the role of endotoxin during typhoid fever and tularemia in man
TRANSCRIPT

Journal of Clinical InvestigationVol. 43, No. 9, 1964
The Role of Endotoxin during Typhoid Fever and Tularemiain Man. III. Hyperreactivity to Endotoxin
during Infection *
SHELDON E. GREISMAN,t RICHARD B. HORNICK, AND THEODORE E. WOODWARD
(From the Departments of Medicine and Physiology, University of Maryland School ofMedicine, Baltimore, Md.)
The intravenous administration of endotoxinsprepared from gram-negative bacteria inducesprofound physiologic derangements in man (2).Nevertheless, their clinical significance during ill-nesses induced by gram-negative bacteria remainsspeculative. One major objection to ascribingany significant role to endotoxin in mediating thepathophysiologic changes during gram-negativebacterial infections is based on the phenomenonof acquired tolerance. Thus, when endotoxinsare administered daily to normal man as singleintravenous injections, resistance to their toxicand pyrogenic activities develops rapidly (3).Such acquisition of tolerance has led some in-vestigators to suggest that circulating endotoxincan play no major role in those infections in whichfever is sustained (4, 5). Others have proposedthat endotoxin can play an important role in sus-tained infection, e.g., typhoid fever, and thattolerance constitutes an important mechanism inrecovery from the illness (6). Support for eitherof these concepts is obtained from the observationthat a high degree of tolerance to the pyrogenicaction of Salmonella typhosa and other bacterialendotoxins is observed during convalescence fromtyphoid fever and tularemia (6, 7). Nevertheless,inferences as to the importance of bacterial endo-toxin during infection based upon observations of
* Submitted for publication March 9, 1964; acceptedMay 12, 1964.
Supported by the Commission on EpidemiologicalSurvey of the Armed Forces Epidemiological Board,contract DA-49-007-MD-751, and U. S. Public HealthService research grant HE-07280-03.A preliminary report of this work was presented at
the Seventy-fifth Annual Meeting of the Association ofAmerican Physicians, May 1962 (1).
t Recipient of Career Development Award from theNational Institutes of Health under contract HE-K3-15,237-C3.
endotoxin tolerance in normal or in convalescentman are not justified. Reactions to endotoxinmust be studied in the infected host during thefebrile phase of illness. The following studieswere performed in man to define a) the effect ofinduced endotoxin tolerance on the subsequent fe-brile and clinical course of two gram-negativebacterial infections, typhoid fever and tularemia,and b) the influence of the typhoid and tularemicinfections on the preinduced endotoxin tolerance.
Materials and Methods
Volunteers for these studies were male inmates of theMaryland House of Correction, Jessup, Md., whose agesranged from 22 to 44. Each volunteer was fully ap-prised of all aspects of the investigation and the at-tendant risk. They were free to cease participation atany time. Complete medical surveys were performed toverify the fitness of each participant.
Infectious agents and nature of clinical illness. Thepreparation and administration of the inocula of S. ty-phosa, Pasteurella tularensis, and sandfly fever virusand the clinical course and treatment of the resultingillnesses have been outlined previously (7). Convales-cence is defined as beginning on the first day that themaximal oral temperature (as recorded at 12 and 8 a.m.and at 12, 4, and 8 p.m.) remained below 1000 F.
Bacterial endotoxins. Two preparations of bacterialendotoxins were employed: a highly purified endotoxinfrom S. typhosa (0-282),' previously described (8), andPseudomonas endotoxin2 prepared by tryptic digestion(9). Both endotoxin preparations were suspended insterile, pyrogen-free physiologic saline and stored in rub-ber-stoppered vaccine bottles at 4° C. The S. typhosaendotoxin was diluted to a concentration of 0.25 gg perml and the Pseudomonas endotoxin to 10 .eg per ml.The diluted endotoxin preparations were bacteriologi-cally sterile, and the same bottle of diluted endotoxinwas always employed throughout any given study. Po-
' Kindly supplied by Dr. Maurice Landy, National In-stitutes of Health.
