the neochord procedure, worldwide experience and …
TRANSCRIPT

THE NEOCHORD PROCEDURE, WORLDWIDE EXPERIENCE AND STATE OF THE ART
Giovanni Speziali, M.D.


The Neochord Operation
Beating heart procedure
provides real-time
confirmation of repair
Off pump avoids complications
due to bypass and cross-clamp
Real-time visual feedback
(TEE) permits dynamic
adjustment of chords versus
static adjustment in standard
surgery



Leaflet Capture and Verification SystemFiber Optic Confirmation
Four white lights on monitor correspond to
leaflet coverage over the four fiber optic lights
in the jaws of the device
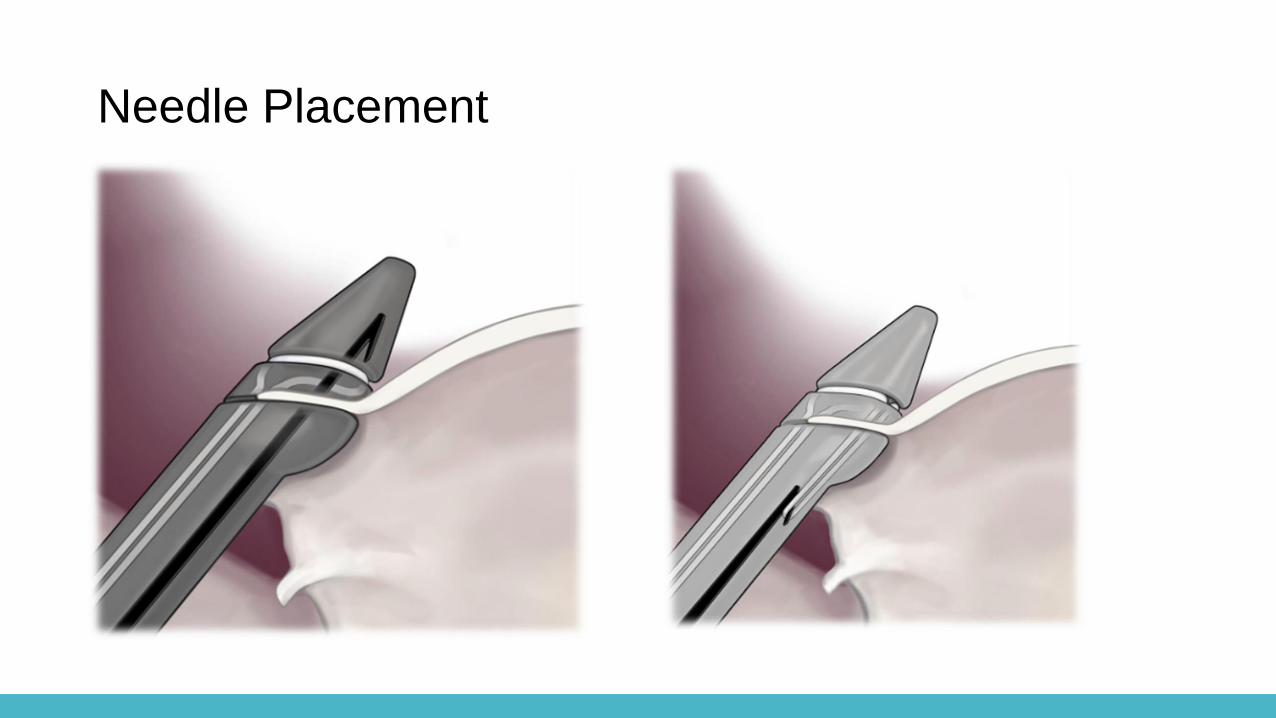
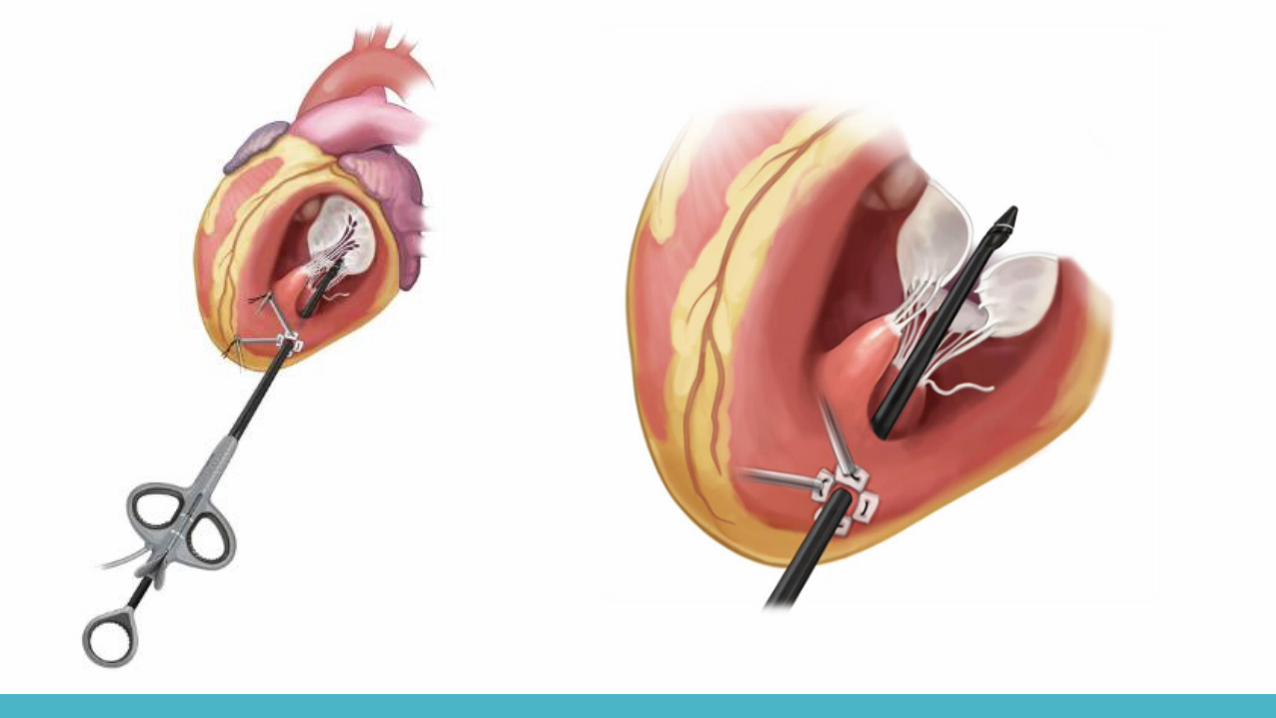
Needle Placement

