the internationa! journal of periodontics & restorative dentistr
TRANSCRIPT
The Internationa! Journal of Periodontics & Restorative Dentistr

521
Histologie Analysis of a FracturedImplant: A Case Report
Gérard Brunei
Serge A rmand"
Neat Miller***
Jacqueline Rue****
This study presents the histoiogic anaiysis of an impiant retrieved 74 months aiter
loading because of a fracture in the collar region. The implant ¡BioventJ was
removed with part of the penimplant tissues, and the block was prepared using
cutting and grinding equipment to obtain 3 sections approximately 30 firn thicfc.
The examination evidenced a high degree oi osseointegration, with a faone-to-
Implant contact of 74% ± T3%. Tho lamellar bone was dense and in c'ose relation
with the hydroxy apatite coating of the implant. The connection between the 0 4-
mm hydroxyapatite coating and the metal was always very tight. The thickness of
the meta/at the breaic point tvas assessed to be í,ó mm. Besides the relative
weakness ofthe metal at the neck of the implant, other possible causes of failure
are discussed, {Int J Periodontics Restorative Dent 2000;20:521-52ó,)
•Professor. Department of Oral Biology, Faculty of Odontology, PaulSabatier University, Toulouse, France.
••Maïtie de Conférence de l'Université, Department of Prosthadontics,Faculty of Odontology, Paul SabatJer University, Toulouse, France.
"Mai'tie de Conférence de l'Université, Department of Periodontology,
Faculty of Odontology, Nancy University, Nancy, Prance.'»Technician, Department of Oral Biology, Faculty of Odontology, Paul
Sabatier University, Toulouse, France.
Reprint requests. Dr Gérard Brunei, Faculté de Chirurgie Dentaire, 3Chemin des Maraîchers, 31062 Toulouse Cedei, Fiance, e-mail:brunel@,dct fr
In spite of a high percentage of long-
term successes, some implant fail-
ures occur for different reasons,
including impaired healing, micro-
btal contamination, or mechanical
problems. Among these possible
complications, fractures hold an
important place,'"" Subsequent
analyses of failed implants, whether
histologie,^ histochemical,* or elec-
tromicroscopic,*'^ provide invaluable
data that contribute to the evolution
of implant systems and the devel-
opment of measures to prevent fail-
ures. It was in thisframeof mind that
the histoiogic analysis of a Biovent
(CoreVent) implant was performed
following the fracture of its collar.
Clinical report
A 50-year-old partially edentulous
patient consulted for a complete
rehabilitation of his maxillary arch.
After clinical and radiographie eval-
uation, it was decided to construct
a dentoimplant-supported fixed
prosthesis on 8 vital residual teeth
(maxillary right second molar,
canine, and lateral incisor and left
Volume 20, Number 5, 2000
522
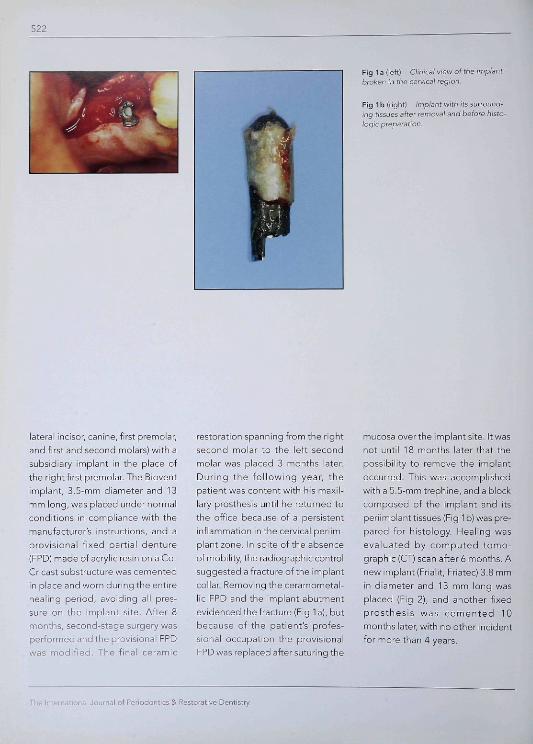
Fig la (left) Clinical view of the implantbroken in the cervical region.
