the rise time of intracranial echo pulsations and intracranial pressure
TRANSCRIPT
A c t a Neurol. Scandinav. 'r8, 116 -123, 1972
Department o f Neurology, Queen's University, Kingston, Outario.
THE RISE TIME OF INTKACRANIAL ECHO I'UISA'I'IONS AND I NT R A CK AN I A 1, 1' R ES SUK E
ABSTI~.4(:1'
It would not appear that measurement o f Rise Times of' echo pulsa- tions either in amplitude or in range will be i iscsful in determining cases of raised intracranial pressure.
111 1964 J t~ppsson first suggcstcd t h a t a rclationstiip niiglit exist be- tween the shape of the pulse synchronous fluctuations in echo mipli- tudc recorded from intcrfaccs in the living h a i n and the ii i t racraiiial pressiire. He citctl Dnuson (1956) \\ ho, \\ i t h an hydraulic analogue, showed that the pressure within a closed but vcntcd \y\teni ( the cranium) through which fluid was flou ing in elastic t u k s at high pressure ( the arterial systerti) , ~vould lie largely detcrmincd liy thc pressure o f fluid flowing through the system in compliant tiibcs ( the venous system). Davsoii later, in discussing the causc o f the increased systolic pulsations recorded as the nicaii C.S.F. prcssurc \\:is increased, stated that these rcsiilted froin thc dislcnsion of thc vciiou\ system due to the cuff compression of the veins near the tlural sinuses by the raised intracranial pressure. He suggested t h a t these distended veins would lead to decreased damping of the systeiii and ascribed the incrcascd C.S.F. systolic pulsations to this causc.
.leppsson sulisec~uciilly clcvcloped this theine (1967) aiid pointcd out that the factors affecting a damped owillation can lie expressed as:
f . - A . c k t s i t i ' ) n f . l
where A-amplitude, f =frequency, k-damping factor and t =time. He pointed out that, from this equation it mas apparent that as k
dccrcascd 110th amplitude and rate of increase in amplitude would increase. He therefore designed and built equipment that measured the increase in echo :iniplitutle driring a givcn pcriod ' I ' cv i consecutive
116
measiirements were averaged to smooth out the effect of respiratory modulation. Such measurements of the magnitude of amplitude in- crease in a constant time, are a function of the rise time of the curve.
We, too, have been interested in the amplitude pulsations of intra- cranial echoes and record them with a device which has been fully described elsewhere (Clark et al. 1971). The echo pulsations both in amplitilde and range are written out by a polygraph and our measure- ments of rise times are made subsequently from the graphs. In this paper and in others that w e have published, Rise time is defined as that period during which the amplitude increase from 10 % to 90 % of its final value.
Our initial studies of Rise times and Delay times of echo amplitudes showed that there was a great scatter in the measurements made from a single normal individual (Campbell et al. 1970). We came to the conclusion (Clark e f al. 1971) that the amplitude of echoes recorded from within the skull was affected by such a large number of different and constantly varying attenuating factors, affecting both the insonating energy and the returning, echo, that it was unlikely that information about resions of the brain, much less about single interfaces, could be derived from their study.
We therefore chose to study the variations in range of individual echoes since such information would at least reflect the range changes of a single interface. Our measurements showed again, that as was the case with the Rise Times and Delay times of amplitude pulsations, the Rise times and Delay times of range pulsations had an equally wide scatter in a single healthy individual or a number of healthy subjects. Campbell e f al. (1970) made 475 measurements of Rise times in 25 normal subjects and found these varied between 33 and 183 msec. He further measured the rise time from 8 separate interfaces near the midline in the same subject in the period of an hour. The rise times, each averaged from 5 separate waves, varied from 83 to ll7msec. Moreover Jenkins et al. (1971) showed that there was no significant change in the Rise times of range changes in persons with known intracranial tumours as compared with normal persons. The reasons for this great scatter in the Rise times we measure has been described in some detail both by Jenkins et al. (1971) and CZark ef al. (1971).
The main reason appears to us to be the fact that the movement of any single cerebral interface will be the integrated movement of a number of neighbouring domains of brain. Each domain will move as a result of the passage through it of the arterial pulse. However this pulse will vary in shape, amplitude and velocity in the various
117
arteries at the centre of each domain. Thus any single cerebral inter- face will move in a pattern which is the integration of the different movements of surrounding domains. Thus no two cerebral interfaces are likely to show an integrated pattern of movement that is identical and the shape of the various wave forms of these movements will thus differ. Under these circumstances, a wide scatter in Rise times would be expected, as we found to be the case.
