the importance of developing a primary core stability...
TRANSCRIPT

The Importance of Developing a
Primary Core Stability Protocol
Angela M. Homan, SPTDuke University
Doctor of Physical Therapy Intern
SportsMedicine of Atlanta
Dr Robert E DuVallPT, DHSc, MMSc, ATC, OCS, SCS, FAAOMPT, DAC, MTC, PCC, CSCS
Shenandoah University, Associate Professor
Alabama State and Northeastern University, Clinical Assistant Professor
SportsMedicine of Atlanta, Inc.
Residency & APTA Fellowship Curricula Director
[email protected] www.SportsMedicineofAtlanta.com
SportsMedicine of Atlanta, Inc.

NMR Research Shown Beneficial
to Reduce Pain and Disability "In America alone, the treatment cost of back pain is
estimated to be $86 billion per year or 9% of the country's
total health expenditure. The search for new ways to
manage this old problem is critical in order to improve the
health and quality of life of individuals who struggle with
this condition.“
According to researchers not only do patients feel less pain,
but patients performing these types of exercises are able to
be more physically active and experience positive effects
over a longer period of time than those who receive other
treatments.
Macedo, Luciana G. Maher, Christopher G. Latimer, Jane. McAuley, James H. Motor Control Exercise for
Persistent, Nonspecific Low Back Pain: A Systematic Review. PTJ 2009;89(1).9-95.
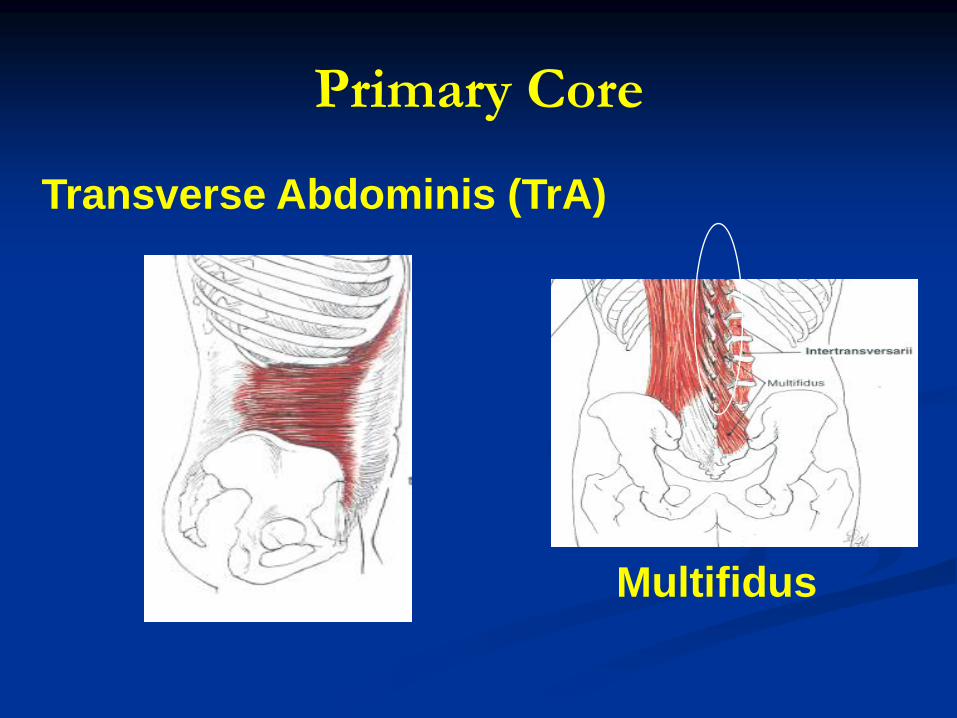
Primary Core
Transverse Abdominis (TrA)
Multifidus

Transverse Abdominis Anatomy
Origin: inner surface of cartilages of lower 6
ribs, interdigitation with diaphragm,
thoracolumbar fascia, anterior ¾ of internal lip
of iliac crest, and lateral 1/3 of inguinal ligament
Insertion: linea alba (broad aponeurosis), pubic
crest, and pecten pubis
Nerve Innervation: T7-T12, L1
(iliohypogastric and ilioinguinal)Kendall et al.

Actions of TrA
Flattens abdominal wall and compress the
abdominal viscera
Decrease infrasternal angle of ribs in expiration
(upper portion of TrA)
No Action in lateral trunk flexion, except to
compress the viscera and to stabilize linea alba
(= better action of anterolateral trunk muscles)Kendall et. al.

Weakness in TrA (observations)
Standing position: Permits bulging of
anterior abdominal wall (= increases
lordosis)
Supine position: during flexion a lateral
bulge tends to occur
Prone position: hyperextension of
trunk with lateral bulge tends to occurKendall et al.

Multifidus Anatomy
Origin: Sacral region: posterior surface of sacrum, medial surface of posterior iliac spine & postero-sacroiliac ligaments. Lumbar, thoracic, & cervical regions: transverse processes of L5-C4
Insertion: Spanning two to four vertebrae, inserting onto spinous process of one of vertebra above from last lumbar to axis (second cervical vertebra
Nerve Innervation: SpinalKendall et al.