Fig 1 b (right) fmpiant with its surround-ing tissues after removal and before histo-logie preparation.
lateral incisor, canine, first premolar,and first and second molars) with asubsidiary implant in the place ofthe right first premolar. The Bioventimplant, 3,5-mm diameter and 13mm long, was placed under normalconditions in compliance with themanufacturer's instructions, and aprovisional fixed partial denture(FPD) made of acrylic resin on a Co-Cr cast substructure was cementedin place and worn during the entirehealing period, avoiding all pres-sure on the implant site. After 8months, second-stage surgery wasperformed and the provisional FPDwas modified. The final ceramic
restoration spanning from the right
second molar to the left secondmolar was placed 3 months later.During the fol lowing year, thepatient was content with his maxil-lary prosthesis until he returned tothe office because of a persistentinflammation in the cervical periim-plant zone. In spite ofthe absenceof mobility, the radiographie controlsuggested a fracture ofthe implantcollar. Removing the ceramometal-lic FPD and the implant abutmentevidenced the fracture (Fig la), butbecause of the patient's profes-sional occupation the provisionalFPD was replaced after suturing the
mucosa over the implant site. It wasnot until 18 months later that thepossibility to remove the implantoccurred. This was accomplishedwith a 5.5-mm trephine, and a blockcomposed of the implant and itsperiimplant tissues (Fig 1 b) was pre-pared for histology. Healing wasevaluated by computed tomo-graph ic{CT) scan after 6 months. Anew implant (Frialit, Friatec) 3.8 mmin diameter and 13 mm long wasplaced (Fig 2), and another fixedprosthesis was cemented 10months later, with no other incidentfor more than 4 years.
The International Journal of Peiiodontics S Restorative Dentistry
523
Histologie preparation
The specimen was fixed in 10% neu-tral buffered formalin soiution, dehy-drated with ethanol containing 0.3%basic fuchsin, and embedded inmethyl methacryiate as describedby Stich.^ The block was sectionedusing a bandsaw and further groundto a thickness of approximately 30|jm. The 3 ground sections werecounterstained with light green andexamined under optic microscopy.The histologie observation assessedthe quality ofthe periimplant bone,the bone-to-implant interface, andthe implant design. Histomorpho-metric analysis was performed oneach section using an image-analy-sis system (Optilab, Graftek) coupledwith a video camera on the micro-scope. The bone-to-implant-contact(BIC) length was measured at a mag-nification of 1OOX as a percentage oftotal implant length."
Results
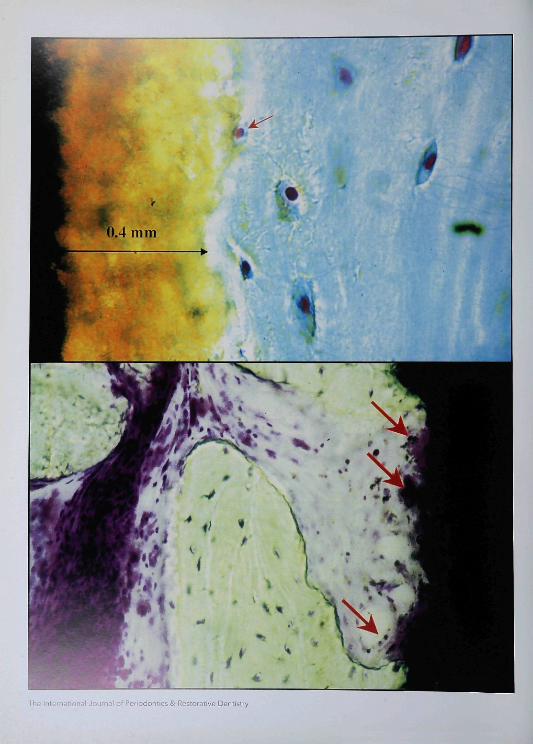
Figure 3 shows a global view of theimplant and its periimplant tissues. Inspite of the loss of these tissues inthe most cervical region during tre-phination, the degree of osseointe-gration appeared to be quite highon the light microscopic level. Theimplant was coated with hydroxyap-atite (HA), the thickness of which wasassessed to be about 0.4 mm (Figs4 and 5). The HA coating was in closerelation with the alveolar bone, andthe BIC mean was 74% ± 13%. Thebone structure was lamellar anddense, with many cells and few
medullar spaces (Fig 4), Some osteo-cytes were directly in contact withthe HA coating (Fig 5). A vascular-ized connective tissue layer pro-duced a very localized résorption ofthe HA coating (Fig 6). The bondingbetween the implant metal and theHA layer was very tight and contin-uous at all points (Fig 5). The designof the implant neck included a nar-rowing of the metal, which was 1.6mm thick in the fracture zone (Fig 7).
