the intei-nat.oniil joj,-nal oí periudort. cs s. rcstoiative dentstry
TRANSCRIPT

The Intei-nat.oniil Joj,-nal oí PeriudorT. cs S. Rcstoiative Dentstry
93
The Influence of Sulfate-ReducingBacteria Colonization of 2 DifferentBioresorbable Barrier Membranes forGTR. An 18-Month Case-ControlledMicrobiologie and Clinical Study
W.-D. Grimm, Dr med dent hab'il'/P. Cichon, Dr med dent hab(7"/H. van derHoeven, PhD'*VR S. Langendijk, PhD""/F. Smith, MS***'VM. G. Worley""-"'/I. Schmitz, PhD**""*/S. Offenbacher; DOS, PhD, MMSc****""
The purpose of the present microbiologie and case-controlled clinical study was toexamine the co'odization of 2 different resorbable barrier mernbranes by stitfate-reduc-ing bacteria [SRBJ. The barrier membranes tested were Guidor matrrx barrier andResolut regenerative material. Ten patients exhibiting 3 Class II furcation defects and 7intrabony defects were included in the study Tfie probing depth and the clinical attach-ment level at 4 surfaces per tooth were taken at tfie beginning oi^thesludy. Microbolo-gic samples were taken irom tfie expérimentai sites and from the approxrmai sites of theadjacent teeth. Both types of resorbable membranes were positive for 5RB colonization.The detection of SRB in 2 of 7 intrabony defects and in all defects witfi furcatjon involve-ment before the membrane placemer^t indicated that these organisms are a commoninhabitant ol sites showing periodontal destruction and are associated with guided tis-sue regeneration (GTR). According to the clinical criteria for healing tendencies used inthissludy, tfie GTR procedures were less successful iri the presence oi SRB. There wereno significant clinical effects of different resorbable membrane materials or membranelayout on attachrnent level changes for either the intrabony defect or furcation groupsafter 18 months. There were no statistical differences for sites that became exposed toSRB when compared to sites that remained unexposed after ) 8 months. The numericsignificance of SRB in relation to the total microbial count needs to be determined togain insight into the écologie role of membrane résorption rates. (Int J PeriodonticsRestorative Dent 2000;20:93-99.)
'Chair and Professor of Perbdontology, University of Witten, Germany; and AdjunctProfessor of Pen odontology. University of North Carolina at Chapel Hill.
"Professor of Pen odontology. University of WItten, Germany."•Professor of Oral Microbiology, Univeisity of Witten, Germany; and Explore Research
Laboratones, Nijmegen, The Netherlands.""Explore Research Laboratories, Nijmegen, The Netherlands.
"•'•Laboratory Manager, Center of Oral and Systemic Diseases, University of North Csroliraat Chapel Hill.
•"•"Information Manager, Center of Oral and Systemic Diseases, University of NorthCarolina at Chapel Hill.
" " " ' Inst i tu t of Pathology, Bergmanns h eil Hospital, University Clinic, Bochum, Geimany.•"'""•Department of Peri odontology. Center of Oral and Systemic Diseases, University of
North Carolina at Chapel Hill.
