the impact of neonatal abstinence syndrome on one west virginia community
TRANSCRIPT
The Impact of Neonatal Abstinence Syndrome on one
West Virginia CommunitySean Loudin MD
Disclosures
I have no financial disclosures
Objectives
Discuss the epidemiology of Neonatal Abstinence
Syndrome (NAS) both nationally and regionally
Understand the mechanism of withdrawal
Discuss the management of infants with NAS
Describe our system of care surrounding NAS
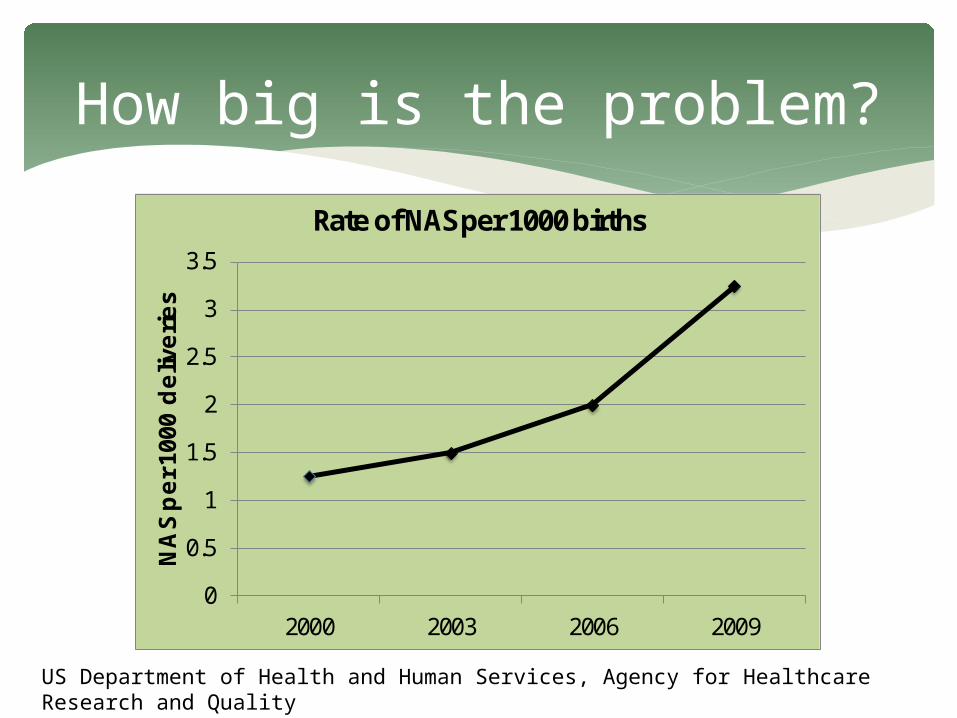
How big is the problem?
0
0.5
1
1.5
2
2.5
3
3.5
2000 2003 2006 2009
NA
S per 1
000
deliv
eries
Rate of NAS per 1000 births
US Department of Health and Human Services, Agency for Healthcare Research and Quality
How big is the problem?
Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009
to 2012Patrick et al. J Perinatology April 2015
Incidence increased from 3.4 to 5.8 per 1000 live births
Geographical variation
East South Central Division (Kentucky, Tennessee,
Mississippi and Alabama) showed 16.2 per 1000 live births
West South Central Division (Oklahoma, Texas, Arkansas
and Louisiana) showed 2.6 per 1000 live births
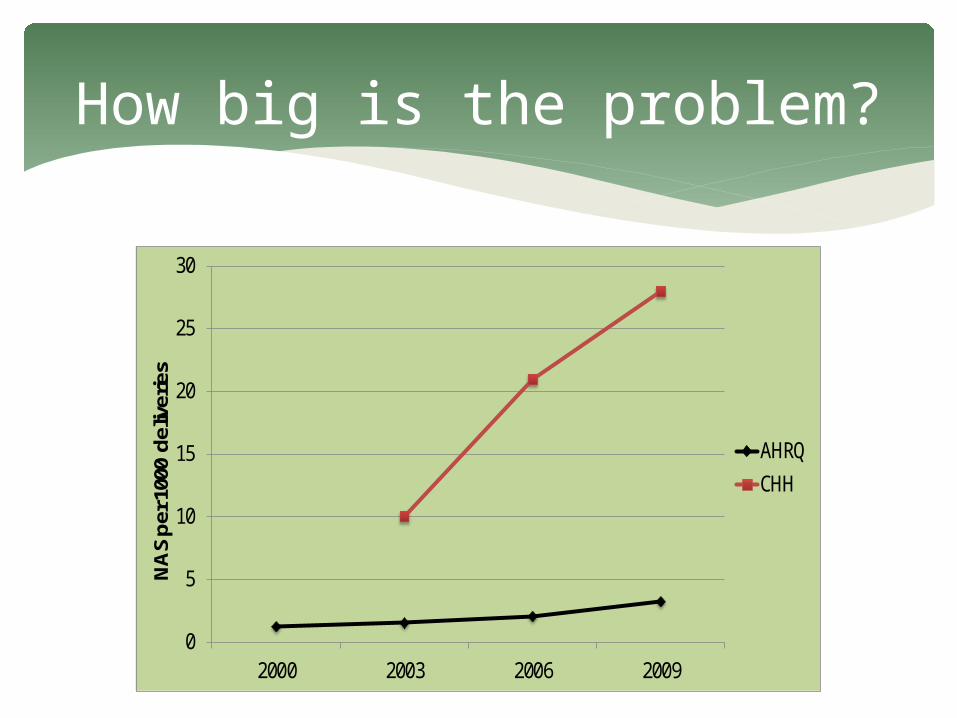
How big is the problem?
0
5
10
15
20
25
30
2000 2003 2006 2009
NA
S pe
r 100
0 de
liver
ies
AHRQCHH
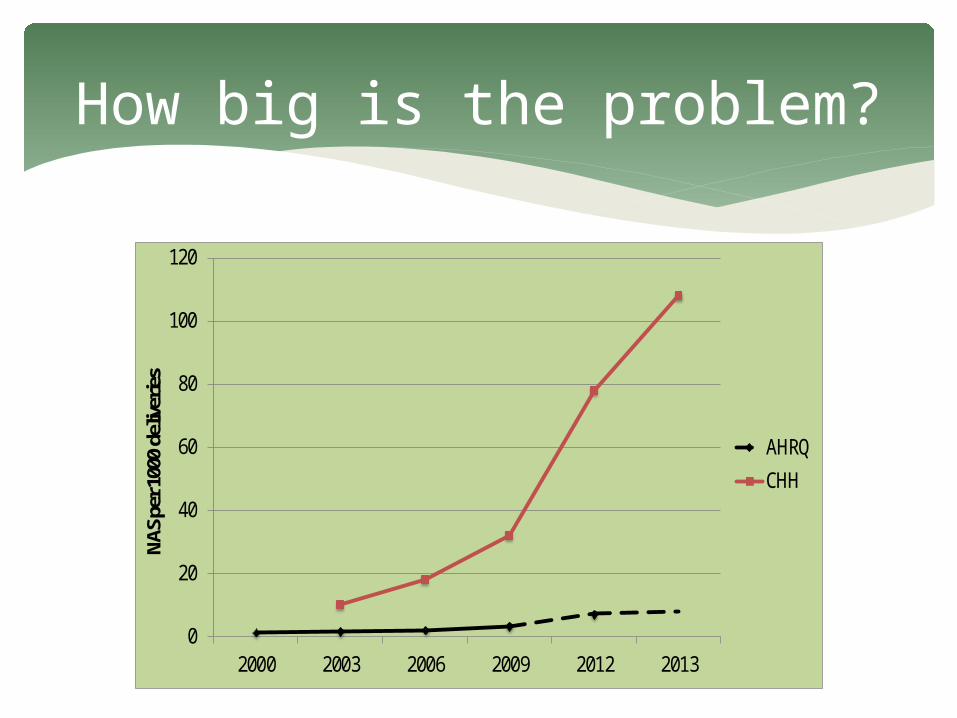
How big is the problem?
0
20
40
60
80
100
120
2000 2003 2006 2009 2012 2013
NAS p
er 10
00 d
elive
ries
AHRQ
CHH
Drugs Causing Withdrawal
Classic NAS due to opiates
Nicotine withdrawal from maternal tobacco
exposure
Alcohol withdrawal and birth defects
Delayed withdrawal secondary to maternal
benzodiazepine or psychotropic medications
