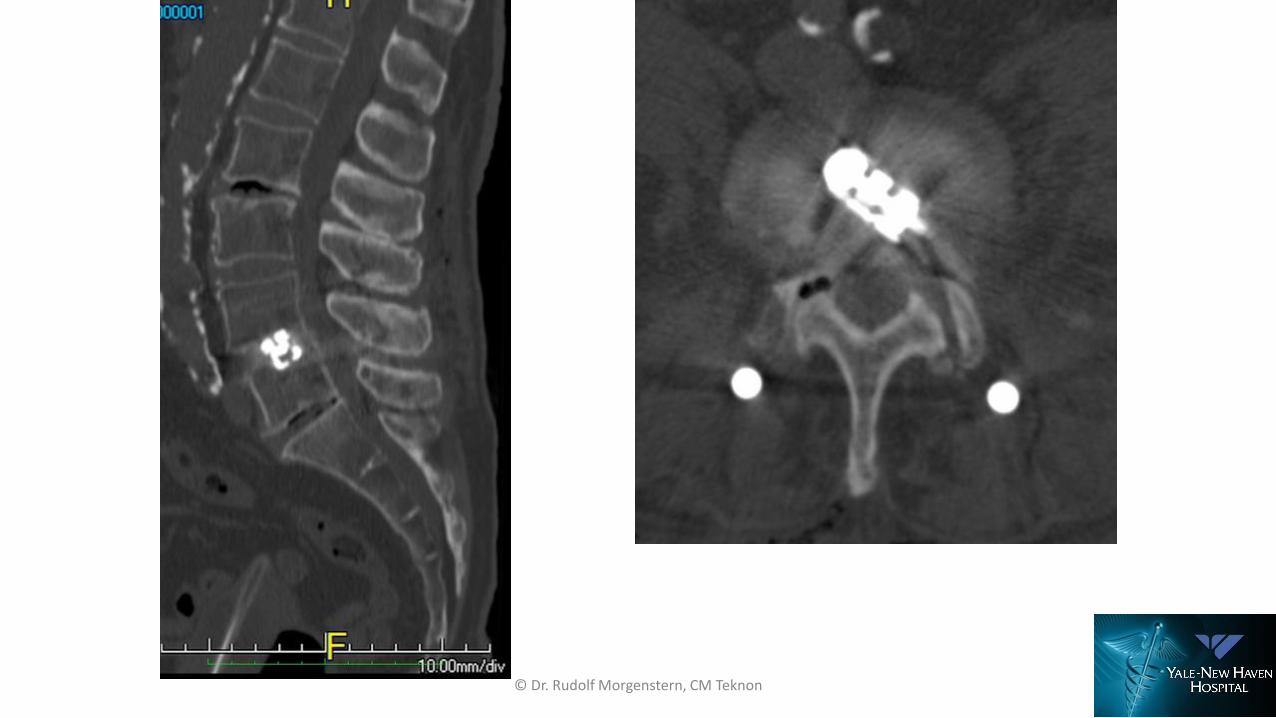
© Dr. Rudolf Morgenstern, CM Teknon
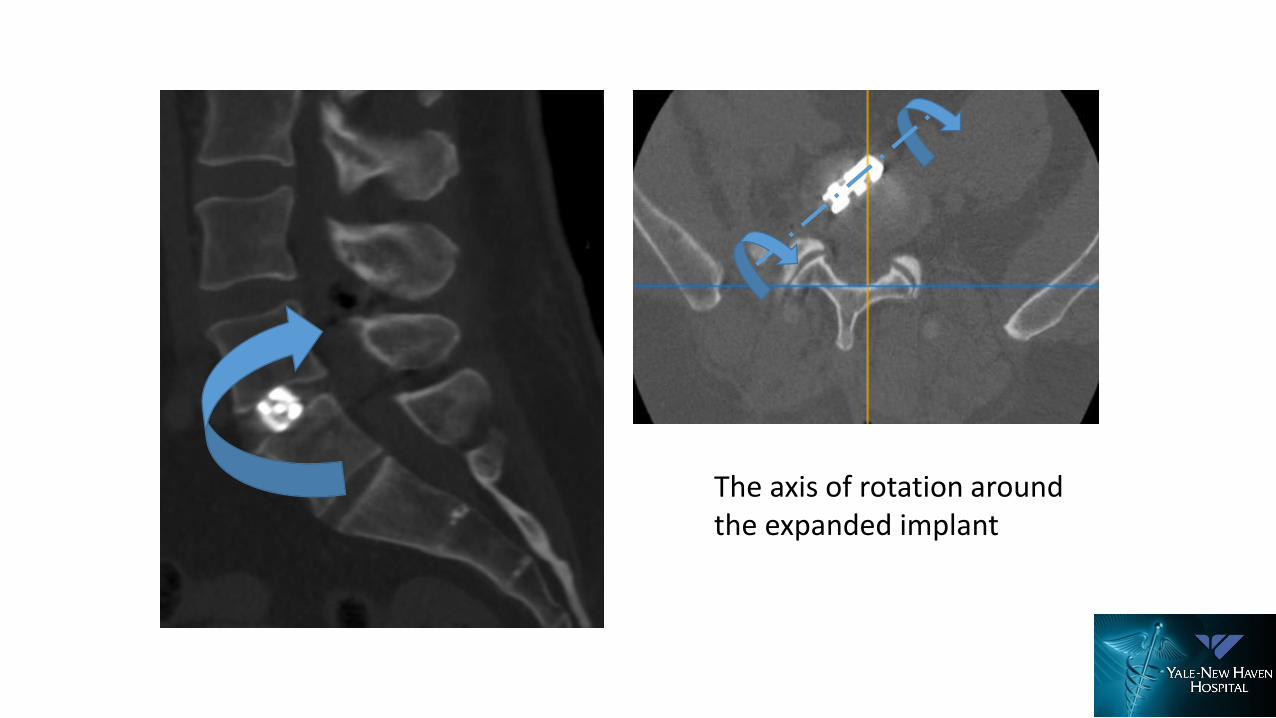
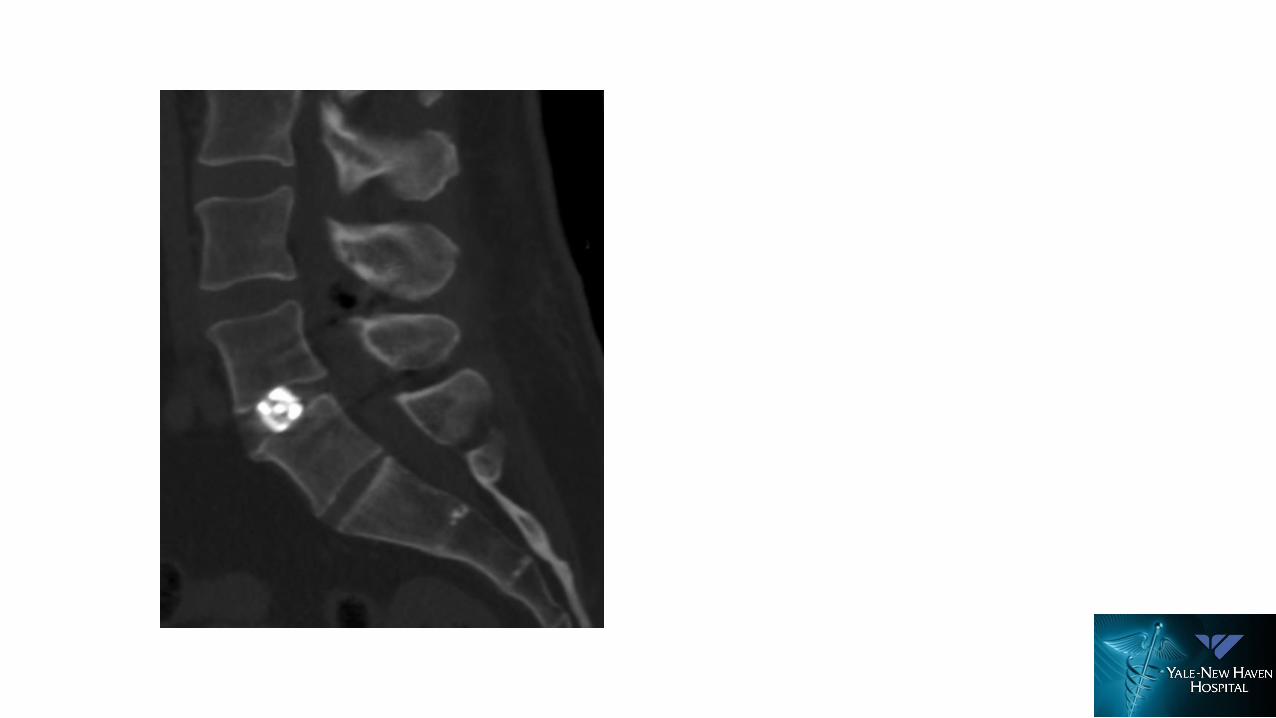
The axis of rotation aroundthe expanded implant