Reprint requests. Prof Dr Grimm, Department of Periodontology, University ofWitten/Herdecke, Alfred-Herrhausen-Strasse 50, 58448 Witten, Germany
Guided tissue regeneration (GTR)
has been used to regenerate perj-
odontal tissues lost as a result of
periodontal diseases. The objective
of a GTR procedure is to promote
formation of new connective tissue
attachment on a root surface that
has been detached because of
plaque-induced inflammation. Ny-
man et aP pioneered GTR using mil-
lipore (paper) filters. This impractical
material was soon replaced by ex-
panded polytetrafluoroethylene (e-
PTFE) membranes^ and by re-
sorbable materials (for review see
Greenstein and Caton- ), including
collagen,''-^ polyglycolic acid,* poly-
lactic add, and copolymers of the
latter 2.''-'2 The ability of both non-
resorbable and resorbable mem-
branes to elicit neoformation of con-
nective tissue attachment has been
fully documented.^•^•"' Infection is a
major complicating factor in GTR.'^
Bactériologie analyses of retrieved e-
PTFE barriers have demonstrated
bacterial contamination.^^"'^ Al-
though the histologie and clinical
events of GTR are well documented,
the role of bacterial enzymes in the
case of guided periodontal wound
Volume 20, Number 1, 2000

94
healing and regeneration is stilllargely poorly understood. The ex-tent of bacterial contamination ofthe barrier membranes correlatedinversely with clinical assessment ofattachment gain.^° One third ofall cultivable organisms were gram-negative anaerobic rods. This in-cluded black-pigmented rods andFusobacterium sp. ^ With respect toproteoglycan destruction, bacterialenzymes may play a significant role.Porphyromonas gingivalis strainsappear to be capable of degradingType I collagen.^^ In addition todirect tissue damage, indirect effectsof enzymes on proteoglycans have
The term sulfate-reducing bac-teria (SRB) describes a heteroge-neous groupé" of microorganismsthat has in common the dissimila-tory reduction of sulfate and oblig-ate anaerobiosis, A broad spectrumof organic substrates can serve aselectron donors; nearly all knownfermentation products from thedegradation of proteins, carbohy-drates, lipids, and components ofpoiylactic acid membranes could beused in a similarway. Sulfate-reduc-ing bacteria thereby produce hydro-gen sulfide. The detection of SRB inperiodontal pockets^^ indicated thatthese bacteria are common inhabi-tants of sites showing periodontaldestruction. The search for SRB wasundertaken because several condi-tions required for the growth ofthese bacteria are met in the peri-odontal pocket: (1) an anaerobicenvironment with a low redox poten-tial, (2) the presence of low-molecu-lar-weight fermentation products.
and (3) a neutral to slightly alkalinepH. Little is known ofthe influence ofSRB on barrier membrane degrada-tion in periodontal wound healingfollowing GTR.
The purpose ofthe present mi-crobiologie and clinical study was toexamine the colonization by SRS of2 different resorbable barrier mem-branes for periodontal regenerationand to follow up on the clinical out-comes over a period of 18 months.
Method and materials
In the study 2 types of commerciallyavailable barrier membranes wereused: Resolut regenerative material(3i/WL Gore) and Guidor matrix bar-rier (John O. Butler). The occlusivefilm in Resolut is composed of acopolymer of 85% polylactide and15% polyglycolide. The randomfiber matrix on both the inner andouter surfaces of the material isdesigned to provide rapid tissueintegration. A composition of 100%polyglycolic acid (PGA) was chosenbecause it satisfied the résorptiontime requirements. The polymermolecular weight and copolymerratio ofthe occlusive film were cho-sen after testing many combinations.The 85:15 composition resorbs moreslowly than the pure PGA fibers, pro-viding the 4- to 0-week occlusive-ness required for a GTR device. TheGuidor membrane is composed ofpoiylactic acid with a multilayerdesign, softened with citric acid toachieve malleability. The résorptionprocess is programmed to ensurebarrier function for a minimum of 6
weeks, after which it slowly resorbswithout interfering with the regen-erative healing process.
Patients
Patients enrolled in this study^* hadclinical evidence of either Glass IIfurcation invasions or intrabonydefects. They were in good physicalhealth and had no previous peri-odontal treatment on the teeth con-sidered for treatment. Ten patientsexhibiting 3 Glass II furcation defeirts(2 Guidor matrix barriers and oneResolut regenerative material) and 7intrabony defects (3 Guidor and 4Resolut) were enrolled in the study.The patients' ages ranged from 28 to49 years. Initial therapy, deep scal-ing, and root planing were per-formed on teeth scheduled forregenerative therapy consideringthe treatment protocol of the au-thors' department (University ofWitten).
