the extremity screen manual: a guide to the … · a guide to the subjective and objective outcomes...
TRANSCRIPT

THE EXTREMITY
SCREEN MANUAL:
A Guide to the Subjective and Objective
Outcomes Assessment of the Upper and
Lower Extremity
Steven G. Yeomans, DC, FACO

INTRODUCTION: • Objective screen for the extremities (ROM using a goniometer)
• To track patient progress
• Couple with the subjective OATs
• Refer to the Extremity Physical Exercise Manual for the exercise options

Joint Range of Motion (ROM)
• Joint flexibility measured with a 2-arm goniometer

Joint Range of Motion (ROM)
• Place in goniometer in the correct plane (frontal, sagittal, or transverse)

Frontal Plane (F)
• Abduction
• Adduction

Sagittal Plane (S)
Flexion Extension
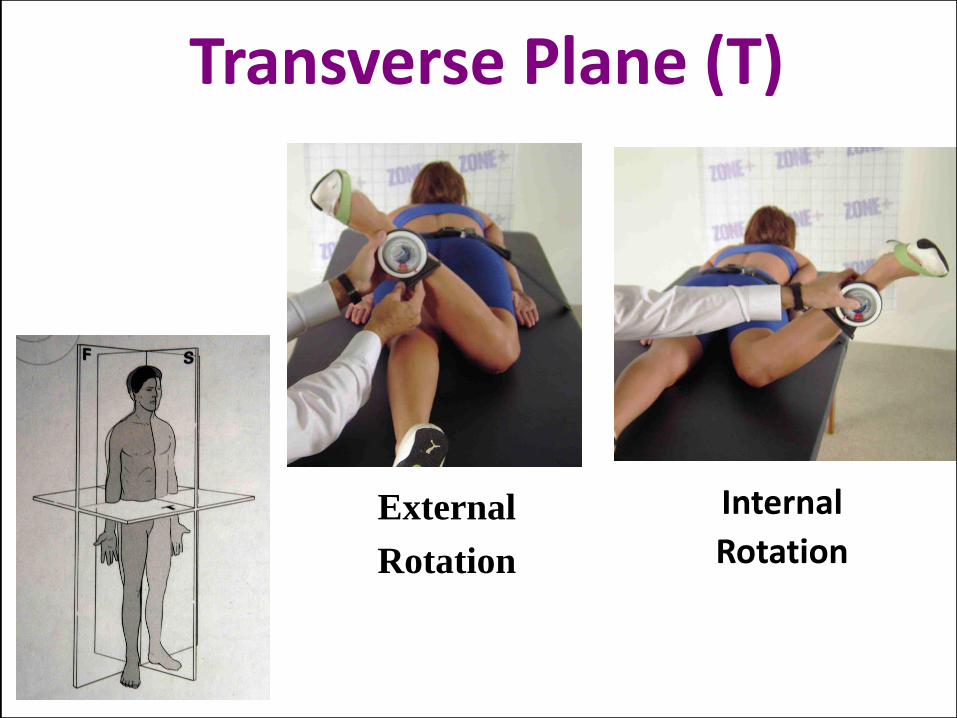
Transverse Plane (T)
Internal
Rotation External
Rotation

Joint Range of Motion (ROM)
• Place the pivot at the joint level

Joint Range of Motion (ROM)
• Active ROM is measured to the end-point and reported.
• Active motion is the patient's movement of the joint
through a specified ROM.
• Passive motion is the examiner's movement of the
extremity/joint through a specified ROM.

PURPOSE
(EXTREMITY ROM SCREEN)
• To practice screening the ROMs of the major joints of the body using a double-armed goniometer.
• Students need to memorize the ROM terminology used to describe different joint motions allowed at the major joints of the body.

PROCEDURES
(Shoulder)
• Three Planes of ROM
– Frontal Plane: Abduction
• If requested measure ROM the scapula 1st moves

PROCEDURES
(Shoulder)
• Three Planes of ROM
– Frontal Plane: Adduction / Adduction
Abduction: 180 Adduction: 50

PROCEDURES
(Shoulder)
• Three Planes of ROM
– Transverse Plane: Internal / External Rotation
External Rotation: 90 Internal Rotation: 90

PROCEDURES
(Shoulder)
• Three Planes of ROM
– Sagittal Plane: Flexion / Extension
Forward Flexion: 180 Extension: 60

