the greater toronto area obstetric network
TRANSCRIPT
2/9/2015
1
Arthur Zaltz MD, FRCSC
Obstetrician and Gynecologist in Chief
Chief of the Women’s and Babies Program
Sunnybrook Health Sciences Centre
Toronto, Ontario
� The Beginning: Formation of Canada’s first obstetric
network
� GTA–OBS Network Terms of Reference
� Three pillars of our Network
� Network’s output and measures
◦ Dashboard
◦ Protocol
◦ Communication
◦ Research Projects
◦ October 29, 2013, 33 people from across the GTA came together
◦ Explored the possibility of integrating the TAHSN* and GTA-wide hospitals in a research network which would focus on establishing evidence-based best practice guidelines
*Toronto Academic Health Science Network
The GTA-OBS Network will aim to become an international leader in research, best practices and advocacy in women’s and infant’s health by leveraging the power inherent in its GTA-wide
collaborative approach
� Improve quality and standards of care: ◦ Create and implement shared standards and guidelines to improve patient-
centered quality of care and, ultimately, the longitudinal health of women and babies across the region.
� Conduct clinical research: ◦ Initiate randomized controlled trials and studies that leverage existing
databases (BORN, ICES, CNN), serving as a forum for discussion of our common research questions
� Develop a shared advocacy: ◦ Influence and drive changes in policy related to women’s and infants’ health
locally, nationally, and internationally
� Promote knowledge sharing: ◦ Foster professional and practice development among all members
2/9/2015
2
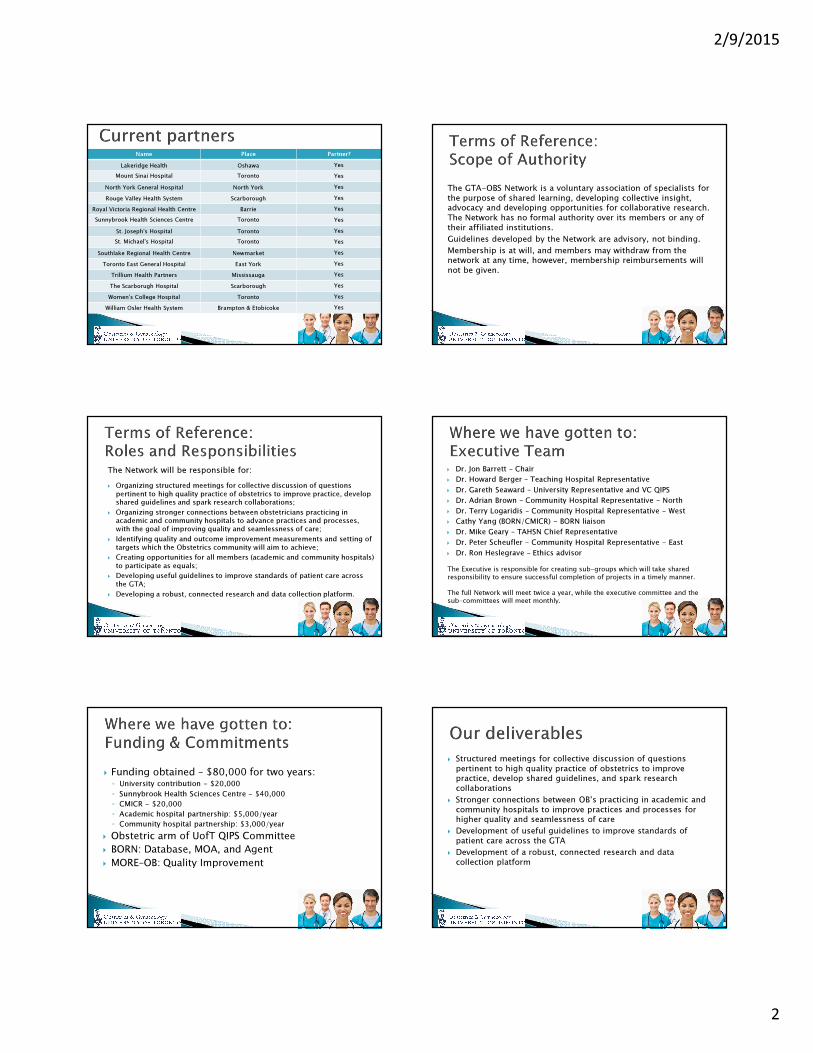
Name Place Partner?
