the investigation of clotting abnormalities in
TRANSCRIPT

Coagulopathy in cytoreductive surgery patients
1
The investigation of clotting abnormalities in cytoreductive
surgery patients through thromboelastography
Dr Gary Sharp MBBS BSc (Hons)
A thesis submitted in fulfilment of the requirements for the degree of master of philosophy
Faculty of Medicine
University of Sydney
2021
Dedicated to my daughters, Poppy and Lola, who’s laughter and love give me such joy.

Coagulopathy in cytoreductive surgery patients
2
TABLE OF CONTENTS
Statement of originality 3
Acknowledgements 3
Assistants and nature of collaboration 4
Introduction 5
Chapter 1. Point of care viscoelastic assay devices (rotational thromboelastometry
and thromboelastography); a primer for surgeons.
13
Chapter 2. A systematic review of coagulopathy in cytoreductive surgery and
hyperthermic intraperitoneal chemotherapy patients.
31
Chapter 3. A pilot study to investigate the role of thromboelastography in
cytoreductive surgery and hyperthermic intraperitoneal chemotherapy patients.
59
Thesis discussion 87
Appendix 1. Project description. 95
Appendix 2. Patient information. 108
Appendix 3. Ethics approval. 110

Coagulopathy in cytoreductive surgery patients
3
STATEMENT OF ORIGINALITY
The work presented in this thesis is, to the best of my knowledge and belief, original except as
acknowledged in the text. I hereby declare that I have not submitted this material, either in full
or in part, for a degree at this or any other institution.
I understand that if my candidature is successful, my thesis will be lodged with the Director of
University Libraries and made available for immediate use.
Dr Gary Sharp
1/9/21
ACKNOWLEDGEMENTS
Thank you Professor Young for the continued support, not only during this MPhil but for the
years you have helped and motivated me. Thank you to the patients who so kindly agreed to
participate in these studies to further the knowledge of clinicians and ultimately help future.
Lastly, thank you to my family who have guided me and supported my dream for all these
years, I could not have achieved what I have without you. Paula, you are my rock.
Coagulopathy in cytoreductive surgery patients
4
ASSISTANTS AND NATURE OF COLLABORATION
Name Job title Nature of collaboration
A/Prof. Christopher
J. Young
Consultant colorectal
surgeon. Royal Prince
Alfred Hospital, Sydney,
Australia.
Supervisor. Reviewer in chief.
Dr Daniel Steffens Deputy director of
Surgical Outcomes
Research Centre, Royal
Prince Alfred Hospital,
Sydney, Australia.
Assistance with statistics during the following articles;
1. 1. Systematic review of the incidence and outcome of
coagulopathy in cytoreductive surgery and heated
intraperitoneal chemotherapy patients.
2. 2. A pilot study to investigate the role of thromboelastography
in cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy patients.
Dr Rebecca
McNamara
Consultant anaesthetist.
Royal Prince Alfred
Hospital, Sydney,
Australia.
Data collection.
Collection of TEGs intraoperatively during “A pilot study to
investigate the role of thromboelastography in cytoreductive
surgery and hyperthermic intraperitoneal chemotherapy
patients”.
Dr Neil Pillinger Consultant anaesthetist.
Royal Prince Alfred
Hospital, Sydney,
Australia.
Data collection.
Collection of TEGs intraoperatively “A pilot study to
investigate the role of thromboelastography in cytoreductive
surgery and hyperthermic intraperitoneal chemotherapy
patients”.
Dr Nabila Ansari Consultant colorectal
surgeon. Royal Prince
Alfred Hospital, Sydney,
Australia.
Assistance with forming a project description for “A pilot
study to investigate the role of thromboelastography in
cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy patients”.
Dr Daniel Oh Senior resident medical
officer. Royal Prince
Alfred Hospital, Sydney,
Australia.
Collected data from medical notes to assist with “A pilot
study to investigate the role of thromboelastography in
cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy patients”.
Coagulopathy in cytoreductive surgery patients
5
Introduction
Abdominal cytoreductive surgery (CRS) is the macroscopic removal of intraperitoneal
malignancy (1, 2). CRS has been utilised in one form or another since the 1930’s during which
time tumour debulking procedures in ovarian malignancy were being undertaken to reduce
tumour burden (3). Further interest in CRS developed until eventually, positive survival
outcomes were consistently reported in the 1960’s (4). Following on from these positive
outcomes seen in gynaecological malignancy, surgeons began to investigate pseudomyxoma
peritonei (PMP), a mucus-producing tumour that arises from an appendiceal tumour or less
commonly an ovarian tumour (5,6). Surgeons set about reducing the PMP tumour burden
through evacuating the space-occupying mucin coupled with resection of affected viscera. The
rationale for this new cytoreductive practice was that if there was less tissue within the
peritoneal cavity the chemotherapy agents would have a greater impact of the residual tissue
volume, plus reducing the risk of later complications such as obstruction (6).
Coupled with the increased enthusiasm for CRS was a desire to identify the most potent but
least toxic route of chemotherapy. The use of intraperitoneal chemotherapy was initially
described by Weisberger et al. in 1955 who utilised intraperitoneal nitrogen mustard to manage
malignant ascites (7). Ensuing canine studies revealed that intraperitoneal chemotherapy,
versus intravenous, had much higher local anticancer effect without increased systemic
toxicity; (8) this remains true to today (9). The advent of a heated chemotherapy delivery
system to deliver intraperitoneal chemotherapy was realised by Spratt et al. (1980) and
although not termed HIPEC as yet it delivered heated chemotherapy safely (10). Spratt et al
went on to treat the first human with their design in 1979 for PMP; he survived.
Coagulopathy in cytoreductive surgery patients
6
CRS research continued to focus mostly on ovarian malignancy until Dr Paul H Sugarbaker of
the United States began to focus on CRS and HIPEC in gastrointestinal malignancies
presenting with peritoneal disease. Dr Sugarbaker’s plethora of research into this area began to
standardise intraabdominal CRS procedures (11). Sugarbaker also highlighted the use of a
“coliseum”, a plastic sheet secured to both the skin edges and a retraction device which elevates
skin edges, to administer the HIPEC solution a defect within the plastic sheet is made, thus
allowing an even distribution of chemotherapy solution throughout the abdomen whilst also
allowing manipulation of intraabdominal viscera by the surgeon to ensure all peritoneal
surfaces are in direct contact with the agent (12).
Next, researchers developed a standardised approach to classify peritoneal malignancy, the
Peritoneal Cancer Index (PCI). PCI was developed by a collaborative group in the 1990’s and
involves dividing the abdomen into 9 segments and the small bowel into a further 4 segments
(13). Each segment is then scored:
• 0 - no disease
• 1 - tumour deposits up to 0.5cm
• 2 - tumour >0.5-5.0cm
• 3 >5.0cm deposits
The score for all segments are calculated to provide a total out of 39 (13). PCI, used to this day,
allows surgeons to evaluate tumour burden and the possible effectiveness of CRS (14).
Subsequent to PCI, completeness of cytoreduction score (CC) was developed which aimed to
catagorise residual tumour following CRS prior to HIPEC (15):
• CC0 - no visible tumour seen post CRS
• CC1 - any single tumour deposit no larger than 2.5mm
Coagulopathy in cytoreductive surgery patients
7
• CC2 - tumour deposits of 2.5mm-2.5cm
• CC3 – tumour deposits >2.5cm (15).
Surgical curative intent is aimed at reaching a CC1 or less. The rationale for this size of tumour
deposit is directly related to the penetration depth of HIPEC, which at maximum is 5mm
(16,17). However, CC0 is the gold standard and produces the best outcome in terms of overall
survival (14). Many trials in the subsequent years have been carried out and the consensus now
is that CRS and HIPEC are beneficial in PMP (18) and selective peritoneal carcinomatosis
(9,14).
Despite evidence highlighting CRS and HIPEC’s survival advantages, it is also acknowledged
that it is a procedure not to be undertaken lightly. CRS procedures are long, some suggesting a
mean of 10.5 hours (16), they are financially demanding for the institution (14) and have
significant morbidity and mortality attached (16,19). Bleeding in the CRS/HIPEC population
is a well-known complication resulting in significant reoperation (16,19). These patients are
also known to be susceptible to coagulopathy (20), the cause of which is not entirely known
but is thought to be multifactorial (5,21). However, the outcome of this coagulopathy continues
to be inadequately understood (22).
Standard laboratory tests are commonly used to assess bleeding. These tests include an
international normalised ratio (INR), prothrombin time (PT) and activated partial prothrombin
time (aPTT). Unfortunately, their accuracy at assessing bleeding risk and managing blood
product replacement has been shown to be lacking (23). Instead, the use of viscoelastic (VE)
assays such as thromboelastography (TEG) have been suggested to be far more appropriate
in diagnosing and treating massive haemorrhage (24). The use of TEG in guiding blood
Coagulopathy in cytoreductive surgery patients
8
transfusion is gaining recognition in its ability to potentially reduce unnecessary blood product
transfusion which in turn reduces patient morbidity (25).
The use of TEG in general surgery is limited and as such, general surgeons and trainees know
little about VE assay mechanisms, interpretation and use. The first aim of this thesis is to
produce a narrative review of VE assay technology, result interpretation, current uses and
potential uses. Although research suggests the presence of CRS coagulopathy and the ensuing
complications there is limited data that actually quantifies this. Thus, the second aim of this
thesis is to highlight the incidence and outcome of coagulopathy in CRS and HIPEC patients
by way of a systematic review. The final chapter, and third aim, is a pilot study to investigate
the role of thromboelastography (TEG) in CRS and HIPEC patients.
REFERENCES
1. Ansari, N, Brown, K, McBride, K et al. (2019). Accelerating the learning curve in
cytoreductive surgery and hyperthermic intraperitoneal chemotherapy using an external mentor
model. ANZ J Surg 89, 1097–1101.
2. Hurdle, H, Bishop, G, Walker, A et al. (2017) Coagulation after cytoreductive surgery
and hyperthermic intraperitoneal chemotherapy: a retrospective cohort analysis, Can J Anesth,
64:1144–1152, DOI 10.1007/s12630-017-0952-7.
3. Meigs, JV (1934). Tumors of the female pelvic organs. New York: The Macmillan
Company.

Coagulopathy in cytoreductive surgery patients
9
4. Munnell, EW (1969). Surgical treatment of ovarian carcinoma. Clin Obstet
Gynecol;12:980-92.
5. Cooksley, T and Haji-Michael, P (2011). Post-operative critical care management of
patients, undergoing cytoreductive surgery and, heated intraperitoneal chemotherapy (HIPEC),
World Journal of Surgical Oncology, 9:169, http://www.wjso.com/content/9/1/169. Accessed
on 15/4/20.
6. Neuwirth, M, Alexander, R, Karakousis, G (2016). Then and now: cytoreductive
surgery with hyperthermic intraperitoneal chemotherapy (HIPEC), a historical perspective, J
Gastrointest Oncol, 7(1):18-28.
7. Weisberger AS, Levine B, Storaasli JP (1955). Use of nitrogen mustard in treatment of
serous effusions of neoplastic origin. JAMA, 159(18):1704–7.
8. Pretorius, RG, Petrilli, ES, Kean, CK, (1981). Comparison of the iv and ip routes of
administration of cisplatin in dogs. Cancer Treat Rep, 65:1055-62.
9. Jaaback K, Johnson N, Lawrie TA (2016). Intraperitoneal chemotherapy for the initial
management of primary epithelial ovarian cancer. Cochrane Database of Systematic Reviews,
Issue 1. Art. No.: CD005340. DOI:10.1002/14651858.CD005340.pub4.
10. Spratt, JS, Adcock, RA, Sherrill, W (1980). Hyperthermic peritoneal perfusion system
in canines. Cancer Res, 40: 253-5.
Coagulopathy in cytoreductive surgery patients
10
11. Sugarbaker, PH (1995). Peritonectomy procedures. Ann Surg, 221: 29-42.
12. Sugarbaker, PH, Yu W, Yonemura Y (2003). Gastrectomy, peritonectomy, and
perioperative intraperitoneal chemotherapy: The evolution of treatment strategies for advanced
gastric cancer. Semin Surg Oncol, 21:233-48.
13. Jacquet, P, Sugarbaker, PH (1996). Clinical research methodologies in diagnosis and
staging of patients with peritoneal carcinomatosis. Cancer Treat Res, 82:359-74.
14. Hallam, S, Tyler, R, Price, M et al. (2019). Meta-analysis of prognostic factors for
patients with colorectal peritoneal metastasis undergoing cytoreductive surgery and heated
intraperitoneal chemotherapy, BJS Open, DOI: 10.1002/bjs5.50179.
15. Glehen, O, Gilly, FN (2003). Quantitative prognostic indicators of peritoneal surface
malignancy: carcinomatosis, sarcomatosis, and peritoneal mesothelioma. Surg Oncol Clin N
Am, 12: 649-71.
16. Bell, J, Rylah, B, Chambers, R et al. (2012). Perioperative Management of Patients
Undergoing Cytoreductive Surgery Combined with Heated Intraperitoneal Chemotherapy for
Peritoneal Surface Malignancy: A Multi-Institutional Experience, Ann Surg Oncol, 19: 4244–
425 1 DOI 10.1245 /s10434-012-2496-y.
17. Gupta, N, Kumar, V, Garg, R et al. (2019). Anesthetic implications in hyperthermic
intraperitoneal chemotherapy, Journal of Anaesthesiology Clinical Pharmacology, 35; 3-11.
Coagulopathy in cytoreductive surgery patients
11
18. Moran B, Baratti D, Yan TD et al. (2008). Consensus statement on the loco-regional
treatment of appendiceal mucinous neoplasms with peritoneal dissemination (pseudomyxoma
peritonei). J Surg Oncol, 98:277– 82.
19. Saxena, A, Yan, T, Chua, C et al. (2009). Risk Factors for Massive Blood Transfusion
in Cytoreductive Surgery: A Multivariate Analysis of 243 Procedures. Ann Surg Oncol, 16:
2195–2203. DOI 10.1245/s10434-009-0484-7.
20. Raspé, C, Flöther, L, Schneider, R et al. (2016). Best practice for perioperative
management of patients with cytoreductive surgery and HIPEC, European Journal of Surgical
Oncology, 43: 1013-1027. DOI.org/10.1016/j.ejso.2016.09.008.
21. Owusu-Agyemang, P, Soliz, J, Hayes-Jordan, A et al. (2014). Safety of Epidural
Analgesia in the Perioperative Care of Patients Undergoing Cytoreductive Surgery with
Hyperthermic Intraperitoneal Chemotherapy, Ann Surg Oncol, 21:1487–1493. DOI
10.1245/s10434-013-3221-1.
22. Korakianitis, O, Daskalou, T, Alevizos, L et al. (2015). Lack of significant
intraoperative coagulopathy in patients undergoing cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy (HIPEC) indicates that epidural anaesthesia is a safe option. Int
J Hyperthermia, 31(8): 857–862.
23. Gonzalez, E, Moore, E, Moore, H (2017). Management of Trauma-Induced
Coagulopathy with Thrombelastography. Crit Care Clin, 33: 119-34.
Coagulopathy in cytoreductive surgery patients
12
24. Thomas, D, Wee, M, Clyburn, P et al. (2010). GUIDELINES. Blood transfusion and
the anaesthetist: management of massive haemorrhage. Association of Anaesthetists of Great
Britain and Ireland. Anaesthesia, 65: 1153-61.
25. Wikkelsø, A, Wetterslev, J, Møller, A et al. (2016). Thromboelastography (TEG) or
thromboelastometry (ROTEM) to monitor haemostatic treatment versus usual care in adults or
children with bleeding. Cochrane Database of Systematic Reviews, Issue 8. Art. No.:
CD007871. DOI: 10.1002/14651858.CD007871.pub3.
Coagulopathy in cytoreductive surgery patients
13
CHAPTER 1
Point of care viscoelastic assay devices (rotational thromboelastometry and
thromboelastography); a primer for surgeons.
Authors:
Gary Sharpa MBBS, BSc (Hons)
A/Prof. Christopher J. Younga,b MBBS, MS, FRACS, FACS, FASCRS
Institutions:
a Department of Colorectal Surgery, Royal Prince Alfred Hospital, Sydney, Australia.
b The University of Sydney, Discipline of Surgery, Sydney, New South Wales, Australia.
Citation
Sharp, G, Young, C (2018). Point‐of‐care viscoelastic assay devices (rotational
thromboelastometry and thromboelastography): a primer for surgeons, ANZ Journal of
Surgery, 89: 291-295.
Coagulopathy in cytoreductive surgery patients
14
Abstract
Introduction
Bleeding is a common occurrence in surgery. Point of care testing with viscoelastic assays such
as TEG and ROTEM has become more common place. TEG and ROTEM have the
potential to guide management of coagulopathy. Many health care professionals still rely upon
standard laboratory tests to manage a bleeding patient. We aimed to investigate the literature
surrounding management of the surgically bleeding patient via viscoelastic assays.
Methods
Literature review of Embase, Medline, Pubmed and the Cochrane library using “TEG,
ROTEM, surgery” search terms.
Results
Via the literature search and reference lists reviewed by both authors, a total of 62 articles have
been evaluated, 35 of these have been included in this review.
Discussion
Viscoelastic assays are used most commonly during orthotopic liver transplantation, trauma,
post-partum haemorrhage and cardiac surgery. Although the evidence is not overwhelming, we
have identified recurrent themes where viscoelastic assays seem to be beneficial. Viscoelastic
assay use, especially when incorporated into an algorithm, appears to reduce blood product
administration which in turn reduces costs and potential adverse events. They are quicker than
standard laboratory tests and they can detect hyperfibrinolysis, the hallmark of coagulopathy,
via in vivo clot analyses which standard laboratory tests are unable to do. Ultimately more
randomised controlled trials are required.
Coagulopathy in cytoreductive surgery patients
15
Point of care viscoelastic assay devices (rotational thromboelastometry and
thromboelastography): a primer for surgeons
Introduction
Haemorrhagic shock accounts for 80% of intraoperative deaths(1). Greater knowledge of
coagulopathy and the potential gains from point of care (POC) testing using viscoelastic (VE)
assays such as rotational thromboelastometry (ROTEM) and thromboelastography (TEG)
may benefit our patients. These two VE assays are very similar and have been evaluated as a
single entity in many reviews(2). Perioperative analysis of coagulation and haemoglobin is
paramount in managing pathological states arising from haemorrhage. Patient assessment starts
long before entering the operating room (OR) via preoperative assessment to identify bleeding
risk(3). Intraoperative monitoring includes diligently recording blood loss, organ perfusion,
haemoglobin concentration, unwanted effects of blood product transfusion and
coagulopathy(3).
Standard laboratory tests (SLT’s) such as INR/PT and aPTT were originally used to diagnose
bleeding disorders and subsequently used to evaluate anticoagulants(1). The end-point of these
tests is the first detectable fibrin level(4) which equates to approximately the first 20-60
seconds of clot formation(5). APTT measures the intrinsic pathway, PT measures the extrinsic
pathway, while INR is a ratio of PT and a “normal” mean PT, it also measures the extrinsic
pathway(2, 6). SLT’s are used routinely within general surgery despite being shown to poorly
correlate with bleeding risk(1, 4, 6). They are poor prognosticators for haemorrhage in the
critically unwell(5). Furthermore, they remain unsatisfactory in the evaluation of orthotopic
liver transplantation (OLT), post-partum haemorrhage (PPH) and trauma-induced
Coagulopathy in cytoreductive surgery patients
16
coagulopathy (TIC)(7). These time-consuming tests(7-9) lack real-time evaluation(7) with
values derived from plasma, not whole blood(8, 10). They also lack information concerning
platelet function, fibrin formation, fibrinolysis(8) and importantly hyperfibrinolysis(11).
Hyperfibrinolysis is the abnormal accelerated breakdown of clot which leads to further
haemorrhage and is seen in many coagulopathies(12). Many studies suggest SLT’s are
inadequate when used alone to guide haemorrhagic resuscitation(5) and management of
coagulopathy, which is present in many critically ill patients upon emergency department (ED)
presentation(6, 7). Recent evidence proposes the use of more robust VE assays such as TEG
and ROTEM(1, 3, 8, 11). VE assays are regarded as POC assays performed on whole blood
which assess clot formation and breakdown(7). They are also regularly utilised worldwide(13)
to guide allogenic blood product resuscitation(4) which is associated with significant costs,
morbidity and mortality(14). The ability of VE assays to rationalise blood product transfusion
subsequently lowers transfusion complications(8) and costs(14) especially in trauma, cardiac
and OLT surgery(15). Lastly, VE assays are quicker to perform than SLT’s and can guide
individual treatment of specific causes of coagulopathy(16).
Techniques of Viscoeleastic assessment of Coagulation
TEG, originally known as “Harterts Instrument”, was produced in 1948 by Hartert at
Heidelberg University School of Medicine(7). Used throughout Europe in the 1950’s to
identify anticoagulant effects, thrombocytopaenia and fibrinolysis, it was later utilised by Swan
et al in 1958 during cardiac surgery(4, 10). It’s use in research then commenced around
1990(10) and began in earnest with trauma patients and the evaluation of TIC(4). TEG is a
POC device that analyses clot production, growth and breakdown(17). It’s performed on whole
blood at the bedside allowing quicker evaluation of coagulation status(8). Once the TEG is
complete clinicians are supplied with a graphical representation and assay data regarding