Drugs in WV
Prevalence of Drug Use in Pregnant West Virginia Patients
Chaffin et al. 2009
During 1 month period (August 2009) all cords at 8
hospitals were tested
759 total samples collected, 146 (19.2%) were positive for
drugs and/or alcohol
Of the positives 40% marijuana, 28% opiates, 27%
alcohol, 12% bezos, 10% methadone, <1% amphetamines
and 0% were positive for cocaine or buprenorphine
Drugs in WV
Buprenorphine now very prominent
Methadone decreasing in frequency
Marijuana still continues to be used at high rates
Prescription opiates decreasing at time of delivery
Heroin use on the rise
Neonatal Abstinence Syndrome
Passive exposure of the newborn occurs when a
mother uses a neuroactive drug during her
pregnancy
When the infant is deprived of these substances
through the birthing process, a withdrawal
syndrome may develop
Neonatal Abstinence Syndrome
Classic NAS consists of a wide variety of CNS signs
of irritability, GI problems, autonomic signs of
dysfunction, and respiratory symptoms
The hallmark of neonatal withdrawal is a striking
disorder of movement, most aptly termed
“jitteriness”~Volpe 2008
Neonatal Abstinence Syndrome
Autonomic over-reactivity is typically exhibited by
yawning, sneezing, mottling and fever
Cerebral irritation results in an irritable and
hypertonic infant
~Oei and Lui 2007
Pathogenesis of NAS
Pathogenesis of NAS
Endogenous opiates (endorphins, enkephalins and
dynorphins)
Complex interactions between endogenous
opiates and their receptors are important in the
developing brain
Locus ceruleus is a nucleus in the brain stem
involved with physiological response to stress and