Lakeridge Health Oshawa Yes
Mount Sinai Hospital Toronto Yes
North York General Hospital North York Yes
Rouge Valley Health System Scarborough Yes
Royal Victoria Regional Health Centre Barrie Yes
Sunnybrook Health Sciences Centre Toronto Yes
St. Joseph's Hospital Toronto Yes
St. Michael's Hospital Toronto Yes
Southlake Regional Health Centre Newmarket Yes
Toronto East General Hospital East York Yes
Trillium Health Partners Mississauga Yes
The Scarborugh Hospital Scarborough Yes
Women's College Hospital Toronto Yes
William Osler Health System Brampton & Etobicoke Yes
The GTA-OBS Network is a voluntary association of specialists for
the purpose of shared learning, developing collective insight, advocacy and developing opportunities for collaborative research.
The Network has no formal authority over its members or any of
their affiliated institutions.
Guidelines developed by the Network are advisory, not binding.
Membership is at will, and members may withdraw from the network at any time, however, membership reimbursements will
not be given.
The Network will be responsible for:
� Organizing structured meetings for collective discussion of questions
pertinent to high quality practice of obstetrics to improve practice, develop shared guidelines and spark research collaborations;
� Organizing stronger connections between obstetricians practicing in academic and community hospitals to advance practices and processes, with the goal of improving quality and seamlessness of care;
� Identifying quality and outcome improvement measurements and setting of
targets which the Obstetrics community will aim to achieve;
� Creating opportunities for all members (academic and community hospitals)
to participate as equals;
� Developing useful guidelines to improve standards of patient care across
the GTA;
� Developing a robust, connected research and data collection platform.
� Dr. Jon Barrett – Chair
� Dr. Howard Berger – Teaching Hospital Representative
� Dr. Gareth Seaward – University Representative and VC QIPS
� Dr. Adrian Brown – Community Hospital Representative - North