Discussion
The histologie examination demon-strated that the Biovent implant wascorrectly osseointegrated, as is thecase with most broken implants,around which authors have de-scribed lamellar bone, both matureand compact, providing 70% to100% contact.''•'•'° The choice of anHA-ccated implant was made be-cause the osteoconductive charac-teristics of this material enable a re-duction of the healing period,^'although some consider the prog-nosis to be uncertain,'^ Although asmall résorption spot was detected inthe HA coating (Fig 6), it is impon:antto insist on the quality of bone-HAand HA-metal interfaces in opposi-tion to other studies that describeHA particles in the cytoplasm cfmultinucleated cells," more or lessextensive dissolution of the coating,or an interruption of HA-metal con-nection.^ In the present case, thequality ofthe osseointegration char-acterized by a BIC of more than 70%can be explained by the fracture just1 year after loading, similar to the
Volume 20, Number 5, 2000

524
Fig 2 Radiograph of the Fnabt impiantrepiacing the Biovenr impiant in the site ofthe ma;<)7l3ry eight first premolar.
Fig 3 Genera! urew ofthe most mediansection. The implant appears well osseoin-tegrated for 'A of its height. The bone inthe cervicai third was iost during removalwith the trephine. The cifcied fragnienf is apiece of metai coated with hydroxyapatitethat was ripped off during the specimengrinding. (Original magnification >' 16;fuchsin and light green slam,J
Fig 4 Higher-power view of section afrom Fig '3. The periimpiant bone appearsnormaiiy dense and presents few meduilarspaces Between the metal ofthe implantand the bone, the thin gray outline is thehydroiyapatite coating. fOfiginai magnifi-cation - 40; fuchsin and iight green stain.)
Fig 5 Bone-hydroxyapatile-metal inter-face. The osseous lissue contains nunierousceils (osteocytes), some of wi^ich are directly¡n contact witfi the hydroxyapatite coating(red arrow], Ciose contacts eiist betweenthe bone and the hydroxyapafite, as well asbetween the hydroxyapatile and the blackmetal. The fhicl ness of ihe coating wasassessed to be 0.4 mm. (Original magnifica-tion / 250: fuchsin and light green stain.)
Fig 6 Higher-power uieiv of section bfrom Fig 3. The direct contacf of a medulla;space wiiii (he hydraxyapalile layer canlocally produce a résorption (arrows) thatreduces the thickness oí coating, (Originalmagnification X ¡60; fuchsin and lightgreen stain,)
Fig 7 Higher-power view of section cfrom Fig 3. On the part of the jmpJant col-isr that is still intact, the thiclfness o'ihemetal is only 1.6 mm, (Original magnifica-tion X 100, fuchsin and light green stain.)
The International Journal of Periodontics & Restorative Dentistry
525
report by Piattelli and Trisi,'^ How-
ever, unlike these authors,^ we did
not observe any osteoid border
along the surface of the coating,
which seems normal for an implant
that had not been loaded for 18
months.
Mechanical ruptures are still
responsible for too many failures in
implantology. In a retrospective sur-
vey of 8 years and 230 implants,
Piattelli et al" determined that of all
oftheirfailures, 40% were because of
fractures. As in this case, the frac-
tures occurred relatively soon after
loading—70% of the fractures were
early. This corroborates the work of
other authors, some of whom ob-
served fractures during the first
year,^'' with most during the first 5
years.'^ Ahead of all other causes,
mechanical tensions are responsible
for implant fractures,^•^''•^* and risks
seem greatest in the posterior re-
gions with short implants of stan-
dard diameters.'" The small-diame-
ter Biovent implant used to replace
the maxillary first premolar was in a
position strategic enough to impose
a canine-guided occlusion to avoid
excessive functional forces. However,
one must admit that there isa sort of
antagonism between the relative
mobility of natural teeth and the
ankylosisofan implant. A fixed pros-
thesis on natural teeth keeps a cer-
tain degree of mobility that produces
repetitive forces concentrated at the
connection between the suprastruc-
ture and the implant. In all implant
systems that have an internal antiro-
tational hexagon like Biovent, the
collar is the region subjected to the
most strain, which at length can
weaken the metal and finally pro-
duce a fracture.^''"^''" These obser-
vations question the indication of
mixed dentoimplant restorations.'•'"
Another risk factor is crestal résorp-
tion, which is inevitable with time'^
and may unfavorably increase the
crown-to-root ratio, thus accentuat-
ing mobility and weakening the cer-
vical region ofthe implants.
