the magazine insights - qiagen · there’s a company that is helping to answer these questions and...
TRANSCRIPT

INSI
GH
TS —
TH
E Q
IAG
EN M
AG
AZ
INE
InsightsThe QIAGEN Magazine
Sample to Insight


A revolution is rapidly evolving our understanding of the building blocks of life – DNA, RNA and proteins.
These advances are impacting our everyday lives, such as improving how people are treated for diseases like cancer, helping to find new medicines, and even safe-guarding the public. But unlocking answers and understanding how breakthroughs can make an impact on our lives remains elusive and challenging.
There’s a company that is helping to answer these questions and helping society benefit from the power of biology. It first revolutionized how to extract DNA and RNA from any sample, including blood, tissue, plants and even bone fragments. Now it is helping customers around the world gain the valuable molecular insights they need to improve healthcare and advance science.
That company is QIAGEN.
Our molecular testing solutions help customers gain insights for virtually any applica-tion involving DNA and RNA. By keeping a finger on the pulse of innovation, we are able to turn the latest breakthroughs into everyday benefits and leverage them across the continuum from basic science to routine healthcare.
We have more than 4,600 passionate employees who care deeply about the impact of their work and have a determination to excel. They are known as QIAGENers, and are driven above all to help customers exceed their own expectations. Our global reach means we are around the world where our 500,000 customers need us.
QIAGEN solutions are critical to the work of virtually every biology lab around the world. We help tackle the bigger challenges that affect all of us. This is how we make improvements in life possible.

2 3
Contents
14The genomic war on cancer
42Between two worlds
30CSI: United States
4Insights in action

2 3
24Life-saving tests
10Interview with Peer M. Schatz
34 Fast-forward
32New insights on cheetah conservation
46On call

4 5
For QIAGEN customers, the real value is not tests, instruments or software – it is the actionable insights unleashed by our end-to-end solutions. Insights enabling a doctor to save a patient’s life. Empowering a scientist to pioneer new frontiers of knowledge. Helping to solve crimes, protect food supplies and safeguard our en -vironment. Starting with raw samples like blood or tissue, QIAGEN solutions lead to impactful results. Sample to Insight.
Insightsinaction

4 5
INSIGHTS | Insights in action
Dr. Heidi Rehm, FACMGDirector of the Laboratory for Molecular Medicine at Partners Healthcare Personalized Medi-cine and Associate Professor of Pathology at Harvard Medical School, Boston, Massachusetts.
» We’re headed to great places with genomics and medicine.«
CREATING THE FUTURE

6 7
Dr. Rong FanAssociate Professor of Biomedi-cal Engineering, Yale University,New Haven, Connecticut.
» Our focus is on translational research. I want to take single-cell sequencing to the clinic and see how it can help diagnose or stratify disease for better treatments.«
PIONEERING SCIENCE

6 7
» On average, every third DNA profile we create, currently trig-gers a hit. I’m very confident that the likelihood of getting positive results will further increase going forward, not only due to the growth of the databases but also due to novel applications being developed.«
Dr. Burkhard RolfDirector of DNA Forensic Services at Eurofins Medigenomix Forensik GmbH in Ebersberg, Germany.
SOLVING MYSTERIES
INSIGHTS | Insights in action

8 9
Prof. Dr. Finn Cilius NielsenHead of the Center for Genomic Medicine, Copenhagen, Denmark.
» We are applying genomic technologies to clinical practice more quickly than anyone anticipated. We talk to clinicians in our hospital, and they are really positive about the benefits of linking genetic mutations to their patients’ diseases and targeted treatments.«
SAVING LIVES

8 9
Dr. Madhuri Hegde, FACMGProfessor of Human Genetics at the Emory University School of Medicine and Executive Director of the Emory Genetics Lab, Atlanta, Georgia.
» The success of genomic medicine will come down to the ability of bioinformatics to help analyze and interpret genetic variations to come up with clinically actionable insights.«
ENABLING ACTION
INSIGHTS | Insights in action

10 11
The news these days is full of stories about advances in the use of genomic information. What is driving this trend?
We are truly living in the middle of a molecular revolution, which is driven by rapid progress in our understanding of DNA and RNA, the building blocks of life. Advances in genomics are occurring at an unprecedented rate and have a major impact on our everyday lives. Consider, for instance, how the treatment of cancer has changed over the past decade. Instead of using a “one size fits all” approach, phy-sicians now routinely personalize treatments guided by molecular insights. But these advances are not limited to healthcare. Molecular technologies are also indispensable in managing food supplies, ensuring public safety and, above all, developing new medicines. Representing the foundation of this progress, academic research is pushing the boundar-ies of science forward at breakneck speed. All this adds up to a really strong momentum.
How is QIAGEN helping to drive this molecular revolution?
Our mission has always been to help our customers access valuable molecular insights faster, more reliably, and more efficiently. This is what drives the passion of our more than 4,600 employees around the world and is behind our vision of making improvements in life possible. We want to help soci-ety benefit from the power of advances in molecular biology.
Interview with QIAGEN’s CEO Peer M. Schatz on our strategy and aspirations, achievements in 2015 and goals in 2016 and beyond, particularly in respect to our growth drivers and the Sample to Insight framework.
» We’re living in a transformative phase«

10 11
Peer M. Schatz Chief Executive Officer, QIAGEN N.V.
What sets QIAGEN apart from other companies participating in this revolution?
A major competitive advantage is our “Sample to Insight” portfolio of differentiated solutions. We are not only an instru-ments company, or a reagents provider, or a supplier of bio-informatics. It is our firm belief that just offering individual components falls too short. Instead, we are taking a holistic view of workflows and challenges our customers face, and we are addressing bottlenecks with complete, streamlined and insight-centric solutions. We aspire to enable our custom-ers to generate the insights they need in a way that exceeds their own expectations.
The ability to offer complete, insight-centric solutions is a nat-ural evolution for QIAGEN and builds on many positions of strength. For example, our leadership position in sample tech-nologies makes QIAGEN literally a gatekeeper to all labora-tory workflows. Sample processing is the starting point of every molecular biology application, and the performance of this step has a significant direct impact on the quality of the end result. That’s why our products are firmly established in all areas of molecular biology where quality of results is par-amount. Customers who are familiar with us are more likely to add more QIAGEN solutions to their workflows. We changed genomics by pioneering components such as sample
INSIGHTS | Interview with Peer M. Schatz

12 13
investments to drive further expansion. Putting in place this new wave of growth was a massive effort, and I’d like to thank our employees and shareholders for their continued sup-port during this transformative initiative. These efforts are now starting to pay off, as our portfolio of growth drivers continued to advance at double-digit rates and exceeded 30 % of our net sales in 2015. We believe these successes will become even more apparent in 2016 and the coming years.
Is tuberculosis control mainly an issue in emerging countries?
Many people in developed countries underestimate the dis-ease – but tuberculosis is a global public health threat. About nine million people are diagnosed with active TB per year around the world and the disease claims about 1.5 million lives, so it is critical to improve the effectiveness of TB control. There are two basic types of tuberculosis infection, latent TB, when the bacterium causes no symptoms, and active TB, when the infection is activated to become contagious and potentially life-threatening. A major element in the global fight against TB is screening and treating at-risk populations for latent infection to prevent future outbreaks of active TB. With a total addressable market potential of more than $1 billion, screening for latent infection represents the majority of TB test-ing in the developed world. We also see emerging and devel-oping regions increasing their efforts in latent TB screening, triggered by new World Health Organization guidelines issued last year. Our QuantiFERON-TB Gold tests are more accurate and cost-effective than the century-old tuberculin skin test and represent the power of modern diagnostics to address this challenge. We are committed to supporting the WHO and others in eradicating this often-deadly disease around the world, in both developed and emerging countries.
What are your plans for the use of the next-generation sequencing technology?
NGS is disseminating quickly in the life science and molecu-lar diagnostics markets, and QIAGEN has been addressing this growing need with a range of universal solutions that resolve many bottlenecks in existing NGS workflows. About 80 percent of NGS operations worldwide already use
technologies, and we are now leading the way into the next wave of molecular testing with our Sample to Insight value proposition.
A further advantage is our global reach, which enables us to seamlessly serve major international organizations, as well as react quickly to unforeseen developments such as disease out-breaks. The recent Ebola epidemic in Africa and the current Zika virus outbreak in the Americas exemplify our ability to leverage our global network to address urgent customer needs.
All of this reinforces the fact that QIAGEN has one of the most admired and highly respected brands among customers involved in the life sciences and molecular diagnostics.
You mentioned sample technologies as an important differentia-tor for QIAGEN, but isn’t real innovation driven instead by novel detection and analysis technologies?
Not anymore – it is the combination of pioneering technolo-gies. Innovation is driven by advances along the entire work-flow from Sample to Insight. For example, sample technologies recently have been a major trigger for the development of new applications: customers are very excited about our leadership in enabling minimally invasive “liquid biopsies,” which tap into molecular information transported through body fluids. Prena-tal testing and cancer diagnostics are two rapidly emerging fields for the application of this breakthrough technology. Another example of sample technologies basically enabling a new industry is microbiome research. The customers require cutting-edge technologies for the analysis of complex microbi-al samples, such as in the environment or even in the human gut. We have expanded our offering in this field with the recent acquisition of MO BIO Laboratories, and we will continue to invest in offering the most innovative sample technologies.
What are other areas of strategic importance to QIAGEN?
In recent years, we have focused on a portfolio of strategic growth drivers – including our franchises in TB control, next-generation sequencing, bioinformatics, personalized health-care and the QIAsymphony platform – and made targeted

