the marik protocol final 2017 -...
TRANSCRIPT
Metabolicresuscitationinsepsis
KElfituriNov2017

Declaration
• FinancialsupportandsponsorshipNil
• ConflictsofinterestTherearenoconflictsofinterest

Outlines
• Verybriefoverviewofthescientificrationale• WhydoesVitaminC help?• WhydoesThiamine help?• VitaminCdeficiencycausesclinicaldisease• Thiaminedeficiencycausesclinicaldisease• ClinicalstudiesofIVVitaminC:• ClinicalstudiesofThiamine:• Marikprotocol• Takehomemessage

Verybriefoverviewofthescientificrationale• SepticpatientsareinvariablydeficientinVitaminC,andfrequentlydeficientinthiamine.
• DeficienciesinVitaminCandthiaminemightexplainmanyoftheabnormalitiesseeninsepsis.
• VitaminCandthiaminehaveanoutstandingtrackrecordofsafety,provenoverdecadesofexperimentationandclinicalexperience.

Verybriefoverviewofthescientificrationale
• ManyRCTshavesuggestedbenefitfromVitaminCorthiamineincriticallyillpatients,withnoevidenceoftoxicity.
• Arecentbefore-afterstudyfoundasubstantialmortalitybenefitfromthecombinationofstress-dosesteroid,IVvitaminC,andIVthiamine.Althoughthisisn'tanRCT,theresultsarequitestriking.
• Furtherresearchisrequired,butintheinterimthisisareasonableinterventiongiventheexcellentsafetyprofileoftheseagents.

VitaminC
Why does VitaminC help?

Why does VitaminC help?
• Antioxidant:qScavengesROSandRNS,qpreventsendothelialdamageqmaintainingmicrovascularintegrity
Why does VitaminC help?
• SynthesisofcatecholaminesActsascofactorinsynthesisofepinephrine,dopamine,andvasopressinallowingformaintenanceofvasculartoneandcardiacoutputqdopaminebeta-hydroxylase ,Thisenzymeconvertsdopamineintoepinephrine
qRate-limitingstepofsynthesising L-DOPA,theprecursorofdopamine

Why does VitaminC help?

Why does VitaminC help?
• ImmunefunctionqSupportslymphocyticproliferation,qassistsinneutrophilickillingofbacteria,qimproveschemotaxisqInhibitsNF-KBactivation

Journal Name: BiofactorsReview Article Title :Mechanism of action of vitamin C in sepsis: Ascorbate modulates redox signaling in endotheliumAuthors: Wilson et al 2009• Conclusion/Recommendation:• VitaminCdeficiencycorrelateswithmultiorgan failureanddeath
• microvascularfunctionmaybeimprovedinsepsisbyparenteraladministrationofascorbateasanadjuvanttherapy

Why does Thiamine help?

Why does Thiamine help? • Thiamine deficiencyiscommoninsepsis,occurringinperhapsone-thirdofpatients.Thisisassociatedwithincreasedmortality(Manganese2011).
• isacriticalco-factorintheglyocolysis andoxidativedecarboxylationofcarbohydratesforenergyproduction.
• ShuntsmetabolismofvitaminCawayfromoxalate(potentialforrenalcrystallisation)

Journal Name: Curr Opin Clin Nutr Metab CareReview Article title :Thiamine supplementation in the critically illAuthors: Manganese 2011
• depletionisfrequentlyunrecognisedandunderdiagnosedbyclinicians.
• Potentiallydeleteriousconsequencesofthiaminedepletionshouldbeavoidedbyearlyandappropriatesupplementation

Why does Thiamine help?

Why does Thiamine help?

Why does Thiamine help?
• ShuntsmetabolismofvitaminCawayfromoxalate(potentialforrenalcrystallisation)

VitaminCdeficiencycausesclinicaldisease

Vitamindeficiencycausesclinicaldisease• VitaminCdeficiencycausesscurvy.• VitaminCisimportantforthemaintenanceofendothelialboundaries,withedemanotedinscurvy.
• VitaminCisalsorequiredforthesynthesisofcatecholamines andcortisol,sodeficiencycausesfailureofthesympatheticnervoussystem.

scurvy

Thiaminedeficiencycausesclinicaldisease
Vitamindeficiencycausesclinicaldisease
• ThiaminedeficiencymaycauseqDelirium
(Wernicke'sencephalopathy)and
qcardiacdysfunction(Beriberi).Beriberiinparticularcanmimicsepsis,bycausingdistributiveshockandlacticacidosis.

