the local management of soft tissue sarcoma
TRANSCRIPT

The Local Management of Soft Tissue Sarcoma Brian O'SuUivan, James Wylie, Charles Catton, Eric Gutierrez, CarolJ. Swallow, Jay Wunder, Patrick Gullane, Peter Neligan, and Robert Bell
Soft tissue sarcomas (STS) are rare tumors arising from the connective tissues. STS can arise at any anatomic site, can demonstrate varied behavior and prognosis, and therefore present a formidable challenge in manage- ment. The local treatment of STS demands technical complexity in the application of diagnostic tools, includ- ing pathology and imaging, as well as treatment ap- proaches, including surgical ablation and reconstruc- tion, radiotherapy, and, in defined cases, chemotherapy. The understanding of the management of these lesions is profoundly dependent on the multidisciplinary set- ting, where experience has been gained and skills are available to increase the likelihood of a successful result. Several proven options are available for optimal
local management, and the choice of approach depends on the prevailing practice and resource profile of the treating center. With modern approaches, the local control rate can be expected to be at least 90% for extremity lesions, which constitute the most common STS. The experience in other anatomic sites is less favorable as a result of a combination of late diagnosis, technically difficult access sites, and possibly less famil- iarity with these less common presentations. The disap- pointing results make it all the more important for patients to be referred to a multidisciplinary setting with experience in sarcoma management to maximize the chance of successful local outcome. Copyright �9 1999 by W.B. Saunders Company
S oft tissue sarcoma (STS) is a rare solid tumor with great heterogeneity in its anatomy, histologi-
cal subtype, and degree of biologic aggressiveness. Management is influenced significantly by anatomic location and tumor stage. Although a number of randomized, controlled trials exist in STS, most of the evidence about local management emanates from the careful reports of outcome from different single institutions. In this article, extremity STS is used as a paradigm for the rationale for management of STS with surgery alone or in combination with radiotherapy (RT). The importance of the pathologi- cal surgical margin in the assessment of the likeli- hood of local recurrence is emphasized. Details of RT planning and technique are provided with attention to the challenges provided by different anatomic presentations of disease. Functional outcome and morbidity of limb salvage treatment are briefly intro- duced but are covered in greater detail in the article by Davis elsewhere in this issue. A brief description of management principles for less common situations, including retroperitoneal, head and neck, and vis- ceral lesions, completes the discussion. Apart from the information about randomized trials, literature
From the Departments of Radiation Oncology (O'Sullivan, Wylie, Carton, Guttierez) and Surgical Oncology (Swallow, Wunder, Gullane, Neligan, Bell), Princess Margaret Hospital, University Health Network and University of Toronto, Toronto, Canada.
Address reprint requests to Brian O'SuUivan, MD, Department of Radiation Oncology, Princess Margaret Hospital, University of Toronto, 610 University Avenue, Toronto, Ontario, M5G 2M9.
Copyright �9 1999 by W.B. Saunders Company 1053-4296/99/0904-0011510.00/0
citations are used to illustrate concepts and discus- sion in a detailed but not exhaustive manner.
General Axioms About Local Management of Soft Tissue Sarcoma
High Local Control Rates Are Expected
The benchmark for local control rates for extremity sarcomas is set at approximately 90% in modern series. The overall 5-year survival of patients with STS is in the range of 60%, 1 although this rate varies as a function of prognostic factors from case to case. This result is achievable with combined RT (usually administered preoperatively or postoperatively, or brachytherapy) combined with surgery, surgery alone in selected cases, or surgery combined with chemo- therapy and RT.
Although the general recommendation for guid- ing practice in oncology is to rely on the randomized trial or possibly the results of meta-analyses, 2 the consistent high success in ektremity STS poses a paradoxical barrier to the design of relevant random- ized trials. It would be incongruous to believe that investigators would be dissatisfied with the treat- ment options, having several effective strategies from which to choose and all capable of achieving the 90% success in local control when executed properly. These are discussed subsequently.
Patients with sarcomas in other anatomic sites do not fare as well, in part, as a result of greater difficulty with surgical and RT access because of the proximity of important adjacent anatomy. In addi- tion, late diagnosis, manifested most commonly by
328 Seminars in Radiation Oncology, Vol 9, No 4 (October), 1999:pp 328-348

Local Management of Soj? Tissue Sarcoma 329
the large size attained by intra-abdominal tumors at the time of presentation, makes cure even less likely. Potentially the rarity of nonextremity lesions also results in a more varied approach to management, which not only may influence the ultimate outcome, but also may have influenced the ability to design and execute clinical trials in the past.
Multidisciplinary Care
Improvement in treatment of extremity and truneal STS has been based on a better understanding of the tumor growth characteristics, new imaging capability with computed tomography (CT) and magnetic reso- nance imaging (MRI), and multidisciplinary treat- ment focusing on both local tumor control and functional tissue preservation. This evolution in man- agement has occurred concurrent with the develop- ment of multidisciplinary groups that combine sub- specialty expertise in diagnostic imaging; pathology; and surgical, radiation, and medical oncology. Many, if not all, patients require interdisciplinary treatment and would likely benefit from initial consultation by a multidisciplinary team. 3,4
Gustafson et al5 studied the quality of treatment in a Swedish population-based series of primary STS of extremity (329 cases) or trunk (46 cases). They compared patients referred to a specialty center before surgery (195 cases), patients referred after surgery (102 cases), and patients not referred for specialty consultation (78 cases). The combined num- ber of primary tumor operations was 1.4 times higher in patients not referred and 1.7 times higher in patients referred after surgery compared with pa- tients referred to a specialty center before a w sur- gery. Moreover, the local recurrence was 2.4 times higher in the group not referred and 1.3 times higher in the group referred to the specialty center only after an initial surgery. Similar observations were made by Clasby et al 6 from the United Kingdom. In another study from the United Kingdom, disappoint- ing results were obtained in a region during a period of time devoid of a dedicated sarcoma unit, which prompted recommendation to introduce multidisci- plinary care. 7
Specific Local Management Approaches in Soft Tissue Sarcoma
Assessment
Local management starts with assessment and clini- cal staging and is dependent on physical examina-
tion, correct performance of biopsy, imaging the extent of the local lesion, and exclusion of metastatic disease. The specific staging classification and prog- nostic issues are discussed elsewhere in this issue in the article by Pisters and Pollock.
Physical Examination and Imaging of the Primary Tumor
Physical examination in the case of an extremity or truncal lesion should determine whether the lesion originates superficial or deep to the fascia at the local site and should indicate if there is evidence of bone, vascular, or neural invasion (uncommon). Optimal imaging of the primary tumor depends on anatomic site. For extremity sarcomas, MRI has been regarded as the imaging modality of choice for soft tissue masses. Mill enhances the contrast between the tumor and adjacent normal tissues. The multiplanar capability of MRI also provides superior imaging for planning surgery and complex RT treatment tech- niques, a,9 A study by the Radiation Diagnostic Oncol- ogy Grou p compared MRI and CT and found no specificadvantage of MRI over CTJ ~ Optimal choice of investigation may vary depending on the anatomic site of disease and especially the relationship to critical structures. MRI findings of bone or neurovas- cular involvement appear more important for tailor- ing surgery than for predicting local recurrence, distant metastasis, or survival. 11 CT may be invalu- able in excluding the uncommon presence of cortical erosion in adjacent bone. Bone involvement may also be evaluated by technetium bone scan, but we recom- mend this only if the lesion is fixed to bone. In the retroperitoneum and abdomen, CT usually provides satisfactory anatomic definition of the lesion. MRI may supply additional definition for tumors arising from the peMs.
Metastatic Staging Chest CT should be an initial staging modality in most patients because of the predilection for pulmo- nary metastases. Regional lymph node metastasis is uncommon in STS but should be evaluated by physi- cal examination and CT if there is clinical evidence of lymphatic involvement. Abdominal CT and ultra- sound of the liver should exclude hepatic metastases in intra-abdominal sarcomas.
Biopsy The biopsy is a critical step in the management of STS. With function preservation management strate- gies, the appropriate placement and technique of the

330 O'Sullivan et al
biopsy has become a major determinant of outcome of local treatment. The Musculoskeletal Tumor Soci- ety has emphasized the risks in biopsies and recom- mends that biopsy should be undertaken by the surgeon who will perform the definitive resection. 12 The biopsy should be undertaken with complete knowledge of the therapy that will be required for local tumor control.
Three biopsy techniques are generally employed: fine-needle aspiration biopsy (FNAB), core needle biopsy, and open surgical biopsy. FNAB is relatively uninvasive; requires only local anesthesia; and usu- ally yields a cytological specimen adequate for grad- mg of nuclear changes, immunohistochemistry, and evaluation of molecular alterations. 1~ Core needle biopsy under local anesthesia provides a more consis- tent tissue specimen and a cell preparation com- pared with FNAB. In our experience, open biopsy of STS is rarely indicated but yields a diagnosis when needle biopsy is unsuccessful (about 10% of cases). The preference for FNAB versus core biopsy largely depends on the experience of the interpreting patholo- gist. 14-19
All soft tissue masses deep to the investing fascia should be considered to be sarcoma until proven otherwise. They should be staged with imaging of the local site and a biopsy specimen obtained without compromising the planning of appropriate manage- ment. Open incisional biopsy of deep tumors is preferred over excisional biopsy to minimize the difficulty of the unplanned excision. 2~ This situa- tion results when the unsuspecting surgeon contami- nates surrounding tissues after an ill-advised attempt to remove a deep-seated lesion without full diagnos- tic assessments completed (discussed later).
Interventional radiologists are often requested to obtain biopsy specimens of deep-seated lesions using ultrasound or CT guidance. An atraumatic biopsy close to critical structures or where the lesion is difficult to palpate can be accomplished. The radiolo- gist should collaborate with the oncologists who will resect or irradiate the lesion. Needle tracts are potential sites of tumor contamination, and the surgeon and radiation oncologist should be involved in planning the optimal route of biopsy and be aware of possible contamination.
Evidence About the Local Management of Soft Tissue Sarcoma
Several randomized, controlled trials have been re. ported and collectively have established important milestones in the evolution of the local management
of STS (Table ! ) . With one exception, these trials have focused on extremity lesions and around the themes of surgery and adjuvant radiotherapy. Re- cently, the randomized trial has also been the tool to evaluate endpoints other than local control alone. 22 Sindelar et a123 have reported On the use ofintraopera- tive RT in retroperitoneal sarcoma. Investigators at University of California Los Angeles performed a randomized, controlled trial comparing two methods of chemotherapy administration concurrently with RT (intra-arterial vs intravenous) with local control and limb salvage as end points (Table 1).24
The sections that follow on specific treatments are organized within a conceptual schema in which function preservation without detriment to survival is paramount. In turn, this schema emphasizes differ- ent degrees of decision making in the overall manage- ment. In the schema, a qualitative decision about how best to deliver a particular treatment would receive less attention than the decision that the treatment is needed in the first place. This frame- work lends itself primarily to the treatment of sarco- mas of the limbs, which constitute the most common presentation of STS. It is also the site where a significant negative outcome (limb amputation) from a patient standpoint is relevant. Nonetheless, the principle of conservation surgery can also be applied to other anatomic sites.
Amputation Versus Limb Salvage
Amputation was previously, a mainstay in treating extremity STS, being used in more than 40% of cases. 25,26 In the 1970s, it became apparent that RT in combination with surgery could achieve an equiva- lent result. 27 Between 1975 and 1981, Rosenberg et al 2a at the National Cancer Institute randomized 43 patients with high-grade sarcoma of the extremities to receive amputation versu~ a limb-sparing opera- tion followed by adjuvant RT (Table 1). There were four local recurrences in the 27 patients receiving limb-sparing surgery and RT and none in the 16 patients who had an amputation. There was no statistical difference in survival. The result of this small randomized trial coupled-with larger series from numerous institutions 29$7 provided the impetus for the U.S. National Institutes of Health to support a Consensus Development Conference on Limb-Spar- ing in sarcoma management. Consideration of the evidence also included a complex decision analysis approach, one of the earliest examples in oncology. 3a The conclusions confirmed the appropriateness of

