the impact of rational emotive behavior therapy...
TRANSCRIPT

1
THE IMPACT OF RATIONAL EMOTIVE BEHAVIOR
THERAPY (REBT) ON CONDUCT DISORDER IN
ADOLESCENT STUDENTS
A final Synopsis of Research carried out for the
Degree of Doctor of Philosophy in Psychology
Research Student
Ms Dawoodi Ghazal Esfnayar Nahid
Guide
Prof. G. Venkatesh kumar
Department of Studies in Psychology
University of Mysore,
Manasagangothri
Mysore - 570 006
2
Introduction
Adolescence is the stage in a person’s life between childhood and adulthood. It is
the period of human development during which a young person must move from
dependency to independence, autonomy and maturity. The young person moves from
being part of a family group to being part of a peer group and to standing alone as an
adult (Mabey and Sorensen, 1995). Generally, the movement through adolescence from
childhood to adulthood involves much more than a linear progression of change. It is
multi-dimensional, involving a gradual transformation or metamorphosis of the person as
a child into a new person as an adult.
With the start of adolescence the nature and behavior of the adolescent also gets
change. Many of the behaviors of adolescents appear unsocial and unsympathetic.
Buhler (1927) defined this period as a negative phase. During the period of adolescence
the boys and girls feel restless, lack of interest in work, feel shy in appearing before
elders, and entertain fear, doubts and frustration. During adolescence the individual
completing changes.
Chronologically, adolescence comes roughly in between the years from 12 to the
early 20s. As defined by the World Health Organization (1992), adolescence is the
period between 10-19 years. The onset of adolescence varies from culture to culture
depending on the socio economics of the country. In this period, great changes occur in
all developmental aspects of the individual. Adolescence is a period of problems. The
main problems of Indian adolescents are to have some economic independence, to get rid
of parental interference, fulfillment of desires, how to spend leisure, and which
philosophy of life he should adopt.
The adolescent is a period of worry and anxieties because with rapid physical and
mental changes he has to face the problem of adjustment in the new environment. He
appears worried, miserable, stormy, intolerant and a rebel. The adolescent is worried
about his social behavior. He tries to escape from others criticisms. This worry gives
birth to undesirable elements in his character, such as: More careless in behavior than
before, less care of others comfort, giving rude replies, short tempered and express
displeasure, interfering in others conversation, quarrelling with guardians for getting
more freedom, beating the younger children in home, serious in thinking, rejecting other
3
people’s advice is acting against it, showing no interest in ideals and principles, getting
irritated on criticism by others.
There are certain problems which are common to adolescents as part of the
developmental processes of this age group; there are also certain kinds of educational,
vocational and social information which can be of help to young people as they grow up.
These may be presented in a group situation and discusses with the realization that their
difficulties are not peculiar to them as individuals, as they often think, but are shared by
fellow students.
Healthy development of adolescents depends on several interactive and complex
factors. They include, the socioeconomic circumstances in which adolescents are born,
the environment in which they grow up, inter-personal relationships within the family,
peer group pressure, value of the community in which they live and opportunities for
education and employment. Despite the multitude of factors, which can influence the
development of adolescents, their mental well being is crucial. Adolescences must learn
to cope with psychological stress, handle peer pressure, deal with their emotions, resolve
conflicts, build bridges with friends and family, develop self-confidence, safeguard
themselves from drug and alcohol as well as cope with other stressors like academic
competition and a hankering for material gains. However, rarely are these sensitive
issues addressed in schools and within families. Psychotherapy in general and group
psychotherapy in particular is a useful way of helping adolescents for whom peer group
values are important.
Emotional and Behavioral Disorders of Adolescents
Although childhood is generally regarded as a carefree time of life, many children
and adolescents experience emotional difficulties growing up.
There are some problems in the social life of adolescents like: rashness of
behavior and un-mindfulness of consequences, desire to reform the society and double
standard of elders. Behavior problems in children and adolescent can be classified into
two major domains of dysfunction, namely externalizing behaviors and internalizing
behaviors (Achenbach & Edelbrock, 1978). The externalizing behaviors are marked by
defiance, impulsivity, hyperactivity, aggression and antisocial features.
4
The internalizing behaviors are evidenced by withdrawal, dysphoria and anxiety.
Behavioral and emotional problems in adolescents affect a significant number of young
people, with considerable personal and societal costs. Estimates of mental health
treatment expenditures for adolescents in the United States are substantial, and
considerably more than for younger children (Ringel & Sturm, 2001). Because these
estimates do not include costs associated with the educational, child welfare, and
juvenile justice systems, or indirect costs of adolescent mental illness such as future lost
wages due to lower educational attainment, they likely underestimate the overall costs
associated with behavioral and emotional problems in adolescents.
Children and youngsters with emotional and behavioral disorders (EBD) are a
vulnerable group in society. Their disorder proofs to be stable and long-term (Fergusson
& Horwood 1992). These children run a high risk of being placed in special education
(Lyon 1996) or in semi-residential specialized care (Eme & Kavanaugh1995). More boys
than girls are affected (3:1 or 4:1) (American Psychiatry Association 1987; Fagot & Leve
1998) and boys show a more violent behavioristic pattern and more externalizing
behavior (Eme & Kavanaugh 1995).
Types of mental, emotional, and behavioral disorders that may occur during
childhood and adolescence are known as: Anxiety Disorders, Severe Depression, Bipolar
Disorder, Attention Deficit Hyperactivity Disorder, Autism, Schizophrenia Learning
Disorders, Conduct Disorder, Eating Disorders. All can have a serious impact on a
child's overall health. Some disorders are more common than others, and conditions
range from mild to severe. Often, a child has more than one disorder (U.S. Department of
Health and Human Services, 1999).
Young people (aged 10–19 years) comprise more than a fifth of India’s
population – an estimated 230 million people (Registrar General of India1996). Although
adolescent health has gained increasing prominence in India’s national health policies,
the focus has been on reproductive and sexual health concerns. Despite reports showing
that suicide is a leading cause of death in young people in India (Aaron R, Joseph A,
Abraham S, Muliyil J, George K, Prasad J, Minz S, Abraham VJ, Bose A, 2004), mental
health has been a low priority in health policy for adolescents. The few published studies
from India have reported prevalence of mental disorders from 2.6% to 35.6% (Srinath S,
Girimaji SC, Gururaj G, Seshadri S, Subbakrishna DK, Bhola P, Kumar N 2005) ;
5
(Verghese A, Beig A.1974 ) . Although comparability between the findings of these
studies is limited owing to methodological factors (Ford T, Goodman R, Meltzer H,
2003), one reason for the wide variation in rates could be the strong influence of social,
cultural and environmental factors on the risk of mental disorders in adolescents.
Adolescents with Conduct disorder as an Emotional and Behavioral Problem
The term conduct disorder (CD) refers to a persistent pattern of antisocial
behavior in which the individual repeatedly breaks social rules and carries out aggressive
acts that upset other people. DSM-IV mentions CD as one of the most frequently
diagnosed conditions in outpatient and inpatient mental health facilities for children. CD
has been separated from the adult diagnosis of antisocial personality in order to
acknowledge what psychiatrists believe to be a greater potential for change in the young.
CD has been classified along with oppositional defiant disorder and attention-
deficit hyperactivity disorder (ADHD) in the attention-deficit and disruptive behavior
disorders section of DSM-IV-TR. The essential feature of CD is a repetitive and
persistent pattern of behavior in which the basic rights of others or major age-appropriate
societal norms or rules are violated. Since its inception in DSM-III, the diagnosis of CD
has undergone several modifications. DSM-IV-TR lists 15 criteria grouped into 4 major
categories: (i) aggression to people and animals; (ii) destruction of property; (iii)
deceitfulness or theft; and (iv) serious violations of rules. Three (or more) of the criteria
should have been present for the last 12 months, with at least one criterion present in the
past 6 months.
The disturbance in behavior should cause clinically significant impairment in
social, academic, or occupational functioning. If the individual is 18 years or older, the
criteria for antisocial personality disorder should not be met. Since the criteria for the
diagnosis of CD vary widely, its manifestations at different developmental stages differ
and because the databases of different studies are not uniform, the prevalence estimates
reported in various studies vary widely. At one end lies the study of Esser and colleagues
(1990) reporting a prevalence of 0.9%, while at the other end is the study by Kashani et
al (1987), reporting a prevalence of 8.7%. DSMIV reports prevalence in males of 6%-
10% and in females of 2%-9%.
6
Psychotherapy
Psychotherapy is an interpersonal, relational intervention used by trained
psychotherapists to aid clients in problems of living. This usually includes increasing
individual sense of well-being and reducing subjective discomforting experience.
Psychotherapy can be defined as a means of treating psychological or emotional
problems such as neurosis or personality disorder through verbal and nonverbal
communication. It is the treatment of psychological distress through talking with a
specially trained therapist and learning new ways to cope rather than merely using
medication to alleviate the distress. It is done with the immediate goal of aiding the
person in increasing self-knowledge and awareness of relationships with others.
Psychotherapy is carried out to assist people in becoming more conscious of their
unconscious thoughts, feelings, and motives. Psychotherapy's longer-term goal is making
it possible for people to exchange destructive patterns of behavior for healthier, more
successful ones.
Group Psychotherapy for Adolescents
Adolescents are social creatures, in the midst of learning their social skills, and
are often more trusting of others their own age than of adults. This makes the group
therapy setting an ideal choice when counseling becomes necessary for this age group.
They are excellent at being able to learn from one another while observing and teaching
appropriate skills as they grow.
The group is a natural setting for adolescents. They are taught in groups, live in
groups, and often play in groups. Group therapy adolescents is an ideal choice, as social
interaction is a key aspect of the developmental process, and as suggested by Bandura
(1989) most social learning takes place by observing others and the results of their
actions. Leader (1991) states that group therapy for adolescence provides the therapeutic
environment where they can work through interpersonal problems and examine the four
basic identity questions: Who am I? With whom do I identify? What do I believe in?
And where am I going?.
7
REBT as Psychotherapy for Adolescents
Rational emotive behavior therapy (REBT) is an active-directive, solution-
oriented therapy which focuses on resolving emotional, cognitive and behavioral
problems in clients, originally developed by the American psychotherapist Albert Ellis.
REBT is one of the first forms of cognitive behavior therapy and was first expounded by
Ellis in 1953. Fundamental to REBT is the concept that emotional suffering result
primarily, though not completely, from our evaluations of a negative event, not solely by
the events per se. In other words, human beings on the basis of their belief system
actively, though not always consciously, disturb themselves, and even disturb themselves
about their disturbances.
In the present study conduct disorder (a sub-type of emotional and behavioral
disorder) is taken as a dependent variable to see whether there would be any change in
them through REBT group psychotherapy.
Importance of Present Study
The unique mental health issues of children have long been a public policy
concern as well as a focus of psychological research and practice. It is widely
recognized that children and adolescents’ mental health problems differ from those of
adults, and failure to treat such problems can potentially lead to later difficulties. Based
on this knowledge, it is disturbing to know that a more effective system has not been
developed to treat children and adolescents’ mental health issues (Saxe, Cross, &
Silverman, 1988). General agreement exists that over 11% of children and adolescents
(approximately 6 to 8 million) have a mental health problem requiring treatment.
However, less than half of this population receives the full range of necessary and
appropriate services to treat their mental health problems effectively (Saxe, Cross, &
Silverman, 1988). The purpose of this study was to examine the effect of Rational
Emotive Behavior Therapy (REBT) on treatment of Conduct Disorder, as a disruptive
behavior disorder, on adolescents for a better help in their mental health issues.
Problem
The Impact of Rational Emotive Behavior Therapy (REBT), on Conduct
Disorder in Adolescent Students.