Placement of NeoChords
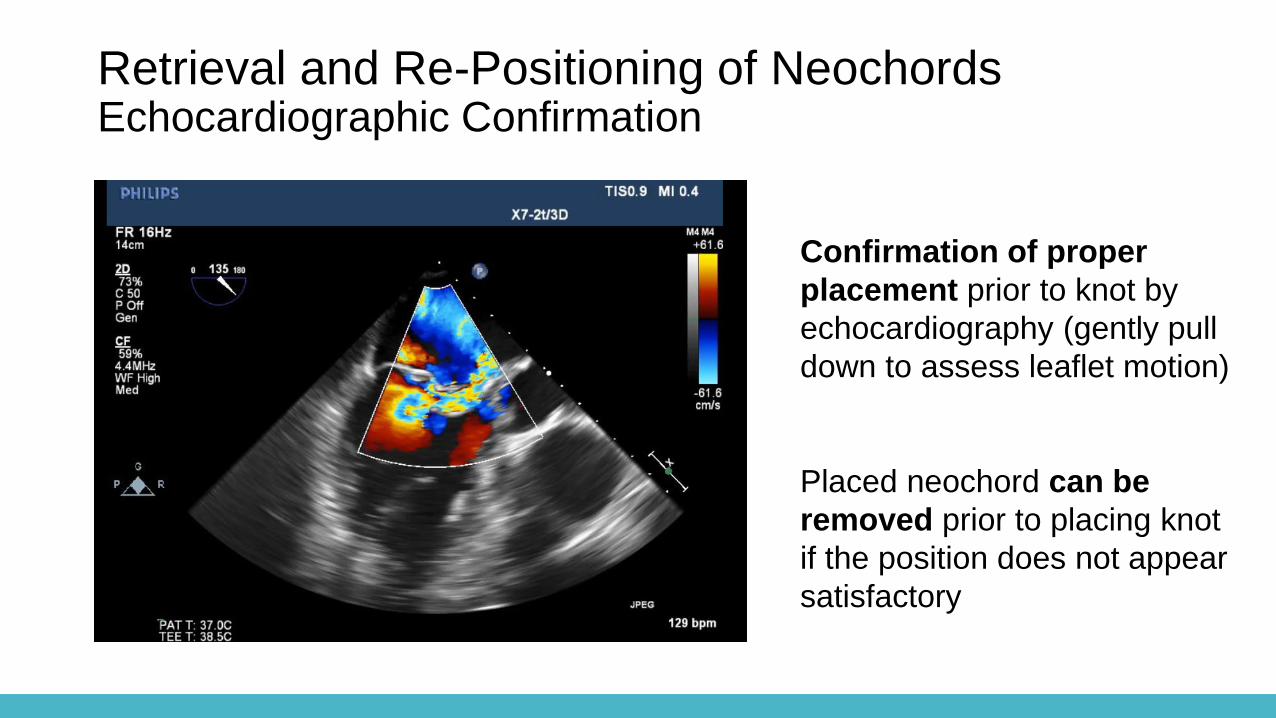
Retrieval and Re-Positioning of NeochordsEchocardiographic Confirmation
Confirmation of proper
placement prior to knot by
echocardiography (gently pull
down to assess leaflet motion)
Placed neochord can be
removed prior to placing knot
if the position does not appear
satisfactory
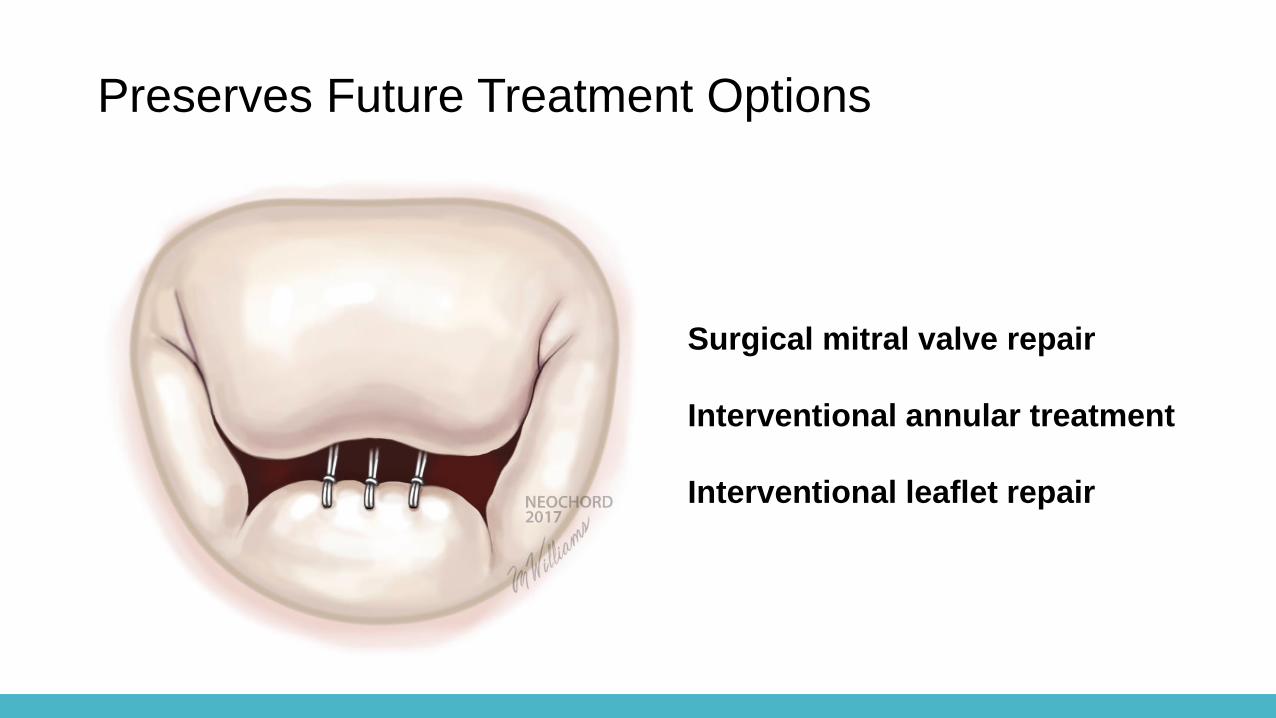
Preserves Future Treatment Options
Surgical mitral valve repair
Interventional annular treatment
Interventional leaflet repair

NeoChord Case Presentation54 Year Old Male Patient with P2 Prolapse and Severe MRCourtesy of Diana Zakarkaite, M.D.Vilnius University Hospital Santaros Klinikos