Local Management of Soft Tissue Sarcoma 331
Table 1. Phase III Randomized, Controlled Trials in the Local Management of Soft Tissue Sarcoma
Study No. Local Center* and Authors Period Site Trial Schema Patients Recurrence Comments
NCI, Rosenberg et 1975-82 Extremity Amputation vs 16 0 (0%) Small trial with imbalance. al 2a Surg + EBRT 27 4 (15%) No survival difference
NCI, Sindelar et al 2~ Not RPS IORT + postop RT 15 6 (40%) Small trial. Significant tox- given vs postop EBRT 20 16 (80%) icity. No survival differ-
ence MSKCC high grade, 1982-92 Extremity, Surg vs 63 19 (30%) No survival difference
Pisters et al 5~ trunk Surg + BRT 56 5 (9%) NCI high grade, 1983-91 Extremity Surg vs 44 9 (20%) No survival difference
Yang et a149 Surg + postop 47 0 (0%) EBRT
MSKCC low grade, 1982-92 Extremity, Surg vs 23 6 (26%) Subset of main trial. Poor Pisters et al 5~ trunk Surg + BRT 22 8 (36%) control in low grade with
NCI low grade, Yang 1983-91 Extremity Surg vs 24 8 (33%) et a149 Surg + postop 26 1 (4%)
EBRT CSG/NCIC CTG, 1994-97 Extremity Preoperative EBRT 84 Too early
O'Sullivan et a122 'vs postop EBRT 92 Too early
UCLA, Eilber et al24 1984-88 Extremity Concurrent RT + 52 5 (8%) IV Dox vs concur- 44 3 (7%) rent RT + IA Dox
BRT Subset of main trial. Equal
control with EBRT for low grade
Follow-up too short to report. Increased wound complications with preop- erative EBRT
Chemotherapy trial with local control endpoint
*NCI, U.S. National Cancer Institute; MSKCC, Memorial Sloan-Kettering Cancer Center; CSG/NCIC CTG, Canadian Sarcoma Group/National Cancer Institute of Canada Clinical Trials Group; UCLA, University of California Los Angeles. Abbreviations: Surg, conservative surgery; EBRT, external beam radiotherapy; RPS, retroperitoneal sarcoma; IORT, intraoperative radiotherapy; postop, postoperative; BRT, brachytherapy; IV Dox, intravenous doxorubicin; IA Dox, intra-arterial doxorubicin.
limb sparing for most extremity STS, thereby herald- ing a new era in STS m a n a g e m e n t 9
There still remains a group of patients who are better treated with amputation. Although high- grade STS was originally considered to have a lower risk of metastasis if treated by amputation, Williard et al 4~ reported no survival advantage to this ap- proach in high-grade STS. These authors then chronicled the practice change from 1968 to 1990 at Memorial Sloan-Kettering Cancer Center (MSKCC) when the amputation rate fell from 50% to less than 5%. 41 At Princess Margaret Hospital, amputation was never popular and used in only 7 of 226 patients with extremity STS treated between 1980 and 1988. 42 Therefore, amputation is only rarely performed and with significant restrictive criteria: (1) It is impos- sible to achieve adequate surgical clearance because the lesion involves major neurovascular structures or multiple compartments (Fig 1); (2) potential major RT complications would result from dose and volume considerations; (3) in some lower extremity distal lesions, a below-knee amputation prosthesis may be more serviceable than a limb damaged by extensive surgery and radiation43; and (4) some cases of recur- rent disease are not amenable to further surgical resection (or adjuvant RT). The management of
local recurrence is detailed more extensively by Catton et al in this issue.
Surgery Alone Versus Surgery and Radiotherapy
Although amputation is avoidable in most cases, it is also helpful to consider whether adjuvant treatment (predominantly RT) is needed to achieve limb conser- vation compared with surgery alone. This issue is complicated by case heterogeneity, but a subgroup of patients with extremity sarcoma probably do not need RT.
Surgery Alone
Several sources of evidence justify using surgery alone, although all rely on single institutional experi- ence with practices involving degrees of selection. Karakousis et al44 retrospectively reviewed 144 con- secutive extremity patients treated at Roswell Park Memorial Institute using a selective combination of modalities. A consistent policy restricted adjuvant postoperative RT to patients with a minimal intra- compartmental surgical margin less than 2 cm, regardless of grade. The estimated 5-year local recur-

332 O'Sullivan et al
rence rates for surgery only and for postoperative RT were indentical (6%), The authors concluded that adjuvant postoperative RT may be applied selec- tively, for inadequate surgical margins, as seen in only 43% of their patients. 44 Similarly, Geer et a145 reported the outcome of American Joint Committee on Cancer/International Union Against Cancer T1 extremity lesions, in which an approach using sur- gery alone predominated from 1982 and 1990. Of 159 patients treated without amputation, 117 underwent surgery alone (wide excision), and the remainder (42 patients) received RT. Those managed with surgery alone fared better with a 5-year local recurrence-free survival of 92% compared with 77% in those treated with combined surgery and RT, again underlining the problem of case selection.
Swedish studies describe the omission of adjuvant
Figure 1. (A) T2-weighted MRI scan of tumor shows the difficulty in treating a lesion arising in the deep posterior calf compartment with abut- ment of the interosseous mem- brane (arrow). Assuming that the lesion is resect~ible, preop- erative radiotherapy would have an important advantage because the dose is moderate, and it may allow a small strip of circumference on two sides of the limb to be spared while treating the centrally located tumor. (B) High signal change (arrow) can be seen in the anterior compartment repre- senting either progression of tumor superior to the interos- seous membrane or peritu- moral edema. The dilemma in this case is whether tumor has infiltrated anteriorly. At the time of writing, the au-" thors have ordered a biopsy of the anterior compartment musculature for this patient. If this biopsy is positive, an amputation will be performed because there is no opportu- nity to achieve an adequate furtctional outcome if resec- tion of three of four compart- ments together with the fibula is necessary.
RT using strict selection criteria. 46 Whether the tumor was subcutaneous, intramuscular, or extramus- cular guided the type of surgery. Local recurrence was seen in 2 of 37 (5%) arfd 2 of 24 (8%) in the subcutaneous and intramuscular categories. Most deep sarcomas were resected without diagnostic biopsy or after only FNAB. This experience is not comparable to the experience in many sarcoma centers, where many patients are referred with lesions already expanding out of a single muscle unit or have undergone biopsy betbre referral. 47
The University of Chicago Medical Center de- scribed wide-margin excision of 62 subcutaneous sarcomas of the extremities. 48 The protocol com- prised careful attention to wide radial surgical mar- gins and resecting unviolated fascia as a natural barrier to tumor spread. The 5-year disease-free

Local Management of Soft Tissue Sarcoma 333
survival was 85% with three local recurrences (5%). All three recurrences were among the 40% of pa- tients who received RT. Although the authors inter- pret this data to suggest that RT is not indicated in subcutaneous tumors, the effect of selection bias in this nonrandomized trial is obvious.
Adjuvant Radiotherapy Superficial lesions, at least in expert hands, may be managed with surgery alone. For stage Tlb, T2a, and T2b tumors, however, the evidence strongly suggests that surgery that does not achieve wide clearance through normal tissue has a significantly higher rate of local failuse. Adjuvant RT with conservative surgi- cal resection was evaluated in two randomized clinical tr ials9 Yang et a149 randomized 91 patients with high-grade extremity lesions after limb-sparing surgery to receive adjuvant chemotherapy alone or concurrent chemotherapy and RT. An additional 50 low-grade tumors were to receive adjuvant RT or no further treatment after the surgery. The local control for those receiving RT was 99% compared with 70% in the control group (P = .0001). The results were similar for high-grade and low-grade tumors (Table 1).
Adjuvant RT was evaluated in a second random- ized trial of 126 cases between 1982 and 1987 (Table 1).5~ Brachytherapy (BRT) was used, consisting of an iridium- 192 implant delivering 42 to 45 Gy over 4 to 6 days. At 5 years, the local control for high-grade tumors was 90% with BRT compared with 65% in surgery-alone controls (P = .04). No improvement in local control was evident in the low-grade tumors (local control was 78% in the controls and 73% with BRT). The full explanation remains unresolved, although one suggestion implicates the relatively long cell cycle of low-grade tumors in which tumor cells may not enter the radiosensitive phases of the cycle during the relatively short BRT dwell time. 5~
Extent of Surgery and Characterization of Margins
The description by Enneking et a151,52 of the extent of surgery as related to the anatomic location of sar- coma within the fascial compartments was an impor- tant contribution. The observations antedated cross- sectional imaging, which substantially improved the characterization of the anatomic extent of disease. Using pathological evaluation, Enneking et al ob- served that most high-grade extremity STS were surrounded by a reactive zone of compressed normal tissue, inflammatory cells, and invasive tumor. Using the reactive zone and the fascial compartments as
boundaries, they described four levels of resection: (1) intralesional the plane of resection passed within the tumor substance; (2) marginal the plane of resection passed through the reactive tissue surround- ing the sarcoma; (3) wide--the plane of resection passed through normal tissue within the compart- ment of STS origin; and (4) radical all tissues within the compartment of origin were resected. A radical resection was suggested for most high-grade sarcomas to encompass all microscopic disease at the margin of the tumor.
Today, Enneking's radical resection is rarely indi- cated. Current imaging techniques demonstrate the radial extent of sarcoma within the compartment and, together with RT, permit conservation of much of the compartmental muscle without increased local failure. Of more importance than the definition of planned surgery is the actual extent of viable residual disease remaining after surgery. This variable (the amount of residual viable disease remaining in the wound after resection) can never be known exactly but is probably best represented by expert pathologi- cal assessment of the surgical margin. Characteriza- tion of the margin guides the need for adjuvant RT for tumors with insufficient normal tissue at the surface to prevent local recurrence reliably.
Patients with positive margins of resection have inferior local control. The Massachusetts General Hospital series 53 reported that the 5-year actuarial local control rates were lower for those with positive margins (97% and 81%). Tanabe et a154 found a similar result in 95 patients treated with preopera- tive RT at M.D. Anderson Hospital except that those with positive margins had a local control of only 62%. We have previously reported greater than 90% local control in patients achieving negative margins. 55 An analysis of 1,041 patients confirmed that microscopi- cally positive margins are an independent adverse prognostic factor for local recurrence. 56
The cause of positive margins is rarely discussed. A previous report from Princess Margaret Hospital reported a 48% rate of involved margins in a group treated by a variety of surgeons in different hospi- tals. 57 This rate contrasted to a margin positive rate of 15% (9 of 62) in a later study in which all patients were operated on within the musculoskeletal oncol- ogy group: 55 Positive margins were related to preser- vation of major neurovascular structures in five patients, were related to large tumors at the limit of limb-sparing surgery in three patients, and were due to surgical error in one patient. The policy in STS surgery should be to achieve negative surgical mar-

