the resurrection of ezetimibe: a story of perseverance · 1 the resurrection of ezetimibe: a story...
TRANSCRIPT
1
The Resurrection of Ezetimibe:
A Story of Perseverance
Harry “Chip” Davis
CVPath Institute
Gaithersburg, MD
(Schering-Plough / Merck)
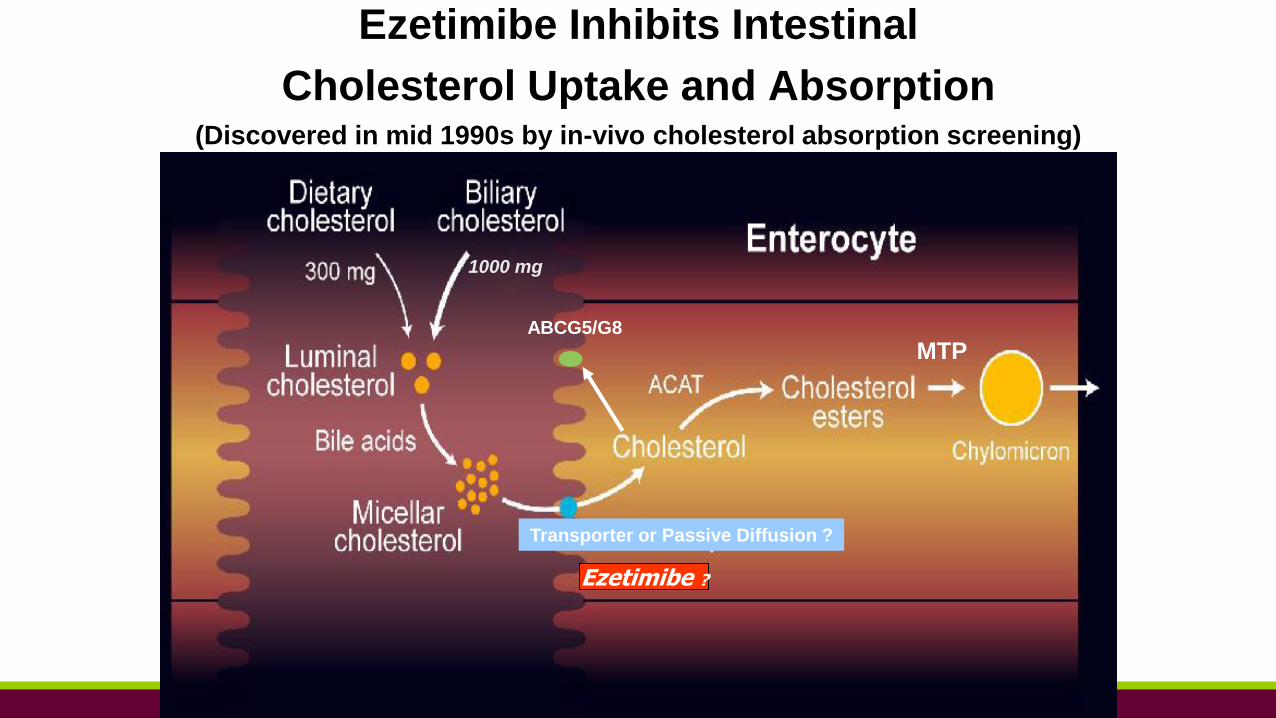
Ezetimibe Inhibits Intestinal
Cholesterol Uptake and Absorption(Discovered in mid 1990s by in-vivo cholesterol absorption screening)
1000 mg
Transporter or Passive Diffusion ?
Ezetimibe ?
MTPABCG5/G8
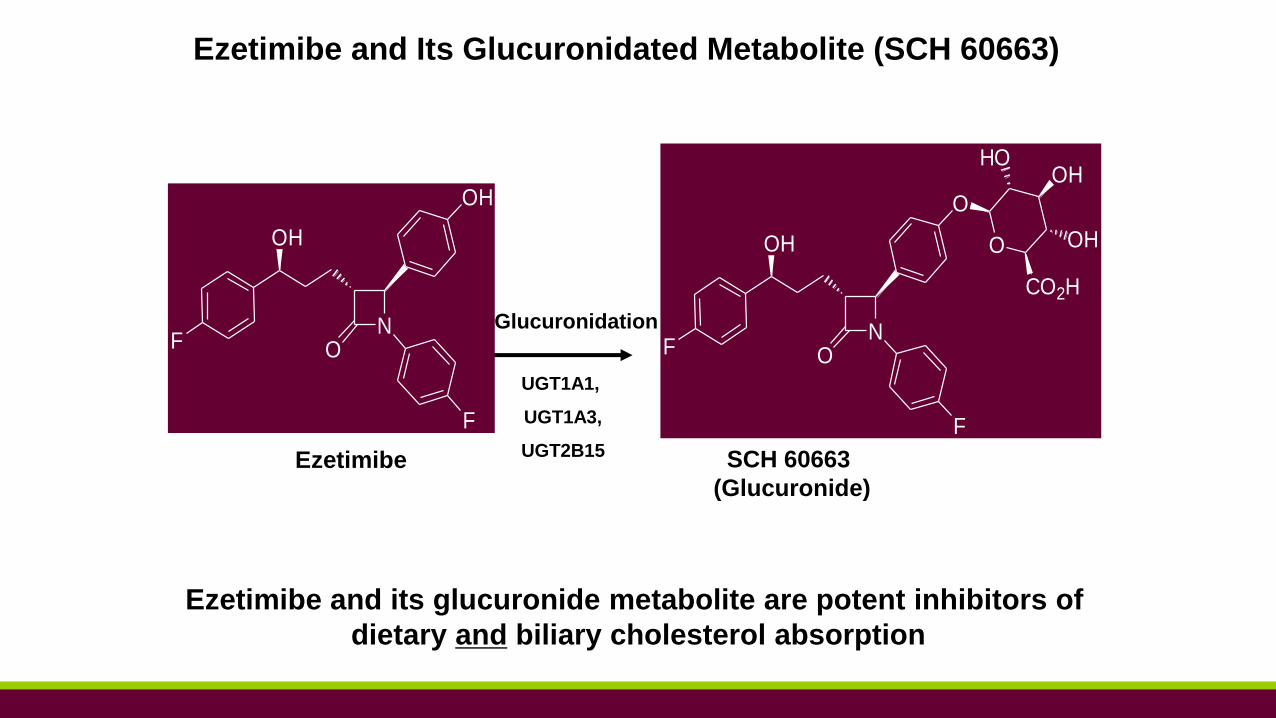
Ezetimibe and its glucuronide metabolite are potent inhibitors of
dietary and biliary cholesterol absorption
Ezetimibe and Its Glucuronidated Metabolite (SCH 60663)
Glucuronidation
SCH 60663
(Glucuronide)
Ezetimibe
NO
OH
O
F
F
O
CO2H
OHHO
OH
NO
OH
OH
F
F
UGT1A1,
UGT1A3,
UGT2B15
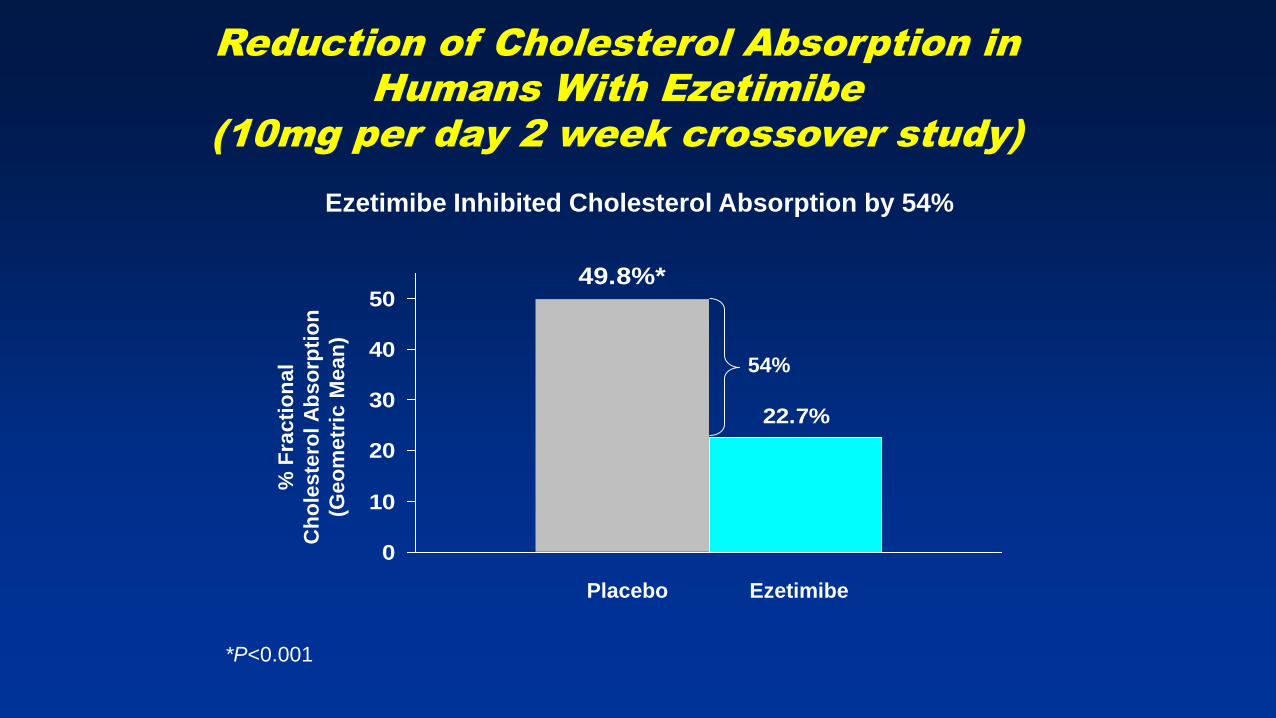
Reduction of Cholesterol Absorption in
Humans With Ezetimibe
(10mg per day 2 week crossover study)
*P<0.001
49.8%*
22.7%
0
10
20
30
40
50%
Fra
cti
on
al
Ch
ole
ste
rol A
bso
rpti
on
(Geo
metr
ic M
ean
)
EzetimibePlacebo
Ezetimibe Inhibited Cholesterol Absorption by 54%
54%
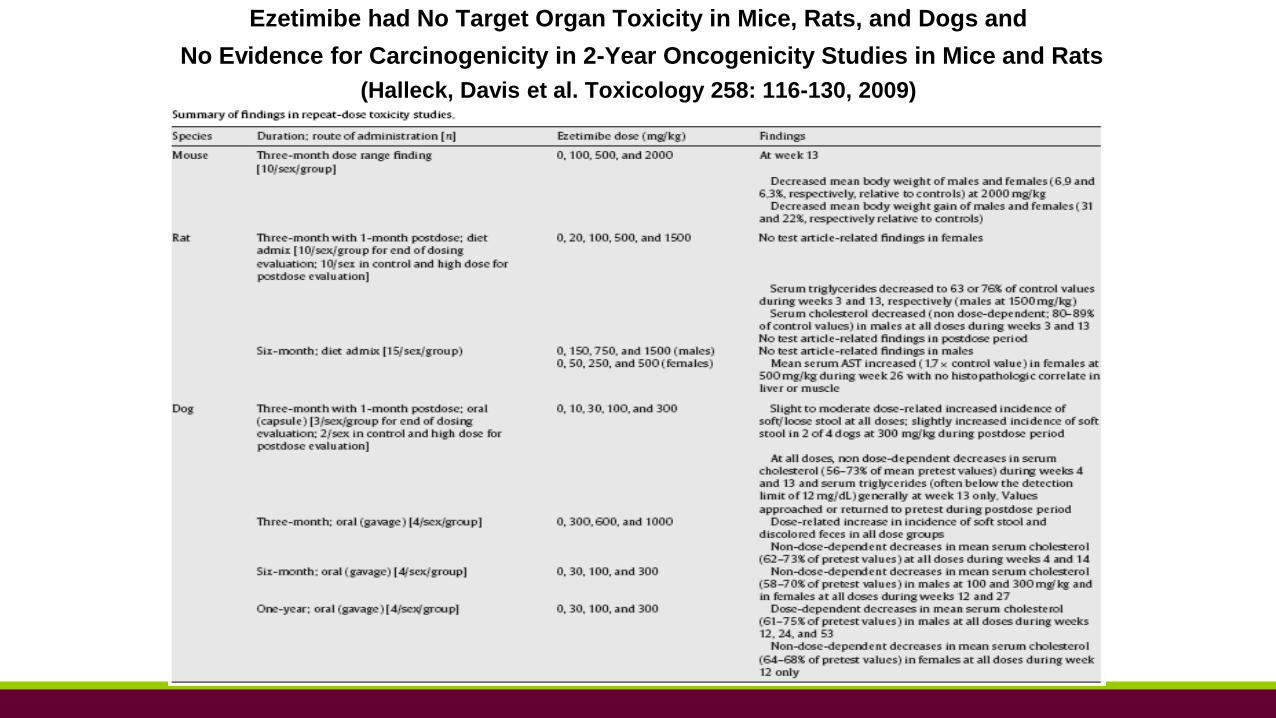
Ezetimibe had No Target Organ Toxicity in Mice, Rats, and Dogs and
No Evidence for Carcinogenicity in 2-Year Oncogenicity Studies in Mice and Rats
(Halleck, Davis et al. Toxicology 258: 116-130, 2009)
Mean
% c
han
ge in
LD
L
fro
m b
aselin
e a
t w
k12
Placebo
(n=52)
-30
-20
-10
0
+10Ezetimibe
0.25 mg
(n=47)
Ezetimibe
1 mg
(n=49)
Ezetimibe
5 mg
(n=49)
Ezetimibe
10 mg
(n=46)
-9.9
* -12.6
*-16.4 *
-18.7 *
+4.3
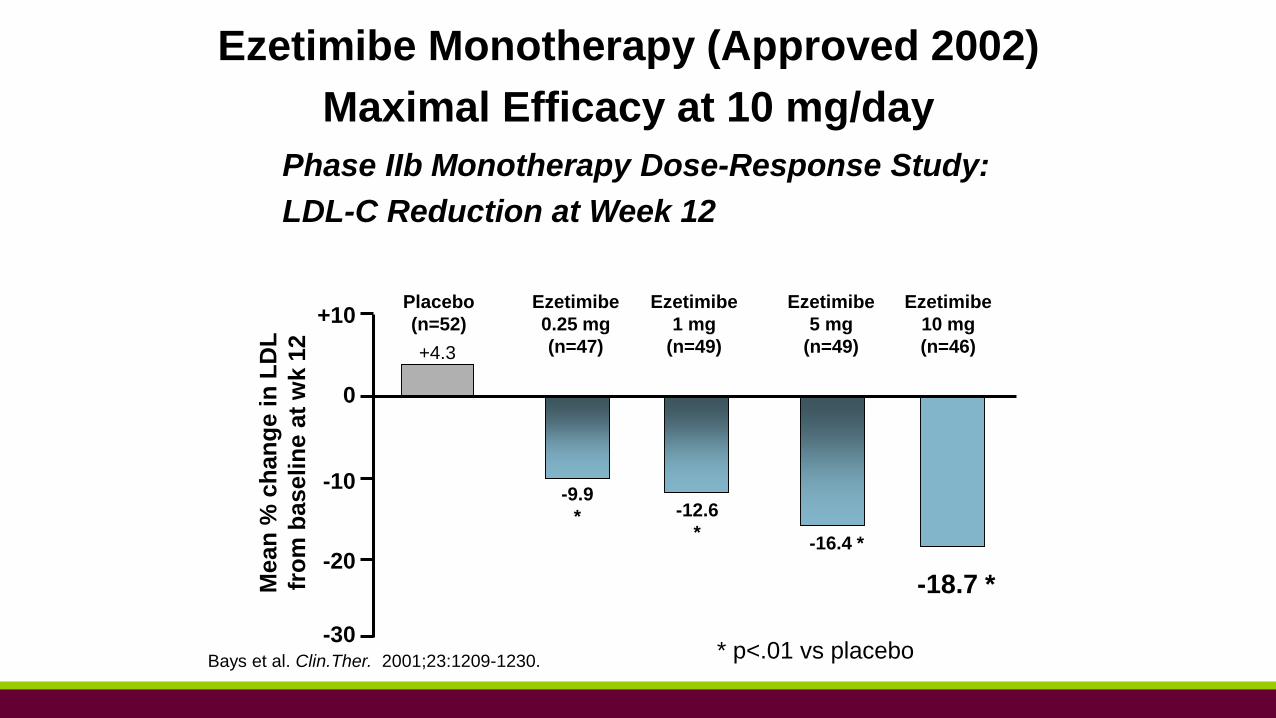
Ezetimibe Monotherapy (Approved 2002)
Maximal Efficacy at 10 mg/day
Phase IIb Monotherapy Dose-Response Study:
LDL-C Reduction at Week 12
Bays et al. Clin.Ther. 2001;23:1209-1230.* p<.01 vs placebo
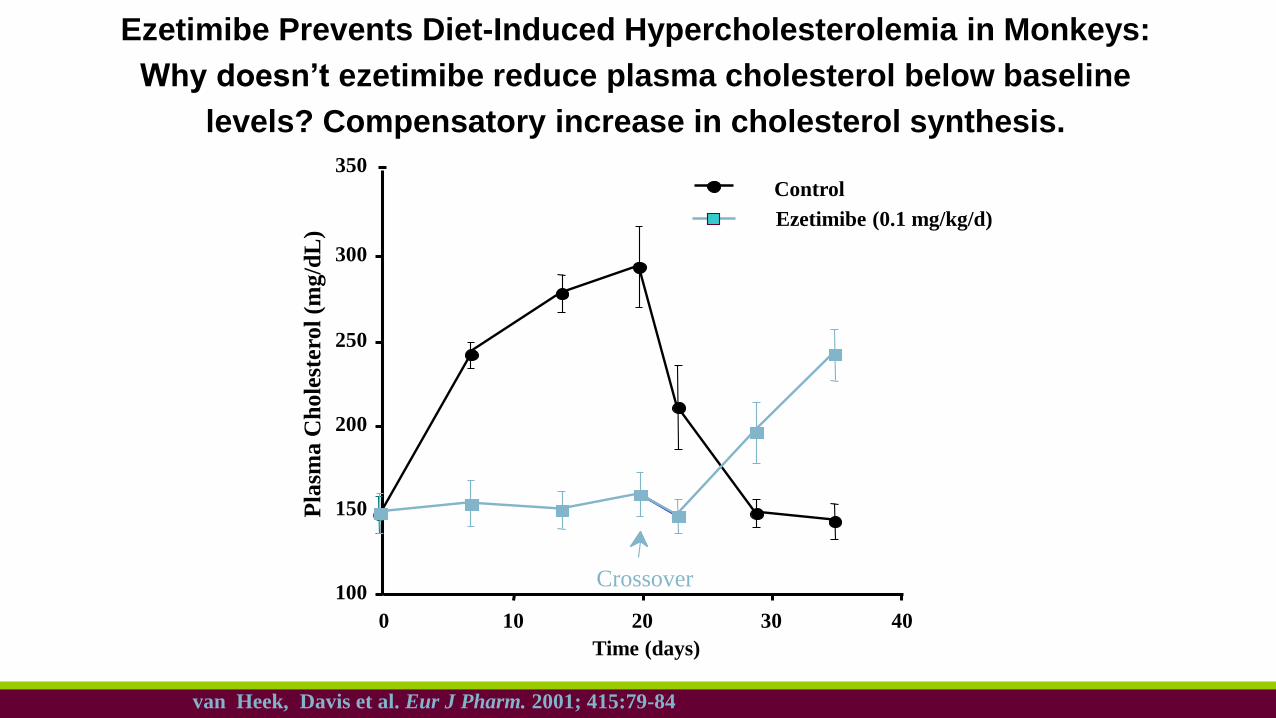
Ezetimibe Prevents Diet-Induced Hypercholesterolemia in Monkeys:
Why doesn’t ezetimibe reduce plasma cholesterol below baseline
levels? Compensatory increase in cholesterol synthesis.