Wernicke'sencephalopathy

Beriberi

Beriberi
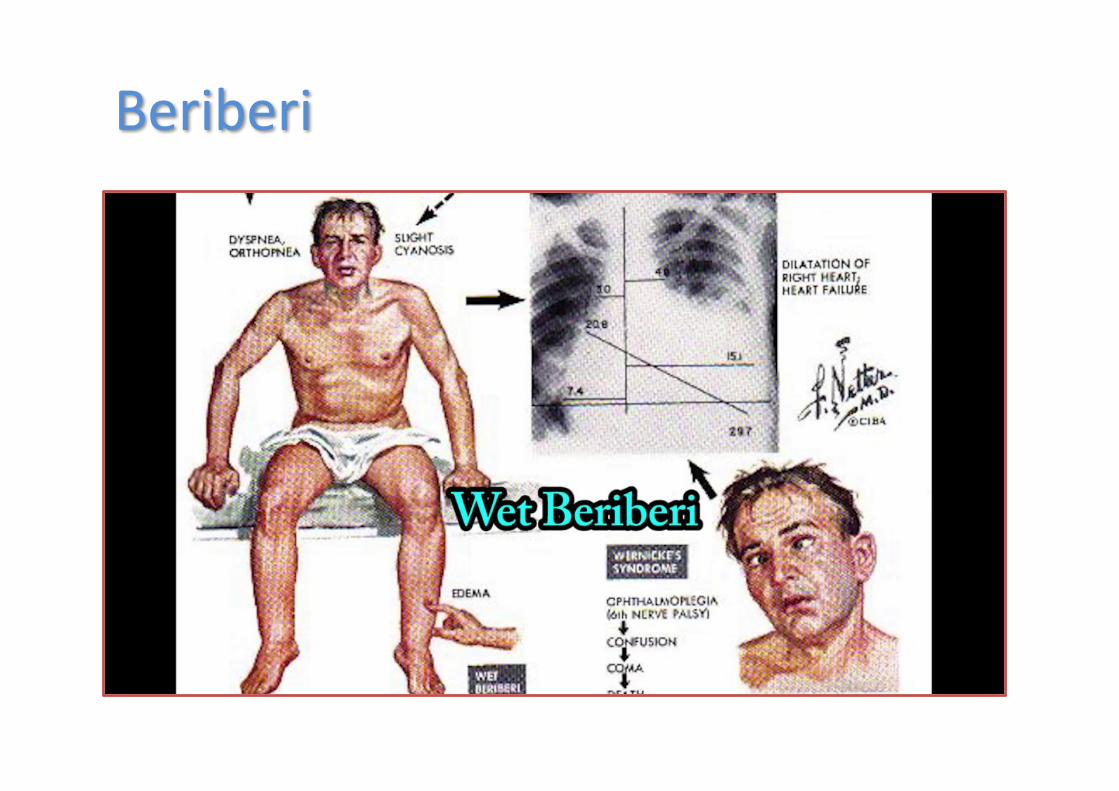
Beriberi

ClinicalstudiesofIVVitaminC:

WhyIV?
IntestinalabsorptionofvitaminCis saturable

ClinicalstudiesofIVvitaminCincardiacpatients

ClinicalstudiesofIVvitaminCincriticallyillpatients:

JournalName:JAMAsurgeryStudyTitle:ReductionofresuscitationfluidvolumesinseverelyburnedpatientsusingascorbicacidadministrationAuthors :TanakaHetal,2000• Studytype,number: N37
AprospectiveRCTinvolvingpatientswithmajorburns(>30%bodysurfacearea).
• Methodology:PatientswererandomizedregardingwhetherornottoreceiveAninfusionofIVvitaminC,66mg/kg/hrforthefirst24hoursofhospitalisation.
TanakaHetal,2000
• Results: patientsinthevitaminCgrouprequiredq lessfluidresuscitation,q hadhigherurineoutput,andq developedlesswoundedema
• Conclusion/Recommendation:• thistranslatedinto
q improvedoxygenationandq lesstimeonmechanicalventilationamongthe
VitaminCgroup(averageof12vs.21daysofventilation,p=0.03).

