the history and development of self-ligating
DESCRIPTION
self ligation in orthodonticsTRANSCRIPT

TBN
Iarpttt
B
ROMb
he History and Development of Self-Ligatingracketsigel Harradine
Self-ligating brackets do not require an elastic or wire ligature, but have an
inbuilt mechanism that can be opened and closed to secure the archwire. In
the overwhelming majority of designs, this mechanism is a metal face to the
bracket slot that is opened and closed with an instrument or fingertip.
Brackets of this type have existed for a surprisingly long time in orthodon-
tics—the Russell Lock edgewise attachment being described by Stolzenberg
in 1935. Many designs have been patented, although only a minority have
become commercially available. In addition, there are lingual self-ligation
brackets, and in general terms, the same challenges and potential differ-
ences apply on the lingual surface. Specific comparison of some types of
lingual self-ligating brackets can be found in the article by Silvia Geron in
this issue. New designs have continued to appear, the Time bracket (Adenta
GmbH, Gliching, Germany) becoming available in 1994, the Damon SL
bracket (“A” Company, San Diégo, CA) in 1996,5,6 and the TwinLock bracket
(Ormco Corp., Orange, CA) in 1998, being three designs from that decade.
Since the turn of the century, the pace of development has greatly acceler-
ated with the launch of at least 13 new brackets and rapidly increasing sales
for such brackets. This article aims to outline the history and development
of this type of bracket and to put the current situation in context. The
generic advantages claimed for these brackets will be described. In addition,
the problems encountered with various bracket types will be discussed to
provide a summary of why, despite these claimed advantages, self-ligation
has for so long and until so recently been a small part of orthodontics.
(Semin Orthod 2008;14:5-18.) © 2008 Elsevier Inc. All rights reserved.
ameabwpptpess
P
T
t is more than 70 years since Stolzenberg1
described a self-ligating edgewise bracketnd the recent proliferation of bracket typesepresents a minority of the types that have beenatented since that time.2-4 Table 1 is not exhaus-
ive, but contains a majority of the bracket typeshat have been available for clinical use. Severalypes appeared in the 1980s, the Damon SL5,6 was
Orthodontic Department, University of Bristol Dental School,ristol, U.K.
Address correspondence to Nigel Harradine, BDS London, FDS,CS Edin, FDS, MOrth, RCS, Eng, MSc(Orth), MB, BS London,rthodontic Department, University of Bristol Dental School, Upperaudlin Street, Bristol, BS1 2LY, U.K. E-mail: Nigel.Harradine@
ristol.ac.uk© 2008 Elsevier Inc. All rights reserved.1073-8746/08/1401-0$30.00/0
wdoi:10.1053/j.sodo.2007.12.002
Seminars in Orthodontics, Vol 14, N
significant introduction in the 1990s and theore recent proliferation of bracket types is appar-
nt in this table. A core intention throughout thisrticle is to clarify which assertions about theserackets are based on reasonably firm evidence,hich seem probable in the light of rather incom-lete evidence, and which ideas are currently hy-otheses in need of formal investigation. It is fair
o say that, as with several popular orthodonticroducts such as preadjusted brackets and super-lastic wires, the clinical popularity of self-ligatingystems has run ahead of the evidence to firmlyupport all the proposed advantages.
roperties of an Ideal Ligation System
he concept that brackets are ligated via tie
ings is so prevalent that it is worthwhile consid-5o 1 (March), 2008: pp 5-18
esacl
●
●
●
●
●
●
●
Btmt
S
Ittwenw
F
Ieweimqetns“t
L
Wtfalmsttdwioctbfmo
T
Ft
6 N. Harradine
ring a list of ideal properties of any ligationystem. This exercise puts in perspective anyssessment of the benefits and difficulties withurrent self-ligating systems. In this authors view,igation should:
Be secure and robust,Ensure full bracket engagement of the arch-wire,Exhibit low friction between bracket and arch-wire,Be quick and easy to use,Permit easy attachment of elastic chain,Assist good oral hygiene, andBe comfortable for the patient.
efore looking at self-ligating brackets in relationo this list, it is instructive to consider the perfor-
ance of conventional wire and elastomeric liga-ures in relation to these requirements.
ecure Robust Ligation
t is highly desirable that once ligated, the sys-em is very resistant to inadvertent loss of liga-ion. Wire ligatures are good in this respect,hereas elastomeric ligatures are much less so,specially if left for too long without being re-ewed. The force decay of elastomerics has been
able 1. Self-Ligating Bracket Types
Bracket Year
Russell Lock 1935Ormco Edgelok 1972Forestadent Mobil-Lock 1980Forestadent Begg 1980Strite Industries SPEED 1980“A” Company Activa 1986Adenta Time 1996“A” Company Damon SL 1996Ormco TwinLock 1998Ormco/“A” Co. Damon 2 2000GAC In-Ovation 2000Gestenco Oyster 2001GAC In-Ovation R 2002Adenta Evolution LT 2002Ultradent OPAL 2004Ormco Damon 3 20043 M Unitek SmartClip 2004Ormco Damon 3 MX 2005Ultradent OPAL metal 2006Forestadent Quick 2006Lancer Praxis Glide 2006Class 1/Ortho Organisers Carrière LX 2006
ell documented.7 s
ull Bracket Engagement
t is a great advantage if the archwire can be fullyngaged in the bracket slot and maintained thereith certainty. Wire ligatures do not stretch to anxtent that engagement once achieved at ligations subsequently lost, so they can meet this require-
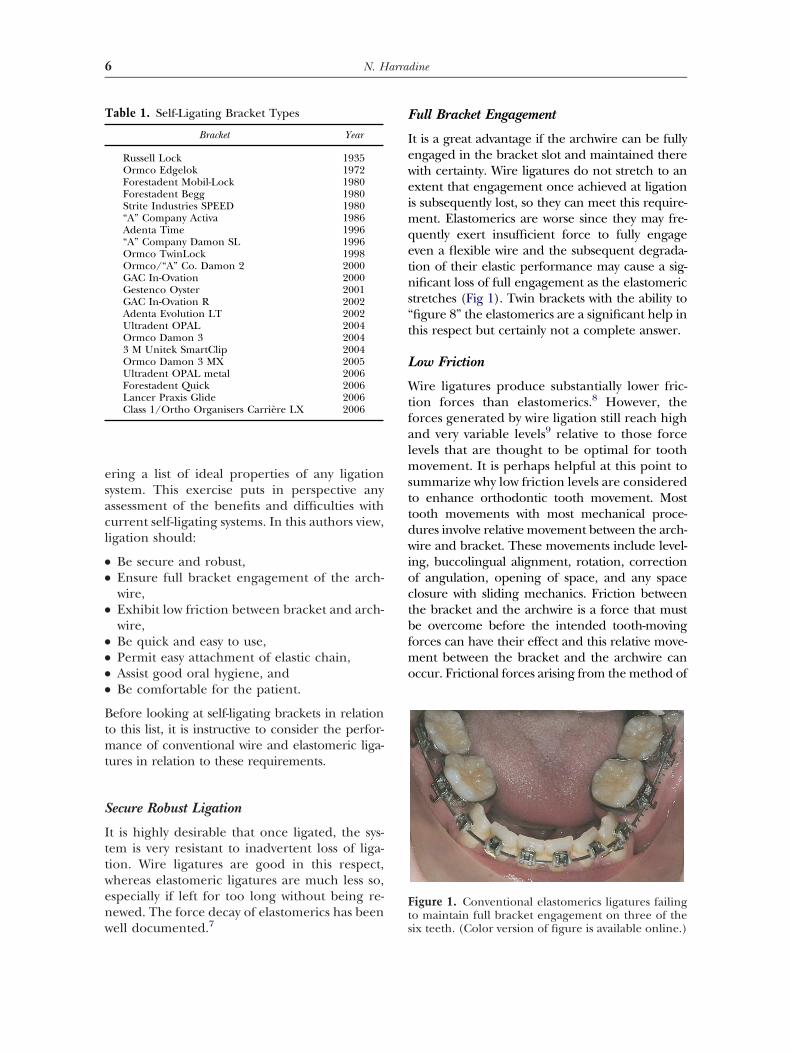
ent. Elastomerics are worse since they may fre-uently exert insufficient force to fully engageven a flexible wire and the subsequent degrada-ion of their elastic performance may cause a sig-ificant loss of full engagement as the elastomerictretches (Fig 1). Twin brackets with the ability tofigure 8” the elastomerics are a significant help inhis respect but certainly not a complete answer.