8
Purpose of the study
Conduct disorder in adolescents is a serious and common mental disorder. Rarely
studies have been reported on adolescents with conduct disorder in India. No adequate
research data have been reported on the treatment of adolescents with emotional and
behavioral problems.
The present study was designed to assess the effectiveness of group Rational
Emotive Behavioral Therapy (REBT) on the treatment of adolescent students suffering
from conduct disorder. The findings may help us develop a better treatment for
adolescents with conduct disorder.
OBJECTIVES
1- To study the impact of Rational-Emotive Behavior Therapy (REBT) on conduct
disorder.
2- To understand the impact of Rational-Emotive Behavior Therapy (REBT) on
other emotional and behavioral disorders co-morbid with conduct disorder.
3- To understand the Gender (Boys and Girls), and Age difference (Early and Late
Adolescents) if any in response to REBT with the regard to effectiveness of
REBT on Conduct Disorder.
Research design
An experimental/control research design was used to examine the impact of
Rational-Emotive Behavior Therapy (REBT) on conduct disorder. In this study, the
control group (CG) was only observed and was exposed to their day to day usual life.
The experimental group was exposed to intervention of Rational-Emotive Behavior
Therapy for seven sessions in seven weeks. The research hypothesizes were tested
statistically.
VARIABLES OF THE STUDY
Dependent Variables
1. Conduct Disorder
Independent Variable