JournalName:AnnSurgStudyTitle :Randomized,prospectivetrialofantioxidantsupplementationincriticallyillsurgicalpatientsAuthors: Nathens ABetal.2002
• Studytype,number:595Randomized,prospectivetrial
• Methodology:TheyrandomisedpatientsshortlyafteradmissiontotheICUtonotherapyvs.acombinationofenteralvitaminEplusIVvitaminC1000mgq8hruntilICUdischarge

Nathens ABetal.2002
• Results:patientstreatedwithvitaminsEandCfaredbetteronavarietyofsecondaryendpointsincluding
qlesstimeontheventilatorandqlessmultiorganfailure
• Conclusion/Recommendation:prophylacticantioxidantsprovidedtosurgicalICUpatientscouldreducepulmonarycomplications
JournalName:JTranslMedStudyTitle :PhaseIsafetytrialofintravenousascorbicacidinpatientswithseveresepsisAuthors: FowlerAetal.2014
• Studytype,number:N24SingleCentre,PRDPCTInvolvingpatientswithseveresepsisinamedicalICU
• Methodology:patientswererandomisedtoreceive
§ placebo,§ low-dosevitaminC(12.5mg/kgIVq6hr),or§ high-dosevitaminC(50mg/kgIVq6hr).

FowlerAetal.2014
• Results:Theprimaryendpointwassafetyandtolerability,withnoadverseeventsnoted
• Conclusion/Recommendation:PatientstreatedwithvitaminCexperienceda
q dose-dependentimprovementinSOFAscoreovertime
q Improvedinflammatorymarkers

JournalName:J Pulm Respir Med,StudyTitle:Impact of intravenous ascorbic acid infusion on novel biomarkers in patients with severe sepsisAuthors :Natarajanetal2014
• Studytype,number: N24Singlecentre,retrospectiverandomized
• Methodology:50 mg/kgor200 mg/kgIVinfusionevery24 h

Natarajanetal2014
• Results:• Conclusion/Recommendation:
q Decreaseinbiomarkersofsepsis(cf-DNAandmtDNA)and
q DecreaseinRDW

JournalName:JResPharmPractStudyTitle:Effectofhigh-doseascorbicacidonvasopressorrequirementinsepticshockAuthors :Zabet MHetal2016
• Studytype,number: N28Singlecentre,DBRCT
• Methodology:AsurgicalICUwithvasopressor-dependentsepticshockwererandomizedtoreceiveplacebovs.VitaminC25mg/kgIVq6hr.
Zabet MHetal2016
• Results:• Conclusion/Recommendation:Reductionin
qvasopressordoseandqvasopressordurationqmortalityamongpatientstreatedwithVitaminC.

ClinicalstudiesofThiamine:

JournalName:Crit CareMedStudyTitleRandomized,double-blind,placebo-controlledtrialofthiamineasametabolicresuscitatorinsepticshock:ApilotstudyAuthors: DonningMW2016
• Studytype,number88patientswithsepticshockRandomised,double-blind,placebo- controlledtrial
Methodology:Investigatingtheeffectofthiamine(200mgIVq12hr)Endpoint:Lactatelevels,timetoshockreversal,SOI,mortality
DonningMW2016
• Results:– Nodifferenceinoverallgroups– Inpatientswithbaselinethiaminedeficiency(35%oftotal):
• Lowerlactate• Decreasedmortality
Conclusion/Recommendation:Withinthispre-specifiedsubgroup,thiamineadministrationdidreducelactatelevelsandmortality

Clinical studies of Thiamine:


• PaulMarik,MBBCh• ChiefofPulmonaryandCriticalCareMedicine

Marik protocol

WhatHeDid:
• ElectronicHeathRecord(EHR)Retrospectivebefore-afterclinicalstudy
• Comparedtheclinicalcourseandoutcomeofconsecutiveseveresepsis(maybeclarifythatthisisthenewdefinition?)andsepticshockpatientsandaprocalcitonin(PCT) ≥2ng/mL:

MarikProtocolcont¢d
• DesignqRetrospectiveobservationalstudyqSinglecentred
• SettingqSinglecentreinUSqJanuary– July2016

MarikProtocolcont¢d
TreatmentGroup• Treatedwithstandardsepsiscare
+q IntravenousvitaminC,q Hydrocortisone andq Thiaminewithin24hoursofICUadmission
ControlGroup:• Treatedwithstandardsepsiscareonly.