ow Friction
ire ligatures produce substantially lower fric-ion forces than elastomerics.8 However, theorces generated by wire ligation still reach highnd very variable levels9 relative to those forceevels that are thought to be optimal for tooth
ovement. It is perhaps helpful at this point toummarize why low friction levels are consideredo enhance orthodontic tooth movement. Mostooth movements with most mechanical proce-ures involve relative movement between the arch-ire and bracket. These movements include level-
ng, buccolingual alignment, rotation, correctionf angulation, opening of space, and any spacelosure with sliding mechanics. Friction betweenhe bracket and the archwire is a force that muste overcome before the intended tooth-movingorces can have their effect and this relative move-
ent between the bracket and the archwire canccur. Frictional forces arising from the method of
igure 1. Conventional elastomerics ligatures failingo maintain full bracket engagement on three of the
ix teeth. (Color version of figure is available online.)
lmtpFdusStbfmce(l
Q
TttBlltnTw
E
Cvcwm
M
Iltarctcmlta
aa
C
Eltoa
SL
●
●
●
●
●
●
Eahfisf
PS
●
●
●
●
Tmwciaarot
7Self-Ligation: History and Development
igation are an additional resistance to this relativeovement. Correspondingly higher forces must
herefore be applied and this has two relatedotential effects that inhibit tooth movement.irst, the net effective force is much moreifficult to assess and is more likely to bendesirably higher than force levels bestuited to create the optimal biologic response.econd, the binding forces are higher both be-ween bracket and wire and also at the contactsetween irregular adjacent teeth. These bindingorces also inhibit the required relative move-
ent. Certain tooth movements, such as spacelosure with closing loops placed in the space,xpansion of a well-aligned arch, and torqueinclination) changes are not facilitated by aow-friction method of archwire ligation.
uick and Easy to Use
his is a significant disadvantage of wire liga-ures and the principal reason for the decline inheir use. Maijer and Smith10 and Shivapuja anderger8 have shown that the process of wire
igation is very slow compared with elastomericigature. In the latter study, the use of wire liga-ures added almost 12 minutes to the timeeeded to remove and replace two archwires.his is the major reason for the decreased use ofire ligation.
asy Attachment of Elastic Chain
onventional brackets have tie wings, which areery convenient for the attachment of elastichain. Some self-ligating brackets have dispensedith tie wings. This is less convenient for attach-ent of elastic chain.
aintenance of Optimal Oral Hygiene
t is a prevailing view that elastomerics accumu-ate plaque more than do wire ligatures andhere is some evidence to support this.11 There islso some evidence that the use of wire ligatureseduces bleeding on probing of the gingivalrevice when compared with elastomeric liga-ures.12 However, a scanning electron micros-opy study13 found no difference in bacterialorphotypes when using elastomerics or steel
igatures. The latter area requires further inves-igation; however, current evidence suggests that
reduction in the bacterial challenge through t
n absence of elastomeric ligation is a reason-ble hypothesis.
omfortable for the Patient
lastomerics are good in this respect, but wireigatures require careful tucking in of the endso avoid soft tissue trauma and even then canccasionally be displaced between appointmentsnd cause patient discomfort.
ummary: Frequently Proposedimitations of Conventional Ligation
Failure to provide and to maintain full arch-wire engagement results in poor control oftooth movement.Frictional values are increased.For elastomerics, the force decays and there-fore tooth control is not optimal.Both wire and elastomeric ligatures sometimesbecome displaced.Oral hygiene is potentially impeded.Wire ligation is a time-consuming clinicalprocedure.
xamples of the deficiencies of conventionalrchwire ligation are common, but cliniciansave become accustomed to tolerating these de-ciencies. Self-ligation offers the opportunity forignificant improvements relative to all of theseactors.
roposed Core Advantages ofelf-Ligating Brackets
More certain full archwire engagement,Low friction between the bracket and thearchwire,Less chairside assistance needed, andFaster archwire removal and ligation.
hese core advantages are now all well docu-ented and additional evidence is appearingith increased frequency. Individually and inombination, each advantage has potential clin-cal benefit. As will become evident later in thisrticle, and in other articles in this issue, therere other proposed advantages, such as moreapid treatment, which can at the present timenly be described as probably true or conjec-ure. There are still further proposed advan-
ages, which at this time can be best described as
vfs
vbmtvatIptt
SF
OhlbcdhttdcptpnasbOaavtsbteilgomt
btacddm
PCA
Tpafdtioatrbdtttrtn0Damiwa1lsobegbta
fc
8 N. Harradine
ery interesting hypotheses. These have arisenrom clinical observation and are in the earlytages of more formal investigation.
The proposed four core advantages listed pre-iously apply in principle to all self-ligatingrackets although the different types of bracketay vary in their ability to deliver these advan-
ages consistently in clinical practice. These ad-antages have been previously discussed14 andre described and supported in other articles inhis issue in relation to individual bracket types.t is helpful, however, to summarize some of theroposed advantages for the unique combina-
ion of low friction and good control, whichhese brackets can provide.
ecure Archwire Engagement and Lowriction as a Combination
ther bracket types—most notably Begg brackets—ave achieved low friction by virtue of an extremely
oose fit between a round archwire and a very narrowracket, but this is at the cost of making fullontrol of tooth position correspondingly moreifficult. Some brackets with an edgewise slotave incorporated shoulders to distance the elas-
omeric from the archwire and thus reduce fric-ion, but this type of design also produces re-uced friction at the expense of reducedontrol. A deformable elastomeric ring cannotrovide and sustain sufficient force to maintain
he archwire fully in the slot without activelyressing on the archwire to an extent that sig-ificantly increases friction. Comparison withmolar tube is helpful in this context, since
uch an attachment is in essence a self-ligatingracket with the clip permanently closed.nce a convertible molar tube is converted tobracket by removal of the slot cap or straps,
n elastomeric or even a wire ligature can proveery ineffective at preventing rotation of theooth if it is moved along the wire or used as aource of intermaxillary traction. With tie wingrackets, an improvement in control is usually athe cost of an increase in friction, especially withlastomerics ligatures. This point has been wellllustrated by Matasa.15 The combination of veryow friction and very secure full archwire en-agement in an edgewise-type slot is currentlynly possible with self-ligating brackets (or witholar tubes) and is likely to be the most advan-
ageous feature of such brackets. It has therefore e
een proposed14 that this combination enables aooth to slide easily along an archwire with lowernd more predictable net forces and yet underomplete control, with almost none of the un-esirable rotation of the tooth resulting from aeformable mode of ligation such as an elasto-eric.