panic
Pathogenesis of NAS
Pathogenesis of NAS
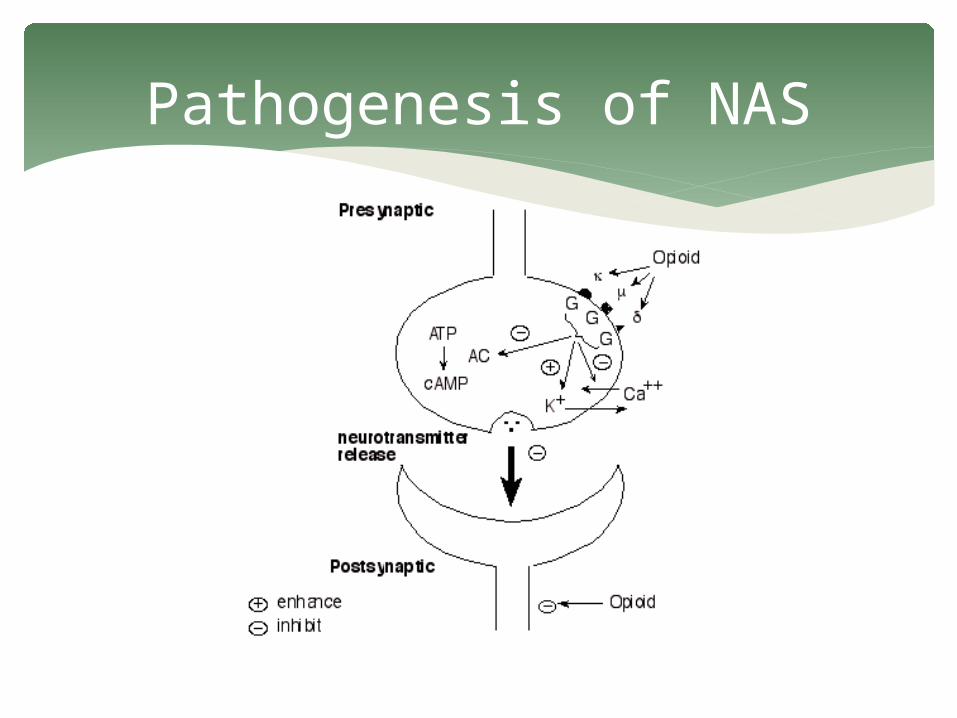
When the opiate is withdrawn, the inhibiting effect
gone
This results in a supranormal increase in
norepinephrine levels, which are the likely cause
of the signs and symptoms of NAS
Pathogenesis of NAS
Disuse Hypersensitivity
A drug may depress certain neural systems
Render the targets hypersensitive to their usual stimuli
Removal of the depressing drug results in a rebound
hypersensitivity of the affected targets
May be caused in part by an increase in synthesis of
certain receptors ~Volpe 2008
Pathogenesis of NAS
Alternate Pathways
Drug may depress a primary neural pathway
An alternate pathway, usually of minor activity,
may become more prominent in attempt to
compensate
When the drug is removed, both pathways may
operate in an additive fashion ~Volpe 2008
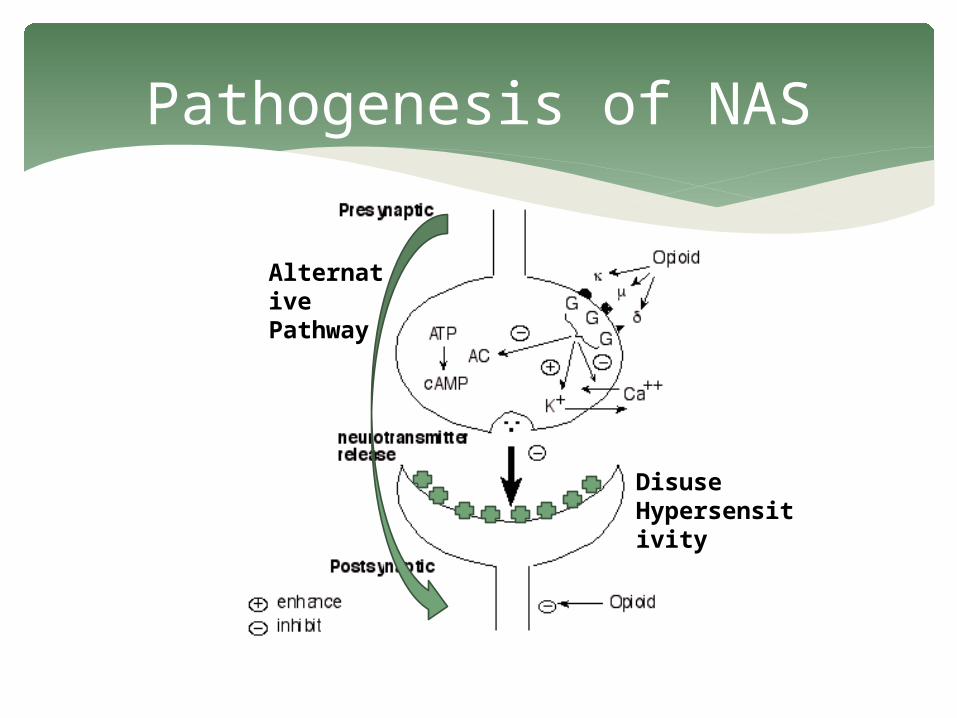
Pathogenesis of NAS
Alternative Pathway
Disuse Hypersensitivity
Identifying Withdrawal
Identifying Withdrawal
2012 AAP Clinical Report: Neonatal Drug Withdrawal Screening for maternal substance abuse is best
accomplished by using multiple methods, including maternal history, maternal urine testing, and testing of newborn urine and/or meconium specimens that are in compliance with local laws.
The duration of urinary excretion of most drugs is relatively short, and maternal or neonatal urinary screening only addresses drug exposure in the hours immediately before urine collection. Thus, false-negative urine results may occur in the presence of significant intrauterine drug exposure.
Identifying Withdrawal