Coagulopathy in cytoreductive surgery patients
17
coagulation(11) allowing rationalised blood product replacement(8, 11, 17). A rapid-TEG
assay will give results within 5-15 minutes(2) due to addition of tissue factor (TF) which
accelerates the clotting process(10). TEG works by placing whole blood into a plastic
cartridge which contains a cup and extending into the whole blood from above is a thin torsion
wire. The plastic cup then rotates at a set rate and degrees of motion(10). The viscoelastic
changes in clot property are registered via the torsion wire and an electromagnetic transducer
which in turn produces a physical trace(10) (Figure 4 and Table 1). As clot lysis occurs the
torsion wire is moved less allowing near real-time clot evaluation(21). Apart from rapid-TEG
all other TEG samples have the anticoagulant citrate within them(10) to ensure whole blood
is tested and not partially clotted/clotted blood(4).
ROTEM is a modified version of Harterts original thromboelastography(22). Whole citrated
blood is inserted into a cuvette and a sensor pin is partially submerged within the sample which
moves back and forth through an angle of 4.75°(22). Reagents are then added to assess specific
clotting pathways(2). Resistance is transmitted to an optical detector system and subsequently
recorded(2). The viscoelastic clot properties are then displayed providing information on
coagulation initiation, growth, strength and breakdown(22). Preliminary results are ready
within 5-10 minutes and the full report within 20 minutes(2). Six assays are routinely utilised:
INTEM, EXTEM, HEPTEM, FIBTEM, APTEM, Na-TEM(2) which isolate the origin of
numerous causes of haemorrhage(22). INTEM assesses clot formation and fibrinolysis via the
intrinsic pathway(23). EXTEM assesses the extrinsic pathway(23). FIBTEM measures the
function, not concentration, of fibrinogen(23).
Trauma
Coagulopathy in cytoreductive surgery patients
18
Worldwide, trauma accounts for approximately six million deaths per annum, with
uncontrolled haemorrhage comprising almost half(18). It is the leading cause of mortality and
morbidity in adults <36 years worldwide(2) and the second most common cause of death in
developed countries(5). Two-thirds of these deaths and 80% of blood product administration
will occur within six hours post-injury(24) from uncontrollable haemorrhage(25).
Haemorrhage, massive transfusion protocol (MTP) and coagulopathy are noted as the most
significant factors regarding outcome(22). Debate continues regarding the best transfusion
ratio, however a 1:1:1 ratio of RBC/FFP/Platelets has been suggested as most appropriate with
significant reductions in mortality due to rapid restoration of haemostasis(8, 11). Activation of
an MTP and subsequent administration of potentially large volumes of blood products is not
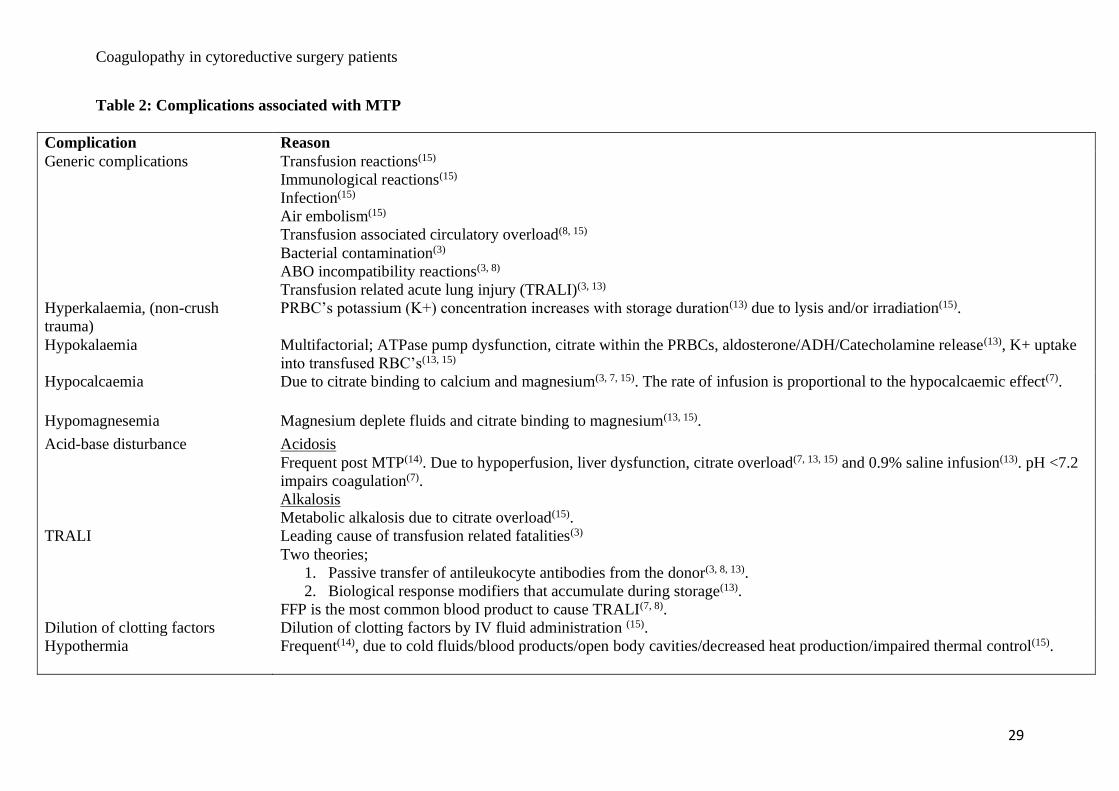
without complication (Table 2) and significant financial costs(18). MTP’s are of proven benefit
in haemorrhagic shock treatment(3, 5), but we must consider not only the blood products
required but other adjuncts to ensure maximal effect(11). Several factors are known to
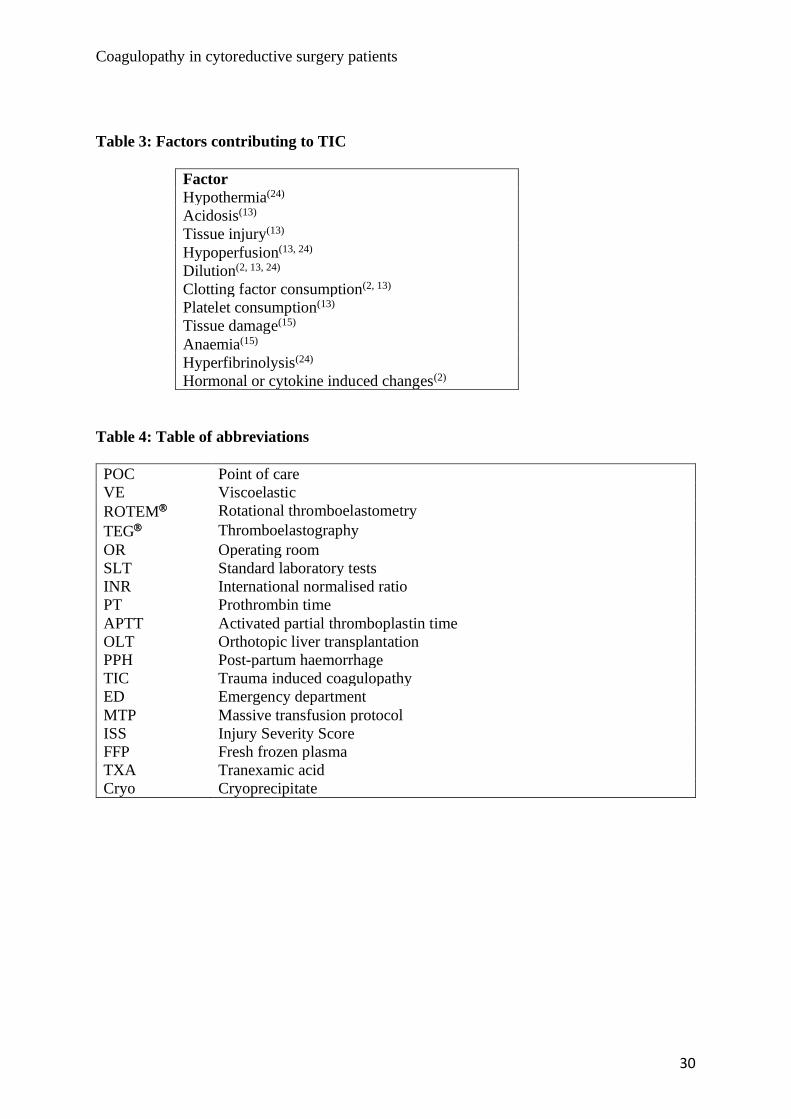
contribute to TIC (Table 3) however, the exact pathophysiology remains unclear(18). TIC is
present in up to 35% of severely injured patients on ED arrival(19). As Injury Severity Score
(ISS) rises, so does the incidence of coagulopathy, mortality(26) and morbidity(2). VE assay-
based MTP versus a generic MTP has been shown to; reduce mortality(19, 20): rationalise
blood product use(2, 10, 25); reduce ICU stay and ventilator days(25). Hyperfibrinolysis,
identified on VE, is an important component of TIC(4, 7) and correlates with trauma
severity(5), poorer outcome(4, 21) and TIC mortality(2, 10, 22). Fulminant hyperfibrinolysis
(complete clot fibrinolysis within <30 minutes) has a mortality of >85%(7).
Cardiac surgery
Perioperative haemorrhage regularly complicates cardiac surgery culminating in increased ICU
stay, morbidity and mortality(2, 16). The aetiology of cardiac surgery coagulopathy is
Coagulopathy in cytoreductive surgery patients
19
multifactorial but includes; heparin use during bypass, coagulation factor
consumption/dilution, platelet dysfunction, hypothermia and hyperfibrinolysis(1, 2, 9, 16). VE
assays are able to discriminate between a large majority of these and guide an individual
approach to haemorrhage management(16). The cause of coagulopathy aside, up to 8% of
cardiac surgical patients require a further procedure for haemorrhage(2) culminating in
cardiothoracic surgery using 5% of all donated blood in the UK(2) and 15-20% worldwide(16).
This consumption comes at vast financial expense and correlates with increased morbidity and
mortality(2, 16). Several studies have highlighted significant reductions in blood product
consumption when following a VE assay-related algorithm compared with SLT’s(2, 3, 9, 16).
As such VE was noted to be cost-saving when compared to SLT’s(2). These beneficial
outcomes have culminated in the National Institute for Health and Care Excellence (NICE)
recommending TEG use during cardiac surgery(13).
Post-partum haemorrhage
Pregnancy induces pronounced vicissitudes in haemostasis(27, 28) preparing the mother for
childbirth(12). PPH remains the greatest cause of obstetric morbidity and mortality
worldwide(27) with a rising incidence(23). In 2012 78,000 maternal deaths were directly
attributed to PPH worldwide(29) with an incidence of ~3.7/1000 births in the UK(2). It is a
common cause for MTP activation(11) with severe PPH leading to emergency hysterectomies,
a mortality rate of 0.6%, and prolonged ICU admissions(12, 23). The most common cause is
uterine atony but multiple aetiologies exist(30) such as dilutional coagulopathy, local and
disseminated coagulation factor consumption and/or hyperfibrinolysis(1, 12). Many PPH cases
remain idiopathic(12). PPH manifests abruptly and requires constant re-evaluation(29). SLT’s
are of poor prognostic value in PPH and may remain normal even in the face of severe blood
loss(12). Management requires identification of the underlying aetiology without delay(27)
Coagulopathy in cytoreductive surgery patients
20
which in turn positively influences maternal outcome(30). VE assays have been hypothesised
to assist in differentiating the cause of PPH and managing it(27). Fibrinogen decline manifests
rapidly and is prognostic of progression to severe PPH(12, 23, 30) thus, prompt correction is
imperative(23). Fibrinogen function can be measured via ROTEM FIBTEM assay(15, 23,
30). A VE assay-based algorithm incorporating FIBTEM testing and fibrinogen concentrate
supplementation was associated with less blood product use, less volume transfused and fewer
adverse outcomes(23).
Orthotopic liver transplant surgery
End-stage liver disease is now commonly treated with OLT(31). This intricate procedure
associated with considerable risk(32) and substantial haemorrhage(33) may require major
blood product replacement(31, 32). A great range of allogenic transfusion rates exists across
transplantation centres worldwide(33), regardless, blood product transfusion within this
population is linked with adverse postoperative outcomes(31, 32) and mortality(33). The
pathogenesis of coagulopathy and subsequent haemorrhage in OLT remains multifactorial(33).
It does however, include hyperfibrinolysis during the anhepatic phase and the patient’s inability
to clear tissue plasminogen activators(33). Several authors noted significant benefits of a VE
assay-based algorithm in OLT such as; reduced transfusion requirements(19, 21, 31, 32),
especially FFP(31), less MTP activation(32), fewer complications(19, 32), re-do surgeries(21,
32), shorter ICU stays, reduced treatment costs(19) and mortality(21). Of note MTP activation
and administration is associated with shorter survival and more renal dysfunction(32) which in
itself is an independent factor known to increase mortality in OLT pts(32).
Other attempted VE assay uses

Coagulopathy in cytoreductive surgery patients
21
• A ROTEM guided algorithm used to treat burns patients was found to reduce blood
product consumption(3).
• TEG guided enoxaparin dosing for thromboprophylaxis in trauma and surgical
patients showed no improvement in venous-thromboembolism rates(34).
• The European Society of Anaesthesiology recommended the use of VE for major
orthopaedic, neurosurgical and paediatric surgery(15).
• The diagnosis of coagulopathy in patients unable to respond verbally and potentially
taking platelet antagonists(17).
• TEG guided haemostatic normalisation in catastrophically injured patients resulted
in fifteen organs being donated from two donors(17).
• Lastly, a study has highlighted the advantageous use of VE assays in venomous snake
bite management(35).
VE assay limitations
A lack of cost-effectiveness when used less than 326 times per year/per device(2). VE assay
devices require quality control(9), regular calibration(13), are costly and not always
available(9). Clinicians must be trained in the correct use and interpretation(2, 12) making them
operator dependent, open to error(4, 13, 17) and inter-sampling inconsistencies(4, 12).
Ultimately there appears to be a lack of current evidence(13) especially regarding improvement
in morbidity or mortality(13) and a significant lack of RCT’s(12).
Conclusion
This literature review describes numerous benefits and limitations regarding VE assays.
Benefits tend to fall into one of the following categories: reduced blood product use(4, 13)
Coagulopathy in cytoreductive surgery patients
22
culminating in reduced costs(2, 13) and diminished exposure to allogenic products and their
associated morbidity and mortality(2). Over 30 million units of blood are transfused in the
United States annually and the rate is rising(6). Any reduction has the potential to reduce
morbidity and costs; in fact this has been noted in cardiac surgery, trauma, postpartum
haemorrhage and liver transplantation(13). Overall VE assays are quicker than SLT’s(2, 11).
VE assays detect hyperfibrinolysis(11), the hallmark of coagulopathy in many catastrophic
situations. VE assays have the ability to detect all facets of clot formation and breakdown(11);
SLT’s do not.
VE assays are also cost-effective when compared to SLT’s in the trauma population(2).
However, VE assays did not show any improvement to clinical outcome in trauma, cardiac
surgery or PPH(2) and several limitations are outlined. Ultimately more robust research is
necessary to identify VE assays’ true potential.
REFERENCES
1. Thomas D, Wee M, Clyburn P et al. (2010). GUIDELINES. Blood transfusion and the
anaesthetist: management of massive haemorrhage. Association of Anaesthetists of Great
Britain and Ireland. Anaesthesia. 65: 1153-61.
2. Whiting P, Westwood M, Ramos M et al. (2015). Viscoelastic point-of-care testing to
assist with the diagnosis, management and monitoring of haemostasis: a systematic review and
cost-effectiveness analysis. Health Technol Assess. 19; 1-228.

Coagulopathy in cytoreductive surgery patients
23
3. Apfelbaum J, Nuttall, G, Connis, R et al. (2015). Practice Guidelines for Perioperative
Blood Management. An Updated Report by the American Society of Anesthesiologists
Task Force on Perioperative Blood Management*. Anesthesiology. 122 (2): 241-75.
4. Gonzalez E, Moore, E, Moore, H (2017). Management of Trauma-Induced
Coagulopathy with Thrombelastography. Crit Care Clin. 33: 119-34.
5. Lier H, Bottiger B, Hinkelbein J et al. (2011) Coagulation management in multiple
trauma: a systematic review. Intensive Care Med. 37: 572-82.
6. Paterson, D (2014). Hemorrhage and Coagulopathy in the Critically Ill. Emerg Med
Clin Am 2014; 32: 797-810.
7. Frith, D, Davenport, R, Brohi, K (2012). Acute traumatic coagulopathy. Curr Opin
Anesthesiol. 25: 229-34.
8. Hayter, M, Pavenski, K, Baker, J (2012). Massive transfusion in the trauma patient:
Continuing Professional Development. Can J Anesth. 59: 1130-45.
9. Sniecinski, J (2011). Bleeding and management of coagulopathy. J Thorac
Cardiovascular Surg. 142: 662-7.
10. Hanke A, Horstmann H, Wilhelmi, M (2017). Point-of-care monitoring for the
management of trauma-induced bleeding. Curr Opin Anaesthesiol. 30 (2): 250-6.

Coagulopathy in cytoreductive surgery patients
24
11. Pham, H, Shaz, B (2013). Update on massive transfusion. British Journal of
Anaesthesia. 111(S1): i71-i82.
12. Solomon, C, Collis, R, Collins, P (2012). Haemostatic monitoring during postpartum
haemorrhage and implications for management. British Journal of Anaesthesia. 109(6): 851-
63.
13. Solomon, C, Asmis, L, Spahn, D (2016). Is viscoelastic coagulation monitoring with
ROTEM® or TEG® validated. Scandinavian Journal of Clinical and Laboratory Investigation.
76(6): 503-7.
14. Gorlinger, K, Fries, D, Dirkmann, D et al. (2012). Reduction of Fresh Frozen Plasma
Requirements by Perioperative Point-of-Care Coagulation Management with Early Calculated
Goal-Directed Therapy. Transfus Med Hemother. 39: 104-13.
15. Sibylle, A, Kozek-Langenecker, A (2013). Management of severe perioperative
bleeding. Guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol. 30:
270-382.
16. Gorlinger, K, Dirkmann, D, Hanke, A (2013). Potential value of transfusion protocols
in cardiac surgery. Curr Opin Anesthesiol. 26(2): 230-43.
17. Walsh, M, Thomas, S, Howard, J et al. (2011). Blood Component Therapy in Trauma
Guided with the Utilization of the Perfusionist and Thromboelastography. The Journal of Extra
Corporeal Technology. 43: 162-7.
Coagulopathy in cytoreductive surgery patients
25
18. Chin, T, Moore, E, Moore, H et al. (2014). A prinicpal component analysis of
postinjury viscoelastic assays: clotting factor depletion versus fibrinolysis. Surgery. 156(3):
570-7.
19. Spahn, D. (2014). TEG®- or ROTEM®-based individualized goal-directed coagulation
algorithms: don’t wait - act now! Critical Care. 18(637).
20. Einerson, P, Moore, E, Chapman, M et al. (2016). Rapid Thrombelastography
thresholds for goal-directed resuscitation of patients at risk of massive transfusion. J Trauma
Acute Care Surg. 82(1): 114-9.
21. Johansson, P, Sorensen, A, Larsen, C et al. (2013). Low hemorrhage-related mortality
in trauma patients in a level 1 trauma center employing transfusion packages and early
thromboelastography-directed hemostatic resuscitation with plasma and platelets. Transfusion.
53: 3088-99.
22. Schochl, H, Frietsch, T, Pavelka, M et al. (2009). Hyperfibrinolysis After Major
Trauma: Differential Diagnosis of Lysis Patterns and Prognostic Value of Thrombelastometry.
The Journal of Trauma, Injury, Infection, and Critical Care. 67(1): 125-31.
23. Mallaiah, S, Barclay, P, Harrod, I et al. (2015). Introduction of an algorithm for
ROTEM-guided fibrinogen concentrate administration in major obstetric haemorrhage.
Anaesthesia. 70: 166-75.

Coagulopathy in cytoreductive surgery patients
26
24. Chapman, M, Moore, E, Ramos, C et al. (2013). Fibrinolysis greater than 3% is the
critical value for initiation of antifibrinolytic therapy. J Trauma Acute Care Surg. 75(6): 961-
7.
25. Gonzalez, E, Moore, E, Moore, H et al. (2016). Goal-directed Hemostatic Resuscitation
of Trauma-induced Coagulopathy. Annals of Surgery. 263(6): 1051-9.
26. Brohi, K, Singh, J, Heron, M et al. (2003). Acute Traumatic Coagulopathy. The Journal
of TRAUMA Injury, Infection, and Critical Care. 54: 1127-30.
27. de Lange, N, Rheenen-Flach, L, Lance, M et al. (2014). Peri-partum reference ranges
for ROTEM thromboelastometry. British Journal of Anaesthesia. 112(5): 852-9.
28. Armstrong, A, Fernando, R, Ashpole, K et al. (2011). Assessment of coagulation in the
obstetric population using ROTEM thromboelastometry. International Journal of Obstetric
Anaesthesia. 20: 293-8.
29. Collins, P, Thachil, J, (2016). For the Subcommittees on Women’s Health Issues in
Thrombosis and Haemostasis and on Disseminated Intravascular Coagulation. Management of
coagulopathy associated with postpartum hemorrhage: guidance from the SSC of the ISTH. J
Thromb Haemost. 14: 205-10.
30. Huissoud, C, Carrabin, N, Audibert, F et al. (2009). Bedside assessment of fibrinogen
level in postpartum haemorrhage by thrombelastometry. BJOG. 116: 1097-102.
Coagulopathy in cytoreductive surgery patients
27
31. Wang, C, Shieh, J, Chang, K et al. (2010). Thrombolastography-guided transfusion
decreases intraoperative blood transfusion during Orthotopic Liver Transplantation:
Randomised Clinical Trial. Transplantation Proceedings. 42: 2590-3.
32. Leon-Justel, A, Noval-Padillo, J, Alvarez-Rios, A et al. (2015). Point-of-care
haemostasis monitoring during liver transplantation reduces transfusion requirements and
improves patient outcome. Clinica Chimica Acta. 446: 277-83.
33. Dalmau, A, Sabate, A, Aparicio, I (2009). Hemostasis and coagulation monitoring and
management during liver transplantation. Current Opinion in Organ Transplantation. 14: 286-
90.
34. Connelly, C, Van, P, Hart, K et al. (2016). Thrombelastography-Based Dosing fo
Enoxaparin for Thromboprophylaxis in Trauma and Surgical Patients. A Randomised Clinical
Trial. JAMA Surgery. 151(10) doi: 10.1001/jamasurg.2016.2069.
35. Nag, I, Datta, S, De, D et al. (2017). Role of thromboelastography in the management
of snake bite: A case report from India. Transfus Apher Sci. 56(2): 127-9.

Coagulopathy in cytoreductive surgery patients
28
Table 1: TEG variables, meaning and treatment of abnormalities
Variable Acronym ROTEM
comparison
Measures Correlates to Value Abnormality
treated with
Clinically
validated
Reaction time †R-time From beginning to clot and fibrin
formation. Reflects coagulation cascade
enzymatic activity(10,17)
Analagous to INR/PT &
APTT(4)
Minutes FFP(17)
Yes(10)
Activated clot time
(Rapid-TEG only)
†ACT CT (clotting
time)
Time taken for tissue factor to activate
clot formation(10, 18, 19)
Coagulation factor
activity and thrombin
generation(18)
Seconds FFP(20) Yes(10)
Angle Rate of clot strength increase and
formation(18, 19, 20)
Fibrinogen concentration
and function(18, 20)
Degrees Cryo(17) or
fibrinogen
concentrate(4)
Yes(10)
Maximum amplitude MA MCF
(maximal
clot
firmness)
Greatest clot strength(18, 19) the widest
width of the TEG(4). Due to function
and number of platelet-fibrin bonding(17)
Platelet count and
function and platelet-
fibrinogen interaction(18,
20)
mm
Platelets(17, 20)
Yes(10)
Lysis at 30 minutes LY 30 CL 30 Percentage of clot lysis at 30mins after
MA(10, 17, 18, 19, 20)
Fibrinolysis (18, 20)
30 minutes TXA(17, 20) Yes(10)
Coagulation Time k-time Occurs at the same time as angle. Angle
has superseded K-time(4)
† R-time and ACT measure the same haemostatic period (factor activation and thrombin)(4)
Coagulopathy in cytoreductive surgery patients
29
Table 2: Complications associated with MTP
Complication Reason
Generic complications Transfusion reactions(15)
Immunological reactions(15)
Infection(15)
Air embolism(15)
Transfusion associated circulatory overload(8, 15)
Bacterial contamination(3)
ABO incompatibility reactions(3, 8)
Transfusion related acute lung injury (TRALI)(3, 13)
Hyperkalaemia, (non-crush
trauma)
PRBC’s potassium (K+) concentration increases with storage duration(13) due to lysis and/or irradiation(15).
Hypokalaemia Multifactorial; ATPase pump dysfunction, citrate within the PRBCs, aldosterone/ADH/Catecholamine release(13), K+ uptake
into transfused RBC’s(13, 15)
Hypocalcaemia Due to citrate binding to calcium and magnesium(3, 7, 15). The rate of infusion is proportional to the hypocalcaemic effect(7).
Hypomagnesemia Magnesium deplete fluids and citrate binding to magnesium(13, 15).
Acid-base disturbance Acidosis
Frequent post MTP(14). Due to hypoperfusion, liver dysfunction, citrate overload(7, 13, 15) and 0.9% saline infusion(13). pH <7.2
impairs coagulation(7).
Alkalosis
Metabolic alkalosis due to citrate overload(15).
TRALI Leading cause of transfusion related fatalities(3)
Two theories;
1. Passive transfer of antileukocyte antibodies from the donor(3, 8, 13).
2. Biological response modifiers that accumulate during storage(13).
FFP is the most common blood product to cause TRALI(7, 8).
Dilution of clotting factors Dilution of clotting factors by IV fluid administration (15).
Hypothermia
Frequent(14), due to cold fluids/blood products/open body cavities/decreased heat production/impaired thermal control(15).
Coagulopathy in cytoreductive surgery patients
30
Table 3: Factors contributing to TIC
Factor
Hypothermia(24)
Acidosis(13)
Tissue injury(13)
Hypoperfusion(13, 24)
Dilution(2, 13, 24)
Clotting factor consumption(2, 13)
Platelet consumption(13)
Tissue damage(15)
Anaemia(15)
Hyperfibrinolysis(24)
Hormonal or cytokine induced changes(2)
Table 4: Table of abbreviations
POC Point of care
VE Viscoelastic
ROTEM Rotational thromboelastometry
TEG Thromboelastography
OR Operating room
SLT Standard laboratory tests
INR International normalised ratio
PT Prothrombin time
APTT Activated partial thromboplastin time
OLT Orthotopic liver transplantation
PPH Post-partum haemorrhage
TIC Trauma induced coagulopathy
ED Emergency department
MTP Massive transfusion protocol
ISS Injury Severity Score
FFP Fresh frozen plasma
TXA Tranexamic acid
Cryo Cryoprecipitate

Coagulopathy in cytoreductive surgery patients
31
CHAPTER 2
Title: Systematic review of coagulopathy in cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy patients.
Short title: Coagulopathy in cytoreductive surgery patients
Authors: Dr Gary Sharp1 BSc (Hons), MBBS (Hons)
Dr Daniel Steffens1,2 BPhty (Hons), PhD
A/Prof Christopher Young1,3,4 MBBS (Hons), MS, FRACS
Affiliations:
1. Surgical Outcomes Research Centre (SOuRCe), Royal Prince Alfred Hospital, Sydney,
Australia.
2. Faculty of Medicine and Health, The University of Sydney, Sydney, Australia.
3. Department of Colorectal Surgery, Royal Prince Alfred Hospital, Sydney, Australia.
4. RPA Institute of Academic Surgery, Royal Prince Alfred Hospital, Sydney, Australia.
Corresponding Author: Gary Sharp
Address: Surgical Outcomes Research Centre (SOuRCe), PO Box M157, Missenden Rd.
Camperdown. NSW. Australia.
Tel: + 61 2 9515 3200
Fax: + 61 2 9515 3200
No funding has been applied for or used during this research project.