Shoulder Hoppenfeld[i] AMA[ii]
Guides
Magee[iii]
[AROM]
Matsen, et al[iv]
[81 normal subjects
60-70 years]
Souza[v] Kapandji[vi]
Abduction 180 180 170-180 M: 160 8
F: 167 7 180 180
Adduction 45 50 50-75 75 30-45
Flexion 90 180 160-180 180 180
Extension 45 50 50-60 60 45-50
Internal
[medial] rotation
55 90 60-100 M: reach to T6
2
F: reach to T5
2
80 with arm at side
50 with arm
abducted
95
External
[lateral] rotation
40-45 90 80-90 M: 72 13
F: 78 15
60 with arm at side
50 with arm
abducted
80
Elevation through
the plane of the
scapula
170-180 170-180
Horizontal
adduction/
Abduction
130 130
Circumduction 200
* From text: The Clinical Application of Outcomes Assessment. ED SG Yeomans. Appleton & Lange, 2000.

PROCEDURES
(ELBOW)
• Two Planes of ROM
– Sagittal Plane: Flexion / Extension
Extension: 0 Flexion 150

PROCEDURES
(ELBOW)
• Two Planes of ROM
– Transverse Plane: Pronation & Supination
Pronation: 90 Supination: 90

From: Clin Applic of OATs, Chapter 15, pg 249, Table 15-9. Elbow ROM from various sources*
Elbow
Hoppenfeld AMA
Guides
Magee
[AROM]
Ombregt, et
al[i]. [PROM]
Kapandji Morrey Evans[ii]
Flexion 135+ 140 140-150 160 AROM: 145
PROM: 160 145 140-150
Extension 0 to –5 0 0 to 10 0 to 10 0 normal
5 to 10 in
subjects with
great laxity of
ligaments
0 0 normal up to 10 of
hyperextensio
n may be seen
especially in
women.
Supination 90 80 90 90 90 85 90
Pronation 90 80 80-90 85 85 75 80-90

PROCEDURES
(WRIST)
• Two Planes of ROM
– Sagittal Plane: Flexion / Extension
(Palmar Flexion / Dorsiflexion)
Dorsiflexion: 70 Palmar Flexion: 80

PROCEDURES
(WRIST)
• Two Planes of ROM
– Frontal Plane: Ulnar and Radial Deviation
Ulnar Deviation: 30 Radial Deviation 20

From: Clin Applic of OATs, Chap. 15, pg 251, Table 15-12. Wrist ROM from various sources*
Wrist
Hoppenfeld AMA
Guides[i]
Magee
[AROM]
Kapandji Evans Gerhardt[ii]
Flexion 80 60 80-90 85 80-90 50
Extension 70 60 70-90 85 70-90 60
Ulnar
deviation 30 30 30-45 45 30-45 20
Radial
deviation 20 20 15 15 15 30

PROCEDURES
(Hip)
• Three Planes of ROM
– Sagittal Plane: Flexion / Extension
Hip Flexion: 130 Extension: 30

PROCEDURES
(Hip)
• Three Planes of ROM
– Frontal Plane: Abduction / Adduction
Abduction: 50 Adduction: 30

PROCEDURES
(Hip)
• Three Planes of ROM
– Transverse Plane: Internal & External Rotation
Internal Rotation: 40 External Rotation: 60

Hip Hoppenfeld Steinberg[i] Magee Ombregt,
et al
[PROM]
Evans Gerhardt
Flexion 120 110 to 120 110-120
135° 140 120 knee flexed;
75-90+ with knee
extended
120
Extension 5-10 20-30
10-15 30 15 normal
30-40 if pelvis is not
adequately fixed
15
Abduction 45-50 40-50 30-50
40-45 45
Abduction
[in flexion]
- 45-60 -
Adduction 20-30 20-40 30 30 20-30 35
Internal
[medial]
rotation
35 25-45
43
30-40 45 40 45
External
[lateral]
rotation
45 45-50
42
40-60 60 45 45
From: Clin Applic of OATs, Chap. 15, pg 251, Table 15-12. Wrist ROM from various sources*

PROCEDURES
(Knee)
• Two Plane of ROM: Sagittal & Transverse
– Sagittal Plane: Flexion & Extension
Knee Extension: 0 Knee Flexion: 148

PROCEDURES
(Knee)
• Two Planes of ROM
– Transverse Plane: Internal & External Rotation
Internal Rotation: 10 External Rotation: 10
?