StandardICUCare:
• Empiricbroadspectrumantibioticsgivinginitially,whichwerede-escalatedaccordingtomicrobiologicaldataandclinicalprogress
• Conservativephysiologic fluidbasedtherapy• Intravenoushydrocortisone 50mgq6hr• Lungprotectivestrategyandavoidanceofhyperoxia
• Limiteduseof sedativeagents(dexmedetomidinewasthepreferredagent)

MarikProtocolcont¢d
• Norepinephrine wasthevasopressorofchoice(titratedtoadoseof20ug/mintargetingaMAP>65mmHg)
• Ifneeded,thenextvasopressoraddedwasvasopressin at0.04U/min,followednextwithbyphenylephrine orepinephrine
• Enteralnutritionwasinitiated24hoursafterICUadmissionandclinicalstabilityachieved
• DVTprophylaxiswithenoxaparin (orheparininpatientswithcreatinine clearance<30ml/min)andsequentialcompressiondevices

VitaminC(Marik)TreatmentProtocol:
• StandardICUcareplus:• IntravenousvitaminC1.5gq6hrx4doruntilICUdischarge
• Hydrocortisone 50mgq6hrx7doruntilICUdischargefollowedbyataperover3d
• Intravenousthiamine 200mgq12hrx4oruntilICUdischarge

Outcomes:• Primary:Hospitalsurvival• Secondary:
– Durationofvasopressortherapy– Requirementforrenalreplacementtherapy(RRT)inpatientswithAKI
– ICUlengthofstay– Changeinserumprocalcitonin(PCT)– ChangeinSOFAscoreoverthefirst72hours

Outcomes:

Figure 1

NNTfordeathwas3.1inthisstudy,roundedupto4treatedpatientstoavoidonedeath
Figure 2
CHEST 2017 151, 1229-1238DOI: (10.1016/j.chest.2016.11.036)

Figure 4
CHEST 2017 151, 1229-1238DOI: (10.1016/j.chest.2016.11.036) Copyright © 2016 American College of Chest Physicians Terms and Conditions

Figure 3
CHEST 2017 151, 1229-1238DOI: (10.1016/j.chest.2016.11.036) Copyright © 2016 American College of Chest Physicians Terms and Conditions

Strengths:
• Nodifferenceinbaselinecharacteristicsbetweengroups
• Consecutivepatientsenrolled• Thestudiedinterventionswerecheap,seeminglysafe andreadilyavailable.However,vitaminCtoxicitycancauserenalfailureandthesafetyprofilewouldbebestevaluatedinthecontextofanRCT
Strengthscont‘d
• Thiswasthefirststudytoevaluatethecombination ofintravenousvitaminC,hydrocortisone,andthiamine
• Aninterestinghypothesisgeneratingstudywhichhassomebiologicallyplausibleexplanationsforbenefitinsepsis

Limitations:
• NotaRCT• Smallsamplesize• Onlyasinglecenterstudy• Useofnon-concurrentcontrols(i.e.,patientswerenotevaluatedduringthesametimeframe)
• PCTisnotreadilyavailableateveryhospital

Limitationscont‘d
• Multipleinterventionsandthereforenotpossibletodeterminewhich,ifany,areassociatedwithimprovedoutcome
• 60%ofpatientsinthecontrolgroupweretreatedwithcorticosteroids
• Details areprovidedfortheunderlyingreasonfordeath(includingadvanceddementia,severeheartfailure,advancedsarcoidosis andsevereCOPD)butnotforthecontrolgroup

Discussion:
• SepsisrelateddeathNopatientsinthetreatmentgroupdiedfromcomplicationsrelatedtosepsis,rathertheirmortalitywassecondarytocomplicationsoftheirunderlyingdisease

Discussioncont’d
• PCTPCT typicallydecreasesinalinearfashioninpatientswithseveresepsis(sepsis?)_andsepticshock,reachingabout30%oftheirbaselinevaluewithin72hours.
• Afallgreaterthan30%over72hoursusuallyindicatesimprovedsurvival

Discussioncont’d
• Synergisticeffects:•Combinationof
qVitaminCqThiamineandqHydrocortisone
↓ Vaso-plegic shock↓ Vasopressorduration

Discussioncont’d
• Vit CdoseTheexactdosingstrategyforVitaminCisunknown,asitisnotbeenwellstudied.Theauthorsconcludethatupto6gramsdailyshouldbeenoughwithoutrunningtheriskofconversiontooxalateandpotentiallycausingworseningrenalimpairmentfromoxalatecrystalformationandrenaldeposition.