Pre-op echoes show P2 prolapse with single anterior-directed jet and severe MR
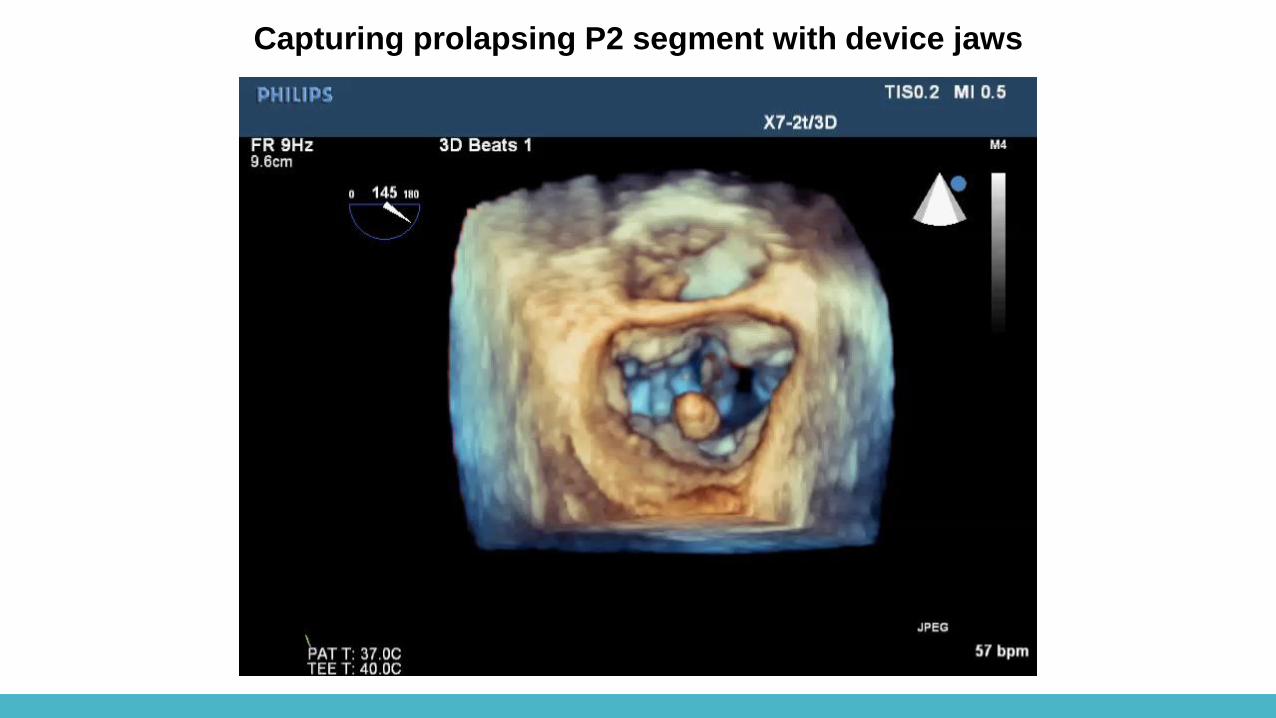
Capturing prolapsing P2 segment with device jaws
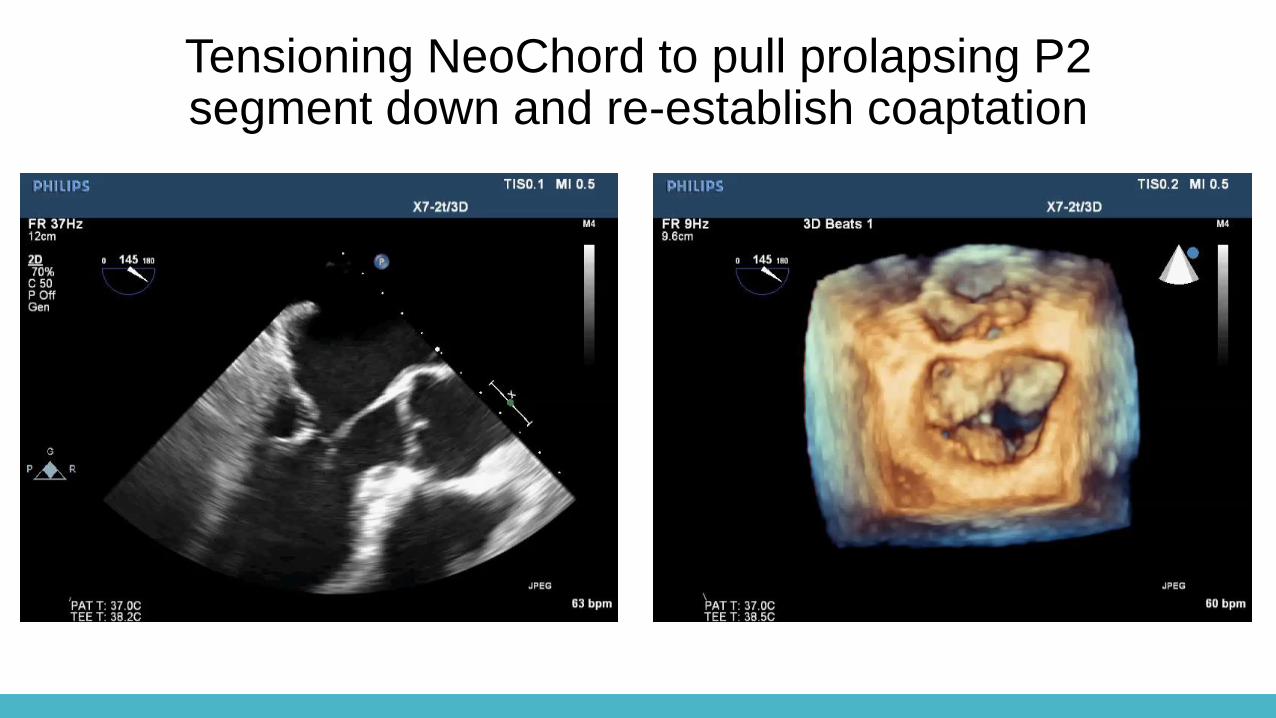
Tensioning NeoChord to pull prolapsing P2 segment down and re-establish coaptation
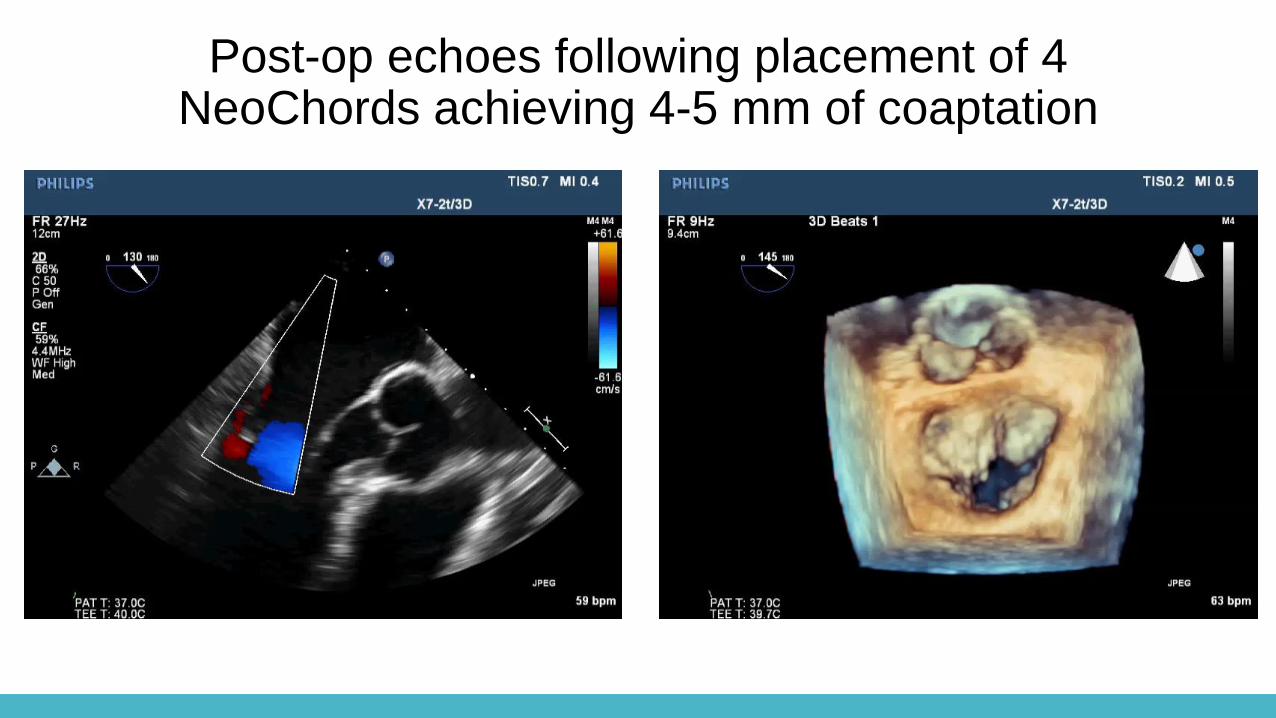
Post-op echoes following placement of 4 NeoChords achieving 4-5 mm of coaptation
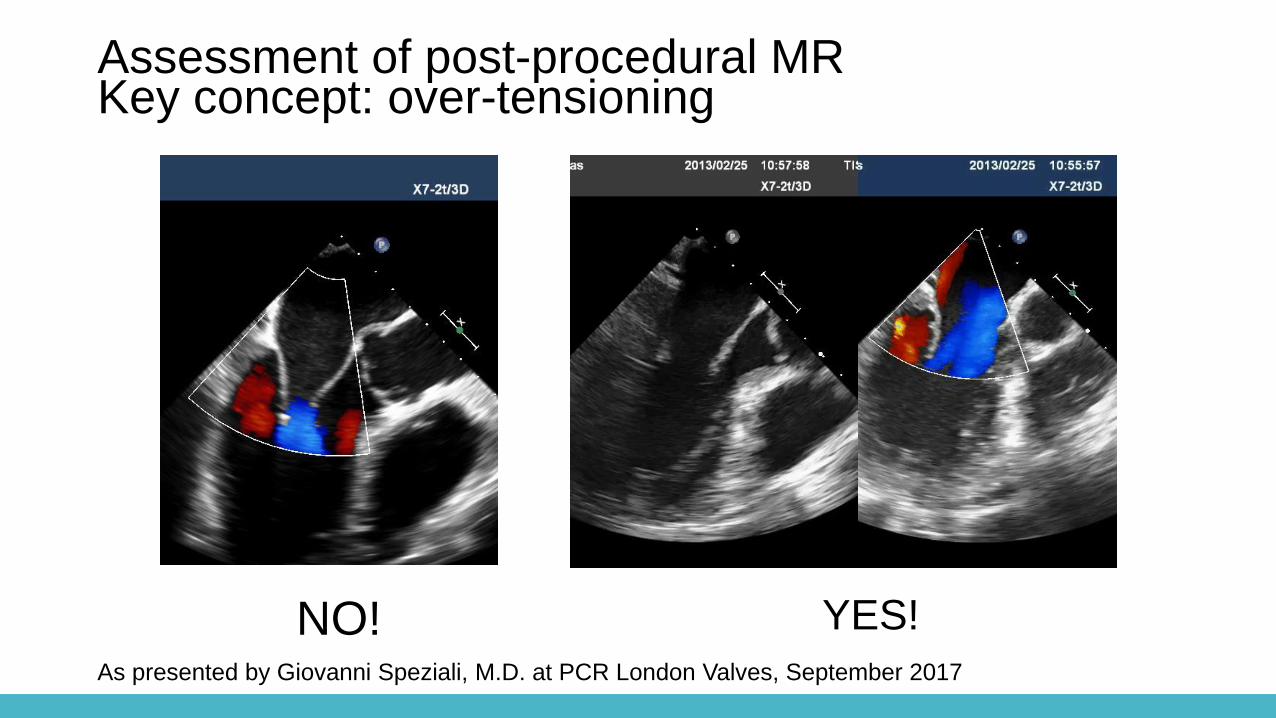