We hoped that, if we always recorded from the same cerebral inter- face, these variations in the pattern of the wave moiion recorded would be eliminated. Since the skull greatly scatters the ultrasonic energy, it is impossible, in our opinion, to identify any one echo with any single structure save in the case of the M-echo, the high amplitude of which distinguishes it from all other intracranial echoes received by a transducer in the bi-temporal axis (White 1970).
However the M-echo is formed as a complex from the echoes from a large number of interfaces (White et al. 1969 a,b) and, due to variations in the pattern of scattering of the energy with small move- ments of the skull relative to the beam (White et al. 19701, it is never possible to be sure one is recording the echo from the same interface on separate occasions. Thus we determined to make our observations at one sitting during which the transducer was rigidly fixed with respect to the skull (Clark e t al. 1971) so that all measurements were made from the same component, indeed the same cycle, of the M-echo complex.
The present work was designed to test the hypothesis that Rise times would lessen with increases in intracranial pressure.
MATERIAL, METHOD AND RESULTS
All our measurements were made from the same single cycle in the M-echo com- plex throughout the whole examination of a single subject. The subjects were patients whose neurological complaints necessitated examination of their C.S.F. by lumbar puncture.
After the sample of C.S.F. had been withdrawn with the patient recumbent, the pressure of the C.S.F. in the lumbar subarachnoid space was measured and, a t the same time the E.C.G. and the fluctuations in range of a single cycle of the M-echo complext were written out on the polygraph. Saline was infused into the subarachnoid space and raised the C.S.F. pressure in steps to a maximum of usually 600 mm H,O. At the same time recordings of the range changes of the same single cycle continued to be written out.
The examination was carried out on a total of eleven patients. We did not usually increase the C.S.F. pressure beyond 600 mm H,O because,
a t that pressure, leakage often occurred around the needle puncture through the meninges, thus rendering pressure measurements unreliable.
118
A./*
190
170
150
RISE 130 TIMES
IMSEC)
110
90
7 0
50
0 0
0
0 . !* . .
** .
*.
. 0.
.
.
0
: 0
. 0 .
. . . I I I I I I t I I 100 W 200 250 300 350 400 450 500 550 149 199 249 299 349 399 449 499 549 599