Surgical protocol
The basic surgical protocol was com-parable to that already described inrecent studies.''^^ The buccal andlingual intrasulcular incisions werecarefully performed for preservingthe interdental papilla (modifiedpapilla presentation technique'*). Afull-thicknessflap was raised past themucogingival junction to providebetter access to the defect. Verticalreleasing incisions were performedas needed to increase defect ac-cessibility. The epithelium and the
The International Journal of Periodontics & Restorative Dentistry

95
granulation tissue ofthe inner sur-face of the flap were removed andthe root surface and/or the furcationarea were cleaned using curettes andan ultrasonic device with a flame-shaped diamond working tip Re-sorbable membranes were adaptedto cover the furcation area or theintrabony defect, extending up to 3mm apical to the bone crest. Thefull-thickness flap was coronally dis-placed for complete coverage ofthemarginal border of the membrane.To accomplish this, a fenestraticnincision ofthe periosteum was per-formed at the base of the flap. Themembrane was tightly attached tothe tooth by a resorbable slingsuture. The flap was sutured.
Soft tissue clinical measure-ments were taken the day of surgery(baseline) and 6 weeks after surgery.To evaluate wound healing, mea-surements were made using a scoreof visible gingival inflammation andexposure ofthe barrier membrane (3grades): normal wound healing with-out visible gingival inflammation(grade 1}; delayed wound healingwith visible signs of gingival inflam-mation (grade 2); and delayedwound healing with barrier mem-brane exposure (grade 3). The fol-lowing clinical measurements weretaken at the time of surgery and 6and 18 months after surgery^^: gin-gival recession (GR), probing depth(PD), and clinical attachment level(CAL), Furcations were probed usinga PCP-11 probe (Hu-Friedy); PD andCAL were measured on 4 surfaces ofthe experimental sites.
Patients were instructed to rinsetwice daily with 0.2% chlorhexidine
and to use modified oral hygieneprocedures for 2 weeks in the treat-ment groups. Professional toothcleaning was performed weekly forthe first 6 weeks.
Microbiologie monitoring
The samples were taken from theexperimental sites and from theapproximal sites of the adjacentteeth before membrane placementand after 6 weeks. Sterile paperpoints were inserted one after theother into the area of the furcationentrance or into the pocket. After20 s, the points were withdrawntogether (pooled samples) anddropped into a 2-mL screw-cap vialwith a semisynthetic medium. Thissemisynthetic basal medium with apH of 7.2 and a redox potentialbelow -100 mV^^ was used forenrichment of SRB in the peri-odontal plaque samples. The sam-ples were incubated in an anaerobicchamber (Braun) at 35°C in an at-mosphere of 91% Nj , 4% Hj, and5% COj, and an oxygen concen-tration below 5 ppm, Agar plateswere prepared with the samemedium, supplemented with 20 g/Lof agar