12 13
» We aspire to enable our customers to generate the insights they need in a way that exceeds their own expectations.«
QIAGEN’s industry-leading sample technologies and our Enzymatics pre-analytical technologies. A similarly high per-centage of NGS users utilize our bioinformatics.
With the recent launch of our GeneReader NGS System, we kicked off a new major phase in our strategy to bring next-generation sequencing into mainstream laboratories, and the customer feedback has been very positive. The GeneReader NGS System integrates our proven technologies and test con-tent with a flexible benchtop platform and advanced bioinfor-matics to deliver the world's first complete Sample to Insight NGS workflow designed for any laboratory to deliver action-able insights. We are very proud of this achievement and are now focusing on successful commercialization and further enhancement of this platform.
How do bioinformatics fit into QIAGEN’s business?
While next-generation sequencing is transforming genomic testing, it continuously generates vast amounts of highly com-plex digitized data. Advanced bioinformatics are the only viable option to efficiently process and analyze this volume of data to arrive at actionable insights, so handling that informa-
tion plays a key role in the entire laboratory workflow. That’s why QIAGEN has decided to address this bottleneck by building industry-leading solutions that mine data, consult vast biomedical databases, and report actionable insights for doctors or researchers. Our bioinformatics solutions have more than 120,000 users, including all of the top 40 Pharma companies and institutions like the FDA, which recently expanded its use of QIAGEN bioinformatics. This diverse informatics portfolio is growing at strong double-digit rates.
How do you see the molecular revolution playing out?
Molecular technologies will change our everyday life over the next 10 -20 years, and most people probably underestimate that impact. But further advances in molecular biology in com-bination with modern IT technologies will spur the pace of innovation and prompt the development of many new appli-cations that are inconceivable today. We’re living in a trans-formative phase. QIAGEN is committed and privileged to be shaping the application of these powerful new molecular technologies. We are delivering on our mission of making improvements in life possible.
INSIGHTS | Interview with Peer M. Schatz

14

The genomicwar on cancer In less than a generation, the medical approach to conquering cancer has shifted from using chemotherapy as a ‘500-pound bomb’ to deploying precision-guided drugs targeted to each patient’s unique genomic characteristics. Personalized healthcare is now a routine strategy against cancer. In the future, advanced gene panels and next-generation sequencing will deliver more victories to oncologists and their patients. by Richard Johnson
15

16 17
Walking into Copenhagen’s Rigshospitalet, the lead-ing specialty hospital in Denmark, a visitor feels the mixture of hope and apprehension that vast
institutions tend to inspire. Sixteen stories of concrete-and-glass functionality, the building stacks floor upon floor of hos-pital rooms, each packed with high-tech equipment and, inter-mittently, staff working to save the lives of patients.
Through the windows of the Center for Genomic Medicine, looking out on Rigshospitalet’s main entrance from one floor up, it is the patients and their families that you notice.
“Many of the patients coming into the hospital are already very sick,” says Professor Finn Cilius Nielsen, head of genom-ic medicine for Rigshospitalet. “As a regional center, we tend to see cancer patients and others who are difficult cases. They may have failed treatments at other hospitals, or relapsed after treatment, so they come here for a higher level of specialized care.”
The Center for Genomic Medicine brings 21st Century weap-ons into this battle.
For patients and doctors, fighting cancer has shifted to the molecular front: Life’s building blocks, DNA and RNA, have
emerged as critical for diagnosing and treating cancers. And so this war on cancer has become a genomic war. In the cen-tury to come, genomic medicine will undoubtedly conquer other frontiers – but today that battle is mostly being fought in cancer.
QIAGEN works hand-in-hand with scientists in universities and life science companies advancing the understanding of cancer – and with doctors deploying companion diagnostics, novel sequencing technologies and advanced bioinformatics to make personalized treatment decisions based on each patient’s genomic data.
Bridging the continuum
Rigshospitalet exemplifies the continuum of healthcare in large, research-based institutions that are leading the war against cancer.
Across the street, the University of Copenhagen is deeply engaged in research into the causes and pathways of cancer, the basic science of how the disease works. In the hospital, the focus is on patients and how to apply the best treatment to reverse the disease or prolong survival. Many of Rigshos-pitalet’s staff members serve dual capacities, in the university and the hospital.
The Center of Genomic Medicine is located right above the main entrance, overlooking the flow of visitors entering the hospital.

16 17
INSIGHTS | The genomic war on cancer
Each year, more than 14 million people are newly diagnosed with cancer, and the disease takes more than 8 million lives, according to the World Health Organiza-tion. Authorities expect the number of new cases worldwide to grow by about 70 % over the next two decades.
The threat is exacerbated because cancer is not one disease, but many. Cancer can take hold in any of more than 100 parts of the body and is often named by its site of origin – lung cancer, breast, colorectal and so on. That was the historical approach to fighting the war on cancer.
Less visibly, cancer wreaks its havoc in the body at the molecular level. As gene muta-tions disrupt the normal growth mecha-nisms of cells, uncontrolled cell division forms tumors in one place or begins to dis-seminate cancer cells through the body.
Viewing cancer as a genomic enemy
The problem is a molecular “variant” in DNA, its RNA messenger system, or pro-teins they use to maintain body functions.
Molecular variants and their combinations are highly individualized – so that one lung cancer patient in a hospital can differ in critical ways from a lung cancer patient in the next bed. In fact, no two patients have exactly the same disease. Their genomic profiles can dramatically influence the development of the disease and the effica-cy of potential treatments.
Personalized healthcare – also called pre-cision medicine – employs molecular diag-nostics to test each patient’s genomic vari-ants as a guide to the best treatment. The tests find biomarkers for changes at the molecular level known to either cause the cancer or affect the usefulness of potential drugs in treating it.
Center for Genomic Medicine www.genomic-medicine.dk
GeneReader NGS System www.genereaderngs.com
Molecular biologist Dr. Christina Westmose Yde focuses on exploring new treatment options for cancer patients.
people are newly diagnosed with cancer every year, accounting for more than 8 million annual deaths.
14 million

18 19
Lung1,824,701Breast
1,671,149
Stomach951,594
Liver782,451
Prostate1,094,916
Esophagus455,784
Bladder429,793
10 most common cancers worldwide by annual incidence and main associated mutations.
Source: GLOBOCAN 2012, QIAGEN Knowledge Base 2016.
The genomics center, a long, narrow strip of offices and lab-oratories jammed with instruments, test kits and patient sam-ples, bridges these worlds – connecting the laboratory bench to the patient’s bedside. From the research end, the latest advances continually create potential new strategies to deal with genomic influences on cancer, its pathways and treat-ment. On the clinical side, the laboratory works closely with oncologists to provide insights into the hospital’s patients and how to address their urgent needs for approaches to fight the disease.
The Rigshospitalet lab has a full range of technologies, from standard tests to screen for individual cancer-causing gene mutations to sophisticated next-generation sequencing (NGS) algorithms for more complex cases. The center runs about 3,500 tests a year.
“In running these tests, the goal is to provide the most promis-ing treatment for each patient,” Professor Nielsen says. “We have access to a large number of targeted therapies for can-cer, whether approved or in clinical trials, and our research role allows us to use deep sequencing to suggest clinical tri-als of more experimental treatments for patients who fail stan-dard therapies.”
A lung cancer patient, for example, came into Rigshospitalet already very ill. Next-generation sequencing on a sample of his tumor revealed a mutation of the BRAF gene, a cancer-causing variant active in about 50 % of melanoma skin can-cers – but not usually seen in lung cancer.
Breast1. PIK3CA p.H1047R2. ESR1 p.K303R3. PIK3CA p.E545K
Stomach1. APC p.T1556fs*32. PIK3CA p.H1047R3. KRAS p.G12D
Bladder1. FGFR3 p.S249C2. CDKN2A c.1_471del4713. HRAS G12V
Cervix1. PIK3CA p.E545K2. KRAS p.G12D3. KRAS p.G12S
Esophagus1. TP53 p.R43H2. TP53 p.R175H3. TP53 p.G154V
Colorectum1,360,602
Non- Hodgkin
lymphoma1,824,701
Cervix527,624
Non-Hodgkin lymphoma1. TP53 p.R43H2. TP53 p.R175H3. TP53 p.G154V
Lung1. CDKN2A c.1_471del4712. EGFR p.L858R3. EGFR p.E746_A750del
Liver1. TP53 p.R249S2. HNF1A p.G292fs*253. CTNNB1 p.A5_A80del
Colorectum1. BRAF p.V600E2. KRAS p.G12D3. KRAS p.G12V
Prostate1. PTEN c.1_1212del12122. HRAS p.Q61L3. BRAF p.V600A