C.S.F PRESSURE lMM.H,O)
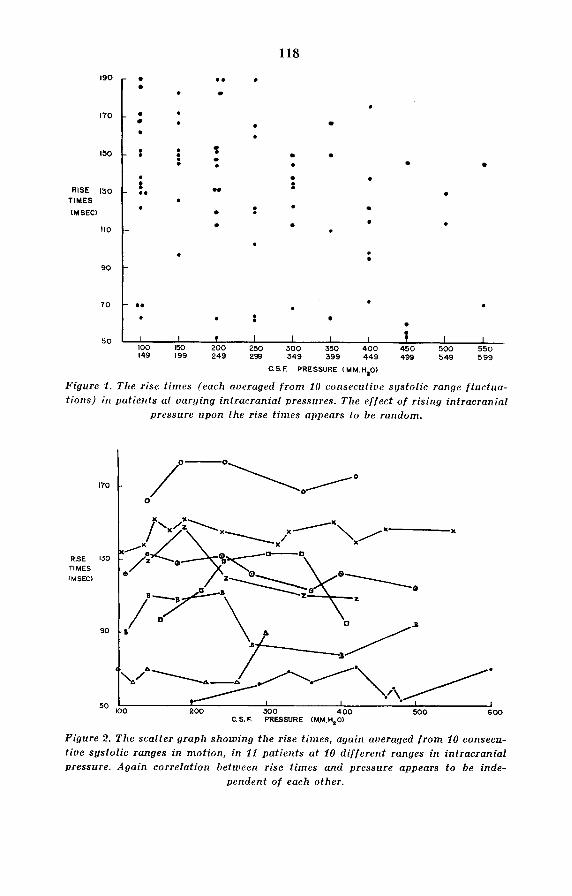
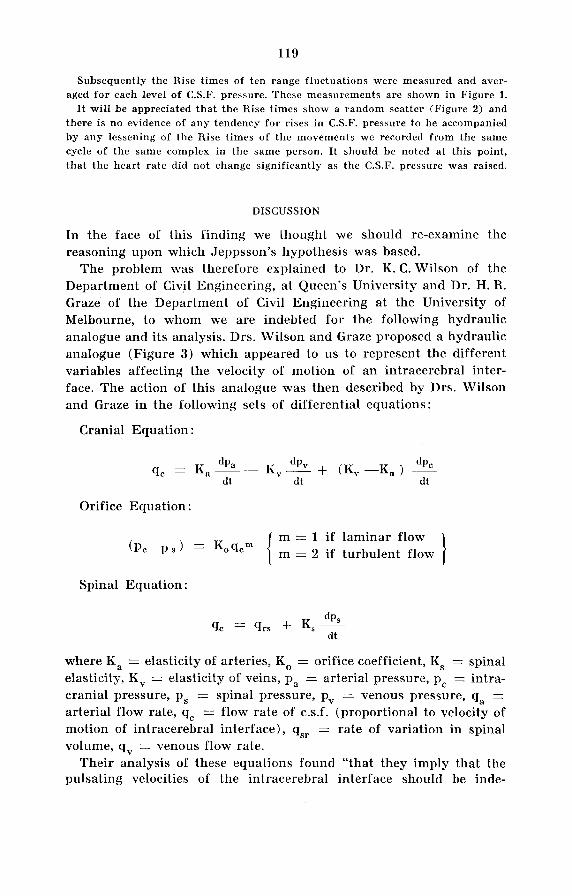
Figure 1. The rise times (each aueraged f r o m 10 consecutiue s!lstolic range f luctua- t ions) in patients at uarging intracranial pressures. The ef fect o f rising intracranial
pressure upon the rise t imes appears to be random.
170 I 0 /o-o\o/o
RISE I30 TIMES IMSEC)
90
Figure 2. The scatter graph showing the rise t imes, again averaged f r o m 10 consecu- tive systolic ranges in motion, in 11 patients at 10 di f ferent ranges in intracranial pressure. Again correlation between rise times and pressure appears to be inde-
pendent of each other.
119
Subsequently the Rise times of ten range fluctuations were measured and aver- aged for each level of C.S.F. pressure. These measurements are shown in Figure 1.
I t will be appreciated that the Rise times show a random scatter (Figure 2) and there is no evidence of any tendency for rises in C.S.F. pressure to be accompanied by any lessening of the Rise times of the movements wc recorded from the same cycle of the same complex in the same person. It should he noted at this point, that the heart rate did not change significantly as the C.S.F. pressure was raised.
DISCUSSION
In the face of this finding we thought we should re-examine the reasoning upon which Jeppsson’s hypothesis was based.
The problem was therefore explained to Dr. K. C. Wilson of the Department of Civil Engineering, at Queen’s University and Dr. H. R. Graze of the Department of Civil Engineering at the University of Melbourne, to whom we are indebted for the following hydraulic analogue and its analysis. Drs. Wilson and Graze proposed a hydraulic analogue (Figure 3) which appeared to us to represent the different variables affecting the velocity of motion of an intracerebral inter- face. The action of this analogue was then described by Drs. Wilson and Graze in the following sets of differential equations:
Cranial Equation :
Orifice Equation :
m = 1 i f laminar flow m = 2 if turbulent flow (Pc-ps) = Koqcm
Spinal Equation :
Qc = Qrs dPS + Ks- dt
where Ka = elasticity of arteries, KO = orifice coefficient, Ks = spinal elasticity, K v = elasticity of veins, pa = arterial pressure, pc = intra- cranial pressure, p, = spinal pressure, pv = venous pressure, q, = arterial flow rate, q, = flow rate of c.s.f. (proportional to velocity of motion of intracerebral interface), qsr = rate of variation in spinal volume, qv = venous flow rate.