Sulfate reduction in the primaryenrichment cultures was indicatedby strong blackening caused by theprecipitation of FeS, Tenfold serialdilutions ofthe enrichment culturewere plated onto agar medium andincubated for 21 days. Blackeningofthe plates indicated the presenceof colonies of SRB, All incubationwas done in the anaerobic chamber.
Results
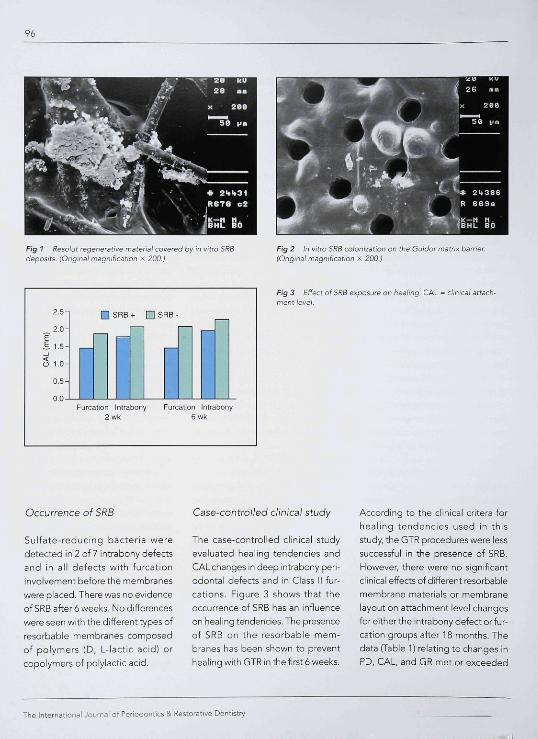
In a preliminary study,^^ the authorsinvestigated the in vitro colonizationof resorbable barrier membranes.Figure 1 shows Resolut regenerativematerial colonized in vitro by SRB,The résorption process programmedto ensure barrier function for a mini-mum of 6 weeks was not disturbed orinfluenced by the presence of SRB,and the barrier membranes slowlyresorbed. Figure 2 shows in vitro SRBcolonization of the Guidor matrix bar-rier. In a further in vitro study,^' theauthors investigated the colonizationof 3 types of of resorbable nonim-pregnated and tetracycline-impreg-nated membranes by strains of SRBand Pgingivalis. The study evaluatedwhether the tetracycline-impreg-nated membranes could inhibit bac-terial adhesion and penetration intomembranes. Strains of SRB wereoriginally isolated from periodontalpockets and were characterized byphylogenetic analysis of 16 S rDNAsequences. Scanning electron micro-scopy (SEM) analysis revealed differ-ences in the accumulation of SRBstrains and P gingivalis on the mem-branes. The tetracycline-impreg-nated membranes showed fewerbacteria attached and less evidenceof colony formation than the non-treated membranes. In general, theaffinity of the bacteria to the mem-branes was low. Cell aggregateswere found primarily on rough areasof the membranes. These in vitrostudies underscore the importance ofcontrolling putative periodonto-pathogens in barrier membranes andthe associated surgical sites in GTR.
Volume 20, Number 1, 200O
96
Fig 1 Résolut regeneratii/e matenal covered by in vitro SRßdeposits. (Original magnification x 200.}
Fig 2 In vitro SRB colonization on ffie Cuidor matrix barrier.(Orrgma) magnilication x 200.)
2.5-
2.0-
S 1.0-
0.5-
Furcalion intrabony Furcation Inlrabony2 wh 6 wk
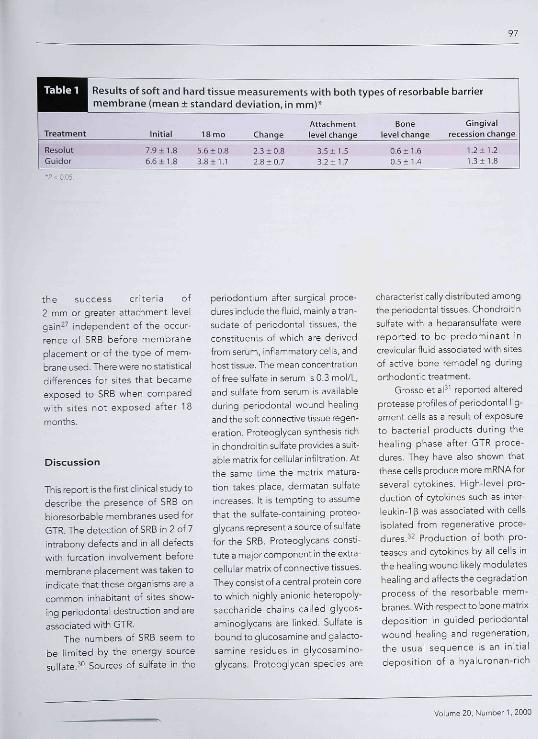
Fig 3 Effect of SRB exposure on healing. CAL = cfínrcaí attach-ment ievel.
Occurrence of SRB
Sulfate-reducing bacteria weredetected in 2 of 7 intrabony defectsand in all defects with furcationinvolvement before the membraneswere placed. There was no evidenceof SRB after 6 weeks. No differenceswere seen with the different types ofresorbable membranes composedof polymers (D, L-lactic acid) orcopolymers of polylactic acid.
Case-controlied clinical study
The case-controlled clinical studyevaluated healing tendencies andCAL changes in deep intrabony peri-odontal defects and in Class II fur-cations. Figure 3 shows that theoccurrence of SRB has an influenceon healing tendencies. The presenceof SRB on the resorbable mem-branes has been shown to preventhealing with GTR in the first 6 weeks.