2012 AAP Clinical Report: Neonatal Drug Withdrawal Although newborn meconium screening also may
yield false-negative results, the likelihood is lower than with urinary screening.
The more recent availability of testing of umbilical cord samples may be considered a viable screening tool, because it appears to reflect in utero exposures comparable to meconium screening.
Identifying Withdrawal
13 Panel USDTL Umbilical Cord Testing• Amphetamines (amphetamine, MDA, MDEA, MDMA, methamphetamine)• Cannabinoids (carboxy-THC)• Cocaine (benzoylecgonine)• Opiates (6-MAM, meconin, codeine, hydrocodone, hydromorphone, morphine)• Phencyclidine (phencyclindine) (PCP)• Methadone (EDDP, methadone)• Barbiturates (amobarbital, butalbital, pentobarbital, phenobarbital,
secobarbital)• Benzodiazepines (alprazolam, diazepam, midazolam, nordiazepam,
oxazepam, temazepam)• Propoxyphene (propoxyphene, norpropoxyphene)• Oxycodone (oxycodone, oxymorphone)• Meperidine (meperidine, normeperidine)• Tramadol (tramadol)• Buprenorphine
Identifying Withdrawal
2012 AAP Clinical Report: Neonatal Drug Withdrawal Signs of drug withdrawal can be scored by using a
published abstinence assessment tool. Together with individualized clinical assessment,
the serial and accurate use of a withdrawal assessment tool may facilitate a decision about the institution of pharmacologic therapy and thereafter can provide a quantitative measurement that can be used to adjust drug dosing.
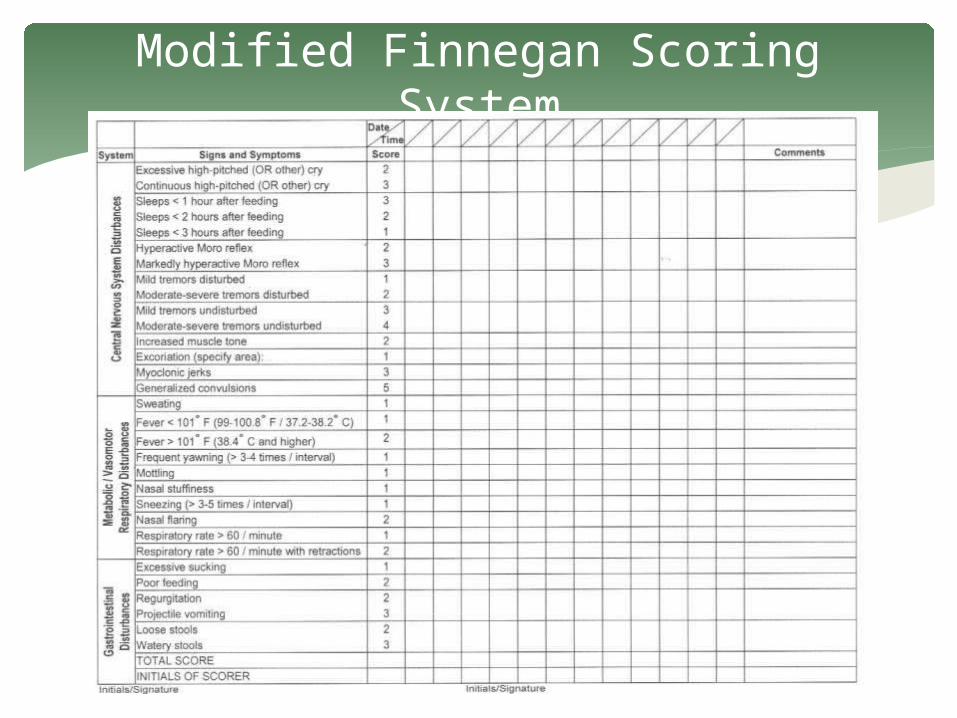
Modified Finnegan Scoring System
Identifying Withdrawal
NAS symptoms in neonates
Tremors
Increased Tone
Autonomic dysregulation
Treatment of NAS