Coagulopathy in cytoreductive surgery patients
32
Original systemic review article.
This is not based upon any previous communications.
Abstract
Introduction
Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC)
procedures are prone to several perioperative complications. Coagulopathy has been
recognised within this population for many years. The exact cause of CRS/HIPEC associated
coagulopathy is unknown as is the incidence and perioperative outcomes.
Methods
Systematic review of literature from database inception to April 2020 (Medline, PubMed,
Cochrane, Embase). Search terms used: Coag*, cytoreductive surgery OR cytoreductive
surgery, HIPEC OR Hyperthermic intraperitoneal chemotherapy OR Heated intraperitoneal
chemotherapy. Eligible studies included the investigation of: incidence/prevalence/reported
occurrence and outcome of coagulopathy in CRS and HIPEC patients. Descriptive analysis
was performed to provide summative figures of the included studies.
Results
Database search located 120 articles, 14 met inclusion criteria. No randomised controlled trials
or systematic reviews were identified. All research was published between 2008-2019 with a
total of 1493 patients. Thirteen articles reported the presence of deranged clotting through
varying tests and definitions; of these, three authors reported a return to the operating theatre
due to bleeding. No direct mortalities associated with abnormal bleeding were documented.
The cause of coagulation was classified as multifactorial.

Coagulopathy in cytoreductive surgery patients
33
Discussion
Coagulopathy incidence ranged from 4-80% but was inadequately documented within the
literature. No consensus exists within the reviewed literature on the definition of coagulopathy
in CRS/HIPEC patients. The use of a standardised coagulopathy definition should be utilised.
From the 1493 patients reviewed 8 required reoperation for bleeding (0.5%). Eight studies
utilised epidural analgesia (N=786). Two studies reported delay in epidural removal due to
abnormal clotting and platelet tests, all were subsequently removed without issue. No other
epidural complications were documented.
Conclusion
A large proportion of CRS/HIPEC patients have deranged clotting tests perioperatively,
however, this review has failed to find a significant level of morbidity attached.

Coagulopathy in cytoreductive surgery patients
34
Introduction
Cytoreductive surgery (CRS) is the surgical resection of macroscopic malignancy and can
involve several intrabdominal procedures (1). CRS has been shown to benefit those presenting
with pseudomyxoma peritonei (2) and selected peritoneal carcinomatosis (1,3).
Heated/hyperthermic intraperitoneal chemotherapy (HIPEC) is the continued turbulent
perfusion of a heated cytotoxic agent into the abdominal cavity, at a temperature of 41-43
degrees celsius (4-7). Hyperthermia results in greater drug uptake by malignant cells, protein
synthesis and mitosis arrest in malignant cells, induction of lysosomal enzymes and accelerates
malignant cell death (5). Contact of cytotoxic agents with the visceral surface ensures a high
concentration with low systemic absorption and elimination of microscopic disease (3,8).
HIPEC should be carried out immediately after CRS but prior to anastomoses formation (9)
and has visceral surface penetration up to 5mm (5). The heat and chemotherapy agents act
synergistically to eliminate malignancy (5). The chemotherapy agent and the time period for
HIPEC perfusion depend on tumour histology (10).
Although CRS and HIPEC has been proven beneficial in the population outlined above it has
also been associated with numerous perioperative physiological disturbances (4,11) and
complications (12). Perioperative coagulopathy is one such disturbance documented in many
studies (3,4,13-17). Coagulopathy has gained recognition as a cause of surgical mortality in
recent times. The impact of coagulopathy is most apparent in trauma (18). Coagulopathy must
be identified and treated in order to control intraoperative haemorrhage (15) and the potential
complications due to blood and blood product resuscitation such as transfusion reactions,
immunological reactions, circulatory overload(19,20) and transfusion-related acute lung injury
(TRALI)(21, 22) to name but a few. Haemorrhagic shock accounts for 80% of intraoperative
Coagulopathy in cytoreductive surgery patients
35
deaths(23). Perioperative analysis of coagulation and haemoglobin is paramount in managing
pathological states arising from haemorrhage. A high proportion of those few CRS and HIPEC
patients who return to the operating theatre (OT) do so due to haemostatic problems (3,14,24).
The cause of the coagulopathy in CRS and HIPEC is multifactorial (17). Suggested operative
causes include long operating times (6,8,13,25,26), large surface area of raw tissue exposed
post-resection (6,8,27), blood loss (5,6,8,15,24,25,26), protein loss (3,6,9), high fluid
exchanges and temperature fluctuations (3,5,6,8,13,15-17,27). Chemotherapy also affects
coagulation through side effects such as acidosis (17) and myelosuppression (9). Lastly,
malignancy malnutrition, with its associated protein loss, also contributes to coagulopathy (17).
All CRS patients are evaluated preoperatively for their suitability and robustness to undertake
such a procedure including a focussed evaluation of their bleeding risk(21). Intraoperative
monitoring includes diligently recording blood loss, organ perfusion, haemoglobin
concentration and coagulopathy(21).
The aim of this systematic review is twofold. Firstly, to investigate the incidence of
coagulopathy in patients undergoing abdominal CRS and HIPEC. Secondly, to investigate the
perioperative outcome of coagulopathy on this patient population.
Methods
Protocol
The protocol of this systematic review followed the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses Protocols (PRISMA-P) guidelines (28). This manuscript also
Coagulopathy in cytoreductive surgery patients
36
followed the PRISMA Statement (29). No institutional review board approval or consent was
required.
Search strategy
A sensitive literature search was conducted on MEDLINE, PubMed, Cochrane and Embase
databases from inception to April 2020. The search was limited to English language and
humans. The search terms used were Coag* (1), cytoreductive surgery OR cytoreductive
surgery (2), HIPEC OR Hyperthermic intraperitoneal chemotherapy OR Heated intraperitoneal
chemotherapy (3). These searches were then combined #1 AND #2 AND #3. References of
included articles and review articles were hand-searched to ensure the search was
comprehensive.
Study selection
Peer-reviewed articles investigating CRS, HIPEC and any reference to coagulation were
selected. Eligible studies should include the investigation on at least one of the following;
incidence/prevalence/reported occurrence and outcome of coagulopathy in CRS and HIPEC
patients. We excluded commentaries, editorials, abstracts, case reports, professional practice
reviews and articles that focussed on a device or system.
Data extraction and critical appraisal
A data extraction sheet was used by two independent reviewers (GS, CY) to extract data from
studies. This data included: demographic details, country, methodology, neoplasm, peritoneal
carcinomatosis index (PCI), surgical time, HIPEC regime used, thoracic epidural insertion,
fluid regime, body temperature, venous thromboembolism (VTE) protocol, length of stay,
mortality, definition of transfusion triggers, transfused volumes intraoperatively, coagulation

Coagulopathy in cytoreductive surgery patients
37
tests used, incidence of coagulopathy and the outcome of coagulopathy. Disagreements within
the data extraction was resolved between the review authors.
Statistical analysis
Descriptive analysis was performed to provide summative figures of the included studies. For
continuous data, range, median and mean have been reported.
Results
Study selection
Search of databases yielded: Embase 58, Medline 22, Pubmed 27, Cochrane 13. A total of 120
articles were found. Of these, 14 met the inclusion and exclusion criteria and were included in
the review (Figure 1).
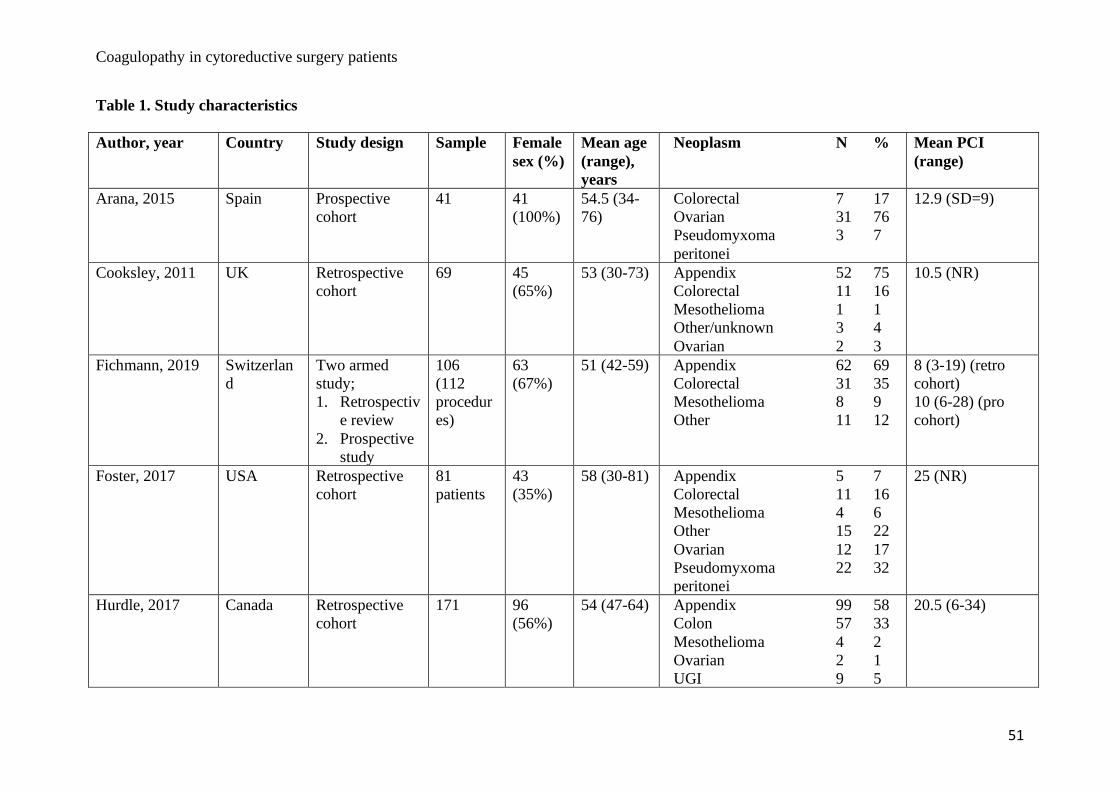
Study characteristics
There were no randomised controlled trials or systematic reviews identified. Of the 14 articles
included, 5 were prospective cohort studies and 8 were retrospective cohort studies and one
had mixed retrospective and prospective groups. The majority of the studies were undertaken
in European institutions (n=6), with the remaining undertaken in USA (n=3), England (n=2),
Australia (n=1), Canada (n=1) and Singapore (n=1). All the included research was published
between 2008-2019 (Table 1).
Patient Characteristics
A total of 1493 patients from the 14 studies were included in the review. Gender was reported
in 12 (86%) studies and female patients accounted for 62% (n=865). Age ranged from 14 to 81
years with an overall mean of 54.3 years (Table 1).

Coagulopathy in cytoreductive surgery patients
38
Malignancy type, PCI and operating time
Eleven studies (79%) reported malignancy type treated in 1213 patients. In descending order
these were; appendiceal 397 (33%), colorectal 246 (20%), pseudomyxoma peritonei 219
(18%), mesothelioma 118 (10%), ovarian 115 (9%), other/unknown 62 (5%), upper
gastrointestinal (UGI) 19 (2%), desmoplastic 17 (1%), “primary peritoneal” 8 (0.7%),
pancreatic 6 (0.5%), sarcoma 4 (0.3%), uterine 2 (0.2%). PCI was recorded in 10 studies (71%)
with the mean ranging from 8-25. Operating time was recorded in 12 studies (86%), the mean
operating time in these was 485.3 minutes (Table 1).
HIPEC, Thoracic epidural use and body temperature
Eleven studies (79%) reported HIPEC agent administered. Mitomycin was the most commonly
employed. Four studies (29%) focussed solely on the use of epidural catheters in CRS/HIPEC
patients (12,15,16, 27). However, epidural analgesia was used in 8 studies (57%), although two
reported only a percentage of their sample receiving such pain management 72% and 61%
respectively (8,27). Body temperature, a core component of coagulation, was poorly
documented with only 3 studies (21%) supplying data (Table 2).
VTE prophylaxis
Two studies (14%) used heparin for venous-thromboembolism (VTE) prophylaxis (3,26), 3
(21%) used low molecular weight heparin (LMWH) (4,7,11), 1 (14%) utilised both LMWH
and heparin (13), 1 used Dextran (24) and 1 prescribed Dalteparin (27). The remainder (43%)
did not document their VTE guidelines.
30-day Mortality and length of stay
Coagulopathy in cytoreductive surgery patients
39
From the total of 1493 patients 8 (0.6%) 30-day mortalities were recorded in 3 studies and
ranged from 0.5%-2.3% (7,16,26). Length of stay ranged from 7-188 days (Table 2).
Blood product transfusion triggers
Six authors (43%) reported packed red blood cell (PRBC) transfusion triggers. There was a
mix of clinical signs and biochemical measurements employed to guide transfusion, with
haemoglobin (Hb) of <80g/dL most commonly utilised (3,7,11,12,26). Korakianitis (2015)(15)
transfused with a Hb <90g/dL. Signs of anaemia that triggered PRBC transfusion were; sinus
tachycardia, SBP <100 mmHg, urine output (UO) <30 ml/h (26). Indication for fresh frozen
plasma (FFP) was documented in two studies (14%) both of whom used INR, not a viscoelastic
assay to define the need for transfusion (11,12). The FFP administration triggers were INR
>1.2 (11) and INR >1.5 (12). Two authors reported the trigger for platelet (PLT) administration
which was platelets <50 x109 L-1 (12,25) (Table 3).
Blood product replacement
Eleven studies (79%) reported intraoperative blood product replacement, the net sample of
these studies was 996. The number of patients who received intraoperative replacements were;
PRBC 489 (49%), PLT 37 (4%), FFP 103 (10%), cryoprecipitate 5 (0.5%), transexamic acid
(TXA) 134 (13%). Postoperative blood product replacements were reported in 4 studies (28%)
with a net sample of 308 (3,4,1,13). The number of patients who received blood product
replacement was as follows; PRBC 93 (30%), PLT 7 (2%), FFP 24 (8%), cryoprecipitate 3
(1%), no documented TXA administration. Only 1 study (8) used an irradiated cell saver.
Lastly, 1 study reported the intraoperative use of fibrinogen and specific factor products (30)
(Table 3).

Coagulopathy in cytoreductive surgery patients
40
Coagulopathy
One study focused on VTE (24) and so was removed from this sub-analysis. The remaining 13
articles reported the presence of deranged clotting within the CRS/HIPEC population. The
diagnostic test used to define coagulopathy differed between studies. Clotting studies: defined
here as international normalised ratio (INR), activated partial thromboplastin time (aPTT) and
prothrombin time (PT), were used in 8 studies (67%) (4,7,8,12,13,15,16,25,26). Rotational
thromboelastometry (ROTEM) was used in 3 studies (25%) (3,11,30) and
thromboelastography (TEG) utilised in 1 study (8%) (27). Whilst nearly all the studies
reported deranged clotting only 4 (29%) reported the incidence of coagulopathy (7,13,26,27).
Hurdle et al. (2017) (13) used clotting studies to define coagulopathy, results showed that 65
patients (38%) suffered “coagulopathy” whilst “severe coagulopathy” was encountered in 8
(4.7%). Saxena et al. (2009) (26) used clotting studies to show that 28 (12%) had impaired
coagulation. Thong et al (2017) (7) too utilised clotting studies to define coagulopathy, their
results showed that N=80 (80%) of their sample had abnormal clotting studies. Teoh et al
(2019) (27) utilised TEG to define coagulopathy in 4 (14%) between the second and fifth
postoperative days. The aforementioned 4 authors reported the following coagulation related
complications: Hurdle et al (2017) (13) recorded 3 patients required return to the operating
theatre for “bleeding complications”, no specifics given; Saxena et al. (2009) (26) reported no
complications: Thong et al (2017) (7) reported 4 postoperative bleeds requiring reoperation
between postoperative day (POD) 1 and 39, Teoh et al. (2019) reported no coagulation
associated complications. Only 1 of the remaining 9 studies reported the need for reoperation
due to bleeding (11), whilst another quoted delayed removal of 2 epidurals due to deranged
clotting (16). Nine studies (69%) reported no coagulation associated complications
(3,4,8,12,15,25-27,30). Those studies which reported the cause of coagulopathy suggested it
was multifactorial (3,4,7,8,11,13,15,16,25,26,27).

Coagulopathy in cytoreductive surgery patients
41
Discussion
The first aim of this systematic review was to investigate the incidence of coagulopathy in
patients undergoing abdominal CRS and HIPEC. As outlined above, coagulopathy incidence
ranged from 4-80% (7,13,26,27). However, the incidence of coagulopathy is poorly
documented within the literature. Most studies instead give mean values for the sample as a
whole which makes it impossible to extrapolate information regarding specific affected
individuals. The literature also has no consensus on the definition of coagulopathy. In the four
studies (7,13,26,27) that reported coagulopathy incidence each used differing definitions or
indeed did not define the definition of coagulopathy at all (7). Hurdle et al. (2017) (13) defined
coagulopathy as an abnormality of platelet count <100 x109/L, INR 1.5, or PTT 45 sec and
“severe coagulopathy” as a platelet count <50 x109/L, INR>2.0, or PTT>60 sec. Saxena et al.
(2009) (26) defined coagulopathy as an INR 1.2. Teoh et al. (2019) (27) used both clotting
studies and TEG to define coagulopathy; abnormal coagulation was defined by any one of:
platelet count <100 x109/L, INR 1.5, PTT 45. Manufacturer reference values were used as
control values for TEG parameters. Thong et al (2017) (7) gave no normal parameters, but
stated that “80% of patients had elevated PT or/and aPTT”. It is our suggestion that a
standardised coagulopathy definition be used and to categorise results; these two simple
strategies would allow the reader to evaluate the true coagulopathy incidence.
The second aim was to highlight the outcome of coagulopathy on this patient population.
Hurdle et al’s. (2017) (13) research had a cumulative number of 73 patients defined as
coagulopathic or severely coagulopathic. Three returned to the OT for “bleeding
complications”. Unfortunately, there was no further information regarding what day the
patients returned to the OT, the procedure they required or their coagulation profile prior to

Coagulopathy in cytoreductive surgery patients
42
theatre return. It would therefore be unwise if we presumed they were coagulopathic at this
point and the return to OT was due to coagulopathy. Despite such a high rate of clotting
derangement the authors interestingly reported no significant changes to PTT values.
Saxena et al. (2009) (26), explain that there were complications in 108 (44%) and 40 (16%)
returned to OT, coupled with 5 (2%) deaths within 30 days. However, no further breakdown
of this information was given so it is not possible to ascertain if these are due to postoperative
coagulopathy or another issue.
Thong et al. (2017) (7) reported 3 patients requiring a return to OT for bleeding complications.
These included postoperative day (POD) 1 diaphragmatic and pancreatic bleed requiring
laparotomy. POD 2 bleeding from a non-defined source necessitating laparotomy. POD 26
“massive” per rectal bleed requiring medical intervention and a POD 39 jejunal bleed requiring
surgical resection. Unfortunately, once again there are no individual clotting assays for these
patients and as such we are unaware of their coagulation profile at the point of bleeding and
return to OT. Regardless, evidence suggests that the coagulopathy recognised post CRS/HIPEC
peaks between 24 and 72 hours post procedure (4,13) and then returns to normal at around
POD 3 (12). If this evidence is correct then perhaps the bleeding events at POD 1 and 2 could
be attributed to postoperative coagulopathy but the POD 26 and 39 episodes of bleeding cannot.
These bleeding events and others might be iatrogenic due to VTE prophylaxis or potentially a
separate second pathological cause. Lastly, Van Poucke et al. (2018) (11) reported that 2
patients required reoperation to treat bleeding complications within the study period; no further
information was given.