According to the clinical critera forhealing tendencies used in thisstudy, the GTR procedures were lesssuccessful in the presence of SRB.hlowever, there were no significantclinical effects of different resorbablemembrane materials or membranelayout on attachment level changesforeitherthe intrabony defect or fur-cation groups after 18 months. Thedata (Table 1) relating to changes inPD, CAL, and GR met or exceeded
The International Journal of Periodontics & Restorative Dentistry
97
Table 1
Treatment
ResolutGuidor
Results of soft and hard tissue measurements with both types of resorbable barriermembrane (mean ± standard deviation, in mm)*
AttachmentInitial 18 mo Change level change
7.9 ± 1.8 5.6 ± 0,8 2.3 ± 0,8 3,5 ±1.5ö,6±1.8 3,8+1.1 2,8±0.7 3.2 + 1.7
Bonelevel change
0.6 ± 1,60,5 ± 1,4
Gingivalrecession change
1,2±1,21.3 + 1.8
the success criteria of2 mm or greater attachment levelgain^^ independent of the occur-rence of SRB before membraneplacement or of the type of mem-brane used. There were no statisticaldifferences for sites that becameexposed to SRB when comparedwith sites not exposed after 18months.
Discussion
This report is the first clinical study todescribe the presence of SRB onbioresorbable membranes used forGTR. The detection of SRB in 2 of 7intrabony defects and in all defectswith furcation involvement beforemembrane placement was taken toindicate that these organisms are acommon inhabitant of sites show-ing periodontal destruction and areassociated with GTR,
The numbers of SRB seem tobe limited by the energy sourcesulfate.^° Sources of sulfate in the
periodontium after surgical proce-dures include the fluid, mainly a tran-sudate of periodontal tissues, theconstituents of which are derivedfrom serum, inflammatory cells, andhost tissue. The mean concentrationof free sulfate in serum is 0.3 mol/L,and sulfate from serum is availableduring periodontal wound healingand the soft connective tissue regen-eration, Proteoglycan synthesis richin chondroitin sulfate provides a suit-able matrix for cellular infiltration. Atthe same time the matrix matura-tion takes place, dermatan sulfateincreases. It is tempting to assumethat the sulfate-containing proteo-glycans represent a source of sulfatefor the SRB. Proteoglycans consti-tute a major component in the extra-cellular matrix of connective tissues.They consist of a central protein coreto which highly anionic heteropoly-saccharide chains called glycos-aminoglycans are linked. Sulfate isbound to glucosamine and galacto-samine residues in glycosamino-glycans. Proteoglycan species are
characteristically distributed amongthe periodontal tissues, Chondroitinsulfate with a he pa ran su If ate werereported to be predominant increvicular fluid associated with sitesof active bone remodeling duringorthodontic treatment.
Grosso et aP' reported alteredprotease profiles of periodontal lig-ament cells as a result of exposureto bacterial products during thehealing phase after GTR proce-dures. They have also shown thatthese cells produce more mRNAforseveral cytokines, i-iigh-level pro-duction of cytokines such as inter-leukin-Tß was associated with cellsisolated from regenerative proce-dures,^^ Production of both pro-teases and cytokines by all cells inthe healing wound likely modulateshealing and affects the degradationprocess of the resorbable mem-branes. With respect to bone matrixdeposition in guided periodontalwound healing and regeneration,the usual sequence is an initialdeposition of a hyaluronan-rich
Volume 20, Number 1, 2000

matrix with plasma proteins. Sulfate-
reducing bacteria require free sul-
fate for their growth, but can also
liberate the sugar-bound sulfate (P,
S. Langendijk, unpublished data).
Sulfatase activity—most likely from
lysozomal origin—in oral bacteria
has been detected so far in Strepto-
cocci and Campy/obacter,^^ which
are found in periodontal pockets.
Sulfate-reducing bacteria produce
equimolar amounts of sulfide from
the reduction of sulfate. Hydrogen
sulfide is considered to be toxic to
mammalian cells by inactivation of
cytochrome oxidase,^'' its ability to
split disulfide bonds in proteins and
binding of various metal ions.
