the rate dependent bundle branch block · the rate-dependent bundle branch block is defined as an...
TRANSCRIPT

295 M.E.J. ANESTH 20 (2), 2009
THE RATE DEPENDENT BUNDLE BRANCH BLOCK
- Transition from left Bundle Branch Block to Intraoperative normal Sinus Rhythm -
- Case Report -
seeMa MIshra*, Prashant nasa#**, gaurav nIrWanI goyal##,
hIManshu khurana#**, DeePak guPta#
***
anD sushMa bhatnagar****
**
AbstractA chronic hypertensive patient with electrocardiogram (ECG) showing left bundle branch
block (LBBB) was given general anesthesia for right modified radical mastectomy. Her ECG reverted to normal sinus rhythm intermittently during peri-operative period. This intermittent rate-dependent LBBB is a rare entity. Though hypertension is one significant co-morbid condition, the risk evalution of LBBB during anesthesia only on an ECG finding, is not justifiable. Rather patient should be investigated further for any cardiac risk.
Keywords: Left bundle branch block, heart-intra ventricular conduction.
IntroductionLeft bundle branch block is a major electrocardiographic abnormality in hypertensive patient.
It may signify associated coronary heart disease. Few cases have been reported on such rate-dependent LBBB developing intraoperatively in a patient with normal ECG1-5 but without LBBB preoperatively.
We report a case of preoperative LBBB which reverted to normal sinus rhythm below critical hear rate, during perioperative period.
Case ReportA 45 year-old 70 kg female diagnosed as a case of carcinoma right breast T2N1Mx (Stage
2) was posted for modified radical mastectomy. Pre-anesthetic evaluation revealed that she was a known case of hypertension of 6 yrs and was on oral losartan hydrochlorthiazide once a day, with good control of blood pressure. She gave no history of chest pain, syncope or dyspnea on exertion. On systemic examination, there was no significant abnormality in the cardiovascular and respiratory systems.
From Unit of Anesthesiology, Institute Rotary Cancer Hospital (IRCH), Ansari Nagar, New Delhi, All India Institute of Medical Sciences, Ansari Nagar, New Delhi India, Pin code: -110029.
* MD, Assistant Professor Anaesthesia.# MD, Senior Resident Anaesthesia.## Senior Research Associate Anaesthesia.** Associate Professor Anaesthesia. Corresponding author: Dr. Seema Mishra, Assist. Prof. Anesthesiology, F-33, AIIMS Residential Campus (West), Ansari
Nagar, New Delhi, Pin: 110029, India. Phone: +91-9899061105, Fax.91-11-26588641, E-mail: [email protected]
296
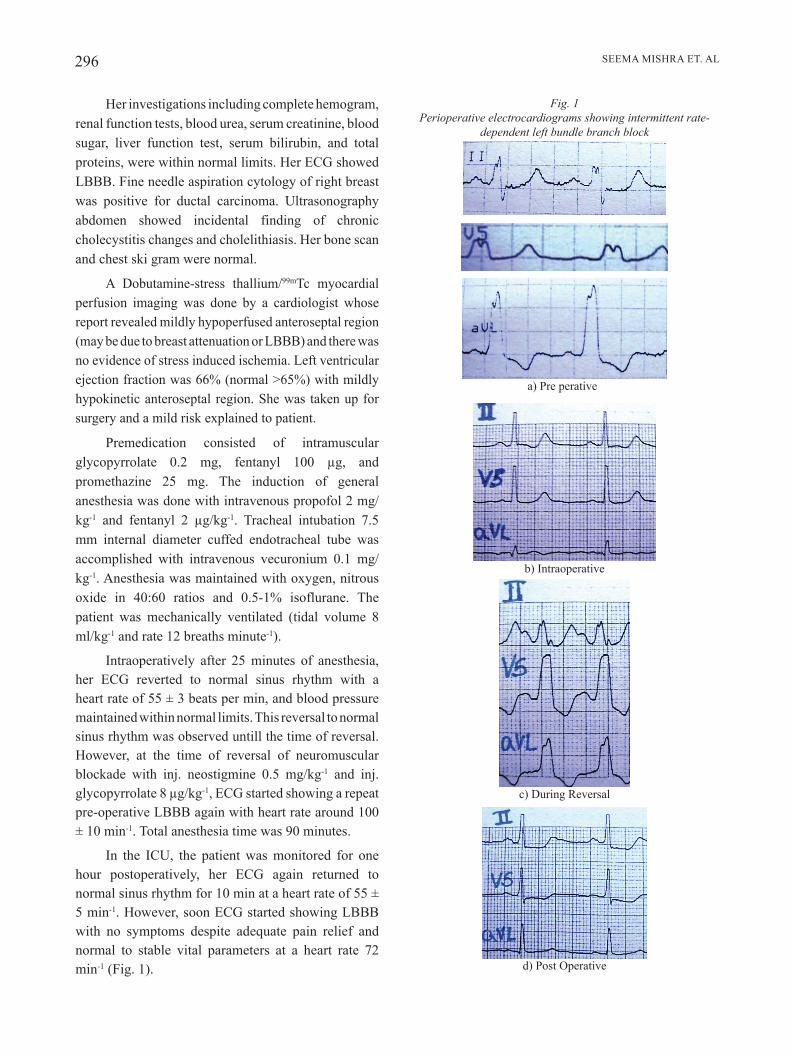
Fig. 1 Perioperative electrocardiograms showing intermittent rate-
dependent left bundle branch block
SEEMA MISHRA ET. AL