allows only one degree of freedom

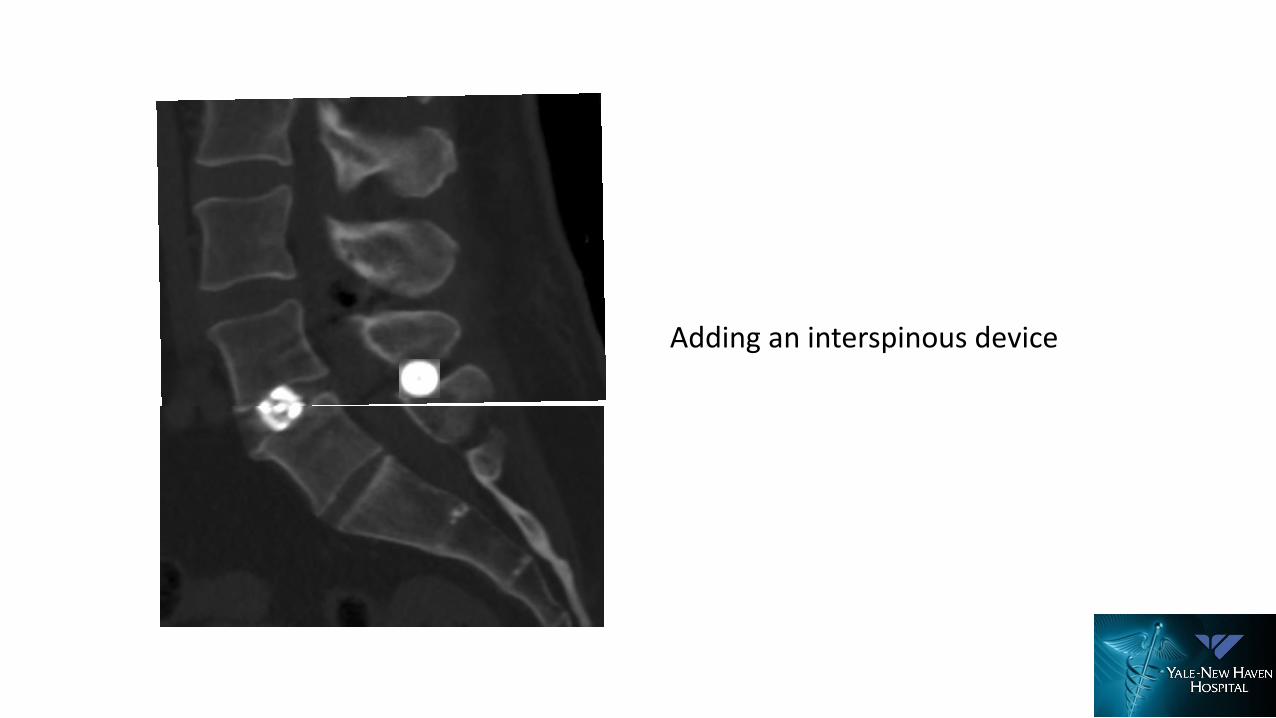
Adding an interspinous device
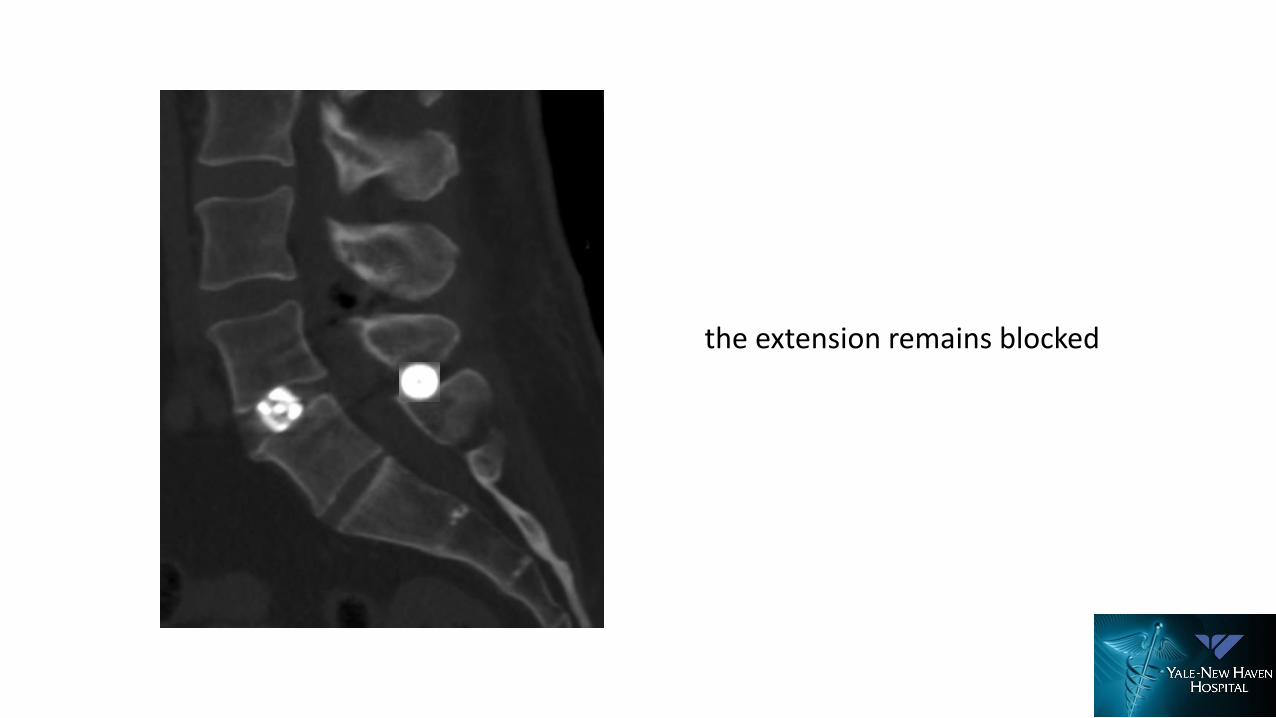
the extension remains blocked