18 19
“There is an approved drug for BRAF, but normally the patient would have melanoma to receive this drug,” says Dr. Lars Joensen, head of the center’s NGS core unit. “This lung can-cer patient was offered a drug that acts against the BRAF-acti-vating mutation, and he responded well to the drug. The patient is alive today, almost a year later, so it’s a very good and happy story.”
The bench-to-bedside continuum uses the same kinds of tools from cancer research to clinical diagnostics: instruments, kits and software to prepare samples, to sequence genes and detect variants, and to sort the results for a clear interpreta-tion. So diagnostic methods migrate from university and industry laboratories, through regulatory processes, into hos-pitals and clinics.
From the early days of biotechnology, QIAGEN has offered an ever-broadening portfolio of the latest and best genomic tools to its customers in life science research and molecular diagnostics. The company’s tools are instrumental in thou-sands of research studies, relied upon in drug development, and used by physicians around the world in the war against cancer.
Making personalized medicine routine
Since the first companion diagnostics emerged in the 1980s, detection of genomic mutations to guide treatment has expanded to the point where personalized medicine has become standard medical strategy for a number of can-cers – routine, and yet continuing to evolve rapidly.
“A lot has happened in the field of genomic profiling in the last few years,” nods molecular biologist Dr. Christina West-mose Yde, who focuses on genomic profiling of patients for whom no approved treatment options are yet available. “Instead of putting a cancer into a certain box based on the initial diagnosis, personalized medicine now enables us to take a deep look into the tumor to find out what’s driving its growth and then to target the specific disease.”
Typically, treatment follows clinical guidelines that provide for testing to detect one or more genetic biomarkers to match patients with targeted therapies that act upon their variants. These protocols amount to decision trees, with each step guid-ed by a single-purpose test.
A patient with non-small cell lung cancer (NSCLC), for exam-ple, would be tested for alterations of the epidermal growth factor receptor (EGFR) gene. Testing “positive” indicates the patient’s tumor growth could be slowed or halted by one of the innovative drugs designed to block the EGFR receptors on cells from binding with enzymes that lead to uncontrolled growth.
“Companion diagnostics based on insights like the EGFR link to lung cancer have come into routine use by oncologists around the world. QIAGEN provides about half of the kits targeting EGFR mutations, and our tests for other cancer bio-markers are disseminating as we steadily gain regulatory approvals,” says Dr. Tadd Lazarus, chief medical officer of QIAGEN. “The emergence of reliable, standardized tests is making a great difference for patients. Before genomic testing
INSIGHTS | The genomic war on cancer
3,500samples, mostly from cancer patients, are processed by the Center of Genomic Medicine a year.
20 21
Taking sequencing to the next generation
In clinical research and healthcare applications, time con-straints are driving a shift to ever-faster platforms that can analyze more and more variants simultaneously. Testing a patient with cancer or a rare disease for a single variant at a time – or, at the other extreme, sequencing the patient’s whole genome – is simply too slow in many cases.
“Turnaround time is really important for the patients. You want to avoid delaying the treatment too much,” Professor Nielsen says. “Some of the patients are very ill to start with, or chil-dren who have already been through a diagnostic odyssey. So we need to get answers.”
Leading institutions like Rigshospitalet are deploying next-gen-eration sequencing and multiplex gene panels to accelerate the process of precision diagnosis and treatment.
“For a cancer patient, any delay in treatment seems like dou-ble time. If you have to wait and the cancer continues to prog-ress, then by the time you have results it may be too late to do the patient any good,” says Dr. Maria Rossing, a physician and staff specialist with the Center for Genomic Medicine. “If we could run a gene panel that looks at the most likely muta-
enabled personalized medicine, cancer treatment was often trial-and-error.”
As the knowledge of cancer continues to expand, the number and type of biomarkers are growing rapidly – as are the treatments targeting those mutations. About 50 genomic vari-ants are now targeted by drugs offering potential benefit in different cancers. So research-driven clinicians like those at Rigshospitalet are broadening their genomic testing to cast a wider net.
“Cancer is complex. Some cases are easy, but some are very difficult,” Professor Nielsen says. “When it comes to many solid cancers, you find a pattern of mutations, so we need to be able to look into a combination of variants and potential treatment approaches. What you are looking for, and there-fore the kind of tests to run, depends on the individual patient.”
The trend is to move from tests for individual biomarkers toward gene panels that analyze dozens or hundreds of gene variants in a particular type of cancer. For different needs, laboratories can access a variety of technologies from PCR to multimodal instruments to next-generation sequencing.
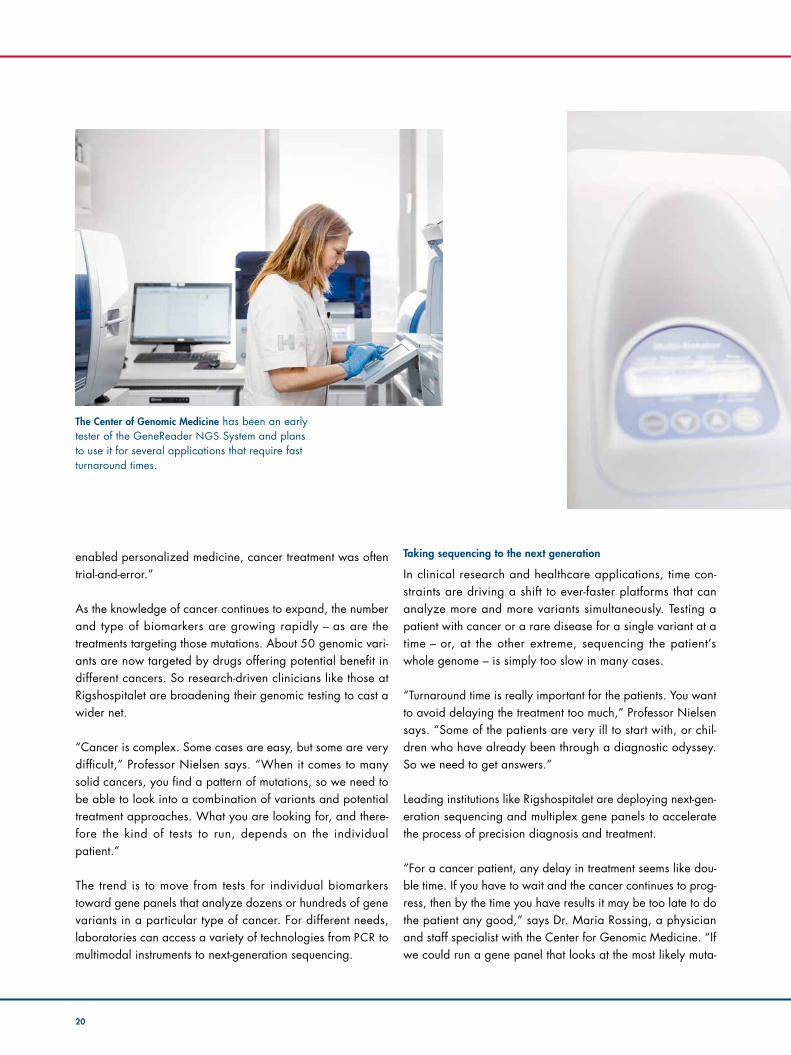
The Center of Genomic Medicine has been an early tester of the GeneReader NGS System and plans to use it for several applications that require fast turnaround times.

20 21
INSIGHTS | The genomic war on cancer
» It’s very helpful to have a small panel, where you cover all of the clinically relevant variants and can quickly deliver actionable insights.«Dr. Lars JoensenBiochemist, Center for Genomic Medicine, Copenhagen, Denmark.
Liquid biopsies from blood and other body fluids hold great promise to improve the diagnostic process and treatment monitor-ing of cancer patients.