334 0"gullivan et al
gins, and this is best achieved by performing surgery at an experienced referral center.
Radiotherapy Approaches Premises for Using Radiotherapy With Surgery in Soft Tissue Sarcoma
The principle Of using RT in combination with surgery is based on two premises supported by clinical trials: (1) Microscopic nests of tumor can be destroyed by RT, and (2) more limited surgery can be performed when RT is combined with surgery, De- spite earlier views to the contrary, radiosensitivity assays performed on sarcoma cell lines grown in vitro have confirmed similar radiosensitivity to other ma- lignancies, such as breast cancer, 58,59 and provide further support for the first premise. The second premise stresses the desire to preserve tissue in the interest of cosmesis and function, as is the case in many extremity, truncal, breast, and head and neck sarcomas. It is also desirable in situations in which adequate surgery to achieve complete tumor clear- ance is impossible because of the constraints of critical unexpendable normal anatomy, although sup- portive evidence in these rare unfavorable situations is unavailable. Examples include retroperitoneal sar- comas, high-risk presentations- in the head and neck with skull base invasion, and spinal canal invasion in truncal lesions.
Many presentations of visceral sarcomas are not usefully managed with RT because of the mobile nature of these anatomic structures within the pelvic, abdominal, or thoracic compartments. After resec- tion of visceral sarcomas, accurate identification of the field at risk is particularly problematic. Contami- nated loops of bowel or mesentery may relocate remotely within the abdominal cavity after surgery, and pleural contamination and mediastinal shift may occur after intrathoracic resections. Fixed lesions in the pelvis or attached to internal truncal walls may occasionally be suited to preoperative or postopera- tive RT. Typically, however, the vast size of the radiation fields needed to cover entire body cavities coupled with the modest doses that can be adminis- tered to organs in these settings confines such ap- proaches for visceral STS to the experimental set- ting.
Anatomic Principles in Using Radiotherapy in Soft Tissue Sarcoma
STS tend to spread in a longitudinal direction within the muscle groups of the extremity. They generally
respect barriers to tumor spread in the axial plane of the extremity, such as bone, interosseous membrane, and major fascial planes. Thus, the margins of RT must be wide in the cephalocaudal direction, but in the cross-section, there may be much greater security in defining structures that are not targeted. For nonextremity lesions, the preferred direction is also along the direction of the involved musculature, but care must be taken to ensure that the fascial planes are appropriately recognized and encompassed in the radiation target volume.
Timing of Radiotherapy Preoperative RT promotes collaboration between the surgical and radiation oncologist and facilitates a complete management plan to be fashioned before any surgical intervention. Preoperative RT is also delivered to an undisturbed and potentially better oxygenated tumor site 6~ and permits administration of lower dosages of radiation without compromising local control. 6~ Nielsen et a162 noted that the field size and number of joints irradiated in preoperative RT was significantly less than if the treatment was administered postoperatively, which may result in improved limb function. 63,64 Pollack et al65 suggested that preoperative RT is preferred in patients present-- ing with gross disease. A retrospective series from Massachusetts General Hospital 66 suggested that preoperative RT may be more efficacious for lesions larger than 5 cm. Preoperative RT is often delivered on a partially representative biopsy specimen, how- ever, and may interfere with future histopathologic analysis. Additional concerns'about preoperative RT include the increased risk of wound complications, which is discussed later.
The conclusions from the available evidence are liable to bias because of the nonrandomized fashion in which treatment was allocated. It is hoped that the major issues will be resolved by our recently com- pleted National Cancer Institfite of Canada Clinical Trial group SR-2 study performed by the Canadian Sarcoma Group. 22 This is the only randomized com- parison between preoperative and postoperative RT and has several endpoints: wound complications, survival, and local control. In addition, quality of life, physical function, economic cost, RTplanning param- eters (field size and numbers of joints irradiated), and incidence of acute and late radiation effects will be evaluated.
Until we complete the analysis of SR-2, our own criteria for preoperative RT are as follows: (1) the need to restrict RT volumes maximally in some anatomic sites (eg, head and neck); (2) the desire to

Local Management of Soft Tissue Sarcoma 335
minimize RT dose in some situations (eg, when critical neurological tissues are in close proximity); and (3) a desire not to irradiate new tissues, espe- cially skin grafts, which are vulnerable to the effects of high-dose postoperative RT once transposed into the target area at the time of surgery. 42 A summary of the relative indications that we use to select patients for preoperative RT is provided in Table 2, notwithstanding the trade-off required between the potential benefits and the risk of wound morbidity.
Radiotherapy Modality
Conventional external-beam radiotherapy versus brachytherapy. Two methods of RT delivery are com- monly employed: external-beam RT (EBRT) in the ambulatory setting and BRT. No randomized data compare these modalities directly. As noted earlier, both have been compared with surgery alone. The 5-year local control achieved with BRT was 89% (high-grade lesions only) compared with 80% to 98% with EBRT (all grades).28,49,5~
BRT has several advantages over EBRT, includ- ing a shorter overall t reatment time (4 to 6 days vs 5 to 6.5 weeks), and treatment can be initiated sooner after surgery when tumor clonogen numbers are at a minimum. The irradiated volume is also smaller, which may confer functional advantages. Savings of $1,000 per patient treated with BRT compared with EBRT may be realized. 67
No apparent benefit for BRT over surgical exci- sion alone is evident in low-grade lesions, 68 and EBRT appears more effective for these tumors. Suit et a166 reported only two local recurrences in 40 patients with low-grade tumors treated with surgery, and we have already observed that the results re- ported by Yang et a149 using EBRT applied equally to low-grade lesions (Table 1).
EBRT may include photons or particle beam (electrons, protons, pions, or neutrons). Protons have similar radiobiologic effects to photons. Their main advantage is when tumors lie in direct proximity to critical structures because of the ability to achieve
Table 2. Relative Indications for Preoperative Radiotherapy, Despite Concerns Related to Wound Complications
Treatment Context~Sarcoma Site Issues of Concern Comments
Head and neck Paranasal sinus
Skull base Cheek and face
Split-thickness skin graft recon- struction (especially lower limb)
Large-volume GTV or CTV occupying celomic cavities
Retroperitoneal
Proximity to optic apparatus (eye, optic nerves, chiasma)
Proximity to spinal cord, brain stem
Skin graft breakdown and conse- quent infection
Proximity to bowel, liver, kidney
Some small bowel lesions with Proximity tO critical anatomy, side-wall adherence
Thoracic wall/pleura especially intestine
Proximity to lung or cardiac structures
Abdominal trunk Walls peMc Proximity to kidney, bowel, liver, side-wall , ovaries
GTV adjacent todose-limiting critical anatomy
Thoracic inlet/upper chest Proximity to brachial plexus wall low neck
/
Medial tJhigh (young male) Proximity to testes Central limb tumor Proximity to other compart-
/ ' ments
Major functional deficit (visual) may be avoided.
Other lesser morbidities (dental, xerostomia) may also be less because of reduced doses and volumes
Many months to years of recreational and/or vocational disability may occur during healing (rare)
Critical organs may be displaced by tumor or not fixed or adherent as is likely in postoperative setting. Entire tumor treated before possible contamination of cavity
Contamination of abdominal cavity renders post- operative radiotherapy unsuitable
Lung may be displaced by chest wall or pleural tumor and can be avoided with preoperative radiotherapy, or permits GTV to be treated before operative contamination
Avoid CTV encroachment on vulnerable anatomy
Dose limitation of critical anatomy lends itself to preoperative radiotherapy. Additional volume considerations
Permanent infertility may be avoided Permit partial circumferential sparing, which
would not be feasible in postoperative setting
Abbreviations: GTV, gross tumor volume; CTV, clinical target volume.