9
1. Rational Emotive Behavior Therapy (REBT)
Biographical Variable
1. Gender- Boys and Girls
2. Age-Early and Late adolescents
Additional Variables Shown by DSM Scales
1- Affective Problems
2- Anxiety Problems
3- Somatic Problems
4- Attention Deficit/Hyperactivity Problems
5- Oppositional Defiant Problems
6- Conduct Problems
Additional Variables Shown by Syndrome Scales
1- Anxious/ Depressed
2- Withdrawn Depresses
3- Somatic Complaints
4- Social Problem
5- Thought Problems
6- Attention Problems
7- Rule-Breaking Behavior
8- Aggressive Behavior
9- Other Problems
10- Internalization
11- Externalization
Additional Variables Shown by Social Competency Scales
1- Activities Scale
2- Social Scale
3- Academic Performance
10
4- Total Competence Score
HYPOTHESES
Hypothesis 1
Rational Emotive Behavior Therapy (REBT) has a positive impact on treatment
of Conduct Disorder.
Hypothesis 2
Rational Emotive Behavior Therapy (REBT) has a positive impact on treatment
of additional variables of DSM Scale.
Hypothesis 3
Rational Emotive Behavior Therapy (REBT) has a positive impact on treatment
of additional variables of Syndrome Scale.
Hypothesis 4
Rational Emotive Behavior Therapy (REBT) has a positive impact on reduction
of Internalizing and Externalizing Groups of Syndromes.
Hypothesis 5
Rational Emotive Behavior Therapy (REBT) has a positive impact on reduction
of scores on Total Problem Score.
Hypothesis 6
Rational Emotive Behavior Therapy (REBT) has a positive impact on increasing
of Total Competency Score.
Hypothesis 7
There is a significant difference of age groups (Early and Late Adolescence) in
response to the REBT with the regard to:
a) Conduct Disorder
b) DSM-Oriented Problems
c) Syndrome Problems
d) Internalizing- Externalizing Groups
e) Total Problem Scores
11
f) Total Competency Score
Hypothesis 8
There is a significant difference of gender groups (Boys and Girls) in response to
the REBT with the regard to:
a) Conduct Disorder
b) DSM-Oriented Problems
c) Syndrome Problems
d) Internalizing- Externalizing Groups
e) Total Problem Scores
f) Total Competency Score
SAMPLE
A stratified random sample of 200 students with conduct disorder, of which 100 were
boys and 100 were girls, studying in schools and colleges between the age group of 11 to
18 years from different schools and colleges located in Mysore City.
Experimental group (EG) Control Group (CG)
100 100
Boys Girls Boys Girls
50 50 50 50
TOOLS USED
For the purpose of the present study the researcher has used the following tools.
1- Youth self-Report (2001), for Ages 11-18 to measure conduct disorder, Designed
by ASEBA, (Achenbach System of Empirically Bused Assessment), research

12
center for Children, youth, and families. (Using YSR DSM-ORIENTED
SCALES FOR BOYS AND GIRLS and YSR SYNDROME SCALES).
2- PROCEDURE
Randomized experimental control group pretest-posttest design is employed in the
present study which requires the utilization of a control group and random assignment of
subjects to groups.
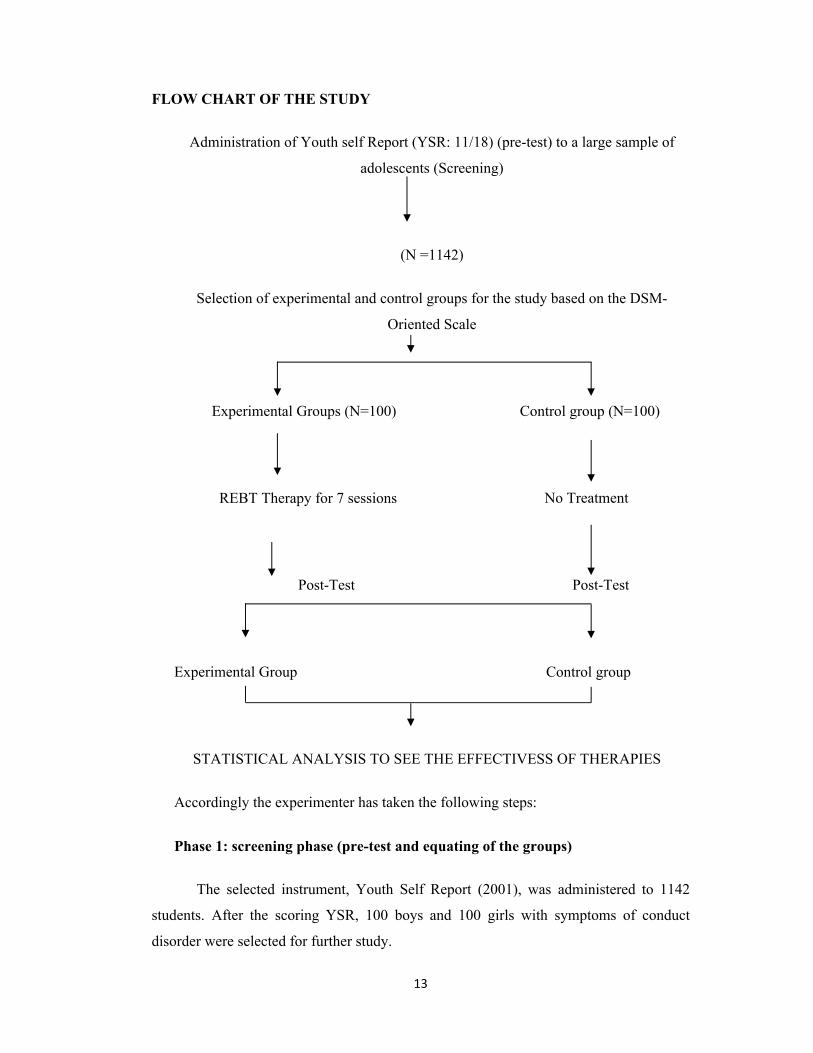
Following flow chart depicts the procedural aspects of the study:
13
FLOW CHART OF THE STUDY
Administration of Youth self Report (YSR: 11/18) (pre-test) to a large sample of
adolescents (Screening)
(N =1142)
Selection of experimental and control groups for the study based on the DSM-
Oriented Scale
Experimental Groups (N=100) Control group (N=100)
REBT Therapy for 7 sessions
Post-Test Post-Test
Experimental Group Control group
STATISTICAL ANALYSIS TO SEE THE EFFECTIVESS OF THERAPIES
Accordingly the experimenter has taken the following steps:
Phase 1: screening phase (pre-test and equating of the groups)
The selected instrument, Youth Self Report (2001), was administered to 1142
students. After the scoring YSR, 100 boys and 100 girls with symptoms of conduct
disorder were selected for further study.
No Treatment