Coagulopathy in cytoreductive surgery patients
43
From the entire sample included in this systematic review (n=1493) we were able to find 8
patients who required reoperation for bleeding, this equates to 0.5%. This low figure of
reoperation seems to be contrary to other authors who have suggested that return to OT
secondary to bleeding is common in this population (3,14,24).
There is great interest in the use and potential complications of epidurals in CRS patients. There
is a high level of concern expressed within the literature regarding epidural complications,
especially epidural haematomas, due to CRS/HIPEC coagulopathy. Within this review, we
included 8 studies (57%) that employed thoracic epidural analgesia (4,8,12,13,15,16,27,30).
The total sample of individuals within the literature having an epidural was 786. Complications
regarding epidurals were noted in 2 studies. Owusu-Agyemang et al. (2014) (16) reported 2
patients had a delay in epidural removal requiring platelets due to thrombocytopaenia. The
epidurals were subsequently removed without issue. Hurdle et al. (2017) (13) also noted a
delay in epidural removal due to abnormal clotting and required blood products. All epidurals
were eventually removed successfully without complication. No epidural haematomas were
documented in any study. As such the epidural complication rate in the study sample was 0.4%.
Interestingly, in one study 5 epidurals were accidentally traumatically removed in patients all
of whom had an INR >1.5 (12). No complications arose in any of these patients.
A large percentage (79%) of the studies reviewed transfused blood and blood products, whilst
TXA use is becoming more common use. However, only 4 studies used a viscoelastic assay,
either ROTEM (3) (3,11,30) and TEG (1) (27) to aid in their transfusion validation. With
such a large proportion of the studies administering blood products one could argue that the
use of viscoelastic assays may have assisted to manage appropriate administration.
Coagulopathy in cytoreductive surgery patients
44
Conclusion
Numerous articles exist regarding the potential complications perioperatively due to
coagulopathy in the CRS/HIPEC population. In this systematic review we have found no
evidence to suggest that there is a significantly high rate of bleeding complications. Thoracic
epidural use was also not associated with an increase in complications. The use of non-
standardised definitions of “coagulopathy” needs to be addressed. The use of more specific
viscoelastic assays may assist in defining coagulopathy.
REFERENCE LIST
1. Ansari, N, Brown, K, McBride, K et al. (2019). Accelerating the learning curve in
cytoreductive surgery and hyperthermic intraperitoneal chemotherapy using an external
mentor model. ANZ J Surg, 89: 1097–1101.
2. Moran B, Baratti D, Yan TD et al. (2008). Consensus statement on the loco-regional
treatment of appendiceal mucinous neoplasms with peritoneal dissemination
(pseudomyxoma peritonei). J Surg Oncol, 98: 277– 82.
3. Arana, L, Fuentes-Garcıa, D, Calvo, M et al. (2015). Alterations in Hemostasis during
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in Patients with
Peritoneal Carcinomatosis, CIR ESP, 93(8): 496-501.
4. Cooksley, T and Haji-Michael, P (2011). Post-operative critical care management of
patients undergoing cytoreductive surgery and heated intraperitoneal chemotherapy
(HIPEC). World Journal of Surgical Oncology, 9:169,
http://www.wjso.com/content/9/1/169. Accessed 15/4/20.
Coagulopathy in cytoreductive surgery patients
45
5. Gupta, N, Kumar, V, Garg, R et al. (2019). Anesthetic implications in hyperthermic
intraperitoneal chemotherapy, Journal of Anaesthesiology Clinical Pharmacology, 35; 1,
3-11.
6. Raspe, C, Piso, P, Wiesenack, C et al. (2012). Anesthetic management in patients
undergoing hyperthermic chemotherapy, Curr Opin Anesthesiol, 25:348–355.
DOI:10.1097/ACO.0b013e32835347b2.
7. Thong, S, Chia, C, Ng, O et al. (2017). A review of 111 anaesthetic patients undergoing
cytoreductive surgery and hyperthermic intraperitoneal chemotherapy, Singapore Med J
2017; 58(8): 488-496. doi: 10.11622/smedj.2016078.
8. Schmidt, C, Moritz, S, Rath, S et al. (2009). Perioperative Management of Patients With
Cytoreductive Surgery for Peritoneal Carcinomatosis, J. Surg. Oncol. 2009;100:297–301.
9. Raspé, C, Flöther, L, Schneider, R et al. (2016). Best practice for perioperative
management of patients with cytoreductive surgery and HIPEC, European Journal of
Surgical Oncology, 43,6,1013-1027.
10. Webb C, Weyker P, Moitra V et al. (2013). An overview of cytoreductive surgery and
hyperthermic intraperitoneal chemoperfusion for the anesthesiologist. Anesth Analg,
116(4):924–31.
Coagulopathy in cytoreductive surgery patients
46
11. Van Poucke, S, Huskens, D, Van der Speeten, K et al. (2018) Thrombin generation and
platelet activation in cytoreductive surgery combined with hyperthermic intraperitoneal
chemotherapy – A prospective cohort study. PLoS ONE 13(6): e0193657.
doi.org/10.1371/journal
12. Piccioni, F, Casiraghi, C, Fumagalli, L et al. (2015). Epidural analgesia for cytoreductive
surgery with peritonectomy and heated intraperitoneal chemotherapyInternational Journal
of Surgery 16 (2015) 99e106, http://dx.doi.org/10.1016/j.ijsu.2015.02.025.
13. Hurdle, H, Bishop, G, Walker, A et al. (2017). Coagulation after cytoreductive surgery
and hyperthermic intraperitoneal chemotherapy: a retrospective cohort analysis, Can J
Anesth, 64:1144–1152. doi 10.1007/s12630-017-0952-7.
14. Sugarbaker, P, Alderman, R, Edwards, G et al. (2006), “Prospective morbidity and
mortality assessment of cytoreductive surgery plus perioperative intraperitoneal
chemotherapy to treat peritoneal dissemination of appendiceal mucinous malignancy.
Ann Surg Oncol, 13, 535-44.
15. Korakianitis, O, Daskalou, T, Alevizos, L et al. (2015). Lack of significant intraoperative
coagulopathy in patients undergoing cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy (HIPEC) indicates that epidural anaesthesia is a safe option.
Int J Hyperthermia, 31(8): 857–862.
16. Owusu-Agyemang, P, Soliz, J, Hayes-Jordan, A et al. (2014). Safety of Epidural
Analgesia in the Perioperative Care of Patients Undergoing Cytoreductive Surgery with
Coagulopathy in cytoreductive surgery patients
47
Hyperthermic Intraperitoneal Chemotherapy, Ann Surg Oncol, 21:1487–1493. doi
10.1245/s10434-013-3221-1.
17. Sheshadri, D and Chakravarthy, M (2016). Anaesthetic Considerations in the
Perioperative Management of Cytoreductive Surgery and Hyperthermic Intraperitoneal
Chemotherapy, Indian J Surg Oncol, 7(2):236–243. doi 10.1007/s13193-016-0508-2.
18. Frith, D, Davenport, R, Brohi, K (2012). Acute traumatic coagulopathy. Curr Opin
Anesthesiol 25: 229-34.
19. Sibylle, A and Kozek-Langenecker, A (2013). Management of severe perioperative
bleeding. Guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol,
30: 270-382.
20. Hayter, M, Pavenski, K, Baker, J (2012). Massive transfusion in the trauma patient:
Continuing Professional Development. Can J Anesth. 59: 1130-45.
21. Apfelbaum, J, Nuttall, G, Connis, R et al. (2015). Practice Guidelines for Perioperative
Blood Management. An Updated Report by the American Society of Anesthesiologists
Task Force on Perioperative Blood Management*. Anesthesiology. 122 (2):241-75.
22. Solomon, C, Asmis, L, Spahn, D (2016). Is viscoelastic coagulation monitoring with
ROTEM or TEG validated. Scandinavian Journal of Clinical and Laboratory
Investigation. 76(6): 503-7.
Coagulopathy in cytoreductive surgery patients
48
23. Thomas, D, Wee, M, Clyburn, P et al. (2010). GUIDELINES. Blood transfusion and the
anaesthetist: management of massive haemorrhage. Association of Anaesthetists of Great
Britain and Ireland. Anaesthesia. 65: 1153-61.
24. Foster, J, Sleightholm, R, Watley, D et al. (2017). The efficacy of dextran-40 as a
venous thromboembolism prophylaxis strategy in cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy, The American Surgeon. 83,134-140.
25. Sargant, N, Roy, A, Simpson, S et al. (2016). A protocol for management of blood loss in
surgical treatment of peritoneal malignancy by cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy, Transfusion Medicine. 26, 118–12.
26. Saxena, A, Yan, T, Chua, T et al. (2009). Risk Factors for Massive Blood Transfusion in
Cytoreductive Surgery: A Multivariate Analysis of 243 Procedures, Ann Surg Oncol,
16:2195–2203. doi 10.1245/s10434-009-0484-7
27. Teoh, D, Hutton, M, Else, S et al. (2019). Epidural analgesia? A prospective analysis of
perioperative coagulation in cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy, The American Journal of Surgery, 217,887e892.
doi.org/10.1016/j.amjsurg.2019.01.034.
28. Shamseer L, Moher D, Clarke M et al. (2015), PRISMA-P Group. Preferred reporting items
for systematic review and meta-analysis protocols (PRISMA-P): elaboration and
explanation, BMJ, 2, 349. doi.org/10.1136/bmj.g7647
Coagulopathy in cytoreductive surgery patients
49
29. Moher D, Liberati A, Tetzlaff J et al. (2009). Preferred Reporting Items for Systematic
Reviews and Meta-Analyses: The PRISMA Statement. BMJ. 339:b2535, doi:
10.1136/bmj.b2535.
30. Fichmann, D, Roth, L, Raptis, D et al. (2019). Standard Operating Procedures for
Anesthesia Management in Cytoreductive Surgery and Hyperthermic Intraperitoneal
Chemotherapy Improve Patient Outcomes: A Patient Cohort Analysis, Ann Surg Oncol,
26:3652–3662, https://doi.org/10.1245/s10434-019-07644-w.

Coagulopathy in cytoreductive surgery patients
50
Figure 1. Flow diagram of study selection
Records identified through database searching
(n = 123)
Additional records identified through other sources
(n = 0)
Records after duplicates removed (n = 86)
Records screened (n = 86)
Records excluded and reasons; abstracts n = 30
Non CRS focussed n = 12 Non-English n = 9 case studies n = 4
letters n = 1 thoracic procedures n =1 chemotherapy trial n = 1
Full-text articles assessed for eligibility
(n = 29)
Full-text articles excluded, with reasons;
Professional practice reviews n = 7 Focussed on a device/system n=2
Animal study n = 1 Case report n = 1
Review of transexamic acid n= 1 Review of hemophagocytic
syndrome n = 1 Focused on colorectal metastatic
disease n = 1 Perioperative fluid review n = 1
Studies included in qualitative synthesis
(n = 14)
Coagulopathy in cytoreductive surgery patients
51
Table 1. Study characteristics
Author, year Country Study design Sample Female
sex (%)
Mean age
(range),
years
Neoplasm N %
Mean PCI
(range)
Arana, 2015 Spain Prospective
cohort
41
41
(100%)
54.5 (34-
76)
Colorectal 7 17
Ovarian 31 76
Pseudomyxoma
peritonei
3 7
12.9 (SD=9)
Cooksley, 2011 UK Retrospective
cohort
69
45
(65%)
53 (30-73)
Appendix 52 75
Colorectal 11 16
Mesothelioma 1 1
Other/unknown 3 4
Ovarian 2 3
10.5 (NR)
Fichmann, 2019 Switzerlan
d
Two armed
study;
1. Retrospectiv
e review
2. Prospective
study
106
(112
procedur
es)
63
(67%)
51 (42-59) Appendix 62 69
Colorectal 31 35
Mesothelioma 8 9
Other 11 12
8 (3-19) (retro
cohort)
10 (6-28) (pro
cohort)
Foster, 2017 USA Retrospective
cohort
81
patients
43
(35%)
58 (30-81)
Appendix 5 7
Colorectal 11 16
Mesothelioma 4 6
Other 15 22
Ovarian 12 17
Pseudomyxoma
peritonei
22 32
25 (NR)
Hurdle, 2017 Canada Retrospective
cohort
171
96
(56%)
54 (47-64)
Appendix 99 58
Colon 57 33
Mesothelioma 4 2
Ovarian 2 1
UGI 9 5
20.5 (6-34)
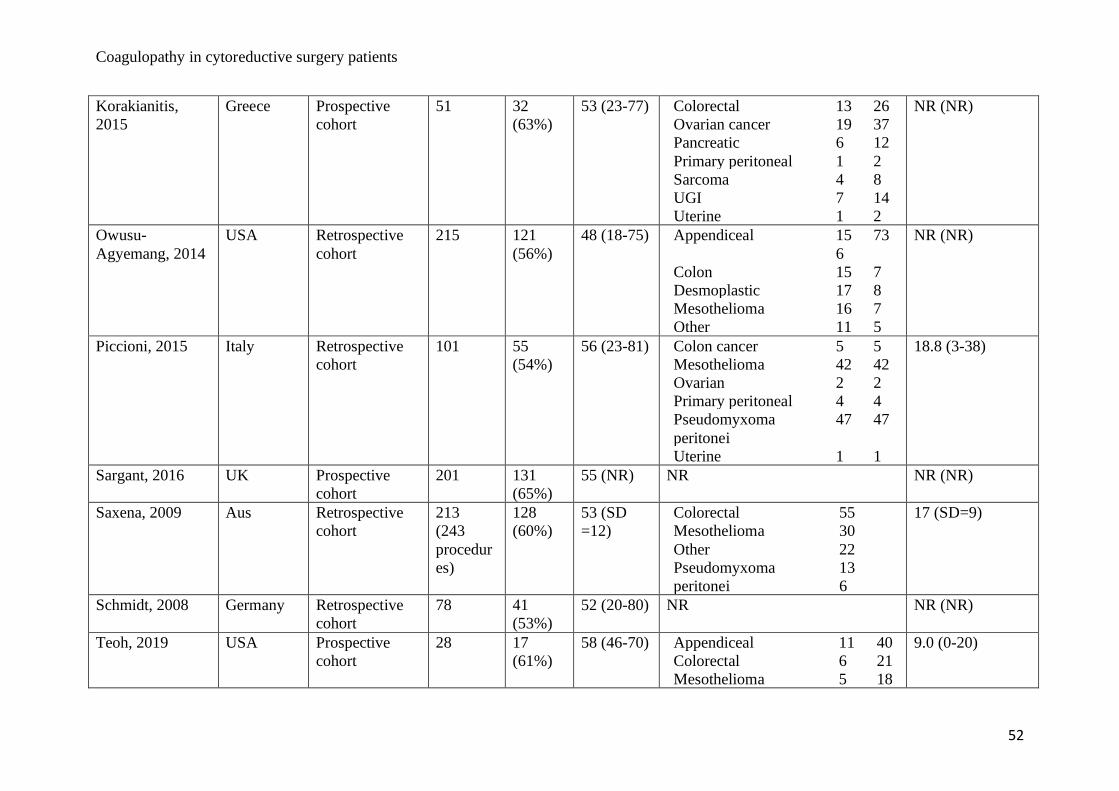
Coagulopathy in cytoreductive surgery patients
52
Korakianitis,
2015
Greece Prospective
cohort
51
32
(63%)
53 (23-77) Colorectal 13 26
Ovarian cancer 19 37
Pancreatic 6 12
Primary peritoneal 1 2
Sarcoma 4 8
UGI 7 14
Uterine 1 2
NR (NR)
Owusu-
Agyemang, 2014
USA Retrospective
cohort
215 121
(56%)
48 (18-75) Appendiceal 15
6
73
Colon 15 7
Desmoplastic 17 8
Mesothelioma 16 7
Other 11 5
NR (NR)
Piccioni, 2015 Italy Retrospective
cohort
101 55
(54%)
56 (23-81) Colon cancer 5 5
Mesothelioma 42 42
Ovarian 2 2
Primary peritoneal 4 4
Pseudomyxoma
peritonei
47 47
Uterine 1 1
18.8 (3-38)
Sargant, 2016 UK Prospective
cohort
201 131
(65%)
55 (NR) NR NR (NR)
Saxena, 2009 Aus Retrospective
cohort
213
(243
procedur
es)
128
(60%)
53 (SD
=12)
Colorectal 55
Mesothelioma 30
Other 22
Pseudomyxoma
peritonei
13
6
17 (SD=9)
Schmidt, 2008 Germany Retrospective
cohort
78 41
(53%)
52 (20-80) NR NR (NR)
Teoh, 2019 USA Prospective
cohort
28 17
(61%)
58 (46-70) Appendiceal 11 40
Colorectal 6 21
Mesothelioma 5 18
9.0 (0-20)
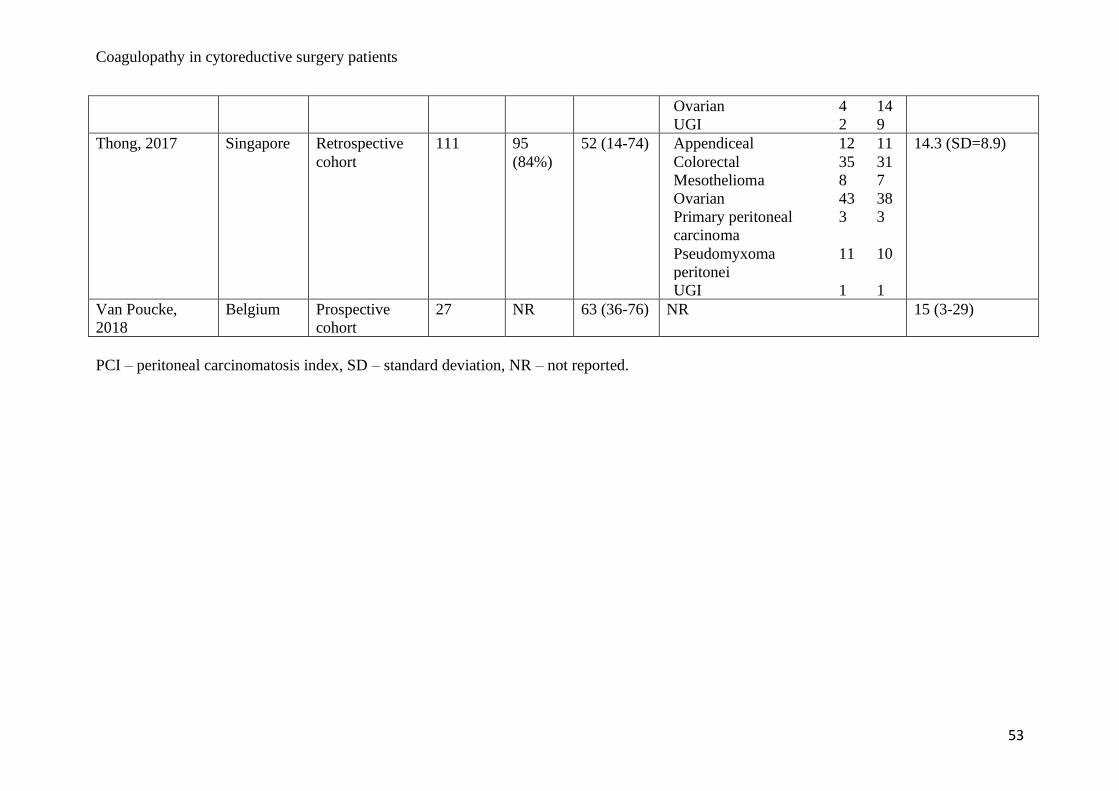
Coagulopathy in cytoreductive surgery patients
53
Ovarian 4 14
UGI 2 9
Thong, 2017 Singapore Retrospective
cohort
111 95
(84%)
52 (14-74) Appendiceal 12 11
Colorectal 35 31
Mesothelioma 8 7
Ovarian 43 38
Primary peritoneal
carcinoma
3 3
Pseudomyxoma
peritonei
11 10
UGI 1 1
14.3 (SD=8.9)
Van Poucke,
2018
Belgium Prospective
cohort
27 NR 63 (36-76) NR 15 (3-29)
PCI – peritoneal carcinomatosis index, SD – standard deviation, NR – not reported.
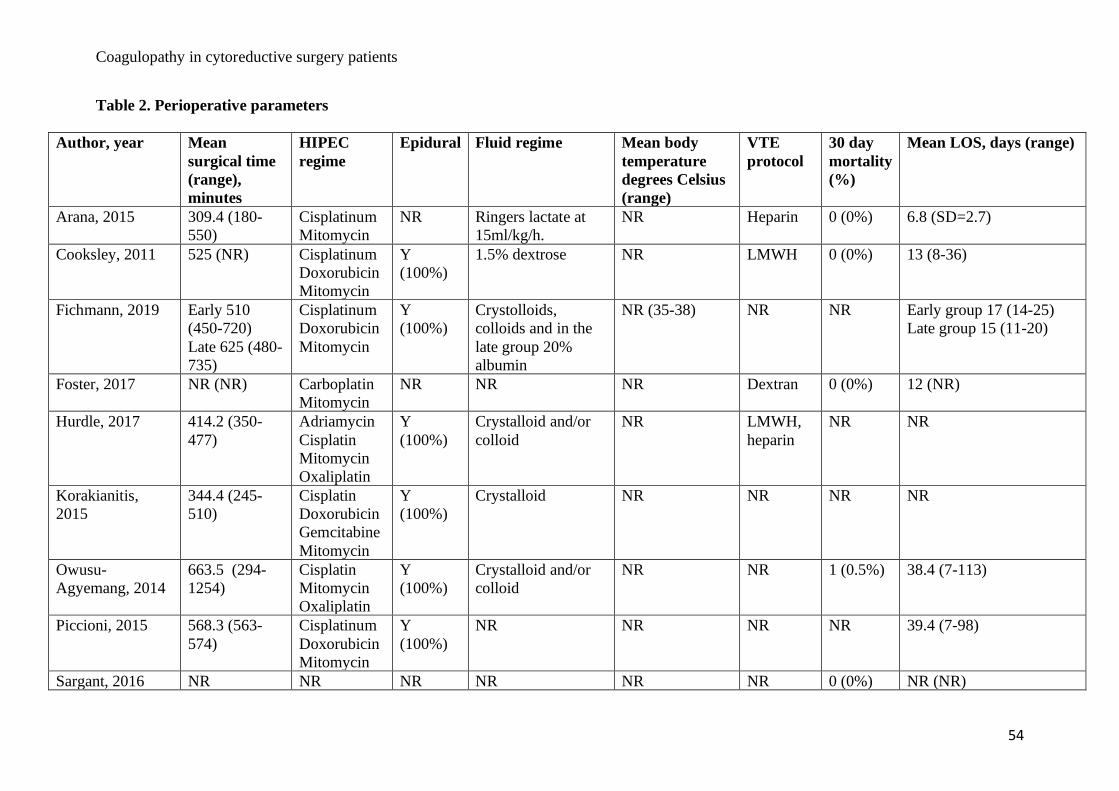
Coagulopathy in cytoreductive surgery patients
54
Table 2. Perioperative parameters
Author, year Mean
surgical time
(range),
minutes
HIPEC
regime
Epidural Fluid regime Mean body
temperature
degrees Celsius
(range)
VTE
protocol
30 day
mortality
(%)
Mean LOS, days (range)
Arana, 2015 309.4 (180-
550)
Cisplatinum
Mitomycin
NR Ringers lactate at
15ml/kg/h.
NR Heparin 0 (0%) 6.8 (SD=2.7)
Cooksley, 2011 525 (NR) Cisplatinum
Doxorubicin
Mitomycin
Y
(100%)
1.5% dextrose NR LMWH 0 (0%) 13 (8-36)
Fichmann, 2019 Early 510
(450-720)
Late 625 (480-
735)
Cisplatinum
Doxorubicin
Mitomycin
Y
(100%)
Crystolloids,
colloids and in the
late group 20%
albumin
NR (35-38) NR NR Early group 17 (14-25)
Late group 15 (11-20)
Foster, 2017 NR (NR) Carboplatin
Mitomycin
NR NR NR Dextran 0 (0%)
12 (NR)
Hurdle, 2017 414.2 (350-
477)
Adriamycin
Cisplatin
Mitomycin
Oxaliplatin
Y
(100%)
Crystalloid and/or
colloid
NR LMWH,
heparin
NR NR
Korakianitis,
2015
344.4 (245-
510)
Cisplatin
Doxorubicin
Gemcitabine
Mitomycin
Y
(100%)
Crystalloid NR NR NR NR
Owusu-
Agyemang, 2014
663.5 (294-
1254)
Cisplatin
Mitomycin
Oxaliplatin
Y
(100%)
Crystalloid and/or
colloid
NR NR 1 (0.5%) 38.4 (7-113)
Piccioni, 2015 568.3 (563-
574)
Cisplatinum
Doxorubicin
Mitomycin
Y
(100%)
NR NR NR NR 39.4 (7-98)
Sargant, 2016 NR NR NR NR NR NR 0 (0%) NR (NR)
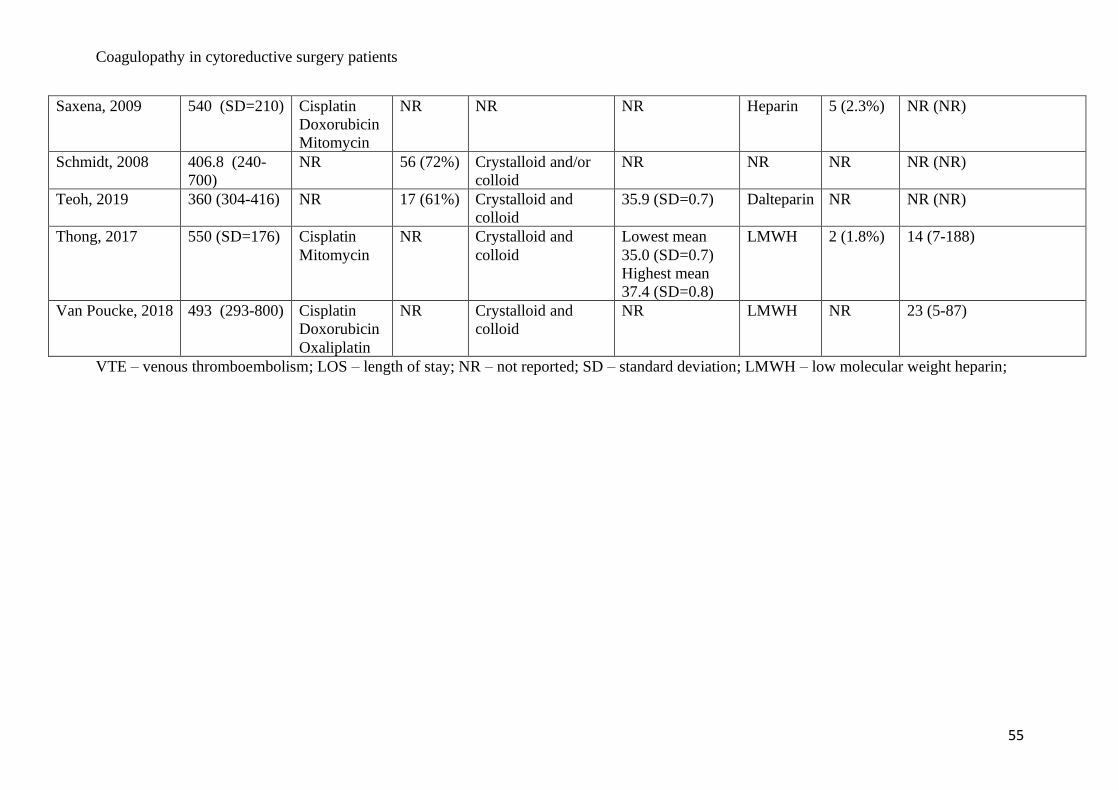
Coagulopathy in cytoreductive surgery patients
55
Saxena, 2009 540 (SD=210) Cisplatin
Doxorubicin
Mitomycin
NR NR NR Heparin 5 (2.3%) NR (NR)
Schmidt, 2008 406.8 (240-
700)
NR 56 (72%) Crystalloid and/or
colloid
NR NR NR NR (NR)
Teoh, 2019 360 (304-416) NR 17 (61%) Crystalloid and
colloid
35.9 (SD=0.7) Dalteparin NR NR (NR)
Thong, 2017 550 (SD=176) Cisplatin
Mitomycin
NR Crystalloid and
colloid
Lowest mean
35.0 (SD=0.7)
Highest mean
37.4 (SD=0.8)
LMWH 2 (1.8%) 14 (7-188)
Van Poucke, 2018 493 (293-800) Cisplatin
Doxorubicin
Oxaliplatin
NR Crystalloid and
colloid
NR LMWH NR 23 (5-87)
VTE – venous thromboembolism; LOS – length of stay; NR – not reported; SD – standard deviation; LMWH – low molecular weight heparin;
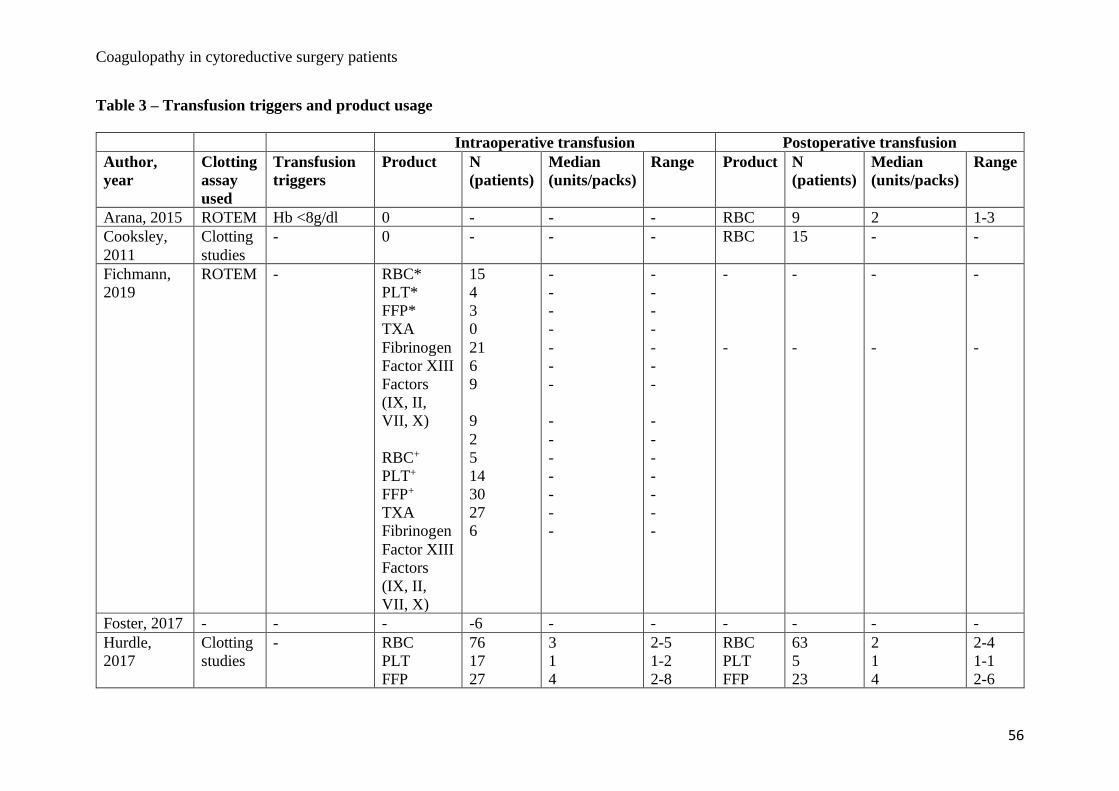
Coagulopathy in cytoreductive surgery patients
56
Table 3 – Transfusion triggers and product usage
Intraoperative transfusion Postoperative transfusion
Author,
year
Clotting
assay
used
Transfusion
triggers
Product N
(patients)
Median
(units/packs)
Range Product N
(patients)
Median
(units/packs)
Range
Arana, 2015 ROTEM Hb <8g/dl 0 - - - RBC 9 2 1-3
Cooksley,
2011
Clotting
studies
- 0 - - - RBC 15 - -
Fichmann,
2019
ROTEM - RBC*
PLT*
FFP*
TXA
Fibrinogen
Factor XIII
Factors
(IX, II,
VII, X)
RBC+
PLT+
FFP+
TXA
Fibrinogen
Factor XIII
Factors
(IX, II,
VII, X)
15
4
3
0
21
6
9
9
2
5
14
30
27
6
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
Foster, 2017 - - - -6 - - - - - -
Hurdle,
2017
Clotting
studies
- RBC
PLT
FFP
76
17
27
3
1
4
2-5
1-2
2-8
RBC
PLT
FFP
63
5
23
2
1
4
2-4
1-1
2-6