336 O'SuUivan et al
more accurate targeting. 69 High linear energy trans- fer radiation, such as neutrons, confers radiobiologic advantages over photons, which include reduced repair of radiation damage in tumor cells, sensitivity of cancer cells to RT throughout the cell cycle, and less protection offered to hypoxic cancer cells. Any such advantages are tempered, however, by potential late damage, and their use remains experimental.
Intraoperative radiotherapy. Most interest for intra- operative RT (IORT) has been in retroperitoneal sarcoma and is discussed later. Some reports also describe it for extremity sarcomas. 7~ It is difficult to determine the precise place for this modality, espe- cially in extremity lesions, in which the use of conventional approaches such as EBRT is not associ- ated with significant local control problems. IORT usually involves the use of electron beam treatments, but there has been experience with high dose rate afterloading to deliver a dose of 15 Gy at the time of surgery followed by 45 Gy postoperatively in retroperi- toneal sarcoma.
Dose Fractionation Issues in External-Beam Radiation Therapy
Radiation prescriptions have tended to follow the prevailing practice in the institute where the patient is managed. Dosages prescribed in postoperative RT depend on the tumor grade and involvement of the surgical margin, typically delivering 50 Gy to a wide field, shrinking to a final boost of 10-16 Gy. 4~ At the M.D. Anderson Cancer Center, the postoperative dose was reduced from 70 Gy for all grades to 60 Gy and 65 Gy for low-grade and high-grade tumors, with no increase in local relapse. 31 The preoperative dose used in most institutions is 50 Gy in daily fractions over approximately 5 weeks. 55,65 In this setting, a postoperative boost (10-16 Gy) is generally restricted to positive-margin cases. 53,55
Dose-response data are sparse. Fein et a174 re -
viewed 67 patients and noted a significant improve- ment in local control in those treated with doses greater than 62.5 Gy. One study with few cases reported improvement in overall sm'vival with increas- ing dose, particularly for larger tumors. This surpris- ing result may reflect case selection. 75
The fraction size used in conventional fraction- ation varies (1.8 Gy vs 2 Gy). 55'76 Sparing of late effects can be expected with smaller fraction size and is particularly important when critical structures are irradiated. Several altered fractionations have been described, including hyperfractionated 77,78 and hypo- fractionated schedules. 79 No improvement in thera-
peutic gain is evident from these various strategies over conventional R T . 49'55'56'76
Optimal Radiation Target Volume
Earlier we outlined principles concerning anatomic planes and the preferential pathways of spread of STS within tissues. In turn, this information facili- tated the design of target areas for irradiation. The basic premise in RT planning is to define a gross tumor volume (GTV) 8~ and place a margin around it to encompass tissues at risk of harboring microscopic disease (clinical target volume [CTV]).
In the preoperative setting, the GTV typically represents the radiologically defined tumor. Some sarcomas have extensive peritumor edema, which extends along fascial planes and may lie at some distance from the primary tumor. It is not known if the edema contains viable tumor cells, s The inclusion of edema within the GTV can influence the length of the treatment field considerably. Our policy is to include this area as part of the GTV (Figs 2 and 3), but this is not universally accepted. Studies correlat- ing the radiological imaging to the pathological findings are required.
Strictly speaking, in the postoperative setting, there is no GTV. For RT planning, however, we still" find it helpful to represent a putative GTV as the surgical field that includes all the tissues handled during the surgical procedure, including all scars and drain sites. A zone of potential microscopic disease beyond this comprises the CTV. Practice varies with respect to the zone at risk of harboring microscopic involvement (CTV). A small retrospective study (n = 64 cases) suggested a dramatically inferior 5-year local control of 30% when the postoperative RT radiation field margin surrounding the tumor bed and scar was less than 5 cm, compared with 93% for larger fields, m Bone, interosseous membranes, and fascial planes are considered barriers to tumor spread in the axial directions, and therefore descrip- tions of radiation margins employed are principally in the craniocaudal direction. Our policy has been to place a field margin of 5 cm around the GTV, including any peritumoral edema, regardless of grade or size of the tumor. At Massachusetts .General Hospital, the following margins are recommended: less than 5 cm for small grade 1, 5 to 10 cm for larger grade 1 and small grade 2 to 3, and 10 to 15 cm for large grade 2 to 3 sarcomas. 7s Lindberg et al31 have advocated a 5-cm and 7-cm margin for low-grade and high-grade lesions.
In contrast, the BRT protocol at MSKCC uses margins of only 2 cm around the surgical bed. 5~

Local Management of Soft Tissue Sarcoma 337
Figure 2. (A) Tl-weighted MRI scan in the sagittal view of the ankle in a patient with neurofibromatosis. A periph- eral nerve sheath tumor is seen posterior to the tibia and talus. The patient also has a large long-standing plexiform neurofibroma at the same site that is not seen on the image. (B) T2-weighted MRI scan for the same lesion as in (A). Note the extensive signal change proximal to the tumor mass consistent with peritumoral edema.
Despite these marked differences, the local control rates reported are approximately 90% if low-grade lesions are excluded from the BRT data (Table 1). This observation suggests that the zone of micro- scopic involvement may be less than previously real- ized, and studies examining this issue are required. Improvements in surgical technique may lessen the degree of intraoperative tumor dissemination, and
the need to irradiate all surgically handled tissues, scars, and drain sites may be overstated today.
Radiotherapy With Other Adjuvants
Chemotherapy. Eilber et a182 pioneered the deliv- ery of concurrent chemotherapy and RT. The intra- arterial route delivers chemotherapy more directly to the tumor and was initially favored. It is more complex, expensive, and prone to complications, however, when compared with the intravenous route. A randomized study comparing the two methods of delivery showed no difference in local control or overall failure rate (Table 1). 24 Additional ap- proaches include the use of actinomycin D and RT outlined by Abbatucci and colleagues 37 but provide results similar to approaches without chemother- apy.49,55,56,76
A European Organization for Research and Treat- ment of Cancer (EORTC) study 83 and a meta- analysis a4 have reported improved local control with adjuvant chemotherapy. The benefit in the EORTC study was greatest in those not receiving RT (about 50% of cases), and the overall local control rates achieved,are inferior to those expected using modern- day RT and surgery. The results should therefore be interpreted with caution.
Hyperthermia and radiosensitizers. Some authors have used hyperthermia as a local adjuvant treat- ment, usually in combination with RT. 85 The exact role of this approach remains experimental, and the results to date do not appear different from those achieved with conventional approaches. Gofman et a186 treated 32 patients with iododeoxynridine and aggressive twice-daily RT. Remarkably, local control was achieved in 20 patients despite 15 of 32 being 15 cm or greater. Further investigation is warranted.
Radiation Alone (Unresectable Disease) The concept of radiation alone except for some radiosensitive STS subtypes, such as embryonal rhab- domyosarcomas and soft tissue Ewing's sarcoma, is synonymous with unresectability. This situation is rare, and our recommendations for medically fit and technically operable patients is to explore combina- tion RT and surgery if possible. For example, rarely disease presents encircling the major vascular struc- tures in the proximal extremity. This situation is found most frequently with proximal inguinal or axillary tumors. Such lesions may undergo complete surgical resection and reconstruction of the involved vascular structures, usually in combination with radia- tion. Rarely, however, a patient with truly inoperable disease may require treatment with EBRT alone,

338 O'Sullivan et al
Figure 3. (A) The patient in Fig 2 on simulator for a three-dimensional treatment plan for preoperative radiotherapy created with planning computed tomography. Note the thermoplastic custom cast for immobilization with field marked on it. As much of the cast as possible will be removed later to achieve maximal skin sparing without sacrificing positioning stability. Note the wire placed at the plantar surface of the heel to facilitate shield placement for this region. There is also wire around the plexiform neurofibroma at the same site that has been present since childhood and will be treated but is not strictly part of the GTV in this case. (B) The simulation field with CTV and GTV identified. The tumor is shown as represented by the magnetic resonance imaging appearance. According to the authors' policy, the GTV is expanded to include the zone of peritumoral edema proximally [see text]. The wire around the plexiform neurofibroma is shown (long arrow), whereas a short arrow indicates the position of the wire at the heel pad. The heel pad shield (Pb) is introduced after 40 Gyofa 50 Gy course.
either with photons 87 or with particle beams. For the latter, this has included protons, neutrons, and pions. 69,88-9~ No formal clinical trials have been per-
formed to compare these strategies with each other, and they are generally adminis tered in an adverse cliriical context. Local control has been reported in 40% to 70% of cases with neutrons, aa Photons in such cases are repor ted to produce local control in approxi- mately 30% of cases. 87
Another option is isolated limb perfusion, in which the surgeon isolates the inflow and outflow vessels to the extremity, thereby establishing an extracorpo- real circulatory system for infusion of cytotoxic drugs. Melphalan and tumor necrosis factor are the most
commonly used drugs. 91 Althgugh associated with potential for severe systemic and local toxicity, tumor response is often dramatic, and limbs that might otherwise undergo amputat ion can be salvaged using this technique.
Technical Issues Concerning Radiotherapy
External-Beam Planning and Delivery Essential elements in external-beam treatment plan-
ning. High-quali ty imaging of the undisturbed lesion is pa ramount for RT t rea tment planning. MRI is superior to other imaging modalities because of its

Local Management of Soft Tissue Sarcoma 339
ability to view the tumor in multiple planes and the excellent tumor resolution depicted on T2-weighted imaging. Treatment planning primarily uses CT scanning for dosimetric reasons, but MRI can provide complementary information on the GTV extent using image fusion technology. 92,93 Further essential information is obtained from the pathology and operative reports, and metallic clips placed at the time of surgery may help define the tumor bed.
It is beneficial to immobilize the treated area if there is any chance of significant movement during treatment. Simple maneuvers, such as placing the limb in a comfortable position or use of custom molds, can help to facilitate reliable and consistent treatment setups (Fig 3A). Consideration should be given to treating superficial tissues, including the scar, with judicious use of bolus materialbut recogniz- ing that this may effect the cosmetic result. Unifor- mity of dose within irregular volumes can be en- hanced using compensators or wedge filters. Every effort should be made to avoid irradiating the entire limb circumference, whole joints, or pressure areas (eg, elbow, heel) for the whole course because this may affect future limb function, healing, and distal edema.
Before embarking on treatment in the vicinity of critical organs, it is prudent to assess baseline func- tion. For example, evaluation of the function of paired organs is advisable before treatment, such as the contralateral eye or the kidney for some head and neck and retroperitoneal tumors. This evaluation is more relevant if functional ablation of a unilateral organ by RT is expected.
Three-dimensionaltreatmentplanning. Three-dimen- sional radiation planning computer systems permit the accurate planning of homogeneous doses to the tissues at risk yet spares unnecessary irradiation of normal tissues that may affect future function and cosmes i s . 94 We find that complex anatomic plans with critical organ sparing require three-dimensional volume reconstruction and beam's eye view planning to permit adequate protection of normal tissue and inclusion of the target volume. Examples are pro- vided from the head and neck (Fig 4) and in a case of retroperitoneal sarcoma (Figs 5 and 6). Complex modulation of the beam is available in some centers with the introduction of intensity-modulated RT, 95,96 but ordinarily these are confined to plans for critical sites, such as the skull base or within the abdomen.
Dose volume histograms. One of the concerns about the treatment of sarcomas is that large volumes of normal tissue are irradiated, frequently to high doses. Because most STS arise in the limbs, vulner-
able organs, with the capacity for life-threatening sequelae from RT damage, are only rarely irradiat- edto such doses. Lesions in other sites, however, are vulnerable to the effects of high-dose RT with the potential for serious damage to neurological tissues in the head and neck (Fig 4) or intra-abdominal organs, including Iiver and small bowel, in retroperi- toneal tumors (Figs 5 and 6). It has also long been known that the tolerance of many normal tissues to radiation depends on the irradiated volume. The development of three dimensional treatment plan- ning has provided tools to quantify the relationships between dose, volume, and normal tissue complica- tions. Models have been developed that permit nor- mal tissue complication probability to be determined for different volume irradiation for organs or tissues to varying dose levels. ~7,98
We have found these concepts helpful for irradia- tion of tumors in the retroperitoneum. Such lesions, if right-sided or of great size, may infiltrate the liver capsule or be shielded by the liver, rendering access to a n appropriate CTV extremely difficult (Figs 5 and 6)': Although the tolerance of the entire liver to radiation is low, Lawrence et al, 99 using the normal tissue complication probability model, have shown that parts of the liver may be treated to much higher doses safely. We have exploited the volume effect supporting the liver's tolerance to irradiation in our preoperative protocol for retroperitoneal sarcoma and plan cases with dose volume histograms (Fig 7).
A note of caution is that subsequent liver resec- tion, which may be required because of tumor infiltra- tion or adherence to the capsule, should be per- formed only after detailed consultation between the surgical and radiation oncology teams. T h e surgeon should be consulted when the preoperative RT plan is being designed. It is also preferable if members of both teams attend the operating room jointly with the detailed dosimetry to ensure that an adequate volume of liver spared from the irradiation volume is left in situ. In cases in which residual viable liver volume after irradiation may be compromised, a segmental resection can usually be avoided. This case would employ, instead, an en bloc nonanatomic resection confined to liver directly abutting the sar- coma. Such resections can be more complicated, especially from a hemostasis standpoint, but are helpful for preservation of vital tissue and function (Fig 5A).
Brachytherapy Planning and Delivery The MSKCC approach requires the tumor bed to be evaluated intraoperatively, and the target volume is