From: Clin Applic of OATs, Chapter 15, pg 264, Table 15-19. Knee ROM from various sources*
Knee
Hoppenfeld Logan Magee
[AROM]
Evans Scott Gerhardt
Flexion
148
135 120 active
140 with hip flexed
160 passive
0 to 135 130-150 110 0-130
Extension 0 5-10 0 to 15 0-15 10 0-10
Rotation 10 internal
10 external
At 0 flexion:
10 lateral rotation
5 medial rotation
At 100 flexion:
15 lateral rotation
10 medial rotation
At full knee flexion:
0 lateral rotation
10 medial rotation
20-30 medial
rotation of tibia on
femur
30-40 lateral
rotation of tibia on
femur
- - -

PROCEDURES
(Ankle)
• Two Planes of ROM
– Sagittal Plane: Plantar & Dorsiflexion
Plantar flexion: 50 Dorsiflexion: 20

PROCEDURES
(Ankle)
• Two Planes of ROM
– Frontal Plane: Inversion & Eversion
Inversion: 35 Eversion: 15

From: Clin Applic of OATs, Chapter 15, pg 270, Table 15-23. Ankle ROM from various sources*
Ankle
Hoppenfeld Logan Jahss Magee
[AROM]
Ombregt, et al Evans
Dorsiflexion 20 20 To an angle of 90
with the knee
extended
20 Angle between dorsum
of the foot and the tibia
< 90
20
Plantar flexion 50 30-50 Limitation is of
no clinical
significance in the
elderly.
50 Dorsal aspect of foot
falls into line with the
leg.
40
Inversion 35° 5 subtalar - - 30
Eversion 15° 5 subtalar - - 20
Supination 45-60
Pronation 15-30

Summary
• Improving joint flexibility is essential for injury prevention.
• One may increase joint flexibility (range of motion) by regular stretching.
• Table 1 summarizes the average ROMs published. Note the differences between references.

TABLE. 1 Average ROMs (Adapted from Luttgens & Hamilton, 1997)
Joint/Segment Movement Source
1*
Source
2*
Source
3*
Source
4*
Elbow Flexion 150° 140 145 145 145
Hyperextension 0 0 0 0-10
Forearm Pronation 80 90 90 80
Supination 80 85 90 90
Wrist
Extension (Dorsiflexion) 60 70 70 50
Flexion (Palmar flexion) 80° 60 90 - 60
Radial Deviation 20° 20 20 20 20
Ulnar Deviation 30° 30 30 35 30
Shoulder
Flexion 180° 180 170 130 180
Hyperextension 60° 50 30 80 60
Abduction 180° 180 170 180 180
Adduction 75° 50 - - -
Shoulder
w/ Abducted Arm
Internal Rotation 90° 90 90 70 60-90
External Rotation 90° 90 90 70 90
Horizontal Adduction NA - - - 135
Horizontal Adduction NA - - - 45

TABLE. 1 Average ROMs (Adapted from Luttgens & Hamilton, 1997) (Continued)
Hip
Flexion 135° 100 120 125 120
Hyperextension 30 10 10 30
Abduction 50° 40 45 45 45
Adduction 30° 20 - 10 0-25
Extended Hip Internal Rotation 40 35 45 40-45
External Rotation 50 45 45 45
Knee Flexion 135° 150 120 140 130
Ankle Plantar flexion 50° 20 45 45 50
Dorsiflexion 30 15 20 20
Joint/Segment Movement Source 1* Source 2* Source 3* Source 4*

If manual muscle testing is utilized as part of the screen, the
following table defines the classic definitions of each grade
(reported as ____ / 5; example = 4/5)
Table 15-1: Muscle Strength Testing Grades (0-5/5 scale).
Numerical
grade
Description
0 Zero: No contraction
1 Trace: Muscle palpably tightens, but does not move the joint
2 Poor: Joint movement is produced only with gravity eliminated
3 Fair: Ability to produce joint movement against gravity only
4 Good: Full contraction, producing joint movement against some external resistance
5 Normal: Full contraction, producing joint movement against external resistance
without notable fatigue
* From text: The Clinical Application of Outcomes Assessment. ED SG Yeomans. Appleton & Lange, 2000.
NOT THE CT’s JOB!