Assessment of post-procedural MRKey concept: over-tensioning
NO! YES!
As presented by Giovanni Speziali, M.D. at PCR London Valves, September 2017
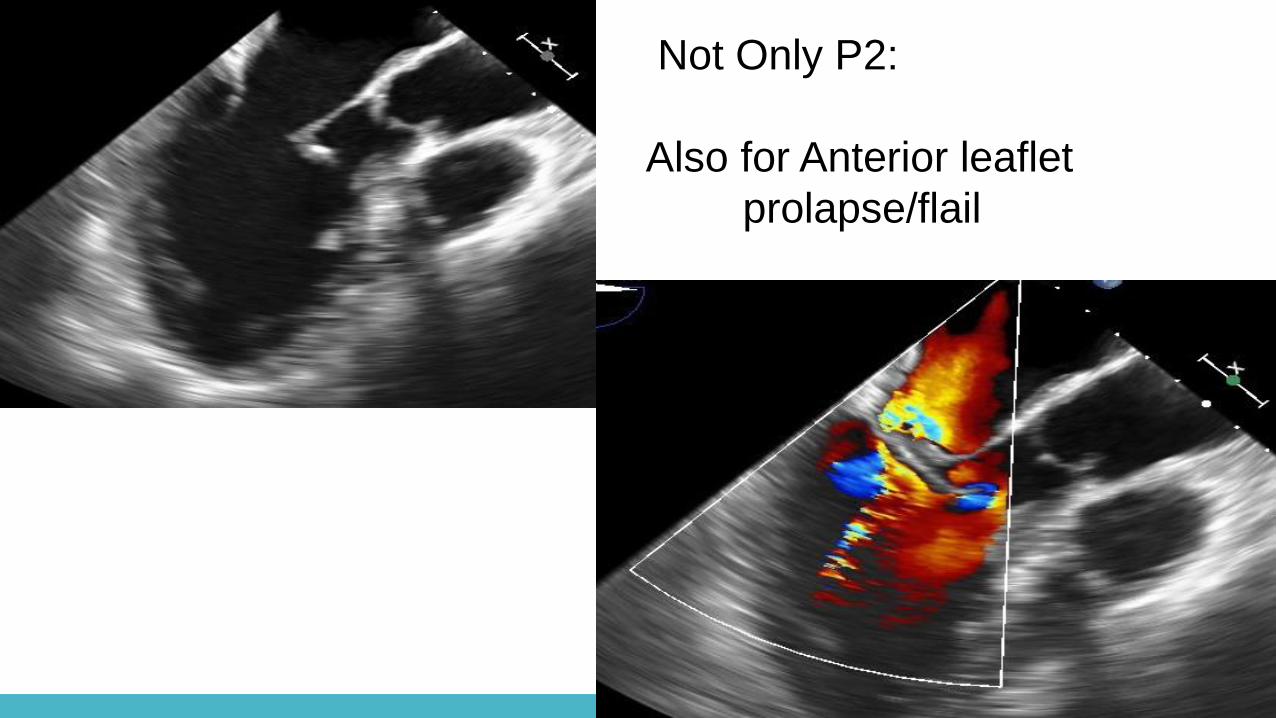
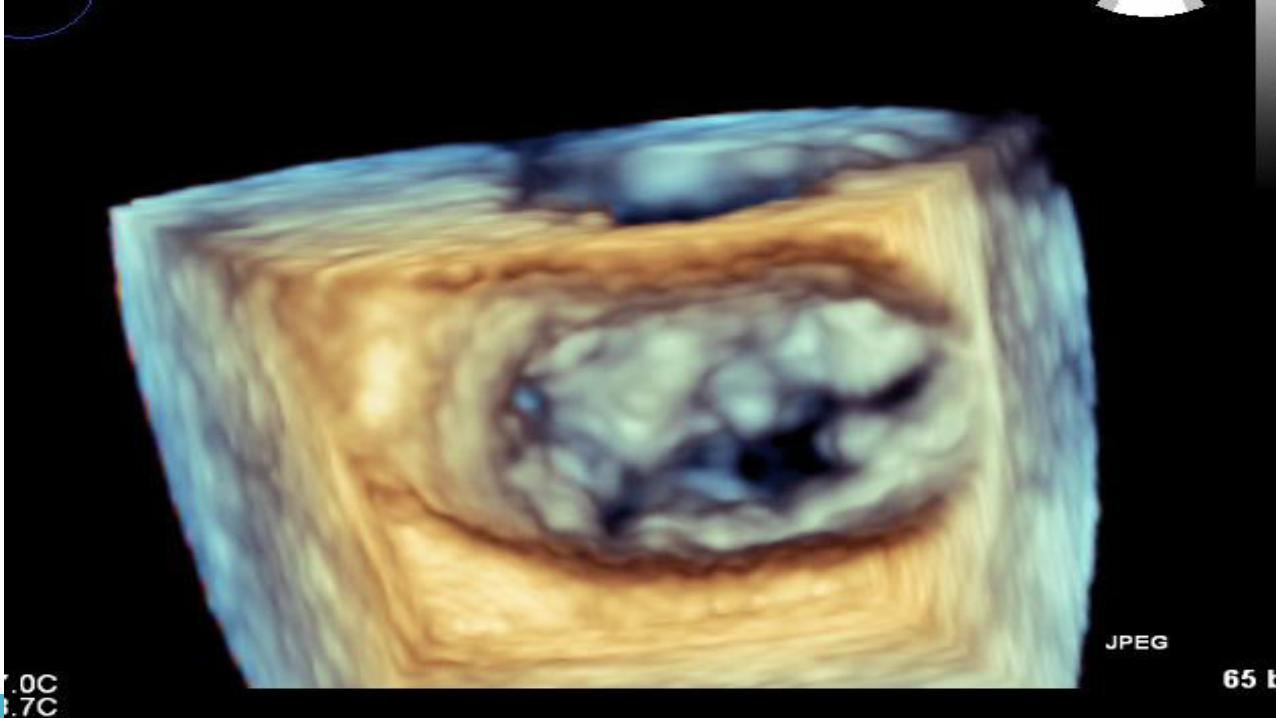
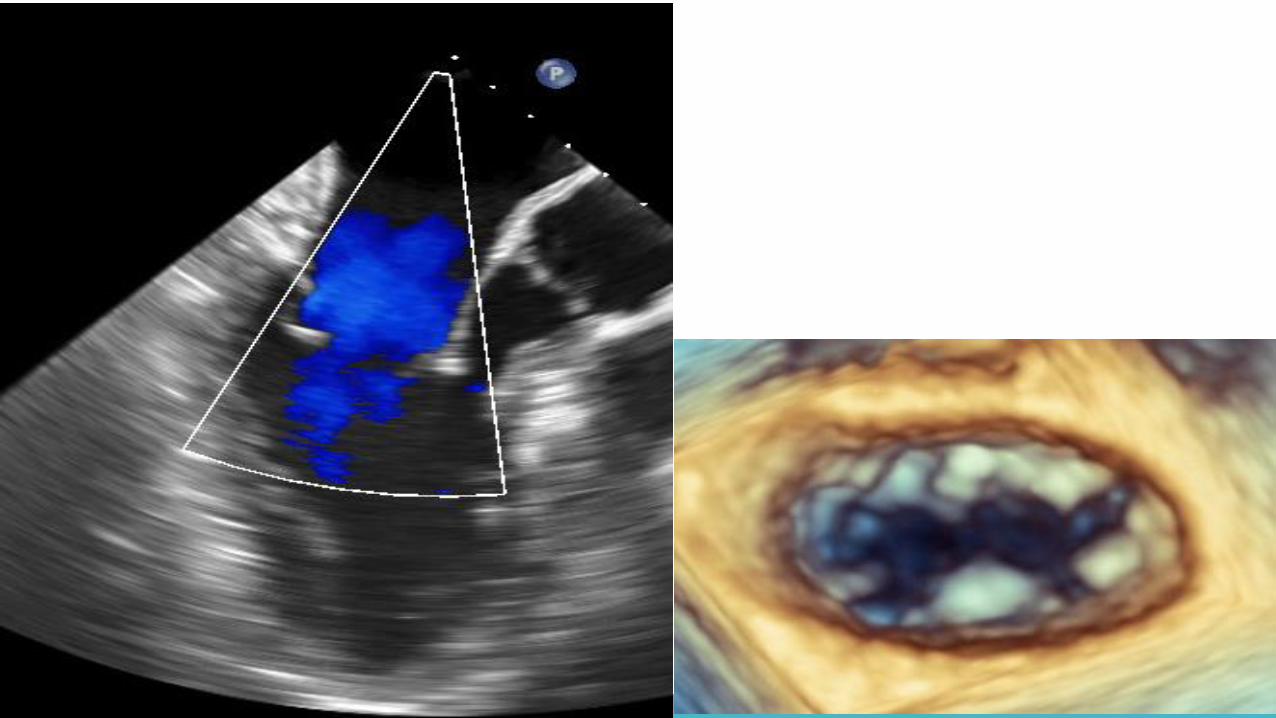
Not Only P2:
Also for Anterior leaflet
prolapse/flail
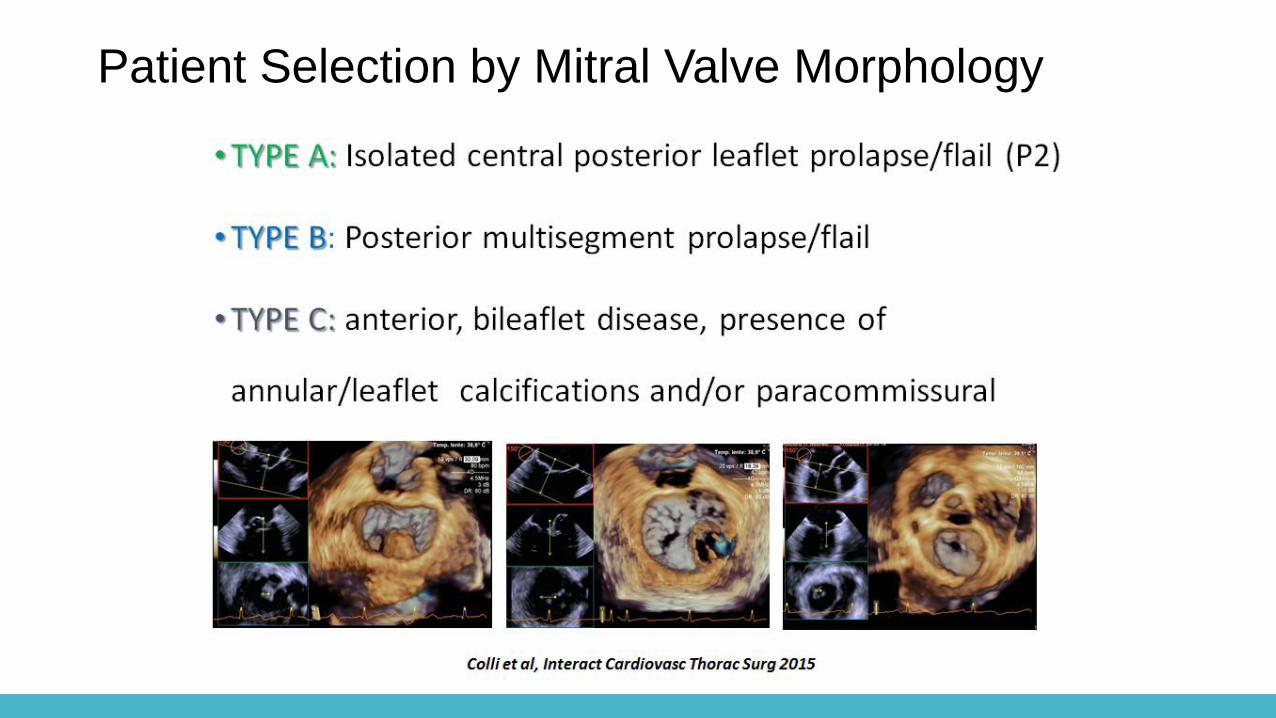
Patient Selection by Mitral Valve Morphology
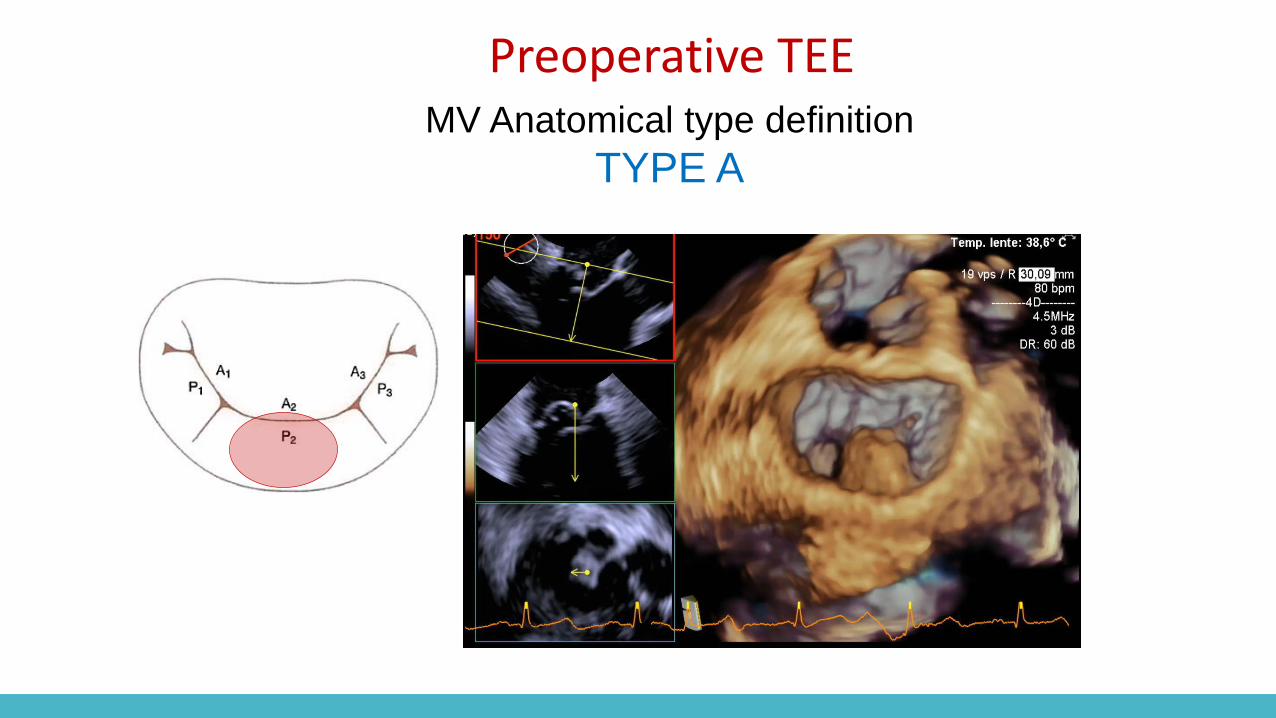
Preoperative TEEMV Anatomical type definition
TYPE A

