the hope act and impact on drug- and alcohol-related intoxication deaths source: drug- and...
TRANSCRIPT
The HOPE Act and Impact on Pharmacists’ Role in Combating
the Opioid Epidemic
Kirsten Forseth, MPHOverdose Prevention Policy AnalystBehavioral Health Administration
Maryland Department of Health and Mental Hygiene
MPhA Annual ConventionJune 26, 2017
Overview
I. Introduction
II. The HOPE Act
III. Naloxone “Train the Trainer”
IV. The Pharmacists’ Role: Beyond Overdose
V. Closing
Learning Objectives
Participants will:
• Recognize the importance of overdose education and
naloxone for reducing overdose deaths
• Understand the changes to naloxone access in
pharmacies resulting from the HOPE Act
• Apply knowledge to successfully conduct patient
education and dispensing of naloxone under the
statewide standing order
• Identify additional opportunities to prevent disease and
protect the health of people who use drugs
INTRODUCTION AND CONTEXT
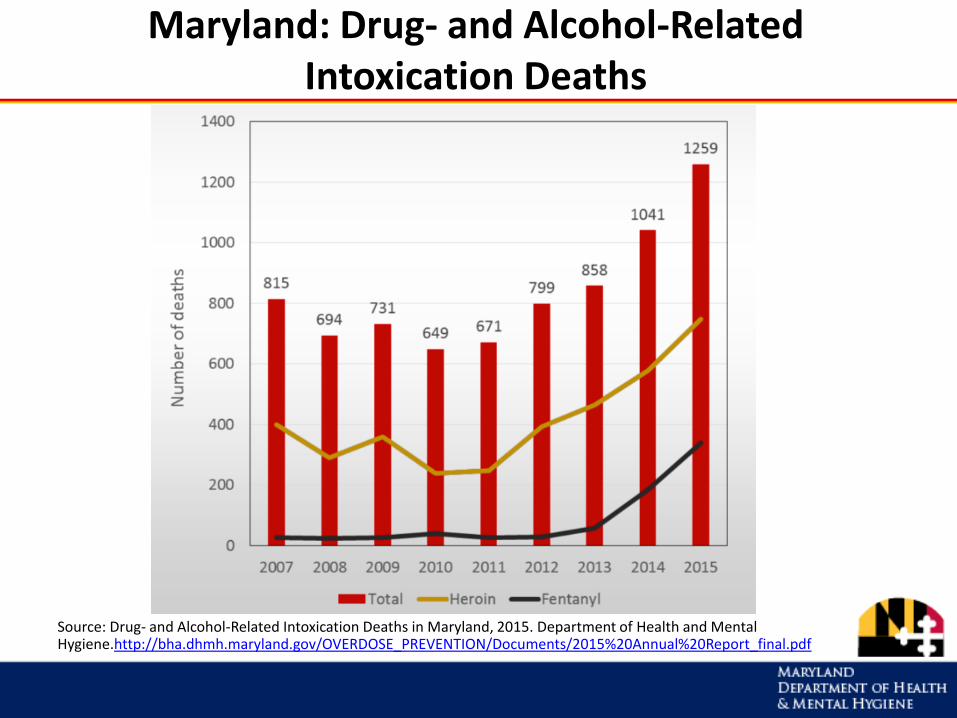
Maryland: Drug- and Alcohol-Related Intoxication Deaths
Source: Drug- and Alcohol-Related Intoxication Deaths in Maryland, 2015. Department of Health and Mental Hygiene.http://bha.dhmh.maryland.gov/OVERDOSE_PREVENTION/Documents/2015%20Annual%20Report_final.pdf
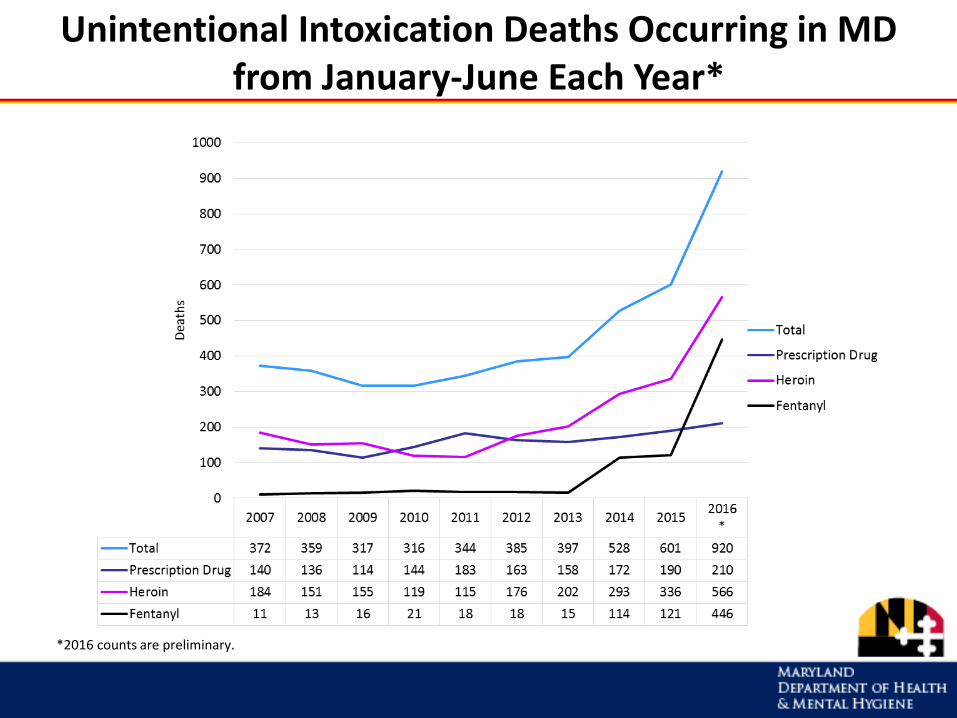
Unintentional Intoxication Deaths Occurring in MD from January-June Each Year*
*2016 counts are preliminary.
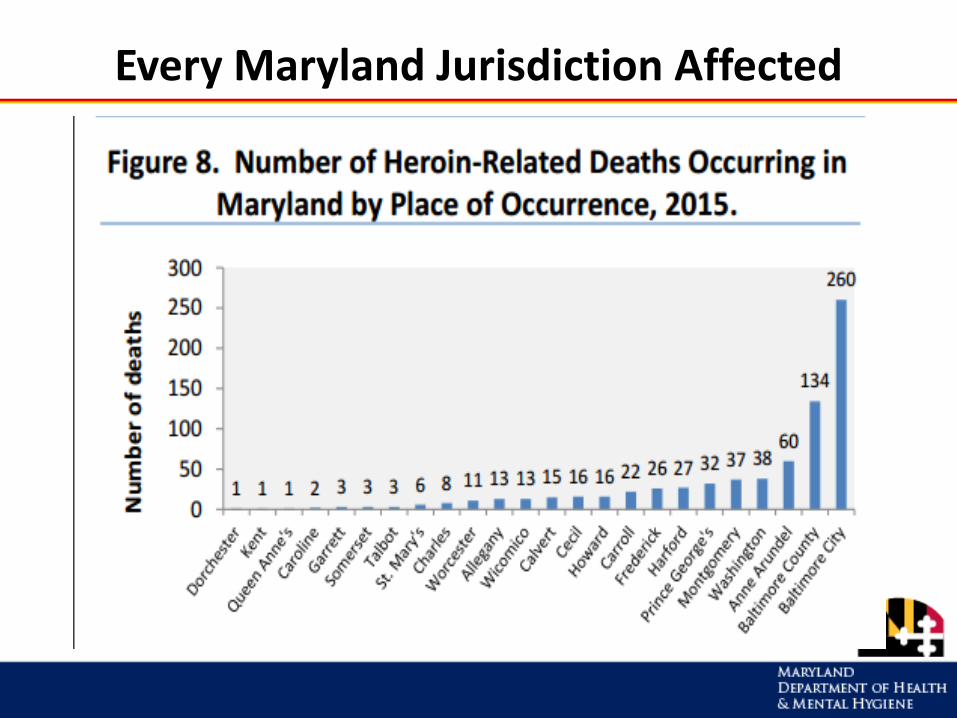
Every Maryland Jurisdiction Affected
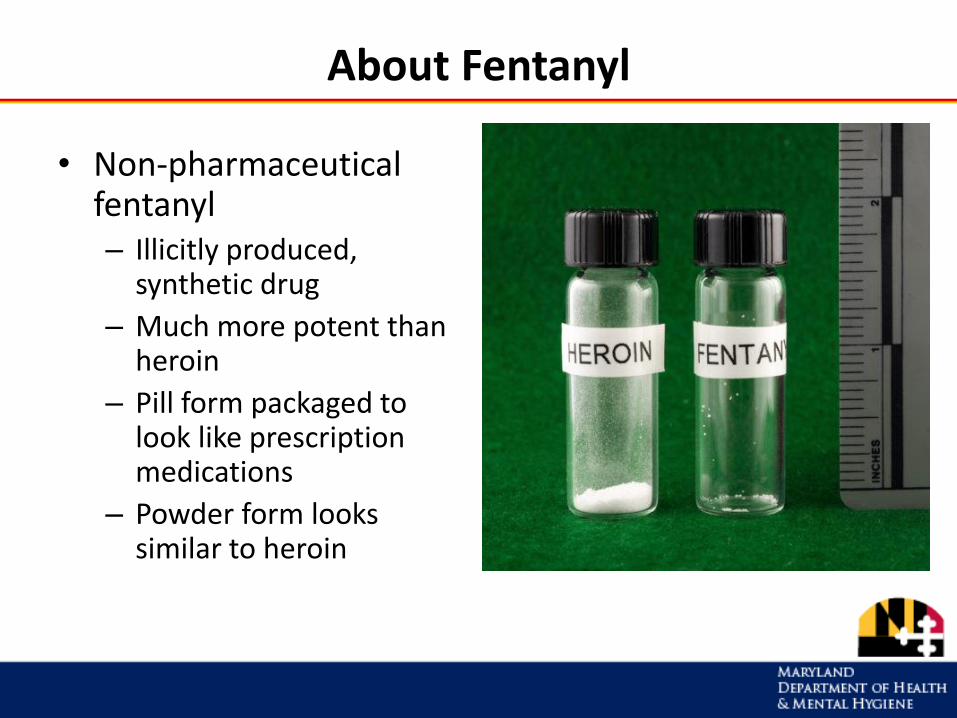
About Fentanyl
• Non-pharmaceutical fentanyl– Illicitly produced,
synthetic drug
– Much more potent than heroin
– Pill form packaged to look like prescription medications
– Powder form looks similar to heroin
Source of Illicitly Manufactured Fentanyl
• Chinese laboratory companies are the main producers of non-pharmaceutical fentanyl and fentanyl precursor chemicals, as well as industrial pill presses used in tableting fentanyls
• Fentanyl and fentanyl precursor chemicals are shipped to a variety of places in North America
• Drug traffickers obtain fentanyl and mix it into heroin or press it into pills on their own. This occurs at a variety of locations such as hotel rooms or homes, sometimes known as fentanyl "mills“
Drug Enforcement Administration. Counterfeit Prescription Pills Containing Fentanyls: A Global Threat. DEA Intelligence Brief. July 2016. https://content.govdelivery.com/attachments/USDOJDEA/2016/07/22/file_attachments/590360/fentanyl%2Bpills%2Breport.pdf
How Does Fentanyl Increase Overdose Risk?
• Higher potency = greater toxicity
• Other chemical properties– high lipid solubility– rapid onset– short duration of effect – meaning need for more frequent dosing
• Nature of illicit drug supply
“…clandestine labs or illicit pill pressing operations have difficulty distributing the active substance evenly across an entire batch of tablets or powders, particularly when the active dose is very small, as when using such potent substances as fentanyl. The result is an uneven distribution of active substance, which means that some tablets or powders might contain a small quantity of the active substance, while other tablets or powders might contain a lethal dose.”