Ezetimibe (0.1 mg/kg/d)
Time (days)
Control
403020100
100
150
200
250
300
Pla
sma C
hole
ster
ol
(mg/d
L)
Crossover
350
van Heek, Davis et al. Eur J Pharm. 2001; 415:79-84
8
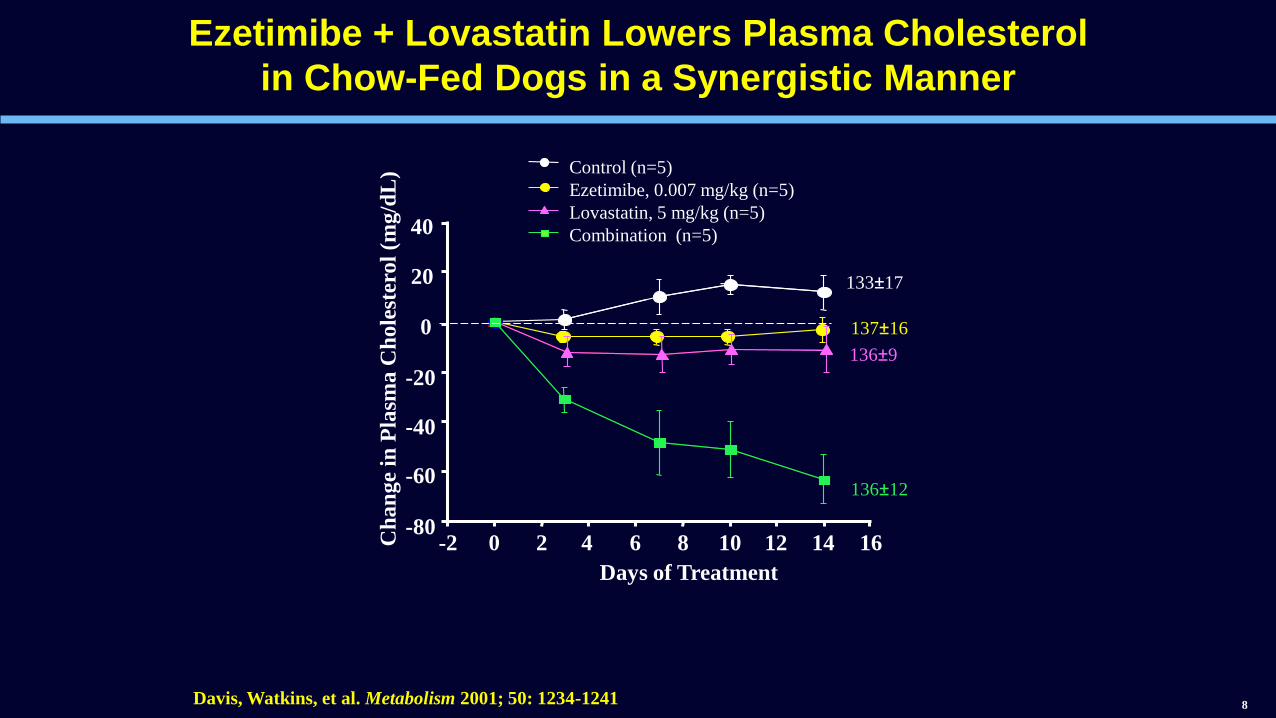
Ezetimibe + Lovastatin Lowers Plasma Cholesterol
in Chow-Fed Dogs in a Synergistic Manner
Control (n=5)
Ezetimibe, 0.007 mg/kg (n=5)
Lovastatin, 5 mg/kg (n=5)
Combination (n=5)
1614121086420-2-80
-60
-40
-20
0
20
40
Days of Treatment
Ch
an
ge
in P
lasm
a C
hole
ster
ol
(mg/d
L)
133±17
137±16
136±9
136±12
Davis, Watkins, et al. Metabolism 2001; 50: 1234-1241
9
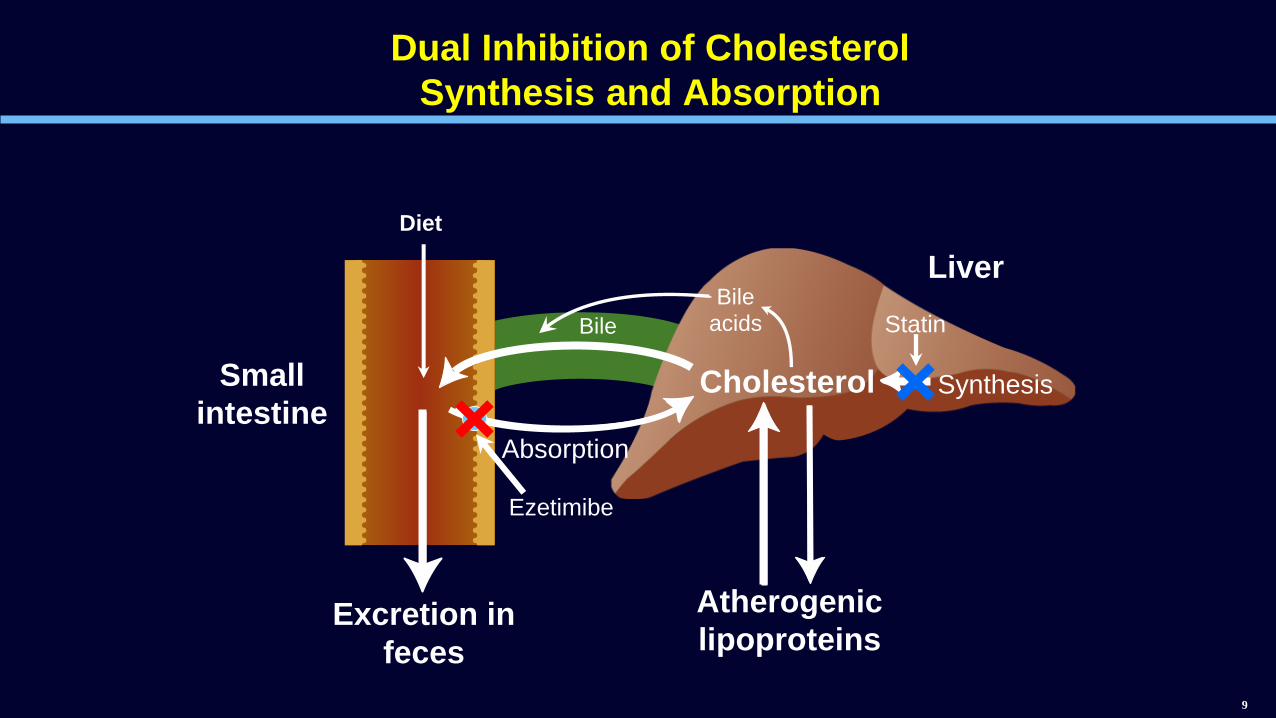
Dual Inhibition of Cholesterol
Synthesis and Absorption
Bileacids
Synthesis
Atherogenic
lipoproteins
Small
intestine
Excretion in
feces
Bile
Absorption
Liver
Diet
Statin
Cholesterol
Ezetimibe
10
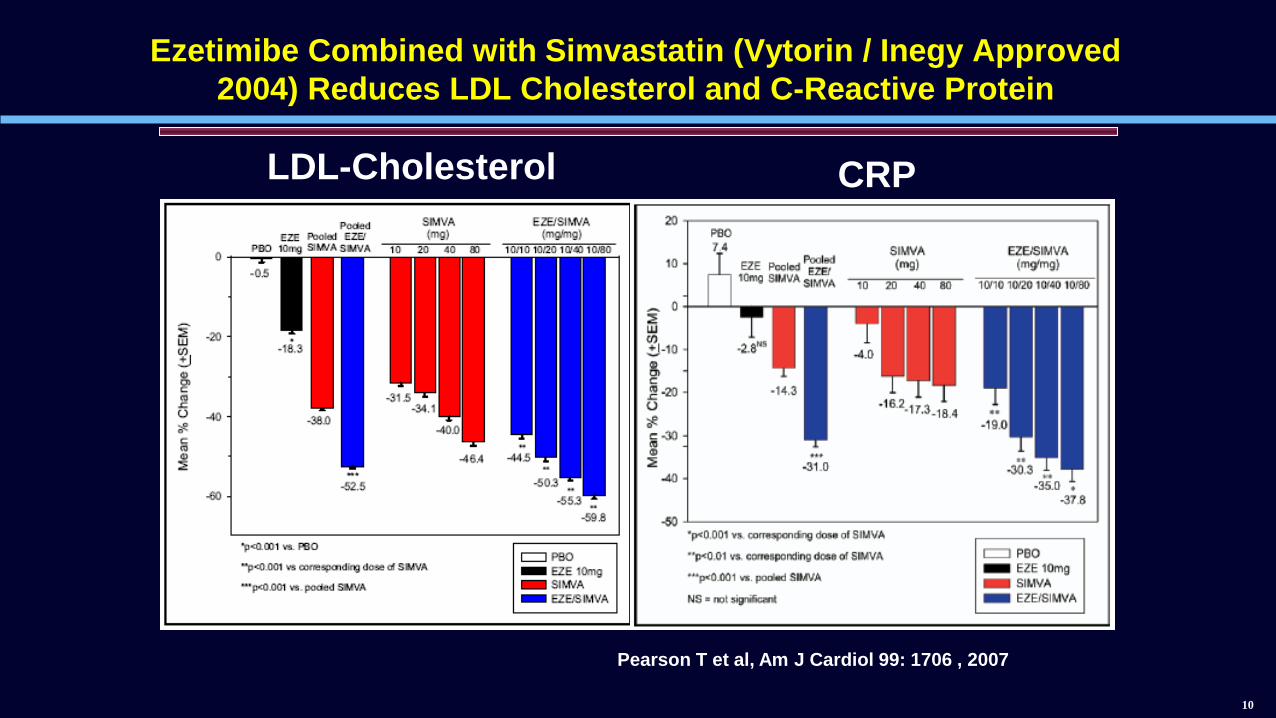
Ezetimibe Combined with Simvastatin (Vytorin / Inegy Approved
2004) Reduces LDL Cholesterol and C-Reactive Protein
Pearson T et al, Am J Cardiol 99: 1706 , 2007
LDL-Cholesterol CRP

Ezetimibe: Clinical Summary
Selective intestinal cholesterol (10 mg average 54% to 65%
reduction) and phytosterol absorption inhibitor (no effect on fat
soluble vitamins, triglycerides, etc)
Maximally effective dose is 10 mg once a day for
hypercholesterolemia and sitosterolemia
Extremely low systemic plasma levels (Cmax 0.021 uM),
circulates enterohepatically, repeatedly delivering the agent
back to the site of action (glucuronide metabolite 88% of total
plasma drug concentration)
LDL-C reduction 18% as monotherapy, and incremental 18-
25% additional reduction with statin co-administration
Plasma phytosterol levels reduced approximately 50% in
patients with sitosterolemia or hypercholesterolemia
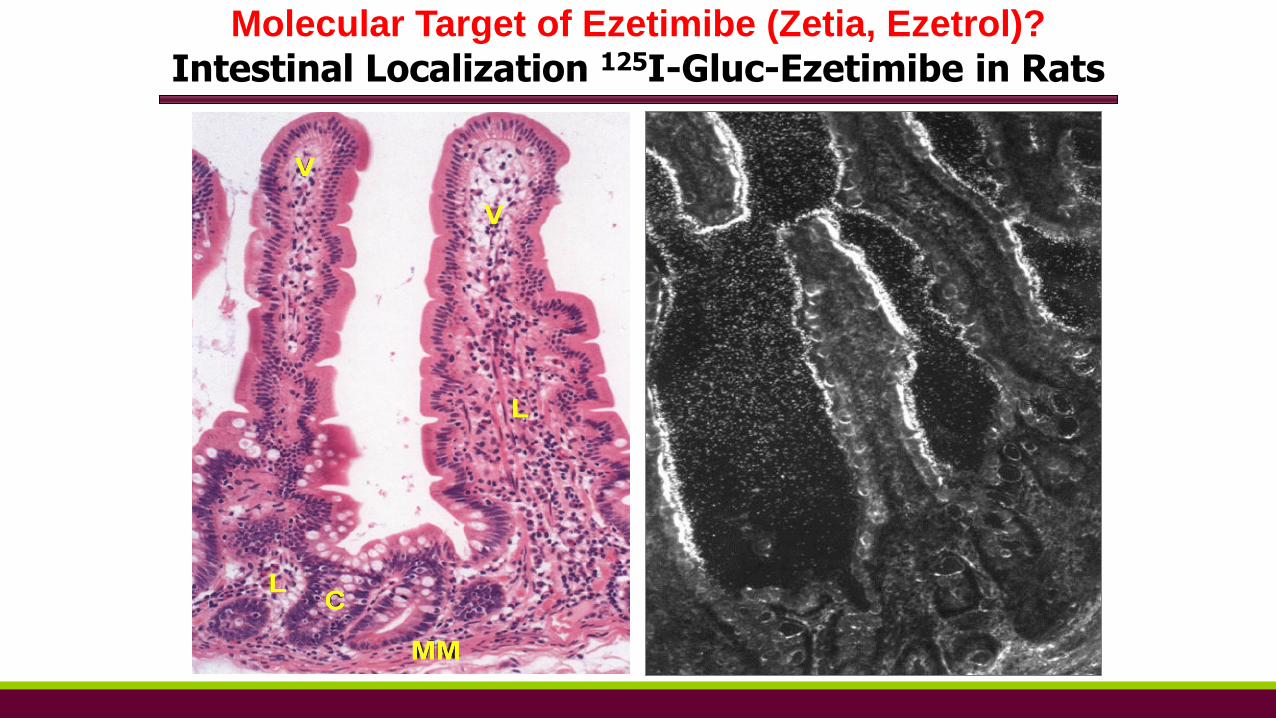
Molecular Target of Ezetimibe (Zetia, Ezetrol)?
Intestinal Localization 125I-Gluc-Ezetimibe in Rats
Genomic/ Bioinformatic Strategy to Identify the
Molecular Target of Ezetimibe
All known sterol processing mechanisms, as well as biochemical and
molecular approaches were evaluated for more than 12 years. All identified
proteins were not involved in the mechanism of action of Ezetimibe.
Genomic/ Bioinformatic Strategy Hypothetical properties of an ideal candidate cholesterol transporter:
Will be expressed in enterocytes in the proximal small intestine
– restricted tissue expression
Membrane bound protein expressed on the surface of the cell
Contain features found in proteins involved in sterol metabolism e.g.
cholesterol regulated expression, sterol sensing domain
Created and sequenced a rat small intestine DNA library of > 16,000 genes
Using bioinformatics these sequences were assembled and human and mouse
databases mined for the properties of the ideal cholesterol transporter
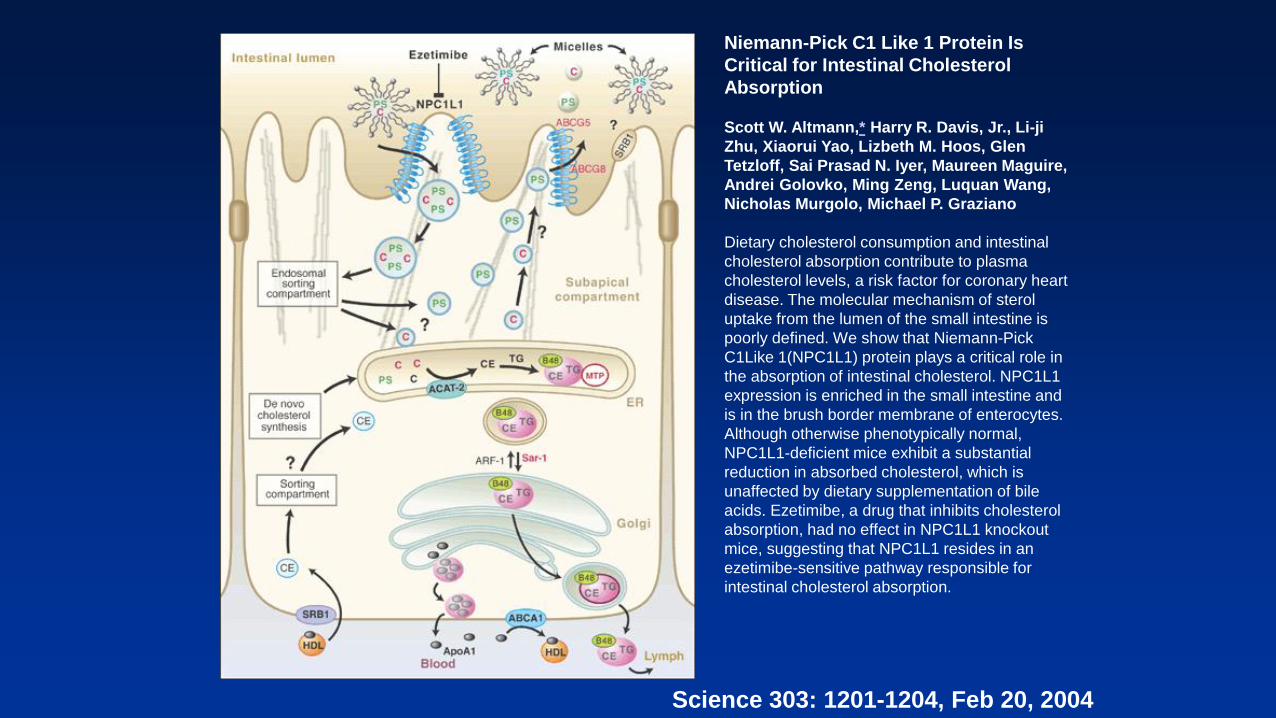
Niemann-Pick C1 Like 1 Protein Is
Critical for Intestinal Cholesterol
Absorption
Scott W. Altmann,* Harry R. Davis, Jr., Li-ji
Zhu, Xiaorui Yao, Lizbeth M. Hoos, Glen
Tetzloff, Sai Prasad N. Iyer, Maureen Maguire,
Andrei Golovko, Ming Zeng, Luquan Wang,
Nicholas Murgolo, Michael P. Graziano
Dietary cholesterol consumption and intestinal
cholesterol absorption contribute to plasma
cholesterol levels, a risk factor for coronary heart
disease. The molecular mechanism of sterol
uptake from the lumen of the small intestine is
poorly defined. We show that Niemann-Pick
C1Like 1(NPC1L1) protein plays a critical role in
the absorption of intestinal cholesterol. NPC1L1
expression is enriched in the small intestine and
is in the brush border membrane of enterocytes.