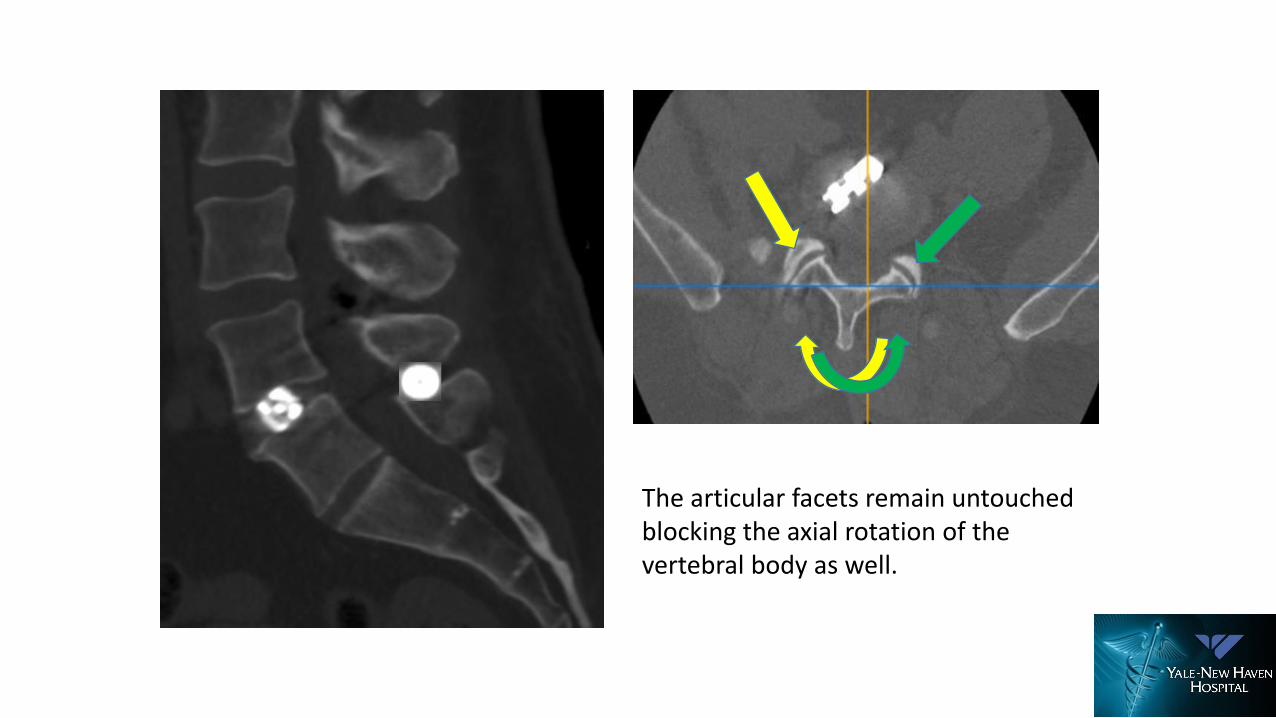
The articular facets remain untouchedblocking the axial rotation of thevertebral body as well.
Concept of Indirect Decompression of Neural Elements
• Disc Height : Mid 90’s BAK Cages Increased Posterior Disc Height 29% at L4-5 and 33.6% at L5-S1
• Foraminal Surface Area: Increased 23% at L4-5 and 22% at L5-S1
Thank You!
Anthony YeungSebastian Reutten
Rudolf Morgenstern