Canadian Centre on Substance Abuse Bulletin. Novel Synthetic Opioids in Counterfeit Pharmaceuticals and Other Illicit Street Drugs. June 2016. http://www.ccsa.ca/Resource%20Library/CCSA-CCENDU-Novel-Synthetic-Opioids-Bulletin-2016-en.pdf
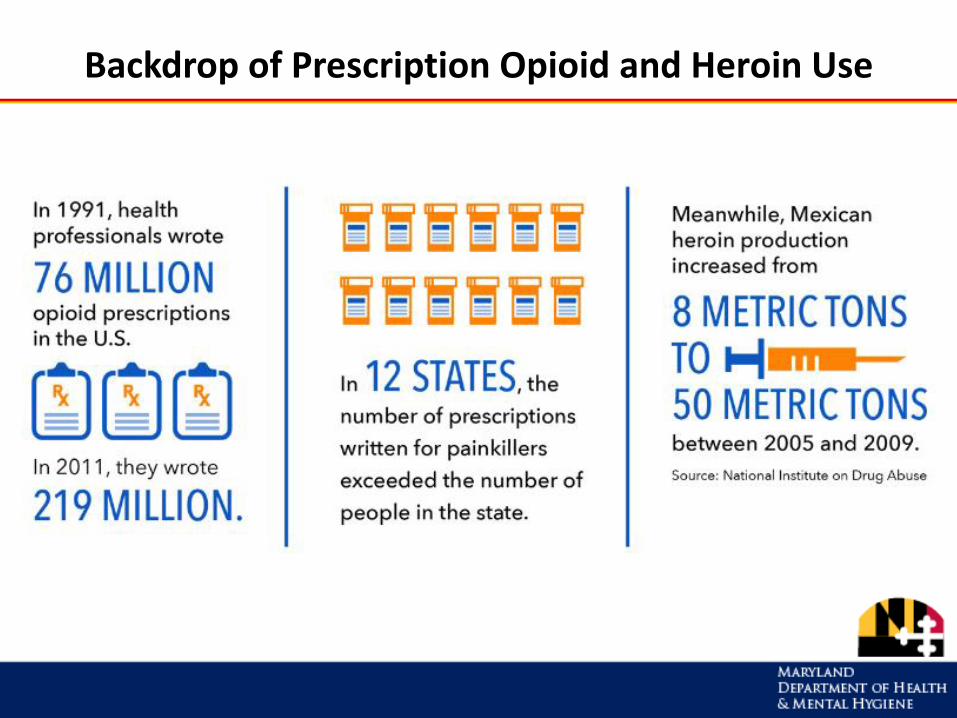
Backdrop of Prescription Opioid and Heroin Use
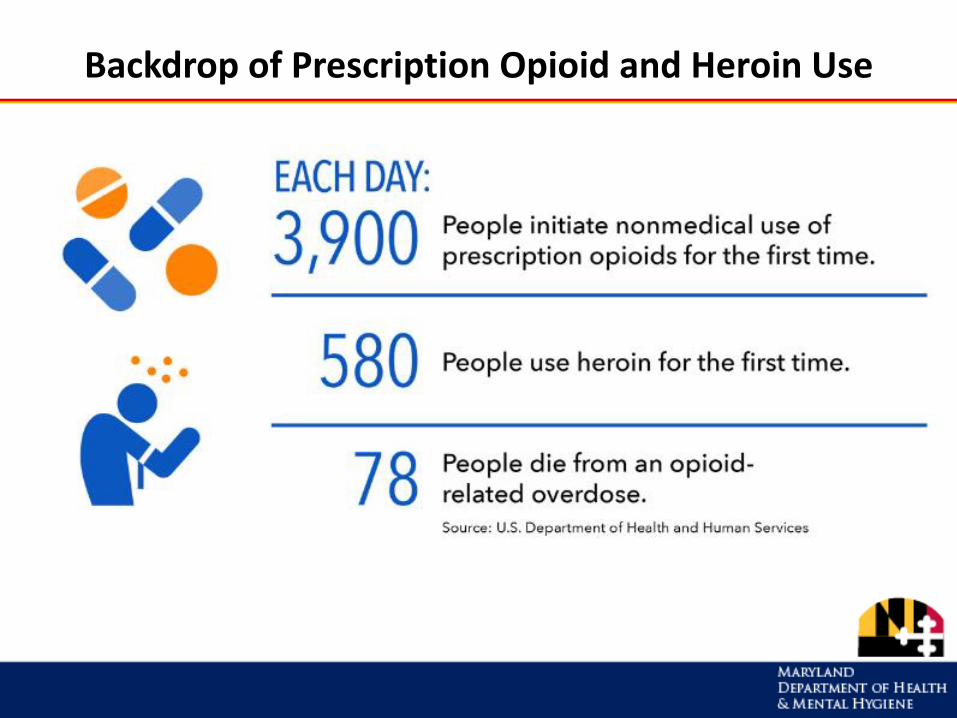
Backdrop of Prescription Opioid and Heroin Use
Multiple Factors Worsen Current Epidemic
• Large number of nonmedical prescription drug users = high demand incentivizing drug traffickers to create counterfeit pills
• Prescription pill use has fewer stigmas and can attract new, inexperienced drug users, creating more fentanyl-dependent individuals
• Change in heroin distribution innovations and new distribution models – heroin being marketed by entrepreneurs in a way that gets it into smaller cities, such as Gary, Madison, Memphis, Minneapolis, Cleveland
• Heroin becoming initial drug of choice? Because of new market strategies and expanded supply
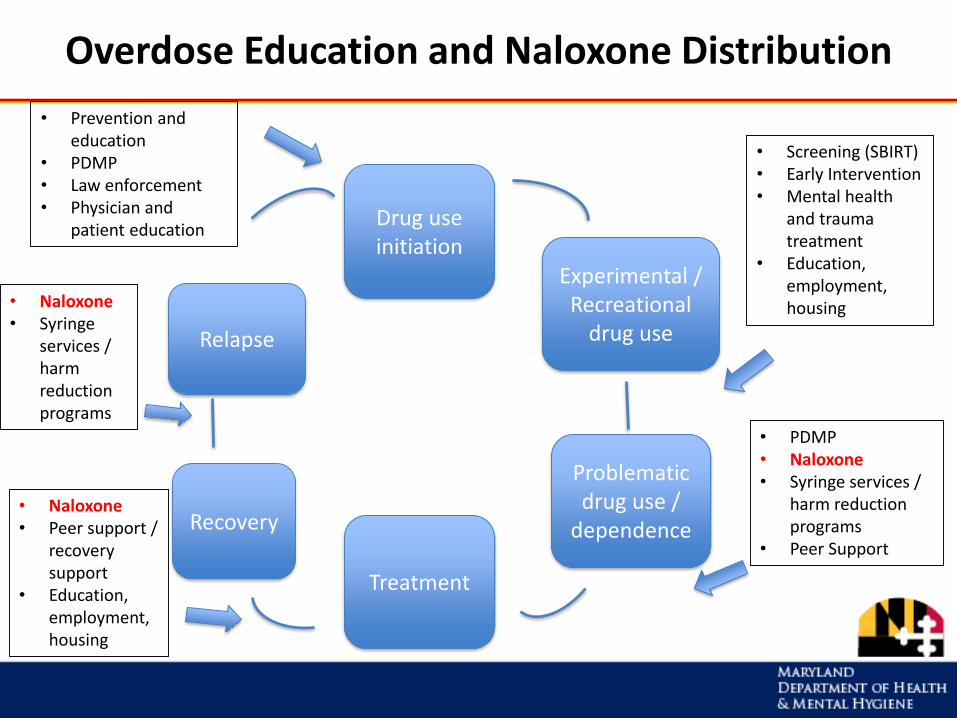
Overdose Education and Naloxone Distribution
Problematic drug use /
dependence
Drug use initiation
Treatment
Recovery
Relapse
Experimental / Recreational
drug use
• Prevention and education
• PDMP• Law enforcement• Physician and
patient education
• Screening (SBIRT)• Early Intervention• Mental health
and trauma treatment
• Education, employment, housing
• PDMP• Naloxone• Syringe services /
harm reduction programs
• Peer Support
• Naloxone• Peer support /
recovery support
• Education, employment, housing
• Naloxone• Syringe
services / harm reduction programs
Harm Reduction Framework
• Goal: minimize the negative effects of drug use for people who use drugs, their families, and their communities
• Harm reduction approaches:– Are rooted in a commitment to public health & human
rights– Combat stigma – Empower people who use drugs to keep themselves
as safe as possible– Meet people where they are – Aim to attain any positive change
(Harm Reduction Coalition, Harm Reduction International)
Context: Overdose Education & Naloxone Distribution
• Overdose education and naloxone distribution (OEND) has been part of the harm reduction landscape for decades
• Originally provided to those at risk for overdose through syringe exchange programs
• OEND provided crucial education on overdose risk
• Naloxone is an empowerment tool for individual and community
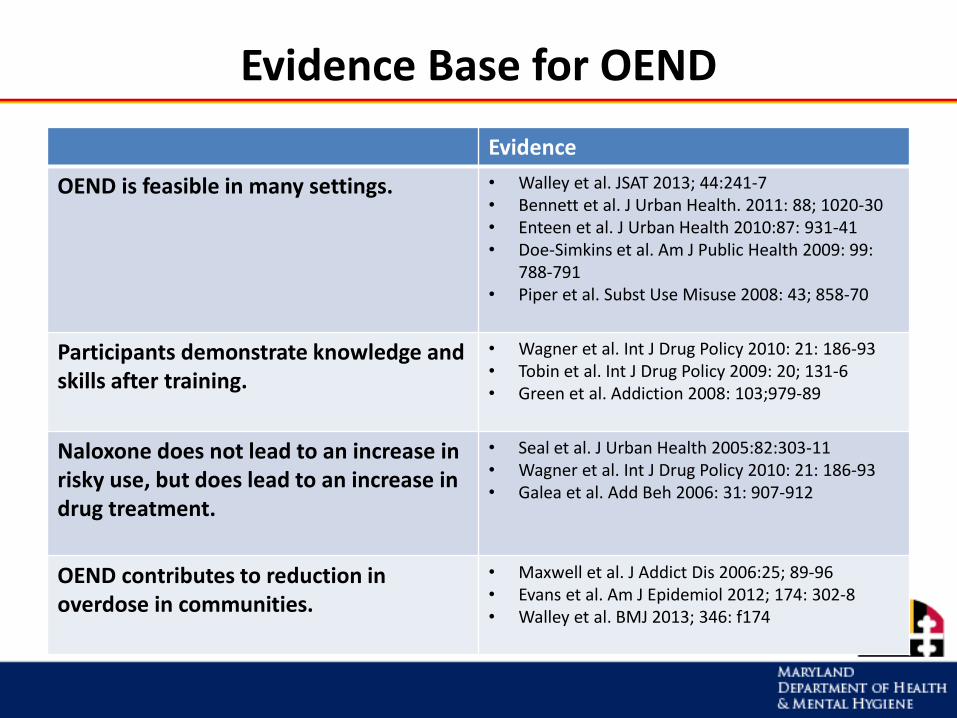
Evidence Base for OEND
Evidence
OEND is feasible in many settings. • Walley et al. JSAT 2013; 44:241-7 • Bennett et al. J Urban Health. 2011: 88; 1020-30 • Enteen et al. J Urban Health 2010:87: 931-41 • Doe-Simkins et al. Am J Public Health 2009: 99:
788-791 • Piper et al. Subst Use Misuse 2008: 43; 858-70
Participants demonstrate knowledge and skills after training.
• Wagner et al. Int J Drug Policy 2010: 21: 186-93 • Tobin et al. Int J Drug Policy 2009: 20; 131-6 • Green et al. Addiction 2008: 103;979-89
Naloxone does not lead to an increase in risky use, but does lead to an increase in drug treatment.