TheBottomLine
• Thisstudyishypothesisgenerating.• AnRCTisrequiredtodeterminetheefficacyofvitaminC,steroidsandthiamineinseveresepsisandsepticshock.

Aretherepotentialharms?VitaminCqVitaminCqcalciumoxalatenephropathyqpro-oxidanteffect

Aretherepotentialharms?
qCalciumoxalatenephropathyqDose-dependenttoxicityqHigherdoses>40grams/day;(Buehner 2016)
qConcurrentuseofthiamineshouldreducetheconversionofvitaminCintooxalate

Aretherepotentialharms?
• pro-oxidanteffect.qThiswasshownnottooccurevenatadoseof7.5gramsIVdaily(Muhlhofer 2004).
Aretherepotentialharms?Thiamine• Thiamine:Rarereportsof
q hypersensitivityorq anaphylaxis,especiallywithrepeatedinjections

Aretherepotentialharms?Steroids• Steroids
qHYPRESSTrialqCORTICUSTrialqAnnaneTrialqTheVANISHtrialqTheADRENALtrial

JournalName: JournaloftheAmericanMedicalAssociation.StudyTitle :"Effectofhydrocortisoneondevelopmentofshockamongpatientswithseveresepsis"Authors: Keh D,etal, 2016HYPRESS• Studytype:number: N=380• Multicenter,placebo-controlled,double-blindRCT• Setting:34sitesinGermany• Enrollment:January13,2009toAugust27,2013• Methodology:
• IVhydrocortisone(n=190)• Placebo(n=190)

HYPRESS
• Results:Conclusion/Recommendation:• SubgroupAnalysis
Therewasnosignificantdifferenceregardingtheprimaryandsecondaryendpointsbetweenthosewithandwithoutrelativeadrenalinsufficiencywhoreceivedhydrocortisoneversusplacebo
• AdverseEvents– Secondaryinfection40(21.5%)vs.32(16.9%)(P=0.26)– Hyperglycaemia 169(90.9%)vs.154(81.5%)(P=0.009)
JournalName:New EnglandJournalofMedicine.2008StudyTitle :"Hydrocortisonetherapyforpatientswithsepticshock"Authors:SprungCL,etal CORTICUS
• Studytype:number:N=499Multicenter,double-blind,parallel-group,randomized,placebo-controlledtrial
• Methodology:N=499
• Hydrocortisone(n=251)• Placebo(n=248)
Meanfollow-up:28days

CORTICUS
• AdverseEvents• NewsepsisorsepticshockOR1.37;95%CI1.05-1.79;NNH26
• Newshock6%vs.2%(OR2.78;95%CI1.02-7.58;NNH25)
• Hyperglycemia 85%vs.72%(OR1.18;95%CI1.07-1.31;NNH8)
• Hypernatremia29%vs.18%(OR1.59;95%CI1.13-2.22;NNH9)

JournalName:Journal oftheAmericanMedicalAssociation.StudyTitle :"Effectoftreatmentwithlowdosesofhydrocortisoneandfludrocortisoneonmortalityinpatientswithsepticshock“Authors:AnnaneD,etal, 2010AnnaneTrial
• Studytype:number: N=300• Randomized,prospective,double-blind,parallel-group,placebo-controlled
trial• Sites:19FrenchICUs• Timeline:1995-1999• Methodology:• N=300patientswithsepticshock
– Corticosteroids(n=151)– Placebo(n=149)

AnnaneTrial
• AdverseEventsTherewasnodifferenceintherateofadverseeventsbetweentheplaceboandsteroidgroupsexceptforahigherrateofsurgicalwoundinfectionintheplacebogroup.