Preoperative TEEMV Anatomical type definition
TYPE B
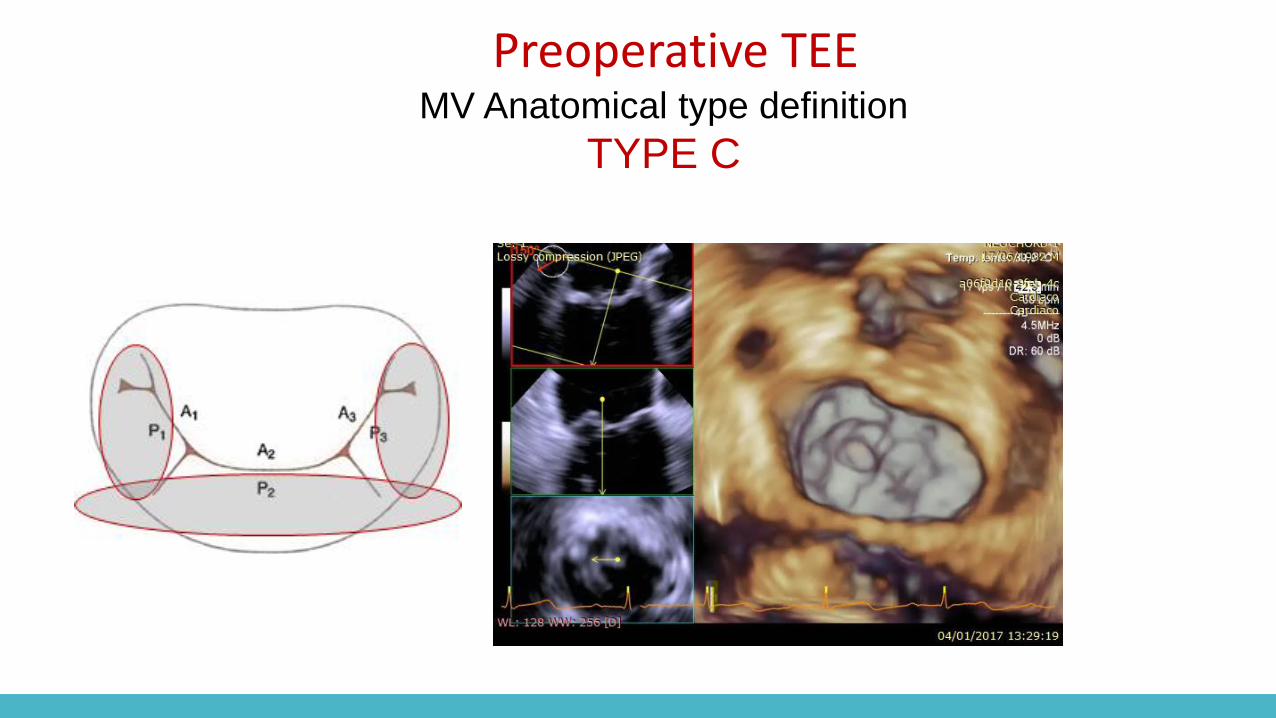
Preoperative TEEMV Anatomical type definition
TYPE C

