the malnutrition universal screening tool (must) · nutrition support in adults: oral nutrition...
TRANSCRIPT

RATIONALE
The Malnutrition Universal Screening Tool (MUST) is now recommended best practice within the Trust as a way to screen patients’ to identify and treat adults at risk of malnutrition in the community. This follows publication of the NICE guidelines for ‘Nutritional Support in Adults’ in February 2006. The MUST is a simple 5 step screening tool which will help to identify adults who are underweight and at risk of malnutrition. Although the term malnutrition can refer to both under and over nutrition, it is used here to refer to under nutrition. In the community, MUST screening scores show that appropriate early nutritional intervention improves outcomes and can reduce GP visits and hospital admissions due to malnutrition associated complications. (MAG, BAPEN 2003) As with all screening tools, clinicians should use this tool to aid and inform their own professional judgement. TARGET GROUP All registered nurses employed by the Trust who provide clinical care for patients in the community setting are required to follow this protocol as part of their role and job description. AIM All community nurses will use this tool to screen for a patients’ potential risk of malnutrition when a full assessment is required or there is a clinical concern. This will indicate if a patient is at risk or potentially at risk, and may benefit from appropriate nutritional intervention. It is a procedure used by staff so that clear guidelines for action can be implemented and appropriate nutritional advice provided. It is a screening tool and is not intended to replace clinical judgement. The MUST tool can be used for patients in whom height and weight are not normally obtainable, as a range of alternative measurements can be used. Screening will need to be repeated at a frequency determined in the care plan.
CLINICAL PROTOCOL
THE MALNUTRITION UNIVERSAL SCREENING TOOL
(MUST)

Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 2/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service
SUMMARY OF THE 5 MUST STEPS STEP 1 Gather nutritional assessments (Height/ Weight/ BMI). If it is not possible to obtain height and weight, use alternative measurements. STEP 2 Note % recent unplanned weight loss and score. STEP 3 Establish acute disease effect. STEP 4 Determine the overall risk score of malnutrition. STEP 5 Use local management guidelines for patients identified as low, medium or high STEP 1 Calculate the Body mass index (BMI) score using the BMI chart. To obtain this you will need the following: Height Use a height stick/ chart where possible. Measure patient without shoes, heels against the height stick or wall chart. Read and document height on MUST score sheet. Weight
Ulna length
Use clinical scales. Check scales have been calibrated and read zero prior to patient standing on them. Weigh subject in light clothing and without shoes. Read and document weight on MUST score sheet. If unable to accurately weigh or measure height of patient, use a recently documented or self reported weight and height (if realistic and reliable). If height cannot be measured or is unknown use one of the following measurements to calculate height:
Knee height Demispan (do not use if patient has severe or obvious curvature of the spine)
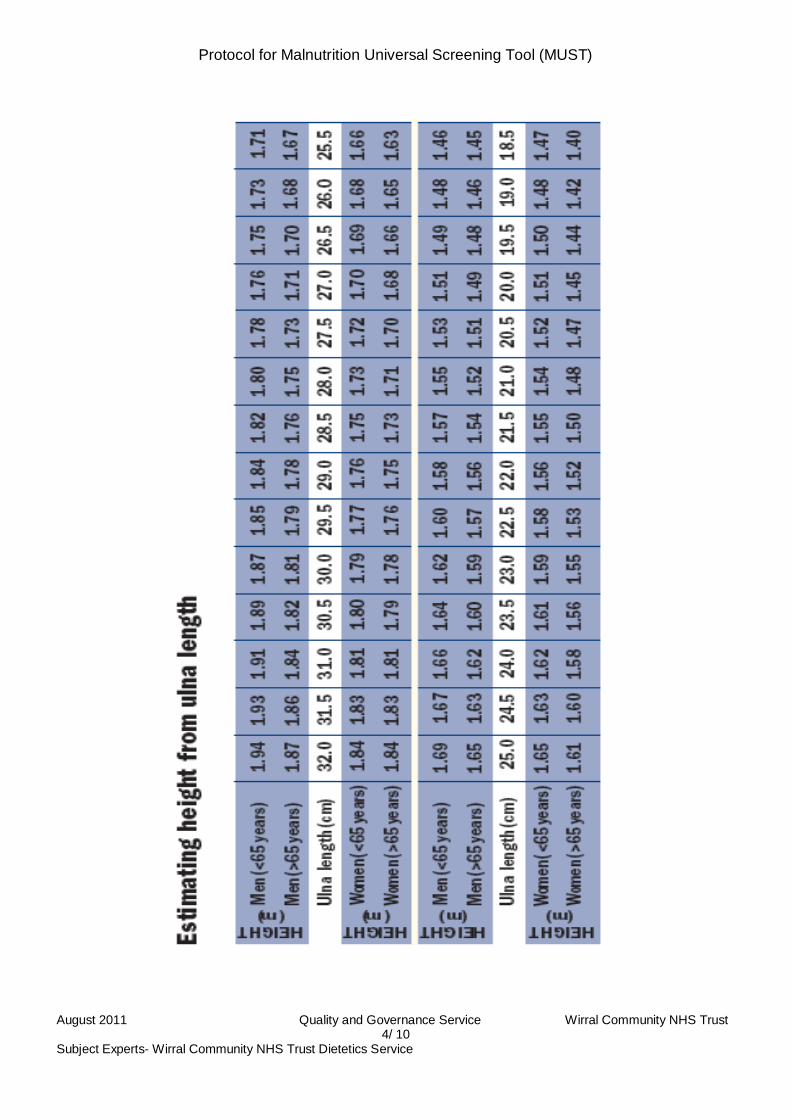
For patients who are bed bound, those with severe disabilities and those with kyphosis or scoliosis, it is preferable to use ulna length to estimate height. Measuring Ulna Length Ask patient to bend an arm (left side if possible) palm across chest, fingers pointing to
opposite shoulder Using a tape measure, measure the length in centimetres (cm) between the point of the
elbow (olecranon) and the mid-point of the prominent bone of the wrist (styloid process) Use table on page 5 to convert ulna length (cm) to height (m) and document

Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 3/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service
Measuring Knee Height Measure left leg if possible Ask patient to sit on a chair; without footwear, with knee at a right angle Hold tape measure between 3rd and 4th
Place hand flat across subjects thigh, about 4 cm behind the front of the knee fingers with zero reading underneath fingers
Extend the tape measure straight down the side of the leg in line with the bony prominence at the ankle (lateral malleolus) to the base of the heel
Use table on page 6 to convert knee height (cm) to height (m) and document Measuring Demispan Ask patient to stand if possible Locate the mid point of the sternal notch (V at the base of the neck) Ask patient to raise right arm until it is horizontal with the shoulder, making sure the wrist is
straight Place a tape measure between the middle and ring finger of the patients right hand, with zero
at the base of the fingers Extend the tape measure along the length of the arm to the mid point of the sternal notch Use table on page 7 to convert demispan length (cm) to height (m) and document
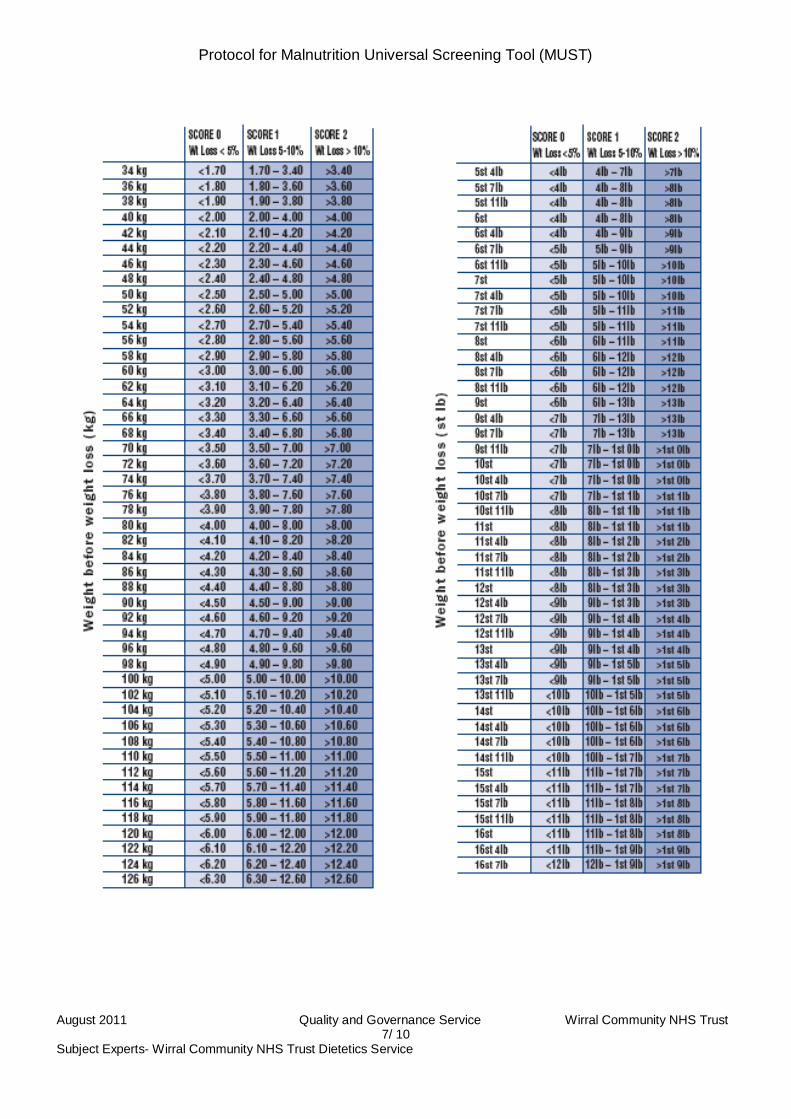
STEP 2 Establish patients weight loss score. This can be achieved by comparing the current weight against a previous weight from the last 3 – 6 months. If there has been no weight loss or there has been an increase score 0. If there has been a weight loss, look up Kg of weight lost on weight loss tables on page 8. Score accordingly. If weight loss 0 - 5% score 0 If weight loss 5 - 10% score 1 If weight loss > 10 % score 2 STEP 3 Establish acute disease effect score. If patient is acutely ill and there has been or is likely to be no nutritional intake for more than 5 days, they are likely to be at nutritional risk. Score 2. STEP 4 Establish overall risk of malnutrition. Add scores from steps 1, 2 and 3 together to give overall risk of malnutrition and document on pressure ulcer and nutrition risk assessment.
Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 4/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service

Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 5/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service

Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 6/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service
Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 7/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service

Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 8/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service

Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 9/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service
Step 5 MANAG E ME NT G UIDE L INE S Record overall risk score on MUST documentation Score 0 = Low Risk Low risk indicates adequately nourished. Therefore no action necessary, repeat screening at intervals dependant on clinical concern.
Initiate generic care plan for nutrition (on intranet site)
Score 1 = Medium Risk Medium risk indicates a medium risk of malnutrition.
Weigh patient weekly (record rational in health records if not feasible) Repeat screening after 4 weeks Evaluate care plan after 4 weeks If weight has been gained or remains stable repeat screening every 2-3 months in the
community
Initiate generic care plan for nutrition (on intranet site)
Score 2 = High Risk High risk indicates a high risk of malnutrition.
Weigh patient weekly (record rational in health records if not feasible) Repeat screening after 4 weeks Evaluate care plan after 4 weeks Make referral to dietitian if no improvement after 4 weeks Repeat screening monthly in community
C L INIC AL R E F E R R AL S If there is extreme concern by a community nurse regarding a patient’s nutritional status within the first 4 week monitoring period then it is essential to refer to an appropriate practitioner e.g. dietitian or general practitioner. NUT R IT ION S UP P OR T Treatment and care should take into account patients’ needs and preferences. Good communication is essential between the community nurse and patient when discussing and establishing a plan for nutrition support. Patients’ should have the opportunity to make informed decisions about their care and treatment. This should be tailored to the patients needs and documented on their nutritional care plan. Community nurses should educate patients and their carers that food and fluid of adequate quantity and quality in an environment conducive to eating are an important part of nutritional support. Patients’ may require modified eating aids, for those who can potentially chew and swallow but are unable to feed themselves.

Protocol for Malnutrition Universal Screening Tool (MUST)
August 2011 Quality and Governance Service Wirral Community NHS Trust 10/ 10
Subject Experts- Wirral Community NHS Trust Dietetics Service
HOME E QUIP ME NT If patient has a hoist, contact Community Equipment Service to request hoist scales Staff need to use scales belonging the Trust that are subject to quality assurance through re calibration checks. R E F E R E NC E S / B IB L IOG R AP HY BAPEN (2003).The ‘MUST’ explanatory booklet: A guide to the ‘Malnutrition Universal Screening Tool’ (‘MUST’) for adults. British Association for Parental and Enteral Nutrition, Redditch. Wirral Community NHS Trust (2008). Guidelines for best practice in the Identification and Treatment of Malnutrition in Adults. Wirral Community Nutrition and Dietetic Service. Wirral Community NHS Trust (2009). Guide to using the malnutrition universal screening tool (MUST: Community nursing training pack. Wirral Community Nutrition and Dietetic Service. NICE (2006). Nutrition support in adults: Oral nutrition support, enteral tube feeding and parental nutrition. National Institute for Health and Clinical Excellence, London. www.bapen.org.uk