JournalName: JAMA.2016.StudyTitle :EffectofEarlyVasopressinvsNorepinephrineonKidneyFailureinPatientsWithSepticShockTheVANISHRandomizedClinicalTrialAuthors:Gordonetal.2016 VANISH
• Studytype:number: N=400• Factorial(2×2)multicentre,doubleblind,RCT• 18adultgeneralICU’s• February2013– May2015
• Methodology:Patientswererandomlyallocatedtoq vasopressin(titratedupto0.06U/min)andhydrocortisone(n = 101),q vasopressinandplacebo(n = 104),q norepinephrineandhydrocortisone(n = 101),orq norepinephrineandplacebo(n = 103).

VANISH
• Seriousadverseevents(includingdigitalormesentericischaemia,life-threateningarrhythmiaandacutecoronarysyndrome)10.7%inthevasopressingroupvs8.3%inthenorepinephrinegroup;difference,2.5%[95%CI,−3.3%to8.2%]
• Nodifferenceinrenalfailure–freedays• Nodifferenceinmortality

Aretherepotentialharms?
All3studies,plusVANISHTrial,showednomortalityincreasewithsteroids

JournalName: EstimatedStudyCompletionDate:December30,2017
StudyTitle :ADjunctive coRticosteroid trEatment iN criticAlly ilLPatientsWithSepticShock(ADRENAL)Authors:Balasubramanian Venkatesh (ADRENAL)
• Studytype:number: 3800patients• amulti-centre,randomised,blinded,placebocontrolledtrial• 70IntensiveCareUnitsrecruitmentcompleted.• Followupofpatientscontinue.• Methodology:• Eligiblepatientswillberandomisedtoreceiveeither
intravenoushydrocortisone200mgorplaceboperdayforsevendays

ANAPPROACHTOSTEROIDSINSEPTICSHOCK• don’tuseinlowriskpatients• considerinhighriskpatients(multi-organfailure)acknowledgingthatsepticshockmayreversemorequicklybutwillnotchangemortality
• uselowdose• vigilanceforsuperinfection• don’tuseashortsynACTHen test• eagerlyawaittheADRENALstudy
Costs
• IVVitaminC:~£66- 196for4-daycoursedrugonly)
• IVThiamine:~£35for4-daycourse(drugonly)
• Hydrocortisone:~£60(drugonly)
ImplementationOptions:AProposal• PatientswithRefractorySepticShock
• Alreadyreceivingsteroids
• NopredictedharmfromaddingVitaminCandthiamineReasonabletoendorseuseinthisgroup
• SepsisandNonRefractorySepticShock
• ThesepatientswouldnototherwisereceivesteroidsperSSCGuidelines
• InadequateEvidence-Basedliteraturetojustifyendorsement
• Therefore,leavetoindividualpractitionerstochoose

AuthorConclusion:
• “OurresultssuggestthattheearlyuseofintravenousvitaminC,togetherwithcorticosteroidsandthiaminemayprovetobeeffectiveinpreventingprogressiveorgandysfunctionincludingAKIandreducingthemortalityofpatientswithseveresepsisandsepticshock.
• Additionalstudiesarerequiredtoconfirmthesepreliminaryfindings.”

ClinicalTakeHomePoint:
• Althoughtheresultsofthisstudyareverypromising,itisimportanttorememberthatthiswasonlyahypothesisgeneratingstudy.Westillneedanexternalvalidationbeforeimplementation(Howmanyothertreatmentsinsepsishavebeentoutedasa“cure”andnotpannedoutinsubsequentstudies?).
References[1]J.X. WilsonEvaluationofvitaminCforadjuvantsepsistherapyAntioxid RedoxSignal, 19 (17) (2013),pp. 2129-2140
[2]P.E. Marik, V. Khangoora, R. Rivera, etal.Hydrocortisone,vitaminC,andthiamineorthetreatmentofseveresepsisandsepticshock:aretrospectivebefore-afterstudyChest, 151 (6) (2017),pp. 1229-1238
[3]H.M. Oudemans-vanStraaten, A.M. Spoelstra-deMan, M.C. deWaard VitaminCrevisited,Crit Care, 18 (4) (2014),p. 460
[4]M.M. Berger, H.M. Oudemans-vanStraaten VitaminCsupplementationinthecriticallyillpatient,Curr Opin Clin Nutr Metab Care, 18 (2) (2015),pp. 193-201
[5]W.A. Koekkoek, A.R. vanZantenAntioxidant vitaminsandtraceelementsincriticalillness,Nutr Clin Pract, 31 (4) (2016),pp. 457-474