340 O'SuUivan et al
then defined by a 2-cm margin superiorly and inferi- orly and 1.5- to 2-cm margin medially and laterally. The area is implanted with afterloading catheters placed percutaneously, spaced at approximately 1-cm increments, and sutured in place with catgut. BRT is given after the sixth postoperative day using an
iridium-192 implant delivering 42 to 45 Gy over 4 to 6 days. 1~176 Our techniques for treatment of limb sarco- mas (almost exclusively in recurrent previously irradi- ated situations) and retroperitoneal sarcoma after preoperative RT are described in greater detail elsewhere in this issue in the article by Carton et al.

Local Management of Soft Tissue Sarcoma 341
We have used a pulse dose rate afterloading system for these indications.
Functional Outcome and Morbidity of Treatment of Extremity Soft Tissue Sarcoma
Functional Assessment
The functional result of extremity sarcoma manage- ment has become a new frontier for outcome assess- ment for these patients. This assessment is difficult because it requires instruments that are valid and reproducible. Many centers have yet to become experienced in the development and use of these methods. Thus far, the variables associated with poorer functional outcome include large tumor size, higher doses of radiation doses and larger volumes, nerve sacrifice, postoperative fractures, and wound healing complication. 64,1~176 To evaluate and com- pare functional outcome, it is imperative that func- tional data be reported consistently. Three disease- specific scoring scales have been reported as useful in assessing STS outcome. 1~ This area is discussed more completely in the article by Davis.
Wound Complications
Wound healing complications have been recognized in 40% of patients undergoing extremity sarcoma surgery. 78,1~176 The variability in reported risk prob- ably relates, at least in part, to differences in the definition of what constitutes wound complications. The factors associated with compromised wound healing include patient age and nutritional status, lower extremity location, and large tumor size as well as preoperative adjuvant treatment. ~~ Most au- thors have found adjuvant treatment (especially preoperative RT) to be a significant factor, but others have reported high rates of surgical complications without radiation or chemotherapy, likely~0nfirming
the risk associated with extensive tumor resection in the extremities. H3 The use of vascularized tissue transfers has been suggested as a method that may decrease the risk of wound healing complica- tions.109,114,115
As described earlier, the SR2 trial will address a number of the issues surrounding functional out- come and treatment morbidity related to RT. The contribution of tissue transfer for wound recon- struction is unlikely to be resolved by SR2, how- ever, because its use in the trial was determined on an individual basis at the surgeon's discretion. Hence, it is suitable only for secondary exploratory analysis .22
Special Situations
Retroperitoneal Sarcoma
Retroperitoneal sarcomas comprise about 15% of.. STS. They present late and are located in regions where the administration of both surgery and RT is often compromised (eg, adjacent to small bowel and liver). Consequently the local control rates of extrem- ity STS with combined modality treatment are not seen in RPS. In a series of 104 RPS patients treated at Princess Margaret Hospital, complete excision was achieved in only 45, macroscopic disease remained in 29, and only a biopsy was possible in 28. The overall locoregional relapse-free rate was 28% and 9% at 5 and 10 years. RT did not improve survival but appeared to lengthen significantly the time to locore- gional relapse, especially with higher doses. Com- plete tumor resection was the only significant prog- nostic variable for survival, locoregional failure, and distant failure, u6 These results are similar to those reported from MSKCC.117
Retroperitoneal sarcoma should be evaluated be- fore resection in a multidisciplinary clinic with access to specific surgical opinion, which may permit newer approaches to be developed. For example, Willett
Figure 4. (A) Coronal view MRI scan of a sarcoma of the base of the skull showing the parietal bone changes in a patient referred after an unsuccessful attempt at resection. The surgical changes of prior craniotomy in the parietal skull and scalp are evident. Disease extension in the infratemporal fossa is evident. The posterior bony orbit was invaded, but no invasion of orbital contents was present. (B) Three-dimensional frontal view depiction of the intended clinical target volume (CTV) to cover the unresected tumor and postoperative changes of prior surgery for preoperative radiotherapy. The extensive CTV includes the temporal and parietal scalp and calvaria superiorly to the infratemporal fossa at the midline inferiorly. Wire frame depicts the surface contour beneath which can be seen the brain and spinal cord. (C) The treatment plan is shown for four static beams with shielding designed to conform the volume for the case in (A) and (B). This is an apical view and illustrates gross tumor volume and CTV. One high-energy (18 MV) photon beam enters the left eye anteriorly to ensure safe coverage of the posterior orbit and exploits the build-up region of the high-energy photons to spare the anterior chamber and cornea from morbidity. The other three beams have shielding of the left eye throughout the course. Bolus is shown overlying the area of previous surgical incision. This patient underwent resection with preservation of orbital contents and reconstruction and remains disease-free with normal ocular function 2 years later.

342 O'SuUivan et al
et a1118 described 20 patients treated with preopera- tive RT, resection, and then intraoperative EBRT and reported a 70% complete resection rate and 81% 4-year local relapse-free rate. We prefer the preopera- tive approach because (1) the tumor bulk often displaces dose-limiting small bowel from the high- dose region, (2) bowel is unlikely to be fixed by surgical adhesions characteristic of the postoperative setting, (3) optimal knowledge of the gross tumor
Figure 5. (A and B) Plan- ning computed tomography scan of a patient with massive retroperitoneal liposarcoma presenting for the first time. The gross tumor volume (GTV) and clinical target vol- ume are outlined on both slices for a course of preoperative radiotherapy. The magnitude of the disease is appreciated on the lower of the two slices (B). The higher slice (A) shows that disease (GTV) is nestled in behind and below the liver where it was adherent to the liver capsule.
location is possible, and (4) the risk ofintraperi toneal tumor dissemination at the time of the operation may be reduced after RT pretreatment . After resec- tion, BRT catheters are placed for additional dose augmentat ion at sites of highest risk. The technique is described elsewhere in this issue (see the article by Cat ton et al). This strategy remains to be evaluated but is used in a prospective protocol with informed consent at Princess Margaret Hospital because of the
Local Management of Soft Tissue Sarcoma 343
disappointing results of the treatment of retroperito- heal sarcoma with current approaches.
Other approaches have used intraoperative RT or postoperative BRT boosts to the tumor bed. As noted earlier, intraoperative RT (20 Gy followed by 35 to 40 Gy postoperatively) was compared with conventional postoperative RT (50 to 55 Gy) in a randomized study of 35 patients (Table 1). The incidence of locoregional recurrences was lower in the experimen-
tal treatment arm, but no survival benefit was demon- strated. 23
Head and Neck Sarcoma
For head and neck STS, high rates of local relapse are reported by numerous institutions. 119-124 Surgical ex- cision is often constrained by anatomic consider- ations. The proximity of dose-limiting structures also limits the administration of high-dose RT. Neverthe- less, advantages to a combined modality approach have been shown in a series in which local control was 52% in those treated with surgery alone versus 90% in those treated with combined RT and surgeryJ 22 Preoperative RT is particularly suited to this site because of the dividend to be gained from smaller volume and lower doses to critical anatomy in diffi- cult surgical access locations (Table 2). Flaps are also commonly used in the reconstruction, and it is our impression that wound healing problems do not occur with the frequency evident with preoperative RT in extremity lesions. This situation may be explained by the better vascularity in the head and neck compared with the lower extremity especially; in addition, the volume defect after surgery in the head and neck is more amenable to obliteration with vascularized tissue transfer than in the extremity, where resection volumes tend to be larger and sometimes beyond the scope of available free flaps.
Breast Sarcomas
Breast sarcomas should be managed according to the same principles used in the trunk and extremities. The primary treatment is wide encompassing exci- sion with negative margins. Lymph node dissection is not required because of the rarity of lymph node metastasis. RT is an effective adjuvant modality, and the prognosis is similar to extremity sarcomas. 125 There is no reason why the winciples of conservation
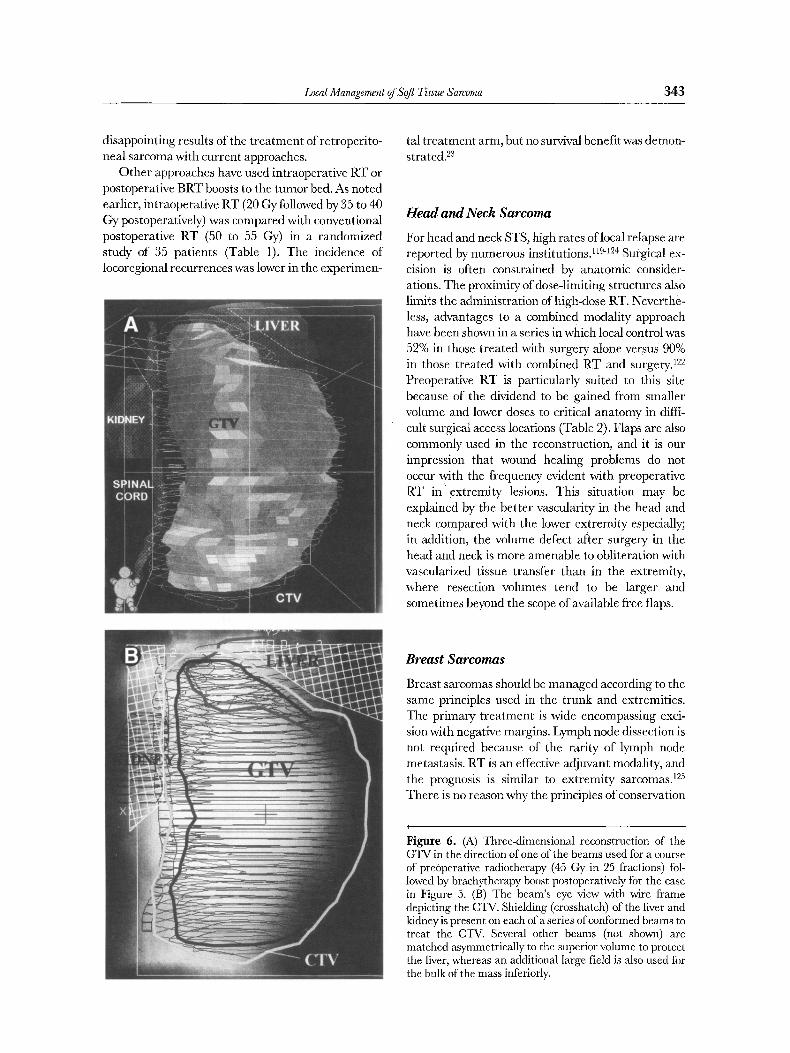
Figure 6. (A) Three-dimensional reconstruction of the GTV in the direction of one of the beams used for a course of preoperative radiotherapy (45 Gy in 25 fractions) fol- lowed by brachytherapy boost postoperatively for the case in Figure 5. (B) The beam's eye view with wire frame depicting the CTV. Shielding (crosshatch) of the liver and kidney is present on each of a series of conformed beams to treat the CTV. Several other beams (not shown) are matched asymmetrically to the superior volume to protect the liver, whereas an additional large field is also used for the bulk of the mass inferiorly.