14
Phase 2: experimental treatment
The experimental group was exposed to treatment (Specially designed REBT-
Rational Emotive Behavior Therapy). REBT was administered on small groups of 10
subjects. There were 10 experimental groups in total. Each group had one session in a
week and it took seven weeks of intervention duration for one group. No treatment was
given to control group, but was kept under observation including the self-introduction.
With the consent of the student’s parents and the college authority the researcher
scheduled the intervention program. The total duration of the intervention program was 4
months. Each session had duration of 90 minutes to 110 minutes. There were 9 stages in
the intervention program.
Intervention consists of four stages:
Stage 1: Introductory Session:
In this stage the researcher tried to make a rapport and build a relationship with
the subjects. During this time some funny comments are made for establishing a better
rapport between the researcher and the members in the group. The group was asked to
think about roles that might be helpful for their group to follow, and the following rules
were put into documents, distributed amongst the group and reviewed before each
session: (a) respect others, (b) no laughing or teasing, (c) raise hand to speak, (d) option
to “pass” if deciding not to participate and (e) keep information discusses in group
confidential .Then for about 10 minutes the group was asked to interact with each other
and share their feelings and ideas.
Towards the end of the session, the researcher talked about the next session and
gave them a small introduction to the REBT and the program in next session. A small
notebook was distributed among them and asking them to carry it in each session. The
notebook was given to them as a motivation in doing their homework assignment which
will be discussed later.
Stage 2: Using Cognitive Techniques of REBT
I: Active Disputing.
15
Here the members are all taught the ABCs of REBT by the researcher, shown
how to find their self-defeating, absolutist should and musts, their awfulizing, their I-
can’t-stand-it-its, their damning of self and of other persons, their over-generalizations,
and their other dysfunctional inferences and attributions, and are shown how to dispute
these with empirical, logical, and pragmatically useful challenges.
ABC Theory of Personality thought to the subjects: A = Activating Event, B =
Belief, C = Emotional and behavioral response, D = Disputing, E = Effect.
Before teaching the member about the ABC, they were asked to talk about their
main emotional problems and their daily difficulties. They mostly talked about having
problems with family, teachers, students, getting angry fast and being hot temper and
getting into fights. As mentioned before they all share four common symptoms,
aggression behavior, destructive behavior, lying or theft and violation of rules. Therefore
the researches focused on the problems which subjects were talking about, and which
was a part of these four symptoms. Then the ABC theory mentioned above is taught to
the students.
Asking for one example from each member about the positions when they were
feeling hurt, the A is assessed and then the B-C connection- the notion that their
emotional problems are determined largely by their beliefs rather than by the activating
event (A) - is shown to them. Then the three major “musts” are taught to them which are:
“I, must do well and get approved”, “you must treat me nicely and kindly”, and “the
word must give me what I want quickly, easily, and with great certainty. After learning
about the irrationality of dogmatic musts, should, outs, and so on, they are learned to
draw a rational conclusion in forms of “anti-awfulizing, e.g. it is bad, but it is not
awful.”, “higher frustration tolerance, e.g “I don’t like it but I can bear it.” and
“acceptance; to accept themselves and others as fallible human beings who cannot
legitimately be given a single global rating”. Then the D which stands for disputing is
worked out by the researcher. Here the therapist helps the client to challenge the
irrational belief (B). Therefore the self-defeating beliefs are dispute and replaced with a
rational one and resulted in an effective philosophy (E).
Although it was more of a theoretical session, students seemed to be more interested
in it when it was explained with the help of examples.

16
II: Rational Coping Self Statements
In groups and at their personal level, members are encouraged to prepare
Rational Beliefs (RBs) and coping statements to substitute for their Irrational Beliefs
(IBs), and to keep using them steadily until they consistently believe and act on them.
Such self-statements can be factual and encouraging (e.g. “I am able to succeed on this
job, and I will work hard to show that I can”). Or, preferably, they can be more
philosophical (e.g., “I’d like very much to success but I don’t have to do so; and if I fail I
am never a failure or a worthless individual”).
The researcher explained the coping self-statement technique with two or three
examples. Described the use and effect of the technique; then asked them to write 10 self
statements pertaining to their life situations. Each statement was again rewritten in a
more easy coping style.
III: Cognitive Homework.
Members are now ready to put their rational beliefs into practice. They are
reminded that the rational emotive behavioral theory of change holds that, in order to
deepen their convictions in their rational beliefs, they need to practice questioning their
irrational beliefs and strengthen their rational beliefs in situations that are the same or
similar to the activating event already assessed.
Cognitive homework is given to the subjects in the form of writing assignments
(self-help homework) at the end of each session. It is done on the notebooks which were
distributed to the subjects during the introduction session. The subjects were asked to
labels “A-B-C-D-E” or “what happened- what I felt- what I was thinking- what was
wrong with those thoughts- what thoughts would be more accurate and helpful.” Using
cognitive homework the researcher could determine if the subjects really understand the
A-B-C‘s of REBT. Also the linguistic confusions and misunderstandings of the theory
became clear and the researcher had a chance to do some invaluable teaching when the
assignment is reviewed in the next therapy session.