Their analysis of these equations found “that they imply that the pulsating velocities of the intracerebral interface should be inde-
120
CRANIUM
KA I Q A - PA 1
Qv- I ) ) bC Pv
’i Kv
CEREBRAL INTERFACE pc
ac- ! PS
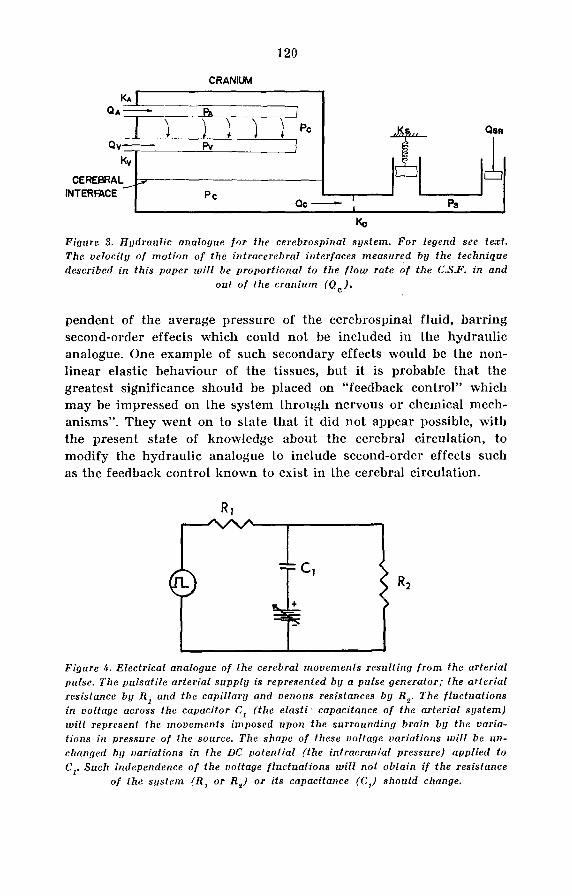
KO Figure 3. Hgdraulic analogue fo r the cerebrospinal sgstem. For legend see text. The velocitg of motion o f the intracerebral interfaces measured by the technique described in this paper will be proportional t o the f l o w rate o f the C.S.F. in and
out o f the cranium (Q,).
pendent of the average pressure of the cerebrospinal fluid, barring second-order effects which could not be included in the hydraulic analogue. One example of such secondary effects would be the non- linear elastic behaviour of the tissues, but it is probable that the greatest significance should be placed on “feedback control” which may be impressed on the system through nervous or chemical mech- anisms”. They went on to state that i t did not appear possible, with the present state of knowledge about the cerebral circulation, to modify the hydraulic analogue to include second-order effects such as the feedback control known to exist in the cerebral circulation.
Figure 4. Electrical analogue o f the cerebral movements resulting f r o m the arterial pulse. The pulsatile arterial s u p p l y is represented bg a pulse generator; the arterial resistance by R , and the capillary and venous resistances by R,. The fluctuations in voltage across the capacitor C, (the elasti ’ capacitance of the arterial sgstem) will represent the movements imposed upon the surrounding brain by the uaria- tions in pressure of the source. The shape of these voltage variations will be un- changed bfj variations in the DC potential ( the intracranial pressure) applied to C,. Such independence o f the voltage f luctuations will not obtain i f the resistance
of the system (R , or Re) or i ts capacitance (C,) should change.
121
If an electrical analogue (Figure 4) is used a similar conclusion will be reached. In Figure 4 i f the voltage changes across the plates of the condenser are representative of the pressure changes in the arterial tree, upon which the motion of the cerebral interfaces depends, then i t will be appreciated that variations in the D.C. potential across the plates will in no way affect the shape of the voltage fluctuations across the plates but merely raise or lower the voltage of these as a whole. This however will only hold good so long as variations in the D.C. potential (intracranial pressure) are not accompanied by varia- tions in the capacitance of the system (i. e. the elasticity of the cerebral circulation). Since we have good evidence that rises in intracranial pressure do cause a redistribution in the cerebral circulation (Green- field & Tindall (1965), and many others) with consequent changes in its elasticity it will be seen that the electrical analogue reaches the same conclusion as the hydraulic analogue.
We may therefore conclude that increases in intracranial pressure alone will not be expected to change the shape or the rise times or the range variations of intracranial interfaces. Decreased damping of these movements would not occur. However, the redistribution of the cere- bral circulation known to result from rises in intracranial pressure will result in changes in the elasticity of the system which will affect the pattern of the range changes of cerebral interfaces. These changes will be so complex that it is, in the present state of knowledge, impos- sible to state to what extent Rise times of these movements would be altered nor whether they would be lengthened or shortened.