• Seal et al. J Urban Health 2005:82:303-11 • Wagner et al. Int J Drug Policy 2010: 21: 186-93 • Galea et al. Add Beh 2006: 31: 907-912
OEND contributes to reduction in overdose in communities.
• Maxwell et al. J Addict Dis 2006:25; 89-96 • Evans et al. Am J Epidemiol 2012; 174: 302-8 • Walley et al. BMJ 2013; 346: f174
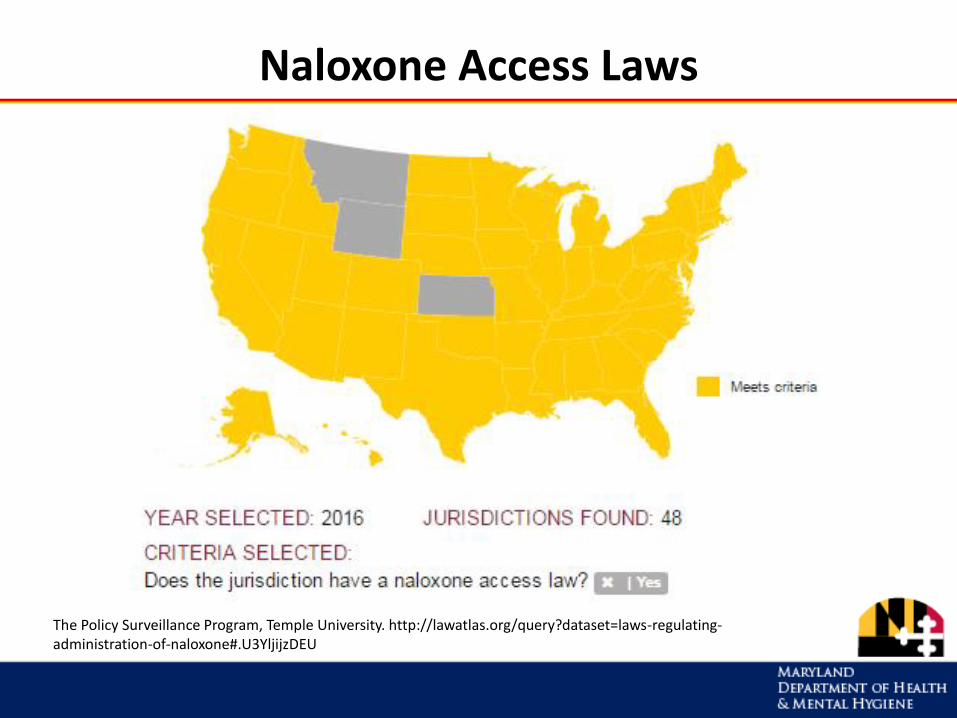
Naloxone Access Laws
The Policy Surveillance Program, Temple University. http://lawatlas.org/query?dataset=laws-regulating-administration-of-naloxone#.U3YljijzDEU
THE MARYLAND OVERDOSE RESPONSE PROGRAM AND THE HOPE ACT
Maryland Overdose Response Program (ORP)
The ORP enables organizations to train and certify individuals most likely to assist someone at risk of dying from an opioid overdose when emergency medical services are not immediately available.
Since FY14:
– 63 programs authorized by DHMH
– 43,683 individuals trained using core curriculum
– 1,634 reported uses
A naloxone kit is provided at the time of training, or the individual can use theirORP certificate to obtain naloxone from a pharmacy under the statewide standing order.
ORP Law and Regulations
ORP = Maryland Overdose Response Program
• Law: Article-Health-General, Title 13, Subtitle 31,
Annotated Code Maryland, §§13-3101 – 3109
• Regulations: COMAR 10.47.08.01-.11 (3/3/14)
Naloxone can also be provided by a physician to any patient
at risk for overdose or likely to witness and respond to an
opioid overdose.
Goals of Maryland Overdose Education and Naloxone Distribution
Reduce overdose death by targeting individuals at risk for overdose and their friends and family through…
• Outreach model
• Peer-delivered training
• Detention center training and dispensing
• Pharmacy-based distribution
• Opioid treatment programs
• Syringe services programs
…to achieve community saturation.
The Heroin and Opioid Prevention Effort (HOPE) and Treatment Act of 2017
• At least 30 bills introduced to combat the opioid crisis
• Proposals focused on prevention, treatment, law enforcement, insurance coverage, public awareness
• Many initiatives from other pieces of legislation merged in the HOPE Act
The Heroin and Opioid Prevention Effort (HOPE) and Treatment Act of 2017
Includes:- Establishing crisis treatment centers for mental health and
substance use crises and a 24/7 health crisis hotline
- Increasing access to opioid addiction treatment medications
- Establishing guidelines for co-prescribing naloxone that are applicable to all licensed healthcare providers
- Developing hospital protocols for discharging a patient treated by the hospital for an overdose or identified as having a substance use disorder
- Increasing access to substance use disorder treatment in local jails and detention centers
- Streamlining ORP operations and increasing access to naloxone
The Heroin and Opioid Prevention Effort (HOPE) and Treatment Act of 2017
Streamlining ORP operations and increasing access to naloxone:
• Removes the ORP certificate requirement
• Affects statewide standing order by allowing any individual to receive naloxone, not just certificate holders
• Will result in naloxone being as close to “over the counter” as possible in Maryland without federal action
Impact to Pharmacists’ Role
• Increased demand for naloxone at pharmacies
• Importance of patient education on naloxone
• Ability to recommend naloxone when prescribing opioids or identifying individuals at risk of overdose
• What else?
OVERDOSE EDUCATION AND NALOXONE “TRAIN THE TRAINER”
Overview
A. What is an Opioid?
B. Recognizing an Opioid Overdose
C. Responding to an Opioid Overdose
D. Information for Trainees
E. Tips for Preventing Opioid Overdose (optional)
F. Suggested Resources for Family & Friends (optional)
WHAT IS AN OPIOID?
Opioids
An opioid is any drug that contains opium (or its derivative).
Opioids can be:
• Natural or synthetic
• Prescription medications or illegal drugs
• Pills, capsules, powder or liquid
• Swallowed, smoked, snorted or injected
About Opioids
Opioids:
• Manage pain, suppress coughs and treat opioid use disorders (addictions)
• Cause feelings of euphoria, contentment and/or detachment
• Have effects lasting from 3 to 24 hours
In excessive amounts, opioids can suppress a person’s urge to breathe.
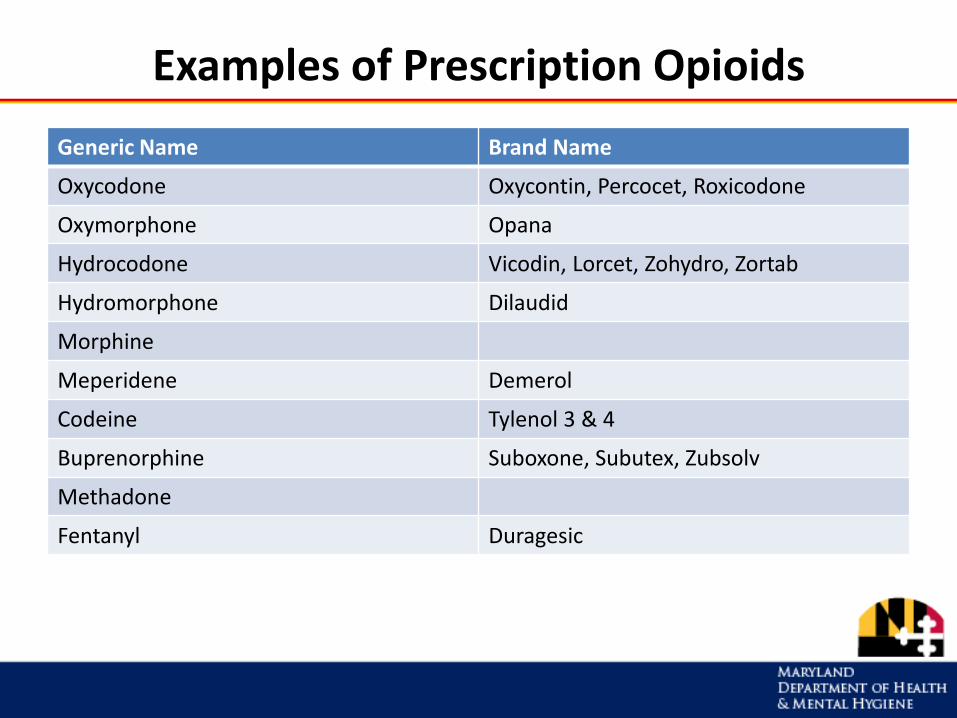
Examples of Prescription Opioids
Generic Name Brand Name
Oxycodone Oxycontin, Percocet, Roxicodone
Oxymorphone Opana
Hydrocodone Vicodin, Lorcet, Zohydro, Zortab
Hydromorphone Dilaudid
Morphine
Meperidene Demerol
Codeine Tylenol 3 & 4
Buprenorphine Suboxone, Subutex, Zubsolv
Methadone
Fentanyl Duragesic
Examples of Illicit Opioids
• Heroin
• Non-pharmaceutical fentanyl– Illicitly produced, synthetic drug
– Pill form packaged to look like prescription medications
– Powder form looks similar to heroin
Fentanyl + heroin can be a deadly combination.
Fentanyl may be hundreds of times more potent than
heroin.
RECOGNIZING AN OPIOID OVERDOSE
What is an Opioid Overdose?
Opioid overdose happens when a toxic amount of an opioid—alone or mixed with other opioid(s), drugs and/or substances—overwhelms the body’s ability to handle it.
Many opioid-related overdoses result from
mixing prescription painkillers or heroin
with benzodiazepines (benzos), cocaine and/or alcohol.
What Leads to Overdose Death?
Respiratory failure
Lack of oxygen in the blood
Vital organs like heart and brain start to fail
Unconsciousness, coma, death
Signs & Symptoms of Opioid Overdose
• Loud snoring or gurgling noises
• Body very limp
• Unresponsive
• Skin pale/gray, clammy
• Lips/fingertips turn blue(ish)
• Pulse slow or erratic
• Breathing very slow, shallow, or not at all
• Unconscious
RESPONDING TO AN OPIOID OVERDOSE
Responding to an Opioid Overdose
1. Rouse & Stimulate
2. Call 911
3. Give Naloxone
4. Further Resuscitation
5. Care for the Person
Step 1: Rouse & Stimulate
• Noise – Shake person’s shoulders and yell:
“[Name!] Are you all right? Wake up!”
• Pain – If no answer, do a sternum rub:
Make a fist & rub your knuckles firmly up and down the breastbone.
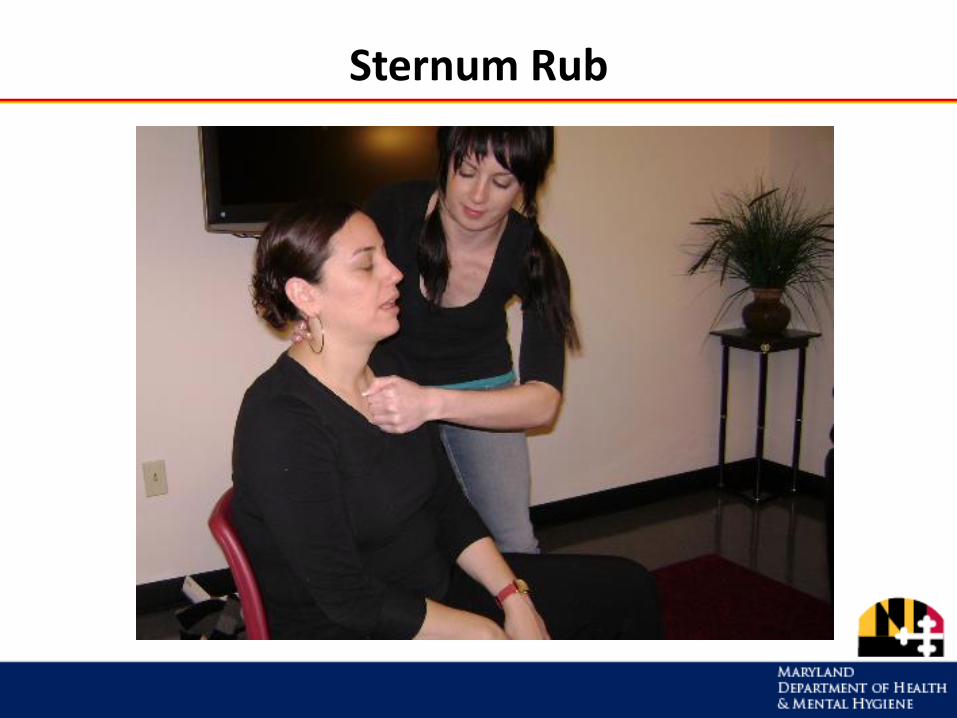
Sternum Rub
Step 2: Call 911
Get emergency medical help for
someone experiencing an overdose!