Although otherwise phenotypically normal,
NPC1L1-deficient mice exhibit a substantial
reduction in absorbed cholesterol, which is
unaffected by dietary supplementation of bile
acids. Ezetimibe, a drug that inhibits cholesterol
absorption, had no effect in NPC1L1 knockout
mice, suggesting that NPC1L1 resides in an
ezetimibe-sensitive pathway responsible for
intestinal cholesterol absorption.
Science 303: 1201-1204, Feb 20, 2004
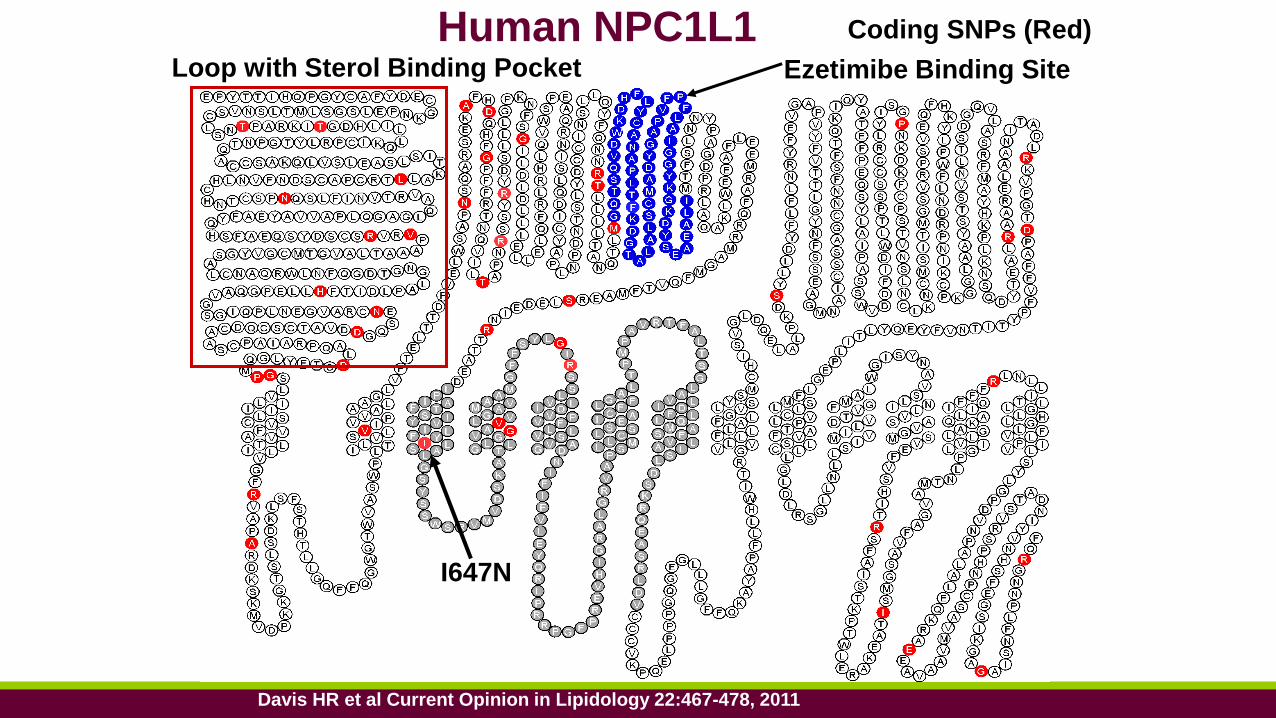
I647N
Ezetimibe Binding Site
Coding SNPs (Red)
Loop with Sterol Binding Pocket
Human NPC1L1
Davis HR et al Current Opinion in Lipidology 22:467-478, 2011
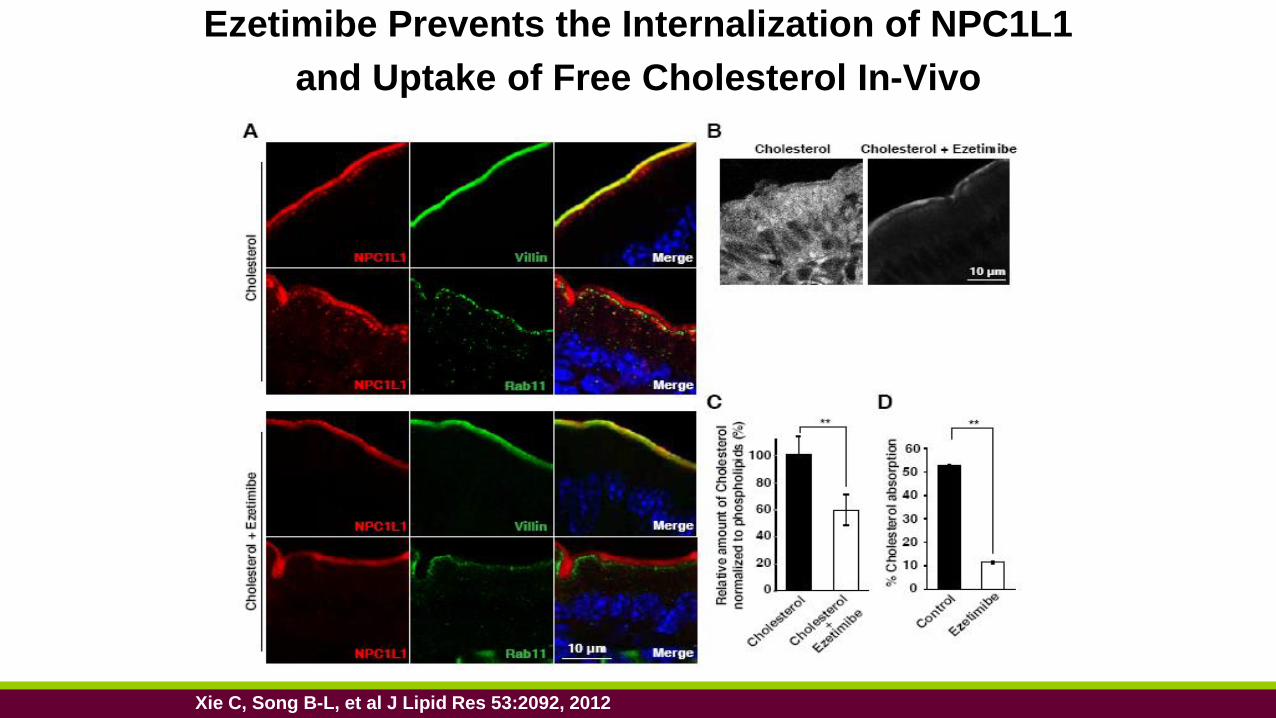
Ezetimibe Prevents the Internalization of NPC1L1
and Uptake of Free Cholesterol In-Vivo
Xie C, Song B-L, et al J Lipid Res 53:2092, 2012
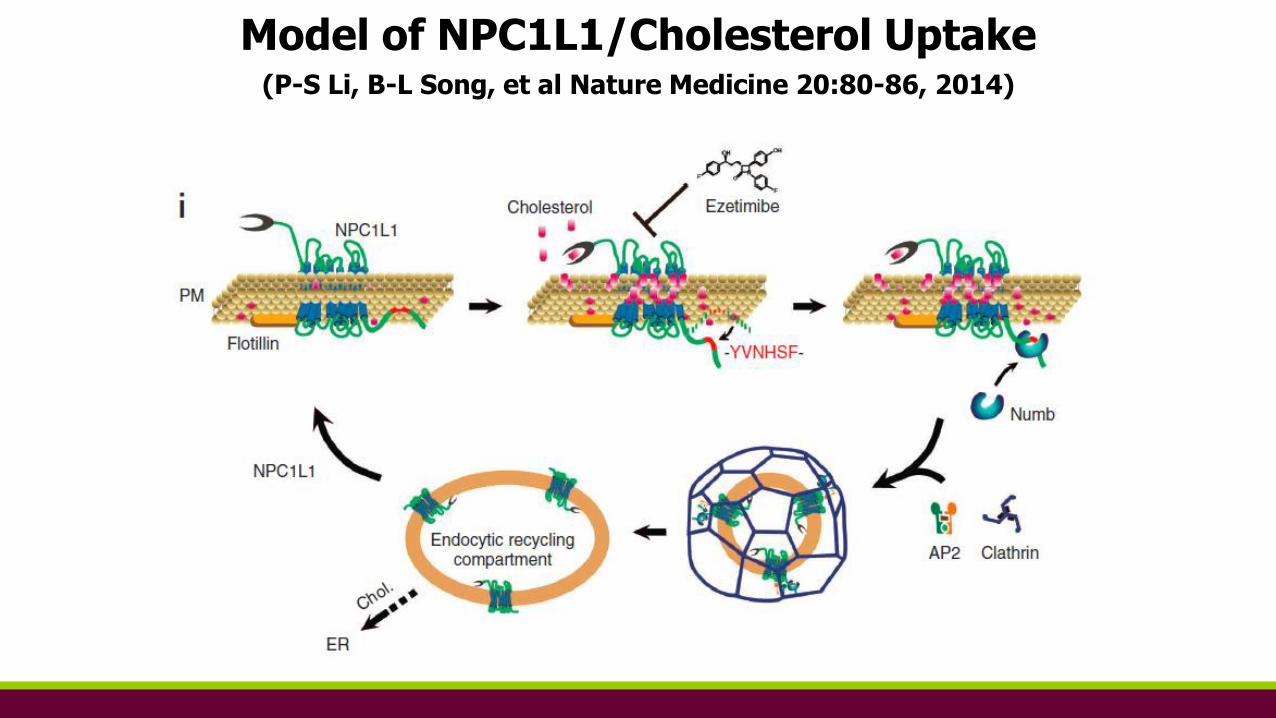
Model of NPC1L1/Cholesterol Uptake(P-S Li, B-L Song, et al Nature Medicine 20:80-86, 2014)
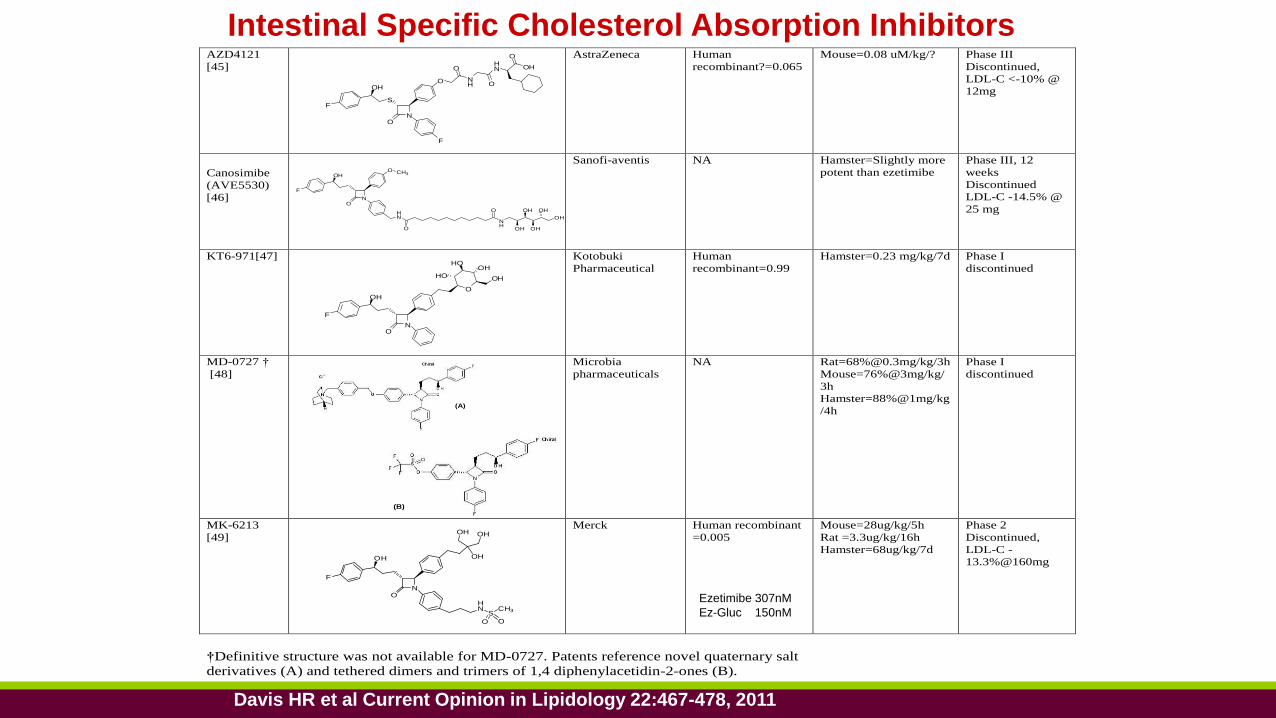
AZD4121
[45]
AstraZeneca Human
recombinant?=0.065
Mouse=0.08 uM/kg/? Phase III
Discontinued,
LDL-C <-10% @
12mg
Canosimibe
(AVE5530)
[46]
Sanofi-aventis NA Hamster=Slightly more
potent than ezetimibe
Phase III, 12
weeks
Discontinued
LDL-C -14.5% @
25 mg
KT6-971[47] Kotobuki
Pharmaceutical
Human
recombinant=0.99
Hamster=0.23 mg/kg/7d
Phase I
discontinued
MD-0727 †
[48]
Microbia
pharmaceuticals
NA Rat=68%@0.3mg/kg/3h
Mouse=76%@3mg/kg/
3h
Hamster=88%@1mg/kg
/4h
Phase I
discontinued
MK-6213
[49]
Merck Human recombinant
=0.005
Mouse=28ug/kg/5h
Rat =3.3ug/kg/16h
Hamster=68ug/kg/7d
Phase 2
Discontinued,
LDL-C -
13.3%@160mg
†Definitive structure was not available for MD-0727. Patents reference novel quaternary salt
derivatives (A) and tethered dimers and trimers of 1,4 diphenylacetidin-2-ones (B).