Actions of Multifidis
Extends vertebral column and rotation toward
opposite side.Kendall et al.

Functions of TrA & Deep Multifidus
Deep Multifidus and TrA provide intersegmental
spinal stability
Deep fibers of Multifidus control intervertebral
motion
Superficial fibers of Multifidus control spine
orientationMoseley GL, Hodges PW, Gandevia SC. Deep and superficial fibers of the lumbar multifidus muscle are differentially active during voluntary arm movements. Spine.
2002;27:E29–E36.
TrA Muscle Activation Patterns
TrA may be controlled independently of the motor command for limb movement in contrast to the other abdominal muscles. Hodges PW, Richardson CA. Transversus abdominis and the superficial abdominal muscles are controlled independently in a postural task.
Neuroscience Letters. 1999;265:91-94.
Feedforward TrA activation pattern with Lower extremity movement Hodges P, Richardson C. Contraction of the abdominal muscles associated with movement of the lower limb. Physical Therapy. 1997;77:132-144.
Feedforward activation TrA activation pattern with upper extremity movement Hodges P, Richardson C. Feedforward contraction of transversus abdominis is not influencedby the direction of arm movement. Experimental Brain
Research. 1997;114:362-370.
Preparatory trunk movement precedes upper extremity movement Hodges P, Cresswell AG, Daggfeldt K, Thorstensson A. Preparatory trunk motionaccompanies rapid upper limb
movement. Experimental Brain Research. 1999;124:69-79. Hodges P, Cresswell AG, Daggfeldt K, Thorstensson A. Three dimensional preparatory trunk motion precedes
asymmetrical upper limb movement. Gait and Posture. 2000;11:92-101.

Core Dysfunction: Anatomy
Transverse Abdominis:
Isometric Knee extension/flexion
tasks identified subjects with LBP had
smaller increase in TrA thickness and
less EMG activity Ferreira PH, Ferreira, Hodges PW. Changes in recruitment of the abdominal muscles in people with low back pain
ultrasound measurement of muscle activity. Spine. 2004;29:2560-2566.

Core Dysfunction: Anatomy
Multifidus:
Atrophy of multifidus has been used as a rationale for spine stabilizing exercises.
Barker et al, found selective ipsilateral atrophy of multifidus in patients with unilateral LBP (low back pain)
MRI analysis of the CSA of Multifidus At level of pain: 21.7 % decrease
Above level of pain: 15.8% decrease
Below level of pain: 16.8% decrease
Decreased CSA at level of pain was positively correlating with duration of pain.
Barker KL, Shamley DR, Jackson D. Changes in the cross-sectional area of multifidus and psoas in patients with unilateral back pain. The relationship to pain and disability. Spine. 2004;29:E515-E519.

Core Dysfunction: Activation
Patterns
Subjects with chronic LBP do not pre-activate TrA prior to rapid upper and lower limb tasks.
Barr KP, Griggs M, Cadby T: Lumbar stabilization: Core concepts and current literature, part 1. Am J Phys Med Rehabil. 2005;84:473-480.
Hodges P, Richardson C. Inefficient muscular stabilisation of the lumbar spine associated with low back pain: a motor controlevaluation of transversus abdominus. Spine. 1996;21:2640-2650.
Onset of internal obliques, multifidus, & gluteus maximus was delayed on the symptomatic side (>20ms)= no feed-forward activation in subjects with sacroiliac joint pain
Hungerford B, Gilleard W, Hodges P, Evidence of altered lumbopelvic muscle recruitment in the presence of sacroiliac joint pain. Spine. 2003;28:1593-1600.