ossible Anchorage Consequences of theombination of Low Friction and Secure Fullrchwire Engagement
ooth movement has been shown to be onlyartially related to the level of force applied,16
lthough in that study in beagle dogs, the lowerorce per unit root area in the anchorage unitid result in much lower rates of movement overhe wide range of forces they used. In clinicalnvestigations, the study by Rajcich and Sad-wsky17 demonstrated extremely good anchor-ge preservation where retraction of canineeeth was pitted against an anchorage unit of theest of the arch. This study using conventionalrackets supports the clinical application of theifferential force theory. More widespread use of
his anchorage-preserving effect is inhibited by theendency with conventional ligation for individualeeth to rotate relative to the archwire and thenequire realignment. A thesis by Srinivas18 con-ains a well-conducted split-mouth study of ca-ine retraction using sliding mechanics on.018�/025� wire. One upper canine had aamon SL bracket and the contralateral canineconventional bracket. Canine retraction wasore rapid, to a clinically and statistically signif-
cant extent (0.24 mm per month), on the sideith Damon SL brackets. This shortened theverage time for canine retraction of 3 mm from6 weeks to 12 weeks. In addition, the anchorageoss was reduced by 0.3 mm on the Damon SLide. Furthermore, canine rotation averaged 8°n the Damon side and 12° on the conventionalracket side. These studies support the hypoth-sis that the combination of low friction andood rotational control exhibited by self-ligatingrackets may also conserve anchorage by facili-ating better use of the differential force theorys will be outlined herein.
With lower friction, the net tooth-movingorces are more predictably low and the recipro-al forces correspondingly smaller. Although the
vidence shows that the relationship between
fdfmmwrtbamwaIrpmbpatreimsTt
A
Aemowtwaafiaditmbwwfca
FA
TirastshieeEt
CFptbi
eCrtthds
F
9Self-Ligation: History and Development
orce level and tooth movement is complex,16 itoes support the idea that within the range of
orces advocated for orthodontic tooth move-ent, lower forces per unit root area lead toore anchorage. The force used by Srinivas18
as 150 gms, which is at the lower and of theange originally suggested by Reitan19 as suitableo induce an optimal histological response whenodily retracting an upper canine (150-250 gms)nd therefore much lower than the recom-ended effective force for bodily movementhen spread over the much larger root surfacerea of the other teeth on that side of the arch.ndividual teeth—for example, canines—can beetracted separately along an archwire and thusotentially reduce the overall anchorage de-ands by reduction of the root area of teeth to
e moved at any one time, but with none of theotential disadvantages of other methods of sep-rate canine retraction, for example, loss of ro-ational control. Following such separate canineetraction, the low friction of self-ligating brack-ts then facilitates sliding mechanics to retractncisors even though there will now be a mini-
um of three brackets distal to the remainingpace through which the archwire must slide.hese considerations apply equally to preserva-
ion of anterior anchorage in hypodontia cases.
lignment of Severely Irregular Teeth
combination of low friction and secure fullngagement is particularly useful in the align-ent of very irregular teeth and the resolution
f severe rotations, where the capacity of theire to release from binding and slide through
he brackets of the rotated and adjacent teethould be expected to significantly facilitatelignment. This relationship between frictionnd derotation has been described and quanti-ed by Koenig and Burstone20 and the potentialdverse forces shown to be very large. This isescribed and discussed in the article by Mavreas
n this issue of Seminars in Orthodontics. Low fric-ion therefore permits rapid alignment and
ore certain space closure, whereas the secureracket engagement permits full engagementith severely displaced teeth and full controlhile sliding teeth along an archwire. It is this
eature that greatly facilitates the alignment ofrowded teeth, which have to push each other
long the archwire to gain alignment. aactors That Have Hindered thedoption of Self-Ligation
he four core advantages listed previously arencreasingly supported by greater clinical expe-ience and by formal investigations.7-12,15,21 Inddition, there are studies that provide someupport for a resulting increase in clinical effec-iveness.18,22,23 It is therefore helpful to describeome of the factors that have, until recently,indered the more widespread use of self-ligat-
ng brackets. The factors have varied with differ-nt bracket designs and can be illustrated byxamples from Table 1. With the exception ofdgelok, the author of this article has used all
he examples used for illustration herein.Edgelok brackets. Edgelok brackets (Ormco
orp., 1717 W. Collins Ave., Orange, CA 92867;ig 2) were the first self-ligating bracket to beroduced in significant quantities. Disadvan-ages included inadequate rotational control,ulkiness, and some inconvenience with open-
ng and closing the slide.SPEED brackets. The well-known SPEED brack-
ts (Strite Industries Ltd., 298 Shepherd Avenue,ambridge, Ontario, N3C 1V1 Canada; Fig 3) have
emained in successful production since 1980. Thisestifies to the inherent soundness of many ofhe original design features. Early brackets wereandicapped by clips, which could too easily beisplaced or distorted. These drawbacks haveince been successfully addressed, but combined
igure 2. Edgelok bracket. (Color version of figure is
vailable online.)
wbhv
e1rdoeTdnTetAos
pwtedwdt
bAgbhwpwibcr
Fai
Fu
F
10 N. Harradine
ith the inherent unfamiliarity for clinicians of aracket with no tie wings, these aspects probablyindered the wider popularity of SPEED in pre-ious years.
Mobil-Lock brackets. Mobil-Lock brackets (For-stadent Bernhard Foerster GmbH, Westliche51 75173 Pforzheim, Germany; Fig 4) had aotating cam, which was turned with a “screw-river,” thus covering part of the labial surfacef the slot. The wire could be tightly or looselyngaged by the degree of rotation of the cam.hese brackets were well engineered by the stan-ards of the day, but a major limitation was thearrowness of the resulting labial face of the slot.his gave very poor rotational control to thextent that upper incisor brackets were givenwin cams to increase the effective bracket width.nother problem was the difficulty of access topen and close premolar brackets with thetraight screwdriver.