17
Stage 3: Using Emotive Techniques of REBT
I: Rational Emotive Imagery:
Group members do REI, both during group sessions and as homework, by
imagining one of the worst things that could happen to them, letting themselves feel very
upset about this image, imploding this disturbed feeling; and then working on their
feeling, to make themselves have healthy or appropriate negative feelings (such as
sorrow, disappointment, or frustration).
The researcher asked each subject to imagine themselves in the troublesome
situations which make them out of control and make them angry or hot temper; or the
situations which they violate the laws; This may allow the researcher to see if the
emotion has changed. If it has, the researcher asked the subjects what they are now
telling themselves. It was a way to rehearse more rational beliefs. Then they were
instructed to change the feeling from a disturbed emotion to a more constructive negative
emotion (e.g., from angry to disappointed).As it usually takes a minute or two to do REI
members were asked to do this during every session and every day for thirty days as their
homework until they automatically experience their healthy negative feelings when they
imagine, or actually encounter, similar “horrible” happenings.
II: Role-Playing:
Another in-session strategy is the use of role playing. In role playing, under the
tutelage of the therapist, the client rehearses a new behavior that is more consistent with
a rational philosophy. In role-playing group members often role-play with other group
members or with the therapist, as when one plays the interviewee for an important job
and the other plays the interviewer. During this form of behavior rehearsal, the rest of the
group critiques how well the member is doing in the role-play and suggests how she or
he could improve. If either of the role player shows anxiety, the role-play is temporary
stopped and this person is asked what he or she was thinking to create the anxiety and
how he or she could think, instead, to allay it.
Here the researcher worked more on problems which was related to conduct
problems. For example one major problem of the subjects was that they were unable to

18
control their anger which resulted in many fights with parents or peers. Role-playing
consisted of two or more individuals acting out a situation in which a group member
experienced anger control difficulties in the past. As the individuals acted out these
situations, they were stopped at key points so that the group members could identify A,
B, and C from the REBT model. They then provided suggestions for D and E so that
similar situations could be handled more rationally in the future.
Role-playing was on the focus of this research as it was more focused on the
behavioral modification of subjects with conduct problems. Subjects participated in role-
playing activities during each session, based on situations in which they personally
experienced anger control problems and other irrational way of solving their problems in
life. Here the researcher worked on the life problems which members were talking about
it regarding to the problems with parents, teachers, friends, getting hot temper and
having low tolerance. Such problems were selected for the role-play. Each group had
five sub-groups. Each sub-group was given 15 minutes for acting out. The exercise was
effective in many ways. They became freer with the group and counselor. They got
insights and solutions for their problems. One who acted and one who observed both
were active in the problem analysis and problem solving in a more rational way.
III: Reverse-Role Play:
In reverse-role play, one group member takes another’s irrational beliefs (e.g.
“so-and so must always love me completely!”) and holds on to it rigidly and forcefully
while playing the irrational member’s role. The person with the irrational belief then has
to talk the other role-player – actually himself or herself- out of this firmly held irrational
beliefs.
The researcher selected the irrational beliefs, (e.g. “they should love me”, “I must
be perfect”, “it is horrible if...” and so on), of each sub-groups and they were worked on
by reverse-role play. This technique was very effective in changing member’s behavior
and accepting the fact that their behavior is irrational and they should react to the
problems in a more rational way.

19
Stage 4: Behavioral Techniques of REBT
I: Skill Training:
In this part, group members often learn and practice particular important
interpersonal skills in the group sessions, For example, learning to listen to others,
accepting them with their poor behavior, communicating openly with them, and forming
relationships with them.
As the subjects in this study are having conduct problem, this skill training was
helping them to increase their interpersonal skills therefore they could have a better
relation with their parents, teachers, and friends and so on. One of the main problems of
adolescents with conduct disorder is their impair relation with other people as they show
aggression and destructive behavior. Skill training is a good option of helping these
adolescents to understand the right of others and to respect them in order to make a better
relation with people. During skill training, the members learned a better way of
communicating with others and they report it to be very effective on their social life.
II: Use of Reinforcement:
Being strongly behavioral, REBT shows group members how to suitably
reinforce themselves by doing something enjoyable only after they have done something
onerous- such as working on a term paper well - that they are avoiding. In group itself
they may be allowed to speak up about their own problems only after they have tried to
help other members with their difficulties.
In this study the researcher gave reinforcement to the members who use to do
their homework assignment for every session. They were given small things such as pen,
pencil, notebooks and like vise. Also the members were asked to reinforce themselves by
meeting a friend or someone who they like to spend time with.
This technique was helpful in motivating the members to do their homework
assignments regularly and to teach them a better method of self-management.

20
III: Use of Penalties:
Many members won’t stop their addictive or compulsive behavior because it is
too immediately pleasurable or reinforcing; and they will not change it for a normal
reinforcement. Thus they will not give up smoking or problem drinking for allowing
themselves to read or enjoy television. Consequently REBT encourages some group
members to penalize themselves after their destructive indulgences-for example, to spend
an hour with a boring person every time they gamble, or light every cigarette they smoke
with a $50 bill. Members also encourage other group members to enact suitable penalties
and monitor their doing so.
As some of the members were not particular on their home work assignment and
also not cooperating with other members, were penalized by giving 5 rupees to one of
the members who has done his or her homework clearly. This stage was also effective
and made the members to be more active in order to get the reinforcement and to avoid
the penalties.
Phase 3: post-test
Both the experimental group and control groups were measured on the dependent
variables and obtained post-test data for experimental group and post-test data for control
group. Significance of the difference between the two means was ascertained with the
help of appropriate statistical techniques. Also another descriptive and qualitative report
was taken from the teachers regarding to the behavior of the subjects.
Data analysis
The analysis used the application of General Linear Model Repeated Measures of
ANOVA for both subjects within group effects and between group effects. GLM
repeated measure of ANOVA is applied to variables of DSM oriented, syndrome
oriented scales, computation and total competence scores.