344 O'Sullivan et al
9 5
9 G I .
85"
75'
78.
gS.
68"
55.
58-
! - 45-
o,e 4 8
35.
38-
25.
28-
15-
1 8
5-
16 VQlume (c;c) : 1783 Gy oT'escr . : 4 5 , 8
15 ~1~, ~ do~e : 2 2 0 . 0 C a l c . VQI , ( ~ ) : 188.8
Dose (Gy) : 14
- m l n : 1 . 9
- m a x : 5 1 . [
13 - m e a n : 2 8 . 4
- medlan : 25,8
12 - ~da l : r L - S . D e v ( ~ ) : G4.3
8 18 2 8 3 0 4 8 5 0 6 8 7 8 8 8 9 8 1 f l S l i S 1 2 8 1 3 8 | 4 0 1 5 8 1 f i O 1 7 8 1 8 8 1 9 8 2 8 8 2 t 8 2 2 8 2 3 8 : : ' 4 8 2 5 8 Dose (~-)
17
16
15
14
13
12
11
92 n
8 -
?
6
5
4
3
2
I
fl
Figure 7. Dose volume histogram (DVH) for the liver for the case in Figures 5 and 6. A total dose of 45 Gy in 25 fractions was administered followed by brachytherapy. The DVtt shows that 50% of the total liver volume received a dose of 24 Gy or less fractionated over 5 weeks. This dose level is within the tolerances described by Lawrence et al. 99 The patient tolerated the combined modality protocol without manifesting radiation hepatitis or other significant adverse sequelae.
with combined modality approaches cannot be ex- tended to breast conservation in appropriate cases.
Visceral Lesions
STS arising within the coelomic cavities is difficuh to manage. 126 Frequently presenting with obstructive symptoms, they may be managed with urgent sur- gery, and the preoperative staging workup may be incomplete. Resection of various intra-abdominal, pelvic, and retroperitoneal organs may be needed to obtain grossly clear margins. In some instances, resection of major vessels may be needed. As indi- cated earlier, RT is normally unrealistic because of the mobility of visceral STS, especially those arising from small bowel, where the position changes readily throughout the day. Moreover the dose is often compromised by organ tolerance, especially small bowel. There are no good data from which to draw strong conclusions about treatment.
Uterine sarcomas have a high recurrence rate after surgerybut have the benefit that the anatomy is relatively fixed in the peMs and would make RT
feasible. In the Gynecological Oncology Group study that examined the effectiveness of adjuvant chemo- therapy in stage I and II, the.use of RT in the protocol was optional.127,~28 A review of those treated with and without radiation therapy showed no difference in survival or site of first recurrence in leiomyosaroma histology, but those with uterine mixed mesodermal sarcomas experienced a statistically significant reduc- tion in pelvic recurrence from the use of adjuvant RT. 128 The conclusions must'be tentative because of the nonrandom selection of patients and the differ- ent RT approaches used. 12a Currently, results of a phase 11I study by the EORTC are awaited. This studywas activated in 1988 and accrued slowly. It was designed to evaluate the role of adjuvant RT in stage I and II uterine sarcoma.
Unplanned Excision
About one third of new patients referred to a special- ized center have undergone an unplanned excision9 Typically, imaging was not performed before surgew, and the sarcoma specialist evaluating the patient

Local Management of Soft Tissue Sarcoma 345
often has difficulty in deciding the exact site of tumor origin. This situation differs from the positive micro- scopic resection margin after a planned at tempt at complete resection. In the unplanned resection, there is likely to be a substantial amount of residual tumor in the wound, although this is rarely detectable by CT or MRI. Microscopic evaluation of the wound
reveals residual sarcoma in 40% to 80% of cases2 ~ In patients treated at Princess Margaret Hospital with RT alone after unplanned resection, 50% of patients sustained a local recurrenceY
The best t reatment for unplanned resection is to prevent its occurrence. All soft tissue masses deep to fascia should undergo radiographic staging and bi- opsy before removal. If the patient is referred after unplanned excision, the patient should undergo re- excision of the tumor bed. The surgical oncologist should first discuss the prior surgical approach and the potentially contaminated structures with the surgeon who performed the original excision. Mll I studies should also be obtained before surgery to show the footprint left behind by the initial surgery. If possible without sacrificing critical structures, all of this contaminated tissue should be removed. The decision whether or not to recommend postoperative (or preoperative) radiation is difficult. If microscopic evidence of sarcoma is identified in the re-excision specimen, we generally recommend RT, unless par- ticularly wide surgery has been undertaken. Sarcoma can be spread at considerable distance into the surrounding soft tissues by an unplanned resection, and it is often difficult to be sure that all contami- nated tissue has been excised.
Conclusion
The local growth pat tern of STS as well as the potential for local control of disease by surgery and radiation is highly dependent on the local site of origin. Improvement in radiographic imaging and surgical techniques as well as recognition that radia- tion is a useful adjuvant t reatment for STS has resulted in marked improvement in local STS control in extremity and truncal STS. Optimization of ap- proach will likely focus in the future on the results of ongoing studies of functional outcome and complica- tions in addition to maintaining the present high rates of local control. At other anatomic sites, there is considerably less success in achieving wide surgical margins, and the radiosensitivity of surrounding critical structures limits the use of RT. The clinical outcome of patients with abdominal or head and neck STS is therefore often determined by failure of
local cancer control. It would seem reasonable that such cases be referred to multidisciplinary sarcoma programs with integrated anatomic expertise in all specialties treating these patients where a consistent approach to management and access to clinical trials may be available.
References
1. Polio& R, Karnell L, Menck H, et al: The National Cancer Data Base report on soft tissue sarcoma. Cancer 78:2247- 2257, 1996
2. Browman GP, Levine MN, Mohide EA, et al: The practice guidelines development cycle: A conceptual tool for practice guidelines development and implementation. J Clin Oncoi 13:502-512, 1995
3. Rydholm A: Centralization of soft tissue sarcoma: The southern Sweden experience. Acta Orthop Scand 273 (suppl): 4-8, 1997
4. Rydholm A: Improving the management of soft tissue sar- coma: Diagnosis and treatment should be given in specialist centres. BMJ 317:93-94, 1998 (editorial)
5. Gustafson P, Dreinhover KE, Rydholm A: Soft tissue sar- coma should be treated at a tumor center: A comparison of quality of surgery in 375 patients. Acta Orthop Scand 65:47-50, 1994
6. Clasby"R, Tilling K, Smith MA, et al: Variable management of soft tissue sarcoma. BrJ Surg 84:1692-1696, 1997
7. Jane MJ, Hughes PJ: Disease incidence and results of extremity lesion treatment: Mersey Region soft tissue sarco- mas (1975-1985). Sarcoma 2:89-96, 1998
8. Manaster BJ: Musculoskeletal oncologic imaging. Int J Ra- diat Oncoi Biol Phys 21:1643-1651, 1991
9. Kuszyk BS, Ney DR, Fishman EK: The current state of the art in three dimensional oncologic imaging: An ovmMew. Int J Radiat Oncol Biol Phys 33:1029-1039, 1995 Panicek DM, Gatsonis C, Rosenthal DI, et al: CT and MR imaging in the local staging of primary malignant musculo- skeletal neoplasms: Report of the Radiology Diagnostic Oncology Group. Radiology 202:237-246, 1997 Panicek DM, Go SD, HealeyJH, et al: Soft-tissue sarcoma involving bone or neurovascular structures: MR imaging prognostic factors. Radiology 205:871-875, 1997 Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited: Members of the Musculoskeletal Tumor Society (see comments). J Bone Joint Surg Am 78:656-663, 1996 Akerman M: Fine-needle aspiration cytology of soft tissue sarcoma: Benefits and limitations. Sarcoma 2:155, 1998 Bennert KW, Abdul-Karim FW: Fine needle aspiration cytology vs. needle core biopsy of soft tissue tumors: A comparison. Acta Cyto138:381-384, 1994 Costa MJ, Campman SC, Davis RL, et al: Fine-needle aspiration cytology of sarcoma: Retrospective review of diag- nostic utility and specificity. Diagn Cytopathol 15:23-32, 1996 Heslin MJ, LewisJJ, WoodruffJM, et ai: Core needle biopsy for diagnosis of extremity soft tissue sarcoma. Ann Surg Oncol 4:425-431, 1997 Ball AB, Fisher C, Pittam M, et al: Diagnosis of soft tissue tumours by Tru-Cut biopsy. BrJ Surg 77:756-758, 1990 Kissin MW, Fisher C, Carter RL, et al: Value of Tru-cut
10.
11.
12.
13.
14.
15.
16.
17.
18.