This finding is a matter of greater significance than the demonstra- tion that measurements of the rise times of echo pulsations are un- likely to yield information about the intracranial pressure. The fact that intracranial pressure pulsations increase when intracranial pres- sure increases has been known for a long time and observed by many workers (Wrighf (19381, Bering (1955) and others). Our own observa- tions showed the same feature and increasing the intracranial pressure by infusing saline invariably was accompanied by an increased am- plitude in the range pulsations we recorded. It has been customary to ascribe these increased pulsations to decreased damping of the system as did Dauson (1956) . Since a change in damping would be accompanied by a change in the pressure wave that causes the move- ment we observe, the present study shows that this explanation cannot be correct either on theoretical or observational grounds. We believe that the increased range of pressure pulsations that result from in- creases in intracranial pressure, are due to re-distribution of the cerebral circulation as a result of the increased intracranial pressure
122
causing venous obstruction. The cerebral circulation is preserved by arteriolar vasodilation so that a greater volume of pulsatile blood enters the capillary bed whose inelastic walls are less able, than the elastic arterial walls, to prevent these pressure pulsations being trans- mitted to the intracranial contents as a whole (White e f al. in prepara- tion).
Finally we do not believe that it will be possible to use changes in the magnitude of the motion changes as a clinical index of the level of intracranial pressure. This is because the magnitude of the motion we record varies with each separate interface and, because of the scattering of the energy by the skull (White & Bahuleyan 1969), it is never possible either to identify the spatial origin of any echo nor to record from any single interface on separate occasions. It would only be possible to infer i f intracranial pressure was rising or falling i f the magnitude of motion was continuously recorded from a single interface over the prolonged period necessary. This is the technique we used in these observations but it is obviously quite impractical as a clinical tool.
In addition to Drs. K. C. Wilson and H. R. Graze, the authors wish to express their indebtedness to their colleagues Drs. H. B. Dinsdale, R. F. Hetherington and W. J. S. Marshall who allowed access to their patients for our measurements.
This work was supported by grants from the Medical Research Council of Canada.
REFERENCES
Bering, E. A. (1955) : Choroid plexus and arterial pulsation of cerebrospinal fluid. Arch. Neurol. Psychiat. 73, 165-172.
Campbell, J. K., J. M. Clark, D. N. White & C. 0. Jenkins (1970) : Pulsatile Echo- encephalography. Acta Neurol. Scand. Suppl. 45 46, 1-57.
Clark, J. M., D. N. White, Curry, G. R., R. J. Stevenson, J. K. Campbell & C. 0. Jenkins (1971) : The measurement of intracranial pulsations. Med. and Biol. Engng. 9, 263-287.
Davson, H. (1956) : Physiology of the ocular and cerebrospinal fluid. Churchill, London. Pp. 305-308, 349-350.
Jenkins, C. O., J. K. Campbell, D. N. White & J. M. Clark (1971) : Ultrasonic echo pulsations in range: a study of rise times and delay times. Acta Neurochir. 24, 1-10.
Jeppsson, S. (1964) : A method for recording the intracranial pressure with the aid of the echoencephalographic technique. Acta Chir. Scand. 128, 218-224.
Jeppsson, S. (1967) : A method for recording the intracranial pressure with the aid of the echoencephalographic technique. Procedings in Echo-Encephalo- graphy. Springer-Verlag, Berlin. pp. 186-189.
123
White, D. N., J. M. Clark, D. A. W. White, J. K. Campbell, li. Bahuleyan, A. S. Kraus & R.A.Brinker (1969): The deformation of the ultrasonic field in passage across the living and cadaver head. Mcd. Biol. Engng. 7, G07-618.
White, D. N., J. M. Clark, J. K. Campbell, J. N. Chesehrough, K. Bahuleyan & G. R. Curry (1969 a) : Experimental observations on the origin of the M-echo. Med. Biol. Engng. 7, 465-479.
White, D. N., J. M. Clark & J. K. Campbell (1969 b) : Inferential observations on the origin of the M-echo. Med. Biol. Engng. 7, 481-491.
White, D. N., K. Bahuleyan (1969) : Restrictions of the A-scan echoencephalographic technique in estimating lateral ventricular size. Med. Biol. Engng. 7, 619-626.
White, D. N. (1970) : Ultrasonic Encephalography. Schwabe Verlag, Basel and Medi- cal Ultrasonics Laboratory, Queen’s University.
White, D. N., C. 0. Jenkins & J. K. CampbelI. Steady and pulsatile intracranial pressures and moverncnts-a hydrodynamic study of the intracranial venting mechanisms and the aetological factors in hydrocephalus. In preparation.
Wright, R. D. (1938) : Experimental observations on increased intracranial pressure. Aust. N. Z. Jo. Surg. 7, 215-235.
Received June 21, 1971. C. 0. Jankins, M.D., Dept. of Neurology, Queen’s University Medical School, Kingston, Ontario, Canada.