21
Results
The obtained data was treated with ‘t’ test for pre- test scores of experimental and
control groups to see any significant differences in DSM oriented scale, syndrome
oriented scales, computation and total competence scores. These tests were done to
confirm randomization of subjects in experimental and control groups. There were no
significant differences between experimental group and control group in relation to DSM
oriented, syndrome oriented scales, computation and total competence scores . Both
groups had equal scores in pre-testing. Thus, the equating as well as randomization of the
groups was taken care of during the pre-test.
ANOVA revealed a significant effect of the intervention program on adolescents with
conduct disorder in experimental group.
1. Considering the major objective of the present study which is to investigate the
effectiveness of REBT on adolescents in relation to conduct disorder, the
experimental group is found to have a significant reduction in conduct disorder
compared to the control group after the intervention program. Between pre-test to
post-test scores a significant difference was observed (F=26.939; P=.000) in
conduct disorders where a decrease of 1.12 (pre-10.91, post-9.79) scores was
noticed irrespective of the groups. The result indicates that, there is a significant
decrease in the mean scores of conduct disorder for experimental group with a
decrease of 2.56 as against .32 for control group. The results show that that the
impact of REBT on conduct disorder is positive.
2. The experimental group is found to have a significant reduction in emotional and
behavioral problems co-morbid with conduct disorder showing in DSM Oriented
Scale, compared to the control group after the intervention program. Between
pre-test to post-test scores a significant difference in affective problems was
observed (F=16.164; P=.000) where a decrease of 0.66 (pre-10.04, post-9.38)
scores was noticed irrespective of the groups. Subjects in experimental group
showed a significant decrease in the mean scores of Affective Problems for
experimental group with a decrease of 1.61 as against 0.3 for control group; In
anxiety problems a non-significant difference was observed (F=2.134; P=.146)
where a decrease of 0.14 (pre-4.78, post- 4.64) scores was noticed irrespective of
the groups. However, when the decrease in anxiety problems were analyzed
22
group wise, (experimental v/s control) a significant F value (F=11.148; P=.001)
was obtained. From the mean scores it is evident that experimental group
reduced its mean by 0.53 (Pre- 4.94 – Post-4.41) scores compared to control
group, which changed its scores by only 0.25 scores (pre 4.62 – Post 4.87). In
somatic problems, between pre-test to post-test scores a non-significant
difference was observed (F=.145; P=.704) where a decrease of 0.02 (pre-3.57,
post-3.59) scores was noticed irrespective of the groups. However, when the
decrease in somatic problems were analyzed group wise, (experimental v/s
control) a significant F value (F=4.371; P=.038) was obtained. From the mean
scores it is evident that experimental group reduced its mean by 0.16 (Pre- 3.63 –
Post-3.47) scores compared to control group, which increased its scores by 0.20
scores (pre 3.51 – Post 3.71). In ODD, between pre-test to post-test scores a non-
significant difference was observed (F=.005; P=.942) where a decrease of 0.01
(pre-4.10, post-4.09) scores was noticed irrespective of the groups. However,
when the ODD were analyzed group wise, (experimental v/s control) a significant
F value (F=5.153; P=.024) was obtained. From the mean scores it is evident that
experimental group reduced its mean by 0.28 (Pre- 4.21– Post-3.93) scores
compared to control group, which increased its scores by 0.22 scores (pre 3.98 –
Post 4.20)
3. The experimental group is found to have a reduction in syndromes showing in
Syndrome Oriented Scales (anxiety/depression, withdrawn/depressed, somatic
complaints, social problems, thought problems, rule breaking behavior,
aggressive behavior, and other problems), compared to the control group after the
intervention program. In anxious/depressed subscale significant change was
observed from pre to post test situation (F=15.988; P=.000) where a decrease of
.75 (pre-10.75, post 10.00) scores was noticed irrespective of the groups.
However, when the decrease in anxious/depressed scale were analyzed group
wise, (experimental v/s control) a significant F value (F=25.904; P=.000) was
obtained. From the mean scores it is evident that experimental group reduced its
mean by 1.75 (Pre- 11.40– Post 9.65) scores compared to control group, which
increased its scores by 0.25 scores (pre 10.10 – Post 10.35). In withdrawn
depressed, between pre to post test scores, a significant change was noticed
23
(F=13.327; P=.000) where a decrease of .48 (pre-7.18, post 6.70) scores was
found irrespective of the groups. However, when the decrease in
withdrawn/depressed scale were analyzed group wise, (experimental v/s control)
a significant F value (F=27.292; P=.000) was obtained. From the mean scores it
is evident that experimental group reduced its mean by 1.21 (Pre- 7.35– Post
6.14) scores compared to control group, which increased its scores by 0.18 scores
(pre 6.86 – Post 7.04). In somatic complaints between pre-test to post-test scores
a non-significant difference was observed (F=.172; P=.679) where a decrease of
0.07 (pre-5.73, post-5.66) scores was noticed irrespective of the groups.
However, when the decrease in somatic problems were analyzed group wise,
(experimental v/s control) a significant F value (F=5.325; P=.022) was obtained.
From the mean scores it is evident that experimental group reduced its mean by
0.32 (Pre- 5.95– Post-5.63) scores compared to control group, which increased its
scores by 0.04 scores (pre 5.13 – Post 5.17).
Between pre to post test scores in social problems, a significant change was
noticed (F=7.696; P=.006) where a decrease of .36 (pre-8.48, post 8.12) scores
was noticed irrespective of the groups. However, when the decrease in social
problems were analyzed group wise, (experimental v/s control) a significant F
value (F=16.219; P=.000) was obtained. From the mean scores it is evident that
experimental group reduced its mean by .92 (Pre- 8.78– Post 7.86) scores
compared to control group, which increased its scores by 0.20 scores (pre 8.19 –
Post 8.39). In thought problems, between pre-test to post-test scores a non-
significant difference was observed (F=.172; P=.679) where a decrease of 0.25
(pre-8.43, post-8.18) scores was noticed irrespective of the groups. However,
when the decrease in thought problems were analyzed group wise, (experimental
v/s control) a significant F value (F=5.325; P=.022) was obtained. From the
mean scores it is evident that experimental group reduced its mean by .70 (Pre-
8.80– Post-8.10) scores compared to control group, which increased its scores by
0.18 scores (pre 8.07 – Post 8.25). Between pre to post test scores in rule
breaking behavior, a significant change was noticed (F=18.822; P=.000) where a
decrease of .77 (pre-8.80, post 8.03) scores was noticed irrespective of the
groups. However, when the decrease in rule breaking behavior were analyzed
group wise, (experimental v/s control) a significant F value (F=29.165; P=.000)
was obtained. From the mean scores it is evident that experimental group