Coagulopathy in cytoreductive surgery patients
57
Cryo
TXA
4
103
10
-
10-10
-
Cryo
3 10 10-10
Korakianitis,
2015
Clotting
studies
Hb <9 RBC
FFP
5
6
2
3
1-6
2-8
- - - -
Owusu-
Agyemang,
2014
Clotting
studies
- - - - - - - - -
Piccioni,
2015
Clotting
studies
Hb <8-8.5
g/dl
FFP - INR
>1.5
PLT <50 x109
L-1
RBC
PLT
FFP
78
6
-
3
1
-
0-20
1-2
-
- - - -
Sargant,
2016
Clotting
studies
Cryo -
fibrinogen <2
g L-1
PLT <50-75
x109 L-1
- - - - - - - -
Saxena,
2009
Clotting
studies
Hb <80 g/l
and signs of
anaemia
(sinus
tachycardia,
SBP <100
mmHg, UO
<30 ml/h due
to ongoing
blood loss)
RBC
PLT
FFP
Cryo
186
-
-
-
4
0
4
0
0-43
0-20
0-40
0-50
- - - -
Schmidt,
2008
Clotting
studies
- RBC litres
(L)
FFP (L)
21
35
6
0.6L
1.2L
0.4L
0.3-1.5L
0.6-3.2L
0.2-1.0L
- - - -

Coagulopathy in cytoreductive surgery patients
58
Irradiated
cell saver
blood (L)
Teoh, 2019 TEG - RBC
PLT
FFP
TXA
8
1
3
17
-
-
-
-
713 ±
374mls
244MLS
1003 ±
1065
mls
-
- - - -
Thong, 2017 Clotting
studies
Hb 8-
10mg/dL and
“… clinical
estimation of
blood loss…”
RBC
PLT
FFP
Cryo
87
7
21
1
1089 mls
(mean)
476 mls
(mean)
604 mls
(mean)
150 mls
250-
3129mls
200-
1000mls
241-
1000mls
-
- - - -
Van Poucke,
2018
ROTEM Hb <8±10
mg/dL and
“… clinical
estimation of
blood loss …”
FFP - INR
>1.2
RBC
PLT
FFP
4
0
3
-
-
-
-
-
-
RBC
PLT
FFP
6
2
1
-
-
-
-
-
-
- = not reported; Hb – haemoglobin; g/dL – grams per decilitre; *this study had an early* and late group+ – the early group comprised of patients
treated prior to the enrolment of an anaesthetic care pathway, those who received this anaesthetic care pathway are termed the late group, PRBC
– packed red blood cells, CCU – coronary care unit; FFP – fresh frozen plasma; PLT – platelets; Cryo – cryoprecipitate; TXA – transexamic
acid;

Coagulopathy in cytoreductive surgery patients
59
CHAPTER 3
Title: A pilot study to investigate the role of thromboelastography in cytoreductive surgery and
hyperthermic intraperitoneal chemotherapy patients
Short title: Thromboelastography in cytoreductive surgery patients
Authors: Dr Gary Sharp1 BSc (Hons), MBBS (Hons)
Dr Rebecca McNamara2 MBBS, FANZCA
Dr Neil Pillinger2 MB BCh MSc, FANZCA
Dr Daniel Steffens1,3 BPhty (Hons), PhD
Dr Nabila Ansari1,4,5 MBBS (Hons), FRACS
Dr Daniel Oh3 MBBS (Hons)
A/Prof Christopher Young1,4,5 MBBS (Hons), MS, FRACS
Affiliations:
1. Surgical Outcomes Research Centre (SOuRCe), Royal Prince Alfred Hospital, Sydney,
Australia.
2. Department of Anaesthesia, Royal Prince Alfred Hospital, Sydney, Australia.
3. Faculty of Medicine and Health, The University of Sydney, Sydney, Australia.
4. Department of Colorectal Surgery, Royal Prince Alfred Hospital, Sydney, Australia.
5. RPA Institute of Academic Surgery, Royal Prince Alfred Hospital, Sydney, Australia.
Corresponding Author: Gary Sharp
Address: Surgical Outcomes Research Centre (SOuRCe), PO Box M157, Missenden Rd.
Camperdown. NSW. Australia.
Coagulopathy in cytoreductive surgery patients
60
Tel: + 61 2 9515 3200
Fax: + 61 2 9515 3200
No funding has been applied for or used during this research project.
Original research article.
This is not based upon any previous communications.
Key words
Thromboelastography, TEG, cytoreductive surgery, HIPEC
ABSTRACT
Introduction
Cytoreductive surgery (CRS) is the surgical excision of macroscopic malignancy whilst
hyperthermic intraperitoneal chemotherapy (HIPEC) is the perfusion of a heated chemotherapy
agent directly into the peritoneal cavity to remove microscopic malignancy. CRS/HIPEC is
associated with abnormal coagulation, as noted through standard laboratory tests. TEG is a
viscoelastic (VE) assay that analyses whole blood coagulation. This pilot study will evaluate
TEG parameters in CRS/HIPEC patients in order to identify a clearer cause/ pattern of
coagulopathy.
Methods
Prospective observational single centre pilot study. Fifteen patients, >18 years old and have no
known deranged liver function tests or coagulation disorders undergoing a general anaesthesia
for CRS/HIPEC. Three TEG samples were taken, the first at point of incision (baseline),
second pre-HIPEC and the third post-HIPEC. Differences were calculated using Wilcoxon
Coagulopathy in cytoreductive surgery patients
61
Signed Rank Test. Differences in baseline, pre HIPEC and post HIPEC TEG scores according
to TXA, PCI and surgical time were calculated using Mann-Whitney U Test.
Results
No bleeding complications were observed. A significant difference was seen in CK R values
between baseline, pre and post HIPEC (P 0.004). CKH R time was also significant (P 0.002).
All other results were not significant. All median results were within normal range. Univariant
analyses of TXA, PCI and surgical time showed no statistical significance. No epidural
complications were observed.
Discussion
The results revealed that there was a significant difference between CK R values throughout
the three tests. Although, clinically they were irrelevant. Only minor abnormal inter quartile
ranges were found, all other results were normal. No detrimental clinical outcome was
encountered in anyone with abnormal TEG results. Despite reservations expressed in studies
concerning thoracic epidural use due to potential bleeding complications we had no epidural
complications within our sample.
Conclusion
This pilot study has shown no detrimental coagulopathy. TEG results showed clinically
insignificant disturbance to coagulation pathways during our studied time period.

Coagulopathy in cytoreductive surgery patients
62
Introduction
Cytoreductive surgery (CRS) is a term encompassing numerous intra-abdominal surgical
procedures/resections to remove macroscopic malignancy (1). Evidence suggests that CRS is
beneficial in peritoneal mesothelioma (2), metastatic peritoneal malignancies (3),
pseudomyxoma peritonei (4) and some ovarian malignancies (5). Heated/hyperthermic
intraperitoneal chemotherapy (HIPEC) is the continuous perfusion of a heated chemotherapy
agent directly into the peritoneal cavity via a circuit (6). The role of HIPEC is the elimination
of microscopic malignant cells after the macroscopic removal of malignant tissues through
CRS (7). The chemotherapy agent is heated due to its synergistic action in eliminating
malignant cells (6).
Prior to CRS, the multidisciplinary team will attempt to calculate the peritoneal cancer index
(PCI) through imaging (8). PCI can also, if achievable, be evaluated preoperatively via
diagnostic laparoscopy (9) and then again at laparotomy. The intraabdominal disease is
assessed and given a numerical score via the PCI as first described by Sugarbaker (1996) (10).
To calculate the PCI one first divides the abdominopelvic cavity into nine regions and the small
bowel into four. Each region is then given a score (0-3) dependent upon the size of malignant
deposits found in that region (10). The total score of all of regions are calculated to give a total
out of 39 (10). The higher the PCI the worse the macroscopic disease. The hope of these
complex procedures is a complete cytoreduction.
Researchers have noted that standard laboratory tests (SLT’s): prothrombin time
(PT)/international normalised ratio (INR) and activated prothrombin time (aPTT), can become
significantly deranged in CRS/HIPEC patients perioperatively. The cause of the coagulopathy
is multifactorial (11) but potentially includes the following: loss of protein due to drainage of
Coagulopathy in cytoreductive surgery patients
63
ascites during laparotomy and extensive debulking of tissue (5-7,11-15). Several blood
disorders have been noted such as a reduction in antithrombin III levels (12), platelet count
(11,14) and generalised blood loss (5-7,11,14-18). The operative exposure required for
CRS/HIPEC is extensive, leading to heat loss but also hyperthermia during the HIPEC phase,
both temperature extremes can negatively affect coagulation (7,19). The complex procedures
involved in CRS result in lengthy operative time which in turn worsen coagulopathy
(7,13,15,17,18). Lastly, the HIPEC agents themselves have been postulated as a cause of
worsening bleeding (5,11). These potential causes are additional to the already nutritionally
deplete cancer patient (11).
The measurement of coagulation during CRS in the vast majority of institutions is with SLT’s
e.g. PT/INR and aPTT. These tests have been used in general surgery and other specialties for
decades and continue to be used despite recent evidence suggesting their poor correlation with
risk of haemorrhage (20-22). SLT’s report information about the early initiation of clotting
only (21) and have been found to be unsatisfactory in multiple surgical populations when
attempting to evaluate the bleeding patient (23). Values of these tests are calculated from
plasma, not whole blood (24,25) and as such do not evaluate numerous factors/pathways
involved in coagulation and clot formation (24). Importantly, SLT’s do not evaluate or
measure hyperfibrinolysis (26) which is abnormal amplified clot lysis, resulting in worsening
haemorrhage and culminating in coagulopathy (27).
TEG is a viscoelastic (VE) assay that analyses whole blood in order to evaluate clot formation
and breakdown (28). TEG utilises cartridges containing a patients blood to supply a graphical
representation and numerical data regarding coagulation based against normal parameters (26)
allowing rationalised blood product replacement (24,26,28). A rapid-TEG assay will give
Coagulopathy in cytoreductive surgery patients
64
results quicker, within 5-15 minutes (29), due to the addition of tissue factor which accelerates
the clotting process (25). TEG uses a torsion wire suspended in the blood to calculate the
viscoelastic clot properties, allowing near real time clot analysis (25). This has the potential for
clinicians to diagnose specific clotting deficits requiring replacement (30), guiding blood
product transfusion, maintaining coagulation equilibrium (21), reducing costs, morbidity and
mortality (30). Viscoelastic (VE) assays, which include TEG, have been beneficially utilised
in multiple surgical specialities including liver transplantation, cardiac surgery and trauma (31).
The rationale for this pilot study was to evaluate TEG parameters in CRS patients in order to
identify a clearer cause/ pattern of coagulopathy. Our aim was to highlight the TEG profile
of CRS and HIPEC patients intraoperatively which may in turn identify possible coagulation
kinetic patterns and better treatment options.
Methodology
Ethical consent was granted by the local health district research ethics and clinical governance
department (X17-0400, HREC/17/RPAH/598) for this prospective observational single-centre
pilot study. The sample size was chosen as 15, no sample size calculations were employed.
Participants had to be >18 years old and have no known deranged liver function tests or
coagulation disorders. No patients were anticoagulated preoperatively. Primary disease
pathology was not an inclusion criteria, as such, if the MDT approved the patient as an
operative candidate they were offered participation. Informed consent was gained by one of
two consultant anaesthetists (NP, RM) during the preoperative anaesthetic assessment of 15
consecutive patients. No patients refused participation.
Coagulopathy in cytoreductive surgery patients
65
The anaesthetists on the day of CRS/HIPEC were those who had gained informed consent
previously, thus ensuring continuity of care and allowing patients to ask clarifying questions.
All patients had a thoracic epidural inserted prior to their general anaesthetic with midazolam
for anxiolysis. Induction of general anaesthesia was achieved with a combination of propofol,
opioid and muscle relaxant. All patients were intubated and mechanically ventilated throughout
the procedure. Anaesthesia was maintained with either a target-controlled infusion of propofol
or inhaled sevoflurane. Once anaesthetised invasive haemodynamic monitoring was achieved
via placement of a central venous catheter and a peripheral arterial line. All patients had
received bowel preparation, were catheterised and placed in the lithotomy position with
appropriate pressure support care. Heparin (5000 IU) was administered in all patients at the
beginning of the surgical procedure one hour post thoracic epidural placement. Antibiotic cover
was given prior to skin incision. Temperature was monitored via an oesophageal temperature
probe. Normothermia was maintained via forced air warming blankets and heated fluids until
the commencement of HIPEC. Hyperthermia was minimised during the HIPEC period using
cooled fluids and forced air warmers placed on a “ambient” setting.
Once the patient was prepped and the midline laparotomy incision made, the first TEG was
taken (baseline). All blood samples were drawn from arterial lines under aseptic conditions and
analysed within 5 minutes via a Rapid TEG 6s analyser (Haemonetics Corporation, USA),
the same machine was used for all samples throughout the study. The Rapid TEG 6s was
maintained and calibrated, only TEG 6s cartridges from verified stockists were used. The
second sample (pre-HIPEC) was taken just prior to the administration of HIPEC and the last
sample (post-HIPEC) taken after completion of HIPEC but before abdominal closure.

Coagulopathy in cytoreductive surgery patients
66
The Rapid TEG 6s uses a citrated 4-chanelled cartridge to which the subjects blood is added
via the instrument itself. Each one of these channels contains several reagents and activators to
execute four tests. These are;
1. CK – citrated kaolin.
2. CRT – citrated rapid TEG, uses both tissue factor and kaolin activators. This test
also supplies the TEG-ACT (activated clotting time) result.
3. CKH – citrated kaolin with heparinase neutralises any potential effect heparin may
have on the test sample.
4. CFF – citrated functional fibrinogen test which uses a platelet inhibiting factor to
evaluate the role of fibrinogen on clot structure and strength (32).
Each sample was evaluated for CK (R, K, angle, MA, LY30, TEG-ACT), CRT (R, K, angle,
MA, LY30), CKH (R, K, angle, MA), CFF (MA). There were no missing TEG data. Baseline
demographics and surgical outcomes were summarised as median (interquartile range) or
frequency (percentage), for continuous and dichotomous outcomes, respectively. Differences
in CK, CRT, CKH, and CFF between baseline and pre HIPEC, baseline and post HIPEC and
pre HIPEC and post HIPEC were calculated using Wilcoxon Signed Rank Test. Differences in
baseline, pre HIPEC and post HIPEC CK scores accordingly to TXA (yes versus no), PCI (≤13
versus >13) and surgical time (≤9.6 hours versus >9.6 hours) were calculated using Mann-
Whitney U Test. All statistical analyses were calculated using SPSS IBM statistical Package
version 25. Statistical significance was set at p<0.05.
HIPEC agent administration depended on tumour type, previous chemotherapy exposure and
allergies. Prior to chemotherapy being added to the circuit, the crystalloid solution (2-4Litres)
was run through the system continuously until a temperature of 41 degrees Celsius was reached.
Coagulopathy in cytoreductive surgery patients
67
Chemotherapy was then added to the circuit. The apparatus delivering the HIPEC was a rollator
pump driven perfusion circuit (HT2000, ThermoChem; ThermaSolutions Inc, MN, USA).
HIPEC consisted of Mitomycin C (15 mg/m2), Oxaliplatin (350 mg/m2) or Mitomycin and
Cisplatin. These agents were perfused for 60 or 30 minutes respectively.
Results
Median age was 56 years, with the majority being female (60%). BMI was within healthy range
for all patients. The majority were ASA grade III (70%), the remainder were grade II. Primary
tumour was classified as colonic 53%, mesothelioma 20%, pseudomyxoma peritonei 20% and
appendiceal 7%. Core body temperature (measured in degrees Celsius) during the CRS stage
of the procedure had a median low of 34.9 (34.5-35.2) and a median high of 36.9 (36.3-37.2).
Temperature during HIPEC increased to a median low of 36.9 (36.2-37.2) and a median high
of 37.6 (37.3-38.0). All patients had an open colosseum during HIPEC. The majority received
Mitomycin C (60%), the remainder received Oxaliplatin (20%) or Mitomycin C and Cisplatin
(20%).
Intraoperative intravenous fluid administration comprised of mostly plasmalyte 4.8 litres (L)
median, followed by compound sodium lactate 1.2L median and finally a single patient
received 1 litre of normal saline. Four percent albumin was used in 67% with a range of 0.2-
3.0L (median 1.2L). Blood product replacement was as follows; 50% received PRBC’s with a
median of 2 units, 2 (13%) received cryoprecipitate with a median volume of 270mls, 3 subjects
received FFP with a median volume of 900mls each. TXA was administered in 67% of the
population with 13% (N-2) of those receiving a 1g dose coupled with an infusion of
125mls/hour for either 4 hours or 2.5 hours. The median TXA volume per subject was 1.73g.

Coagulopathy in cytoreductive surgery patients
68
The PCI median was 13.0 (5-27) and 90% had a CC0 score, one patient had a CC1 score.
Surgical operative time ranged between 8.3-10.1 hours with a median of 9.6 hours. The
majority were extubated in the operating theatre (OT) (70%), the remained were extubated in
the intensive care unit (ICU). All patients went to ICU and spent a median of 5 days there. All
patients were extubated by the latest day 2 (median 0.5 days). Thoracic epidural analgesia was
utilised in 100% of the sample, there were no epidural haematomas and no other complications.
Epidural removal was not hampered by coagulopathy either. The median hospital stay was 17
days. There were no 30 day mortalities. A single return to the OT was encountered for fascial
wound breakdown which required wound wash out only. There were no bleeding complications
observed.
A P value <0.05 was considered significant when analysing the TEG data (tables 2-5). There
was a significant difference seen in CK R values between baseline, pre and post HIPEC
(P=0.004) (table 2). CKH R time was also significant (P 0.002) (table 2). All other results were
not significant. All median results were within normal range. When evaluating IQR data,
several abnormalities were identified on the baseline TEG: CRT angle elevation by 1.4
degrees: CRT MA was elevated by 1.3mm; CKH R time was elevated by 1.4 minutes and the
CFF MA was elevated by 2.1 mm. All pre-HIPEC IQR data were within normal range. Post
HIPEC IQR data highlighted only one abnormality in CKH angle which was elevated by
0.8mm. Univariant analyses of TXA (received V did not receive); PCI ≤13 or >13) and surgical
time (≤9.6h or >9.6h) showed no statistically significant between any CK variables (tables 3-
5).