Activa brackets.4 Activa brackets (“A” Com-any, San Diego, CA; Fig 5) had a rotating slide,hich therefore gave a concave inner radius to
he labial surface of the slot. This increased theffective slot depth with small diameter wires,iminishing labiolingual alignment with suchires. The slide was retained on the mesial andistal ends of the slot and this made for a wider
han average bracket, which reduced the inter-
igure 3. SPEED bracket. More details are in therticle by Berger in this issue. (Color version of figure
s available online.) aracket span with the consequent disadvantages.potential advantage of self-ligation is that the
ood archwire control permits use of narrowerrackets and thus greater interbracket span andence lower forces and a longer range of actionith any given archwire during the alignmenthase. The absence of tie wings was a nuisancehen placing elastomeric chain and the unfamil-
ar shape of the early bonding base maderacket positioning more difficult. Finally, aombination of the design features substantiallyeduced bond strength. Despite these substan-
igure 4. Mobil-Lock bracket. (Color version of fig-re is available online.)
igure 5. Activa bracket. (Color version of figure is
vailable online.)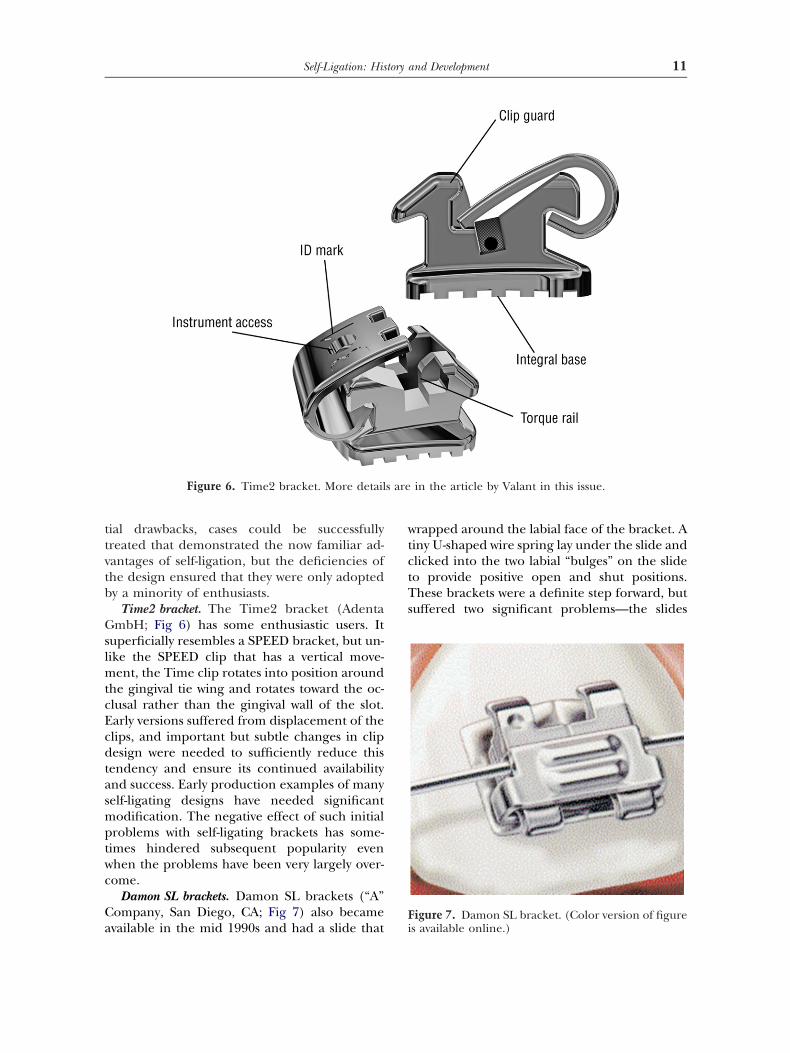
ttvtb
GslmtcEcdtasmptwc
Ca
wtctTs
s are
F
11Self-Ligation: History and Development
ial drawbacks, cases could be successfullyreated that demonstrated the now familiar ad-antages of self-ligation, but the deficiencies ofhe design ensured that they were only adoptedy a minority of enthusiasts.
Time2 bracket. The Time2 bracket (AdentambH; Fig 6) has some enthusiastic users. It
uperficially resembles a SPEED bracket, but un-ike the SPEED clip that has a vertical move-
ent, the Time clip rotates into position aroundhe gingival tie wing and rotates toward the oc-lusal rather than the gingival wall of the slot.arly versions suffered from displacement of thelips, and important but subtle changes in clipesign were needed to sufficiently reduce this
endency and ensure its continued availabilitynd success. Early production examples of manyelf-ligating designs have needed significantodification. The negative effect of such initial
roblems with self-ligating brackets has some-imes hindered subsequent popularity evenhen the problems have been very largely over-ome.
Damon SL brackets. Damon SL brackets (“A”ompany, San Diego, CA; Fig 7) also became
Figure 6. Time2 bracket. More detail
vailable in the mid 1990s and had a slide that i
rapped around the labial face of the bracket. Ainy U-shaped wire spring lay under the slide andlicked into the two labial “bulges” on the slideo provide positive open and shut positions.hese brackets were a definite step forward, but
uffered two significant problems—the slides
in the article by Valant in this issue.
igure 7. Damon SL bracket. (Color version of figure
s available online.)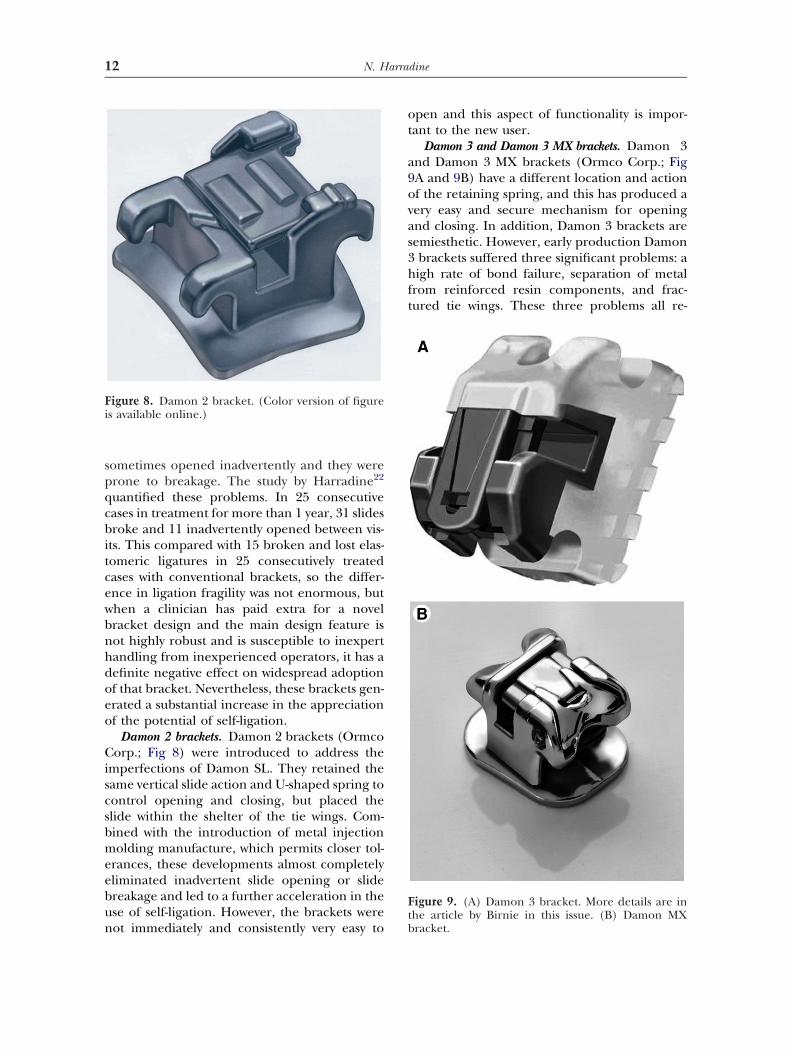
spqcbitcewbnhdoeo
Ciscsbmeebun
ot
a9ovas3hft
Fi
Ft
12 N. Harradine
ometimes opened inadvertently and they wererone to breakage. The study by Harradine22
uantified these problems. In 25 consecutiveases in treatment for more than 1 year, 31 slidesroke and 11 inadvertently opened between vis-
ts. This compared with 15 broken and lost elas-omeric ligatures in 25 consecutively treatedases with conventional brackets, so the differ-nce in ligation fragility was not enormous, buthen a clinician has paid extra for a novelracket design and the main design feature isot highly robust and is susceptible to inexpertandling from inexperienced operators, it has aefinite negative effect on widespread adoptionf that bracket. Nevertheless, these brackets gen-rated a substantial increase in the appreciationf the potential of self-ligation.