TrA Muscle Activation
Three different techniques used in clinical practice:
Drawing-in Maneuver
Abdominal Bracing
Posterior Pelvic Tilt
Drawing-in Maneuver is more selective in coactivating the TrA and multifidus than the other 2 techniques.
Hodges, PW, Richardson, GA, and Jull, G: Evaluation of the relationship between laboratory and clinical tests of transversus abdominis function. Physiother Re Internat 1(1):30, 1996.
Richardson, C, Jull, G, et al: Techniques for activae lumbar stabilisation for spinal protection: A pilot study. Austral J Physiother 38:105, 1992.
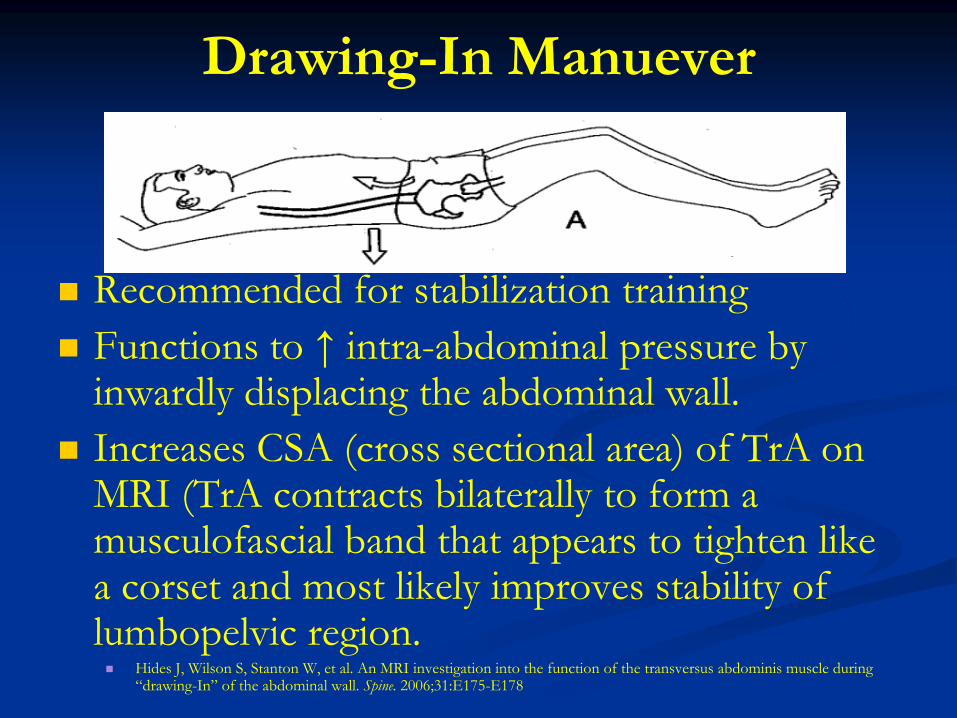
Drawing-In Manuever
Recommended for stabilization training
Functions to ↑ intra-abdominal pressure by inwardly displacing the abdominal wall.
Increases CSA (cross sectional area) of TrA on MRI (TrA contracts bilaterally to form a musculofascial band that appears to tighten like a corset and most likely improves stability of lumbopelvic region. Hides J, Wilson S, Stanton W, et al. An MRI investigation into the function of the transversus abdominis muscle during
“drawing-In” of the abdominal wall. Spine. 2006;31:E175-E178
Drawling-in Maneuver:
Patient starts in hook-lying position and assumes a neutral spine position & attempts to maintain it while drawing in and hollowing the abdominal muscles.
Kendal, F, McCreary, E, and Provance, PG: Muscles: Testing and Function, ed 4. Williams & Wilkins, Baltimore, 1993.
Subtle posterior pelvic tilt & flattening of lumbar spine.
No flaring of lower ribs, bulging out of abdominal wall or ↑ pressure through feet.
Instructions: draw the “belly button” up and in toward the spine while exhaling

Feedback Techniques
If patient is having difficulty activating the Transverse Abdominis, the following has been used to assist with learning:
Pressure transducer for clinical testing and visual feedback (Pressure Bio-Feedback Chatanooga Pacific)
Biofeedback with surface electrodesHagins, M, et al: Effects of practice on the ability to perform lumbar stabilization exercises. J Orthop Sports Phys Ther 29(9):546, 1999.
Jull, GA, and Richardson, CA: Rehabilitation of Active Stabilization of the Lumbar Spine. In Twomy, LT and Taylor (eds): Physical Therapy of the Lumbar Spine, ed 2. Churchill Livingstone, New Yourk, 1994.
Richardson, C, Jull, G, et al: Techniques for active lumbar stabilization for spinal protection: A pilot study. Austral JPhysiother 38:105, 1992.
Richardson C, and Jull, G: An historical perspective on the development of clinical techniques to evaluate and treat the active stabilizing system of the lumbar spine. Austral J Physiother Monograph 1:5, 1995.

Visual Feedback- hook-lying
Place small inflatable bladder with pressure sensor
(similar to BP cuff) under lumbar spine and inflate it to
40-mm Hg.
Correct Activation: 10-mm Hg increase in pressure
Large increase occurs if activating rectus abdominis
and/or increased lumbar flexion (posterior pelvic tilt).
No change in pressure = no activation of TrA

Visual Feedback- hook-lying

Biofeedback with surface electrodes
Electrodes placed over rectus abdominis &
external obliques (near attachment on the 8th
rib).
Correct activation: minimal to No activation of
these muscles
Can be used in conjunction with inflatable cuff.