Upper Extremity Functional Index Name________________________________ Date__________DOI__________ (Key: LEFT/RIGHT)
We are interested in knowing whether you are having any difficulty at all with the activities listed below because of your
upper limb problem for which you are currently seeking attention. Please check (√) an answer for each activity.
Today, do you or would you have any difficulty at all with:

Upper Extremity Functional Index (Continued)

Upper Extremity Functional Index (Continued)
Stratford PW, Binkley JM, Stratford DM. Development and initial validation of the upper
extremity functional index. Physiotherapy Canada Fall 2001;259-266.
Score /80 MDC (minimum detectable change) = 9 pts /15% Error +/- 5 scale points

Upper Extremity Functional Index (Continued)
• Scoring Method – FORMULA: PT Score / TOTAL possible (80) TIMES
(X) 100 = ______%
– EXAMPLE: 43 / 80 = .56 x 100 = 56%

2: Use IF previously treated:
Patient’s Global Impression of Change (PGIC) (Bolton, et al):
Since beginning treatment at this clinic, how would you describe the change (if
any) in ACTIVITY LIMITATIONS, SYMPTOMS, EMOTIONS, and OVERALL
QUALITY OF LIFE, related to your painful condition? (Circle one number):
Much Better No Change Much Worse
______________________________________________________________________
0 1 2 3 4 5 6 7 8 9 10
SCORE: 0-2/10 = A meaningful, satisfying change
Hurst H, Bolton J. Assessing the clinical significance of change scores recorded on subjective
outcome measures. J Manipulative Physiol Ther 2004;27:26-35

3) Pain Level (QVAS):
Right Now: _______ / 10
Usual / Typical: _______ / 10
At Best: _______ / 10
At Worst: _______ / 10
Quadruple Visual Analogue Scale (QVAS)
Spine, 18, Von Korff M, Deyo RA, Cherkin D, Barlow SF, Back pain in primary care:
Outcomes at 1 year, 855-862, 1993, with permission from Elsevier Science.

FOR OFFICE USE ONLY:
4) ROM (active, active assisted and/or passive) (visual, goniometer, inclinometer, other:_____)

ELBOW RANGE OF MOTION TABLE

WRIST RANGE OF MOTION TABLE

NEUROLOGICAL EXAMINATION

Lower Extremity Functional Scale Name________________________________ Date__________DOI__________ (Key: LEFT/RIGHT)
We are interested in knowing whether you are having any difficulty at all with the activities listed below because
of your lower limb problem for which you are currently seeking attention. Please check (√) an answer for each activity.
Today, do you or would you have any difficulty at all with:
4 3 2 1 0

Lower Extremity Functional Index (Continued)

Binkley JM, Stratford POW, Lott SA, Riddle DL. The lower extremity functional scale (LEFS): Scale development, measurement
properties, and clinical application. Physical Therapy 1999;79:371-383.
Score /80 MDC (minimum detectable change) = 9 pts / 15 Error +/- 5 scale points
Lower Extremity Functional Index (Continued)

Lower Extremity Functional Scale (Continued)
• Scoring Method – FORMULA: PT Score / TOTAL possible (80) TIMES
(X) 100 = ______%
– EXAMPLE: 43 / 80 = .56 x 100 = 56%

2: Use IF previously treated:
Patient’s Global Impression of Change (PGIC) (Bolton, et al):
Since beginning treatment at this clinic, how would you describe the change (if
any) in ACTIVITY LIMITATIONS, SYMPTOMS, EMOTIONS, and OVERALL
QUALITY OF LIFE, related to your painful condition? (Circle one number):
Much Better No Change Much Worse
______________________________________________________________________
0 1 2 3 4 5 6 7 8 9 10
SCORE: 0-2/10 = A meaningful, satisfying change
Hurst H, Bolton J. Assessing the clinical significance of change scores recorded on subjective
outcome measures. J Manipulative Physiol Ther 2004;27:26-35

3) Pain Level (QVAS):
Right Now: _______ / 10
Usual / Typical: _______ / 10
At Best: _______ / 10
At Worst: _______ / 10
Quadruple Visual Analogue Scale (QVAS)
Spine, 18, Von Korff M, Deyo RA, Cherkin D, Barlow SF, Back pain in primary care:
Outcomes at 1 year, 855-862, 1993, with permission from Elsevier Science.

4) ROM (active, active assisted and/or passive) (visual, goniometer, inclinometer, other:______________)
HIP – Range of Motion

KNEE – Range of Motion

ANKLE – Range of Motion

NEUROLOGICAL EXAMINATION
NOT THE CT’s JOB!
• Screening procedures – range of motion (ROM) utilizing a
goniometer to measure the range of motion of the peripheral
joints
• Objective method of tracking progress of patients during the
active care/physical exercise portion of case management
• Subjective outcomes assessment tools located on pages 16 and
18 (upper and lower extremity, respectively), track activity
tolerance
CONCLUDING REMARKS

• Use BOTH the subjective and objective outcome measures
regardless of the clinical diagnosis or specific functional loss
• Use the ROM screen when assessing patients before the
initiation of active care/physical exercise
•Use the Extremity Physical Exercise Manual when utilizing
active care with patients in the clinical setting
CONCLUDING REMARKS