Damon 2 brackets. Damon 2 brackets (Ormcoorp.; Fig 8) were introduced to address the
mperfections of Damon SL. They retained theame vertical slide action and U-shaped spring toontrol opening and closing, but placed thelide within the shelter of the tie wings. Com-ined with the introduction of metal injectionolding manufacture, which permits closer tol-
rances, these developments almost completelyliminated inadvertent slide opening or slidereakage and led to a further acceleration in these of self-ligation. However, the brackets were
igure 8. Damon 2 bracket. (Color version of figures available online.)
ot immediately and consistently very easy to b
pen and this aspect of functionality is impor-ant to the new user.
Damon 3 and Damon 3 MX brackets. Damon 3nd Damon 3 MX brackets (Ormco Corp.; FigA and 9B) have a different location and actionf the retaining spring, and this has produced aery easy and secure mechanism for openingnd closing. In addition, Damon 3 brackets areemiesthetic. However, early production Damonbrackets suffered three significant problems: aigh rate of bond failure, separation of metal
rom reinforced resin components, and frac-ured tie wings. These three problems all re-
igure 9. (A) Damon 3 bracket. More details are inhe article by Birnie in this issue. (B) Damon MX
racket.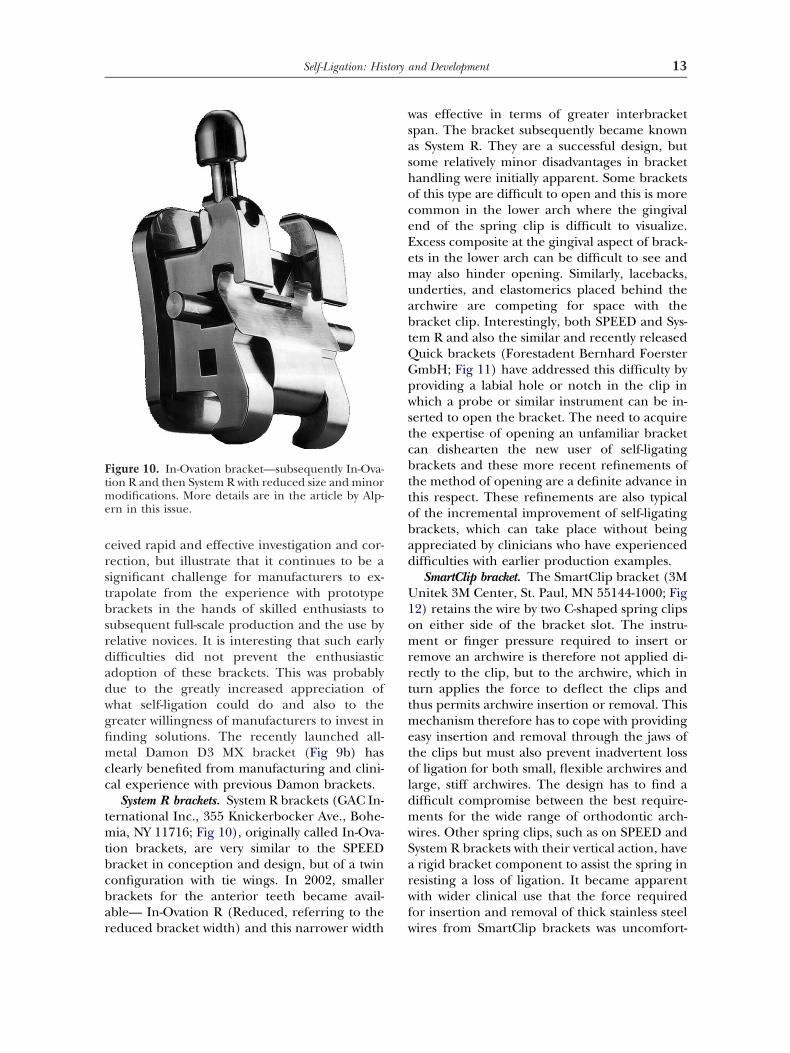
crstbsrdadwgfimcc
tmtbcbar
wsashoceEemuabtQGpwstcbttobad
U1omrrttmetoldmwSarwf
Ftme
13Self-Ligation: History and Development
eived rapid and effective investigation and cor-ection, but illustrate that it continues to be aignificant challenge for manufacturers to ex-rapolate from the experience with prototyperackets in the hands of skilled enthusiasts toubsequent full-scale production and the use byelative novices. It is interesting that such earlyifficulties did not prevent the enthusiasticdoption of these brackets. This was probablyue to the greatly increased appreciation ofhat self-ligation could do and also to thereater willingness of manufacturers to invest innding solutions. The recently launched all-etal Damon D3 MX bracket (Fig 9b) has
learly benefited from manufacturing and clini-al experience with previous Damon brackets.
System R brackets. System R brackets (GAC In-ernational Inc., 355 Knickerbocker Ave., Bohe-
ia, NY 11716; Fig 10), originally called In-Ova-ion brackets, are very similar to the SPEEDracket in conception and design, but of a twinonfiguration with tie wings. In 2002, smallerrackets for the anterior teeth became avail-ble— In-Ovation R (Reduced, referring to the
igure 10. In-Ovation bracket—subsequently In-Ova-ion R and then System R with reduced size and minor
odifications. More details are in the article by Alp-rn in this issue.
educed bracket width) and this narrower width w
as effective in terms of greater interbracketpan. The bracket subsequently became knowns System R. They are a successful design, butome relatively minor disadvantages in bracketandling were initially apparent. Some bracketsf this type are difficult to open and this is moreommon in the lower arch where the gingivalnd of the spring clip is difficult to visualize.xcess composite at the gingival aspect of brack-ts in the lower arch can be difficult to see anday also hinder opening. Similarly, lacebacks,
nderties, and elastomerics placed behind therchwire are competing for space with theracket clip. Interestingly, both SPEED and Sys-em R and also the similar and recently releaseduick brackets (Forestadent Bernhard FoerstermbH; Fig 11) have addressed this difficulty byroviding a labial hole or notch in the clip inhich a probe or similar instrument can be in-
erted to open the bracket. The need to acquirehe expertise of opening an unfamiliar bracketan dishearten the new user of self-ligatingrackets and these more recent refinements ofhe method of opening are a definite advance inhis respect. These refinements are also typicalf the incremental improvement of self-ligatingrackets, which can take place without beingppreciated by clinicians who have experiencedifficulties with earlier production examples.