Abdominal Bracing
Occurs by setting the abdominals and actively
flaring out laterally around the waist
Technique has been taught years
It has been shown to activate the oblique
abdominal musclesRichardson, C, Jull, G, et al: Techniques for active lumbar stabilization for spinal protection: A pilot study. Austral JPhysiother 38:105,1992.
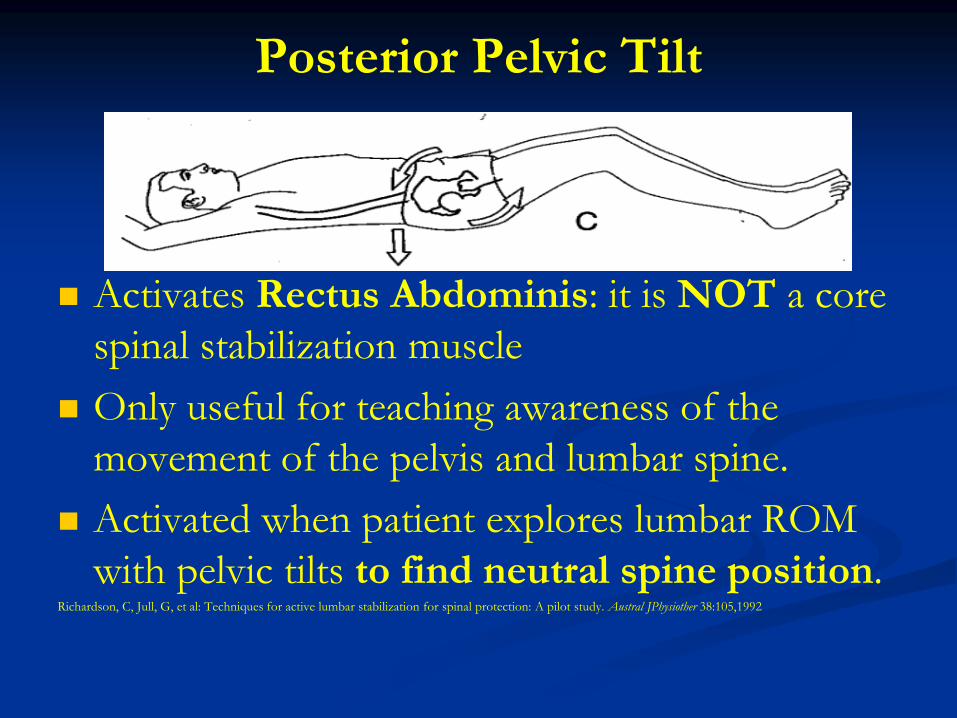
Posterior Pelvic Tilt
Activates Rectus Abdominis: it is NOT a core
spinal stabilization muscle
Only useful for teaching awareness of the
movement of the pelvis and lumbar spine.
Activated when patient explores lumbar ROM
with pelvic tilts to find neutral spine position.Richardson, C, Jull, G, et al: Techniques for active lumbar stabilization for spinal protection: A pilot study. Austral JPhysiother 38:105,1992

Lower Abdominal Progression
Levels developed by Shirley A. Sahrmann
Purposes:
To improve the performance of abdominal muscles
(external obliques, rectus abdominis, transverse
abdominis)
To learn to prevent lumbar spine motions associated with
leg motion
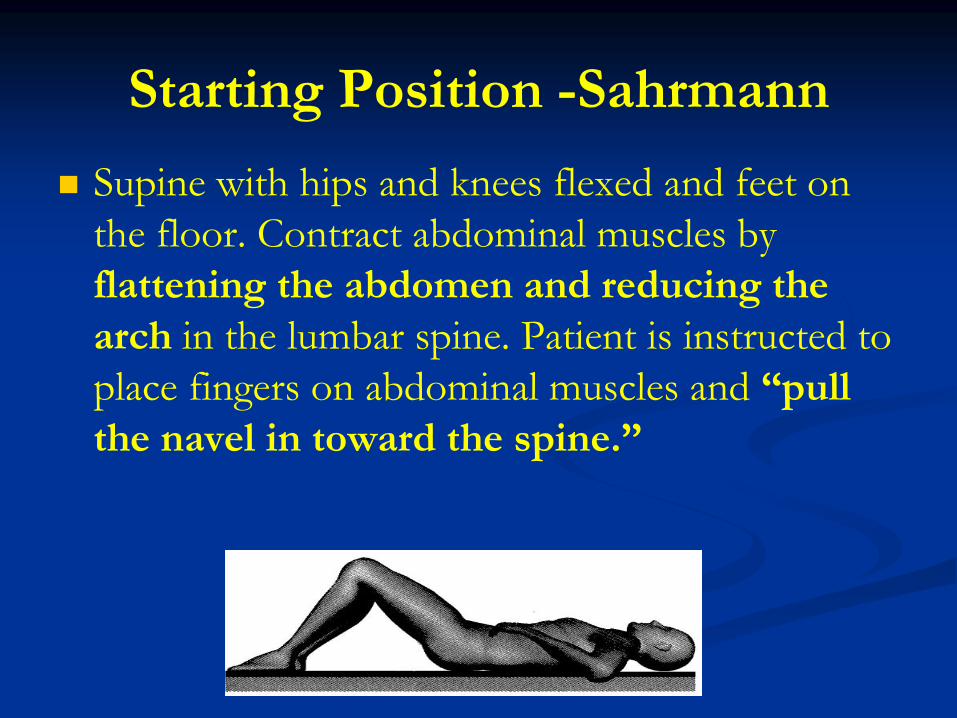
Starting Position -Sahrmann
Supine with hips and knees flexed and feet on
the floor. Contract abdominal muscles by
flattening the abdomen and reducing the
arch in the lumbar spine. Patient is instructed to
place fingers on abdominal muscles and “pull
the navel in toward the spine.”