Why?
• Naloxone is only temporary.
• Person may:– have complications or other health problems
– need more naloxone
• May be a non-opioid overdose situation.
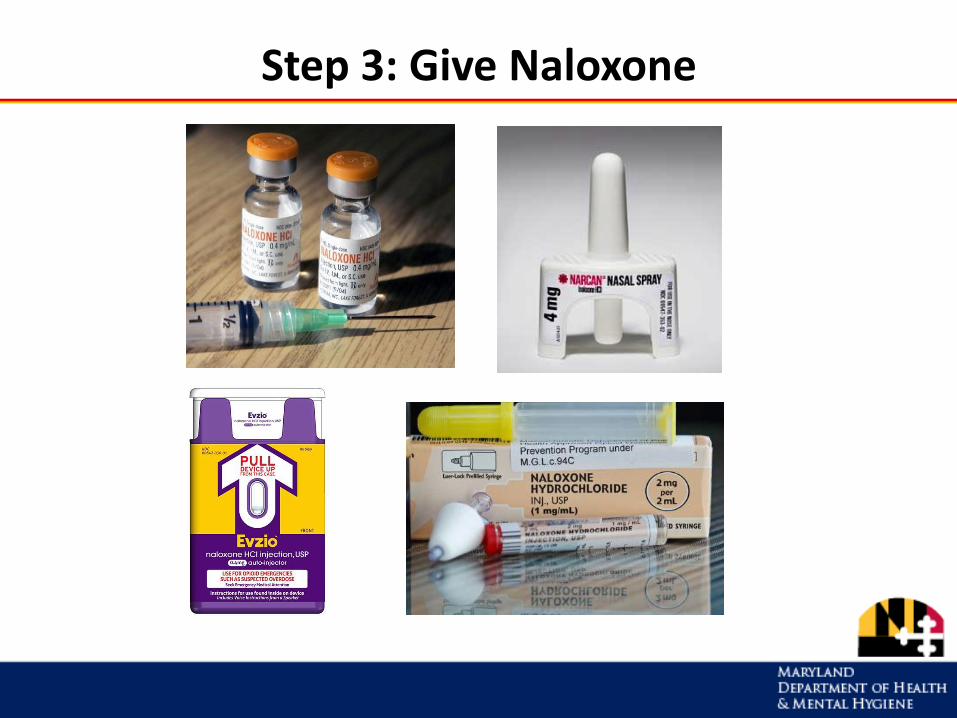
Step 3: Give Naloxone
What is Naloxone?
Naloxone is a medicine that reverses opioid overdose by restoring breathing.
About naloxone:
• Wears off in 30 - 90 minutes
• Safe for children and pregnant women
• Delivery: intramuscular, intranasal or intravenous
• No potential for misuse or getting high
• No effect on someone who hasn’t taken opioids
• Side effects are minimal and rare
Naloxone is only effective in reversing opioid overdoses.
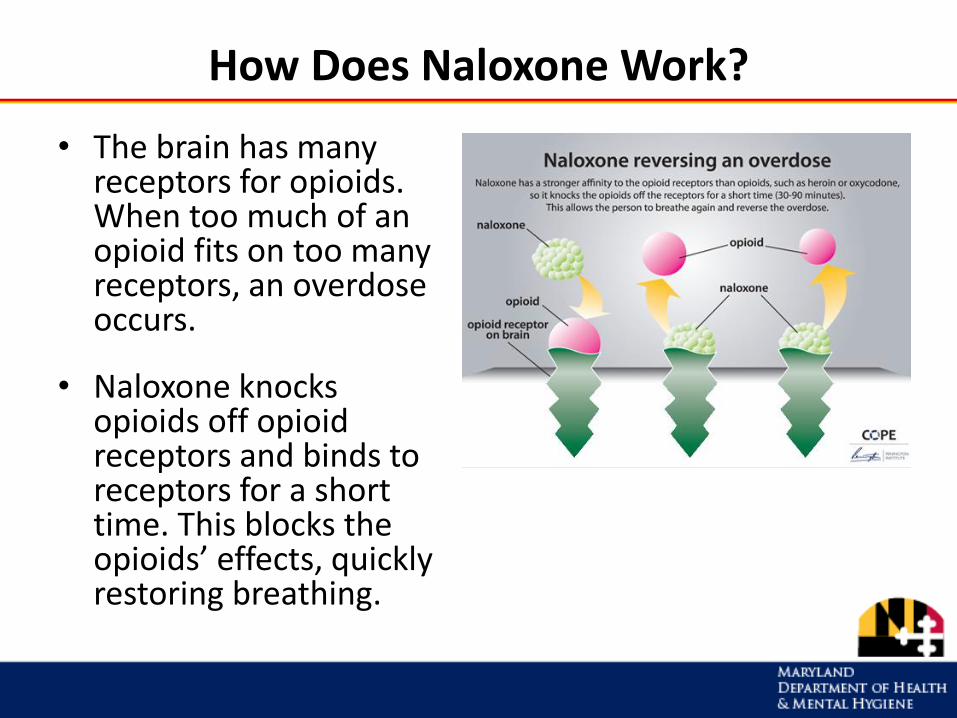
How Does Naloxone Work?
• The brain has many receptors for opioids. When too much of an opioid fits on too many receptors, an overdose occurs.
• Naloxone knocks opioids off opioid receptors and binds to receptors for a short time. This blocks the opioids’ effects, quickly restoring breathing.
Naloxone Storage & Disposal
Storage• Do not attach naloxone to delivery device until ready to use • Store in original package at room temperature• Avoid exposure to light• Keep in a safe place away from children & pets, but easy to
access in case of emergency
Disposal
• Naloxone devices with syringes: dispose as medical sharps (in a rigid container)
• Other devices: dispose in household trash
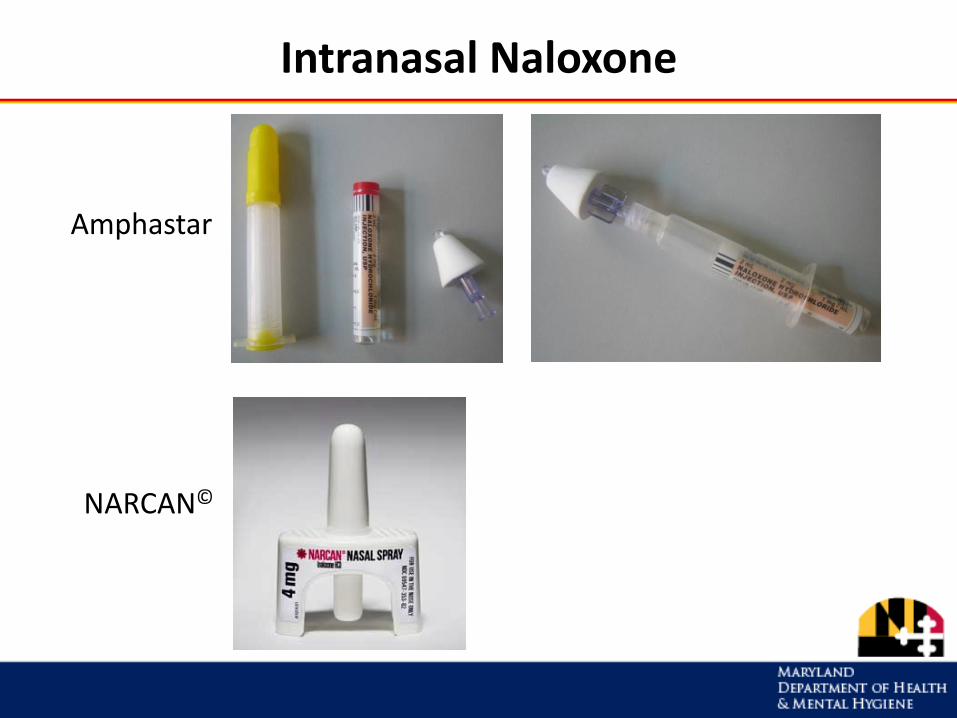
Intranasal Naloxone
Amphastar
NARCAN©
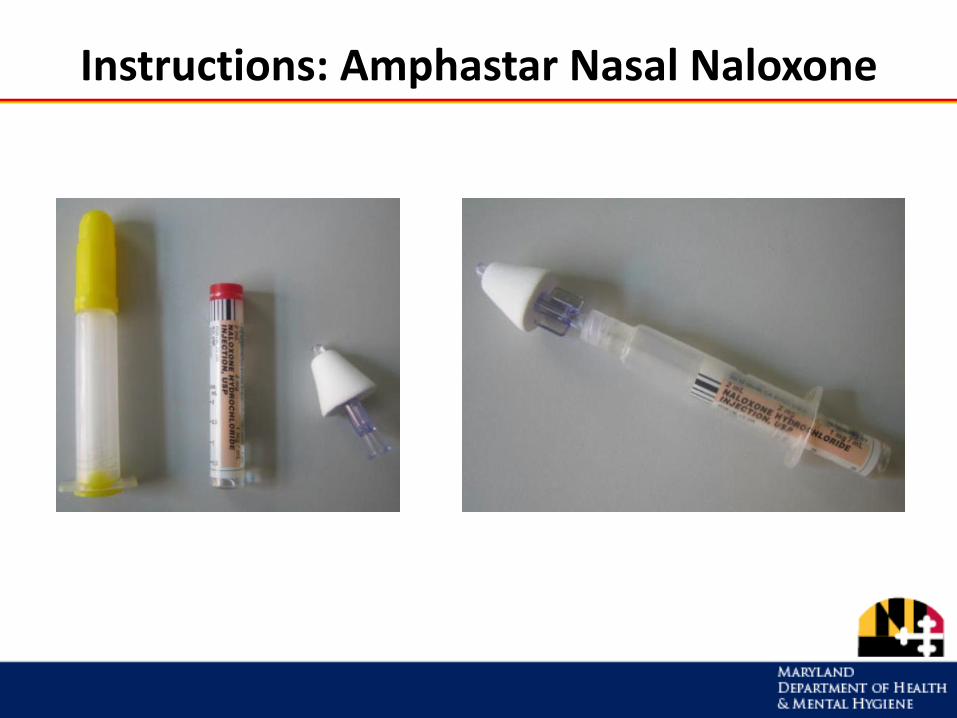
Instructions: Amphastar Nasal Naloxone
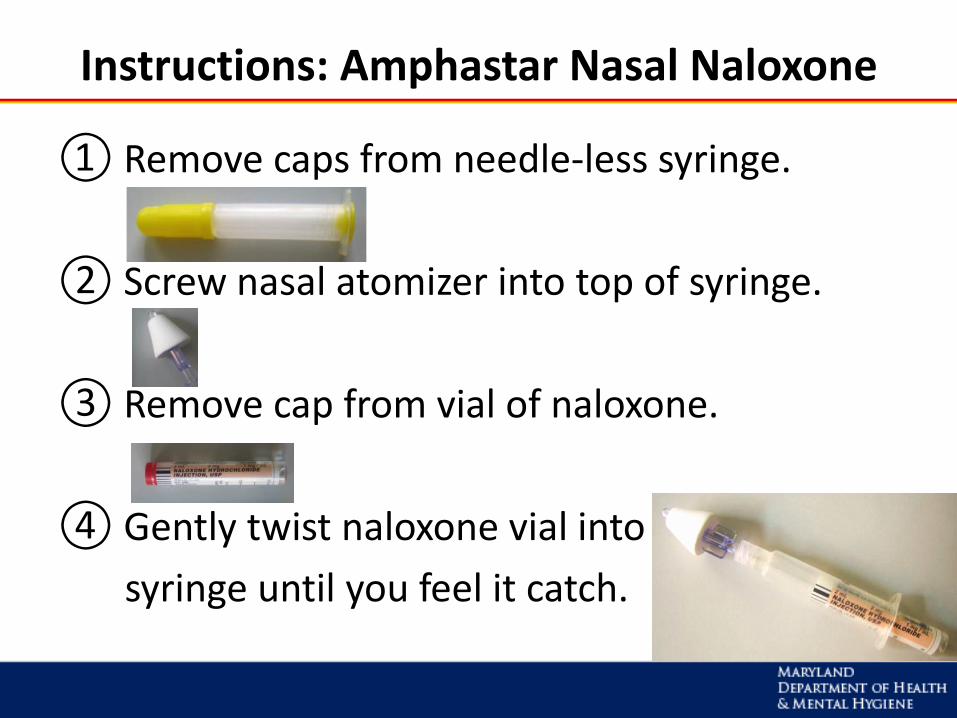
Instructions: Amphastar Nasal Naloxone
① Remove caps from needle-less syringe.