NO
OH
F
O
OHHO
OHHO
NO
OH
F
O CH3
HN
O
NH
O
OH
OH
OH
OH
OH
NO
S
OH
F
O NH
HN
F
O
O
OH
O
NO
OH
F
OH
HN
SCH3
O O
OHOH
(A)(A)
(B)(B)
Intestinal Specific Cholesterol Absorption Inhibitors
Davis HR et al Current Opinion in Lipidology 22:467-478, 2011
Ezetimibe 307nM
Ez-Gluc 150nM
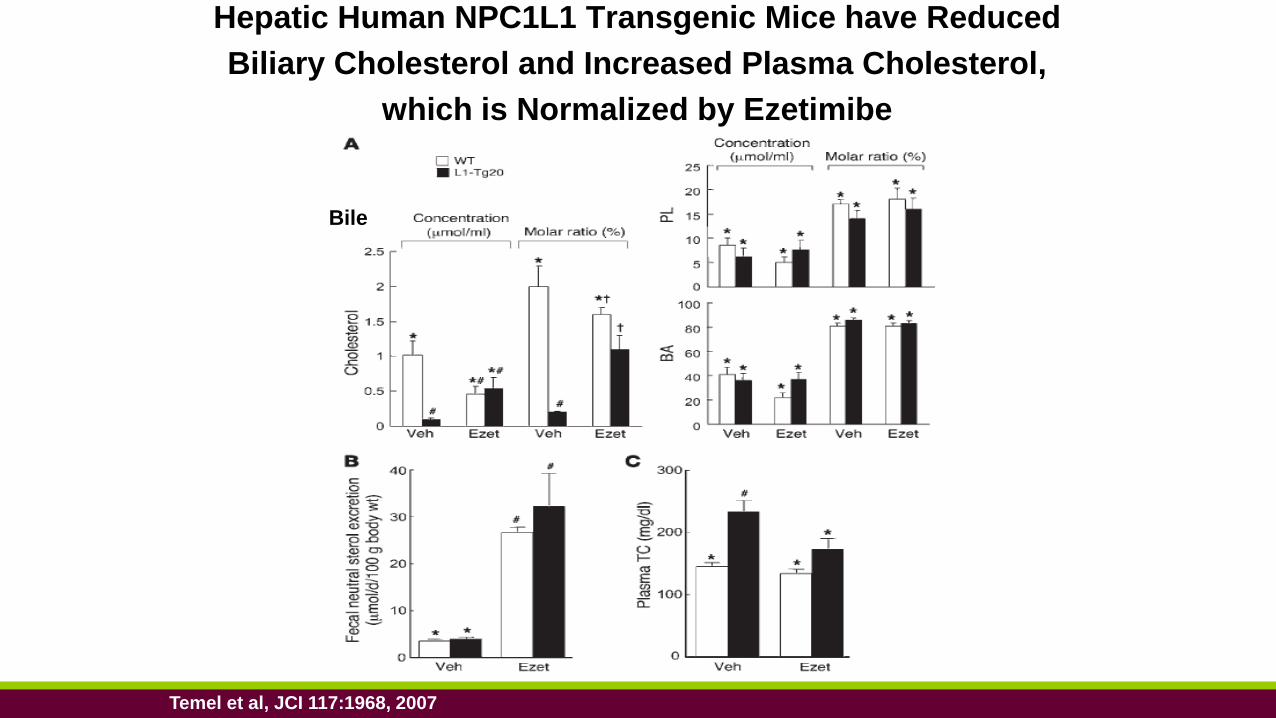
Hepatic Human NPC1L1 Transgenic Mice have Reduced
Biliary Cholesterol and Increased Plasma Cholesterol,
which is Normalized by Ezetimibe
Temel et al, JCI 117:1968, 2007
Bile
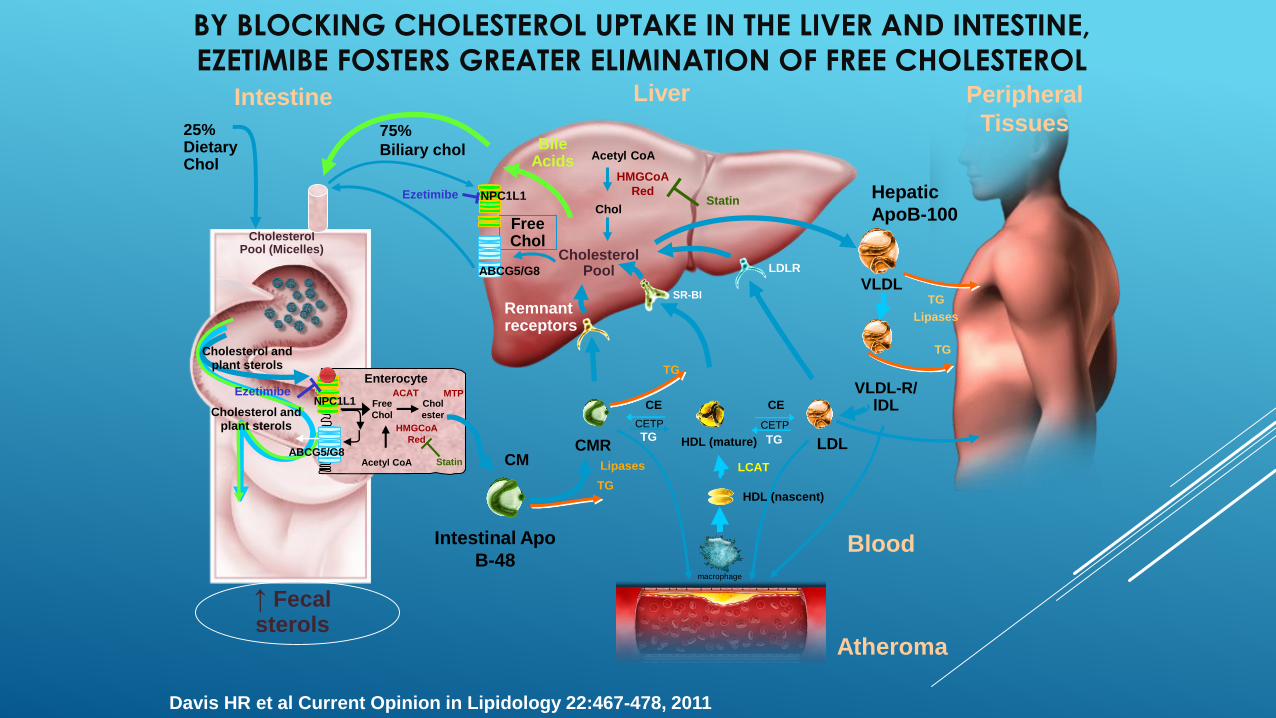
Atheroma
LiverIntestine
CholesterolPool (Micelles)
25%Dietary Chol
Bile Acids
FreeChol
↑ Fecalsterols
Remnantreceptors
Hepatic
ApoB-100
Intestinal Apo
B-48
LDLR
75%
Biliary chol
Cholesterol Pool
CMRCM
VLDL
VLDL-R/lDL
LDL
Blood
Peripheral
Tissues
TG
TG
Lipases
Lipases
TG
TG
CE
CETP
TG
CETP
TG
CE
HDL (mature)
SR-BI
LCAT
HDL (nascent)
Cholesterol andplant sterols
Cholesterol andplant sterols
Acetyl CoA
Chol
HMGCoA
RedStatin
ABCG5/G8
NPC1L1Ezetimibe
Enterocyte
ABCG5/G8
NPC1L1 Chol
ester
Free
Chol
ACAT
Acetyl CoA
MTP
HMGCoA
Red
Statin
Ezetimibe
macrophage
Davis HR et al Current Opinion in Lipidology 22:467-478, 2011
BY BLOCKING CHOLESTEROL UPTAKE IN THE LIVER AND INTESTINE,
EZETIMIBE FOSTERS GREATER ELIMINATION OF FREE CHOLESTEROL
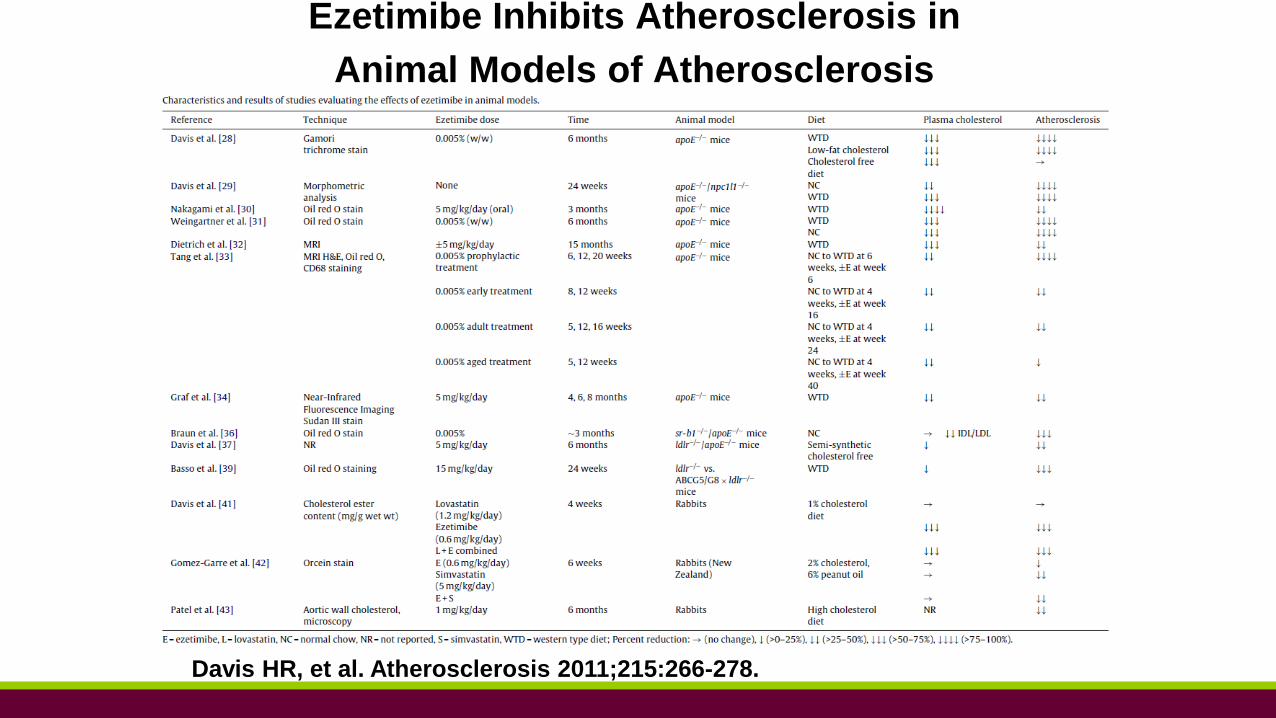
Ezetimibe Inhibits Atherosclerosis in
Animal Models of Atherosclerosis
Davis HR, et al. Atherosclerosis 2011;215:266-278.
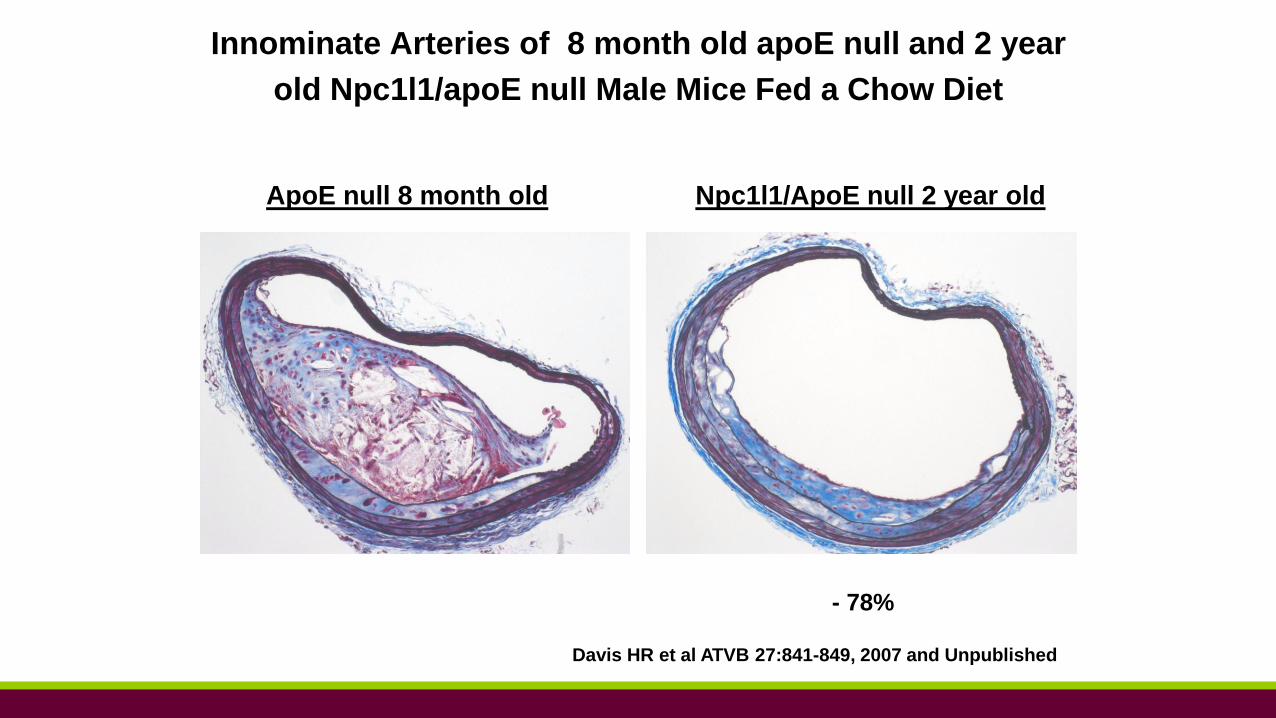
Davis HR et al ATVB 27:841-849, 2007 and Unpublished
ApoE null 8 month old Npc1l1/ApoE null 2 year old
Innominate Arteries of 8 month old apoE null and 2 year
old Npc1l1/apoE null Male Mice Fed a Chow Diet
- 78%
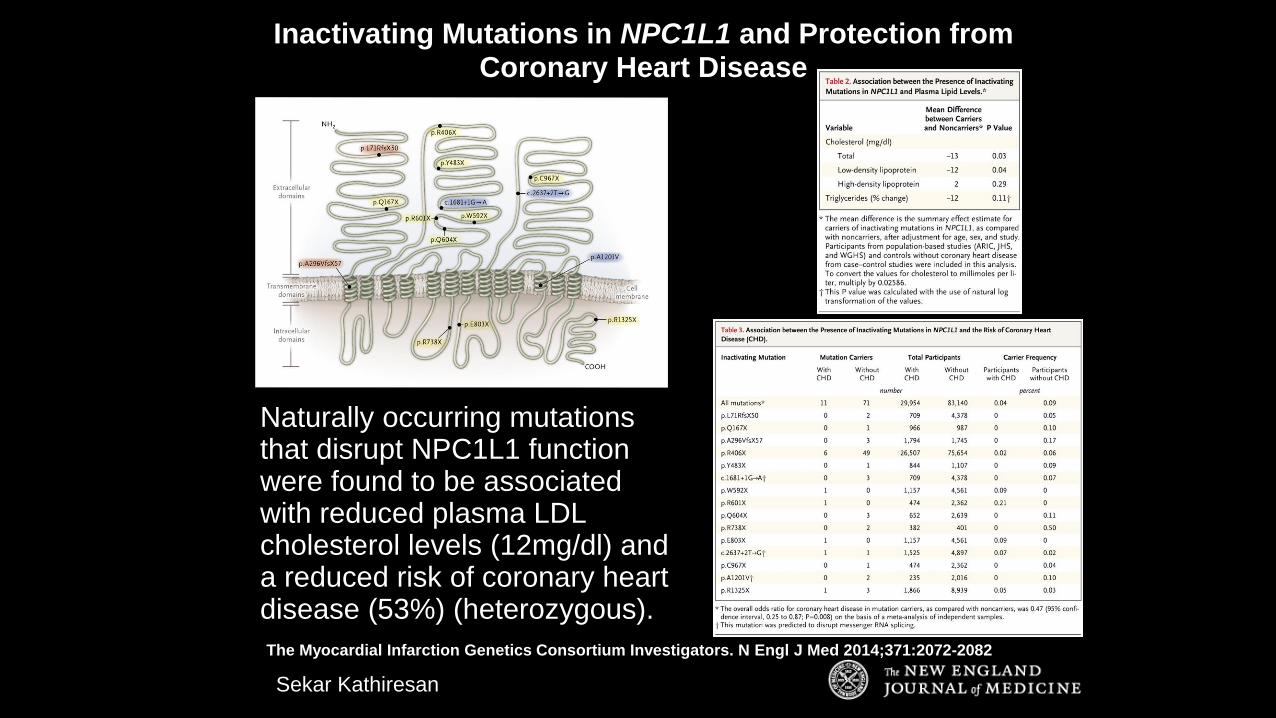
The Myocardial Infarction Genetics Consortium Investigators. N Engl J Med 2014;371:2072-2082
Naturally occurring mutations that disrupt NPC1L1 function were found to be associated with reduced plasma LDL cholesterol levels (12mg/dl) and a reduced risk of coronary heart disease (53%) (heterozygous).
Inactivating Mutations in NPC1L1 and Protection from Coronary Heart Disease
Sekar Kathiresan
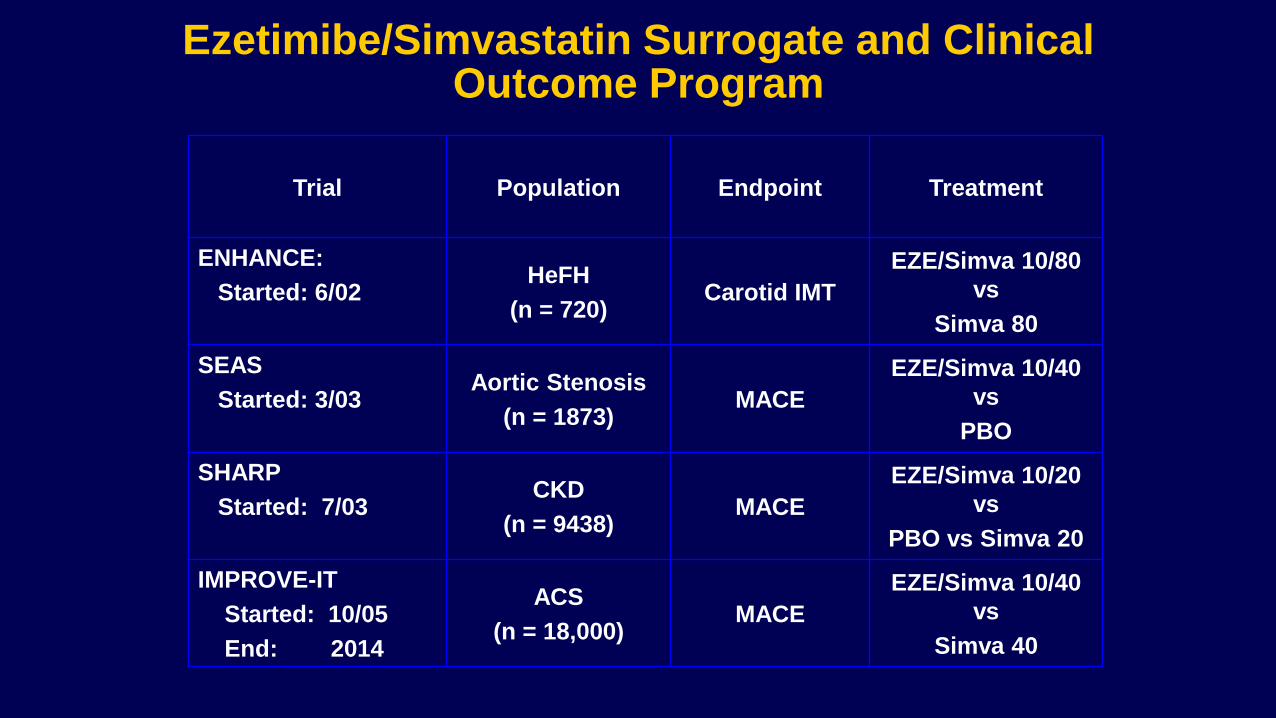
Ezetimibe/Simvastatin Surrogate and Clinical Outcome Program
Trial Population Endpoint Treatment
ENHANCE:
Started: 6/02HeFH
(n = 720)Carotid IMT
EZE/Simva 10/80
vs
Simva 80
SEAS
Started: 3/03Aortic Stenosis
(n = 1873)MACE
EZE/Simva 10/40
vs
PBO
SHARP
Started: 7/03CKD
(n = 9438)MACE
EZE/Simva 10/20
vs
PBO vs Simva 20
IMPROVE-IT
Started: 10/05
End: 2014
ACS
(n = 18,000)MACE
EZE/Simva 10/40
vs
Simva 40
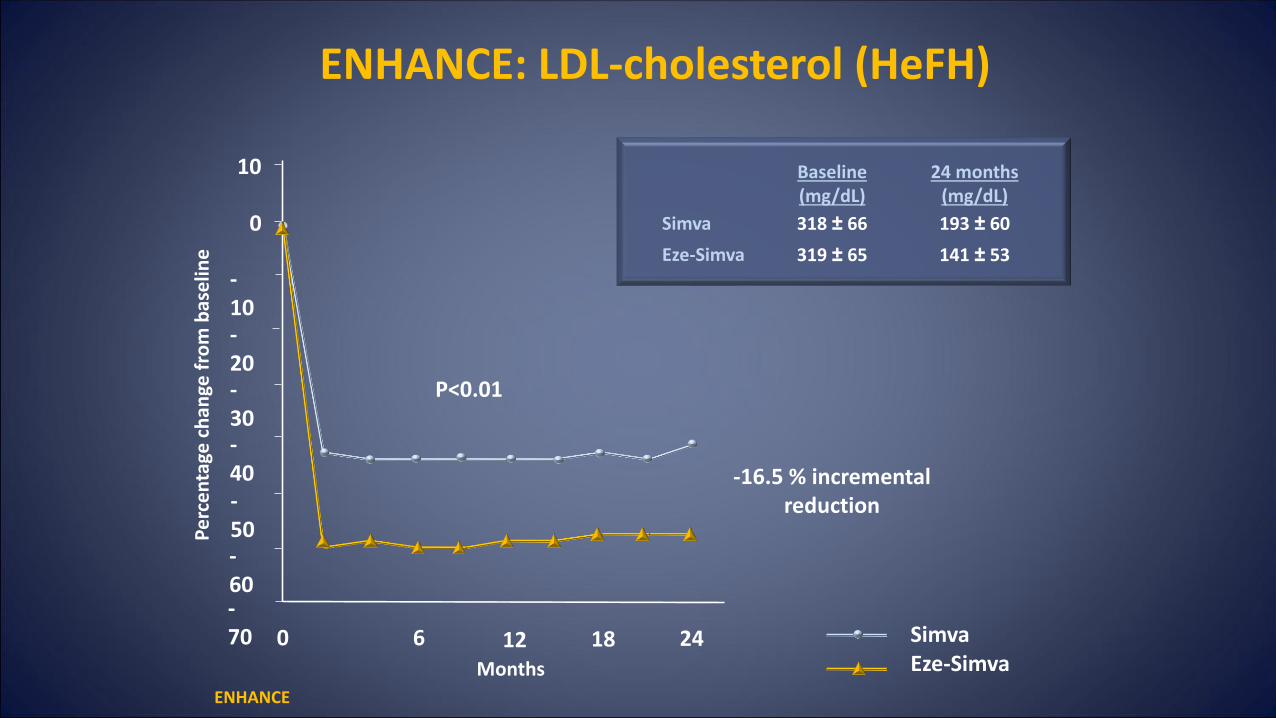
Months
ENHANCE: LDL-cholesterol (HeFH)
ENHANCE
SimvaEze-Simva
-40
0 6 12 18 24
-50-60-70
0
-10-20-30
10
Pe
rce
nta
ge c
han
ge f
rom
bas
elin
e
P<0.01
-16.5 % incremental reduction
Baseline (mg/dL)
24 months (mg/dL)
Simva 318 ± 66 193 ± 60
Eze-Simva 319 ± 65 141 ± 53
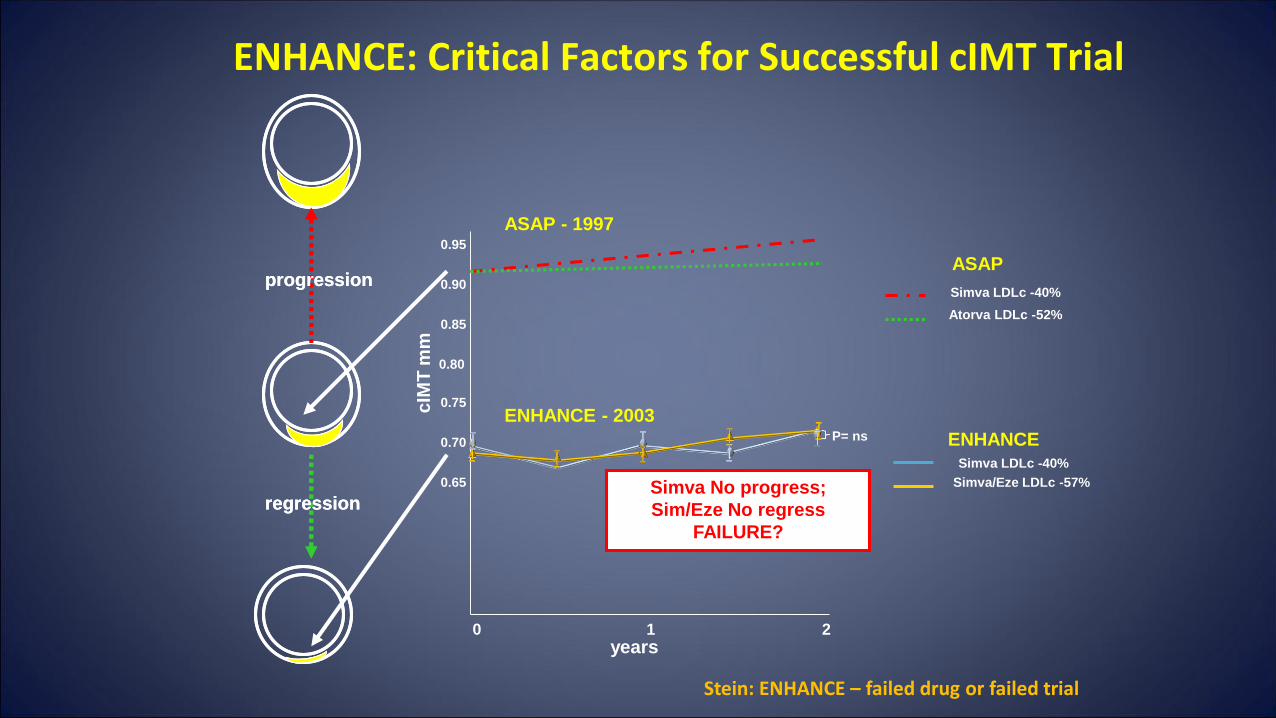
ENHANCE: Critical Factors for Successful cIMT Trial
regression
progression
regression
progression
cIM
T m
m
years0 1 2
0.80
0.85
0.75
0.90
0.95
0.70
0.65
ASAP - 1997
ENHANCE - 2003
ENHANCE
Simva LDLc -40%
Simva/Eze LDLc -57%
ASAP
Simva LDLc -40%
Atorva LDLc -52%
P= ns
Simva No progress;
Sim/Eze No regress
FAILURE?