22 23
tions, coming up with a preliminary answer in five days rather than weeks, that would be a good thing.” In late 2015 QIAGEN introduced a novel solution that prom-ises to address this need for clinical research labs: the Gene-Reader NGS System and the platform’s first application, the Actionable Insights Tumor Panel. This multiplex assay targets 12 clinically actionable genes implicated in prevalent cancer types, including breast, ovarian, colorectal, lung and melano-ma. While not yet approved for diagnostic use, this platform will soon be the solution sought by many labs.
The Actionable Insights panel can detect up to 1,250 differ-ent genetic mutations in a sample. The assay integrates with QIAGEN Clinical Insight, a cloud-based bioinformatics solu-tion that helps to identify important genetic variants – includ-ing those that are in approved drug labels, professional guidelines and active phase III clinical trials.
The Rigshospitalet genomics center, which uses a wide range of NGS technologies, put the GeneReader NGS System and Actionable Insights panel through their paces this winter in carefully controlled tests – and the reactions from the staff involved were positive.
“We managed to have a turnaround time of around five days, from sample to answer,” says Dr. Joensen. “It’s very helpful to have a small panel, where you cover all of the clinically rele-vant variants and can quickly deliver actionable insights.”
For understanding the biology behind a disease, researchers use whole genome or exome sequencing to capture every possible bit of genomic evidence – but when a patient is in the hospital, the doctors’ focus is on getting to the right deci-sion on treatment. “There are some practical obstacles to sequencing full genomes, including a longer time to result and more challenging data analysis,” Dr. Yde explains. “But

22 23
Prof. Dr. Finn Cilius Nielsen Head of the Center for Genomic Medicine, Copenhagen, Denmark.
» There is no doubt that we should do genomic tests as early as possible. When we come in very early, we know that we can actually change the course of disease for the patient.«
the main question is what you’re adding in terms of action-able insights. As of today, I believe that targeted sequencing approaches cover most of what you’re looking for to guide treatment decisions.”
Professor Nielsen says the QIAGEN focus on clinical rele-vance and fast turnaround, combined with GeneReader’s automated handling from sample to final report, will allow any laboratory without research-level NGS expertise or bio-informatics staff to begin to take advantage of NGS. The inte-gration of QIAGEN Clinical Insight, drawing on continually updated, expertly curated knowledge bases, also provides a powerful interpretive tool to determine the relevance of genet-ic variants found in a sample with the latest information in the rapidly developing field of cancer research. “It’s a democra-tization of the process,” Professor Nielsen says.
Working toward tomorrow’s victories
The struggle against cancer is a war of insights – with medi-cine striving both to understand the mechanisms of the dis-ease and to find the best treatments for each individual patient. The victories are adding up, and the campaign is gaining momentum.
The Rigshospitalet team embraces increasing standardization and automation of genomic testing, including NGS, to save money and to drive the growing use of precision medicine. Professor Nielsen sees a future of expanding reliance on molecular diagnostics for clinical insights – both earlier in the process and later in the course of treatment.
“There is no doubt that we should do genomic tests as early as possible. When we come in very early, we know that we can actually change the course of disease for the patient,” Professor Nielsen says. “If you ask me, I would like to have the first biopsy available and do all the tests then – the gene
panels, the NGS sequencing. The earlier it’s done, the better the outcome.”
The emergence of relatively inexpensive, minimally invasive “liquid biopsies” will also benefit the diagnostic process and enable the monitoring of outcomes while treatment progresses, Professor Nielsen says. Liquid biopsies use easily collected samples of blood or other fluids to detect circulating tumor cells or genomic molecules shed by cancer anywhere in the body, and these patient-friendly tests can replace difficult and sometimes risky surgical biopsies.
“Every day in the newspaper, people discuss the increasing cost of using cancer drugs,” Professor Nielsen adds. “If we can reduce those expenses by monitoring how the treatment is working with an easy test and by tailoring the use of the drug to the patient’s precise need, it’s good for the patient but it’s also very good for society.”
Medicine has advanced in the war on cancer. There is wide variation among cancer types and patient circumstances, but most cancers have become more survivable. Across all variet-ies, 68 percent of U.S. patients survive more than five years, up from 49 percent two decades earlier. Other countries also have seen dramatic improvements. With early diagnosis, innovative therapies plus targeting through genomic medi-cine, the blunt news “You have cancer” is giving way to a sys-tematic, personalized process aimed at curing or managing the disease.
“The patients we see are in advanced stages, but even if they do not get complete remission, they are gaining some good additional time to live, where they are feeling much better,” Dr. Rossing says. “Not to be personal, but had it not been for the good successes we have seen in our patients, I could not function as an M.D. in this setting. That makes it worthwhile.”
INSIGHTS | The genomic war on cancer

Life -saving tests
Elisabetta Chiarini from Bergamo, Italy, is having a blood sample taken. Every three months, she and her husband travel 250 kilometers to the Clinic of Cardiology at Sant’Orsola- Malpighi University Hospital for this procedure. Suffering from severe cardiac insuf-ficiency, she received a new heart in May 2014. Before that, she was on “la lista” for a year and a half – the list of all patients waiting for an organ transplant. The operation in a different Italian hospital was a success, but the side effects of immunosuppressants she was given there were severe.

INSIGHTS | Life-saving tests
Shortly before you reach her office on the second floor of Building 11, the yellow warning signs grow more frequent, and the wooden doors are replaced by dramatic-looking steel ones, several centi-
meters thick, with little glass windows. It’s through windows like these that trapped characters in Hollywood movies throw their loved ones a final kiss. A sign on a door on the right says “Tiziana Lazzarotto.” The door opens and sunlight pours into the corridor.
“Ciao, I’m Tiziana!” Professor Tiziana Lazzarotto says with a friendly smile. The CV of this lively 58-year-old is so extensive you have to scroll right down your screen to read it all: Professor of Microbiology and Clinical Microbiology at the University of Bologna, Italy, with 180 scien-tific articles, countless medical congresses and six prizes. “I work with passion,” she says. The silent witnesses on her desk include a Paris pencil holder, an “I Love Berlin” glass and a miniature koala bear – all souvenirs from conferences.
With a CV like that, Tiziana Lazzarotto is clearly an authority in her field, a coryphaeus in clinical virology. As an Italian she might empathize with that Latin word, and in particular with one of its present-day English meanings: “leader of the chorus.” That is how Tiziana Lazzarotto sees her role – a facilitator who ensures the success of entire projects to help patients. Specifically by helping transplant patients live with a new organ. And even more specifically by collecting and evaluating data about their health status: “Diagnostics can assess if there’s a threat of infection, or even death.”
War! That is what Professor Lazzarotto is waging along with a team of serious yet friendly physicians and assistants; a war fought on the side of patients who need help to fight off the attacks of viruses and bacteria. The battlefield is the transplant patients’ immune system. “In the first 20 days after a transplant, it’s initially the risk of a bacterial infection that is high,” Professor Lazzarotto says. “Afterwards, it’s mainly the cytomega-lovirus (CMV).” Over 80 % of transplant patients have to fight infection with CMV, a common virus that can cause severe symptoms or death in people with weakened immune systems.
Tiziana Lazzarotto cares for people who have organ transplants – serving not at their hospital beds, but in the virology laboratory of one of Europe’s most renowned transplant clinics. Valuable insights from QIAGEN tests help guide decisions critical to the patients’ lives. by Martin Zöller
Prof. Dr. Tiziana Lazzarotto is a professor of microbiol-ogy and clinical virology. Her work is mainly devoted to the cytomegalovirus, and to protecting transplant patients from it.
25
26 27
This is because after a transplant, the patient’s immune system must be suppressed; yet if it is suppressed too far, infection sets in. So how far is “too far”? Up till now, it has been difficult to individualize post-operative medication. Some patients have received too many immunosuppres-sants, and some too few. What has been lacking is insight into exactly how much medication each patient needs so that his or her immune sys-tem is weak enough to accept the new organ but strong enough to repulse dangerous viruses and bacteria.
“We have two types of monitoring tests and both must be carried out at the same time,” explains Professor Lazzarotto. Viral load tests such as QIAGEN’s artus PCR kits are used in Bologna to help determine the presence and concentration of a specific virus, and immunological tests like QuantiFERON-CMV add another layer of information by measuring the patient’s immune response to the infection. “Our task is to prevent the progression of a viral infection towards active disease,” says Profes-sor Lazzarotto. “So if we diagnose an infection and see only a poor immune response to it, we need to help the patient by either reducing the immunosuppressant or initiating an antiviral therapy.”
Now, a new tool, QuantiFERON Monitor, promises to further advance the management of post-transplant patients. The novel test helps to assess the strength of the immune system of patients who are given immunosuppression therapy after a transplant by measuring their indi-vidual cell-mediated immune response. For the first time ever, it is possi-ble to decide on the right amount of medication based on a patient’s specific immune response. Up until now, clinics have only monitored the concentration of the medication, irrespective of its effect on the immune system.
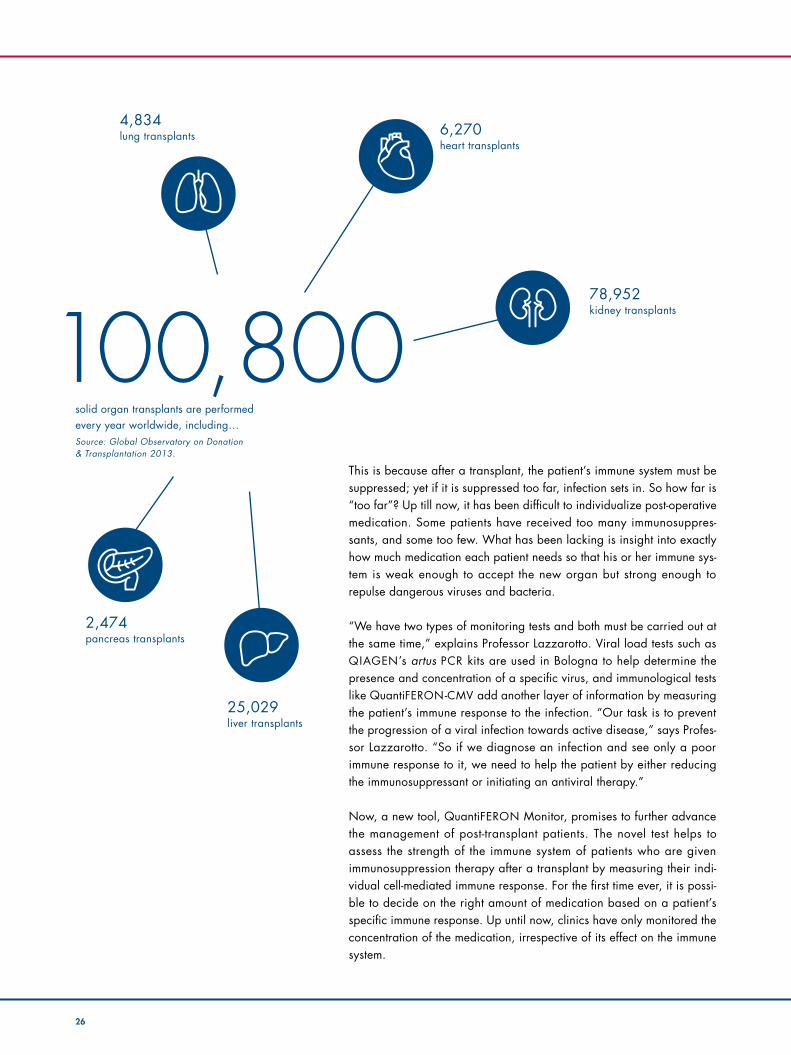
100,800solid organ transplants are performed every year worldwide, including…Source: Global Observatory on Donation & Transplantation 2013.
78,952 kidney transplants
4,834 lung transplants 6,270
heart transplants
2,474 pancreas transplants
25,029 liver transplants