② Screw nasal atomizer into top of syringe.
③ Remove cap from vial of naloxone.
④ Gently twist naloxone vial into
syringe until you feel it catch.
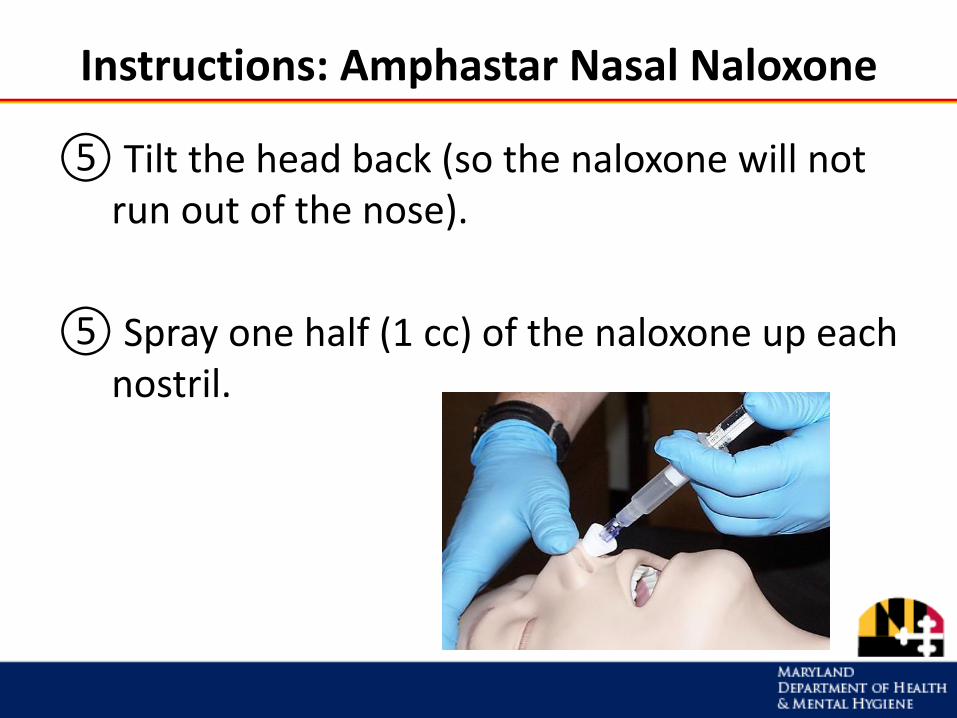
Instructions: Amphastar Nasal Naloxone
⑤ Tilt the head back (so the naloxone will not run out of the nose).
⑤ Spray one half (1 cc) of the naloxone up each nostril.
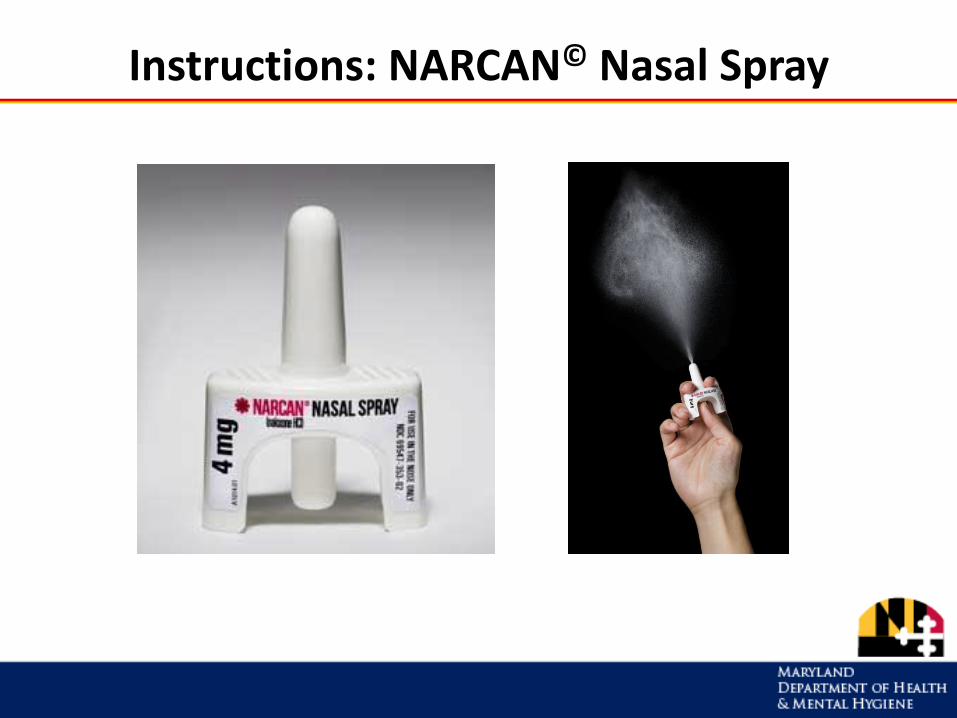
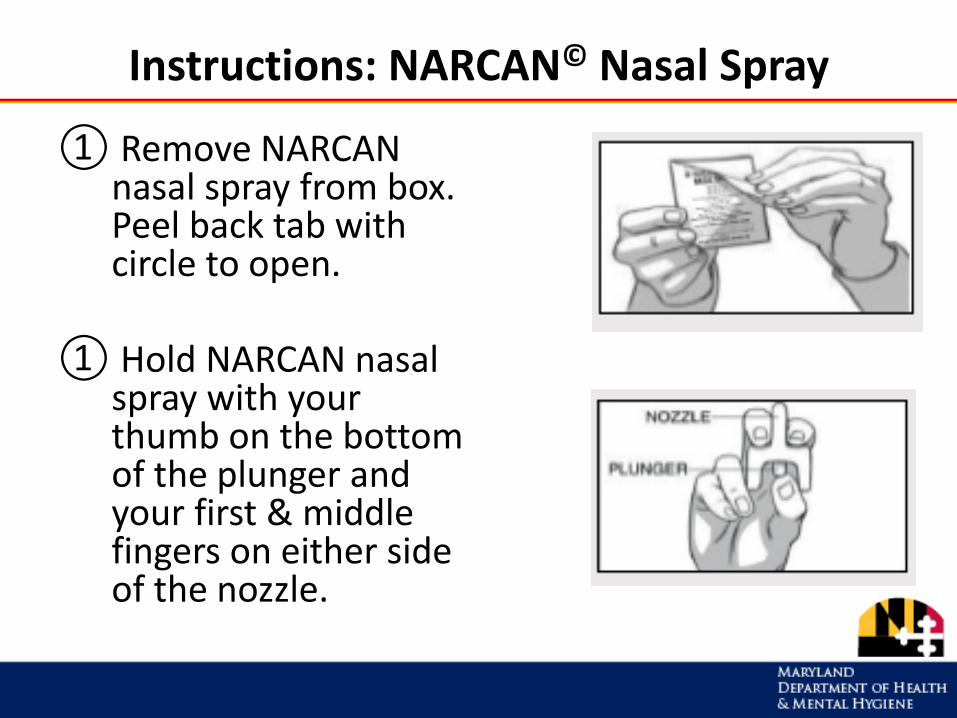
Instructions: NARCAN© Nasal Spray
Instructions: NARCAN© Nasal Spray
① Remove NARCAN nasal spray from box. Peel back tab with circle to open.
① Hold NARCAN nasal spray with your thumb on the bottom of the plunger and your first & middle fingers on either side of the nozzle.
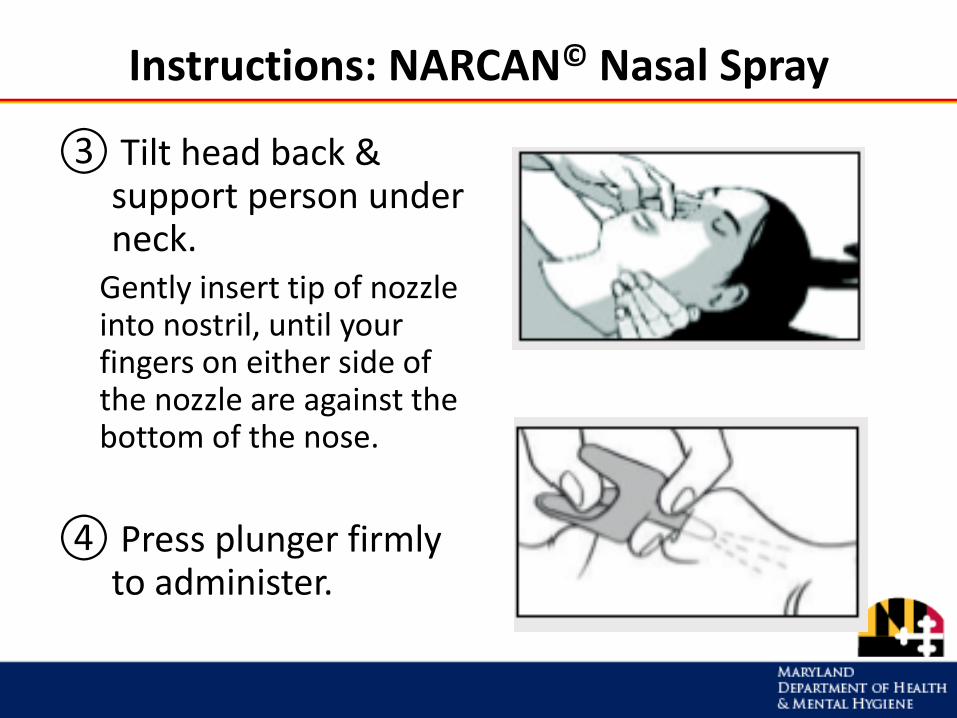
Instructions: NARCAN© Nasal Spray
③ Tilt head back & support person under neck.
Gently insert tip of nozzle into nostril, until your fingers on either side of the nozzle are against the bottom of the nose.
④ Press plunger firmly to administer.