Treatment of NAS
No established optimal treatment
2005 Cochrane reviews suggest lack of high-
quality evidence for any specific treatment
Expert opinion suggest opioids as the class of
agents with the greatest efficacy
Treatment of NAS
2012 AAP Clinical Report: Neonatal Drug Withdrawal
The optimal threshold score for beginning pharmacologic therapy is unknown
Vomiting, diarrhea, dehydration, and poor weight gain are reasons to initiate treatment
Limited evidence as to which medication is the preferred treatment for NAS

Treatment of NAS
Opioid agents used Morphine sulfate Neonatal opium solution Methadone Buprenorphine ???
Adjunct agents Phenobarbital Clonidine

Treatment of NAS
Cabell Huntington Hospital
Methadone inpatient weaning protocol
Clonidine is used for adjunct agent
Weight based-symptom driven 9 step wean
Average length of stay 27-29 days
Utilize the NICU and the Neonatal Therapeutic Unit
Dedicated nursing staff
Before Meds Consider This
2012 AAP Clinical Report: Neonatal Drug Withdrawal Nonpharmacologic supportive measures that
include minimizing environmental stimuli, promoting adequate rest and sleep, and providing sufficient caloric intake to establish weight gain should constitute the initial approach to therapy.
Therapeutic Handling
Reducing Stimuli
Infants react to light, noise, touch, movement, and those individuals around them
Need quiet and calm environment
Attempt to only handle infant for feeding and cluster care
Therapeutic Handling
Swaddling
Calms infants by controlling their bodies
Therapeutic Handling
C position
Bring swaddled baby’s knees up toward chest and chin slightly down
Use this position when feeding and calming infant
Therapeutic Handling
Sway and clap
Stand and rock side to side, the baby will sense head to toe movement
Don’t bounce up and down
Rhythmic patting the infants bottom may aid in relaxation
Therapeutic Handling
Vertical Rock
Seeing the caregivers face may be too stimulating
Turn infant away from you, hold in the C position, and alternate infant slowly up and down
Therapeutic Handling