346 O'Sullivan et al
biopsy in the diagnosis of soft tissue mmours. Br J Surg 73:742-744, 1986
19. Serpell JW, Fish SH, Fisher C, et al: The diagnosis of soft tissue tumours. Ann R Coil Surg Eng174:277-280, 1992
20. Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity (see comments).J Bone Joint Surg Am 78:650-655 , 1996
21. Davis AM, Kandel RA, Wunder JS, et al: The impact of residual disease on local recurrence in patients treated by initial unplanned resection for soft tissue sarcoma of the extremity.J Surg Onco166:81-87, [997
22. O'Sullivan B, Davis A, Bell R. et al: Phase III randomized trial of pre-operative versus p0st-operative radiotherapy in the curative management of extremity soft issue sarcoma: A Canadian Sarcoma Group and NCI Canada Clinical Trials Group study. Proc Am Soc Clin Oncol 18:534a, 1999
23. Sindelar WF, Kinsella TJ, Chen PW, et al: [ntraoperative radiotherapy in retroperitoneal sarcomas: Final results of a prospective, randomized, clinical trial. Arch Surg 128:402- 410, 1993
24. Eilber FR Giutiano AE. HuthJF, et al: Intravenous (IV) vs. intraarterial (IA) Adriamycin, 2800r radiation and surgical excision for extremity soft tissue sarcomas: A randomized prospective trial. Proc Am Soc Clin Oncol 9:309. 1990 (abstract)
25. Shiu MIt, Castro EB, Hajdu SI, et al: Surgical treaunent of 297 soft nssue sarcomas of the lower extremity. Ann Snrg 182:597-602, 1975
26. Abbas JH, Holyoke ED, Moore R. et al: The surgical treat- ment and outcome of soft-tissue sarcoma. Arch Surg 116:765- 769. 1981
27. Suit HD, Russell WO: Radiation therapy of soft tissue sarcomas. Cancer 36:759-764, 1975
28. Rosenberg SA, TepperJ, Glatstein E, et al: The treatment of soft-tissue sarcomas of the extremities: Prospecnve random- ized evaluations of (1) limb-sparing surgery plus radiation therapy compared with amputation and (2) the 'role of adjuvant chemotherapy. Ann Surg i96:305-315, 1982
29. Hintz BL, Charyulu KK, Miller WE. et al: Adjuvant role of radiation in soft tissue sarcoma in adults. J Surg Oncol 9:329-338, 1977
30. Eilber FR, MirraJJ, Grant TT, et al: Is amputation necessary for sarcomas? Ann Surg 192:431-437, 1980
31. Lindberg RD, Martin RG, Romsdahl MM, et al: Conserva- tive surgery and postoperative radiotherapy in 300 adults with soft-tissue sarcomas. Cancer 47:2391-2397, 1981
32. Suit HI), Proppe KH, Mankin HJ, et al: Preoperative radia- tion therapy for sarcoma of soft tissue. Cancer 47:2269-2274, 1981
33. Carabell SC, Goodman RL: Radiation therapy for soft tissue sarcoma. Semin Onr 8:201-206, 1981
34. Coe MA, Madden FJ, Mould RF: The role of radiotherapy in the treatment of soft tissue sarcoma: a retrospective study 1958-73. Clin Radio132:47-51, 1981
35. Leibel SA, Tranbaugh RF, Wara WM, et al: Soft tissue sarcomas of the extremities: survival and patterns of failure with conservative surgery and postoperative irradiation com- pared to surgery alone. Cancer 50:1076-1083, 1982
36. Mansson E, Willems J, Aparisi T, et al: Preoperative radia- tion therapy of high malignancy grade soft tissue sarcoma: A preliminary investigation. Acta Radiol Oncol 22:461-464, 1983
37. AbbatucciJS, Boulier N, de RanieriJ, et al: Radiotherapy as
an integrated part of the treatment of soft tissue sarcomas. Radiother Oncol 2:115-121, 1984
38. Moskowitz AJ, Pauker SG: A decision analytic approach to limb-sparing treatment for adult soft tissue and osteogenic sarcoma. Cancer Treat Symp 3:11-26. 1985
39. National Institutes of Health Consensus Development Panel on limb-sparing treatment of adult soft tissue sarcomas and osteosarcomas: Conclusion. Cancer Treat Symp 3:1-5, 1985
40. Williard WC, Hajdu SI, Casper ES, et al: Comparison of amputation with limb-sparing operations for adult soft tissue sarcoma of the extremity (see comments/. Ann Surg 215:269- 275, 1992
41. Williard WC, Collin C, Casper ES, et al: The changing role of amputation for soft tissue sarcoma of the extremity in adults. Surg Gynecol Obstet 175:389-396, 1992
42. Le Vay J, O'Sullivan B, Catton C, et al: Outcome and prognostic factors in soft tissue sarcoma in the adult. Int J Radiat Oncol Biol Phys 27:1091-1099, 1993
43. Colterjohn NR. Davis AM. O'Sullivan B, et al: Functional outcome in limb-salvage surgery for soft tissue tumours of the foot and ankle. Sarcoma 1:67-74, 1997
44. Karakousis C, Emrich L, Rao U, et al: Limb salvage in soft tissue sarcomas with selective combination ofmodalities. Eur
J Surg Onco117:71-80, 1991 45. Geer RJ, WoodruffJ, Casper ES. et al: Management of small
soft-tissue sarcoma of the extremity in adults Arch Surg 127:1285-1289, 1992
46. Rydholm A, Gustafson P, Rooser B. et al: Subcutaneous sarcoma: A population-based study of 129 patients. J Bone Joint Surg Br 73:662-667, 1991
47. Stotter A, Fallowfield M, Mott A, et al: Role of compartmen~ tal resection for soft tissue sarcoma of the limb and limb girdle. BrJ Surg 77:88-92, 1990
48. Gibbs CP, Peabody TD. Mundt AJ, et al: Oncological out- comes of operative treatment of subcutaneous soft-tissue sarcomas of the extremines. J Bone Joint Surg Am 79:888- 897, 1997
49. YangJC, Chang AE, Baker AR, et al: Randomized prospec- tive study of the benefit of adjuvant radiation therapy in the treatment of soft tissue sarc6mas of the extremity. J Clin Oncol 16:197-203, 1998
50. Pisters PW, Harrison LB, Leung DH, et al: Long-term results of a prospective randomized trial of adjuvant brachytherapy in soft tissue sareoma.J Clin Oncol 14:859-868, i996
51. Simon MA, Enneking WF: The management of soft-tissue sarcomas of the extremities. J Bone Joint Surg Am 58:317- 327, 1976
52. Enneking WF, Spanier SS, Goodman MA: Current concepts review: The surgical staging of musculoskeletal sarcoma. J Bone Joint SurgAm 62:1027-1030, 1980
53. Sadoski C, Suit HD, Rosenberg A, et al: Preoperative radia- tion, surgical margins, and local control of extremity sarco- mas of soft tissues.J Surg Onco152:223-230, 1993
54. Tanabe KK, Pollock RE, Ellis LM, et al: Influence of surgical margins on outcome in patients with preoper~ifively irradi- ated extremity soft tissue sarcomas. Cancer 73:1652-1659, 1994
55. Wilson AN, Davis A, Bell RS, et al: Local control of soft tissue sarcoma of the extremity: The experience of a multidisci- plinary sarcoma group with definitive surgery and radio- therapy. EurJ Cancer 30A:746-751, 1994
56. Pister PWT, Leung DHY, Woodruff J, et al: Analysis of prognostic factors in 1041 patients with localized soft tissue sarcomas of the extremities.J Clin Onco114:1679-1689, 1996

Local Management of Soft Tissue Sarcoma 3 4 7
57. Belt RS, O'Sullivan B, Liu FF, et al: The surgical margin in soft-tissue sarcoma (see comments). J Bone Joint Surg Am 71:370-375, 1989
58. Ruka W, Taghian A, Gioioso D, et al: Comparison between the in vitro intrinsic radiation sensitivity of human soft tissue sarcoma and breast cancer cell lines. J Surg Oncol 6t:290- 294, 1996
59. Weichselbaum RR, Beckett MA, Simon MA, et al: In vm-o radiobiological parameters of human sarcoma cell lines. IntJ Radiat Oncol Biol Phys 15:937-942, 1988
60. Tyldesley S, Fryer K, Minchinton A, et at: Effects of debulk- lng surgery on radiosensitivity, oxygen tension and kinetics in a mouse tumour model. Clin Invest Med 20(suppl):S83, 1997 (abstract)
61 Suit HI), Mankin HJ, Wood WC, et al: Preoperative, intraop- erative, and postoperative radiation in the treatment of primary soft tissue sarcoma. Cancer 55:2659-2667, 1985
62. Nielsen OS, Cummings B, O'Sullivan B, et al: Preoperative and postoperative irradiation of soft tissue sarcomas: Effect of radiation field size. Int J Radiat Oncol Biol Phys 21:1595- 1599, 1991
63. Robinson MH, Spruce L, Eeles R, et al: Limb function following conservation treatment of adult soft tissue sar- coma. EurJ Cancer 27:1567-1574, 1991
64. Stinson SF, DeLaney TI c, Greenberg J, et al: Acute and long-term effects on limb function of combined modality limb sparing therapy for extremity soft tissue sarcoma. In tJ Radiat Oncol Biol Phys 21:1493-1499, 1991
65. Pollack A, Zagars GK, Goswitz MS, et al: Preoperative vs. postoperative radiotherapy in the treatment of soft tissue sarcomas: A matter of presentation. Int J Radiat Oncol Biol Phys 42:563-572, 1998
66. Suit HD, Mankin HJ, Wood WC, et al: Treatment of the patient with stage M0 soft tissue sarcoma. J Clin Oncol 6:854-862, 1988
67. Janjan NA, Yasko AW, Reece GP, et al: Comparison of charges related to radiotherapy for soft-tissue sarcomas treated by preoperative external-beam irradiation versus interstitial implantation. Ann Surg Oncol 1:415-422, 1994
68. Pisters PW, Harrison LB, WoodruffJM, et al: A prospective randomized trial of adjuvant brachytherapy in the manage- ment of low-grade soft tissue sarcomas of the extremity and superficial trunk.J Clin Oncol 12:1150-1155, 1994
69. Isacsson U, Hagberg H, Johansson KA, et al: Potential advantages of protons over conventional radiation beams for paraspinal tumours. Radiother Onco145:63-70, 1997
70. Dubois JB, Debrigode C, Hay M, et al: Intra-operative radiotherapy in soft tissue sarcomas. Radiother Onco134:160- 163, 1995
71. Haddock MG, Petersen IA, Pritchard D, et al: IORT in the management of extremity and limb girdle soft tissue sarco- mas. Front Radiat Ther Onco131:151-152, 1997
72. Brennan MF, Casper ES, Harrison LB: Soft tissue sarcoma, in de Vita V, Helman S, Rosenberg S (eds): Cancer: Prin- ciples and Practice of Oncology. Philadelphia, PA, Lippincott- Raven, 1997, pp 1738-1788
73. Suit H, Spiro I: Preoperative radiation therapy for patients with sarcoma of the soft tissues. Cancer Treat Res 67:99-105, 1993
74. Fein DA, Lee WR, Lanciano RM, et al: Management of extremity soft tissue sarcomas with limb-sparing surgery and postoperative irradiation: Do total dose, overall treatment time ~, and the surgery-radiotherapy interval impact on local control? IntJ Radiat Oncol Biol Phys 32:969-976, 1995
75. Wolfson AH, Benedetto PW, Mnaymneh W, et al: Does a radiation dose-response relation exist concerning survival of patients who have soft-tissue sarcomas of the extremities? Radiation dose-response relation for soft-tissue sarcomas. AmJ Clin Onco121:270-274. 1998
76. Suit HD, Spiro I: Role of radiation in the management of adult patients with sarcoma of soft tissue. Semin Surg Oncol 10:347-356, 1994
77. Robinson M, CassoniA, Harmer C. et al: High dose hyperfrac- tionated radiotherapy in the treatment of extremity soft tissue sarcomas. Radiother Onco122:118-126, 1991
78. Brant TA~ Parsons JT, Marcus RB, et al: Preoperative irradiation for soft tissue sarcomas of the trunk and extremi- ues in adults. IntJ Radiat Oncol Biol Phys 19:899-906, 1990
79. Ashby MA, Ago CT, Harmer CL: Hypofractionated radio- therapy for sarcomas. IntJ Radiat Oncol Biol Phys 12:13-17, 1986
80. ICRU 50: Prescribing, Recording, and Reporting Photon Beam Therapy. Bethesda, MD, International Commission on Radiation Units and Measurement, I993
81. Mundt AJ, Awan A, Sibley GS. et al: Conservative surgery and adjuvant radiation therapy in the management of adult soft tissue sarcoma of the extremities: Clinical and radiobio- logical results. IntJ Radiat Oncol Biol Phys 32:977-985, 1995
82. Eilber F, EckardtJ, Rosen G, et al: Preoperative therapy for soft tissue sarcoma. Hematol Oncol Clin North Am 9:817- 823, 1995
83. Bramwell V, RouesseJ, Steward W, et al: Adjuvant CYVADIC chemotherapy for adult soft tissue sarcoma--reduced local recurrence but no improvement in survival: A study of the European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group.J Clin Oncol 12:1137-1149, 1994
84. Sarcoma Meta-analysis Collaboration investigators: Adju- vant chemotherapy for localised resectable soft-tissue sar- coma of adults: Meta-analysis of individual data. Lancet 350:1647-1654, 1997
85. Brizel DM, Scully SP, HarrelsonJM, et al: Radiation therapy and hyperthermia improve the oxygenation of human soft tissue sarcomas. Cancer Res 56:5347-5350, 1996
86. Gofman T, Tochner Z, Glatstein E: Primary treatment of large and massive adult sarcomas with iododeoxyuridine and aggressive hyperfractionated irradiation. Cancer 67:572-576, 1991
87. TepperJE, Suit HD: Radiation therapy alone for sarcoma of soft tissue. Cancer 56:475-479, 1985
88. Pickering DG, Stewart JS, Rampling R, et al: Fast neutron therapy for soft tissue sarcoma. IntJ Radiat Oncol Biol Phys 13:1489-1495, 1987
89. Slater JD, McNeese MD, Peters LJ: Radiation therapy for unresectable soft tissue sarcomas. Int J Radiat Oncol Biol Phys 12:1729-1734, 1986
90. Greiner RH, Blattmann HJ, Thum P, et al: Dynamic pion irradiation of unresectable soft tissue sarcomas. In tJ Radiat Oncol Biol Phys 17:1077-1083, 1989
91. Eggermont AM, Schraffordt Koops H, Klausner JM, et al: Isolated limb perfusion with tumor necrosis factor and melphalan for limb salvage in 186 patients with locally advanced soft tissue extremity sarcomas: The cumulative multicenter European experience. Ann Surg 224:756-765, 1996
92. Austin-Seymour M, Chert GT, RosenmanJ, et al: Tumor and target delineation: Current research and future challenges. IntJ Radiat Oncol Biol Phys 33:1041-1052, 1995