Level 0.3 (E1)-Sahrmann
Lift one foot with alternate foot on floor
Method:
Flex one hip while keeping knee flexed.
Return the LE to starting position and repeat with
opposite LE.
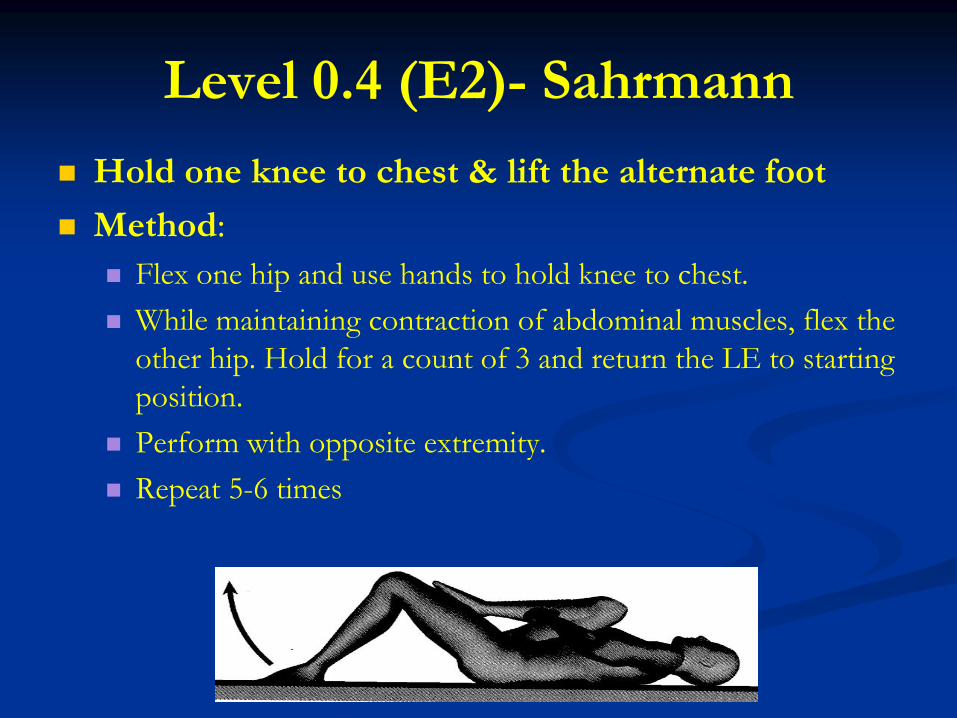
Level 0.4 (E2)- Sahrmann
Hold one knee to chest & lift the alternate foot
Method:
Flex one hip and use hands to hold knee to chest.
While maintaining contraction of abdominal muscles, flex the
other hip. Hold for a count of 3 and return the LE to starting
position.
Perform with opposite extremity.
Repeat 5-6 times

Level 0.5- Sahrmann LIGHTLY hold one knee toward the chest and lift
the alternate foot
Methods:
Flex one hip and use one hand to hold knee to chest, but hold it less firmly than level E2 (0.4).
While maintaining contraction of abdominal muscles, flex other hip.
Hold for a count of 3 and return the LE to starting position
Perform with the opposite extremity.
Repeat 5-6 times

Level 1A- Sahrmann Flex the hip to > 90˚and lift the alternate foot
Methods:
Contract the abdominal muscles; flex one hip to > 90 degrees by lifting the foot from the table.
Contract the abdominal muscles and flex the other hip by lifting the foot off the table.
Maintain the contraction of
abdominal muscles and lower
the legs, one at a time, to
starting position.
Repeat by starting the
sequence with opposite leg.
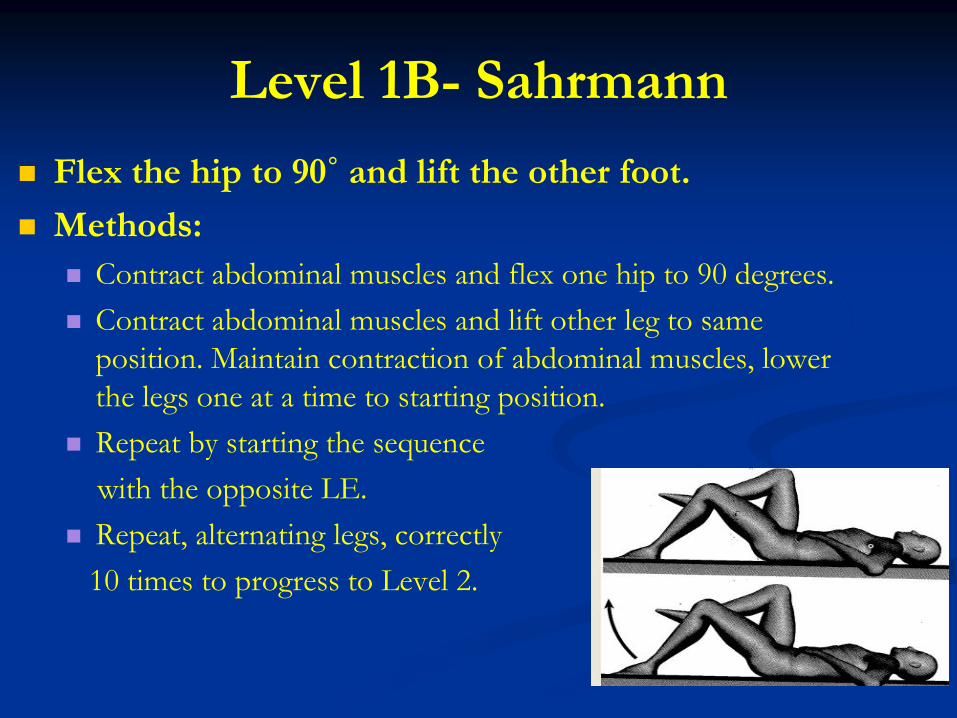
Level 1B- Sahrmann
Flex the hip to 90˚ and lift the other foot.
Methods:
Contract abdominal muscles and flex one hip to 90 degrees.
Contract abdominal muscles and lift other leg to same
position. Maintain contraction of abdominal muscles, lower
the legs one at a time to starting position.
Repeat by starting the sequence
with the opposite LE.
Repeat, alternating legs, correctly
10 times to progress to Level 2.