[6]Castellanos-Ortega, B. Suberviola, L.A. García-Astudillo, etal.Impactofthesurvivingsepsiscampaignprotocolsonhospitallengthofstayandmortalityinsepticshockpatients:resultsofathree-yearfollow-upquasi-experimentalstudy,Crit CareMed, 38 (4) (2010),pp. 1036-1043
[7]Y. Sakr, M.J. Dubois, D. DeBacker, etal.PersistentmicrocirculatoryalterationsareassociatedwithorganfailureanddeathinpatientswithsepticshockCrit CareMed, 32 (9) (2004),pp. 1825-1831
[8]J.L. Vincent, D.R. Nelson, M.D. WilliamsIs worseningmultipleorganfailurethecauseofdeathinpatientswithseveresepsis? Crit CareMed, 39 (5) (2011),pp. 1050-1055
[9]E.J. Seeley, G.R. BernardTherapeutictargetsinsepsis:past,present,andfutureClin ChestMed, 37 (2) (2016),pp. 181-189
[10]M. Prucha, R. Zazula, S. Russwurm Immunotherapyofsepsis:blindalleyorcallforpersonalizedassessment? ArchImmunol Ther Exp (Warsz), 65 (1) (2017),pp. 37-49

[11]G.R. Bernard, J.L. Vincent, P.F. Laterre, etal.RecombinanthumanproteinCworldwideevaluationinseveresepsis(PROWESS)studygroup.EfficacyandsafetyofrecombinanthumanactivatedproteinCforseveresepsisN Engl JMed, 344 (10) (2001),pp. 699-709[12]A.J. Martí-Carvajal, I. Solà, D. Lathyris, etal.Human recombinantactivatedproteinCforseveresepsis,Cochrane DatabaseSyst Rev, 3 (2012),Article CD004388
[13]P.M. Honore, R. Jacobs, I. Hendrickx, etal.Adjuvant vitaminCtreatmentinsepsis-howmanyorangesadaykeep(vasopressor-dependent)septicshockaway? JThorac Dis, 8 (9) (2016),pp. E993-E995
[14]J.M. May, F.E. HarrisonRole ofvitaminCinthefunctionofthevascularendotheliumAntioxid RedoxSignal, 19 (17) (2013),pp. 2068-2083
[15]T.A. Treschan, J. PetersThe vasopressinsystem:physiologyandclinicalstrategies,Anesthesiology, 105 (3) (2006),pp. 599-612
[16]J.A. RussellBench-to-bedsidereview:vasopressininthemanagementofsepticshock,CritCare, 15 (4) (2011),p. 22617]A.C. Carr, G.M. Shaw, A.A. Fowler, etal.Ascorbate-dependentvasopressorsynthesis:arationaleforvitaminCadministrationinseveresepsisandsepticshock?, Crit Care, 19 (2015),p. 418
[
[18]T. Sharshar, R. Carlier, A. Blanchard, etal.Depletion ofneurohypophyseal contentofvasopressininsepticshock,Crit CareMed, 30 (3) (2002),pp. 497-500
[19]TA. Rudiger, M. SingerMechanisms ofsepsis-inducedcardiacdysfunctionCrit CareMed, 35 (6) (2007),pp. 1599-1608
[20]M. Duggan, I. Browne, C. FlynnAdrenal failureinthecriticallyillBrJAnaesth, 81 (3) (1998),pp. 468-470,ArticlePDF(122KB)
[21]J.M. May, Z.C. Qu, M.E. MeredithMechanisms ofascorbicacidstimulationofnorepinephrinesynthesisinneuronalcells,Biochem Biophys ResCommun, 426 (1) (2012),pp. 148-152,ArticlePDF(526KB)
[22]P.F. Dillon, R.S. Root-Bernstein, C.M. LiederAntioxidant-independentascorbateenhancementofcatecholamine-inducedcontractionsofvascularsmoothmuscle,Am JPhysiol HeartCirc Physiol, 286 (6) (2004)
([23]J.P. Gaut, A. Belaaouaj, J. Byun, etal.Vitamin Cfailstoprotectaminoacidsandlipidsfromoxidationduringacuteinflammation,Free Radic Biol Med, 40 (9) (2006),pp. 1494-1501,ArticlePDF(312KB)
[24]J. Armour, K. Tyml, D. Lidington, etal.Ascorbate preventsmicrovasculardysfunctionintheskeletalmuscleofthesepticrat,J Appl Physiol (1985), 90 (3) (2001),pp. 795-803