� Dr. Terry Logaridis – Community Hospital Representative - West
� Cathy Yang (BORN/CMICR) - BORN liaison
� Dr. Mike Geary – TAHSN Chief Representative
� Dr. Peter Scheufler - Community Hospital Representative - East
� Dr. Ron Heslegrave – Ethics advisor
The Executive is responsible for creating sub-groups which will take shared
responsibility to ensure successful completion of projects in a timely manner.
The full Network will meet twice a year, while the executive committee and the
sub-committees will meet monthly.
� Funding obtained – $80,000 for two years: ◦ University contribution - $20,000
◦ Sunnybrook Health Sciences Centre - $40,000
◦ CMICR - $20,000
◦ Academic hospital partnership: $5,000/year
◦ Community hospital partnership: $3,000/year
� Obstetric arm of UofT QIPS Committee
� BORN: Database, MOA, and Agent
� MORE–OB: Quality Improvement
� Structured meetings for collective discussion of questions
pertinent to high quality practice of obstetrics to improve practice, develop shared guidelines, and spark research
collaborations
� Stronger connections between OB’s practicing in academic and
community hospitals to improve practices and processes for higher quality and seamlessness of care
� Development of useful guidelines to improve standards of
patient care across the GTA
� Development of a robust, connected research and data
collection platform
2/9/2015
3
When you are content to be simply yourself and don’t compare or compete, everyone will respect you.” - Lao Tzu
“If you do tomorrow what you did today, you will get tomorrow what you got today.” – Benjamin Franklin
I am thankful for all of those who said NO to me. It’s because of them I’m doing it myself.” –Albert Einstein
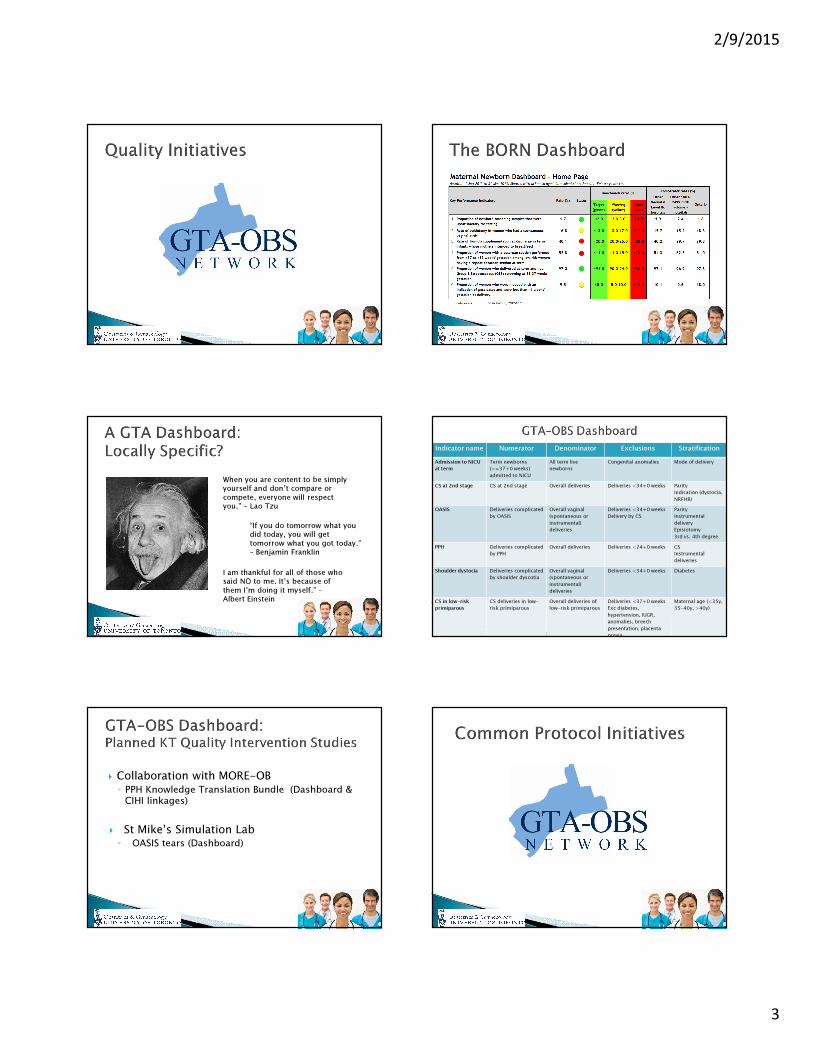
Indicator name Numerator Denominator Exclusions Stratification
Admission to NICU
at term
Term newborns
(>=37+0 weeks)
admitted to NICU
All term live
newborns
Congenital anomalies Mode of delivery
CS at 2nd stage CS at 2nd stage Overall deliveries Deliveries <34+0 weeks Parity
Indication (dystocia,
NRFHR)
OASIS Deliveries complicated
by OASIS
Overall vaginal
(spontaneous or
instrumental)