Level 2-Sahrmann Flex one hip to 90˚ and lift & slide the other foot to extend
the hip and knee.
Methods: Contract abdominal muscles and flex hip to 90 degrees, lifting foot off
the table.
Maintain contraction of abdominal muscles; lift other leg up to same position.
Maintain one leg at 90 degrees, place other heel on table and slowly slide heel along table until hip and knee are extended.
Return leg to starting position by sliding hell along table.
Repeat extension motion with other LE and return it to starting position.
Repeat, alternating legs, correctly 10 times to progress to Level 3.

Level 3-Sahrmann Flex one hip to 90 degrees, and lift the foot and extend the
leg without touching the support surface.
Methods: Flex hip to 90 degrees, lifting foot from the table.
Maintain contraction of abdominal muscles and lift other leg up to same position.
Maintain one hip at 90 degrees, extend the other hip and knee while holding the foot off the table until hip and knee are resting in an extended position on the table.
Return leg to the hip and knee flexed position.
Maintain contraction of abdominal muscles, extend and lower the other leg and return it to the 90 degree position.
Repeat, alternating legs, correctly 10 times to progress to Level 4.

Level 4-Sahrmann Slide both feet along the supporting surface into
extension and return to flexion
Methods:
Begin in supine position with both legs in extension.
Contract abdominal muscles and slide heels along table,
flexing both hips and knees while bringing them toward the
chest.
Once hips and knees are flexed, pause
and reinforce abdominal contraction.
Slide both legs back into extension.
Repeat correctly 10 times to
progress to Level 5

Level 5-Sahrmann
Lift both feet off the supporting surface, flex the hips to 90 degrees, extend the knees, and lower both extremities to supporting surface.
Methods: Begin with LE extended position.
Contract abdominal muscles
while simultaneously flex hips
and knees, lifting both feet
off the table to bring the hips
to 90 degrees.
Reinforce the contraction of
abdominal muscles, extend the
knees and lower LEs to table.

Primary Core Protocols
Transverse Abdominis (Levels I-V)
Multifidus (Levels I-III)
http://lowerabexercises.blogspot.com/

The TrA Level Progression
These proposed levels were designed from the research and are clinically applied to strengthen the Transverse Abdominis in isolation.
Purpose:
To have a common terminology among practicing clinicians in the same physical therapy setting.
To improve the performance of TrA muscle.
To prevent lumbar spine motion (neutral spine) during functional activity.

Starting Position: TrA Level I
Method:
Supine with hips & knees flexed and feet on the
floor.
Patient is instructed keep a Neutral lumbar spine
using the „Drawing-in Maneuver‟ and place two
fingers on transverse abdominus and one hand on
superficial abdominal muscles.
Next, patient is asked to “pull the navel in toward
the spine” without tightening superficial abdominal
muscles and only the TrA.

TrA Level I
Level I will be the starting position for all levels
I-V.
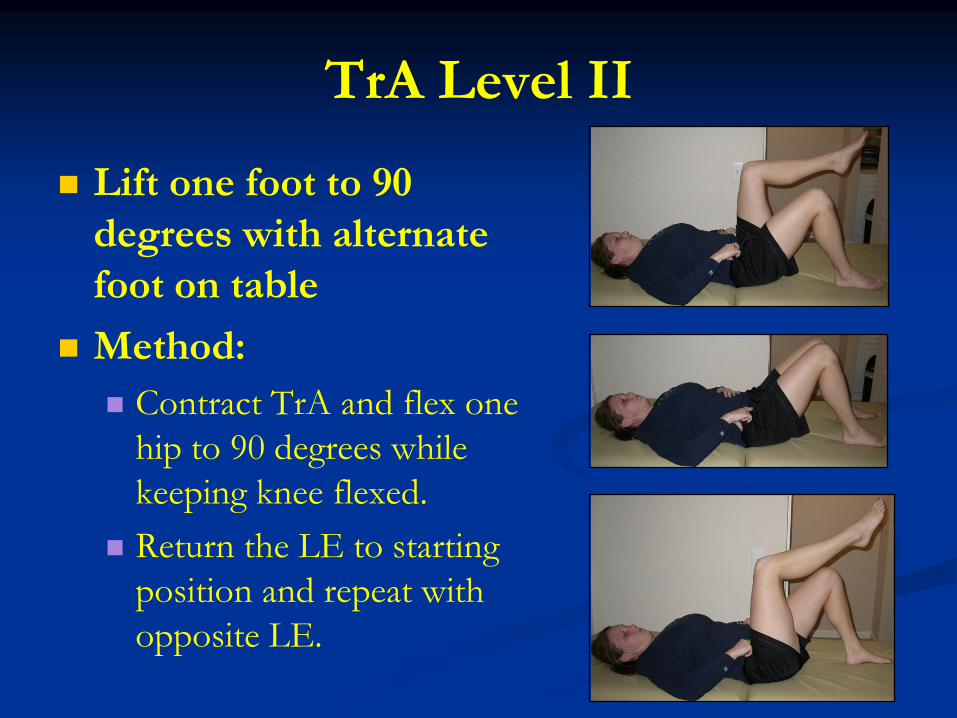
TrA Level II
Lift one foot to 90
degrees with alternate
foot on table
Method:
Contract TrA and flex one
hip to 90 degrees while
keeping knee flexed.
Return the LE to starting
position and repeat with
opposite LE.