24
reduced its mean by 1.84 (Pre- 9.10– Post 7.26) scores compared to control
group, which increased its scores by 0.30 scores (pre 8.50 – Post 8.80). As far as
the aggressive behavior is considered, between pre to post test scores a significant
change was noticed (F=27.041; P=.000) where a decrease of 1.27 (pre-14.95, post
13.68) scores was noticed irrespective of the groups. However, when the
decrease in aggressive behavior were analyzed group wise, (experimental v/s
control) a significant F value (F=32.726; P=.000) was obtained. From the mean
scores it is evident that experimental group reduced its mean by 2.68 (Pre- 14.96–
Post 12.28) scores compared to control group, which increased its scores by 0.14
scores (pre 14.94 – Post 15.08). In other problems also, between pre to post test
scores, a significant change was noticed (F=9.006; P=.000) where a decrease of
.39 (pre-7.03, post 6.64) scores was noticed irrespective of the groups. However,
when the decrease in rule other problems were analyzed group wise,
(experimental v/s control) a significant F value (F=18.897; P=.000) was obtained.
From the mean scores it is evident that experimental group reduced its mean by
1.84 (Pre- 7.17– Post 6.18) scores compared to control group, which increased its
scores by 0.30 scores (pre 6.89– Post 7.09).
4. There was a reduction of score on internalizing and externalizing groups of
syndromes in experimental group compared to the control group after the
intervention program. In internalization scores, between pre-test to post-test
scores a non-significant difference was observed (F=.787; P=.376) where a
decrease of 1.52 (pre-66.04, post-64.52) scores was noticed irrespective of the
groups. However, when the decrease in internalization scores were analyzed
group wise, (experimental v/s control) a significant F value (F=17.124; P=.000)
was obtained. From the mean scores it is evident that experimental group
reduced its mean by 4.72 (Pre- 66.93– Post-62.21) scores compared to control
group, which increased its scores by 1.68 scores (pre 65.15 – Post 66.83). In
externalization scores, between pre to post test scores a significant change was
noticed (F=17.291; P=.000) where a decrease of 2.26 (pre-66.78, post 64.52)
scores was noticed irrespective of the groups. However, when the decrease in
externalization scores were analyzed group wise, (experimental v/s control) a
significant F value (F=23.626; P=.000) was obtained. From the mean scores it is
evident that experimental group reduced its mean by 4.86 (Pre- 67.07– Post
25
62.21) scores compared to control group, which increased its scores by 0.14
scores (pre 66.48 – Post 66.83)
5. The experimental group showed a reduction in Total Problem Scores compared to
the control group after the treatment. Between pre to post test scores a significant
change was noticed (F=7.894; P=.005) where a decrease of 1.56 (pre-67.03, post
65.47) scores was noticed irrespective of the groups. However, when the
decrease in total T scores were analyzed group wise, (experimental v/s control) a
significant F value (F=13.132; P=.000) was obtained. From the mean scores it is
evident that experimental group reduced its mean by 3.67 (Pre- 67.76– Post
64.09) scores compared to control group, which increased its scores by 0.14
scores (pre 66.30 – Post 66.86).
6. The experimental group did not show a significant differences on Competency
Score compared to the control group after the intervention. In total competency
scores, the intervention did not have any significant change from pre to post test
situation irrespective of the groups, as the obtained F value of .404 was found to
be non-significant (P=.526). No differential change for either groups –
experimental or control groups were observed from pre to post test session
(F=3.43; P=.066).
7. There were no significant differences between age groups in response to the
intervention program on all the variables taken in this study.
8. Also the experimental group showed no significant differences of gender in
response to the intervention program on all the variables taken in this study.
Verification of the Hypotheses
The research hypotheses were developed to investigate the impact of Rational
Emotive Behavior Therapy (REBT) on Conduct Disorder in adolescents, and also with
other problems shown on DSM Scale, symptoms of problems shown on Syndrome scale,
competency of adolescents and internalize externalize symptoms.

26
Research hypotheses # 1, Rational Emotive Behavior Therapy (REBT) has a
positive impact on treatment of Conduct Disorder. This hypothesis is accepted as the
result shows a reduction of 8.61% in conduct disorder in experimental group.
Research hypotheses # 2; Rational Emotive Behavior Therapy (REBT) has a
positive impact on treatment of additional variables of DSM Scale. This hypothesis is
accepted as the results shows a reduction of 6.57% in Affective Problems, 2.92% in
Anxiety Problems, 0.56% in Somatic Problems, and 0.24% in ODD Problems.
Research Hypotheses # 3, Rational Emotive Behavior Therapy (REBT) has a
positive impact on treatment of additional variables of Syndrome Scale. This hypothesis
too is accepted as the results shows a reduction of 5.30% in anxiety/depression, 6.68% in
withdrawn/depressed, 1.22% in somatic complaints, 4.24% in social problems, 2.96% in
thought problems, 8.75 % in rule breaking behavior, 8.49% in aggressive behavior, and
5.54% other problems.
Research hypotheses # 4, Rational Emotive Behavior Therapy (REBT) has a
positive impact on reduction of Internalizing and Externalizing Groups of Syndromes.
Hypothesis was supported by the results as there was a reduction of 2.30% in
Internalizing and 3.38% in Externalizing.
Research hypotheses # 5, Rational Emotive Behavior Therapy (REBT) has a
positive impact on reduction of scores on Total Problem Score. The hypothesis is
accepted by results showing a reduction of 2.32 % in Total Score.
Research hypotheses # 6, Rational Emotive Behavior Therapy (REBT) has a
positive impact on increasing of Total Competency Score. This hypothesis was not
supported by the findings as there were a comparative differences and not a significant
differences between experimental and control group. The hypothesis is rejected.
Research hypotheses # 7, there is a significant difference of age groups (Early
and Late Adolescence) in response to the REBT with the regard of: Conduct Disorder,
DSM-Oriented Problems, Syndrome Problems, Internalizing- Externalizing Groups,
Total Problem Scores, and Total Competency Score. This hypothesis was not accepted as
there were no significant of differences regarding to age groups on response to REBT
intervention on any variables of the study. This hypothesis is also rejected.
Research hypotheses # 8, there is a significant difference of gender groups (Boys
and Girls) in response to the REBT with the regard of: Conduct Disorder, DSM-Oriented