Of course, the design of certain
implant systems is also a source of
fragility,'^ like the holes in the hol-
low-cylinder implants.'" Indeed, the
thickness ofthe metal at the neck of
the Biovent implant did not seem
sufficient and could have presented
an aggravating risk in the presence
of unfavorable biomechanical con-
ditions.
This histoiogic analysis suggests,
though it does not present absolute
proof, that the strains caused by the
type of dentoimplant restoration
could have been the cause of the
fracture of the irnplant collar. The
thinness ofthe metal in this region
surely provided a "locus minoris
resistentiae" that increased the risk
of fracture.
Volume 20, Number 5, 2000
526
References
1, Lekholm U, van Steenberghe D, HerrmannI, Bolendef C, Folmer T, Gunne J, et alOsseointegrated implants in the treatmentof partially edentulous jaws-A prospective5-year multicenter study, Int J OralMaxilWac Implants 1994;9:627-635.
2, Friberg B, Jemt T, Leiiholm U, Early failuresin 4,641 consecutively placed Branemarkimplants: A study from stage 1 surgery tothe connection of completed prostheses,Int J Oral Maxillofac Implants 1991;6:142-146,
3, Balshi TJ, An analysis and management offractured implants: A clinical report. Int JOral Maxillofac Implants 1996;11 bbQ-ùbb.
4 Piattelli A, Scarano A, Piattelli M. Histologieobservations on 230 retrieved dentalimplants: 8 years' experience (1939-1996).J Periodontol 1998.69:178-184
5. Albrektsson T, Astrand P, Seeker W,Eriksson AR, Lekholm U, Malmquist J,Sennerby L. Histologie studies of faileddental implants: A letrieval analysis of fourdifferent oral implant designs Clin Mater1992:10:225-232
6. Piattelli A, Trisi P A light and laser scanningmicroscopystudyofbone/hydroxyapatite-coated titanium implants interface:Histochemical evidence of unmineralizedmaterial in humans. J Biomed Mater Res1994,28 529-536
7. Takeshita F, Matsushita Y, Ayukawa Y,Suetsugu T, Fractures of hydroxyapatite-coated blade implants connected with nat-ural teeth. A histobgical study using SEM,light microscopy, and an image processingsystem, J Penodontol 1996;67:86-92.
8. Stich H. Herstellung der Schliffpräparate.ln:SchroederA(ed) Orale Implantologie.Stuttgart: Thieme, 1988.109-115,
9. Gotfredsen K, Nimb L, Buser D, Hjarting-Hansen E. Evaluation of guided bone gen-eration around implants placed into freshextraction sockets: An experimental studyin dogs J Oral Maxillofac Surg 1993:51:879-884.
10. Piattelli A, Scarano A, Piattelli M, Vais E,Matarasso S. Hollow Implants retrievedfor fracture: A light and scanning electronmicroscope analysis of 4 cases. JPeriodontol 1998:09:18S-189.
11. Kay JF Calcium phosphate coatings fordental implants. Dent Clin North Am1992:36:1-18.
12. Biesbrock AR, Edgerton M. Evaluation ofthe clinical predictability of hydroxyap-atite-coated endosseous dental implantsA review of the literature. Int J OralMaxillofac Implants 1995;10:712-720,
13. Piattelli A, Trisi P. Microscopic and chem-ical analysis of bone-hydroxyapatite inter-face in a human retrieved implant. A casereport. J Periodontol 1993:64:906-909.
14 Rangert B, Krogh PH, Langer B, VanRoekel N. Bending overload and implantfracture A retrospective clinical analysis.Int J Oral Ma>;illofac Implants 1995:10:326-334
15 Steflik DE, Parr GR, Singh BB, Lake FT,Sisk AL, Howell FV, Shelton TW. Lightmicroscopic and scanning electron micro-scopic analyses of dental implants re-trieved from humans, J Oral Implantol1994:20:8-24,
16. ZarbG, Osseointegration: A requiem forthe periodontal ligament, Int JPeriodontics Restorative Dent 1991;1188-91.
17. Patterson EA, Johns RB. Theoreticalanalysis of the fatigue life of f xture screwsin osseointeg rated dental implants, Int JOral Maxillofac Implants 1992:7:2éH-33
18. SpiekermannH, Jansen VK, Richter EJ. A10-year follow-up study of IMZ and TPSimplants in the edentulous mandibleusing bar-retained overdentures. Int J OralMaxillofac Implants 1995;10:231-243.
The International Journal of Periodontics & Restorative Dentistry