Stein: ENHANCE – failed drug or failed trial
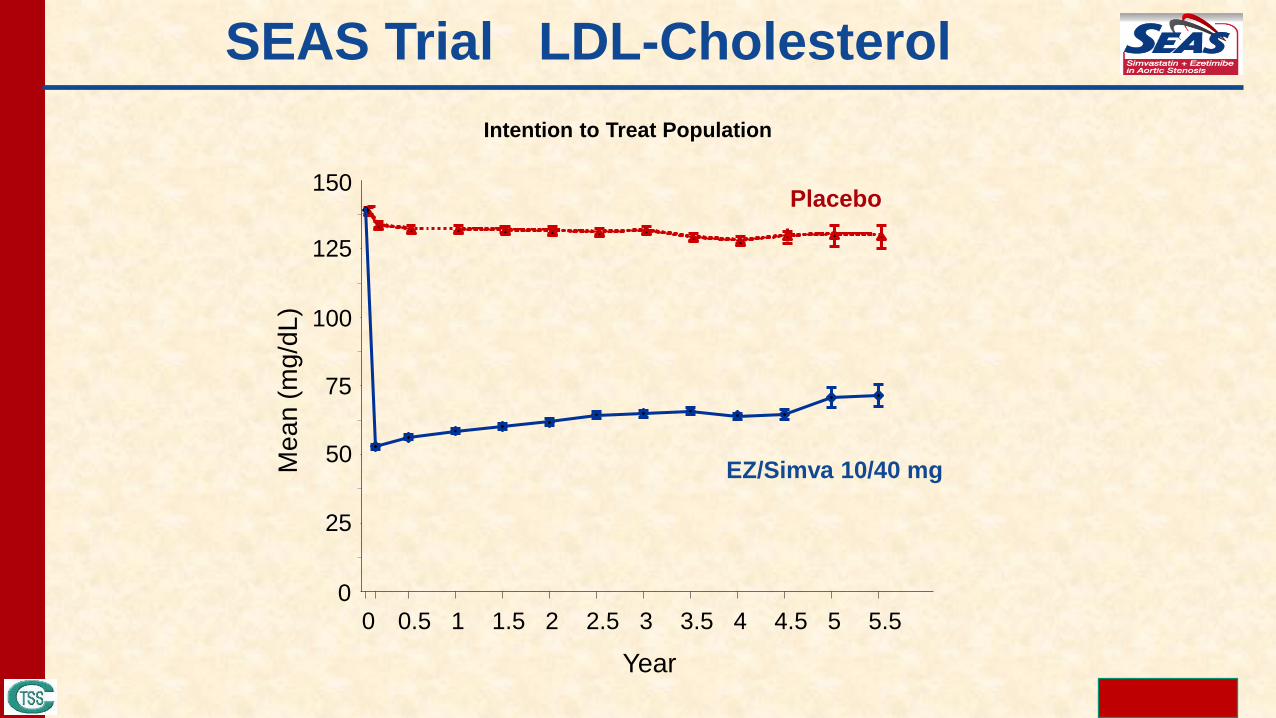
SEAS Trial LDL-Cholesterol
Intention to Treat Population
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 5.5
Year
0
25
50
75
100
125
150
Me
an
(m
g/d
L)
EZ/Simva 10/40 mg
Placebo
28
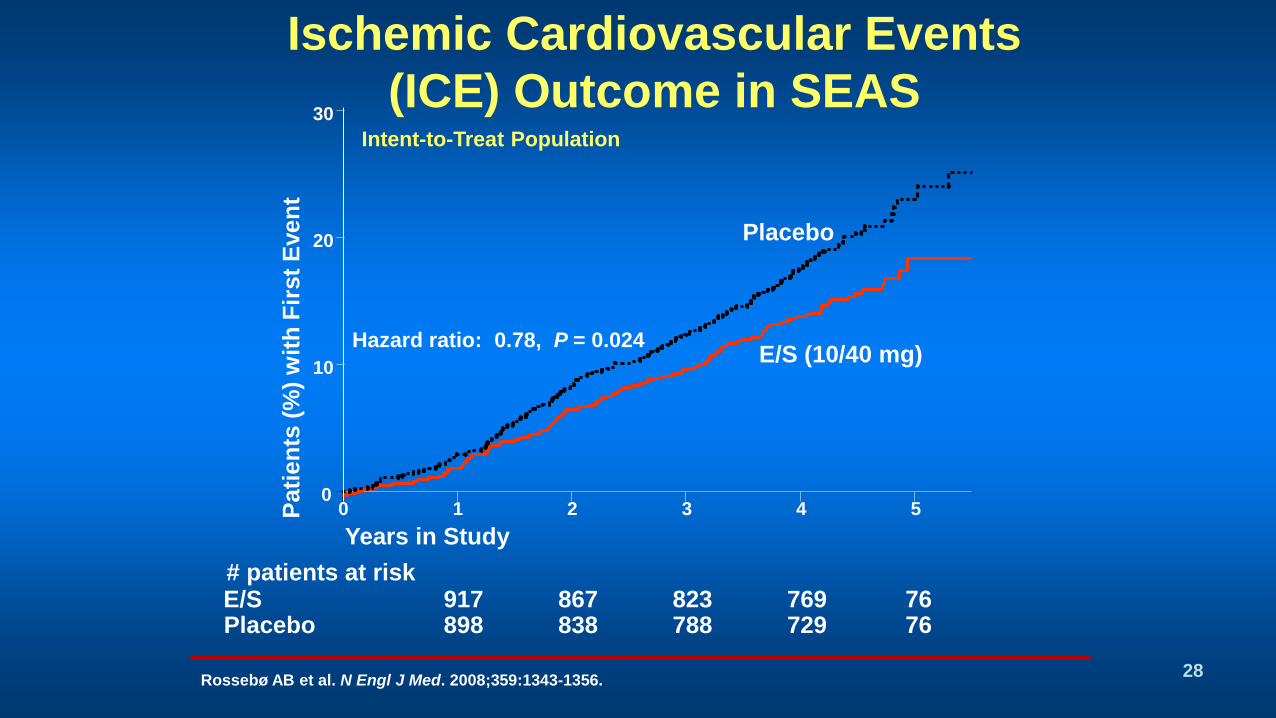
Ischemic Cardiovascular Events
(ICE) Outcome in SEAS
PlaceboE/S# patients at risk
917 898
867 838
823 788
769 729
76 76
Intent-to-Treat Population
Pati
en
ts (
%)
wit
h F
irst
Even
t
Years in Study
Hazard ratio: 0.78, P = 0.024E/S (10/40 mg)
Placebo
0 1 2 3 4 50
10
20
30
Rossebø AB et al. N Engl J Med. 2008;359:1343-1356.
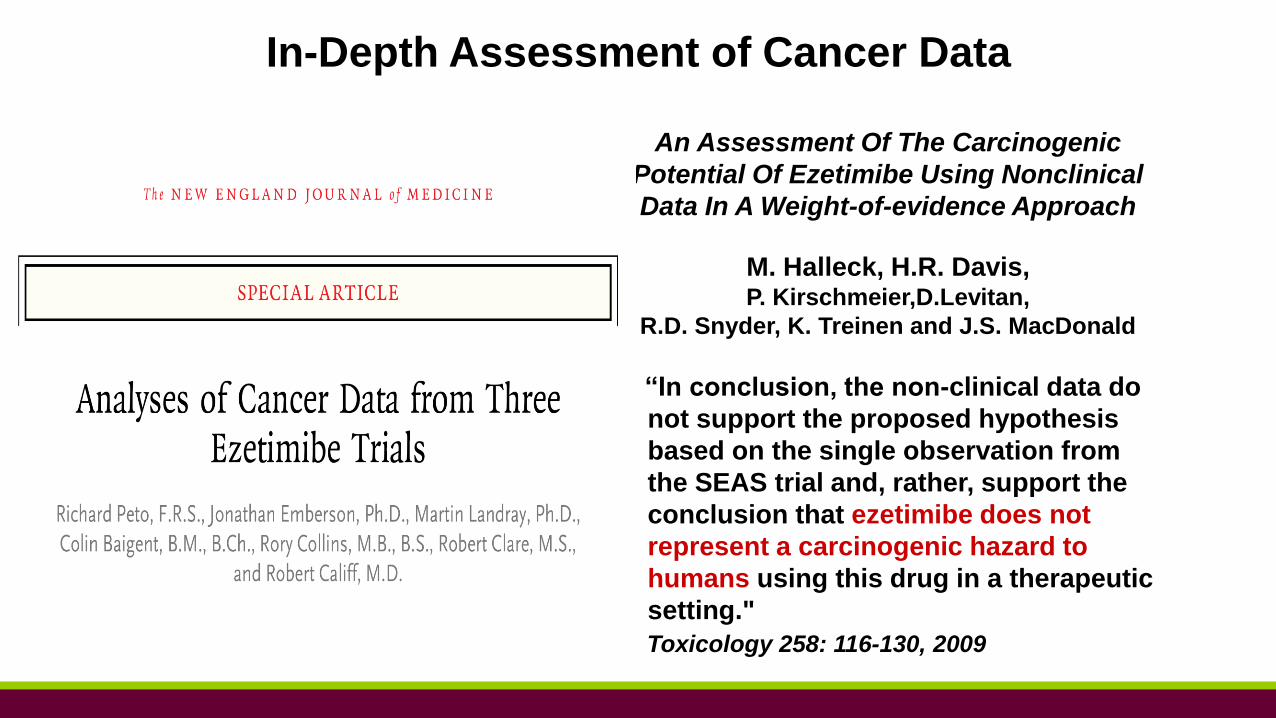
In-Depth Assessment of Cancer Data
“In conclusion, the non-clinical data do
not support the proposed hypothesis
based on the single observation from
the SEAS trial and, rather, support the
conclusion that ezetimibe does not
represent a carcinogenic hazard to
humans using this drug in a therapeutic
setting."