26 27
What are the main challenges you face in your work today? My area of expertise is heart transplants. We see an ongoing decline in the number of organ donations all across Europe, so we find ourselves transplanting patients in worse conditions than those a few years ago. This makes the post-transplant man-agement more complex because weakened patients are at higher risk of post-surgical infection. At the same time, we face increas-ing pressure to optimize resources while providing every patient the best treatment possible.
What’s so difficult about managing the infec-tion risk?We have highly effective antiviral drugs to treat potential infections, but those medi-cines are very costly and can have severe side effects. Considering that every single
patient responds differently to an infection, our goal is to customize the therapeutic strategy as much as possible. But to achieve this we need to measure exactly what we are doing, we need to understand how the patient’s immune system is responding to a treatment. For instance, if I knew that a patient’s immune system is already respond-ing to a CMV infection, I could use a lower dose of the medicine or for a shorter period of time, effectively reducing the risk of side effects and saving money.
How do QIAGEN products help you to achieve this vision? Thanks to the close collaboration with Pro-fessor Lazzarotto and QIAGEN, we were able to develop different strategies to moni-tor the immune system and effectively man-age our patients. We’ve been using the QuantiFERON-CMV test for several years
now on patients suffering from side effects of antiviral therapy to determine if their immune system is responding to the CMV infection. QuantiFERON Monitor is still fair-ly new, but I think that it will be important for the future. I believe monitoring is an essential next step in customizing therapy. We’re currently running a study with around 100 patients and receiving very interesting initial results. They suggest that I can identi-fy patients at greatest risk of infection and monitor them more closely, or modulate the immunosuppressant therapy to avoid a clin-ical event. These results need to be con-firmed in a follow-up phase of our study, but we are expecting a great deal from this test going forward and I believe that this is essential as the next step in customizing therapy.
Dr. Luciano Potena discusses transplants
INSIGHTS | Life-saving tests
Dr. Luciano Potena is a cardiologist. His department currently cares for about 500 outpatients who have undergone a heart transplant and whose immunosuppressants are constantly being customized. An additional 800 patients from all over Italy are under observation for a possible transplant.

28 29
In view of the fact that immunosuppression is responsible for 40 –70 % of all deaths following an organ transplant, QuantiFERON Monitor meets a critical medical need by allowing doctors to assess an individual’s immune response, helping guide patient management and treatment decisions to reduce the risks of organ rejection and infection. The test was launched with a CE-mark in Europe in 2015, and a regulatory sub-mission is planned for the U.S. as well.
Dr. Luciano Potena, a 43-year-old cardiologist at the Sant’Orsola-Malpi-ghi University Hospital in Bologna, presently cares for 500 heart trans-plant patients, of whom 100 are already being observed using the QuantiFERON Monitor: “We have fewer organ donations these days and the patients who are waiting are consequently in an increasingly poor state of health. So it is all the more important to perfect each indi-vidual transplant and post-operative care,” he says. That means individ-ualization. After all, a majority of Italians carry the cytomegalovirus, which post-operative immunosuppressing therapy can set off again.
Professor Lazzarotto and Dr. Potena are on first-name terms. That is typ-ical for Bologna, as the laboratories here are allies cultivating constant interaction with physicians. “We are in a continuous dialogue about the management of individual patients as well as clinical research projects,” explains Dr. Potena. “Thanks to this close collaboration and the diagnos-tic tools provided by QIAGEN, we’ve been able to develop a clinical management system that is tailor-made to the needs of our patients.”
Above all, patients are the ones who benefit from precise monitoring of immune response, says Professor Lazzarotto: “Antiviral medication is
The Sant’Orsola-Malpighi Clinic already has 30 years’ experience with heart transplants. Currently, an average of 23 heart trans-plants are carried out every year. The cooper ation between the clinic and the lab-oratory at Sant’Orsola has been repeatedly cited as the basis for Bologna’s success. The clinic in Bologna was one of the first cooperation partners for the QuantiFERON Monitor, which is presently being used to monitor about 100 patients there.
23heart transplants
University of Bologna www.unibo.it/en
QuantiFERON www.quantiferon.com
Prof. Dr. Tiziana Lazzarotto shows her support for the worldwide physicians’ initiative #stopcmv by carrying a small silver loop on her lapel.

INSIGHTS | xxxxx
28 29
very effective, but also very aggressive,” she explains. “It is important to reduce the number of tablets.” What’s more, the clinic also benefits: “By measuring the strength of a patient’s immune system, the QuantiFERON Monitor test may provide important insights to assess how much medica-tion we really need in order to be effective.” That saves money and reduces the number of days in which beds are occupied. “We are given targets like reducing the number of bed-days. A good laboratory and good, reliable tests help everyone, patients and the clinic alike,” she says.
Nowadays, consumer products from chocolates to gym shoes and teddy bears are all personalized. But in medicine, personalization still has a lot of catching up to do. Up until now, it has been extremely challenging to individualize the management of post-transplant patients due to the lack of adequate diagnostics to measure the specific status of their immune system. QuantiFERON Monitor holds great promise to fill this gap. “Personalization is the future and I see great potential here,” says Professor Lazzarotto. She carries the battle against CMV around with her in the form of a silver loop on her lapel. That is how you recognize supporters of the worldwide physicians’ initiative #stopcmv. That is her passion.
In the first quarter of 2016 alone, Tiziana Lazzarotto had three confer-ences where she passed on her experience – in Venice, Amsterdam, and China. Any suggestions for souvenirs? A small gondola, a wooden shoe, a Chinese paper dragon? They would certainly look good on this profes-sor’s desk on the second floor of Building 11.
INSIGHTS | Life-saving tests
Professor Lazzarotto and her team value QIAGEN technologies due to their high level of standardization, ease of use and reproducibility.
In Bologna, the laboratory is not merely seen as a mute service provider but plays an integral part in the clinical manage-ment of patients.