Further, H S in periodontal sites
during wound healing may well ori-
ginate from the degradation of cys-
teine by SRB. The numeric sig-
nificance of SRB in relation to the
total microbial count needs to be
determined to gain insight into the
écologie role of membrane résorp-
tion rates.
References
1 Nyman S, Gottlow J, Karring F, Lindhe J,The regenerative potential of the peri-odontal ligament. An experimental studyin the monkey. J Periodontol 1982;9:257-265.
2. Caffesso RG, Smith BA, Castelli WA,NasjIetiCE. New attachment achieved byguided tissue regeneration in beagledogs. J Periodontol 19e8;59:589-594.
3. Greenstein G, Caton JG. Biodegradablebarriers and guided tissue regenerationPcnodontol 2000 1993,1 36-45.
4. MinabeM. A critical review of the biolog-ic rationale for guided tissue regenera-tion. J Periodontol 1991;62:171-179.
5. PfeiferJ,Van5wolRL,EllingerR. Epithelialexclusion and tissue regeneration using acollagen membrane barrier in chronic peri-odontal defects: A histologie study. Int JPeriodontics Restorative Dent 19e9;9:2Ó3-273.
Ó. Gager AH, Schute AJ. Treatment of peri-odontal defects with an absorbablemembrane (polyglactin 910) with andwithout osseous grafting: Case reports, JPeriodontol 1991;á2;276-283.
7. LaurellL, FaIkH, FornellJ,JohardG,Got-tlomJ.Cllnicaluseof abioresorbablema-trix barrier in guided tissue regenerationtherapy. Case series. J Periodontol 1994;65:967-975.
8. Falk H, Laurell L, Ravald N,Teiwil< A, Pers-son R. Guided tissue regeneration thera-py of 203 consecutively treated intrabonydefects using a bioabsorbable matrix bar-rier. Clinical and radiographie findings. JPeriodontol 1997;68;571-581.
9. LundgrenD, Laurell UGottlomJ, RylanderH, Mathisen T, Nyman S, Rask M, The influ-ence of the design of two different biore-sorbable barriers on the results of guidedtissue regeneration therapy. An intra-indi-vidual comparative study in the monkey. JPeriodontol 1995;66:605-612.
10. Becker W, Becker BE, Mellonig J, Caf-fesse RG, Warrer K, Caton JG, Reid T. Aprospective multi-center study evaluat-ing penodontal regeneration for Class IIfurcation invasions and intrabony defectsafter treatment with a bioabsorbablebarrier membrane: 1-year results. JPeriodontol 1996;67:641-649.
11. Hürzeler MB, QuifionesCR, Caffesse RQ,Schupbach P, Mornson EC. Guided peri-odontal tissue regeneration in interprox-imal intrabony defects following treat-ment with a synthetic bioabsorbable bar-rier J Periodontol 1997;68:489-a97
12. Hurzeler MB, Quiñones CR, Caffesse RG,Schupbach P, Morrison EC. Guided peri-odontai tissue regeneration in Class II fur-cation defects following treatment witha synthetic bioabsorbable barrier. JPeriodontol 1997;68:498-505.
13. Chnstgau M, Schmalz G, Wenzel A, HillerKA. Periodontal regeneration of intra-bony defects with resorbable and non-resorbable membranes: 30-monthresults. J Clin Periodontol 1997;24:17-27.
14. Cortellini P, Pini Prato G, Tonetti S. Perio-dontal regeneration of human intrabonydefects with bioresorbable membranes.A controlled clinical trial. J Periodontol1996;67:217-223.
15. Mombelli A, Lang NP, Nyman S, Isolationof periodontal species after guided tissueregeneration. J Periodontol 1993;64:1171-1175
10. Machtei EE, Cho Ml, Dunford R, NoiderydJ, Zambón JJ, Genco RJ. Clinical, micro-biological, and histological factors whichinfluencethe success of regenerative peri-odontal therapy. J Periodontol 1994,65:154-1Ó1.
17. Nomzari H, Slots J. Microorganisms inpolytetrafluoroethylene barrier mem-branes for guided tissue regeneration. JClin Periodontol 1994;21:203-210.