3 4 8 O'SuUivan et al
93. Kessler M, Pitluck S, Petti P, et ah Integration of muitimodal- ity imaging data for radiotherapy treatment planning. Int J Radiat Oncol Biol Phys 21:1653-1667, 1991
94. Robinson Mtt, Bidmead AM, Harmer CL: Value of confor- mal planning in the radiotherapy of soft tissue sarcoma. Clin Oncol (R Coll Radiol) 4:290-293, 1992
95. Fraass BA, Kessler ML, McShan DL, et al; Optimization and clinical use of multisegment intensity-modulated radiation therapy for high,dose conformal therapy. Semin Radiat Oncol 9:60-77, 1999
96. Boyer AL, Yu CX: Intensity-modulated radiation therapy with dynamic multileaf collimators. Semin Radiat Oncol 9:48-59, 1999
97. Burman C, Kutcher GJ, Emani B, et ah Fitting of normal tissue tolerance data to an analytic function. Int J Radiat Oncol Biol Phys 21:123-135, 1991
98. Kutcher GJ, Burman C, Brewster L, et ah Histogram reduction method for calculating complication probabilities for three-dimensional treatment planning evaluations. In tJ Radiat Oncol Biol Phys 21:137-146, 1991
99. Lawrence TS, Haken RKT, Kessler ML, et al: The use of 3-D dose volume analysis to predict radiation hepatitis. Int J Radiat Oncol Biol Phys 23:781-788, 1991
100. Harrison LB; Franzese F, GaynorJJ, et al: Long-term results of a prospective randomized trial of adjuvant brachytherapy in the management of completely resected soft tissue sarco- mas of the extremity and superficial trunk. Int J Radiat Oncol Biol Phys 27:259-265, 1993
101. Pitcher ME, Thomas JM: Functional compartmental resec- tion for soft tissue sarcomas. EurJ Surg Oncol 20:441-445, !994
102. Karasek K, Constine LS, Rosier R: Sarcoma therapy: Func- tional outcome and relationship to treatment parameters. IntJ Radiat Oncol Biol Phys 24:651-656, 1992
103. Bell RS, O'Sullivan B, Davis A, et ah Functional outcome in patients treated with surgery and irradiation for soft tissue tumours.J Surg Oncol 48:224-231,1991
104. Davis AM, Bell RS, Badley EM, et ah Evaluating functional outcome in patients with lower extremity sarcoma. Clin Orthop 358:90-100, 1999
105. SkibberJM, Lotze MT, Seipp CA, et ah Limb-sparing surgery for soft tissue sarcomas: Wound related morbidity in patients undergoing wide local excision. Surgery 102:447-452, 1987
106. Ormsby MV, Hilaris BS, Nori D, et ah Wound complications of adjuvant radiation therapy in patients with soft-tissue sarcomas. Ann Surg 210:93-99, 1989
107. Schray MF, Martinez A, Howes AE: Toxicity of open-field whole abdominal irradiation as primary postoperative treat- ment in gynecologic malignancy. IntJ Radiat Oncol Biol Phys 16:397-403, 1989
108. Arbeit JM, Hilaris BS, Brennan MF: Wound complications in the multimodality treatment of extremity and superficial truncal sarcomas.J Clin Oncol 5:480-488, 1987
109. Peat BG, Bell RS, Davis A, et al: Wound-healing complica- tions after soft-tissue sarcoma surgery. Plast Reconstr Surg 93:980-987, 1994
110. Chmell MJ, Schwartz HS: Analysis of variables affecting wound healing after musculoskeletal sarcoma resections. J Surg Oncol 61:185-189,1996
111. Bujko t~ Suit HD, Springfield DS, et ah Wound healing after preoperative radiation for sarcoma of soft tissues. Surg Gynecol Obstet 176:124-134, 1993
112. Cheng EY: Lower extremity amputation level: Selection using noninvasive hemodynamic methods of evaluation. Arch Phys Med Rehabi163:475-479, 1982 Saddegh MK, Bauer HC: Wound complication in surgery of soft tissue sarcoma: Analysis of 103 consecutive patients managed without adjuvant therapy. Clin Orthop 289:247- 253, 1993
114. Bell RS, Mah'oney J, O'Sullivan B, et ah Wound healing complications in soft tissue sarcoma management: Compari- son of three treatment protocols. J Surg Oncol 46:190-197, 1991 Barwick WJ, Goldberg JA, Scully SP, et al: Vascularized tissue transfer for closure of irradiated wounds after soft tissue sarcoma resection. Ann Surg 216:591-595, 1992 Catton CN, O'Sullivan B, Kotwall C, et ah Outcome and prognosis in retroperitoneal soft tissue sarcoma. IntJ Radiat Oncol Biol Phys 29:1005-1010, 1994
117. Heslin MJ, Lewis JJ, Nadler E, et al: Prognostic factors associated with long term survival for retroperitoneal sar- coma: Implications for management.J Clin Oncol 15:2832- 2839, 1997
118. Willett CG, Suit HD, Tepper JE, et ah Intraoperative electron beam radiation therapy for retroperitoneal soft tissue sarcoma. Cancer 68(2):278-283, 1991
119. Le VayJ, O'Sullivan B, Catton C, et ah An assessment of prognostic factors in soft-tissue sarcoma of the head and neck. Arch Otolaryngol Head Neck Surg 120:981-986, 1994
120. Le QT, Fu KK, I~-oll S, et ah Prognostic factors in adult. soft-tissue sarcomas of the head and neck. Int J Radiat Oncol Biol Phys 37:975-984, 1997
1211 Mark RJ, Tran LM, Sercarz J, et ah Angiosarcoma of the head and neck: The UCLA experience 1955 through 1990. Arch Otolaryngol Head Neck Surg 119:973-978, 1993
122. Tran LM, Mark R, Meier R, et al: Sarcomas of the head and neck. Cancer 70:169-177, 1992
123. Willers H, Hug EB, Spiro IJ, et al: [Soft tissue sarcoma of the head and neck area in adults: Outcome of combined surgm 7 and irradiation and radiotherapy alone]. Strahlenther Onkol 173:131-135, 1997
124. Kraus DH, Dubner S, Harrison LB, et ah Prognostic factors for recurrence and survival in head and neck soft tissue sarcomas. Cancer 74:697-702, 1994
125. Johnstone PA, Pierce LJ, Merino MJ, et ah Primary soft tissue sarcomas of the breast: Local-regional control with post- operative radiotherapy. IntJ Radiat Oncol Biol Phys 27:671- 675, 1993
t26. CrosbyJ, Carton C, Davis A, et al: Malignant GI Stromal Tumors (M-GIST): 52 cases from a prospective database. CanJ Surg 42(3):22, 1999 (abstract)
127. Omura GA, BlessingJA, Major F, et al: A randomized clinical trial of adjuvant adriamycin in uterine sarcomas: A Gyneco- logic Oncology Group Study.J Clin Oncol-3:12-40-1245, 1985
128. Hornback NB, Omura G, Major FJ: Observations on the use of adjuvant radiation therapy in patients with stage I and II uterine sarcoma. IntJ Radiat Oncol Biol Phys 12:2127-2130, 1986
113.
115.
116.