TrA Level III
Flex the hip to 90˚ and lift the other foot.
Methods:
Contract TrA and flex one hip to 90 degrees.
Lift other leg to same position. While maintaining contraction
of TrA, lower the legs one at a time to starting position.
Repeat by starting the sequence
with the opposite LE.
Repeat, alternating legs, correctly
10 times to progress to Level 4.

TrA Level III

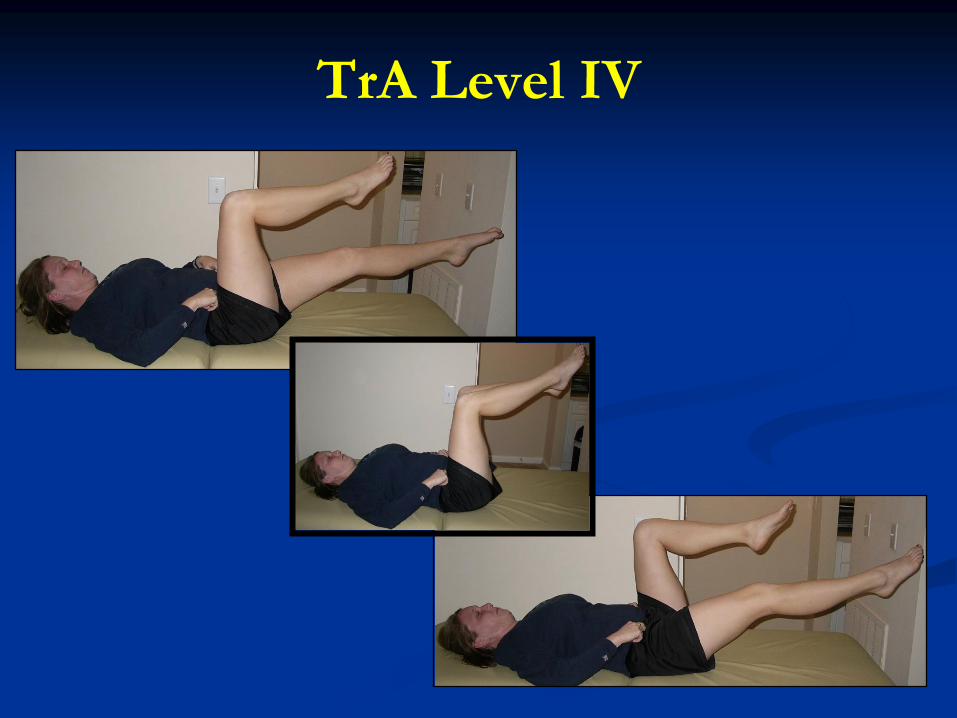
TrA Level IV
Flex one hip to 90 degrees, and lift the other foot. Extend the one leg without touching the support surface.
Methods:
Flex hip to 90 degrees, lifting foot from the table.
Maintain contraction of TrA and lift other leg up to same position.
Maintain one hip at 90 degrees, extend the other hip and knee while holding the foot off the table.
Return leg to the hip and knee flexed position.
Maintain contraction of abdominal muscles, extend other leg and return it to the 90 degree position.
Repeat, alternating legs, correctly 10 times to progress to Level 5.
TrA Level IV

TrA Level V
Flex the hips to 90 degrees and extend the knees without touching the support surface.
Methods:
Flex hip to 90 degrees, lifting foot from the table.
Maintain contraction of TrA and lift other leg up to same position.
Extend both hips and knees while holding the feet off the table.
Return legs to the hip and knee flexed position.
Repeat correctly 10 times.

TrA Level V

Multifidus Level Progression (I-III)
These proposed levels were designed from the research and are clinically applied to strengthen the Multifidus in isolation.
Purpose:
To have a common terminology among practicing clinicians in the same physical therapy setting.
To improve the performance of Multifidus muscle.
To prevent lumbar spine motion (neutral spine) during functional activity.