2 Kindly supplied as Piromen by Dr. T. A. Garrett,Baxter Laboratories, Morton Grove, Ill.
1747
S. E. GREISMAN, R. B. HORNICK, AND T. E. WOODWARD
tency of the diluted endotoxins was tested before thehuman studies by a standard pyrogen assay procedureemploying acclimatized, loosely restrained, albino rab-bits. Repeat assays conducted at the conclusion of thestudies, in groups of five rabbits each with two doselevels for each group, indicated no loss of pyrogenicity.Pyrogen assay in man. Volunteers were hospitalized,
and all responses to endotoxin were assayed after thesubjects were confined to bed and covered with a lightblanket. Syringes were either of the sterile, pyrogen-free, disposable type 3 or were heated overnight in a dry-
3 Burron Medical Products, Bethlehem, Pa.
air oven to 1800 C to eliminate extraneous pyrogens.Each test was begun between 8 and 9 a.m. Flexiblethermocouples were inserted into the rectum for fixeddistances (6 inches) and temperatures recorded by atelethermometer.4 Temperatures were monitored im-mediately before and every half-hour after the intrave-nous injection of endotoxin. The results were plottedon standard graph paper, and the area under the 7-hourfever curve, with the initial temperature as the base line,was calculated by summing the number of enclosed small
4 Yellow Springs Instruments Co., Yellow Springs,Ohio.
TYPHOID STUDY A
TF * 33 AGE 37
10 10 10 10e 10 10 10 10 PSEUDOMONAS ENDOTOXIN (us. I.V.) 10
I III1X 11W .4 jFEVERINDEX
1200-
1000-
8000
600
400-
200-
(1+1
1:40
S.TYPHOSA
(2+)
00)
(0)
(t)
DAY 14'131211 10 98 T
TFf 34 AGE 42
10 10 10 10
II (0) (0)(0)
1:40 1:40 1:1280 1:1280 (0)
*6 5-4 3 2 II-4112 3 4 5 *6 'I *8*9 10'11'12 13'14'15' '22'2
TYPHOID STUDY B
10 10 0 o lo lo PSEUDOMONAS ENDOTOXIN (ug i"v)I,
600-
400-
200-
(2
s
N
s
s
s
si Li
S. TY PHOSA
T-1~33+)
I+)
1(40
(1+)
(+±
0) (0) (dX 10) (0)
u a S I-.80
1160)RA1160L(3)1:160 1 160 1:320 61;641*
FIGuRE 1.
RECTALTEMP('F)
105
104
103
102
101
10099
98
97
FEVERINDEX
000-
800-1
10
RECTALTE M.P(OF)
105
-104
-103
-102
I0I
-100
_ 99
- 98
- 970
14(13 12 11 K 9 8 f76 5 '4 3 21 -- 2 3 4 5 6 ' 789'1011'12'13'14'15 '2223
I
s
l1748
ENDOTOXIN DURING TYPHOID FEVER AND TULAREMIA
TYPHOID STUDY CTF* 37 AGE 25
2.5 40 500 R5l0 (0 20 50 100100 200 200 l000 500 500 500 ENDOTOXIN (mg. LV.) 2.5
FEVER + + + + .i + i + i *' -INDEX (4+)
((+)
(0)s( j(,)(2+)(,))
~;Aft)
1±)
(0)
(2+) S.TYPHOSAri
(0)
(4+)
AWh
REGTALTEMP('F)
105
-104
-103-102
-101
-100
99
- 98Ad ii !i 6is] is i6iH11:12801-2560 IH IPOI 111280
16 1514 13 12 11 10 9 8 7 6 5 4 3 2 1-+ 1 2 3 4 5 6 7 8 9 10 11 12
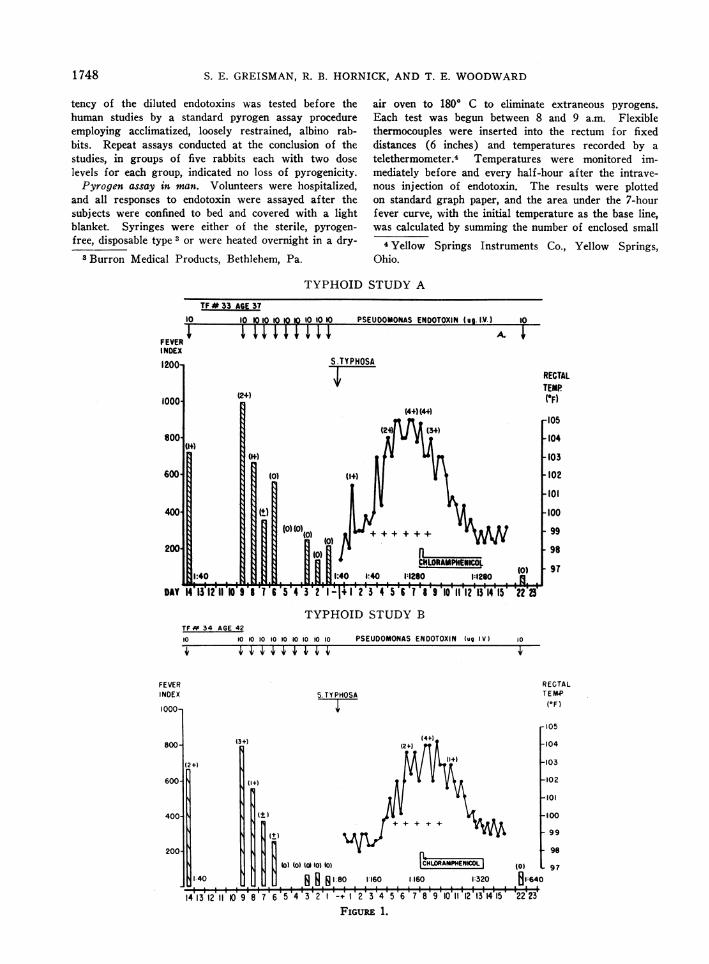
FIG. 1. TYPHOID FEVER IN ENDOTOXIN-TOLERANT SUBJECTS. A, B. INABILITY OF