[25]B.J. Fisher, I.M. Seropian, D. Kraskauskas, etal.Ascorbic acidattenuateslipopolysaccharide-inducedacutelunginjury,Crit CareMed, 39 (6) (2011Jun),pp. 1454-1460
[26]S.J. Mo, E.W. Son, D.K. Rhee, etal.Modulation ofTNF-alpha-inducedICAM-1expression,NOandH2O2 productionbyalginate,allicin andascorbicacidinhumanendothelialcells,Arch PharmRes, 26 (3) (2003),pp. 244-251
[27]J. Haendeler, A.M. Zeiher, S. DimmelerVitamin CandEpreventlipopolysaccharide-inducedapoptosisinhumanendothelialcellsbymodulationofBcl-2andBax,Eur JPharmacol, 317 (2–3) (1996),pp. 407-411
ArticlePDF (341KB)[28]C. Fiorito, M. Rienzo, E. Crimi, etal.Antioxidants increasenumberofprogenitorendothelialcellsthroughmultiplegeneexpressionpathways,Free Radic Res, 42 (8) (2008),pp. 754-762
[29]P.E. Marik“Vitamin S”(steroids)andvitaminCforthetreatmentofseveresepsisandsepticshock!Crit CareMed, 44 (6) (2016),pp. 1228-1229[30]C.J. Schorah, C. Downing, A. Piripitsi, etal.Total vitaminC,ascorbicacid,anddehydroascorbicacidconcentrationsinplasmaofcriticallyillpatients,Am JClin Nutr, 63 (5) (1996),pp. 760-765
[31]J.X. WilsonMechanism ofactionofvitaminCinsepsis:ascorbatemodulatesredoxsignaling inendotheliumBiofactors, 35 (1) (2009),pp. 5-13

[32]A.A. Fowler 3rd, A.A. Syed, S. Knowlson, etal.Phase IsafetytrialofintravenousascorbicacidinpatientswithseveresepsisJTranslMed, 12 (2014),p. 32[33]K. Timmermans, M. Kox, G.J. Scheffer, etal.Plasma nuclearandmitochondrialDNAlevels,andmarkersofinflammation,shock,andorgandamageinpatientswithsepticshock,Shock, 45 (6) (2016),pp. 607-612
[34]K. Nakahira, S.Y. Kyung, A.J. Rogers, etal.Circulating mitochondrialDNAinpatientsintheICUasamarkerofmortality:derivationandvalidationPLoS Med, 10 (12) (2013),Article e1001577[35]A. Rhodes, M. CecconiCell-freeDNAandoutcomeinsepsis,Crit Care, 16 (6) (2012),p. 170
[36]R. Natarajan, B.J. Fisher, A.A. Syed, etal.Impact ofintravenousascorbicacidinfusiononnovelbiomarkersinpatientswithseveresepsisJPulm Respir Med, 4 (214) (2014)[37]C.H. Kim, J.T. Park, E.J. Kim, etal.An increaseinredbloodcelldistributionwidthfrombaselinepredictsmortalityinpatientswithseveresepsisorsepticshock,Crit Care, 17 (6) (2013),p. R282
[38]V. Yawalkar, M.K. Parashar, J. PunekarRole ofredcelldistributionwidthasaprognosticmarkerinpatientswithseveresepsisandsepticshockJAssoc PhysiciansIndia, 64 (1) (2016),p. 120[39]M.H. Zabet, M. Mohammadi, M. Ramezani, etal.Effect ofhigh-doseascorbicacidonvasopressor'srequirementinsepticshockJResPharmPract, 5 (2) (2016),pp. 94-100[40]H. Tanaka, T. Matsuda, Y. Miyagantani, etal.Reduction ofresuscitationfluidvolumesinseverelyburnedpatientsusingascorbicacidadministration:arandomized,prospectivestudy,Arch Surg, 135 (3) (2000),pp. 326-331
Diolch yn fawr