Her investigations including complete hemogram, renal function tests, blood urea, serum creatinine, blood sugar, liver function test, serum bilirubin, and total proteins, were within normal limits. Her ECG showed LBBB. Fine needle aspiration cytology of right breast was positive for ductal carcinoma. Ultrasonography abdomen showed incidental finding of chronic cholecystitis changes and cholelithiasis. Her bone scan and chest ski gram were normal.
A Dobutamine-stress thallium/99mTc myocardial perfusion imaging was done by a cardiologist whose report revealed mildly hypoperfused anteroseptal region (may be due to breast attenuation or LBBB) and there was no evidence of stress induced ischemia. Left ventricular ejection fraction was 66% (normal >65%) with mildly hypokinetic anteroseptal region. She was taken up for surgery and a mild risk explained to patient.
Premedication consisted of intramuscular glycopyrrolate 0.2 mg, fentanyl 100 µg, and promethazine 25 mg. The induction of general anesthesia was done with intravenous propofol 2 mg/kg-1 and fentanyl 2 µg/kg-1. Tracheal intubation 7.5 mm internal diameter cuffed endotracheal tube was accomplished with intravenous vecuronium 0.1 mg/kg-1. Anesthesia was maintained with oxygen, nitrous oxide in 40:60 ratios and 0.5-1% isoflurane. The patient was mechanically ventilated (tidal volume 8 ml/kg-1 and rate 12 breaths minute-1).
Intraoperatively after 25 minutes of anesthesia, her ECG reverted to normal sinus rhythm with a heart rate of 55 ± 3 beats per min, and blood pressure maintained within normal limits. This reversal to normal sinus rhythm was observed untill the time of reversal. However, at the time of reversal of neuromuscular blockade with inj. neostigmine 0.5 mg/kg-1 and inj. glycopyrrolate 8 µg/kg-1, ECG started showing a repeat pre-operative LBBB again with heart rate around 100 ± 10 min-1. Total anesthesia time was 90 minutes.
In the ICU, the patient was monitored for one hour postoperatively, her ECG again returned to normal sinus rhythm for 10 min at a heart rate of 55 ± 5 min-1. However, soon ECG started showing LBBB with no symptoms despite adequate pain relief and normal to stable vital parameters at a heart rate 72 min-1 (Fig. 1).
a) Pre perative
b) Intraoperative
c) During Reversal
d) Post Operative

M.E.J. ANESTH 20 (2), 2009
297THE RATE DEPENDENT BUNDLE BRANCH BLOCK
neurogenic or functional depression with or without underlying pathological lesions of the conducting tissue10. Rate-dependent bundle branch block can revert to sinus rhythm at critical heart rate11. The transition from normal to abnormal may occur by alterations in heart rate by only 1 or 2 beats/min-10. This critical heart rate is dependent on change in heart rate3. With rapid decrease in heart rate, sinus rhythm may appear at higher rates and with rapid acceleration in heart rate, it may appear at lower heart rate, as the heart rate increase RR interval shortens and the descending impulses finds one of the bundle branches still in its refractory period9.