Coagulopathy in cytoreductive surgery patients
69
Discussion
The aim of this study was to highlight the TEG profile of CRS and HIPEC patients
intraoperatively. Our hypothesis was that if we could identify disturbances in TEG variables
subsequent blood product replacement and intraoperative management could be more specific.
The results revealed a significant difference between CK R values throughout the 3 tests
(P=0.005) coupled with CKH R time also being significant throughout the 3 tests (P=0.002).
Although these parameters were significant, clinically they are irrelevant as the baseline test
was normal and became more normal in subsequent tests.
When analysing the interquartile ranges (IQR) there were 4 minor abnormal results found
within the IQR for baseline TEGs and 1 minor abnormality in the IQR for post-HIPEC TEG
all other results were normal. The aforementioned deranged results did not have a detrimental
clinical outcome, neither did they cause a deviation in perioperative management. All median
TEG ranges were normal for all variables. Nonetheless, there were a number of other
interesting findings.
It is well known that CRS can result in vast blood loss (7,17,33), what is not currently known
is the true cause of this population’s coagulopathy (7,15). Saxena et al. (2009) investigated
preoperative and intraoperative risk factors for massive RBC transfusion within the CRS
population. (18) Their results found several significant risk factors for intraoperative bleeding,
these included operation length >9h, and PCI 16 (18). We found no significant link between
either length of surgical procedure and TEG variables or PCI and TEG variables within our
study. However, Saxena et al. (2009) did report a higher mean transfusion rate of 5.9 units per
procedure and 77% received blood (18) when compared to our results which showed only 50%
received PRBCs, similar to other research (33,34), with a median of 2 units. Therefore it could

Coagulopathy in cytoreductive surgery patients
70
be argued that their population was more morbid than ours and at higher risk of bleeding.
Regardless, the administration of PRBCs is associated with an increased morbidity and
mortality in some surgical oncology groups with the accepted principle that transfusion should
only occur when completely necessary (19,35,36).
Upon reviewing other blood product use, 20% of our sample received FFP and only 13%
received cryoprecipitate. These figures are encouraging, especially when coupled with the
normal TEG results. Some authors have suggested the pre-emptive administration of blood
products, such as FFP and/or cryoprecipitate in the hopes to treat any potential bleeding issues
before they arise (34). Piccioni et al. (2015) admitted to administering “extreme” amounts of
FFP in order to maintain an INR<1.5 in the non-bleeding CRS patient (37). Others see this pre-
emptive strategy as unwarranted and argue product replacement should only be administered
when there is a clinical need (7,19). Furthermore, the administration of blood products without
a clear issue potentially puts the patient at more harm than benefit due to well-known infusion
complicatons. Our results suggest pre-emptive product replacement is not necessary.
TXA was administered in 67% of our sample. Results found no CK TEG differences between
those who received versus those who did not receive TXA. Its use appears to becoming more
common place in CRS with research focusing on its potential to reduce transfusion
requirements (17). Sargant et al. (2016) used a protocol with the proactive administration of
TXA and cryoprecipitate to investigate the effect on product transfusion (17). They
administered TXA at the start of surgery and 4 hours into the procedure, coupled with 2 pools
of cryoprecipitate once surgical haemorrhage started but before 2L of blood loss. Their
prospective study consisting of 95 patients found that pre-emptive treatment with TXA and
cryoprecipitate resulted in significantly less intraoperative PRBC, FFP and platelet transfusion
Coagulopathy in cytoreductive surgery patients
71
(17). Raspe et al. (2016) agree and state that routine TXA every 8 hours perioperatively should
be considered in the CRS/HIPEC population (19). Teoh et al. (2019) also utilised TXA in 57%
of their sample and found no TEG abnormalities in either those receiving TXA or those who
didn’t (38). Interestingly, in a recent Cochrane review focussing on the effectiveness of TXA
in reducing blood loss in CRS/HIPEC for advanced ovarian cancer they found only 1 study
that met inclusion criteria (39). Ultimately, the recommendation from this review was that there
was insufficient evidence to routinely use TXA in this population (39). It is clear these findings
cannot be extrapolated to non-ovarian malignancies being treated with CRS/HIPEC, however,
the use of TXA in further CRS/HIPEC populations is a potential area of future research.
One hundred percent of our sample underwent uncomplicated insertion and removal of a
thoracic epidural. CRS/HIPEC is a painful procedure (11) and thoracic epidural analgesia has
been referred to as the ideal analgesic choice (11). Epidural analgesia use is not solely
beneficial for analgesia in patients undergoing major abdominal surgery, it is also effective in
reducing opioid use and quicker return of normal bowel function. It has also been suggested
that epidural analgesia is a factor assisting in early extubation within the OT (33) reducing
ventilator-associated complications (40). Conversely, some suggest thoracic epidural use may
result in a higher risk of spinal haematoma in CRS/HIPEC patients due to coagulopathy (15).
The literature regarding coagulopathy and epidural analgesia highlights the potential
catastrophic complications, such as spinal haematoma and epidural abscess (5,6), however, in
this small pilot study no such issues were found, this is mirrored by the results of several other
studies (5,14,33,34). Research within the CRS/HIPEC community actually appears to highlight
the fact that thoracic epidurals are well tolerated (37). In the only other TEG study within the
CRS population Teoh et al. (2019) also found no TEG abnormalities and reported no epidural
complications (38). However, Teoh et al. (2019) unfortunately reported that >50% of their
Coagulopathy in cytoreductive surgery patients
72
sample complained of poor analgesia despite having a functional epidural in situ (38). There
are of course situations were an epidural is not appropriate such as profound coagulopathy (5)
and the removal of epidurals must be treated with as much respect as the insertion with at the
least normal SLT’s available before removal (14).
Thermal regulation is paramount in any surgical patient. Despite our best efforts temperatures
during CRS were at times hypothermic. Perioperative hypothermia, defined as a core body
temperature <36 degrees Celsius, is a common occurrence (41) especially in the CRS
population (15) but must be controlled to ensure normal coagulation (6). Hypothermia has the
ability to negatively affect coagulation and worsen blood loss (41). CRS is known to cause
hypothermia, due to multiple factors, and despite the use of heated fluids, heated air blankets
and appropriately warmed OT’s we were still unable to consistently keep the core temperature
above 36 degrees Celsius. Interestingly, it did not affect coagulation as per the TEG results.
HIPEC can lead to hyperthermia (7,11) which too must be prevented to ensure normal
coagulation (6) and inhibit unwanted systemic effects such as vasodilatation resulting in
reduced systemic vascular resistance and mean arterial pressure (11). The level of hyperthermia
was minimal in our study population with the median highest temperature during HIPEC being
37.6 with a range of 37.3-38.0 degrees Celsius.
Despite several authors suggesting the use of TEG and other VE assays to assist in CRS and
HIPEC periopeartive management (6,7,11,19,34) we have not found this to be the case. Due to
the nature of this pilot study the sample size is small and findings cannot be extrapolated to the
wider community. TEGs can be time consuming to carry out, they are an added cost (42) to
an already expensive procedure and they are not warranted for all CRS patients (42). Perhaps
Coagulopathy in cytoreductive surgery patients
73
carrying out TEG studies post operatively may highlight further coagulopathy especially in
light of most authors stating their clotting derangement peaked between 24 (19,40) and 48
hours (13,43). Although this study has not highlighted any coagulopathy in our sample the
CRS/HIPEC team must remain vigilant to possible coagulopathy.
Conclusion
This pilot study has shown no detrimental coagulopathy. TEG results showed clinically
insignificant disturbance to coagulation pathways. Regardless, coagulopathy in CRS/HIPEC
patients can cause greater morbidity and mortality and must be recognised and acted upon,
TEG or a similar viscoelastic assay may be beneficially in such patients.
REFERENCES
1. Ansari, N, Brown, K, McBride, K et al. (2019). Accelerating the learning curve in
cytoreductive surgery and hyperthermic intraperitoneal chemotherapy using an external mentor
model. ANZ J Surg, 89, 1097–1101.
2. Youssef, H, Newman, C, Chandrakumaran, K et al. (2011). Operative findings, early
complications, and long-term survival in 456 patients with pseudomyxoma peritonei syndrome
of appendiceal origin. Disease of the Colon & Rectum, 54, 293–299.
3. Arana, L, Fuentes-Garcıa, D, Calvo, M et al. (2015). Alterations in Hemostasis during
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in Patients with
Peritoneal Carcinomatosis, CIR ESP, 93(8): 496-501.

Coagulopathy in cytoreductive surgery patients
74
4. Moran, B, Baratti, D, Yan, TD et al. (2008). Consensus statement on the loco-regional
treatment of appendiceal mucinous neoplasms with peritoneal dissemination (pseudomyxoma
peritonei). J Surg Oncol, 98:277– 82.
5. Korakianitis, O, Daskalou, T, Alevizos, L et al. (2015). Lack of significant
intraoperative coagulopathy in patients undergoing cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy (HIPEC) indicates that epidural anaesthesia is a safe option. Int
J Hyperthermia, 31(8): 857–862.
6. Gupta, N, Kumar, V, Garg, R et al. (2019). Anesthetic implications in hyperthermic
intraperitoneal chemotherapy, Journal of Anaesthesiology Clinical Pharmacology, 35; 1, 3-11.
7. Schmidt, C, Moritz, S, Rath, S et al. (2009). Perioperative Management of Patients
With Cytoreductive Surgery for Peritoneal Carcinomatosis, J. Surg. Oncol, 100:297–301.
8. Webb C, Weyker P, Moitra V et al. (2013). An overview of cytoreductive surgery and
hyperthermic intraperitoneal chemoperfusion for the anesthesiologist. Anesth Analg,
116(4):924–31.
9. Hallam, S, Tyler, R, Price, M et al. (2019). Meta-analysis of prognostic factors for
patients with colorectal peritoneal metastasis undergoing cytoreductive surgery and heated
intraperitoneal chemotherapy, BJS Open, DOI: 10.1002/bjs5.50179.
10. Jacquet, P and Sugarbaker, PH. Clinical research methodologies in diagnosis and
staging of patients with peritoneal carcinomatosis. Cancer Treat Res, 82:359–74.
Coagulopathy in cytoreductive surgery patients
75
11. Sheshadri, D and Chakravarthy, M (2016). Anaesthetic Considerations in the
Perioperative Management of Cytoreductive Surgery and Hyperthermic Intraperitoneal
Chemotherapy, Indian J Surg Oncol, 7(2):236–243. DOI 10.1007/s13193-016-0508-2
12. Arana, L, Fuentes-Garcıa, D, Calvo, M et al. (2015). Alterations in Hemostasis during
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in Patients with
Peritoneal Carcinomatosis, CIR ESP, 93(8): 496-501.
13. Hurdle, H, Bishop, G, Walker, A et al. (2017). Coagulation after cytoreductive surgery
and hyperthermic intraperitoneal chemotherapy: a retrospective cohort analysis, Can J Anesth,
64:1144–1152. DOI 10.1007/s12630-017-0952-7.
14. Owusu-Agyemang, P, Soliz, J, Hayes-Jordan, A et al. (2014). Safety of Epidural
Analgesia in the Perioperative Care of Patients Undergoing Cytoreductive Surgery with
Hyperthermic Intraperitoneal Chemotherapy, Ann Surg Oncol, 21:1487–1493. DOI
10.1245/s10434-013-3221-1.
15. Raspe, C, Piso, P, Wiesenack, C et al. (2012). Anesthetic management in patients
undergoing hyperthermic chemotherapy, Curr Opin Anesthesiol, 25:348–355.
DOI:10.1097/ACO.0b013e32835347b2.
16. Foster, J, Sleightholm, R, Watley, D et al. (2017). The efficacy of dextran-40 as a
venous thromboembolism prophylaxis strategy in cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy, The American Surgeon, 83,134-140.
Coagulopathy in cytoreductive surgery patients
76
17. Sargant, N, Roy, A, Simpson, S et al. (2016). A protocol for management of blood loss
in surgical treatment of peritoneal malignancy by cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy, Transfusion Medicine, 2016, 26, 118–12.
18. Saxena, A, Yan, T, Chua, T et al. (2009). Risk Factors for Massive Blood Transfusion
in Cytoreductive Surgery: A Multivariate Analysis of 243 Procedures, Ann Surg Oncol,
16:2195–2203. DOI 10.1245/s10434-009-0484-7.
19. Raspé, C, Flöther, L, Schneider, R et al. (2016). Best practice for perioperative
management of patients with cytoreductive surgery and HIPEC, European Journal of Surgical
Oncology, 43,6,1013-1027.
20. Thomas D, Wee M, Clyburn P et al. (2010). GUIDELINES. Blood transfusion and the
anaesthetist: management of massive haemorrhage. Association of Anaesthetists of Great
Britain and Ireland. Anaesthesia, 65: 1153-61.
21. Gonzalez E, Moore, E, Moore, H (2017). Management of Trauma-Induced
Coagulopathy with Thrombelastography. Crit Care Clin, 33: 119-34.
22. Paterson, D (2014). Hemorrhage and Coagulopathy in the Critically Ill. Emerg Med
Clin Am, 32: 797-810.
23. Frith, D, Davenport, R, Brohi, K (2012). Acute traumatic coagulopathy. Curr Opin
Anesthesiol, 25: 229-34.
Coagulopathy in cytoreductive surgery patients
77
24. Hayter, M, Pavensk,i K, Baker, J (2012). Massive transfusion in the trauma patient:
Continuing Professional Development. Can J Anesth, 59: 1130-45.
25. Hanke, A, Horstmann, H, Wilhelmi, M. (2017). Point-of-care monitoring for the
management of trauma-induced bleeding. Curr Opin Anaesthesiol, 30 (2): 250-6.
26. Pham, H and Shaz, B (2013). Update on massive transfusion. British Journal of
Anaesthesia, 111(S1): i71-i82.
27. Solomon C, Collis R, Collins P (2012). Haemostatic monitoring during postpartum
haemorrhage and implications for management. British Journal of Anaesthesia, 109(6): 851-
63.
28. Walsh, M, Thomas, S, Howard, J (2011). Blood Component Therapy in Trauma Guided
with the Utilization of the Perfusionist and Thromboelastography. The Journal of Extra
Corporeal Technology, 43: 162-7.
29. Whiting, P, Westwood, M, Ramos, M (2015). Viscoelastic point-of-care testing to
assist with the diagnosis, management and monitoring of haemostasis: a systematic review and
cost-effectiveness analysis. Health Technol Assess, 19 (58).
30. Gorlinger, K, Dirkmann, D, Hanke, A. (2013) Potential value of transfusion protocols
in cardiac surgery. Curr Opin Anesthesiol, 26(2): 230-43.
Coagulopathy in cytoreductive surgery patients
78
31. Sibylle, A and Kozek-Langenecker, A (2013). Management of severe perioperative
bleeding. Guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol, 30:
270-382.
32. Dias, J, Haney, E, Mathew, B et al. (2016). New-Generation Thromboelastography
Comprehensive Evaluation of Citrated and Heparinized Blood Sample Storage Effect on Clot-
Forming Variables, Arch Pathol Lab Med. doi: 10.5858/arpa.2016-0088- OA.
33. Schmidt, C, Creutzenberg, M, Piso, P et al. (2008). Peri- operative anaesthetic
management of cytoreductive surgery with hyperthermic intraperitoneal chemotherapy,
Anaesthesia, 63, pages 389–395. doi:10.1111/j.1365-2044.2007.05380.x.
34. Bell, J, Rylah, B, Chambers, R et al. (2012). Perioperative Management of Patients
Undergoing Cytoreductive Surgery Combined with Heated Intraperitoneal Chemotherapy for
Peritoneal Surface Malignancy: A Multi-Institutional Experience, Ann Surg Oncol, 19:4244–
425 1 DOI 10.1245 /s10434-012-2496-y.
35. Kwon, H, Kim, B, Kim, Y (2019). Association of preoperative anemia and
perioperative allogenic red blood cell transfusion with oncologic outcomes in patients with
non-metastatic colorectal cancer, Curr Oncol, 26(3):e357-e366.
36. Pang, Q, An, R Liu, H (2019) Perioperative transfusion and the prognosis of colorectal
cancer surgery: a systematic review and meta-analysis, World Journal of Surgical Oncology,
17:7 https://doi.org/10.1186/s12957-018-1551-y.
Coagulopathy in cytoreductive surgery patients
79
37. Piccioni, F, Casiraghi, C, Fumagalli, L et al. (2015). Epidural analgesia for
cytoreductive surgery with peritonectomy and heated intraperitoneal chemotherapy.
International Journal of Surgery, 99e106, http://dx.doi.org/10.1016/j.ijsu.2015.02.025.
38. Teoh, D, Hutton, M, Else, S et al. (2019). Epidural analgesia? A prospective analysis
of perioperative coagulation in cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy, The American Journal of Surgery, 217,887e892.
https://doi.org/10.1016/j.amjsurg.2019.01.034.
39. Kietpeerakool, C, Supoken, A, Laopaiboon, M et al. (2016). Effectiveness of
tranexamic acid in reducing blood loss during cytoreductive surgery for advanced ovarian
cancer. Cochrane Database of Systematic Reviews, Issue 1. CD011732.
DOI:10.1002/14651858.CD011732.pub2.
40. Cooksley, T and Haji-Michael, P (2011). Post-operative critical care management of
patients, undergoing cytoreductive surgery and, heated intraperitoneal chemotherapy (HIPEC),
World Journal of Surgical Oncology, 9:169, http://www.wjso.com/content/9/1/169.
41. Ruetzle, K and Kurz, A (2018).Consequences of perioperative hypothermia, Handbook
of Clinical Neurology. 157:687-697, 2018.
42. Fichmann, D, Roth, L, Raptis, D et al. (2019). Standard Operating Procedures for
Anesthesia Management in Cytoreductive Surgery and Hyperthermic Intraperitoneal
Chemotherapy Improve Patient Outcomes: A Patient Cohort Analysis, Ann Surg Oncol,
26:3652–3662, https://doi.org/10.1245/s10434-019-07644-w.
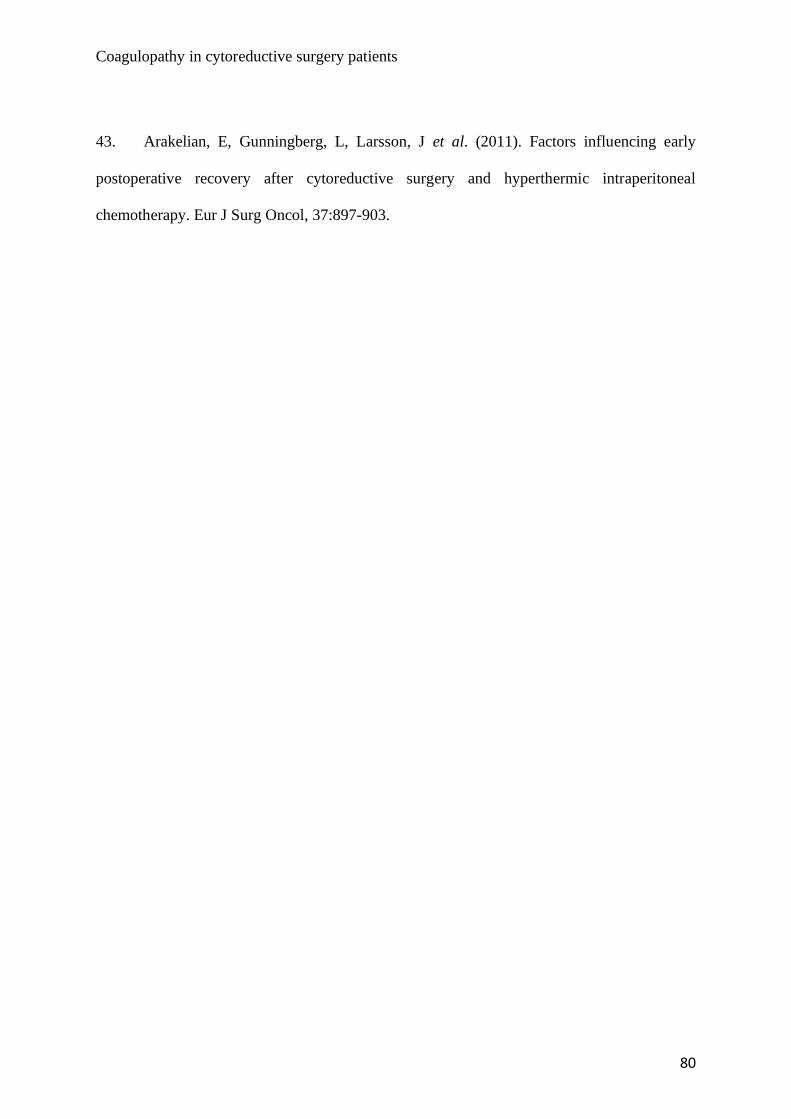
Coagulopathy in cytoreductive surgery patients
80
43. Arakelian, E, Gunningberg, L, Larsson, J et al. (2011). Factors influencing early
postoperative recovery after cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy. Eur J Surg Oncol, 37:897-903.