deliveries
Deliveries <34+0 weeks
Delivery by CS
Parity
Instrumental
delivery
Episiotomy
3rd vs. 4th degree
PPH Deliveries complicated
by PPH
Overall deliveries Deliveries <24+0 weeks CS
Instrumental
deliveries
Shoulder dystocia Deliveries complicated
by shoulder dyscotia
Overall vaginal
(spontaneous or
instrumental)
deliveries
Deliveries <34+0 weeks Diabetes
CS in low-risk
primiparous
CS deliveries in low-
risk primiparous
Overall deliveries of
low-risk primiparous
Deliveries <37+0 weeks
Exc diabetes,
hypertension, IUGR,
anomalies, breech
presentation, placenta
previa
Maternal age (<35y,
35-40y, >40y)
� Collaboration with MORE-OB◦ PPH Knowledge Translation Bundle (Dashboard &
CIHI linkages)
� St Mike’s Simulation Lab◦ OASIS tears (Dashboard)
2/9/2015
4
� Step 1: Survey ✔
� Step 2: Analysis of common ground ✔
� Step 3: Proposal of a common protocol ✔
� Step 4: Ratification (February, 2015)
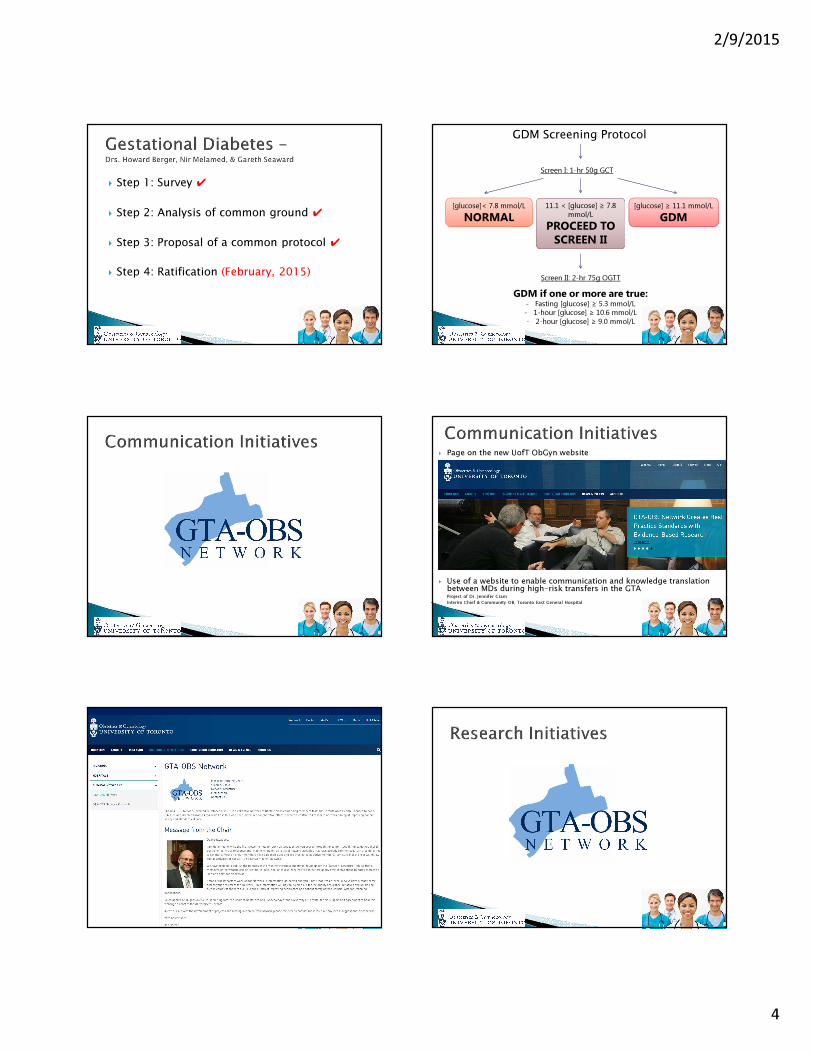
Screen I: 1-hr 50g GCT
Screen II: 2-hr 75g OGTT
GDM if one or more are true:- Fasting [glucose] ≥ 5.3 mmol/L
- 1-hour [glucose] ≥ 10.6 mmol/L- 2-hour [glucose] ≥ 9.0 mmol/L
[glucose]< 7.8 mmol/L
NORMAL
11.1 < [glucose] ≥ 7.8 mmol/L
PROCEED TO
SCREEN II
GDM Screening Protocol
[glucose] ≥ 11.1 mmol/L
GDM
� Page on the new UofT ObGyn website
� Use of a website to enable communication and knowledge translation between MDs during high-risk transfers in the GTAProject of Dr. Jennifer Cram
Interim Chief & Community OB, Toronto East General Hospital
2/9/2015
5
� Retrospective data analysis on outcomes following GDM within the GTA - Drs. Howard Berger & Nir Melamed ◦ In progress: data exchange with BORN-Ontario
� RCT on induction of labour with large size foley vs PG -Dr. Anne Berndl◦ Project submitted: awaiting funding
� RCT on low pressure wound device –collaboration with Dr. Greg Davies, Queen’s University
� RCT on use of anti-TNF drugs in APLA women - Dr. Carl Laskin
� Secure funding platform
� GTA–OBS Network Representative in each partnered site
� Prospective studies: collect outcome data in ongoing studies and RTCs
� Wider linkages outside of the GTA