An Assessment Of The Carcinogenic
Potential Of Ezetimibe Using Nonclinical
Data In A Weight-of-evidence Approach
M. Halleck, H.R. Davis,P. Kirschmeier,D.Levitan,
R.D. Snyder, K. Treinen and J.S. MacDonald
Toxicology 258: 116-130, 2009
30
The SHARP StudyStudy of Heart and Renal Protection
VYTORIN® (ezetimibe/simvastatin) and ZETIA®
(ezetimibe) in Patientswith Chronic Kidney Disease
Baigent C. et al. Lancet 377:2181-2192, 2011
SHARP was designed and implemented by the
Clinical Trial Service Unit (CTSU) at the University of Oxford
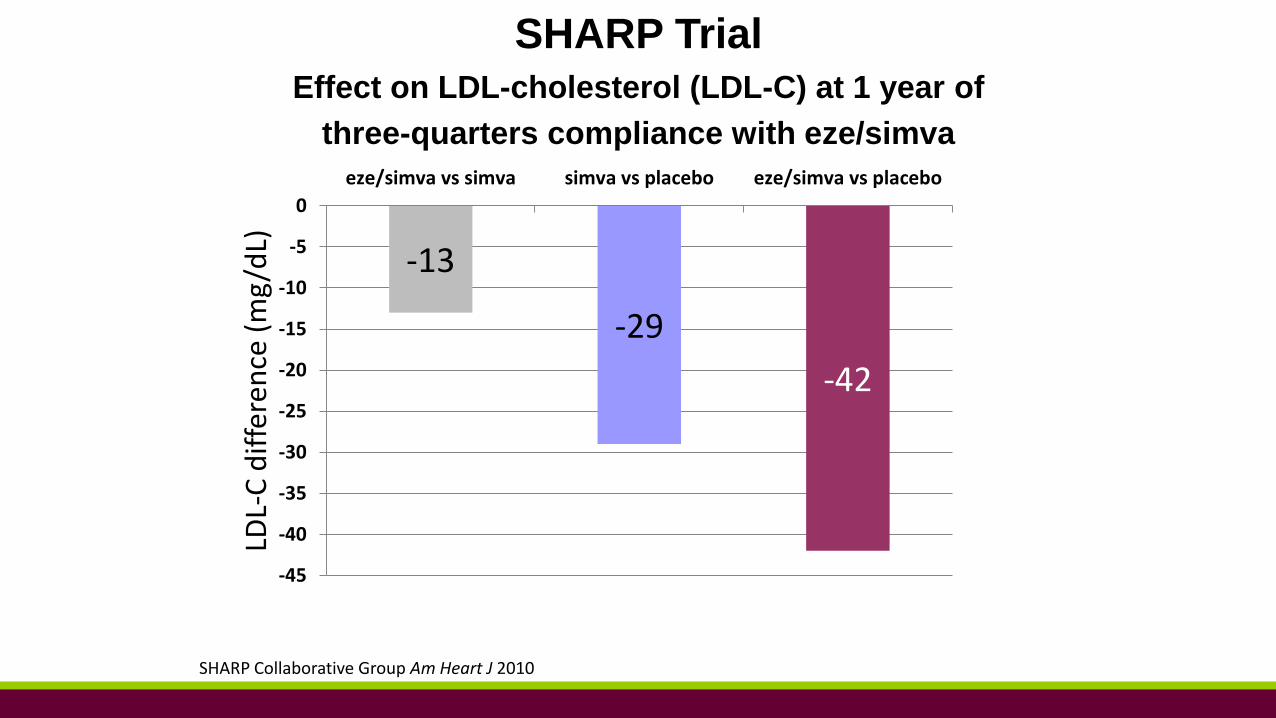
SHARP TrialEffect on LDL-cholesterol (LDL-C) at 1 year of
three-quarters compliance with eze/simva
SHARP Collaborative Group Am Heart J 2010
-13
-29
-42
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
eze/simva vs simva simva vs placebo eze/simva vs placebo
LDL-
C d
iffe
ren
ce (
mg
/dL)
0 1 2 3 4 5
Years of follow-up
0
5
10
15
20
25
Pro
po
rtio
n s
uff
erin
g ev
ent
(%)
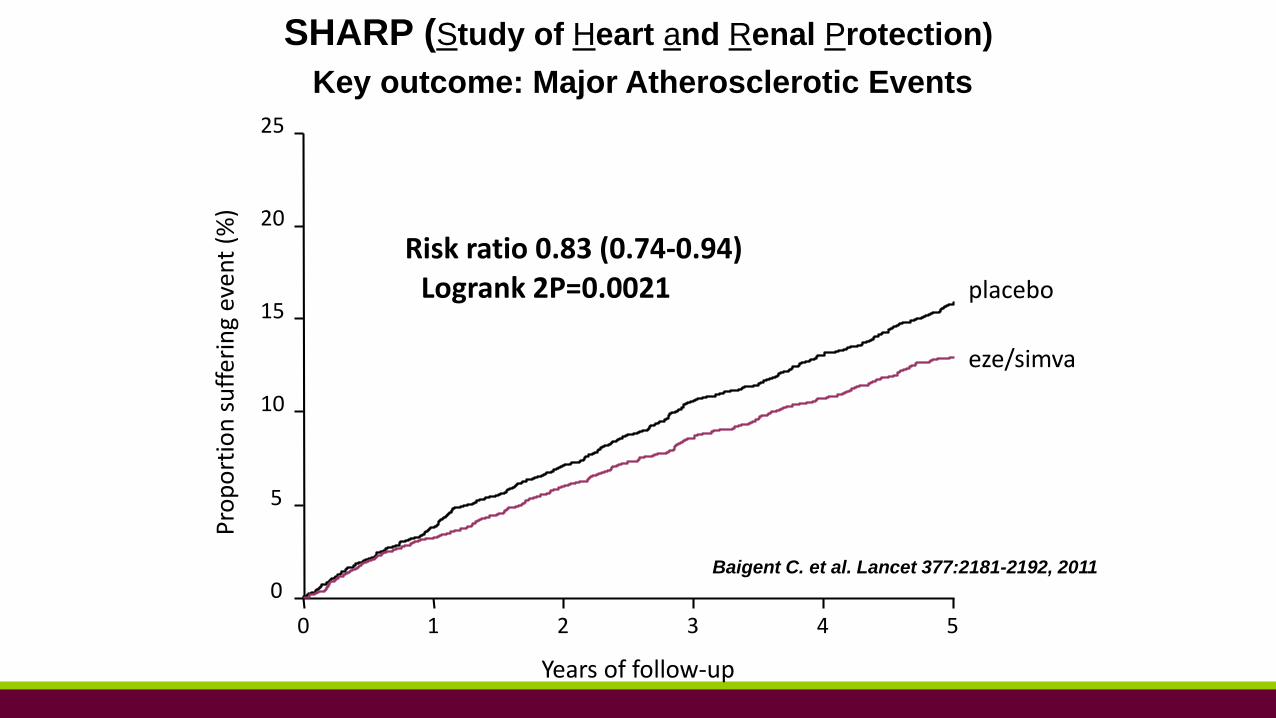
Risk ratio 0.83 (0.74-0.94) Logrank 2P=0.0021 placebo
eze/simva
SHARP (Study of Heart and Renal Protection)
Key outcome: Major Atherosclerotic Events
Baigent C. et al. Lancet 377:2181-2192, 2011
IMProved Reduction of Outcomes: Vytorin Efficacy International Trial
A Multicenter, Double-Blind, Randomized Study to Establish the
Clinical Benefit and Safety of Vytorin (Ezetimibe/Simvastatin Tablet) vs
Simvastatin Monotherapy in High-Risk Subjects Presenting
With Acute Coronary Syndrome
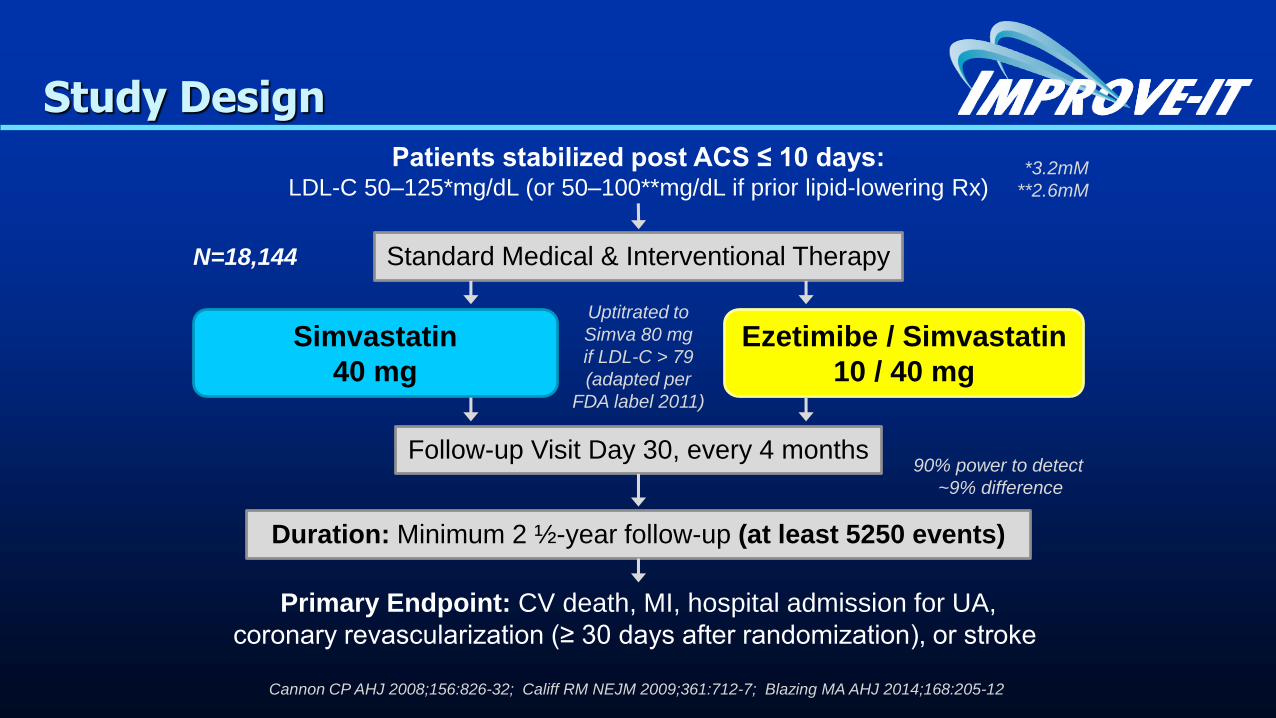
Patients stabilized post ACS ≤ 10 days:LDL-C 50–125*mg/dL (or 50–100**mg/dL if prior lipid-lowering Rx)
Standard Medical & Interventional Therapy
Ezetimibe / Simvastatin
10 / 40 mg
Simvastatin
40 mg
Follow-up Visit Day 30, every 4 months
Duration: Minimum 2 ½-year follow-up (at least 5250 events)
Primary Endpoint: CV death, MI, hospital admission for UA,
coronary revascularization (≥ 30 days after randomization), or stroke
N=18,144
Uptitrated to
Simva 80 mg
if LDL-C > 79
(adapted per
FDA label 2011)
Study Design
*3.2mM
**2.6mM
Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:205-12
90% power to detect
~9% difference
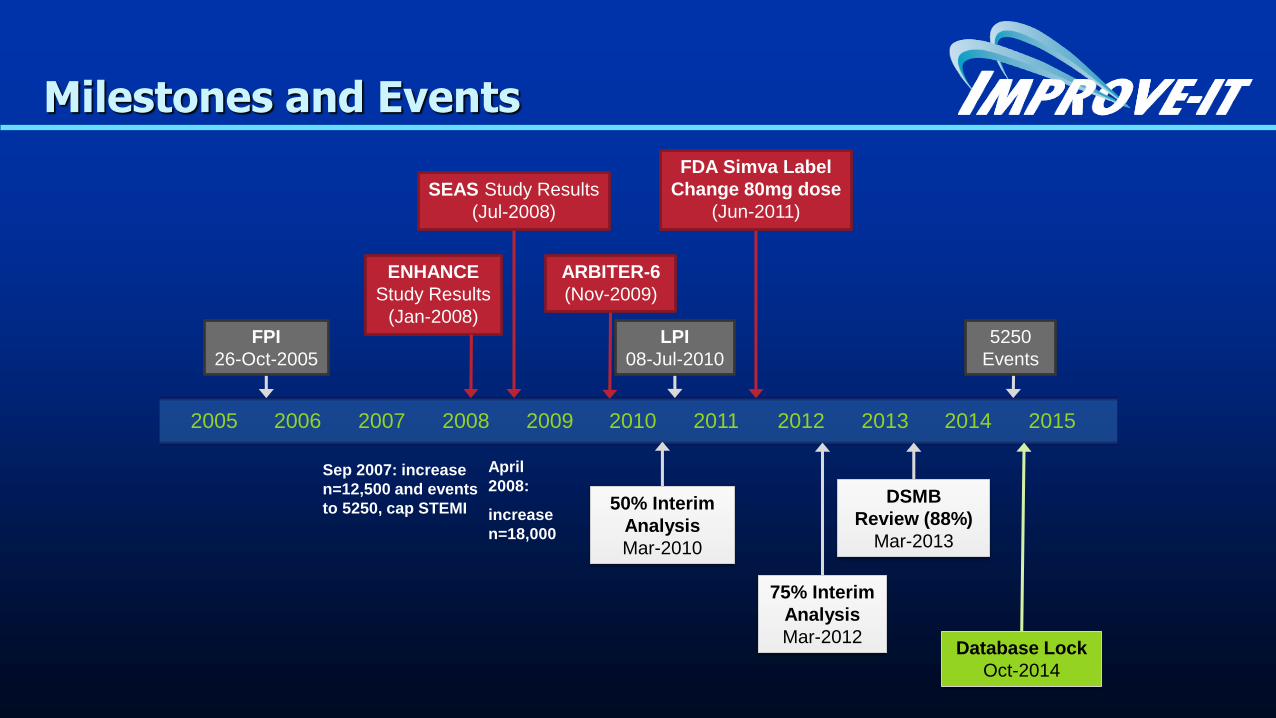
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Milestones and Events
ENHANCE
Study Results
(Jan-2008)
75% Interim
Analysis
Mar-2012
DSMB
Review (88%)
Mar-2013
Database Lock
Oct-2014
LPI
08-Jul-2010
50% Interim
Analysis
Mar-2010
ARBITER-6
(Nov-2009)
FDA Simva Label
Change 80mg dose
(Jun-2011)
5250
Events
SEAS Study Results
(Jul-2008)
FPI
26-Oct-2005
Sep 2007: increase
n=12,500 and events
to 5250, cap STEMI
April
2008:
increase
n=18,000
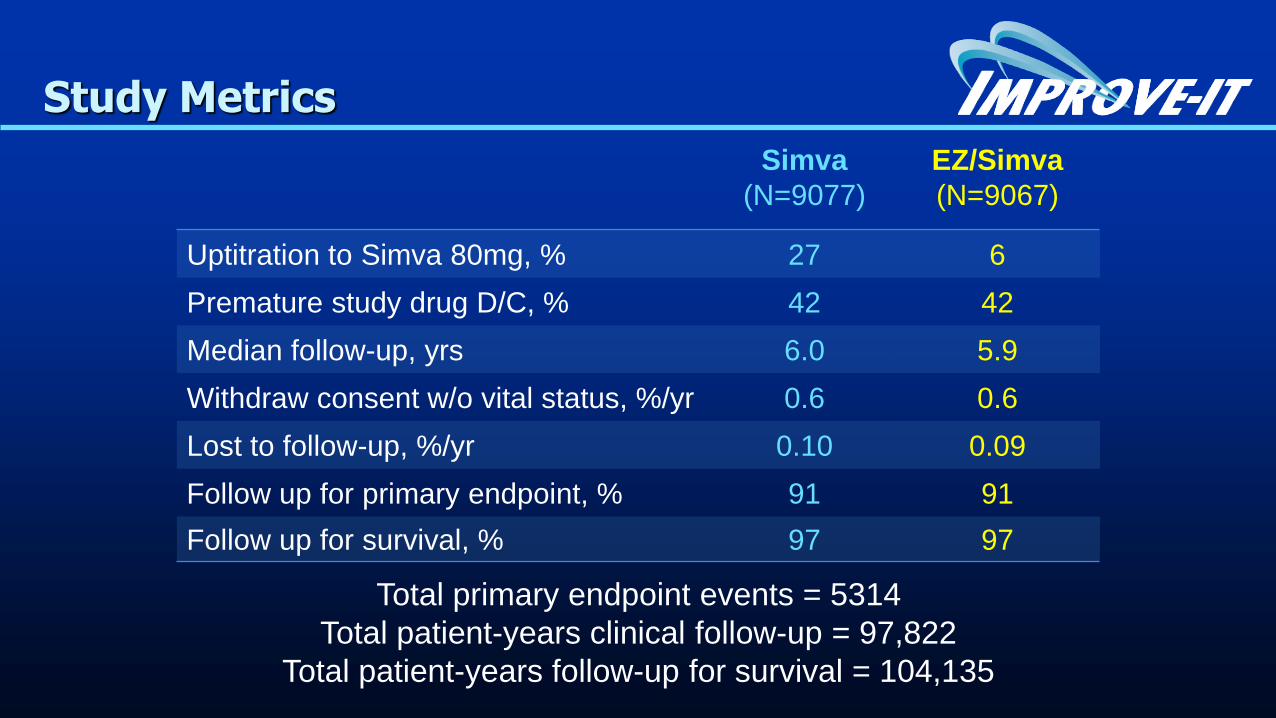
Study Metrics
Simva
(N=9077)
EZ/Simva
(N=9067)
Uptitration to Simva 80mg, % 27 6
Premature study drug D/C, % 42 42
Median follow-up, yrs 6.0 5.9
Withdraw consent w/o vital status, %/yr 0.6 0.6
Lost to follow-up, %/yr 0.10 0.09
Follow up for primary endpoint, % 91 91
Follow up for survival, % 97 97
Total primary endpoint events = 5314
Total patient-years clinical follow-up = 97,822
Total patient-years follow-up for survival = 104,135
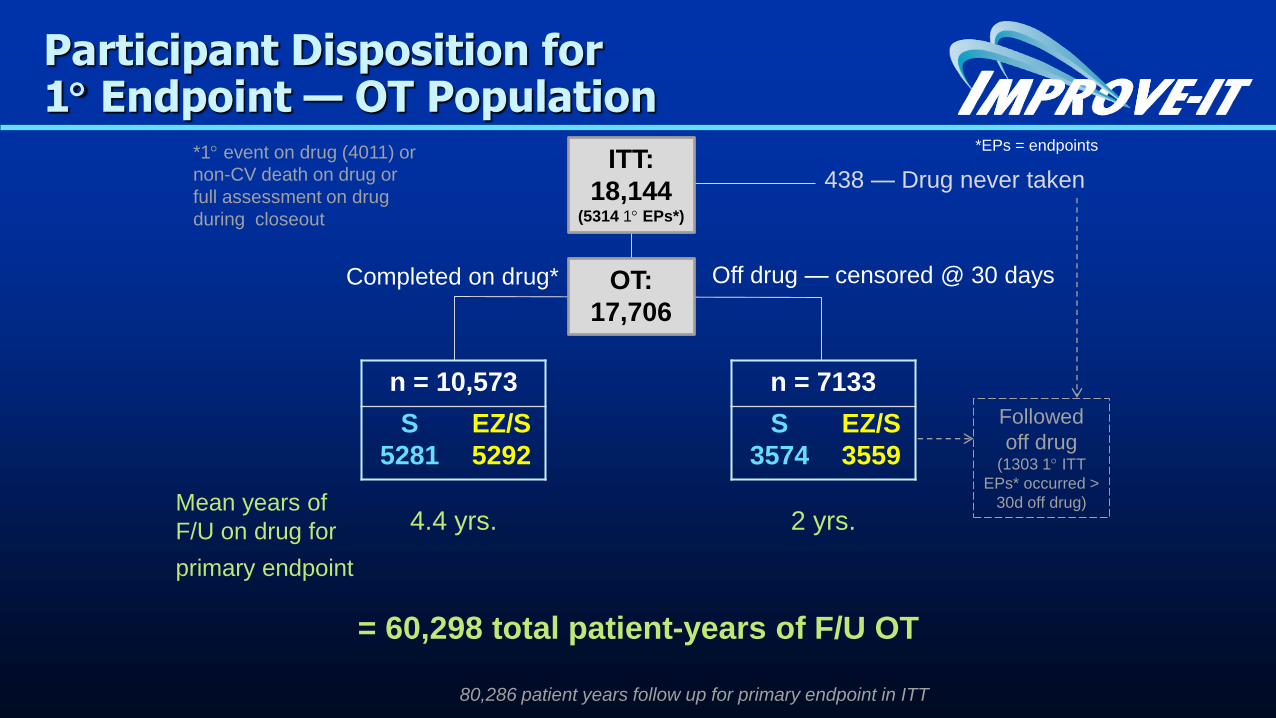
438 — Drug never taken
Participant Disposition for1 Endpoint — OT Population
Off drug — censored @ 30 daysCompleted on drug*
80,286 patient years follow up for primary endpoint in ITT
ITT:
18,144(5314 1 EPs*)
n = 7133
S
3574
EZ/S
3559
2 yrs.
OT:
17,706
n = 10,573
S
5281
EZ/S
5292
4.4 yrs.