NeoChord Five-Year Durability Data on Initial Patients (Leipzig Heart Center)
Good Five-Year Durability of Transapical Beating Heart Off-Pump Mitral
Valve Repair With Neochordae1
“In select patients MV repair using the NeoChord system results in
very good long term results without recurrent prolapse, MR, or annular dilatation.”1
1Kiefer P, Meier S, Noack T, Borger MA, Ender J, Hoyer A, Mohr FW, Seeburger J, Good Five-Year Durability of Transapical Beating Heart
Off-Pump Mitral Valve Repair With Neochordae, The Annals of Thoracic Surgery (2018), doi: 10.1016/j.athoracsur.2018.01.092.
• Mitral annular dilatation was moderate at the time of surgery and did not
show further increase over time

Patient 1 Patient 2 Patient 3
FOLLOW-UP
NYHA pre-op II-III II-III II-III
NYHA 5Y-FU I-II I I
MR grade pre-op severe severe severe
MR grade 5Y-FU trace mild-
moderate
mild
AP Diameter (mm)
End Systolic pre-op
27 32 39
AP Diameter (mm)
End Systolic 5Y-FU
27 30 37
Kiefer P, Meier S, Noack T, Borger MA, Ender J, Hoyer A, Mohr FW, Seeburger J, Good Five-Year Durability of Transapical Beating Heart Off-
Pump Mitral Valve Repair With Neochordae, The Annals of Thoracic Surgery (2018), doi: 10.1016/j.athoracsur.2018.01.092.
NeoChord Five-Year Durability Data on Initial Patients (Leipzig Heart Center)
Seven Centers Enrolled 213 Patients, 2013-2016
Eur J Cardiothorac Surg 2018; doi:10.1093/ejcts/ezy064
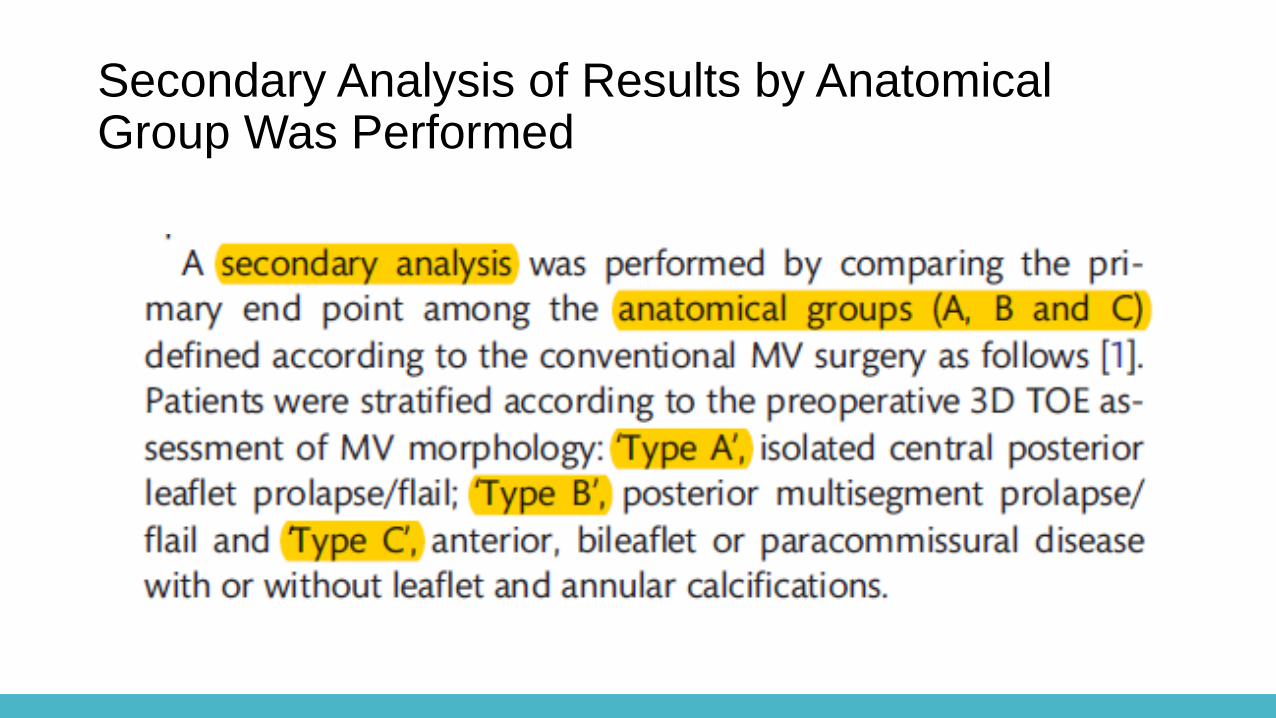
Secondary Analysis of Results by Anatomical Group Was Performed
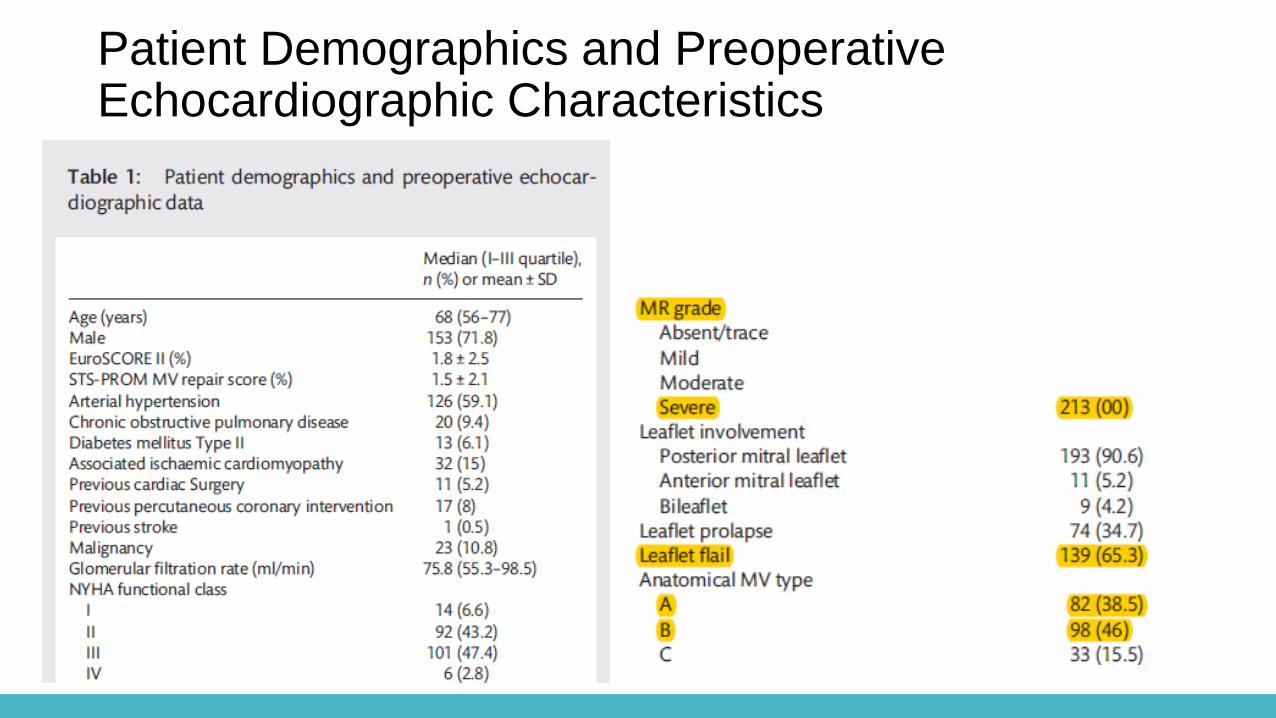
Patient Demographics and Preoperative Echocardiographic Characteristics