30 1–5 6 –10 >10
CSI: United States As the single biggest market for human ID and forensic applications, the United States sets the pace worldwide. A new expanded standard set of markers to be used for DNA profiling is now bringing dramatic transformation, forcing U.S. laboratories to adopt new products and workflows. As the first new entrant in two decades to the U.S. market for forensic and human ID tests, QIAGEN is driving the change with technologies to help labs cope with increasing sample volumes and the need for efficiency.
by Lena Amberge
Labs contributing to the National DNA Index System (NDIS).
Washington D.C.
Florida
Hawaii
Alaska
Figures represent number of DNA profiles uploaded to NDIS per state as of December 2015.
22,623
14,431311,837
158,951
33,305
261,481104,626 320,366
288,192
416,68325,814
210,739166,442
326,239
492,704
30,987
351,824
102,623
108,651
351,245
32,046
23,718
581,966
104,443
170,474
141,299
34,931
31,253
55,788
670,268
351,698
124,564
195,255
258,670
127,920
286,459
406,329
155,959
213,904
257,003
31,435
110,872
136,496
10,824
19,003
1,182,186
California
2,500,139 895,281
1,032,278
51,935
303,201criminal investigations aided by CODIS as of December 2015.
598,686

31
3 Questions to Dr. Anke Prochnow Associate Director Global Market Management Human ID & Forensics, QIAGEN
States with the highest known backlog of unexamined samples.
What makes the U.S. human ID and forensics market special? With around 400 accredited forensic labs analyzing more than 4 million samples each year, the United States is clearly the world’s largest market for human ID applications. The U.S. also leads in forensic research, so many other countries adapt its methods and standards. More than 40 law enforcement laboratories in over 25 countries use the FBI Laboratory’s Combined DNA Index System (CODIS) software for their own database initiatives, and the CODIS marker set is used in the majority of countries worldwide.
Why did QIAGEN decide to enter the U.S. STR market in 2015? We’re not new to the U.S. forensics market. Our sample technolo-gies and automation solutions are well established in many human ID and forensic labs, setting the benchmark for DNA purification from casework samples. Previously, the legal situation prevented us from offering testing solutions in the U.S. for genomic markers known as short tandem repeats (STRs). This changed in 2015. Also, the CODIS system is expanding from 13 to 20 STR markers
Sources: FBI 2015, Joyful Heart Foundation 2015.
20,000
0
5,000
10,000
15,000
20,000
FloridaMichiganTexas
15,217
13,435
U.S. expansion of genetic markers to be tested brings advantages for forensics
facilitates discrimination between samples
helps in missing person investigations
encourages international cooperation by increasing
the number of common markers for comparison
by 2017. This forces forensic laboratories to establish new work-flows, creating a great opportunity for QIAGEN as the first new entrant in more than 20 years in the U.S. market for STR kits.
Why do you expect labs to switch to the QIAGEN system?The use of DNA evidence in criminal investigations has grown rapidly in recent years and now reaches into a broader range of crimes. Many labs struggle to cope with the expanding num-ber of samples and are seeking automated workflows that ensure highest quality results. We can meet these requirements and offer additional innovative features to speed up forensic investigations and provide more insights. One example is QIAGEN’s built-in Quality Sensor, a unique technology that helps evaluate the quality of DNA in each sample and enables labs to determine the right interpretation and rework strategy for cases they process. Customer feedback has been very positive, and we continue to invest in this market to support our forensic customers worldwide.
Human ID & Forensic Testing www.qiagen.com/forensics
Number of DNA profiles in the National DNA Index System (NDIS).
0
2,000,000
2000 2002 2004 2006 2008 2010 2012 2015
4,000,000
6,000,000
8,000,000
10,000,000
12,000,000 Offender Profiles
Arrestee Profiles
Forensic Profiles
INSIGHTS | CSI: United States

New insights on cheetahconservation
32

Once widespread throughout the African plains into Asia, cheetah populations have plummeted after decades of habitat loss, competition with rival carnivores, such as lions, leopards, and hyenas, and human persecution; in addition, they have an unusually low genetic variability that impedes adaptability to changes in the environment. With fewer than 10,000 animals remaining in the wild, cheetahs are at grave risk of extinction. The Cheetah Conservation Fund (CCF) – an expert global organization that aims to protect the cheetah and ensure its future – employs the latest genomic technologies to provide unique, new insights into this fascinating big cat species. by Sara Sharpe
W ide-ranging scientific research into cheetahs – from health assessments, ecological research on predators and ecosystem, human-wildlife conflict,
and resolution to genetics – is essential in CCF’s work. With approximately 3,500 individuals, Namibia has the world’s largest population of cheetahs. Located in the Namibian bush, the dedicated Conservation Genetics Laboratory is a vital resource in advancing CCF’s knowledge. Ongoing genetic research explores cheetah population-structure and individual genetic identification through non-invasive tech-niques. QIAGEN kits have been used in the research, since the laboratory first became operational.
“We rely on non-invasive research techniques, such as scat (or fecal) material analysis,” said Dr. Anne Schmidt-Küntzel, Assistant Director for Animal Health and Research, who set up the laboratory in 2008 and steers the CCF’s scientific pro-gram. “However, it is extremely difficult to assess the quality of cheetah DNA within cheetah scat, because it is highly
degraded and contains a wide variety of other DNA from prey and parasites. In this research, sensitive PCR reactions are crucial.We found out that the QIAGEN Multiplex PCR kits amplify important genetic markers 10 to 20 times better than any other tests known to us.”
Scat analysis enables CCF to assign a genetic ID to individu-al cheetahs, and combine genotyping of the DNA obtained from scat samples with photographs obtained from camera trap studies to match a visual ID to the individual. Population and health studies can then be carried out towards creating a genome resource bank and disease surveillance program for cheetahs, amongst other conservation priorities.
“Our conservation efforts are based on the best science pos-sible,” said Dr. Schmidt-Küntzel. “Advanced molecular tests significantly enhance our understanding of cheetahs’ needs towards stabilizing and growing cheetah numbers. This is made possible by companies like QIAGEN.”
Cheetah Conservation Fund www.cheetah.org
33

Fast- forward
34

We asked three well-known leaders in the genomic revolution to discuss the future of molecular testing and medicine. The panelists are Elaine Mardis, Ph.D., the Robert E. and Louise F. Dunn Distinguished Professor of Medicine at Washington University and co-director of the McDonnell Genome Institute; Heidi Rehm, Ph.D., FACMG, associate professor of pathology at Harvard Medical School and director of the Laboratory for Molecular Medicine at Partners Healthcare; and Tadd Lazarus, M.D., a physician who serves as chief medical officer of QIAGEN.by Richard Johnson
35

36 37
In five or ten years, what role do you expect geno-mics to play in medicine?
Dr. Mardis: We have clear indications today that genomics can add evidence to medical practice in terms of helping to better define diagnoses, treat-ments, prognoses, etc. I don’t think that genomics is always the answer or will provide the complete and only answer. But we are seeing evidence of where it is becoming incredibly helpful in the prac-tice of medicine.Dr. Lazarus: In my 18 years doing this, I have to say, what was considered wildly esoteric just a few years ago is considered ho-hum today. When I was an attending physician in a hospital in New York, it took an act of God to get authorization to run a PCR-based test. Back then, PCR occupied multiple rooms and took an entire day for the best technologists. Now, automation and plug-and-play systems make PCR routine. Today, we’re bringing in next-generation sequencing, which is radically different in the amount of data generated, the breadth and depth of insights. This has not taken all that long to emerge. So looking five to ten years down the road, what we’re talking about today will become routinized tomorrow for hospitals and physicians.Dr. Rehm: Over the next five to ten years I anticipate that we will increasingly move to exome and genome sequencing as a routine aspect of care both for diagnostics and preventative care. But we still have a lot of work to do to understand the pre-dictive capabilities of our genomes.
In the future, will a patient receiving a first diagnosis, say for cancer, be tested for genetic mutations as a routine procedure?
Dr. Rehm: It’s already happening. We have access to multiple tests, and different genes and mutations are being analyzed across many tumor types. So, yes, genetic testing will become more common-place, even in community practices where it isn’t as common today. Over time, every tumor patient will have a genetic test to help inform both the treatments as well as prognostic information. Dr. Mardis: Of course, it’s going to be a different answer for different people, types of tumors and access to a biopsy specimen. The paradigm here that’s quite interesting is lung cancer, because there are a large number of targeted therapies linked to genetic alterations that indicate a likeli-hood of response. It’s taken just 10 years from when mutations in the EGFR gene were first linked to responses to tyrosine kinase inhibitors to where we are offering these drugs as first-line therapy to patients with EGFR mutations. Just 10 years. With next-generation sequencing, and the increasing numbers of genes indicating targeted agents, I expect healthcare providers to turn to testing earlier in the process for more cancers.Dr. Lazarus: If I could offer a third scenario – may-be looking out 10 years – I wonder if we’re going to get to the point where we’re not even going to wait until we see solid tumors but will be able to have a degree of surveillance that we don’t have presently. With the emergence of liquid biopsies,
» There will come a day when an entire set of genetic variants found in a patient can be reliably put in electronic health records and a physician will be able to ask questions of that data in real time.«

36 37
INSIGHTS | Fast-forward
Dr. Heidi Rehm, FACMG Associate Professor of Pathology at Harvard Medical School and Director of the Laboratory for Molecular Medicine at Partners Health-care, Boston, Massachusetts.
which are much less invasive, it is very much in the realm of possibility.Dr. Mardis: That’s future-forward, but definitely a place where you’d like to be – cancer prevention as opposed to cancer treatment.
Speaking of prevention, what about testing for genetic factors that predispose people to a particular disease?
Dr. Rehm: It’s being done commonly now in fami-lies where an individual has a disease and is iden-tified as having a particular mutation. That leads to other family members being screened genetically before they develop symptoms. That’s been shown to be very effective at preventing adverse out-comes, whether it’s cardiomyopathy or breast can-cer. In some cases it may make sense even in the absence of a family history. Over the next five years, genome or exome sequencing may emerge as a common part of preventative health plans. Dr. Mardis: One limiting factor is that there aren’t enough genetic counselors to go around and deal with all of the sequencing data. When you do these tests, you can’t enter into them lightly because you don’t know what you’re going to find. What you find may be very sobering and change the patient’s life in a dramatic way. We have to be prepared in ways other than simply being able to offer the tests.