Multifidus Level Ia
Start position: Quadriped
Neutral lumbar spine
Have patient lift one lower extremity (LE) ( knee) ~ 1 inch from table
Hold position ~ 5 seconds
Alternate with the other LE.
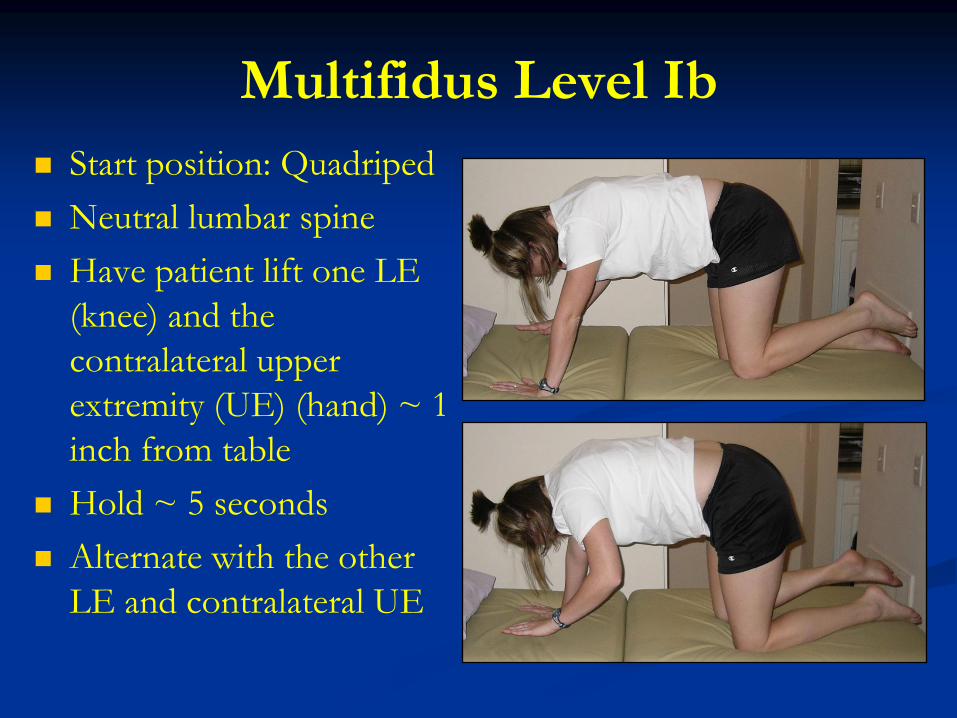
Multifidus Level Ib
Start position: Quadriped
Neutral lumbar spine
Have patient lift one LE
(knee) and the
contralateral upper
extremity (UE) (hand) ~ 1
inch from table
Hold ~ 5 seconds
Alternate with the other
LE and contralateral UE

Multifidus Level II
Starting position: Prone
Maintain neutral lumbar spine (i.e. placement of
pillow)
Lift one UE and contralateral LE from the table
Alternate with other UE and contralateral LE.
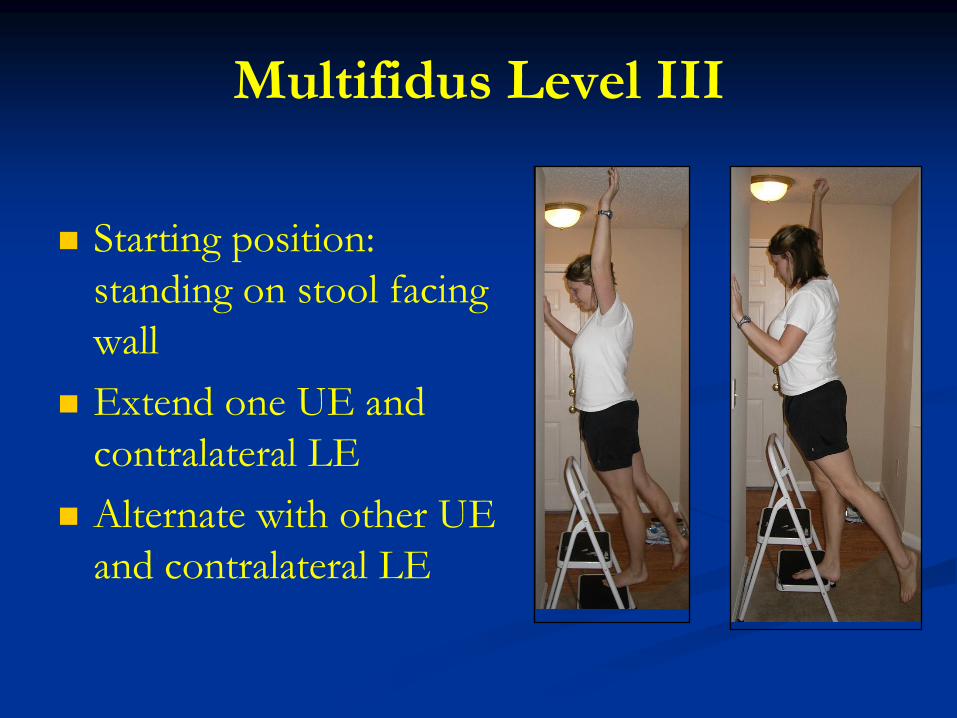
Multifidus Level III
Starting position:
standing on stool facing
wall
Extend one UE and
contralateral LE
Alternate with other UE
and contralateral LE

Clinical Biomechanics:
Intervention Skill Sets
NMR (97112)
Longus Colli Isolation

Text References
Kendall, FP et al. Muscles Testing and Function
with Posture and Pain. Fifth edition, 2005.
Sahrmann, SA. Diagnosis and the Treatment of
Movement Impairment Syndromes. 2002.
Kisner, C & Colby LA. Therapeutic Exercise:
Foundations and Techniques. Fourth edition,
2002.