18. Nowzari H, MacDonald ES, Flynn J,London RM, Morrison JL, Slots J. Thedynamics of microbial colonization of bar-rier membranes for guided tissue regen-eration. J Periodontol 1996;67:694-702.
The International Journal of Periodontics & Restorative Dentistry
99
19. Simionlvl,TrisiP, MaglioneM,PiattelliA,A preliminary report on a method forstudying the permeability of expandedpolytetrafluoroethylene membrane tobacteria in vitro: A scanning electronmicroscopic and histological study. JPeriodontol 1994:65:755-761.
20. Selvig KA, Nilveus RE, Fit^morris L,Kersten B, Thorsandi SS. Scanning elec-tron microscopic observations of cell pop-ulation and bacterial contamination ofmembranes used for guided periodontaltissue regeneration in humans. JPeriodontol 1990;61:515-520.
21, Mombelli A, Zappa U, Brägger U, LangNP. Systemic antimicrobial treatment andguided tissue regeneration. Clinical andmicrobiological effects in furcationdefects. J Clin Periodontol 1996:23:3B6-396.
22, Smalley JM, Birss AJ, Shuttleworth CA.The degradation of Type I collagen andhuman plasma fibronectin by the trypsin-lil<e enzyme and extracellular membranevesicle of Sacterrodes gingivslis W50.Arch Oral Biol 1988:33:323-329.
23, Kuramitsu HK. Molecular genetic ap-proach for identifiying virulence factorsof Pofphyromonas gingivalrs. In: GencoR led). Molecular Pathogenesis of Peri-odontal Disease. Washington, DC: ASMPress, 1994:25-32.
24. Langendijk PS, Sandmeier H, Meyer J,van der Hoeven JS. Phylogenetic analy-sis of sulphate-reducing bacteria in theperiodontal pocket [abstr 1717], J DentRes 1997;76:228.
25, van der Hoeven JS, van der KieboomCWA, Schaecken MJM. Sulfate-reducingbacteria in the periodontal pocket. OralMicrobiol Immunol 1995:10:288-290.
26. Grimm W-D, Cichon P, Crawford L, LoreyT, Klinische Längsschnittstudie zur ges-teuerten Geweberegeneration mit resor-bierbaren Membranen (Gore Resolutregenerative material). Parodontologie1996;3:237-245,
27. Tonetti S, Fini PratoG,CortelliniP Factorsaffecting the healing response of intra-bony defects following guided tissueregeneration and access flap surgery. JClin Periodontol 1996:23:548-556.
28. Grimm W-D, van der Hoeven JS, van derKieboom CWA. Colonization of barriermembranes for periodontal regenera-tions by sulfate-reducing bacteria [abstr802]. J Dent Res 1997:76114.
29. Grimm W-D, Grimm K, van der HoevenH, Langendijk P, Schmitz I, Lee HJ, Wil-liams R. Degradation and colonization ofresorbable non-impregnated and tetra-cycline-impregnated membranes forperiodontal regeneration by periodon-topathogens. Proceedings of the 84thAnnual Meeting ofthe American Acad-emy of Periodontology, Boston, 12-16September 1998, 167.
30. Kenney E, Ash MM. Oxidation reductionpotential of developing plaque, peri-odontal pockets and gingival sulci. JPeriodontol 1969;40:630-633.
31. Grosso LT, Iha DK, Niu J, WakabayashiRC. Protease profiles of cells isolated fromregenerative membranes are associatedwith clinical outcome. J Periodontol 1997:68:809-B18,
32. Wakabayashi RC, Iha DK, Niu J, JohnsonPW. Cytoklne production by cells adher-ent to guided tissue regeneration mem-branes. J Penodontal Res 1997,32:215-224.
33. WyssCCampylobacter-Wolinella grouporganisms are the only bacteria that formarylsulfatase-actjve colonies on a syn-thetic indicator medium. Infect Immunol1969:57:1380-1383.
34 Nicholls P, Kim KJ. Sulphide as an inhibitorand electron donor for the cytochrome coxidase system. Can J Biochem 1982:60:613-Ó23.
Volume 20, Number 1, 2000