Procedural and 30-Day Outcomes

Overa
ll D
eg
ree o
f M
R

TY
PE
AD
eg
ree
of
MR
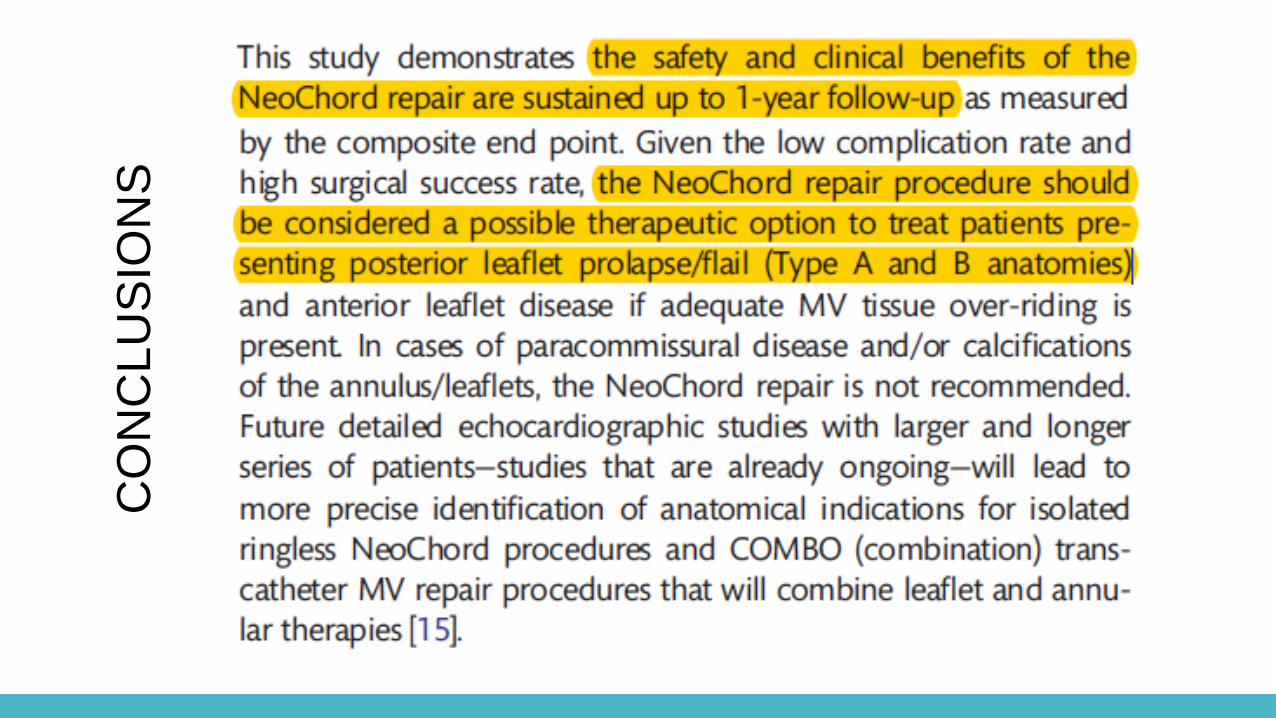
CO
NC
LU
SIO
NS
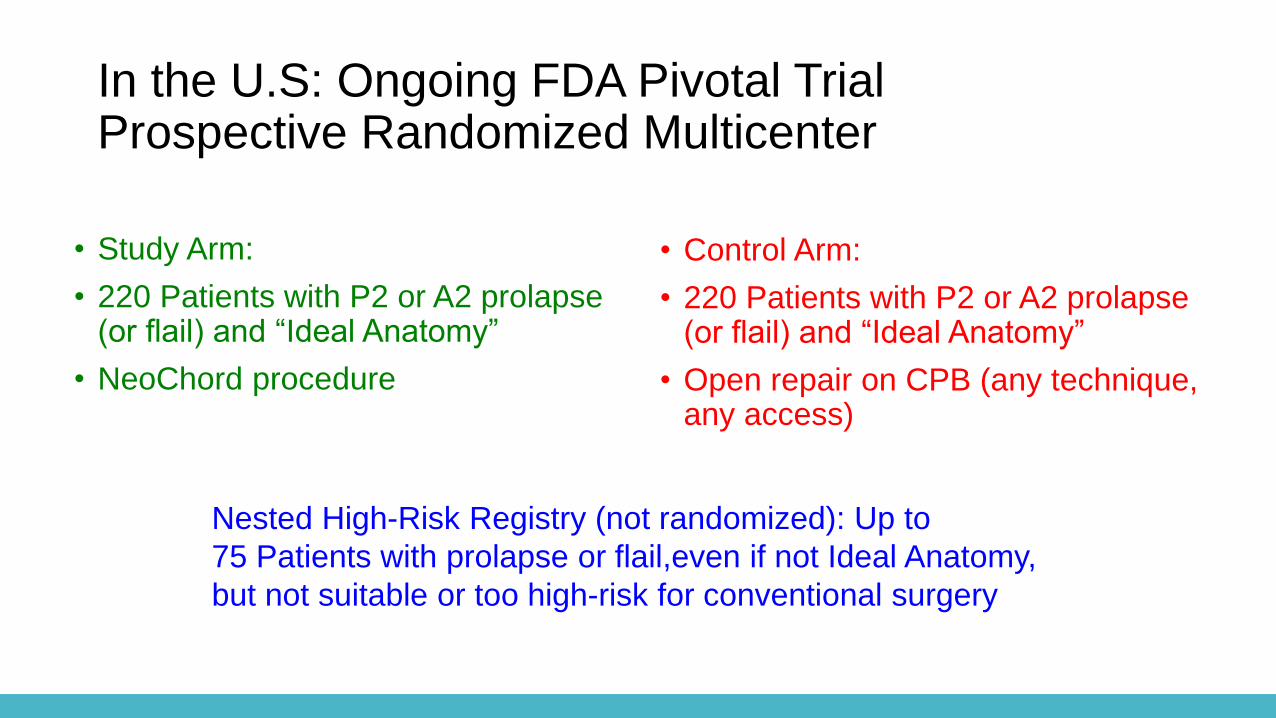
In the U.S: Ongoing FDA Pivotal TrialProspective Randomized Multicenter
• Study Arm:
• 220 Patients with P2 or A2 prolapse (or flail) and “Ideal Anatomy”
• NeoChord procedure
• Control Arm:
• 220 Patients with P2 or A2 prolapse (or flail) and “Ideal Anatomy”
• Open repair on CPB (any technique, any access)
Nested High-Risk Registry (not randomized): Up to
75 Patients with prolapse or flail,even if not Ideal Anatomy,
but not suitable or too high-risk for conventional surgery