38 39
Dr. Elaine MardisProfessor of Genetics at Washington University and Director of Technology Development at the McDonnell Genome Institute, St. Louis, Missouri.
» Just having the ability to sequence a lot, in and of itself, does not solve the world’s problems. We have to be able to interpret the data and interpret it correctly. I see the next big challenge, especially in the clinical environment, coming from real data integration.«
Let’s talk about the people side. Are we ready for this genomic revolution, in terms of MDs and genetic counselors?
Dr. Mardis: There is an education issue for MDs. For genetic counselors, there just aren’t enough of them, quite frankly. It’s not a profession that attracts a lot of individuals, so there aren’t enough people to go around for all the genetic testing we’d like to do.Dr. Lazarus: From the point of view of someone who was teaching medical students and house staff for 15 years, I do wonder if we’re giving the next generation of clinicians the cognitive and lin-guistic skills they need. The majority of cancer care, for example, is in community-based centers, so those physicians have to be able to explain genetic information to patients. They can’t view the testing component as a black box. Many still view PCR that way, so with NGS as a more powerful and more mysterious tool, we need to provide insights in medical education.Dr. Rehm: I do think genetics is becoming more commonplace in medical schools. We haven’t done it perfectly, but there is a lot of effort to under-stand and support the introduction of genetics into the routine practice of medicine, as opposed to only in medical genetics clinics.

38 39
Two of you are employed in research hospitals and great universities, doing cutting-edge work. Do you expect to see a democratization of these genomic technologies?
Dr. Mardis: Clearly the goal is to democratize. If you look at current panel testing for cancer patients, for example, most people today are not getting access to these types of tests. To change this we’ve got to secure insurance reimbursement. And we need technologies that are easy to oper-ate. For example, I think devices like the Gene-Reader NGS System recently introduced by QIAGEN will aid that democratization process because it offers a fairly straightforward workflow, doesn’t require a lot of technical expertise, and delivers the back-end analysis that’s so critically needed for community-based care centers. Dr. Rehm: We’ll have to see whether these tests will be done on-site in every hospital or sent to large reference laboratories. In the beginning, academ-ic labs are the ones who typically pilot the cutting-edge technologies. They get them validated, dem-onstrate the utility and prove it to the market, then the larger reference labs pick them up for broader clinical use. At some point, a transition to more robust approaches happens with lower cost invest-ments for set up. You see that starting to happen now with panel-based tests in cancer, but exome and genome sequencing are still in cutting-edge academic labs and a small number of commercial reference labs.
How do you see bioinformatics aiding doctors for diagnoses in the future?
Dr. Rehm: There will come a day when an entire set of genetic variants found in a patient can be reliably put into electronic health records and a physician will be able to ask questions on that data in real time. You could support a physician
with a tool that allows him to ask questions the moment he’s interacting with a patient, so a patient says, “Well, Doc, I’ve had this chest pain and I’ve also had shortness of breath and I’ve been very tired.” A physician could use a bioinformatics tool to query a person’s genome at that moment – and see if genetic information might help explain the patient’s condition. But much higher quality genom-ic knowledge bases will be needed to enable this type of direct physician use.Dr. Mardis: In a tool like QIAGEN Clinical Insight, the interface puts the resources there to support the clinician. It’s not just a black and white text, it’s an ability to link out to published peer-reviewed litera-ture that supports that variant and the therapy or set of therapies. The physician can click through to read additional information, connect to clinical trials, and see the information that’s out there. It’s a supporting infrastructure for decision making rather than a directive that says, “Mutation X in Gene Y equals treatment A.” And that’s what physicians want.
What is your view on the privacy of patients’ genomic information?
Dr. Rehm: This is a really important topic, privacy and data sharing. It is challenging in research, because in the past we had de-identified access to patient data but then had to worry about wheth-er we could share important findings. I think the paradigm going forward is to consider the indi-vidual an active participant in research, to help him understand the benefits of sharing data for research, and enable the patient to drive his own data sharing, which allows a better balancing of risks and benefits that aligns with the patient’s own wishes, which are usually to increase sharing of this data.
INSIGHTS | Fast-forward

40 41
Dr. Mardis: Right now, we spend an extraordinary amount of energy, time and caution trying to pro-tect data and keep it private. If we could change the emphasis to criminalizing the misuse of data, such as for discrimination or another illegal pur-pose, that would free us to do things for medical research that we’d dearly love to do.Dr. Lazarus: At least we have established, with the Affordable Care Act in the United States, some provisions that lend themselves to protecting the patients. The abolition of prior existing condition exclusionary periods and portability of coverage, for example, are terribly important.
What roadblocks do you see to the adoption of genomic medicine?
Dr. Rehm: Right now, one of the things we’re des-perately struggling with is a lack of insurance cov-erage for genetic and genomic testing. Part of the problem is that amassing enough information on each medical indication is challenging, especially demonstrating improved outcomes and cost sav-ings. The other aspect is our inability to effectively understand much of the information we’re getting and interpret it for the patient and a physician in an accurate and understandable way.Dr. Mardis: I absolutely agree. The educational component, I think, is critically important. And to some extent, we also have to up the ante in help-ing the general public to understand the impor-tance of genomics in medicine. That’s harder, but I think it will happen over time. Dr. Lazarus: It’s also difficult for regulatory agen-cies to keep up with innovation. Next-generation sequencing is so radically different, it’s going to be
an uphill trek. And for reimbursement, the industry needs to implement those difficult trials to show clinical utility and outcomes.
Do you foresee a pivotal “next big thing“ in genomics, or more incremental expansion?
Dr. Mardis: Well, the major transformation has occurred around next-generation sequencing, but it also relies heavily on appropriate computational analysis of NGS data. Just having the ability to sequence a lot, in and of itself, does not solve the world’s problems. We have to be able to interpret the data and interpret it correctly. I see the next big challenge, especially in the clinical environment, coming from real data integration. Dr. Rehm: I wholeheartedly agree. We had a major advance with next-generation sequencing, and the incremental advances will be in the interpretive process. There was this belief that the DNA is black and white, with four letters – A, G, C, and T – and therefore whatever it tells you is true. What we know now is that, yes, it’s useful information, but it must be contextualized and combined with other information from exposures and other omic data. Developing the tools to integrate all of these pieces of information will be a critical step to informing health. Dr. Lazarus: For me, one of the next big things is the microbiome, both external and internal. Our knowledge of the interactions between microbial organisms and the immune function, as well as sur-veillance activities of the human gut, is really at the most rudimentary level. The microbiome is going to be extraordinary in what it reveals.

40 41
Dr. Tadd LazarusQIAGEN Chief Medical Officer Germantown, Maryland.
After cancer, what is the next disease that will yield to genomically-guided treatment?
Dr. Rehm: Germline genetics is an area where genetic information already is being used routine-ly. Collectively, if you add up the rare hereditary genetic disorders, they account for an enormous burden of disease. A lot of these cases are muta-tions where there is no family history, so just because it’s not in your parents or your relatives doesn’t mean it’s not genetic. Cardiomyopathy, the most common cause of sudden cardiac death under age 35, is one example. It is found in only one in 500 individuals but affects thousands of individuals.Dr. Lazarus: Autoimmune diseases are a field where clinicians very much need more insight. Diagnosis now is only at a descriptive level, so the application of NGS to autoimmune diseases is potentially very powerful. Near-term, infectious dis-ease is another area where NGS can be of great assistance. This is a very practical need we can address, the clinician’s dilemma of diagnosing sepsis and poly-microbial infections, as well as the physician’s issue, “I have good antibacterial cover-age but should I be covering for fungi?” That is sometimes the great question in severe infections and, tragically, for many patients the diagnosis only occurs post mortem.
» Autoimmune diseases are a field where clinicians very much need more insight. Diagnosis now is only at a descriptive level, so the application of NGS to autoimmune diseases is potentially very powerful.«
INSIGHTS | Fast-forward
McDonnell Genome Institute genome.wustl.edu
Partners Healthcare www.partners.org