= 60,298 total patient-years of F/U OT
Mean years of
F/U on drug for
primary endpoint
*1 event on drug (4011) or
non-CV death on drug or
full assessment on drug
during closeout
Followed
off drug(1303 1 ITT
EPs* occurred >
30d off drug)
*EPs = endpoints
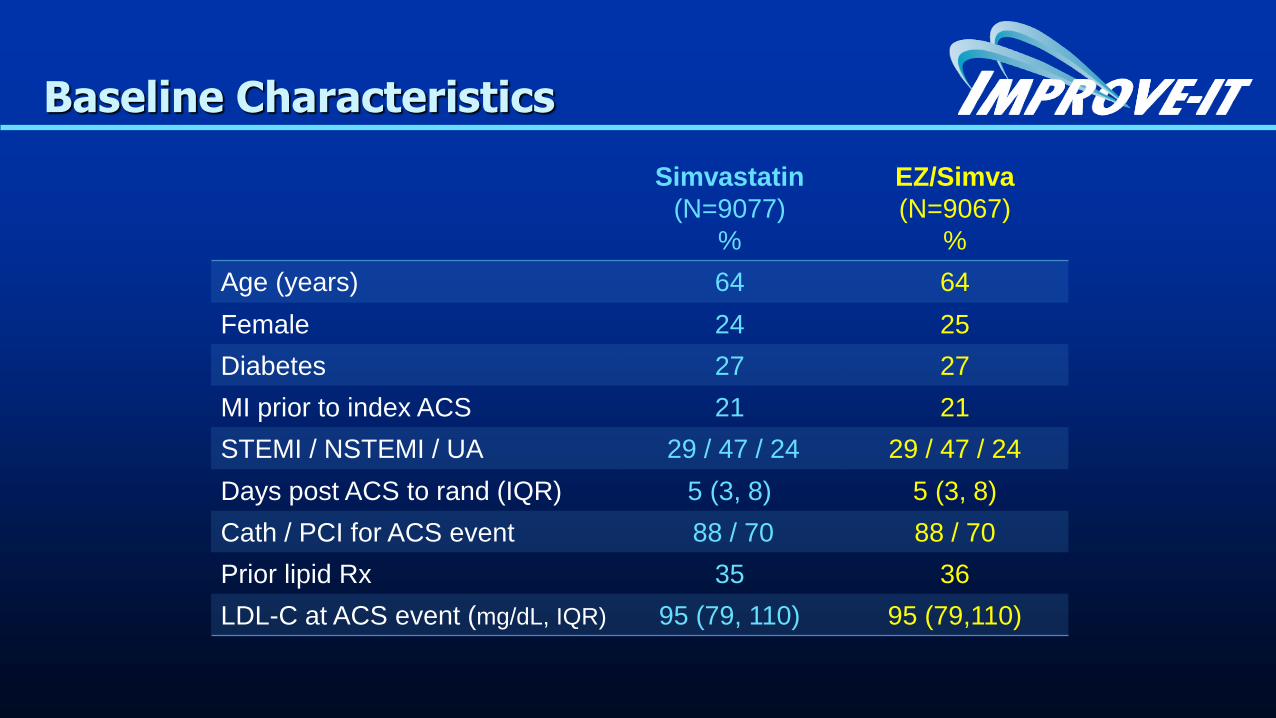
Baseline Characteristics
Simvastatin
(N=9077)
%
EZ/Simva
(N=9067)
%
Age (years) 64 64
Female 24 25
Diabetes 27 27
MI prior to index ACS 21 21
STEMI / NSTEMI / UA 29 / 47 / 24 29 / 47 / 24
Days post ACS to rand (IQR) 5 (3, 8) 5 (3, 8)
Cath / PCI for ACS event 88 / 70 88 / 70
Prior lipid Rx 35 36
LDL-C at ACS event (mg/dL, IQR) 95 (79, 110) 95 (79,110)
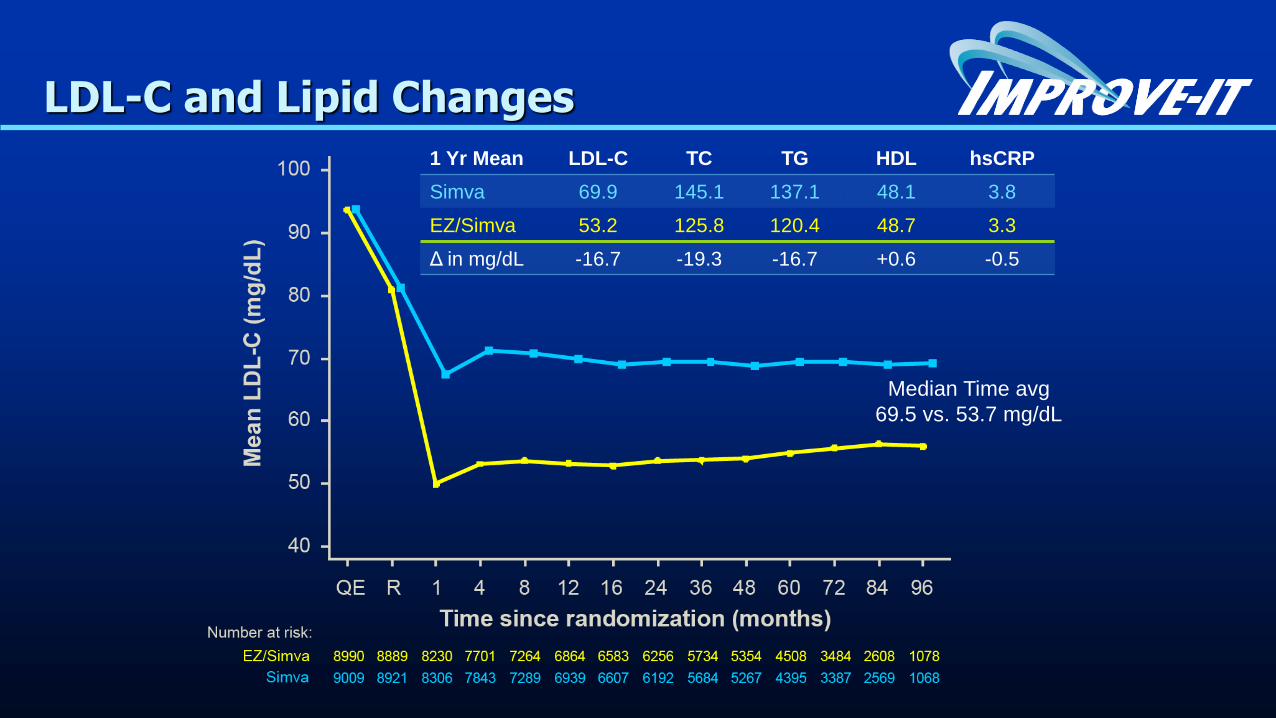
LDL-C and Lipid Changes
1 Yr Mean LDL-C TC TG HDL hsCRP
Simva 69.9 145.1 137.1 48.1 3.8
EZ/Simva 53.2 125.8 120.4 48.7 3.3
Δ in mg/dL -16.7 -19.3 -16.7 +0.6 -0.5
Median Time avg
69.5 vs. 53.7 mg/dL
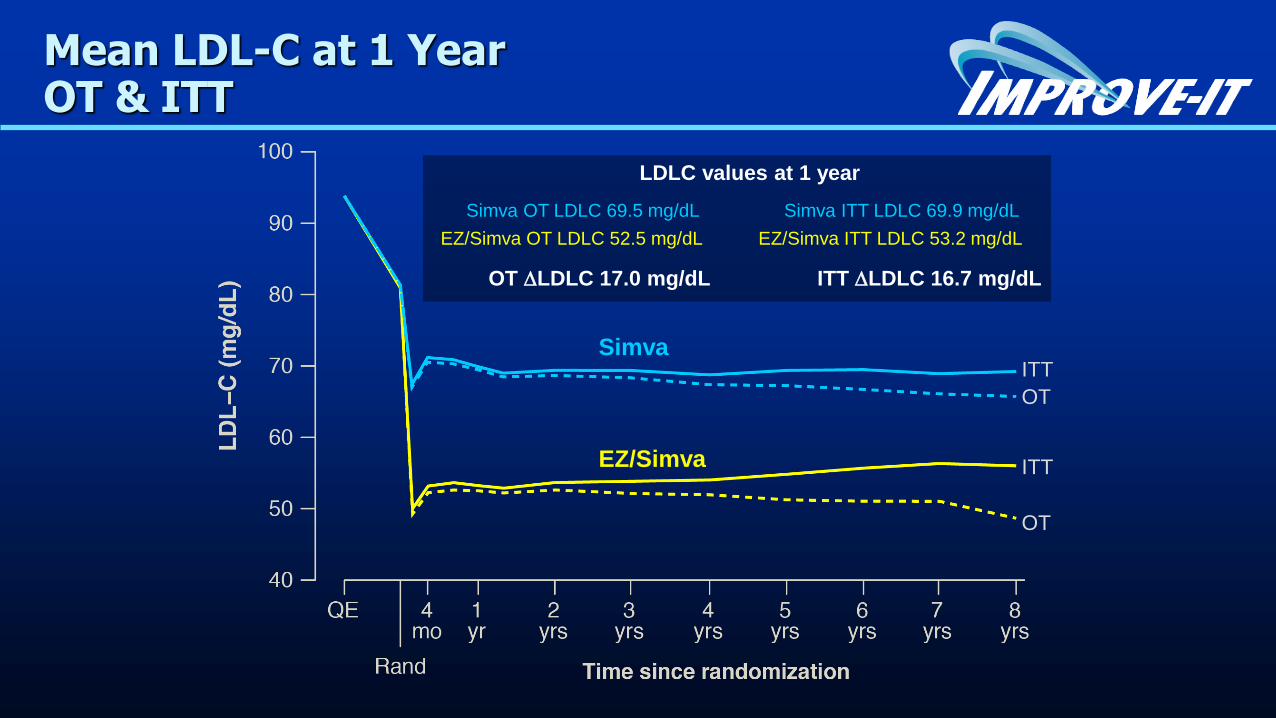
Mean LDL-C at 1 Year OT & ITT
Simva OT LDLC 69.5 mg/dL Simva ITT LDLC 69.9 mg/dL
LDLC values at 1 year
ITT
OT
ITT
OT
EZ/Simva OT LDLC 52.5 mg/dL EZ/Simva ITT LDLC 53.2 mg/dL
OT LDLC 17.0 mg/dL ITT LDLC 16.7 mg/dL
EZ/Simva
Simva
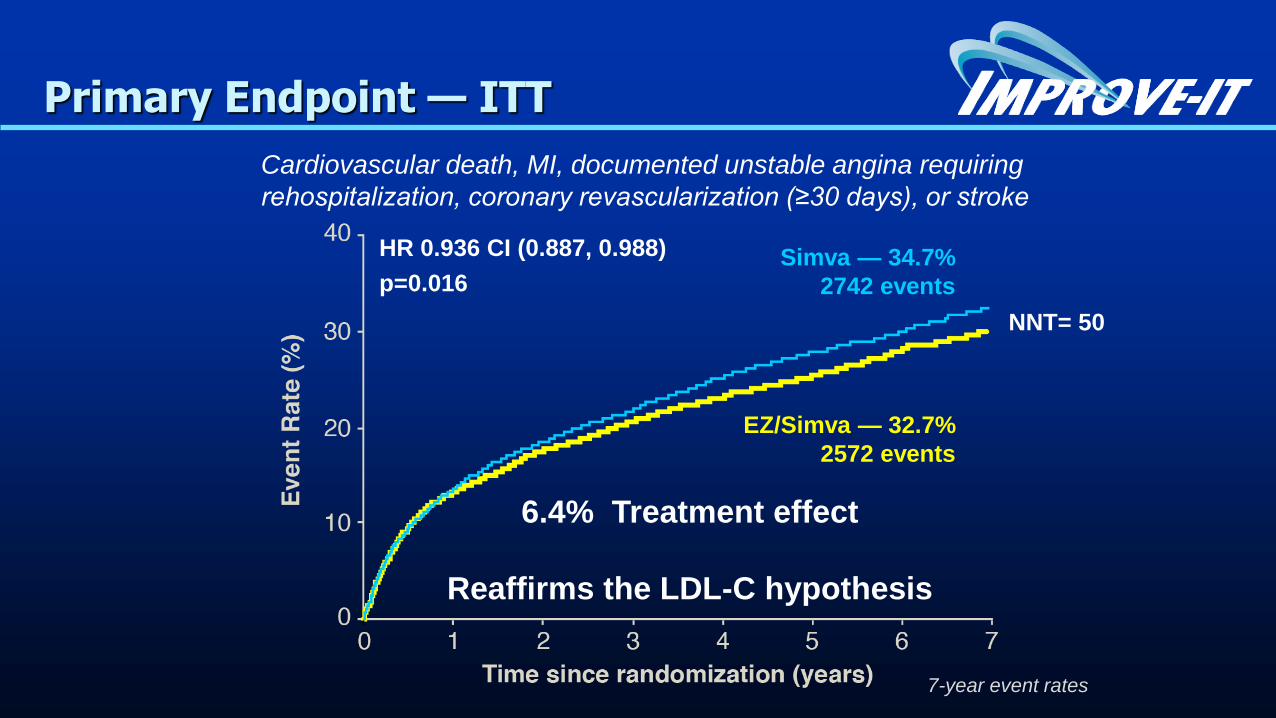
Primary Endpoint — ITT
Simva — 34.7%
2742 events
EZ/Simva — 32.7%
2572 events
HR 0.936 CI (0.887, 0.988)
p=0.016
Cardiovascular death, MI, documented unstable angina requiring
rehospitalization, coronary revascularization (≥30 days), or stroke
7-year event rates
NNT= 50
6.4% Treatment effect
Reaffirms the LDL-C hypothesis
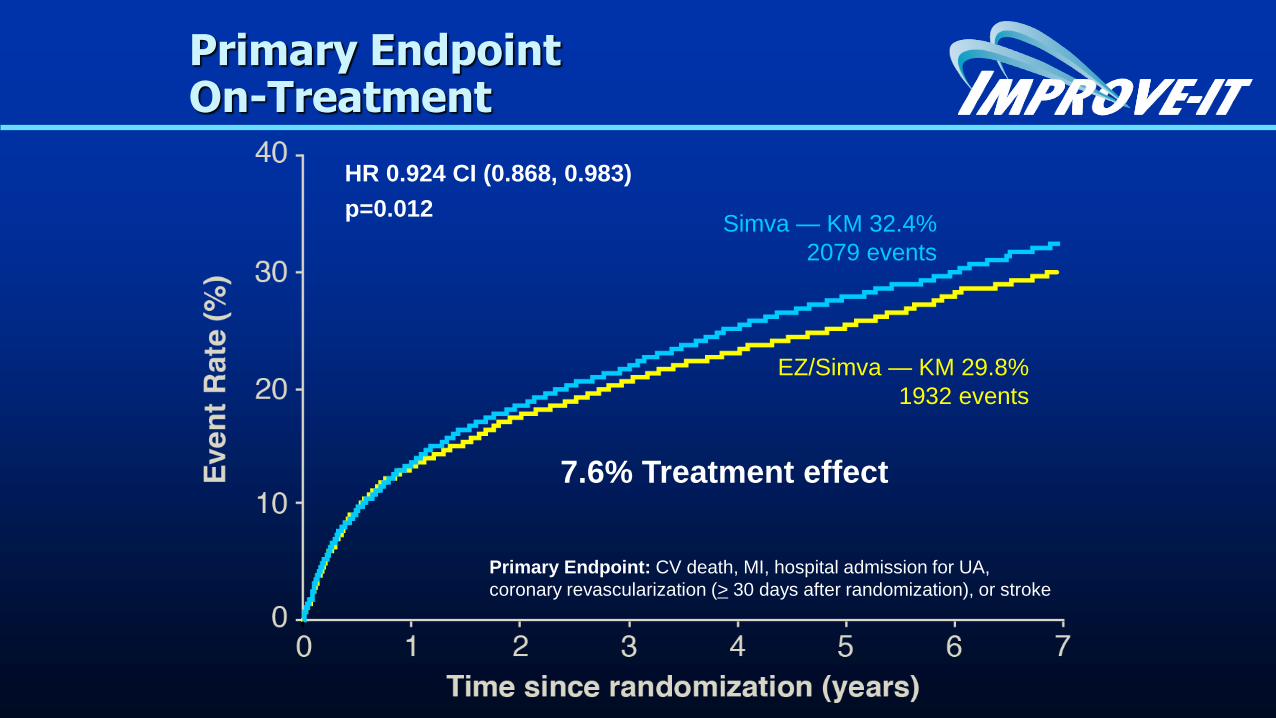
Primary Endpoint On-Treatment
Simva — KM 32.4%
2079 events
EZ/Simva — KM 29.8%
1932 events
HR 0.924 CI (0.868, 0.983)
p=0.012
Primary Endpoint: CV death, MI, hospital admission for UA,
coronary revascularization (> 30 days after randomization), or stroke
7.6% Treatment effect
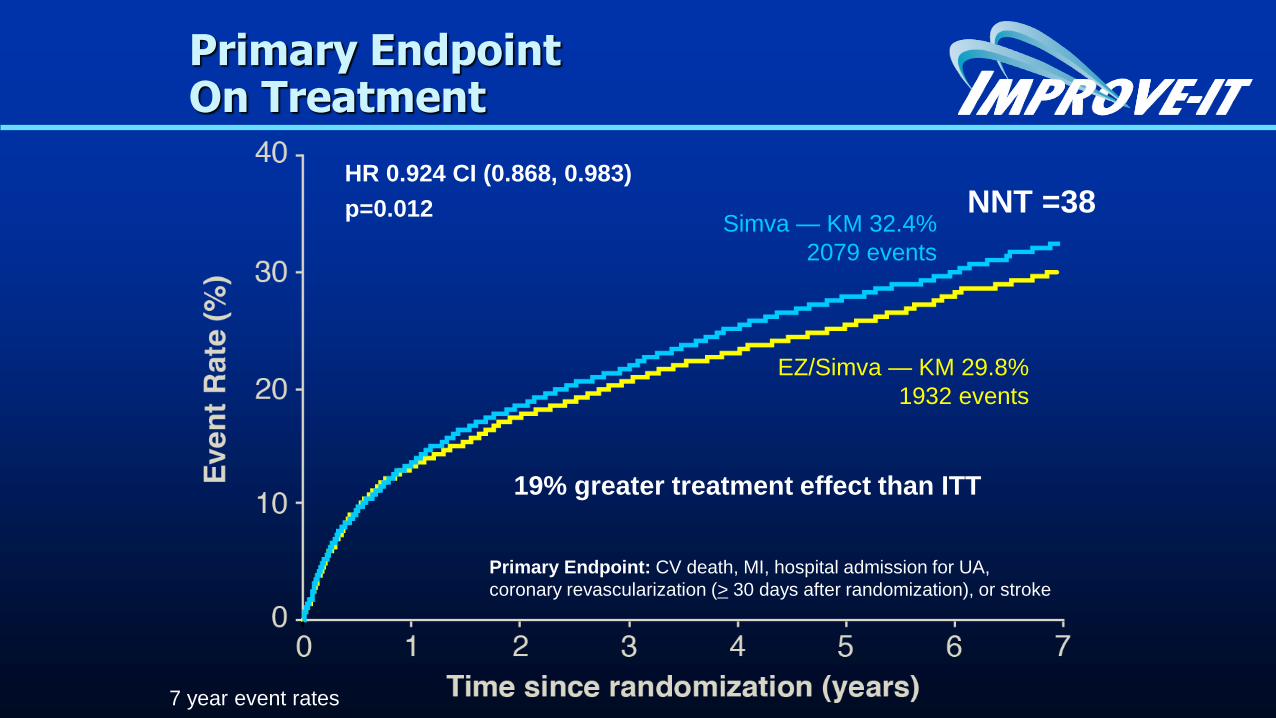
Primary Endpoint On Treatment
Simva — KM 32.4%
2079 events
EZ/Simva — KM 29.8%
1932 events
HR 0.924 CI (0.868, 0.983)
p=0.012
Primary Endpoint: CV death, MI, hospital admission for UA,
coronary revascularization (> 30 days after randomization), or stroke
19% greater treatment effect than ITT
NNT =38
7 year event rates
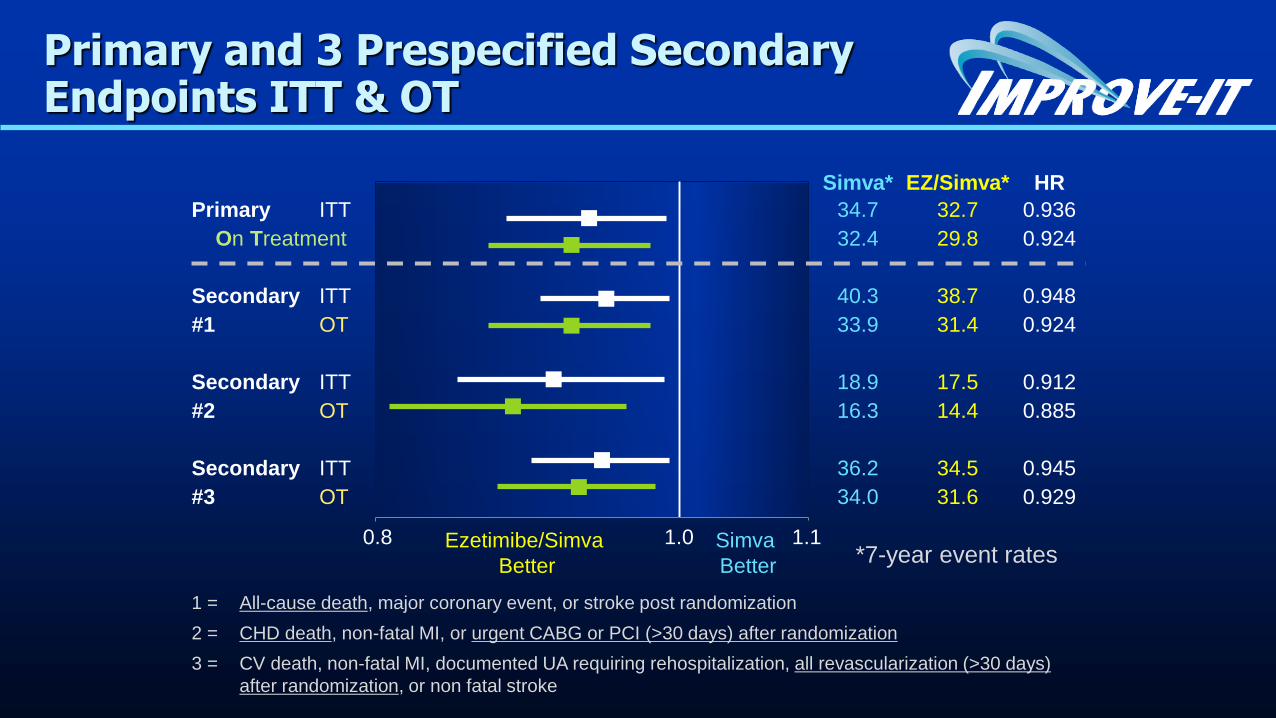
Simva* EZ/Simva* HR
Primary ITT 34.7 32.7 0.936
On Treatment 32.4 29.8 0.924
Secondary ITT 40.3 38.7 0.948
#1 OT 33.9 31.4 0.924
Secondary ITT 18.9 17.5 0.912
#2 OT 16.3 14.4 0.885
Secondary ITT 36.2 34.5 0.945