Intramuscular (Injectable) Naloxone
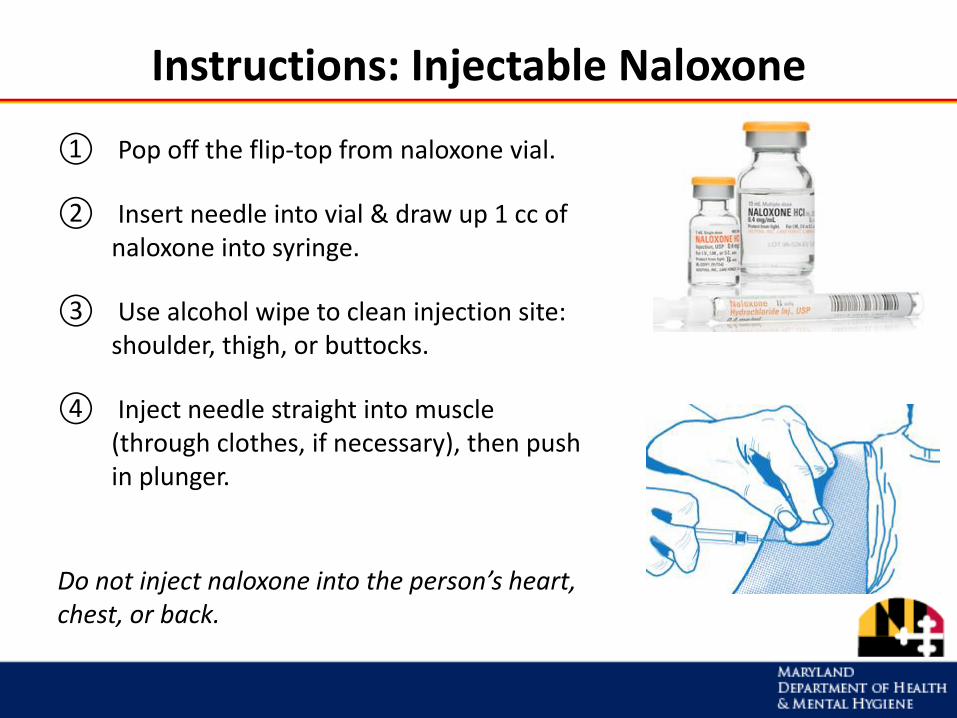
Instructions: Injectable Naloxone
① Pop off the flip-top from naloxone vial.
② Insert needle into vial & draw up 1 cc of naloxone into syringe.
③ Use alcohol wipe to clean injection site: shoulder, thigh, or buttocks.
④ Inject needle straight into muscle (through clothes, if necessary), then push in plunger.
Do not inject naloxone into the person’s heart, chest, or back.
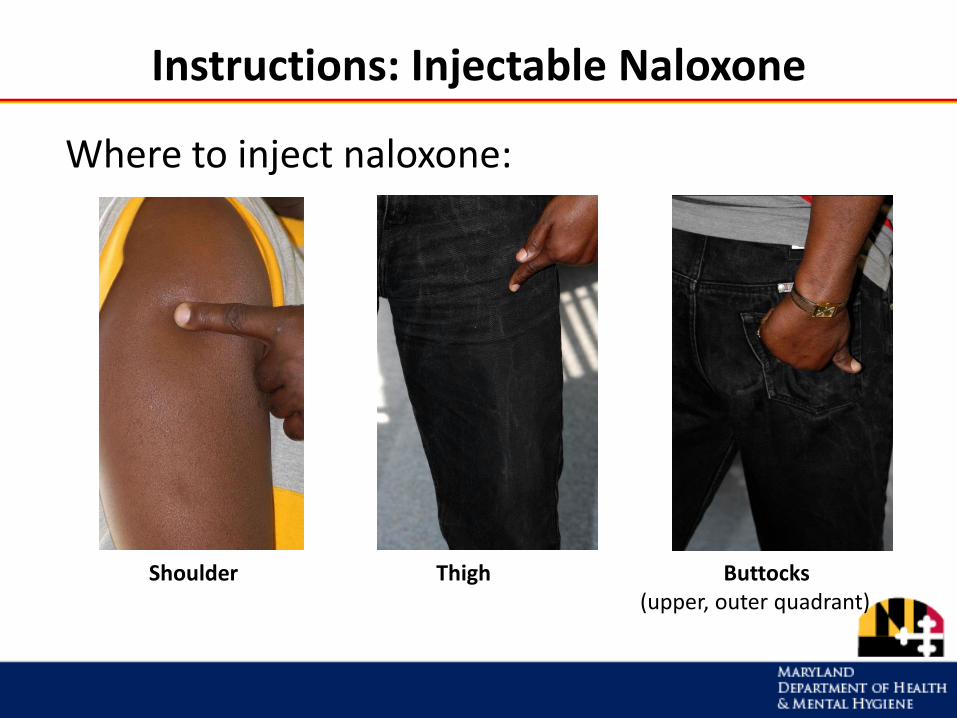
Instructions: Injectable Naloxone
Shoulder Thigh Buttocks(upper, outer quadrant)
Where to inject naloxone:
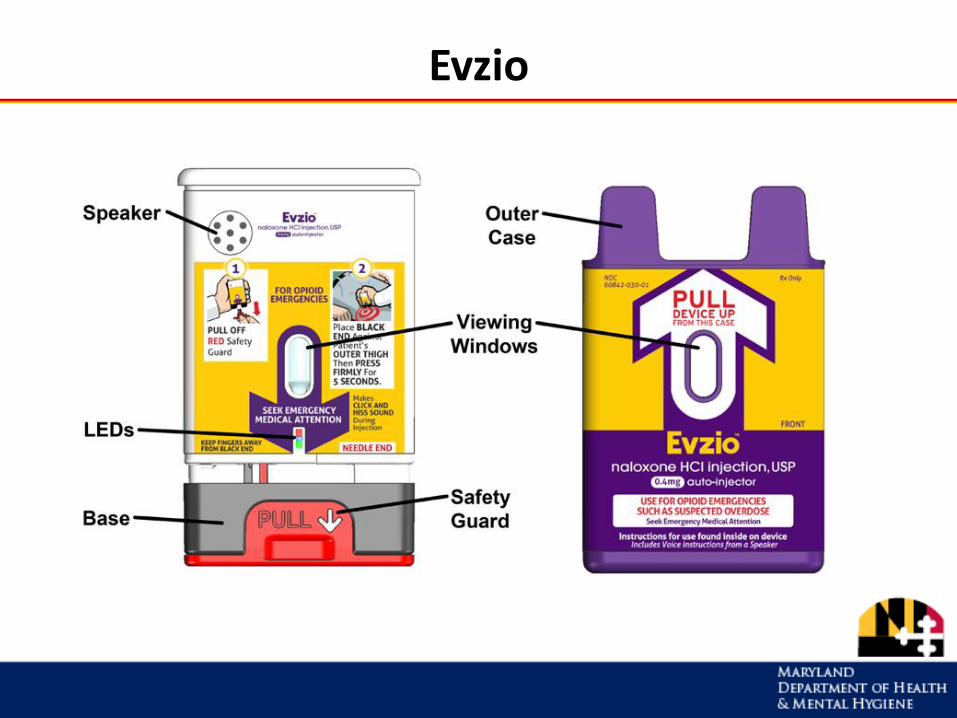
Evzio
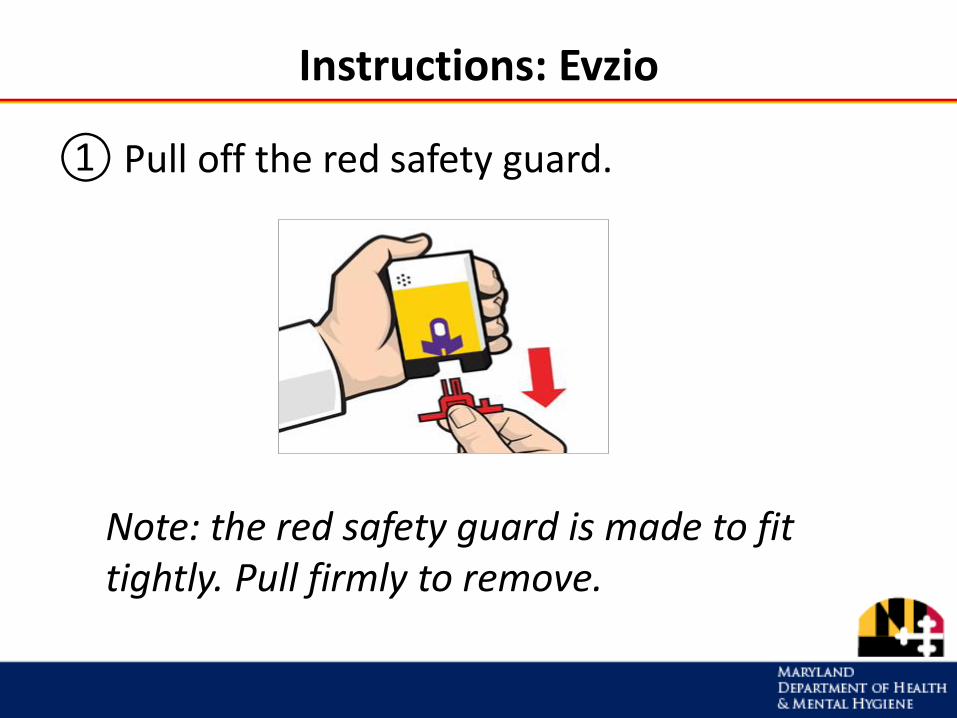
Instructions: Evzio
① Pull off the red safety guard.
Note: the red safety guard is made to fit tightly. Pull firmly to remove.
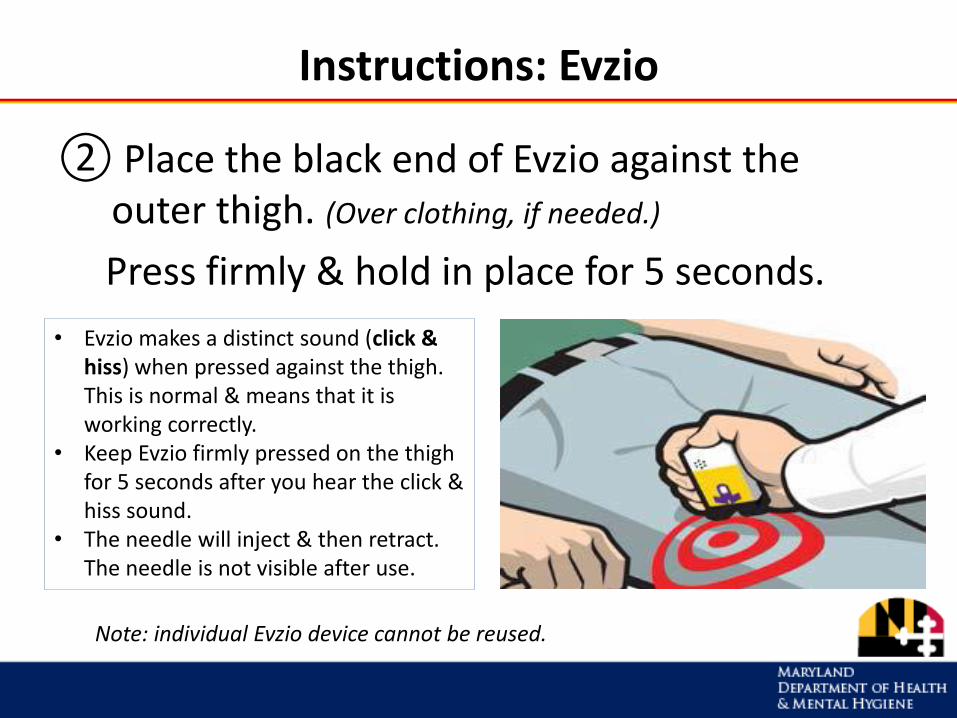
Instructions: Evzio
② Place the black end of Evzio against the outer thigh. (Over clothing, if needed.)
Press firmly & hold in place for 5 seconds.
• Evzio makes a distinct sound (click & hiss) when pressed against the thigh. This is normal & means that it is working correctly.
• Keep Evzio firmly pressed on the thigh for 5 seconds after you hear the click & hiss sound.
• The needle will inject & then retract. The needle is not visible after use.
Note: individual Evzio device cannot be reused.