SmartClip bracket. The SmartClip bracket (3Mnitek 3M Center, St. Paul, MN 55144-1000; Fig
2) retains the wire by two C-shaped spring clipsn either side of the bracket slot. The instru-ent or finger pressure required to insert or
emove an archwire is therefore not applied di-ectly to the clip, but to the archwire, which inurn applies the force to deflect the clips andhus permits archwire insertion or removal. This
echanism therefore has to cope with providingasy insertion and removal through the jaws ofhe clips but must also prevent inadvertent lossf ligation for both small, flexible archwires and
arge, stiff archwires. The design has to find aifficult compromise between the best require-ents for the wide range of orthodontic arch-ires. Other spring clips, such as on SPEED andystem R brackets with their vertical action, haverigid bracket component to assist the spring in
esisting a loss of ligation. It became apparentith wider clinical use that the force required
or insertion and removal of thick stainless steel
ires from SmartClip brackets was uncomfort-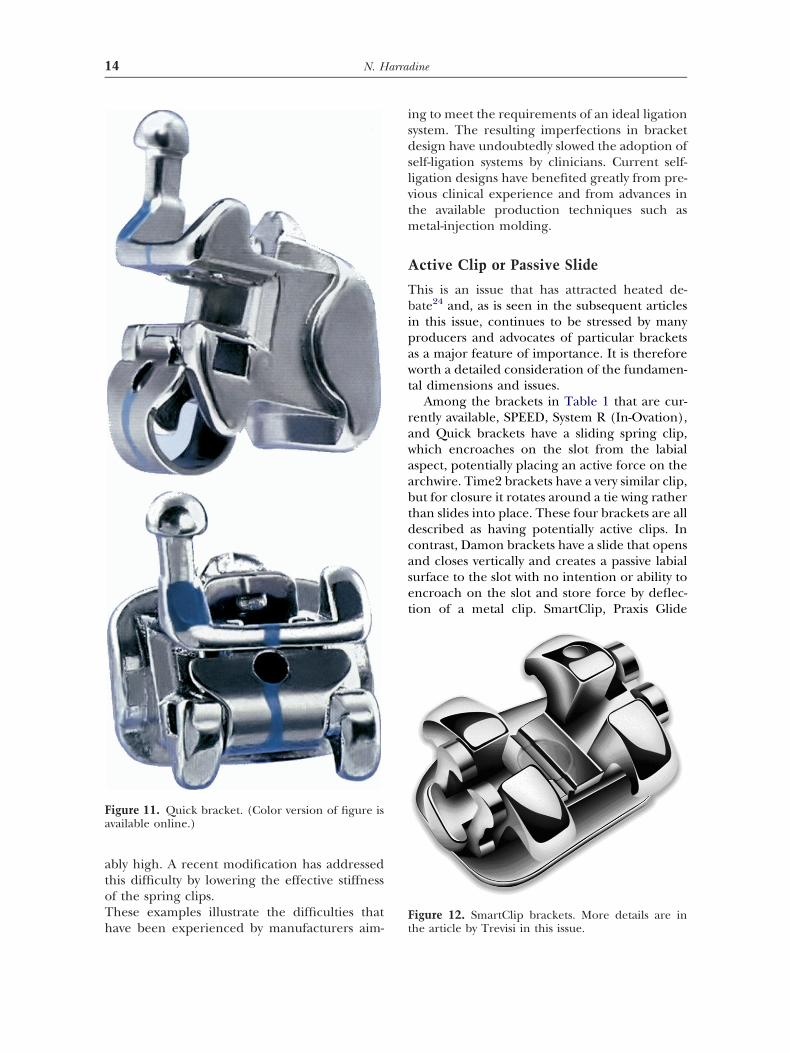
atoTh
isdslvtm
A
Tbipawt
rawaabtdcaset
Fa
F
14 N. Harradine
bly high. A recent modification has addressedhis difficulty by lowering the effective stiffnessf the spring clips.hese examples illustrate the difficulties that
igure 11. Quick bracket. (Color version of figure isvailable online.)
ave been experienced by manufacturers aim- t
ng to meet the requirements of an ideal ligationystem. The resulting imperfections in bracketesign have undoubtedly slowed the adoption ofelf-ligation systems by clinicians. Current self-igation designs have benefited greatly from pre-ious clinical experience and from advances inhe available production techniques such as
etal-injection molding.
ctive Clip or Passive Slide
his is an issue that has attracted heated de-ate24 and, as is seen in the subsequent articles
n this issue, continues to be stressed by manyroducers and advocates of particular bracketss a major feature of importance. It is thereforeorth a detailed consideration of the fundamen-
al dimensions and issues.Among the brackets in Table 1 that are cur-
ently available, SPEED, System R (In-Ovation),nd Quick brackets have a sliding spring clip,hich encroaches on the slot from the labialspect, potentially placing an active force on therchwire. Time2 brackets have a very similar clip,ut for closure it rotates around a tie wing ratherhan slides into place. These four brackets are allescribed as having potentially active clips. Inontrast, Damon brackets have a slide that opensnd closes vertically and creates a passive labialurface to the slot with no intention or ability toncroach on the slot and store force by deflec-ion of a metal clip. SmartClip, Praxis Glide
igure 12. SmartClip brackets. More details are in
he article by Trevisi in this issue.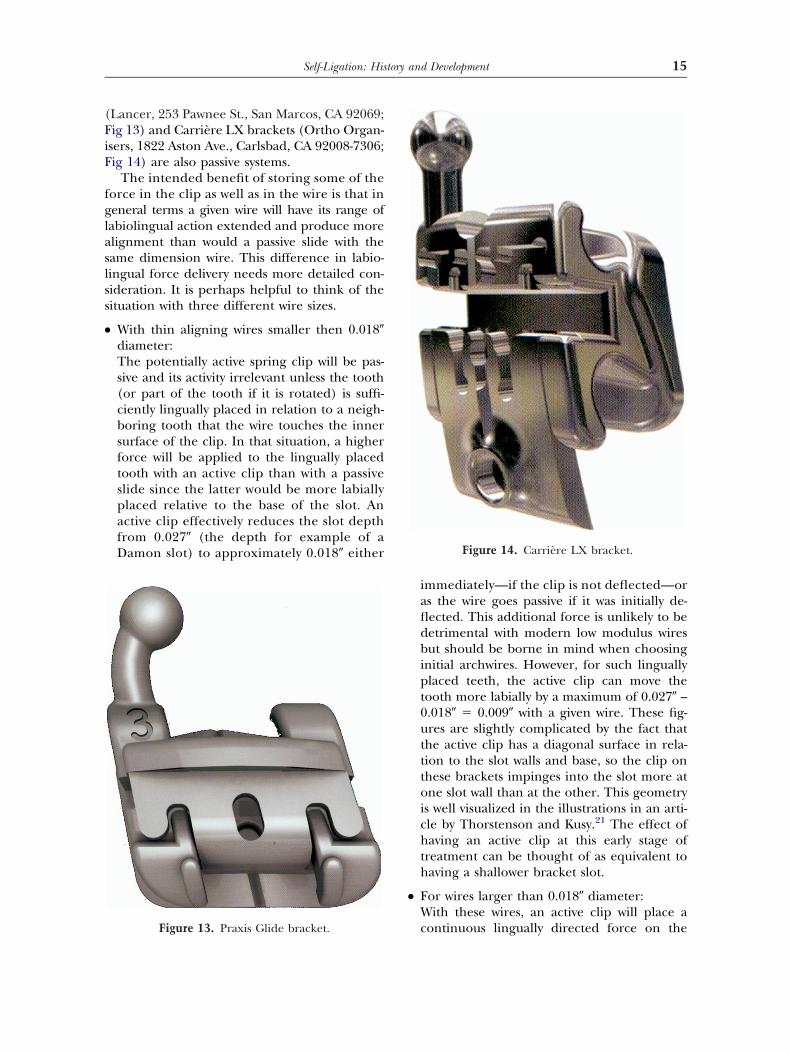
(FiF
fglaslss
●
●
15Self-Ligation: History and Development
Lancer, 253 Pawnee St., San Marcos, CA 92069;ig 13) and Carrière LX brackets (Ortho Organ-sers, 1822 Aston Ave., Carlsbad, CA 92008-7306;ig 14) are also passive systems.