A clear differentiation of LBBB into a benign rate-dependent LBBB, and LBBB associated with myocardial ischemia or infarction, may avoid the unnecessary postponement of a case because of high cardiac risk. Various convenient methods exist for the diagnoses of rate-dependent LBBB during anesthesia. Manouvers like carotid massage, deep inspiration and pharmacological agents like esmolol12, metoprolol6, propanolol, neostigmine and edrophonium which all decrease the heart rate and thus change this aberrant conduction block to normal13. Holter examination, however, is the gold standard.
In a chronic hypertensive patient with LBBB, it is always better to do further cardiac evaluation, like stress-imaging, in order to rule out an associated CAD.
In conclusion, rate-dependent left bundle branch block is a rare entity. LBBB with other co morbid condition, like hypertension, though a significant finding, yet the evaluation of risk during anesthesia only on an ECG finding, is not justifiable. Rather patient should be further investigated for any associated cardiac co morbid conditions.
The postoperative period remained uneventful except for asymptomatic LBBB. Holter examination showed that the ECG changes were rate-dependent left bundle branch block.
DiscussionLeft bundle branch block is major clinical
finding in cases of known hypertension. It may also signify associated coronary artery disease, aortic valve disease or cardiomyopathies6. Isolated left bundle branch block in a healthy young adult may be benign, but in hypertensive or older patients it may signify a progressive degenerating myocardium involving cardiac conduction system7-9.
The stress-perfusion imaging of the patient showed a relatively normal cardiac performance. Her ECG which was showing LBBB preoperatively, became normal peri-operatively at a heart rate of <60 beats per minute.
Our hypothesis is that the LBBB in the present case was not of organic origin as proved by stress-perfusion imaging and the fact that LBBB reverted back to normal sinus rhythm. When heart rate was at 60 ± 10 beats per minute intraoperatively, and especially postoperatively for some time, LBBB reverted to sinus rhythm. So pre-operative abnormal ECG rhythm was rate-dependent LBBB, reverting into normal sinus rhythm at lower heart rates (critical heart rates).
The rate-dependent bundle branch block is defined as an intraventricular conduction defect that may return, if only temporarily, to sinus rhythm at lower heart rates9. The exact mechanism of such a block is unclear but may result from anatomic or physiological interruptions in cardiac conduction system either due to ventricular enlargement or from

298 SEEMA MISHRA ET. AL
exercise- induced left bundle branch block. JAMA; 1998, 279:153-156.
8. fahy gj, PInskI sl, MIller DP, et al: Natural history of isolated bundle branch block. American Journal of Cardiology; 1996; 77:1185-1190.
9. Intraventricular Conduction defects. In: Wagner GS, ed. Marriott’s Practical Electrocardiography. Lipincott Williams & Wilkins, Philadelphia, 2001, 96-116.
10. bauer ge. Transient Bundle branch Block. Circulation; 1964, 29:730-738.
11. josePhson Me: Intraventricular conduction disturbances. In: Clinical Cardiac Electrophysiology: Techniques and Interpretations. Lipincott Williams & Wilkins, Philadelphia, 2001, 110-139.
12. rajesh, bhoI s, kuMar M, sharMa b, guPta bb. Rate dependent left bundle branch block with chest pain in a 38 year old female. J Ind Acad Clin Med; 2002, 3:193-194.
13. WallaCe ag, laszlo j: Mechanism influencing conduction in a case of intermittent bundle branch block. Am Heart J; 1961, 61:548-555.
References
1. rorIe Dk, MulDoon sM, krabIll Dr: Transient bundle branch block occurring during anesthesia. Anesthesia Analgesia; 1972, 51:633-637.
2. elDerMan DM, hurlbert bj: Intermittent left bundle branch block during anesthesia. Anesthesia Analgesia; 1980, 59:628-630.
3. DoMIno kb, la MantIa kl, geer rt, klIneberg Pl: Intraoperative diagnosis of rate-dependent bundle branch block. Can Anesth Soc J; 1984; 31:302-306.
4. reyforD h, De groote P, guerMouChe t, boufflers e, Menu h, aDnet P: Intermittent left bundle branch block revealed during anaesthesia. British Journal of Anaesthesia; 1994, 72:700-701.
5. tyagI a, sethI ak, agarWal v, Mohta M: Rate-dependent left bundle branch block during anaesthesia. Anaesthesia and Intensive Care; 2004, 32:715-718.
6. lIttMann l, syMnaskI jD: Hemodynamic complications of left bundle branch block. J Electrocardiology; 2000, 33 suppl: 115-121.
7. graDy ta, ChIu aC, snaDer Ce, et al: Prognostic significance of