Feeding
Always feed in a calm, quiet environment
Hold in the C position
Middle finger under chin for support may be necessary
Therapeutic Handling
System of Care

System of Care
Increasing incidence of the neonatal abstinence syndrome in U.S. neonatal ICUs
Tolia et al. NEJM May 2015 NICU admissions from 2004-2013 across the
Pediatrix hospital database 7 cases per 1000 admissions to 27 cases per 1000
admissions length of stay increased from 13 days to 19 days total percentage of NICU days attributed to NAS
increased from 0.6% to 4.0% Infants increasingly received pharmacotherapy (74%
in 2004–2005 vs. 87% in 2012–2013)
System of Care
Different environments for different roles
NICU
Neonatal Therapeutic Unit
Lily’s Place

Places For Treatment
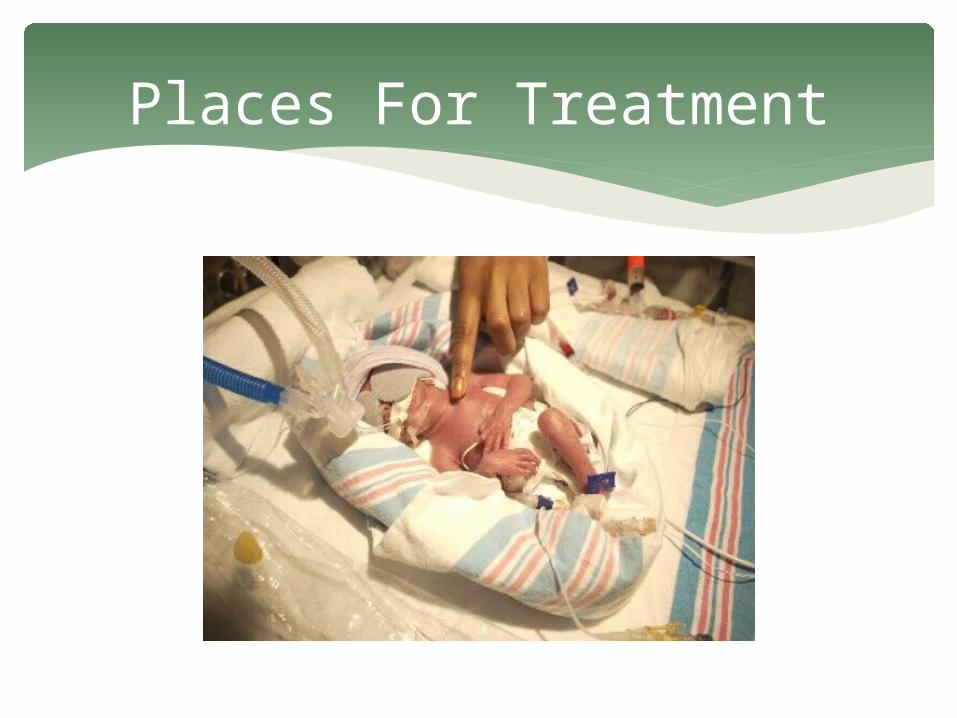
Places For Treatment

Neonatal Therapeutic Unit
Locked unit Unit clerk controls visitors
Places For Treatment
5 rooms 3-4 beds per room Visiting hours 10 am-4 pm
Places For Treatment

Keep room lights dimmed Natural light from window
Places For Treatment

Places For Treatment

Lily’s Place
Established as 501c3 Community support from day 1 Building donated and renovated Nurseries were sponsored Building brought up to code
Lily’s Place
Licensed WV DHHR DEA City of Huntington
West Virginia HB 2999
Lily’s Place

Lily’s Place
Lily’s Place
Future Directions
Future Directions
Increase access to substance abuse resources for
adults Educate various populations about the
consequences of substance abuse Continue to develop innovative ways to treat
patients of all ages Expand research in the field of neonatal
abstinence syndrome
Thank You