The intended benefit of storing some of theorce in the clip as well as in the wire is that ineneral terms a given wire will have its range ofabiolingual action extended and produce morelignment than would a passive slide with theame dimension wire. This difference in labio-ingual force delivery needs more detailed con-ideration. It is perhaps helpful to think of theituation with three different wire sizes.
With thin aligning wires smaller then 0.018�diameter:The potentially active spring clip will be pas-sive and its activity irrelevant unless the tooth(or part of the tooth if it is rotated) is suffi-ciently lingually placed in relation to a neigh-boring tooth that the wire touches the innersurface of the clip. In that situation, a higherforce will be applied to the lingually placedtooth with an active clip than with a passiveslide since the latter would be more labiallyplaced relative to the base of the slot. Anactive clip effectively reduces the slot depthfrom 0.027� (the depth for example of aDamon slot) to approximately 0.018� either
Figure 13. Praxis Glide bracket.
immediately—if the clip is not deflected—oras the wire goes passive if it was initially de-flected. This additional force is unlikely to bedetrimental with modern low modulus wiresbut should be borne in mind when choosinginitial archwires. However, for such linguallyplaced teeth, the active clip can move thetooth more labially by a maximum of 0.027� –0.018� � 0.009� with a given wire. These fig-ures are slightly complicated by the fact thatthe active clip has a diagonal surface in rela-tion to the slot walls and base, so the clip onthese brackets impinges into the slot more atone slot wall than at the other. This geometryis well visualized in the illustrations in an arti-cle by Thorstenson and Kusy.21 The effect ofhaving an active clip at this early stage oftreatment can be thought of as equivalent tohaving a shallower bracket slot.
For wires larger than 0.018� diameter:With these wires, an active clip will place a
Figure 14. Carrière LX bracket.
continuous lingually directed force on the

●
Oa
Tppsigcteoe
swwatcsttnienFtiiwa
p
16 N. Harradine
wire even when the wire has gone passive. Onteeth that are in whole or in part lingual to aneighboring tooth, the active clip will againbring the tooth slightly more labial than wouldhave been the case with a passive clip at 0.027�slot depth. The maximum difference in labialtooth movement will be the difference be-tween the labiolingual dimension of the wireand 0.027�. For a typical 0.016� � 0.022� inter-mediate wire, this would give a maximum dif-ference of 0.005 �. 0.016� � 0.025� or 0.014� �0.025� nickel titanium wires are recom-mended as the intermediate aligning wire forthe passive Damon system and this wire re-duces the potential difference to 0.002�. Lin-gually placed teeth would have a slightlyhigher initial force with an active clip whenusing wires of this intermediate size.
With thick rectangular wires:An active clip will make a labiolingual differ-ence in tooth position of 0.002� or less, whichis very small clinically. It has been suggestedthat continued lingually directed force on thewire from an active clip will cause additionaltorque from an undersized wire. This wouldbe a useful action in such brackets, because itwould overcome the diminished torquing abil-ity in one direction, which inevitably resultsfrom the active clip needing to encroach intothe slot. This encroachment diminishes thelabiolingual slot depth on one side of the slotand therefore the generation of torque fromthe gingival and occlusal slot walls. The sug-gestion that the lingually directed force froman active clip can generate effective torqueperhaps reflects a degree of misunderstandingor optimism about the generation of torque inan edgewise slot. The diagonally directed lin-gual force may not contribute to any effectivethird order interaction between the wire cor-ners and the upper and lower walls of thebracket slot, which is the origin of torquingforce. SPEED brackets have therefore morerecently addressed this question on upper in-cisors by extending the gingival walls of theslot either side of the clip to the full slot depthas “torquing rails.” This should indeed restorethe torquing effectiveness. Time2 bracketsalso have two torquing rails within the overallclip width. Similarly, System R (In-Ovation)
brackets have a small central portion of the islot wall of some brackets that is full depth andtherefore provides full torquing capacity onthat section. It should be noted that whileSPEED and System R brackets have a clip thatimpinges on the slot at the gingival slot wall, thereverse is the case for Time2 brackets, so a po-tential effect on torque in an upper incisorwould be on palatal root torque with the formerbrackets and labial root torque with Time2. Thearticle in this issue by John Valant on Time2brackets reports dimensions that indicate thatthe slot encroachment is 0.002� greater on theTime2 brackets, so these issues have a little morecomplexity than may initially seem the case.
verall Advantages or Disadvantages ofn Active Clip
he actual clinical consequences of having aotentially active clip impinging into the slot areerhaps harder to assess than a first thoughtuggests. It is probable that with an active clip,nitial alignment is more complete for a wire ofiven size to an extent that is potentially usefullinically. However, the increased clearance be-ween a given wire and a passive slide will gen-rate lower forces and may facilitate dissipationf binding forces and the ability of teeth to pushach other aside as they align.
With modern low modulus wires it is possible toubsequently insert thicker wires into a bracketith a passive slide and arrive at the working arch-ire size after the same number of visits as with anctive clip—for example, to store all the force inhe wire rather than dividing it between wire andlip. The relative stiffness of archwires and thepring clip is not well documented. If it is assumedhat the spring clip has the same stiffness as ahicker nickel titanium wire, then both mecha-isms would produce the same labiolingual align-
ng force with wires of that size. In fact, the differ-nt active clips are made from a variety of alloys—ickel-titanium, stainless steel and Elgiloy Co-Cr-e-Ni alloy—which will have different moduli, sohe clips will very probably have differing rigid-ties. If the clip is more rigid, then for a givenrregularity that deflects an archwire, the wireill be deflected more and the clip deflected lessnd vice versa.