Instructions: Give Naloxone
• Allow 1 to 3 minutes for the naloxone to work. Continue resuscitation as necessary.
• If breathing is not restored after 2 or 3 minutes, give another dose of naloxone.
Continue resuscitation as necessary.
• Stay with the person & provide care as directed until medical help arrives.
Practice: Naloxone Devices
• When you train people to use naloxone, it’s important to give them a chance to practice using the device (especially if it requires assembly).
Tips:• Injectable naloxone: practice injecting into an
orange.• Amphastar nasal spray: refill the glass vial with
water.• Use expired naloxone for practice kits. Dispose of the
naloxone liquid & refill with water.• Evzio: every package of Evzio includes a training
device and two doses of naloxone. Point out which is the trainer & which is the naloxone.
Step 4: Further Resuscitation
Assess breathing.
If the person is not breathing, or breath is shallow or short:
– Give rescue breaths
OR– Follow the 911 dispatcher’s instructions
OR– Give CPR (chest compressions + rescue breaths) if you are
trained in it
Assess Breathing
Look, listen & feel for breath.
If shallow or short breaths, or not breathing start rescue breathing right away
About Rescue Breathing
Rescue breathing is:
• the quickest way to get oxygen into the body
• one of the most important things you can do to prevent someone from dying from an opioid overdose
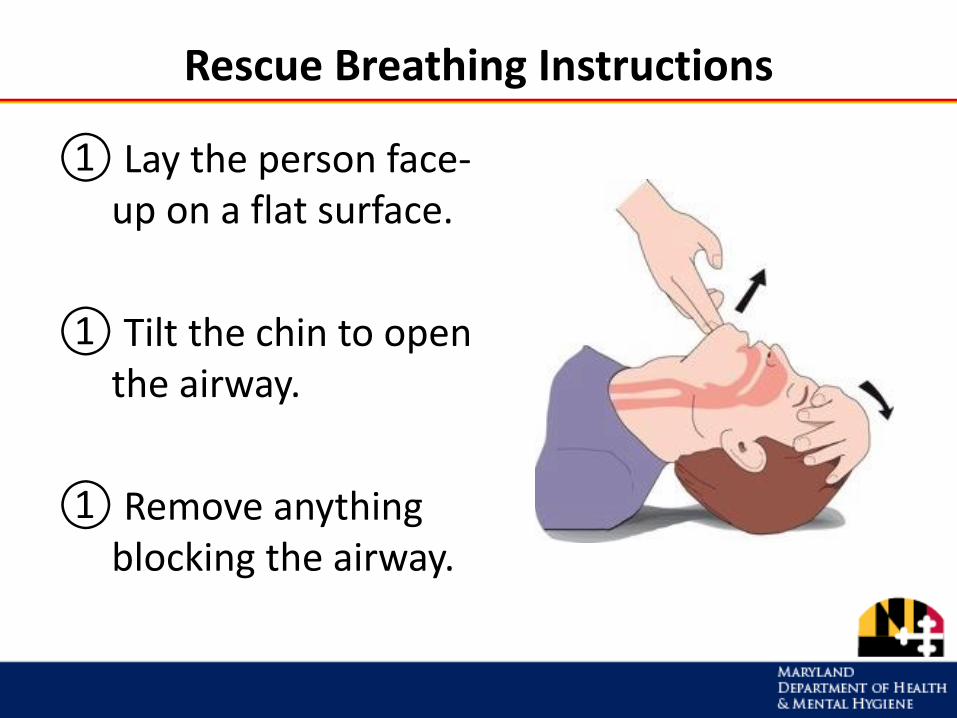
Rescue Breathing Instructions
① Lay the person face-up on a flat surface.
① Tilt the chin to open the airway.
① Remove anything blocking the airway.
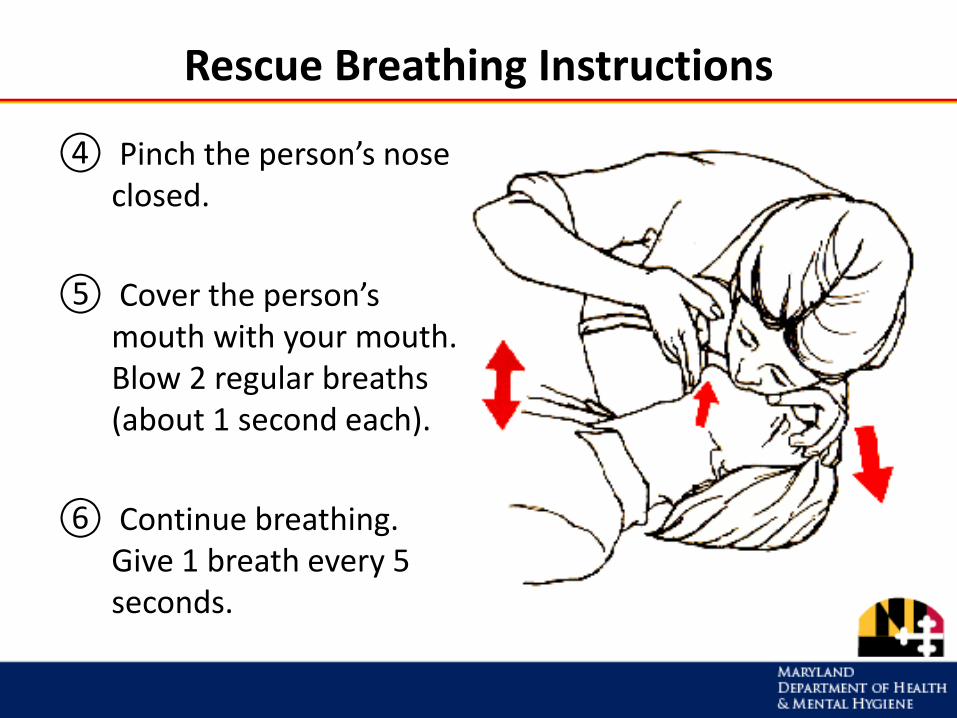
Rescue Breathing Instructions
④ Pinch the person’s nose closed.
⑤ Cover the person’s mouth with your mouth. Blow 2 regular breaths (about 1 second each).
⑥ Continue breathing. Give 1 breath every 5 seconds.
Step 5: Care for the Person
• Stay with the person until medical help arrives.
• If person cannot sit up, put him/her in recovery position.
• Keep person calm.
• Encourage person not to take more opioids.
• If overdose happens again, give another dose of naloxone.
Care for the Person
After receiving naloxone, a person may:
• Feel physically ill or vomit
• Feel withdrawal symptoms (unpleasant but not life-threatening)
• Become agitated and upset
• Have a seizure (this is rare)
Recovery Position
If you have to leave the person (even briefly) put him/her into the recovery position.
This keeps the airway clear and prevents choking or aspiration if vomiting occurs.
Recovery Position
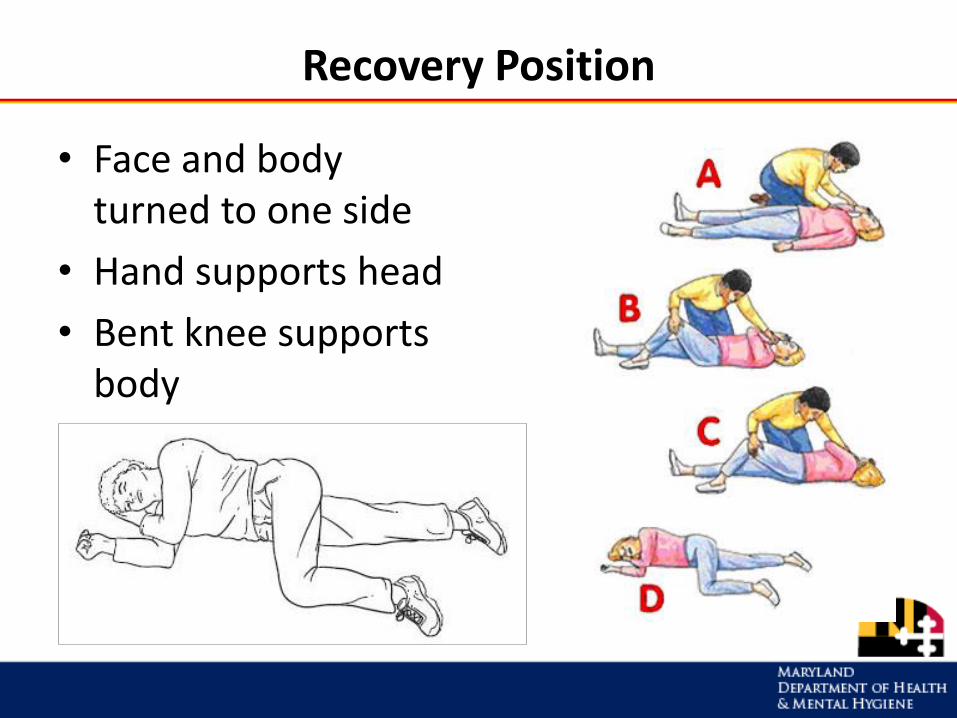
• Face and body turned to one side
• Hand supports head
• Bent knee supports body
If You Administer Naloxone…
• Call the Poison Center within 2 hours: 1-800-222-1222
• Or contact the training entity that issued your certificate
INFORMATION FOR TRAINEES
Good Samaritan Laws in Maryland
These laws are meant to encourage people to:
• call 911 for help when someone overdoses
• administer naloxone
Good Samaritan Laws in Maryland
• A person who helps someone who is overdosing cannot be arrested, charged, or prosecuted for:– Possession of a controlled dangerous substance– Possession or use of drug paraphernalia– Providing alcohol to minors
• Calling 911 in an overdose situation will not affect your parole or probation status.
• You cannot be held liable for a good faith attempt to help someone by administering naloxone.
See: Code of Maryland, Criminal Procedure Article , §1–210, and Health General §13-3110
How to Get Naloxone
• Naloxone may be dispensed directly by a Maryland ORP training entity
• Ask your provider for a prescription for naloxone
• Get naloxone through the statewide standing order at a participating pharmacy (no education, training, or certificate required)
For a list of pharmacies that stock naloxone, go to www.bha.dhmh.maryland.gov/naloxone
TIPS FOR PREVENTING OPIOID OVERDOSE
Activity
Brainstorming Prevention Tips
Opioid Overdose Prevention Tips
For everyone:
• Keep medicine in a safe place, like a locked cabinet. (Naloxone should be kept readily available.)
• Properly dispose of expired or unwanted medications.
• Only take medicine prescribed for you.
• Take medicine only as directed.
• Never share prescription drugs with others.
• If you have breathing problems (like asthma or sleep apnea), check with your doctor before taking opioids.
• Never mix pain medication with alcohol, benzos, sleeping pills, muscle relaxants, anti-nausea drugs, other opioids, or illegal drugs.
Opioid Overdose Prevention Tips
If you use drugs:
• Do not use alone.
• Make an overdose prevention plan. Share it with someone you trust to give you naloxone if needed.
• If you have not used opioids in a few days, your tolerance will be lower and your risk for overdose greater. Use less opioids than you normally would.
• You are at greater risk for overdose if you have overdosed before.
• Always keep naloxone on hand. Tell others where it is.
• Get treatment for drug dependence or addiction.
• Seek professional help if you are depressed.
• Call a crisis hotline or 911.
TAILORING THE TRAINING
Overview: Tailoring the Training
A. Content
B. Training structure1. Quick trainings (5-10 minutes)
2. Classroom-style training (1 hour)
C. Audience1. General public
2. People who use drugs
3. Family & friends
4. Patients of opioid treatment programs
5. Others
Training Content
Patient education for naloxone should include:
1. When to administer naloxone (recognizing the signs & symptoms of opioid overdose)
2. How to administer naloxone (including demonstration)
3. Informing patients to alert others about the medication, how to use it and where it’s kept, as it is generally not self-administered
Quick Trainings
• 10 minutes
• Suggested materials– One-page handout with key info– Practice kits
• Teaching tips– Start with what people know: ask questions and add or
correct info as needed (e.g., “What are some signs of an opioid overdose?”)