Coagulopathy in cytoreductive surgery patients
81
Table 1. Baseline characteristics
Age 56.0 (44.0 to 71.0)
Sex
Female 9 (60%)
Male 6 (40%)
BMI 29.3 (25.9 to 30.8)
ASA score
II 4 (30%)
III 11 (70%)
Temperature during CRS
Lowest 34.9 (34.5 to 35.2)
Highest 36.9 (36.2 to 37.2)
Temperature during HIPEC
Lowest 36.9 (36.2 to 37.1)
Highest 37.6 (37.3 to 38.0)
Intravenous fluid administration
(litres)
Compound Sodium Lactate 1.2 (0-5)
Plasmalyte 4.8 (0-8)
Saline 1 (0-1)
4% albumin 1.2 (0.2-3.0)
RBC received
Yes 8 (50%)
No 7 (50%)
RBC (units) 2.0 (1.0 to 3.0)
Cryoprecipitate received 13%
Cryoprecipitate (mls) 270 (240-300)
FFP received 20%
FFP (mls) 900 (540-1350)
TXA received
TXA infusions
TXA no infusion
67%
13%
54%
TXA (g) 1.73 (1.0 to 2.0)
Primary tumour
Colonic 8 (53%)
Mesothelioma 3 (20%)
Pseudomyxoma Peritonei 3 (20%)
Appendiceal 1 (7%)
PCI 13.0 (5.0 to 27.0)
HIPEC agent
Mitomycin 9 (60%)
Oxaliplatin 3 (20%)
Mitomycin and Cisplatin 3 (20%)
Surgical time, hours 9.6 (8.3 to 10.1)
CC score
CC0 14 (90%)
CC1 1 (10%)
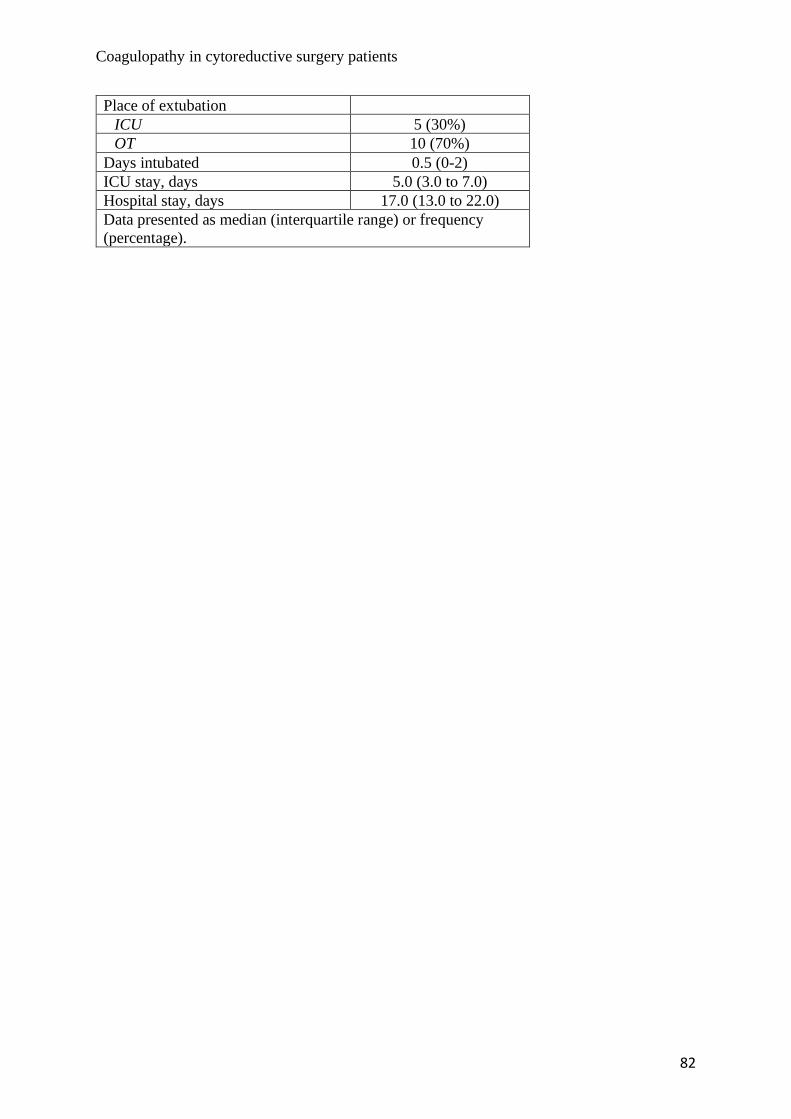
Coagulopathy in cytoreductive surgery patients
82
Place of extubation
ICU 5 (30%)
OT 10 (70%)
Days intubated 0.5 (0-2)
ICU stay, days 5.0 (3.0 to 7.0)
Hospital stay, days 17.0 (13.0 to 22.0)
Data presented as median (interquartile range) or frequency
(percentage).
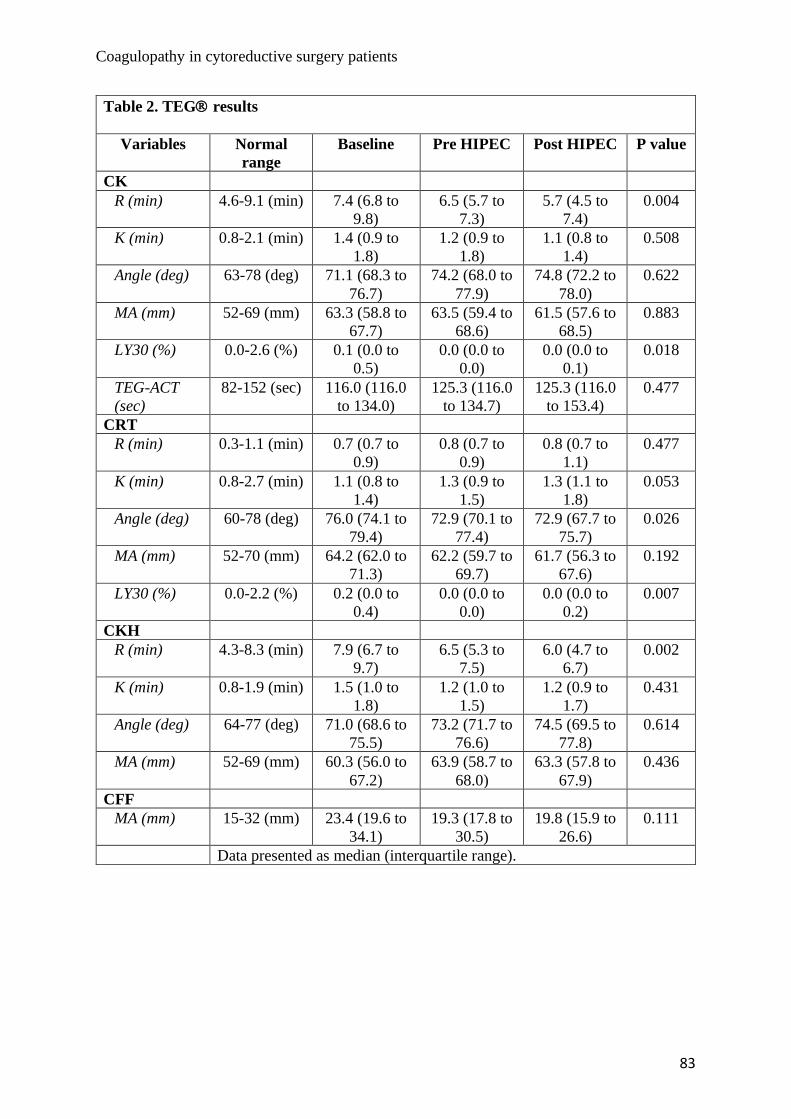
Coagulopathy in cytoreductive surgery patients
83
Table 2. TEG results
Variables Normal
range
Baseline Pre HIPEC Post HIPEC P value
CK
R (min) 4.6-9.1 (min) 7.4 (6.8 to
9.8)
6.5 (5.7 to
7.3)
5.7 (4.5 to
7.4)
0.004
K (min) 0.8-2.1 (min) 1.4 (0.9 to
1.8)
1.2 (0.9 to
1.8)
1.1 (0.8 to
1.4)
0.508
Angle (deg) 63-78 (deg) 71.1 (68.3 to
76.7)
74.2 (68.0 to
77.9)
74.8 (72.2 to
78.0)
0.622
MA (mm) 52-69 (mm) 63.3 (58.8 to
67.7)
63.5 (59.4 to
68.6)
61.5 (57.6 to
68.5)
0.883
LY30 (%) 0.0-2.6 (%) 0.1 (0.0 to
0.5)
0.0 (0.0 to
0.0)
0.0 (0.0 to
0.1)
0.018
TEG-ACT
(sec)
82-152 (sec) 116.0 (116.0
to 134.0)
125.3 (116.0
to 134.7)
125.3 (116.0
to 153.4)
0.477
CRT
R (min) 0.3-1.1 (min) 0.7 (0.7 to
0.9)
0.8 (0.7 to
0.9)
0.8 (0.7 to
1.1)
0.477
K (min) 0.8-2.7 (min) 1.1 (0.8 to
1.4)
1.3 (0.9 to
1.5)
1.3 (1.1 to
1.8)
0.053
Angle (deg) 60-78 (deg) 76.0 (74.1 to
79.4)
72.9 (70.1 to
77.4)
72.9 (67.7 to
75.7)
0.026
MA (mm) 52-70 (mm) 64.2 (62.0 to
71.3)
62.2 (59.7 to
69.7)
61.7 (56.3 to
67.6)
0.192
LY30 (%) 0.0-2.2 (%) 0.2 (0.0 to
0.4)
0.0 (0.0 to
0.0)
0.0 (0.0 to
0.2)
0.007
CKH
R (min) 4.3-8.3 (min) 7.9 (6.7 to
9.7)
6.5 (5.3 to
7.5)
6.0 (4.7 to
6.7)
0.002
K (min) 0.8-1.9 (min) 1.5 (1.0 to
1.8)
1.2 (1.0 to
1.5)
1.2 (0.9 to
1.7)
0.431
Angle (deg) 64-77 (deg) 71.0 (68.6 to
75.5)
73.2 (71.7 to
76.6)
74.5 (69.5 to
77.8)
0.614
MA (mm) 52-69 (mm) 60.3 (56.0 to
67.2)
63.9 (58.7 to
68.0)
63.3 (57.8 to
67.9)
0.436
CFF
MA (mm) 15-32 (mm) 23.4 (19.6 to
34.1)
19.3 (17.8 to
30.5)
19.8 (15.9 to
26.6)
0.111
Data presented as median (interquartile range).
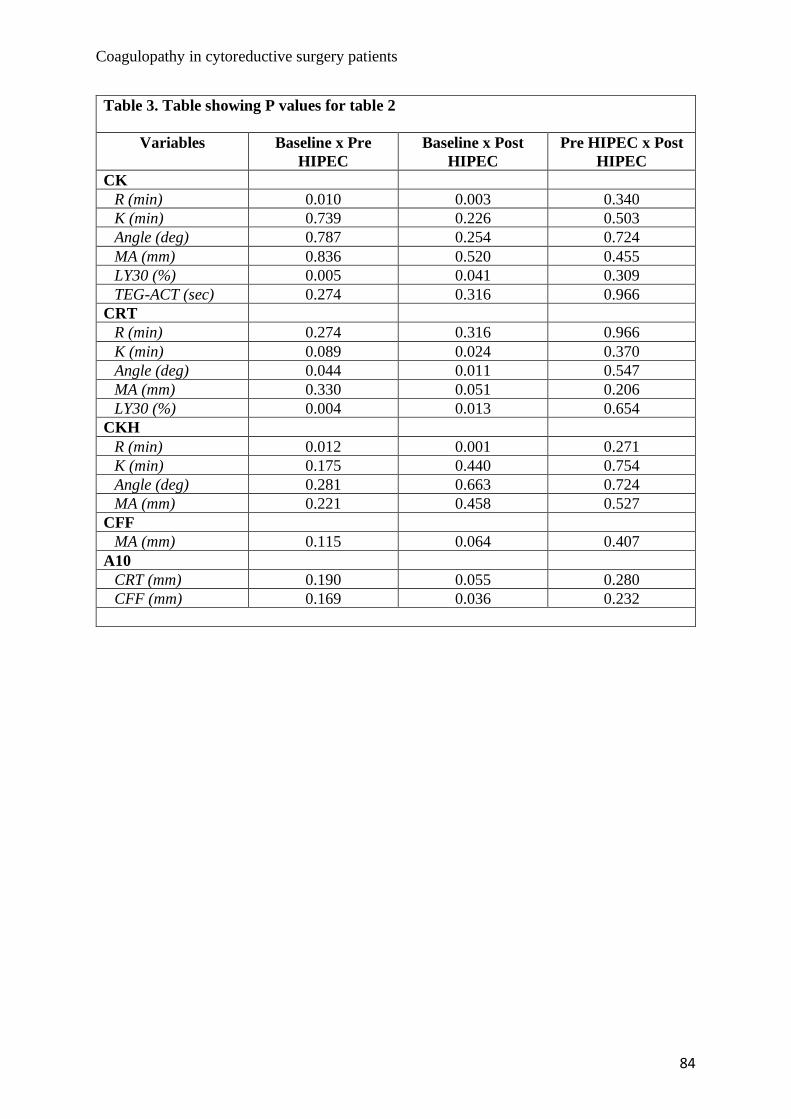
Coagulopathy in cytoreductive surgery patients
84
Table 3. Table showing P values for table 2
Variables Baseline x Pre
HIPEC
Baseline x Post
HIPEC
Pre HIPEC x Post
HIPEC
CK
R (min) 0.010 0.003 0.340
K (min) 0.739 0.226 0.503
Angle (deg) 0.787 0.254 0.724
MA (mm) 0.836 0.520 0.455
LY30 (%) 0.005 0.041 0.309
TEG-ACT (sec) 0.274 0.316 0.966
CRT
R (min) 0.274 0.316 0.966
K (min) 0.089 0.024 0.370
Angle (deg) 0.044 0.011 0.547
MA (mm) 0.330 0.051 0.206
LY30 (%) 0.004 0.013 0.654
CKH
R (min) 0.012 0.001 0.271
K (min) 0.175 0.440 0.754
Angle (deg) 0.281 0.663 0.724
MA (mm) 0.221 0.458 0.527
CFF
MA (mm) 0.115 0.064 0.407
A10
CRT (mm) 0.190 0.055 0.280
CFF (mm) 0.169 0.036 0.232

Coagulopathy in cytoreductive surgery patients
85
Table 3. Table showing univariant analysis of TXA and TEG
Variables Baseline Pre HIPEC Post HIPEC
CK Yes - TXA (N=10) NO TXA (N=5) Yes - TXA (N=10) NO TXA (N=5) Yes - TXA (N=10) NO TXA (N=5)
R (min) 7.4 (7.0 to 9.9) 7.4 (6.7 to 9.7) 6.3 (5.4 to 6.9) 7.1 (5.3 to 8.7) 5.6 (4.7 to 7.4) 6.2 (4.1to 7.5)
K (min) 1.5 (0.8 to 1.9) 1.3 (1.0 to 1.8) 1.1 (0.8 to 1.4) 1.6 (1.2 to 2.1) 1.0 (0.8 to 1.4) 1.3 (1.0 to 1.6)
Angle (deg) 69.9 (67.5 to 78.2) 71.9 (68.3 to 75.8) 74.8 (72.1 to 78.5) 68.2 (65.3 to 74.5) 75.6 (72.4 to 78.3) 73.2 (69.1 to 75.3)
MA (mm) 65.4 (58.8 to 68.6) 61.5 (57.4 to 65.5) 66.6 (59.8 to 70.3) 60.2 (58.2 to 64.0) 62.5 (57.4 to 68.8) 60.0 (56.1 to 63.2)
LY30 (%) 0.0 (0.0 to 0.5) 0.4 (0.0 to 0.6) 0.0(0.0 to 0.0) 0.0 (0.0 to 0.1) -- --
TEG-ACT
(sec)
116.0 (113.6 to
125.3) 134.7 (111.3 to 134.7) 125.3 (116.0 to 137.0) 125.3 (116.0 to 139.3)
125.3 (116.0 to
155.7)
116.0 (111.3 to
144.0)
Data presented as median (interquartile range). No statistical difference between groups observed.
Table 4. Table showing univariant analysis of PCI and TEG
Variables Baseline Pre HIPEC Post HIPEC
CK PCI ≤13 (N=8) PCI >13 (N=7) PCI ≤13 (N=8) PCI >13 (N=7) PCI ≤13 (N=8) PCI >13 (N=7)
R (min) 7.4 (6.7 to 9.7) 7.4 (6.8 to 10.3) 5.8 (4.5 to 6.6) 7.1 (6.2 to 7.6) 5.2 (4.4 to 5.2) 6.2 (5.6 to 7.6)
K (min) 1.6 (0.92 to 1.9) 1.1 (0.9 to 1.8) 1.2 (0.9 to 1.3) 1.6 (0.9 to 1.8) 1.1 (0.8 to 1.7) 1.3 (0.8 to 1.4)
Angle (deg) 69.4 (67.1 to 76.9) 75.0 (68.3 to 76.7) 74.5 (736 to 77.9) 68.7 (66.6 to 77.9) 74. (67.8 to 77.4) 73.2 (72.2 to 78.3)
MA (mm) 60.4 (67.1 to 76.9) 66.0 (59.2 to 67.7) 62.8 (60.4 to 69.1) 65.8 (55.6 to 68.6) 61.4 (58.0 to 66.9) 58.1 (54.8 to 68.7)
LY30 (%) 0.0 (0.0 to 0.8) 0.1 (0.0 to 0.5) 0.0 (0.0 to 0.0) 0.0 (0.0 to 0.0) -- --
TEG-ACT
(sec)
125.3 (116.0 to
134.7) 116.0 (106.6 to 125.3) 125.3 (116.0 to 125.3) 125.3 (116.0 to 144.0)
120.6 (116.0 to
125.3)
144.0 (116.0 to
162.7)
Data presented as median (interquartile range). No statistical difference between groups observed.
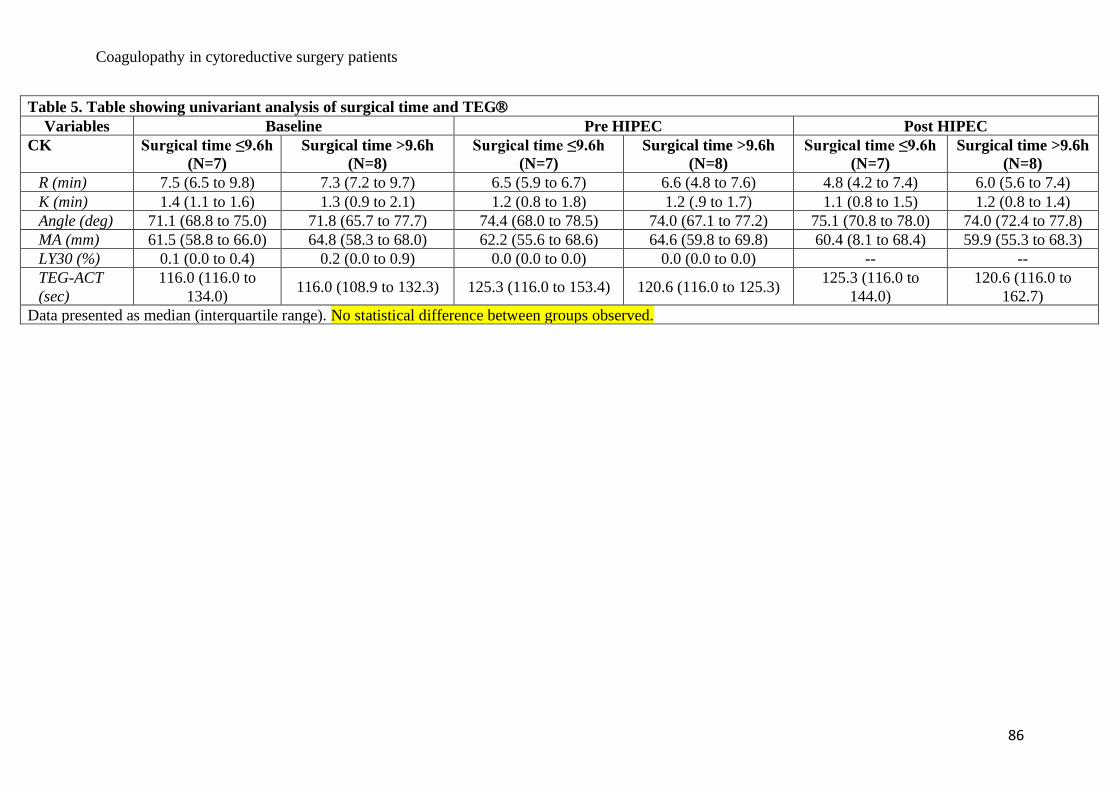
Coagulopathy in cytoreductive surgery patients
86
Table 5. Table showing univariant analysis of surgical time and TEG
Variables Baseline Pre HIPEC Post HIPEC
CK Surgical time ≤9.6h
(N=7)
Surgical time >9.6h
(N=8)
Surgical time ≤9.6h
(N=7)
Surgical time >9.6h
(N=8)
Surgical time ≤9.6h
(N=7)
Surgical time >9.6h
(N=8)
R (min) 7.5 (6.5 to 9.8) 7.3 (7.2 to 9.7) 6.5 (5.9 to 6.7) 6.6 (4.8 to 7.6) 4.8 (4.2 to 7.4) 6.0 (5.6 to 7.4)
K (min) 1.4 (1.1 to 1.6) 1.3 (0.9 to 2.1) 1.2 (0.8 to 1.8) 1.2 (.9 to 1.7) 1.1 (0.8 to 1.5) 1.2 (0.8 to 1.4)
Angle (deg) 71.1 (68.8 to 75.0) 71.8 (65.7 to 77.7) 74.4 (68.0 to 78.5) 74.0 (67.1 to 77.2) 75.1 (70.8 to 78.0) 74.0 (72.4 to 77.8)
MA (mm) 61.5 (58.8 to 66.0) 64.8 (58.3 to 68.0) 62.2 (55.6 to 68.6) 64.6 (59.8 to 69.8) 60.4 (8.1 to 68.4) 59.9 (55.3 to 68.3)
LY30 (%) 0.1 (0.0 to 0.4) 0.2 (0.0 to 0.9) 0.0 (0.0 to 0.0) 0.0 (0.0 to 0.0) -- --
TEG-ACT
(sec)
116.0 (116.0 to
134.0) 116.0 (108.9 to 132.3) 125.3 (116.0 to 153.4) 120.6 (116.0 to 125.3)
125.3 (116.0 to
144.0)
120.6 (116.0 to
162.7)
Data presented as median (interquartile range). No statistical difference between groups observed.
Coagulopathy in cytoreductive surgery patients
87
THESIS DISCUSSION
Prior to the first cytoreductive procedures in the 1930’s, peritoneal malignant disease was
deemed inoperable with a 100% mortality. The pioneers of CRS have since slowly reduced
that mortality. Dr Paul H Sugarbaker revolutionised CRS surgery, producing complete
operative manuals for peritoneal and visceral resections which are utilised to this day. The
standardised approach to classifying peritoneal malignancy, via PCI, has culminated in
treatment being offered to those who will benefit most. PCI also allows surgeons to anticipate
those with the potential to achieve a CC0 resection.
CRS is one of the largest general surgical procedures performed today. As such the morbidity
and mortality attached are not to be taken lightly. There are a plethora of potential
complications. This thesis concentrated upon viscoelastic assay technology and CRS/HIPEC
induced coagulopathy. CRS/HIPEC coagulopathy is thought to be multifactorial (1,2), but in
reality is still poorly understood and can culminate in reoperation (3,4).
SLTs are no longer as reliable as once thought when evaluating bleeding risk and identification,
in fact they can be rather misleading especially when used in a resuscitative capacity. Focus
has instead been directed towards the use of viscoelastic (VE) assays. In chapter 1 attention
was on current evidence-based use of VE assays in the surgical population. VE’s assays, which
include TEG, are assays that use whole blood and the constituents therein to formulate a
clotting profile. This clotting profile is then represented in graphical and numerical form. Data
can subsequently be analysed to guide blood product or factor replacement. Evidence suggests
that VE assays are superior in assessing bleeding (5) and potentially reducing morbidity (6).
However, the use of VE assays is limited to a few specialist procedures currently, namely
orthotopic liver transplantation, trauma, post-partum haemorrhage and cardiac surgery, due to
Coagulopathy in cytoreductive surgery patients
88
cost and lacking evidence of their benefits elsewhere. Benefits within the subset outlined above
showed potential benefits in the rationalisation and utilisation of blood product use, which in
turn reduced allogenic exposure and reduces cost. VE assays have the unique ability to detect
hyperfibrinolysis, the marker of trauma induced coagulopathy and other coagulopathies. As
such they are able to detect abnormalities undetected by SLT’s. However, it is acknowledged
that further research into their use outside of the specialist subset of patients is required.
Following on from the findings in chapter 1, we investigated the association between
CRS/HIPEC and the related bleeding risk and coagulation derangements. No clear cause of
CRS/HIPEC coagulopathy exists currently. Most literature explains the concomitant
coagulopathy as multifactorial. In Chapter 2 a systematic literature review was carried out to
highlight the incidence, cause and impact of CRS-induced coagulopathy, the results of which
highlighted that the current incidence was difficult to calculate. There are several reasons for
this: firstly coagulopathy reporting is modest at best, the definition of coagulopathy is not
standardised within any studies.
The aetiology of CRS coagulopathy was unanimously deemed “multifactorial”. The systematic
review did not shed further light on a potential single pathophysiological cause. CRS and
HIPEC have many potential risk factors for induction of coagulopathy and one may argue that
multifactorial pathogenesis is in fact the most accurate aetiological definition. However, when
defining CRS coagulopathy there is no standardised definition, thus each author employs their
own criteria to define coagulopathy. Interestingly, most authors still use SLT results to define
their criteria for CRS coagulopathy; only 4 studies used VE assays (7-10).

Coagulopathy in cytoreductive surgery patients
89
The impact of CRS coagulopathy was also poorly reported. Due to the aforementioned and
retrospective reporting there is a paucity of information regarding the actual cause of bleeding
and return to OT. Return to OT due to “bleeding” was found in 0.5% of the sample.
Unfortunately no SLT or VE assays defined quantitatively the clotting deviation associated
with the return to OT. Thus, the return to OT may not be due to coagulopathy but in fact due
to inadequate surgical haemostasis. These results question previous suggestions that bleeding
and reoperating is common place in CRS patients (8,11,12). Ultimately the incidence of
coagulopathy was not calculated, the cause not really explained and the impact seemed
insignificant.
In light of the above, a pilot study was launched to investigate the role of thromboelastography
in cytoreductive surgery and hyperthermic intraperitoneal chemotherapy patients. Through this
prospective study, the CRS/HIPEC patients TEG results would follow their operative journey
and highlight the specific clotting deficiencies. The aspiration was to find a specific coagulation
deformity of this patient population that could be targeted by either individual clotting facets
or products to reduce the morbidity and cost associated with generalised blood product
transfusion.
Our results concluded that there was a significant difference between CK R values throughout
the three tests (P=0.005) coupled with CKH R time also being significant throughout the three
tests (P=0.002). However, clinically theses statistical findings were irrelevant as the baseline
test was normal and became more normal in subsequent tests. All median TEG ranges were
normal for all variables. Nonetheless, there were a number of other interesting findings.
Coagulopathy in cytoreductive surgery patients
90
We found no link between operative length or PCI and level of coagulopathy, unlike other
authors (4). Our blood product use was far less than others have documented. We did not
transfuse “pre-emptively” and were not led to transfuse simply by an INR unlike previous
researchers (3,13) and we did not have worse outcomes for it.
There is debate within the literature regarding the use of thoracic epidurals in CRS patients and
the potential risk of epidural haematomas due to coagulopathy. Epidural haematomas and their
sequelae can lead to spinal cord compression and ultimately paralysis. With this catastrophic
complication in mind, some anaesthetists avoid their use. Nonetheless, the debate regarding
epidural use and associated risks appears to be a theoretical one. In our review we found no
evidence of any catastrophic thoracic epidural-associated complications. In fact the most
sinister complications were delays in epidural removal reported due to deranged SLTs (14,15).
All epidurals were subsequently removed uneventfully. The overall thoracic epidural
complication rate was 0.4%, all of which were minor. All of our patients received an
uncomplicated insertion and removal of a thoracic epidural. As such the use of this powerful
analgesic adjunct should be made available to CRS/HIPEC patients.
The use of TXA has increased in recent years and was ultilised in 67% of our sample. We
found no TEG variation between those who did and those who did not receive TXA, results
mirrored by others (9). A recent Cochrane review focussing on the effectiveness of TXA in
reducing blood loss in CRS for advanced ovarian cancer concluded that insufficient evidence
exists to routinely use TXA (16). As such we would recommend not using TXA.
Temperature control of CRS/HIPEC patients is vital to inhibit coagulopathy (17). The team
struggled to maintain normothermia and indeed there were several times during the procedures
Coagulopathy in cytoreductive surgery patients
91
that hypothermia was encountered. Despite the hypothermia being clinically irrelevant without
TEG disturbance, this is an area that needs to be improved upon. To conclude, our study did
not find a significant level of TEG disturbance nor a significant bleeding risk. We concede
that our sample is small and that we focussed solely on intraoperative coagulation. It may in
fact be the case that most coagulopathy develops further in the postoperative period. The hope
is to further reduce the morbidity and mortality and as such postoperative coagulation profiling
is an area of future interest.
REFERENCE LIST
1. Cooksley, T and Haji-Michael, P (2011). Post-operative critical care management of
patients undergoing cytoreductive surgery and heated intraperitoneal chemotherapy (HIPEC).
World Journal of Surgical Oncology, 9:169, http://www.wjso.com/content/9/1/169.
2. Owusu-Agyemang, P, Soliz, J, Hayes-Jordan, A et al. (2014). Safety of Epidural
Analgesia in the Perioperative Care of Patients Undergoing Cytoreductive Surgery with
Hyperthermic Intraperitoneal Chemotherapy, Ann Surg Oncol, 21:1487–1493. DOI
10.1245/s10434-013-3221-1.
3. Bell, J, Rylah, B, Chambers, R et al. (2012). Perioperative Management of Patients
Undergoing Cytoreductive Surgery Combined with Heated Intraperitoneal Chemotherapy for
Peritoneal Surface Malignancy: A Multi-Institutional Experience, Ann Surg Oncol, 19:4244–
425 1 DOI 10.1245 /s10434-012-2496-y.
4. Saxena, A, Yan, T, Chua, T et al. (2009). Risk Factors for Massive Blood Transfusion
in Cytoreductive Surgery: A Multivariate Analysis of 243 Procedures, Ann Surg Oncol,
16:2195–2203. DOI 10.1245/s10434-009-0484-7.
Coagulopathy in cytoreductive surgery patients
92
5. Thomas D, Wee M, Clyburn P et al. (2010). GUIDELINES. Blood transfusion and the
anaesthetist: management of massive haemorrhage. Association of Anaesthetists of Great
Britain and Ireland. Anaesthesia, 65: 1153-61.
6. Wikkelso, A, Wetterslev, J, Moller, AM et al. (2016). Thromboelastography (TEG) or
thromboelastometry (ROTEM) to monitor haemostatic treatment versus usual care in adults
or children with bleeding, Cochrane database of systematic reviews, Issue 8, DOI:
10.1002/14651858.CD007871.pub3.
7. Van Poucke, S, Huskens, D, Van der Speeten, K et al. (2018). Thrombin generation
and platelet activation in cytoreductive surgery combined with hyperthermic intraperitoneal
chemotherapy – A prospective cohort study. PLoS ONE 13(6): e0193657.
https://doi.org/10.1371/journal.
8. Arana, L, Fuentes-Garcıa, D, Calvo, M et al. (2015). Alterations in Hemostasis during
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in Patients with
Peritoneal Carcinomatosis, CIR ESP, 93(8): 496-501.
9. Teoh, D, Hutton, M, Else, S et al. (2019). Epidural analgesia? A prospective analysis
of perioperative coagulation in cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy, The American Journal of Surgery, 217,887e892.
https://doi.org/10.1016/j.amjsurg.2019.01.034.
10. Fichmann, D, Roth, L, Raptis, D et al. (2019). Standard Operating Procedures for
Anesthesia Management in Cytoreductive Surgery and Hyperthermic Intraperitoneal