27
Problems, Syndrome Problems, Internalizing- Externalizing Groups, Total Problem
Scores, and Total Competency Score. This hypothesis was not supported by the findings
as there were no significant of differences regarding to gender groups on response to
REBT intervention on any variables of the study. The hypothesis is rejected.
Summary and conclusion of the study
A sample of 1142 students, boys and girls , aged 11 to 18 years old, was
administered the Youth self Report (YSR). Out of this sample 200 adolescents diagnosed
of conduct problems by the help of DSM-Oriented Scale were selected for the study. Out
of 200 students, 100 were taken as experimental group (consist of 50 boys and 50 girls),
and another 100 (50 boys and 50 girls) were taken as control group. Each experimental
group went under seven sessions of REBT in duration of seven weeks. No treatment was
given to control group but it was kept under observation. One month after the last REBT
session, post-test is taken from experimental and control group. Results were analyzed
and hypothesizes were tested.
The results showed that REBT is highly effective on treatment of conduct
disorder with adolescents. REBT was also effective on other emotional and behavioral
problems co-morbid with conduct disorder.
We can conclude that REBT is an effective treatment module for adolescents
with emotional and behavioral problems.
28
References
Aaron R, Joseph A, Abraham S, Muliyil J, George K, Prasad J, Minz S, Abraham VJ,
Bose A., (2004) Suicides in young people in rural southern India. Lancet ; 363: 1117 –
18.
Achenbach, T.M., Edelbrock C.S. (1978) The classification of child psychopathology: A
review and analysis of empirical efforts. Psychological Bulletin, 85, 1275 –1301.
American Psychiatric Association.( 1987). Diagnostic and Statistical Manual of Mental
Disorders. 3d ed., revised. Washington, DC: American Psychiatric Association.
Bandura, A. (1989). A social cognitive theory of action. In J. P. Forgas & M. J. Innes
(Eds.), Recent advances in social psychology: An international perspective (pp. 127-
138). North Holland: Elsevier.
Buhler, C. (1927). Die ersten sozialen Verhaltungsweisen des Kindes. In C. Buhler, H.
Hetzer and B. Tudor-Hart (Eds.), soziologische und Psychologische Studien uber das
Erste Lebensjahr. Jena : Gustav Fischer.
Eme, R. F., & Kavanaugh, L. (1995). Sex differences in conduct disorder. Journal of
Child Clinical Psychology, 24(4), 406-426.
Esser G, Schmidt MH, Woerner W. (1990), Epidemiology and course of psychiatric
disorders in school-age children-results of a longitudinal study. J Child Psychol
Psychiatry;31: 243-63.
Fagot, B., & Levy, L (1998). Gender identity and play. In D.P. Fromberg & D. Bergen
(Eds.), Play from birth to twelve an beyond (pp. 187-192). New York: Gartland.
Fergusson D.M. & Horwood L.J. (1992) Attention deficit and reading achievement.
Journal of Child Psychology and Psychiatry. 33, 375 – 385.
Ford T, Goodman R, Meltzer H. (2003). The British Child and Adolescent Mental Health
Survey 1999: the prevalence of DSM–IV disorders. J Am Acad Child Adolesc
Psychiatry, 42: 1203 –11.
Kashini, J.H., Beck, N.C., Hoeper, E.W., Fallahi, C., Corcoran, C.M., McAllister, M.,
Rosenberg, T.K.(1987). Psychiatric disorders in a community sample of adolescents.
American Journal of Psychiatry, 144, 584-89.

29
Leader, E. (1991). Why adolescents group therapy. Journal of Child and Adolescent
Group Therapy, 1, 81-93.
Lyon G.R. (1996) Learning disabilities. Future Child. 6, 54-76.
Mabey , j., and Sorensen, B. (1995). Counseling for Young People. Buckingham” Open
University Press.
Registrar General of India (1996). Population projection for India and States, 1996–
2016. Report of the Technical Group of Population Projection. Planning Commission,
New Delhi.
Ringel, J. S., & Sturm, R. (2001). National estimates of mental health utilization and
expenditures for children in 1998. Journal of Behavioral Health Services and Research,
28(3), 319-332.
Saxe, L, Cross, T., and Silverman, N. (1988). Children’s mental health: The gap between
what we know and what we do. American Psychology, 43(10), 800-807.
Srinath S, Girimaji SC, Gururaj G, Seshadri S, Subbakrishna DK, Bhola P, Kumar
N.(2005). Epidemiological study of child and adolescent psychiatric disorders in urban
and rural areas of Bangalore, India. Indian J Med , 122: 67 –79.
U.S. Department of Health and Human Services. (1999). Mental Health: A Report of the
Surgeon General. Rockville, MD: U.S. Department of Health and Human Services.
Verghese A, Beig A., (1974) Psychiatric disturbances in children: an epidemiological
study. Indian J Med Res 62: 1538 –42.
World Health Organization (WHO), (1992). International Statistical classification of
diseases and related health problems (10th rev.). Geneva: Author.
Signature of the Guide Signature of the Research Scholar