Subject has an indication for isolated surgical mitral valve repair per ACC/AHA and ESC/EACTS
guidelines.
Subject has Severe (degenerative) mitral valve regurgitation per Echo Core Lab assessment.
Subjects ≥ twenty-one (21) years of age.
Subject is a candidate for mitral valve surgery with cardiopulmonary bypass.
Subject with history of Coronary Artery Disease amenable to PCI should have completed the PCI
procedure at least three (3) months prior to index procedure.
Subject may have a history of previous Coronary Artery Bypass Graft(s)
Anatomical considerations:
Isolated segmental prolapse of the P2 or A2 segment.
Anterior leaflet covers at least 65% of the anterior-posterior annular length.
Anatomic suitability as determined by Subject Screening Committee
Subject has provided written informed consent and authorization for release of personal health
information prior to index procedure.
FDA Pivotal Trial Inclusion Criteria
Primary Effectiveness Endpoint
Freedom from moderate/ severe mitral
valve regurgitation at one (1) year and;
Freedom from mitral valve replacement or
mitral valve re-intervention at one (1) year.
Core Lab: Paul Grayburn, Baylor University, Dallas TX

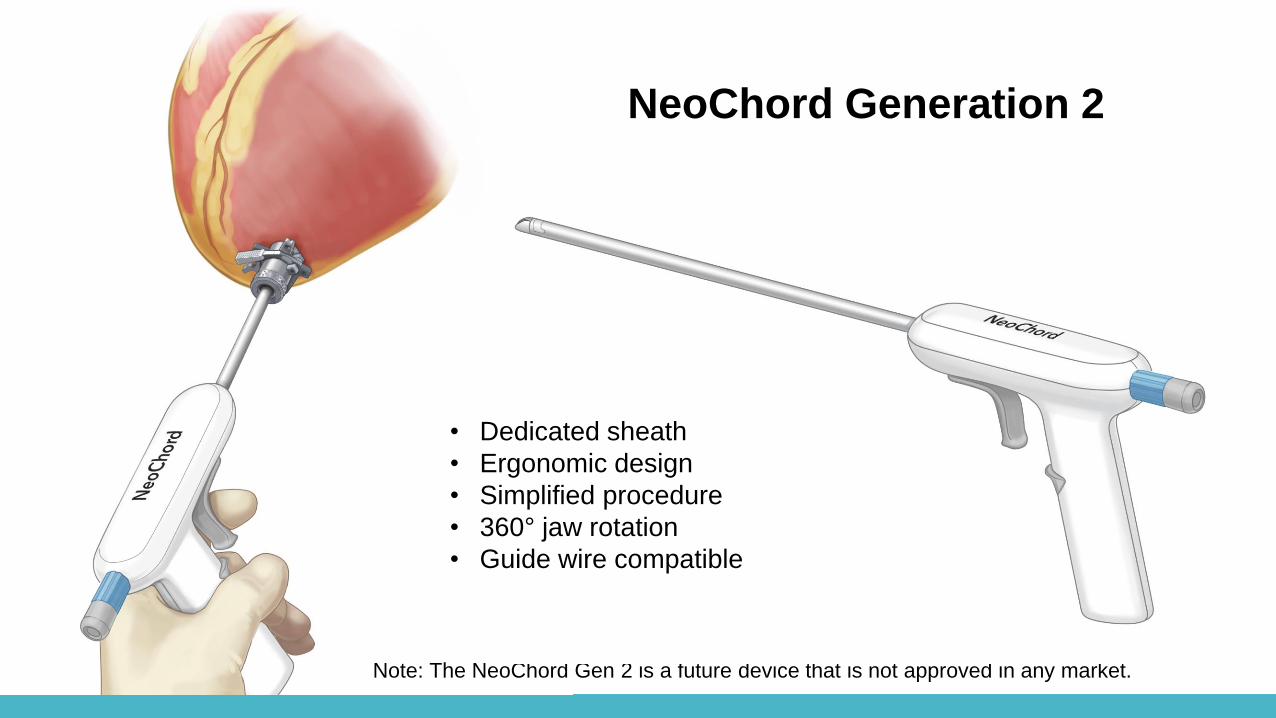
NeoChord Generation 2
Note: The NeoChord Gen 2 is a future device that is not approved in any market.
• Dedicated sheath
• Ergonomic design
• Simplified procedure
• 360° jaw rotation
• Guide wire compatible
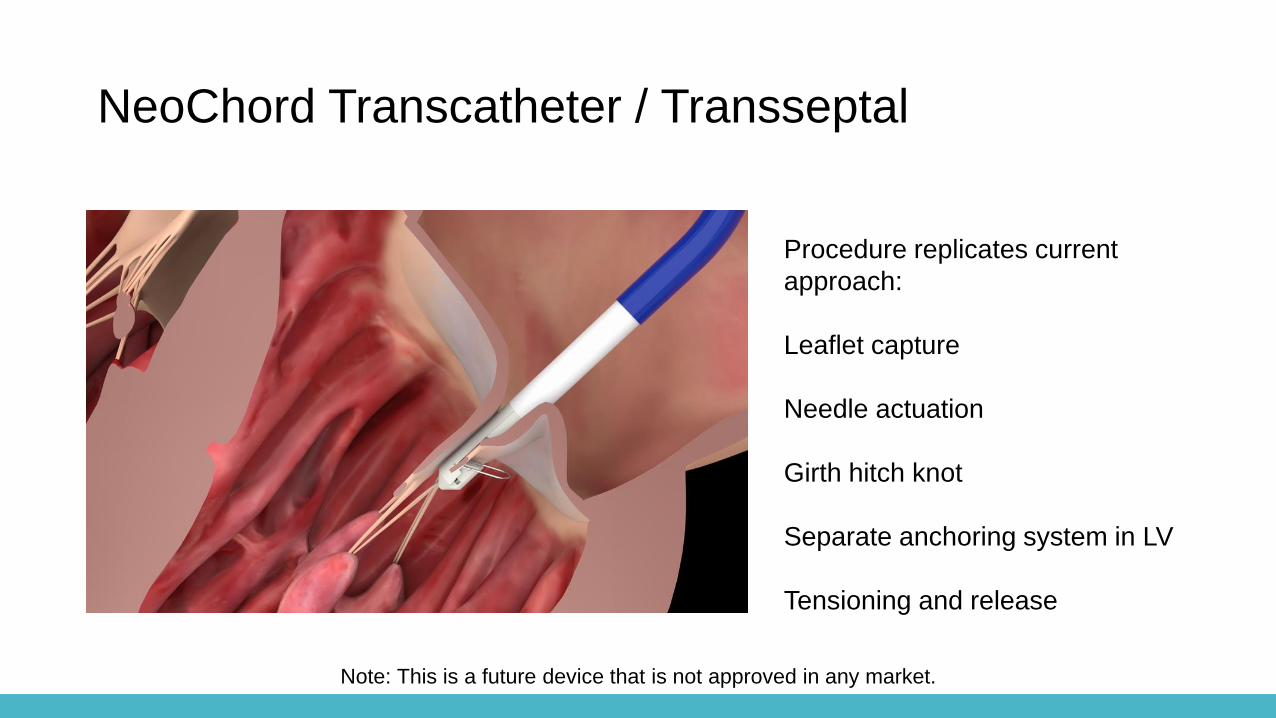
Procedure replicates current
approach:
Leaflet capture
Needle actuation
Girth hitch knot
Separate anchoring system in LV
Tensioning and release
NeoChord Transcatheter / Transseptal
Note: This is a future device that is not approved in any market.

THANK YOU