Coagulopathy in cytoreductive surgery patients
93
Chemotherapy Improve Patient Outcomes: A Patient Cohort Analysis, Ann Surg Oncol,
26:3652–3662, https://doi.org/10.1245/s10434-019-07644-w.
11. Sugarbaker, P, Alderman, R, Edwards, G et al. (2006), “Prospective morbidity and
mortality assessment of cytoreductive surgery plus perioperative intraperitoneal chemotherapy
to treat peritoneal dissemination of appendiceal mucinous malignancy. Ann Surg Oncol, 13,
535-44.
12. Foster, J, Sleightholm, R, Watley, D et al. (2017). The efficacy of dextran-40 as a
venous thromboembolism prophylaxis strategy in cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy, The American Surgeon, 83,134-140.
13. Piccioni, F, Casiraghi, C, Fumagalli, L et al. (2015). Epidural analgesia for
cytoreductive surgery with peritonectomy and heated intraperitoneal
chemotherapyInternational Journal of Surgery 16 (2015) 99e106,
http://dx.doi.org/10.1016/j.ijsu.2015.02.025.
14. Hurdle, H, Bishop, G, Walker, A et al. (2017). Coagulation after cytoreductive surgery
and hyperthermic intraperitoneal chemotherapy: a retrospective cohort analysis, Can J Anesth,
64:1144–1152. DOI 10.1007/s12630-017-0952-7.
15. Owusu-Agyemang, P, Soliz, J, Hayes-Jordan, A et al. (2014). Safety of Epidural
Analgesia in the Perioperative Care of Patients Undergoing Cytoreductive Surgery with
Hyperthermic Intraperitoneal Chemotherapy, Ann Surg Oncol, 21:1487–1493. DOI
10.1245/s10434-013-3221-1.

Coagulopathy in cytoreductive surgery patients
94
16. Kietpeerakool, C, Supoken, A, Laopaiboon, M et al. (2016). Effectiveness of
tranexamic acid in reducing blood loss during cytoreductive surgery for advanced ovarian
cancer. Cochrane Database of Systematic Reviews, Issue 1. CD011732.
DOI:10.1002/14651858.CD011732.pub2.
17. Ruetzle, K and Kurz, A (2018).Consequences of perioperative hypothermia, Handbook
of Clinical Neurology. 157:687-697, 2018.
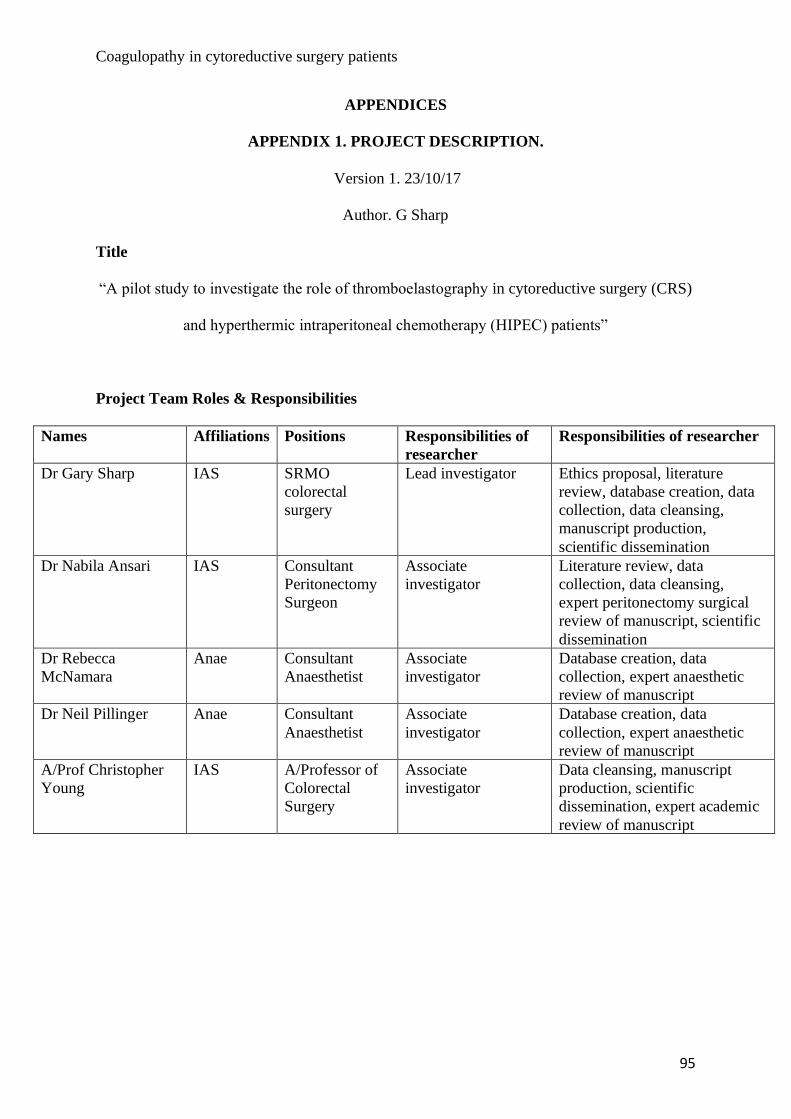
Coagulopathy in cytoreductive surgery patients
95
APPENDICES
APPENDIX 1. PROJECT DESCRIPTION.
Version 1. 23/10/17
Author. G Sharp
Title
“A pilot study to investigate the role of thromboelastography in cytoreductive surgery (CRS)
and hyperthermic intraperitoneal chemotherapy (HIPEC) patients”
Project Team Roles & Responsibilities
Names Affiliations Positions Responsibilities of
researcher
Responsibilities of researcher
Dr Gary Sharp IAS SRMO
colorectal
surgery
Lead investigator Ethics proposal, literature
review, database creation, data
collection, data cleansing,
manuscript production,
scientific dissemination
Dr Nabila Ansari IAS Consultant
Peritonectomy
Surgeon
Associate
investigator
Literature review, data
collection, data cleansing,
expert peritonectomy surgical
review of manuscript, scientific
dissemination
Dr Rebecca
McNamara
Anae Consultant
Anaesthetist
Associate
investigator
Database creation, data
collection, expert anaesthetic
review of manuscript
Dr Neil Pillinger Anae Consultant
Anaesthetist
Associate
investigator
Database creation, data
collection, expert anaesthetic
review of manuscript
A/Prof Christopher
Young
IAS A/Professor of
Colorectal
Surgery
Associate
investigator
Data cleansing, manuscript
production, scientific
dissemination, expert academic
review of manuscript
Coagulopathy in cytoreductive surgery patients
96
Resources
• Resources necessary for the project to be conducted include;
o Thromboelastography (TEG) machines (already available and used routinely
in the operating theatre during cytoreductive surgery (CRS) and HIPEC
procedures) (figure 1).
o TEG cartridges to carry out the assays (already available) (figure 2)
Figure 1. TEG machine Figure 2. TEG cartridges.
• Funding/support being sought or secured
o Nil.
o TEG is supplied by the anaesthetics department as a routine test.
Background
Cytoreductive surgery (CRS) is a combination of peritonectomy procedures and visceral
resections employed to remove all macroscopic peritoneal disease. This is combined with
hyperthermic intraperitoneal chemotherapy (HIPEC) to address microscopic peritoneal

Coagulopathy in cytoreductive surgery patients
97
disease. HIPEC involves instillation of a heated chemotherapeutic agent into the abdominal
and pelvic cavities for between 30-60 minutes. HIPEC is used to treat microscopic tumour
deposits whereas surgery removes macroscopic tumour. CRS is a maximally invasive
procedure performed on appropriate patients with surgically resectable malignant disease
which has metastasised within the abdominal cavity to involve the peritoneum. CRS is usually
performed through a large midline incision (a laparotomy) running from the lower sternal edge
to the pubic bone to ensure adequate access to all quadrants of the abdomen (figure 3).
Figure 3. A laparotomy incision
Through this incision, surgeons perform a thorough examination of the peritoneal cavity and
an assessment of the extent of disease is made using the Peritoneal Carcinomatosis Index (PCI).
CRS is then performed with an aim to remove all macroscopic disease using a combination of
peritonectomy procedures and visceral resection where the extent of surgery is determined by
the volume of disease. Following CRS, HIPEC is circulated through the abdominal cavity using
a closed system and a delivery pump via an open colosseum technique (Figure 4, 5). These
procedures can be long lengthy.

Coagulopathy in cytoreductive surgery patients
98
Figure 4. Schematic of HIPEC set up.
Figure 5. Open abdomen with the HIPEC being administered.
Once CRS and HIPEC is complete, any bowel anastomoses are formed, drains inserted and the
abdomen is closed. Postoperatively, the patient is transferred to intensive care accompanied by
the consultant anaesthetist. During the surgical procedure it is not uncommon for patients to
receive blood product replacement, this has significant morbidity and cost associated.

Coagulopathy in cytoreductive surgery patients
99
We as the peritonectomy group (anaesthetist and surgeons) have noticed that all of our patients
post operatively have a level of coagulopathy as defined by their INR/PT/aPTT. There is a
great paucity of evidence in CRS and HIPEC as such no research has been carried out to define
why these patients are coagulopathic. There are many suggestions and indeed many possible
causes but as-yet we have failed to define the cause or suggest a reasonable hypothesis. What
we do know through evidence-based medicine is that greater knowledge of coagulopathy and
the benefits of point of care (POC) testing using TEG assays may benefit patients.
What is TEG?
TEG, originally known as “Harterts Instrument”, was produced in 1948 by Hartert. Used
throughout Europe in the 1950’s to identify anticoagulant effects, thrombocytopaenia and
fibrinolysis and later utilised by Americans Swan et al in 1958 during cardiac surgery. Its use
in research then commenced around 1990 and began in earnest with trauma patients and the
evaluation of trauma induced coagulopathy (TIC). TEG is a POC device that analyses clot
production, growth and breakdown. It’s performed on whole blood at the bedside allowing
quicker evaluation of in-vivo haemostasis thus guiding resuscitation. Each element of the
TEG trace correlates to a specific aspect of coagulation (figure 4).
Figure 4. A TEG trace.
Coagulopathy in cytoreductive surgery patients
100
Once the TEG is complete, clinicians are supplied with a graphical representation and assay
data regarding coagulation allowing rationalised blood product replacement. TEG works by
placing whole blood into a plastic cartridge which contains a cup; extending into the whole
blood from above is a thin torsion wire. The plastic cup then rotates at a set rate and degrees of
motion. This motion continues throughout clot formation and as fibrin strands form onto the
torsion wire it begins to move the torsion wire. These viscoelastic changes in clot property are
registered by an electromagnetic transducer which in turn is interpreted by the TEG software
and a physical trace is produced. The trace made can then be evaluated against set parameters
defined by the manufacturer. As clot lysis occurs the torsion wire is moved less allowing near
real time clot evaluation.
Perioperative analysis of coagulation and haemoglobin is paramount in managing pathological
states arising from haemorrhage. Intraoperative monitoring of patients includes diligently
recording blood loss, organ perfusion, haemoglobin concentration, unwanted effects of blood
product transfusion and coagulopathy. Standard laboratory tests (SLT’s) such as INR/PT and
PTT were originally used to diagnose bleeding disorders and subsequently used to evaluate
anticoagulants. The end-point of these tests is the first detectable fibrin level which equates to
approximately the first 20-60 seconds of clot formation. SLT’s are used routinely within
general surgery but have been shown to poorly correlate with bleeding risk and are a poor
prognosticators for haemorrhage in critically unwell patients. These time-consuming tests lack
real-time evaluation with values derived from plasma, not whole blood. They also lack
information concerning platelet function, fibrin formation, fibrinolysis and importantly
hyperfibrinolysis. Many studies suggest SLT’s are inadequate when used alone to guide
haemorrhagic resuscitation and coagulopathy. Recent evidence proposes the use of more robust
Coagulopathy in cytoreductive surgery patients
101
assays such as TEG. TEG assays are regarded as POC assays performed on whole blood
which assesses clot formation and breakdown. They are regularly utilised worldwide to guide
allogenic blood product resuscitation and define coagulopathy. Allogenic blood product
transfusion is associated with significant cost, morbidity and mortality. The ability of TEG
assays to rationalise blood product transfusion subsequently lowers transfusion complications
and costs especially in trauma, cardiac and OLT surgery.
• Rationale/Justification
o There is very little current research available of the role of using TEG in
patients undergoing CRS/HIPEC
o There is a need to better to define the extent of perioperative coagulopathy
encountered in patients with peritoneal malignancy undergoing CRS/HIPEC
o This research will hopefully lead to improved practice in CRS/HIPEC through
rationalisation of blood product replacement, by highlighting specific
coagulation issues
o This research will hopefully lead to improved practice in CRS through
rationalisation of blood product replacement, by highlighting specific
coagulation issues
• Research questions
o What is the Thromboelastography (TEG) profile of CRS/HIPEC patients
intraoperatively
• Research aims
o To identify possible patterns in TEG profiles of CRS/HIPEC patients
Coagulopathy in cytoreductive surgery patients
102
• Research objectives
o To have a greater knowledge of the coagulation profile of CRS/HIPEC
patients to aid allogenic blood product replacement which in turn will reduce
morbidity and cost
• Expected outcomes
o TEG may show a consistent pattern of coagulopathy unique to CRS patients
due to the unique insults experienced by this patient population (HIPEC and
lengthy surgery)
Project Design
• Research project setting
o Physical site – Royal Prince Alfred Hospital, Missenden Road, Camperdown,
NSW 2250.
• Methodological approach
o Patients will be consented as per normal – explanation of surgery and
possibility for blood product transfusion.
o Patients will be anaesthetised as per normal.
o CRS patients will have an arterial line inserted after induction of general
anaesthesia as per normal. Meaning no additional invasive procedures are
required.
o The arterial line will be utilised to draw off 5 mls of blood at defined time
periods from the commencement of knife to skin.

Coagulopathy in cytoreductive surgery patients
103
o These times will be at the beginning of the operation when we would usually
perform blood gas analysis, immediately pre HIPEC and at HIPEC
completion, again when we would normally perform blood gas analysis. The
final TEG would be at the end of the procedure as the patient’s epidermis is
being sutured.
o If they require additional TEG assays outside of these set times they will be
carried out and acted on appropriately by the consultant anaesthetists as per
normal.
o Routine INR/APTT/PT will be utilised as per normal at the same times as the
four TEG assays stated above.
o Blood product and fluid resuscitation will be guided by routine investigations
(INR/APTT/PT and urine output) as per normal.
o TEG is already carried out as standard in these patients so the only thing to
change will be the standardised times that they will be taken.
o The paper print-out produced by the TEG machine will be filed with the
anaesthetic notes within the confidential medical notes.
o Dr Gary Sharp will collate and enter the details of these assays into an
anonymised Excel spreadsheet which will be held on a computer in the
Anaesthetic department at Royal Prince Alfred Hospital. No information will
be taken off-site by any members of the project team.
o The rationale behind this method is to allow the peritonectomy team to
evaluate the intraoperative and postoperative coagulation profile of
CRS/HIPEC patients. This will better our knowledge of the unique
coagulation profile of these patients which in turn equates to abnormalities
anticipated and acted upon quicker.
Coagulopathy in cytoreductive surgery patients
104
• Participants
o CRS/HIPEC patients. 15 in total.
o Inclusion criteria. >18 years, CRS/HIPEC patients.
o Exclusion criteria – known deranged liver function tests, known coagulation
disorder.
• Sample size and statistical or power issues
o This is only a pilot study and asuch power issues will not be addressed. This
will of course be acknowledged as a limitation of the study.
• Participant recruitment strategies
o CRS/HIPEC patients.
o TEG is already carried out as standard in this patient population as a known
beneficial adjunct during these procedures. It is likened to taking blood from
their arterial line to check haemoglobin concentration which occurs routinely
at the standardised times defined above. As such consent will be implied.
• Timeframes
o This study will run until 15 participants have been evaluated. We estimate the
study to cease by the end of March 2018.
• Research Activities
o Participant commitment – to have four TEG readings taken at set points
outlined above from an already inserted arterial line.

Coagulopathy in cytoreductive surgery patients
105
o Project duration – roughly 4 months
o Participant follow-up – none.
• Data Collection/Gathering
o We will collect four TEG assays per patient intraoperatively.
o We will collect the TEG assay print outs from the TEG machine. The
anonymised data will be added to a spreadsheet by Dr Gary Sharp. The TEG
assay print outs with be filed along with the anaesthetic charts in the patient’s
confidential medical notes.
o Impact of and response to participant withdrawal – this is a test that is already
carried out as per normal management of CRS/HIPEC patients. If any patients
explicitly refuse TEG assays, we will of course refrain.
• Data Management
o Data will be stored on a private computer owned and housed in the anaesthetic
department of RPA hospital. Data will be entered and analysed on this
computer only.
o Access to the spreadsheet data will only be made available to members of the
project group via a classified password on this single computer.
o We will use the data to produce a scientific manuscript for publication and as
a presentation for a scientific meeting.
o We will destroy the information stored on this computer after seven years.
o The information will be archived on the single computer for seven years.
• Data Analysis
Coagulopathy in cytoreductive surgery patients
106
o We will analyse the data utilising the following information;
▪ Demographic information – age, sex etc
▪ Primary cause of Peritoneal Carcinomatosis (if known)
▪ Past medical history
▪ Past surgical history
▪ CRS uses a scoring system known as Peritoneal Cancer Index (PCI),
this will used to define subgroups.
▪ Duration of surgery (from knife to skin to wound closure)
▪ Organs resected
▪ Surgical complications
▪ Mean temperature
▪ Duration of HIPEC
▪ Type of HIPEC
▪ HIPEC complications
▪ Blood loss
▪ Volume replacement – e.g. albumin, crystalloid
▪ Blood products if any
▪ Haemoglobin
▪ Anaesthetic complications
▪ TEG assay parameters
▪ Date and time extubated
▪ Days in ICU
▪ Normal clotting (INR/APTT/PTT) intraoperative
▪ Calcium, magnesium, phosphate
▪ Fibrinogen level if applicable
Coagulopathy in cytoreductive surgery patients
107
• For research involving an investigational device
o Approved name – Thromboelastography.
o Trade name - TEG
o Manufacturer – Haemonetics USA.
o Known adverse events – none.
o Known contra-indications or warnings – none.
o Approved by - CE marked, ISO certified and FDA approved, European and
British guidelines include TEG in their massive transfusion protocol
Results, Outcomes and Future Plans
• Plans for return of results of research to participants
o They will be made aware of the study and if they wish to be sent a copy of
results once published we will make this available free of charge.
• Plans for dissemination and publication of project outcomes
o Publication in a scientific journal.
o Presentation at a scientific conference.
• Other potential uses of the data at the end of the project
o None.
• Plans for sharing and/or future use of data and/or follow-up research
o None.
Coagulopathy in cytoreductive surgery patients
108
APPENDIX 2. PATIENT INFORMATION
A pilot study to investigate the role of thromboelastography in Cytoreductive surgery (CRS)
and Hyperthermic intraperitoneal chemotherapy (HIPEC) patients.
INFORMATION FOR PARTICIPANTS
Introduction
You are invited to take part in a research study if you are about to undergo Cytoreductive
surgery with Hyperthermic intraperitoneal chemotherapy. This study will investigate if there
are any changes in blood clotting whilst you are undergoing the surgery. Blood clotting or
“coagulation” can be altered by many variables during surgery including temperature, blood
loss, fluid replacement and electrolytes. Patients with pre-existing conditions such as cancer
may also have altered coagulation. During a prolonged operation such as CRS, it is common
for your anaesthetist to periodically test how your blood is clotting in order to guide whether
blood products to assist clotting need to be administered. In the past, these blood tests needed
to be sent to the laboratory which took up to an hour to be returned. Now we are able to test
clotting at the bedside using a machine called a Thromboelastograph or TEG machine allowing
results to be available in real time.
Specific Purpose of the Study
The specific purpose of this study is to determine what is the clotting profile of patients
undergoing Cytoreductive surgery and HIPEC Intraoperatively and post operatively .
The study is being conducted by the following investigators:
• Dr Gary Sharp, Lead investigator, Colorectal Surgery
• Professor Christopher Young, Colorectal Surgery
• Dr Neil Pillinger, Department of Anaesthetics
• Dr Rebecca McNamara, Department of Anaesthetics
• Dr Nabila Ansari, Consultant CRS Surgeon
Study Procedures
If you agree to participate in this study, you will be asked to sign the Participant Consent
Form. We will ask you a few questions about your health and about any medications you
might be taking to ensure your blood is suitable for the experiment. During your operation
three blood samples (total 15mL) will be taken from a blood sampling cannula which is
placed routinely in all cases. One blood sample will be taken post operatively in the
Intensive care unit. Your anaesthetic care will then be standard care. You will have donated
blood for testing in the laboratory only, and there will be no alteration to your elective
surgery or anaesthetic at all.
Risks
Since we are taking the blood from the intraarterial cannula you will have for the anaesthetic,
there should be no additional risk or discomfort whatsoever.
Benefits
Coagulopathy in cytoreductive surgery patients
109
While we intend that this research study furthers medical knowledge and may improve our
provision of blood products or transfusion management in the future, it will not be of direct,
additional benefit to you.
Costs
Participation in this study will not cost you anything, nor will you be paid.
Voluntary Participation
Participation in this study is entirely voluntary. You do not have to take part in it. If you do
decide to take part, you can withdraw at any time up until the blood sample is collected from
you without having to give a reason.
Confidentiality
All the information collected from you for the study will be treated confidentially, and only
the researchers named above will have access to it. The study results may be presented at a
conference or in a scientific publication, but individual participants will not be identifiable in
such a presentation.
Further Information
When you have read this information, Dr Pillinger or Dr Sharpe or your anaesthetist will
discuss it with you further and answer any questions you may have. If you would like to
know more at any stage, please feel free to contact Dr Gary Sharp via the hospital
switchboard 02 95156111.
This information sheet is for you to keep.
Ethics Approval and Complaints
This study has been approved by the Ethics Review Committee (RPAH Zone) of the Sydney
Local Health District. Any person with concerns or complaints about the conduct of this study
should contact the Executive Officer on 02 9515 6766 and quote protocol number _______.
Coagulopathy in cytoreductive surgery patients
110
APPENDIX 3. ETHICS APPROVAL