Once in the thick working archwire, theotential disadvantages of an active clip are
ncreased friction and potentially reduced

tbtltodimffaeFstatbtspAdtbifmi
C
CmbeHscpg
d
●
●
●
●
Tnm
mDisomtowccttactoitpibebtaaovoti
C
Ctfaetoao
17Self-Ligation: History and Development
orquing capacity in one direction with somerackets. To put the friction levels in context,hese higher friction forces are still very muchower than those found with elastomeric liga-ures on a conventional tie-wing bracket. Allther factors being equal, higher friction is aisadvantage in many tooth movements, but it
s hard to assess the effect on clinical perfor-ance which arises from this level of increased
riction. The trend to having a full slot depthor part of the encroached slot wall with somective self-ligating brackets reduces any differ-nce in potential torquing ability and control.inally, there are the questions of robustness,ecurity of ligation and ease of use. Is a cliphat is designed to flex, more prone to break-ge or permanent deformation or to inadver-ent opening or closing? This question has noteen formally investigated. Studies involvinghe use of different self-ligating brackets in theame patient or randomly assigned to differentatients are needed to test such hypotheses.lthough the different effects can be eluci-ated, it is hard to weigh the extent to whichhe differences between active and passiverackets affect clinical performance. However,
t is hoped that this section of the article use-ully informs a consideration of the claims
ade in this context in later articles in thisssue.
ost and Treatment Efficiency
urrently available self-ligating brackets areore expensive than most good quality tie wing
rackets. A modest balancing factor is the cost oflastic ligatures that are, of course, not required.owever, this significant extra cost must be mea-
ured against savings in time—an expensiveommodity. If self-ligating brackets save any ap-reciable chairside time as some studies8,10 sug-est, this would provide an offsetting saving.
A study of treatment efficiency by Harra-ine22 found the following:
a very modest average time saving from a re-duction in archwire placement/removal of 24seconds per arch,A mean reduction of 4 months in active treat-ment time from 23.5 to 19.4 months,A mean reduction of four visits during active
treatment from 16 to 12, and tThe same average reduction in Peer Assess-ment Rating scores for matched cases.
hese cases were treated in the late 1990s witho change in extraction philosophy or treat-ent goals.This finding of a mean reduction of 4
onths in treatment time was also reported byr. Robert Fry in a presentation at the Amer-
can Association of Orthodontists Annual Ses-ion in Toronto 2001. He had converted onef his two offices to Damon SL. The officeanagement software subsequently revealed
hat his treatment times reduced by an averagef 4 months compared with his other officehere he had, for the time being, stayed withonventional ligation. A study by Eberting andoworkers3 of intrapractitioner differences inhree practices found an average reduction inreatment time of 7 months (from 30 to 25)nd seven visits (from 28 to 21) for Damon SLases compared with conventional ligation. Inwo of the three centers, the American Boardf Orthodontists irregularity scores were more
mproved with the Damon SL brackets to a statis-ically significant extent. These three reports sup-ort a view of clinically significant improvements
n treatment efficiency with passive self-ligatingrackets. The more recent bracket types would bexpected to show still better treatment efficiencyecause they are less prone to breakage or loss ofhe clips and slides, are easier to open and close,re frequently of more effective slot dimensions,nd are used with greater understanding of theptimal archwire selection and appointment inter-als. Further studies are in progress with a varietyf bracket types and some of these that deal withhe early alignment phase of treatment are alreadyn press, so this is a rapidly moving field of enquiry.
onclusions
urrently available self-ligating brackets offerhe very valuable combination of extremely lowriction and secure full bracket engagementnd—at last—they are sufficiently robust and us-r-friendly to deliver most of the potential advan-ages of this type of bracket. The core advantagesf self-ligation are now established and readilyvailable. These developments offer the possibilityf a significant reduction in average treatment
imes and maybe also in anchorage requirements,
pmeabw
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
18 N. Harradine
articularly in cases requiring large tooth move-ents. Evidence of better treatment effectiveness
xists but is incomplete. While further refinementsre desirable and further studies essential, currentrackets appear able to deliver measurable benefitith good robustness and ease of use.
eferences1. Stolzenberg J: The Russell attachment and its improved
advantages. Int J Orthod Dent Child 21:837-840, 19352. Wildman AJ: Round table—the Edgelok bracket. J Clin
Orthod 6:613-623, 19723. Berger JL: The SPEED appliance: a 14 year update on
this unique self-ligating orthodontic mechanism. Am JOrthod Dentofacial Orthop 105:217-223, 1994
4. Harradine NWT, Birnie DJ: The clinical use of Activaself-ligating brackets. Am J Orthod Dentofacial Orthop109:319-328, 1996
5. Damon DH: The rationale, evolution and clinical applicationof the self-ligating bracket. Clin Orthod Res 1:52-61, 1998
6. Damon DH: The Damon low friction bracket: a biolog-ically compatible straight-wire system. J Clin Orthod 32:670-680, 1998
7. Taloumis LJ, Smith TM, Hondrum SO, et al: Force decayand deformation of orthodontic elastomeric ligatures.Am J Orthod Dentofacial Orthop 111:1-11, 1997
8. Shivapuja PK, Berger J: A comparative study of conven-tional ligation and self-ligation bracket systems. Am JOrthod Dentofacial Orthop 106:472-480, 1994
9. Khambay B, Millett D, Mc Hugh S: Evaluation of meth-ods of archwire ligation on frictional resistance. EurJ Orthod 26:327-332, 2004
0. Maijer R, Smith DC: Time saving with self-ligating brack-ets. J Clin Orthod 24:29-31, 1990
1. Forsberg C, Brattström V, Malmberg E, Nord CE: Liga-ture wires and elastomeric rings: two methods of liga-tion, and their association with microbial colonization ofStreptococcus mutans and lactobacilli. Eur J Orthod
13:416-420, 19912. Turkkahraman H, Özgür SM, Yesim BF, et al: Archwireligation techniques, microbial colonization, and peri-odontal status in orthodontically treated patients. AngleOrthod 75:231-236, 2005
3. Sukontapatipark W, El-Agroudi MA, Selliseth NJ, ThunoldK, Selvig KA: Bacterial colonisation associated with fixedorthodontic appliances. A scanning electron microscopystudy. Eur J Orthod 23:475-484, 2001
4. Harradine NWT: Self-ligating brackets: where are wenow? J Orthod 30:262-273, 2003
5. Matasa CG: Brackets’ shape influences friction. TheOrthodontic Materials Insider 13:2-5, 2001
6. Pilon JGM, Kuijpers-Jagtman AM, Maltha JC: Magnitudeof orthodontic forces and rate of bodily tooth move-ment. An experimental study. Am J Orthod DentofacialOrthop 110:16-23, 1996
7. Rajcich M, Sadowsky C: Efficacy of intra-arch mechanicsusing differential moments for achieving anchoragecontrol in extraction cases. Am J Orthod DentofacialOrthop 112:441-448, 1997
8. Srinivas S: Comparison of canine retraction with self-li-gated and conventional ligated brackets—a clinical study.2003. Thesis in fulfillment of postgraduate degree, Tamil-nadu Medical University, Chennai, India
9. Reitan K: Some factors determining the evaluation offorces in orthodontics. Am J Orthod 1957;43:32-46
0. Koenig HA, Burstone CJ: Force systems from an idealarch—large deflection considerations. Angle Orthod 59:11-16, 1989
1. Thorstenson BS, Kusy RP: Effect of archwire size andmaterial on the resistance to sliding of self-ligatingbrackets with second-order angulation in the dry state.Am J Orthod Dentofacial Orthop 122:295-305, 2002
2. Harradine NWT: Self-ligating brackets and treatmentefficiency. Clin Orthod Res 4:220-227, 2001
3. Eberting JJ, Straja SR, Tuncay OC: Treatment time, out-come and patient satisfaction comparisons of Damonand conventional brackets. Clin Orthod Res 4:228-234,2001
4. Matasa CG: Self-engaging brackets: passive vs. active. The
Orthodontic Materials Insider 9:5-11, 1996