#3 OT 34.0 31.6 0.929
Ezetimibe/Simva
Better
Simva
Better
1 = All-cause death, major coronary event, or stroke post randomization
2 = CHD death, non-fatal MI, or urgent CABG or PCI (>30 days) after randomization
3 = CV death, non-fatal MI, documented UA requiring rehospitalization, all revascularization (>30 days)
after randomization, or non fatal stroke
*7-year event rates
Primary and 3 Prespecified Secondary Endpoints ITT & OT
0.8 1.0 1.1
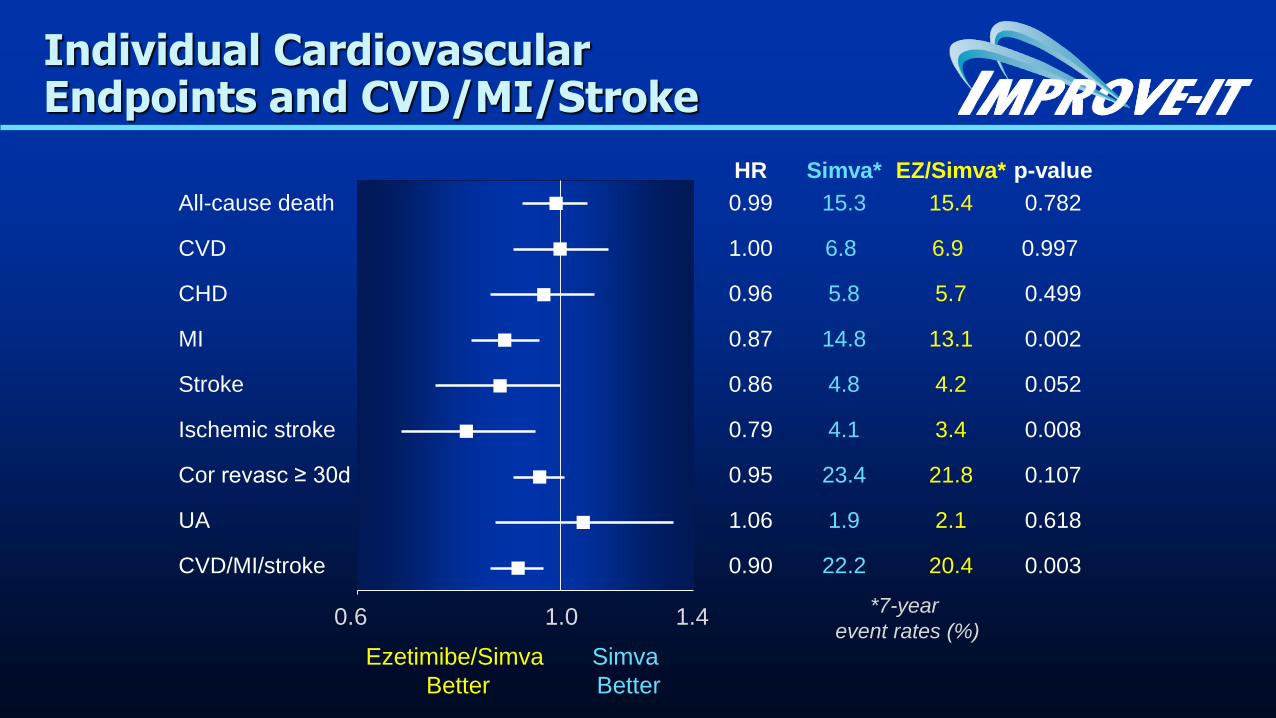
HR Simva* EZ/Simva* p-value
All-cause death 0.99 15.3 15.4 0.782
CVD 1.00 6.8 6.9 0.997
CHD 0.96 5.8 5.7 0.499
MI 0.87 14.8 13.1 0.002
Stroke 0.86 4.8 4.2 0.052
Ischemic stroke 0.79 4.1 3.4 0.008
Cor revasc ≥ 30d 0.95 23.4 21.8 0.107
UA 1.06 1.9 2.1 0.618
CVD/MI/stroke 0.90 22.2 20.4 0.003
Ezetimibe/Simva
Better
Simva
Better
Individual Cardiovascular Endpoints and CVD/MI/Stroke
0.6 1.0 1.4*7-year
event rates (%)
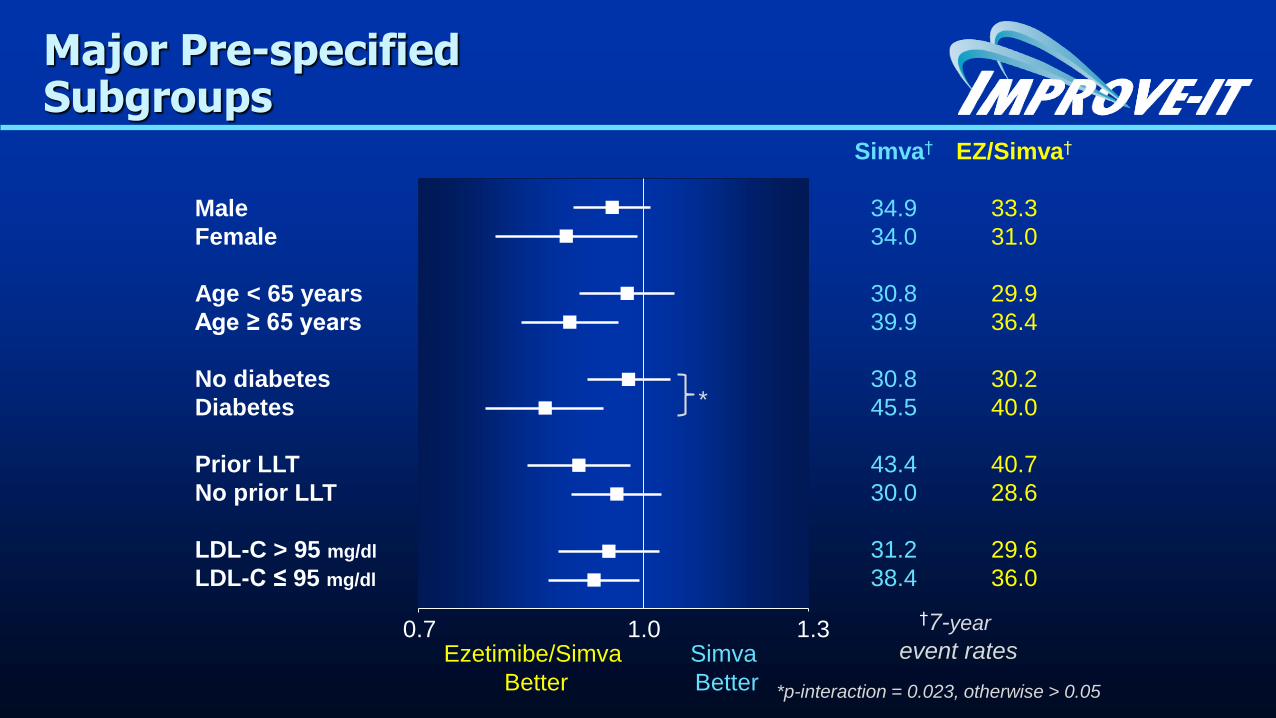
Simva† EZ/Simva†
Male 34.9 33.3
Female 34.0 31.0
Age < 65 years 30.8 29.9
Age ≥ 65 years 39.9 36.4
No diabetes 30.8 30.2
Diabetes 45.5 40.0
Prior LLT 43.4 40.7
No prior LLT 30.0 28.6
LDL-C > 95 mg/dl 31.2 29.6
LDL-C ≤ 95 mg/dl 38.4 36.0
Major Pre-specified Subgroups
Ezetimibe/Simva
Better
Simva
Better
0.7 1.0 1.3†7-year
event rates
*
*p-interaction = 0.023, otherwise > 0.05
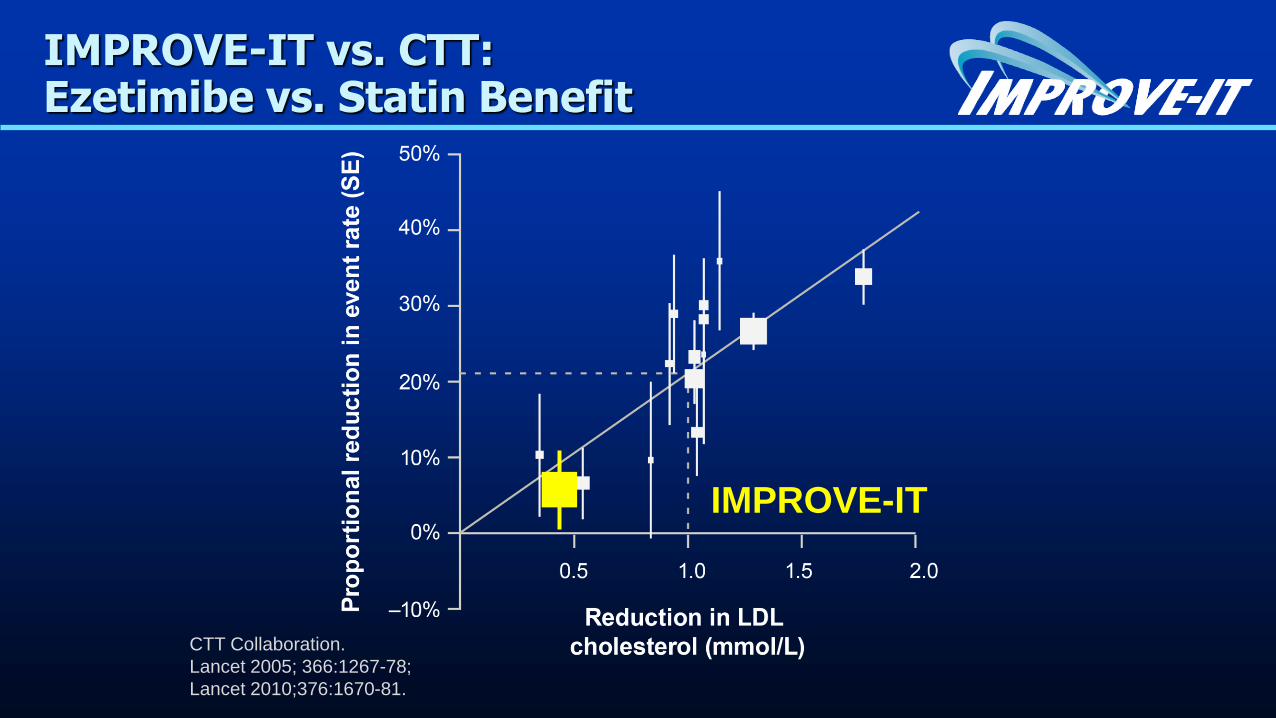
IMPROVE-IT vs. CTT: Ezetimibe vs. Statin Benefit
CTT Collaboration.
Lancet 2005; 366:1267-78;
Lancet 2010;376:1670-81.
IMPROVE-IT
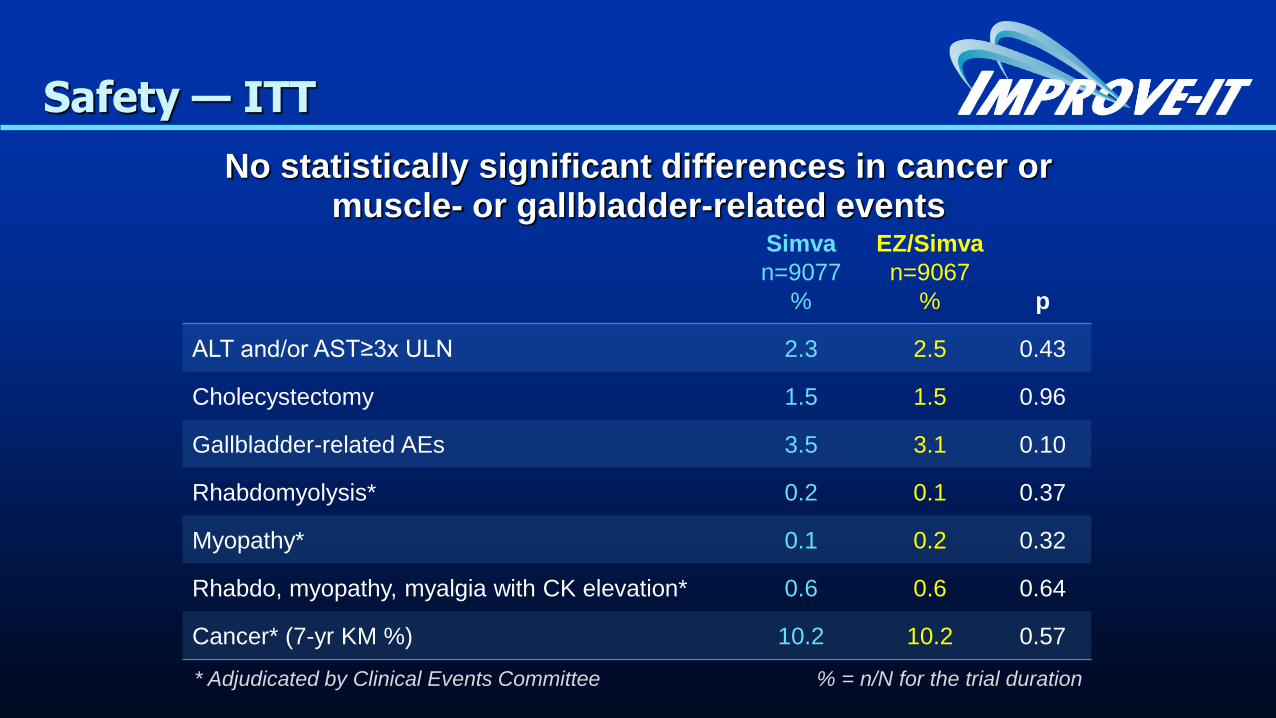
Safety — ITT
No statistically significant differences in cancer or muscle- or gallbladder-related events
Simva
n=9077
%
EZ/Simva
n=9067
% p
ALT and/or AST≥3x ULN 2.3 2.5 0.43
Cholecystectomy 1.5 1.5 0.96
Gallbladder-related AEs 3.5 3.1 0.10
Rhabdomyolysis* 0.2 0.1 0.37
Myopathy* 0.1 0.2 0.32
Rhabdo, myopathy, myalgia with CK elevation* 0.6 0.6 0.64
Cancer* (7-yr KM %) 10.2 10.2 0.57
* Adjudicated by Clinical Events Committee % = n/N for the trial duration
Conclusions
IMPROVE-IT: First trial demonstrating incremental
clinical benefit when adding a non-statin agent (ezetimibe) to statin therapy:
YES: Non-statin lowering LDL-C with ezetimibereduces cardiovascular events
YES: Even Lower is Even Better(achieved mean LDL-C 53 vs. 70 mg/dL at 1 year)
YES: Confirms ezetimibe safety profile
Reaffirms the LDL hypothesis, that reducing LDL-C prevents cardiovascular events
Results could be considered for future guidelines