– Let people practice assembling and using the naloxone device
– Ask people to teach you
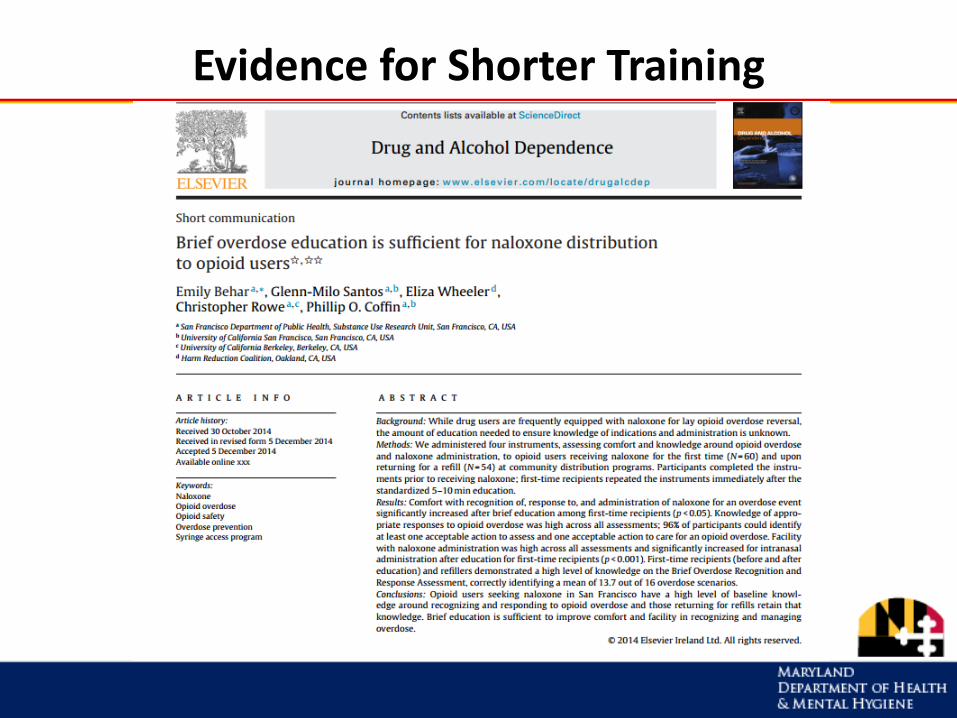
Evidence for Shorter Training
Tailoring to the Audience
• Consider space in pharmacy:
– Can people overhear the training?
– Will the person feel comfortable?
• How much time is needed?
• How much time can you give?
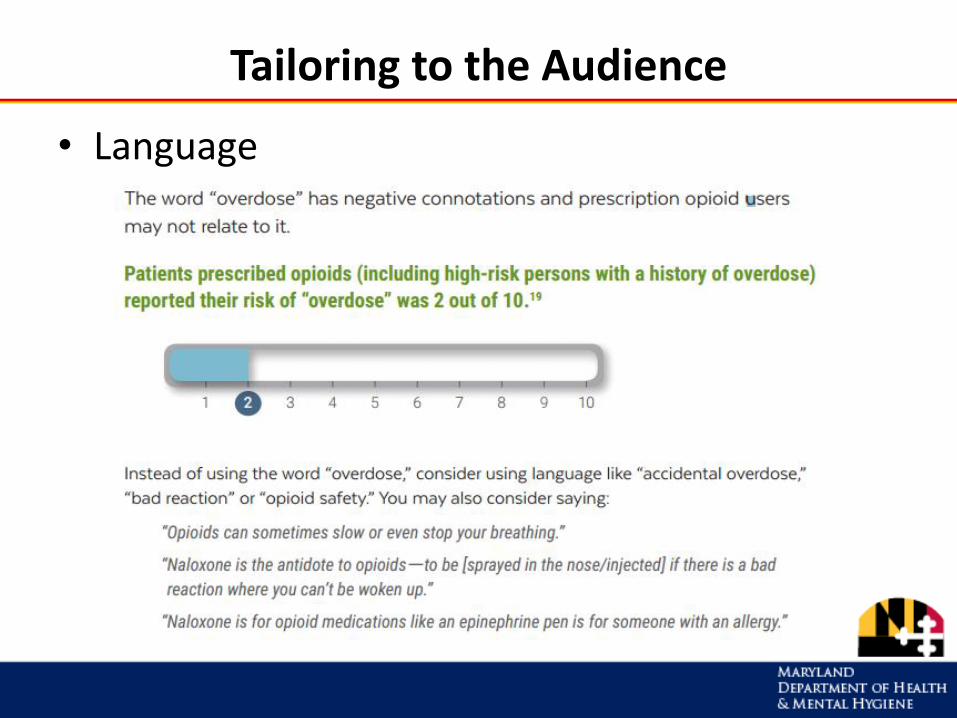
Tailoring to the Audience
• Language
Naloxone Dispensing
• Store and dispense naloxone according to existing protocols
• Using the standing order:
– Keep copy of standing order on file
– Place copy with patient records
– Reference standing order guidance document
Activity: Practice Teach
Pharmacy Barriers
• Reimbursement for training
• Reimbursement for naloxone and atomizer
• Time and space for training
• Liability concerns
• Others?
THE PHARMACISTS’ ROLE: BEYOND OVERDOSE
HIV and Hepatitis C
• 190 people were diagnosed with HIV in Scott County, Indiana, in 2015 after HIV was introduced into a network of people who inject drugs
HIV and Hepatitis C
• Injection drug use is the most significant risk factor in the transmission of HCV, estimated to be the cause of more than 50% of new infections. New HCV cases have risen significantly in recent years among those under 30 years old.
• According to the CDC, there was a 365% increase in new HCV between 2006 and 2012. A study looking at four states, including West Virginia, attributed this rise to injection drug use in suburban and rural settings.
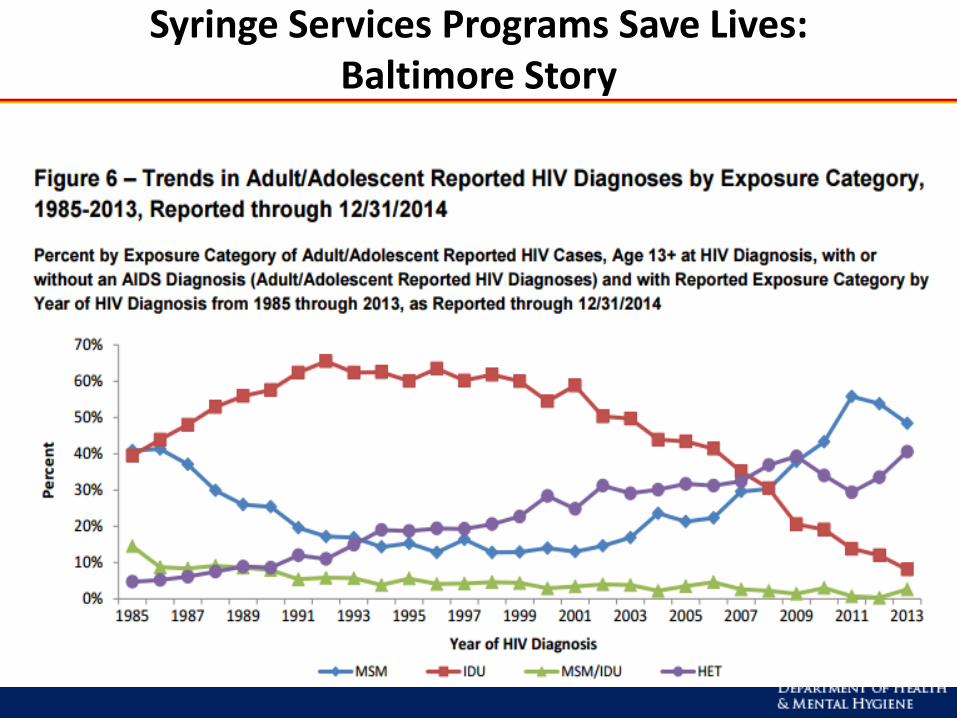
Syringe Services Programs Save Lives: Baltimore Story
Syringe Services Programs: Statewide Expansion
• During the 2016 MD legislative session, a law passed allowing local jurisdictions and community-based organizations in MD to operate syringe services programs
• Prospective programs must apply to DHMH and become authorized by the Department
• Applications from several jurisdictions are currently being developed
Pharmacy Sales of Syringes: Evidence
• After Connecticut changes its prescription laws in 1992 to allow for sales of syringes, needle sharing among persons who inject drugs (PWID) dropped 40%
• One year after Minnesota legalized pharmacy sales of syringes without a prescription, PWID reported a 17% reduction in syringe sharing

Pharmacy Sales of Syringes: Policy Statements
The American Public Health Association supports the prescribing of syringes by health care providers to injection drug users who cannot or will not stop injecting, in order to prevent disease.
The APA encourages Boards of Pharmacy to revise laws and regulations to permit the unrestricted sale or distribution of sterile syringe and needles by or with the knowledge of a pharmacist in an effort to decrease the transmission of blood-borne diseases.
COMAR Says
10.13.08.01 The sale of needles and syringes or other paraphernalia shall be made by the pharmacist only in good faith to patients showing proper identification and indication of need.
MD Board of Pharmacy: April 18, 2007 Meeting
• A constituent question was asked, “Is the prevention of transmission of disease an acceptable indication of need for the sale of needles and syringes?
• The Board voted unanimously to approve the Practice Committee’s response that the prevention of disease is an acceptable indication of need for the sale of needles and syringes.
This means that in all jurisdictions in the state except for Baltimore City, the only legal way to access syringes in through a pharmacy. Pharmacies, therefore, have a vital role in ensuring access to sterile injecting equipment, reducing the spread of HIV and HCV through the sharing of used syringes and to connecting people who use drugs to Syringe Services Programs as they launch.
Case Study: Whitesell Pharmacy
Discussion
• Do Maryland pharmacists know that there is no legal requirement that they ask for a prescription when selling syringes?
• What barriers do you imagine exist to pharmacy sales w/o a prescription?
• How can we work together to recruit pharmacists to the cause of expanding access to sterile injection equipment?
CLOSING
Pharmacist Responses to the Opioid Epidemic
Pharmacists have an essential role in responding to the opioid overdose epidemic by:
• Recommending and providing access to naloxone for patients
• Counseling every recipient of a prescription opioid on safe storage and disposal
• Providing nonprescription syringes for patients who inject opioids to reduce the risks of injection-related infections
“Pharmacy-initiated conversations may have the greatest impact on overdose rates in rural areas.”
Opioids, naloxone, and beyond: The intersection of medication safety, public health, and pharmacy. Bratberg, Jeffrey P. In: Journal of the American Pharmacists Association. March – April 2017, Volume 57, Issue 2, Naloxone Supplement, S1-S184.
Learning Objectives
Participants will:
• Recognize the importance of overdose education and
naloxone for reducing overdose deaths
• Understand the changes to naloxone access in
pharmacies resulting from the HOPE Act
• Apply knowledge to successfully conduct patient
education and dispensing of naloxone under the
statewide standing order
Additional Resources
• Guide to Developing & Managing Overdose Prevention & Take-Home
Naloxone Projects (Harm Reduction Coalition)
http://harmreduction.org/issues/overdose-prevention/tools-best-
practices/manuals-best-practice/
• Naloxone Access: A Practical Guideline for Pharmacists
https://cpnp.org/_docs/guideline/naloxone/naloxone-access.pdf
• SAMHSA-sponsored CE training for pharmacists:
http://www.powerpak.com/course/preamble/112666
• Prescribetoprevent.org
ORP website: http://bha.dhmh.maryland.gov/NALOXONE
Thank you!
Kirsten Forseth, MPH
Overdose Prevention Policy Analyst
Maryland DHMH/ Behavioral Health Administration
Office: 410-402-8659