42 43
Between two worldsSoonmyung Paik, M.D., Director of the Yonsei Biomedi-
cal Research Institute in Seoul, South Korea, is one of today’s leading pathologists in breast cancer research.
He has been especially recognized for his translational research that led to the development of a genetic test to deter-mine whether breast cancer patients can benefit from chemo-therapy. But that’s not all. Professor Paik is also a scientist who knows first hand the research landscape in both western and emerging markets of Asia. For over 35 years, he has worked in medical research, first in the United States, then during the last decade more and more in South Korea. This appears to be no coincidence. Over the last years, South Korea – along with other Asian countries – has forcefully been entering the world stage in biotechnology.
You graduated from Korea’s Yonsei University in 1981. Why did you leave your home country in order to study in the United States?
When I was in medical school, Korea really didn’t have any research infrastructure worth mentioning. There was no gov-ernment funding and medical school was for teaching. Being interested in medical research I decided to go to the U.S.
Why not Europe?
Aside from medical research I was still interested in working as a physician. I always wanted to have an impact on patient care. And I knew that in the U.S. I would have the option to do both.
Were you already interested in breast cancer pathology?
Research careers rarely develop in a straight line. In my case, in the beginning I was actually interested in brain science and molecular biology. But I ended up accepting a residency-training program at the National Surgical Adjuvant Breast and Bowel Project (NSABP) in Pittsburgh, Pennsylvania. It was more serendipity than anything else.
Serendipity?
Almost every other school rejected me. The climate back then was extremely unfavorable to foreign medical graduates. Pittsburgh was one of only two hospitals that accepted me.
Did you start out doing genetic research there?
No. At NSABP from 1982 to 1984, I studied many, many slides of biological tissue trying to find chemical markers for different kinds of cancer. We were not dealing with molecu-lar medicine at the time.
When did genetic testing come up?
After three years in Pittsburgh, I wanted broader molecular training. So I decided to go to the State University of New York. First I did neuropathology, trying to find a molecular marker for HIV in brain tissue. We created a lot of plasmids using ultracentrifugation – each time, it took more than a week – and if QIAGEN’s purification kit had existed back then, it would have made everybody’s life a lot easier. At the same time, I became more interested in the pathology of
by Hubertus Breuer

42 43

44 45
Being a cancer survivor himself, Prof. Paik’s work focuses on improving the therapy of breast cancer, the most frequent malignancy among women.
With 155 research institutes and more than 28,000 students, the Yonsei University is one of the most renowned colleges in South Korea.

44 45
INSIGHTS | Between two worlds
» I always wanted to have an impact on patient care.«
breast cancer. So after two years I moved on – I worked in labs run by breast cancer researchers Marc Lippman at the National Cancer Institute and then at the Georgetown Univer-sity. The focus of my work at those places was to develop tests for biomarkers in cancers that allow planning treatment. But I realized that the best way to do this was to work with the breast cancer tissue collections at the NSABP rather than using established cancer cell lines, and so in 1996 I went back as co-director and later director in pathology.
Is this when you developed the OncotypeDX test?
The idea of a test was always there, but it took until 2004 for it to see the light of day. It was based on many studies and clinical trials. The central idea behind it is that not all women with early-stage breast cancer benefit from chemotherapy. But some do. This test measures the expression of 21 genes in breast cancer tissue in order to discover who may benefit. It also gives an estimate for the cancer’s chance of recurrence.
Do you use QIAGEN products for this research?
Sure, we use them all the time, especially for nucleic acid extraction. QIAGEN sets the standard here. Can we even imagine extracting RNA from 2,000 cases using ultracentri-fugation?
OncotypeDX sounds like an early step in the direction of “preci-sion medicine.”
Yes, that’s true. But as popular as this idea is, today it would be much harder to develop. Back then, I could fairly easily evaluate a test in a clinical trial; today in the U.S. trials are under intense regulatory scrutiny after a cancer researcher at Duke University fabricated data. Thinking back, our work would have been much more challenging in the current envi-ronment.
Did this prompt you to go back to South Korea?
The connection was rekindled earlier. At the end of 1999 I was diagnosed with gastric cancer – and a colleague of mine at Yonsei University in South Korea was familiar with the operation. While I was still recovering in the ward, researchers from the oncology department asked me to help them with a grant application. South Korea had just begun to spend a lot more money on biomedical research back then. This one was for US$ 10 million for ten years. They got the grant and that started our collaboration. So once I felt that the research environment was gaining momentum, Korea became more attractive to me.
Can you do better research in South Korea?
Don’t get me wrong: There are problems here, too – for example, you have a genomics initiative pushed by the gov-ernment, but it is mainly simply about sequencing. But you need more – sequencing should be tied to clinical trials for targeting genetic markers. We need a national infrastructure for clinical genome sequencing.
But doesn’t more money for research help?
Yes. But currently the funding is too much tied to the idea of creating commercial products within two to three years, or to producing papers. A talented young researcher should not be constrained by that. I understand that a government has to justify expenditure, but they should think more long-term.
How does South Korea compare in biomedical research with other countries in the region, like Japan or China?
Japan is investing soundly as far as I can tell; we are at least a decade behind them. China is also doing well, as it has many researchers who were trained in the U.S. and are coming back and bringing an entrepreneurial spirit with them.
Prof. Dr. Soonmyung Paik Director of the Yonsei Biomedical Research Institute, Seoul, South Korea.
Yonsei University Health System www.yuhs.or.kr/en/

46 47
On callQIAGEN’s commitment is to deliver state-of-the-art service for every customer. More than 550 service experts are eager to respond – no matter when or where – even to the most challenging requests. When customers achieve results in ways that exceed their own expectations, we have done our job.
98 %of all standard orders are fulfilled within 24 hours of receipt.
of the world’s countries are currently supported by our global distribution network.
133
40,000customer requests a year are handled by our field service.
46

46 47
INSIGHTS | On call
75,000customer e-mails are answered each year.
or 12 % of our employees are providing service to customers.
550250,000customer contacts annually are conducted by our teams.
100,000incoming calls are answered each year.
millionkits were shipped to our customers in 2015.2.7
47

48 MF
Corporate Communications
FOR INVESTORS
Phone worldwide: + 49 2103 29 11711 Phone U.S.: + 1 240 686 2222 Email: [email protected] ir.qiagen.com
FOR MEDIA
Phone worldwide: + 49 2103 29 11826 Phone U.S.: + 1 240 686 7425 Email: pr @ qiagen.com pr.qiagen.com
QIAGEN on the Web
www.qiagen.com www.facebook.com /QIAGEN
www.twitter.com /QIAGEN www.linkedin.com/company/QIAGEN www.youtube.com/QIAGEN
Imprint
Credits
CONCEPT AND DESIGN
3st kommunikation, Mainz www.3st.de
PRINTING
Eberl Print GmbH www.eberl.de
PHOTOGRAPHY
Andreas Fechner Jun Michael ParkUPS Shutterstockgettyimages
EDITOR
Przemyslaw Jedrysik
Publication Date
February 2016
Trademarks
Our name together with our logo is registered as a trademark in the United States and a number of other countries: QIAGEN®.
For a complete list of QIAGEN’s trade-marks and disclaimers, please refer to QIAGEN’s webpage under www.qiagen.com/trademarks_disclaimers.aspx
In this annual report QIAGEN uses the term molecular diagnostics. The use of this term is in reference to certain countries, such as the United States, limited to products subject to regulatory requirements. As of February 2016, QIAGEN molecular diagnostics products included 18 FDA (PMA approved or 510k cleared) products, 17 clinical sample concentrator products (13 kits and 4 instruments), 70 EU CE IVD assays, 10 EU CE IVD sample preparation products, 21 EU CE IVD instruments for sample purification or detection, 32 China CFDA IVD assays and 11 China CFDA IVD instruments.
This Annual Report may also contain trade names or trademarks of companies other than QIAGEN.
© 2016 QIAGEN, all rights reserved.
This document contains detailed financial information about QIAGEN prepared under generally accepted accounting standards in the U.S. (U.S. GAAP) and included in our Form 20-F annual report filed with the U.S. Securities and Ex change Commission. QIAGEN also publishes an Annual Report under IFRS accounting standards, which is available on our website at www.qiagen.com.
carbon neutralnatureOffice.com | DE-141-826726
print production

QIAGEN at a Glance
Product Categories Percentage share of 2015 net sales
Molecular Diagnostics Physicians, hospitals and health care providers use QIAGEN technologies to save lives and fight disease. Our products support disease prevention such as screening women for risk of cervical cancer; profiling patients to pinpoint many diseases; personalized healthcare to guide treatment decisions; and point-of-need testing to provide on-site diagnosis.
Academia Researchers at life science laboratories around the world depend on QIAGEN to advance our understanding of the molecular basis of life. Customers include universities and research institutes.
Applied Testing Professionals in fields such as human identification and forensics, food testing and veterinary medicine use QIAGEN technologies in commercial applica-tions beyond human healthcare. Our products are helping to solve crimes, secure food supplies and detect potentially devastating livestock diseases.
Pharma Scientists in the phar maceutical and biotechnology industries look to QIAGEN to advance gene-based drug discovery and development, supporting the crea-tion of new medical breakthroughs.
Instruments are used with consumables, enabling customers to automate processes from the preparation of clinical samples to the delivery of valuable results.
87 %
13 %
Consumables and related productsare specialized kits that contain all necessary materials to support the use of sample and / or assay technologies as well as bioinformatics solutions for analysis, interpretation and reporting of biological data.
50 %Molecular Diagnostics
9 %Applied Testing
19 %Pharma
22 %Academia
Customer Classes Percentage share of 2015 net sales

INSI
GH
TS —
TH
E Q
IAG
EN M
AG
AZ
INE
WWW.QIAGEN.COM 1101132