PYROGENIC TOLERANCE INDUCED BY DAILY INTRAVENOUS INJECTIONS OF 10 ,AG Pseudo-monas ENDOTOXIN TO MITIGATE TYPHOID FEVER. Note that tolerance is seen upon re-
testing on day 11 of afebrile convalescence. Figures in parentheses represent theintensity of subjective reactions (see text). S. typhosa 0 agglutinin titers are givenabove bottom line. + = blood culture positive for S. typhosa. C. INABILITY OFPYROGENIC TOLERANCE INDUCED BY DAILY INTRAVENOUS INJECTIONS OF INCREASING
QUANTITIES OF Pseudomonas ENDOTOXIN TO INHIBIT TYPHOID FEVER. This subjectwas shown to possess cross-tolerance to 2.5 lug of S. typhosa endotoxin on days 8and 2 before challenge with viable S. typhosa (shaded bars). Note that toleranceto the S. typhosa endotoxin is demonstrable on day 4 of afebrile convalescence.
squares. This value, termed the fever index, representsa measure of the height and duration of the febrile re-sponses (10). The ordinates were plotted so that 100small squares represented a fever index of 100 and re-flected a 10 F rise in rectal temperature for a 1-hourduration. The diurnal variation of normal body tem-perature was so great that temperatures seldom returnedto preinjection values. In such instances, the fevercurves were extrapolated to the base line. In additionto the fever index, subjective reactions (headache, chills,myalgia, anorexia) after endotoxin administration-weregraded as follows: 1 + = mild, 2 + = moderate, 3 + =severe, and 4 + = extremely severe.
ResultsEffect of endotoxin tolerance on induced typhoid
fever. Before oral challenge with viable S. ty-phosa, two subjects were rendered tolerant bydaily intravenous injections of 10 ug Pseudo-monas endotoxin (Figure 1A and B). A third
volunteer was rendered tolerant by daily intra-venous injections of progressively increasing quan-tities of the Pseudomonas endotoxin (Figure 1C).Pseudomonas, rather than S. typhosa endotoxin,was employed in these initial studies to circumventthe possible induction of specific immunity to theviable S. typhosa. In one subject, a high degreeof cross-tolerance was created to S. typhosa en-dotoxin as evidenced by the minimal responses toslow infusions of 2.5 pg S. typhosa endotoxinadministered on days 8 and 2 before challengewith viable S. typhosa organisms (Figure 1C).Five normal control subjects infused with one-tenth this quantity of the same S. typhosa endo-toxin preparation exhibited marked febrile andsubjective reactions (mean fever index, 1,880;SE ± 230; mean subjective reaction, 3 +). De-spite this tolerance to Pseudomonas and to S.
ss
s
s
s
NIs
s
s
N
s
N
1749
II
i.
S. E. GREISMAN, R. B. HORNICK, AND T. E. WOODWARD
TYPHOID STUDY A
1071
1061
06,
104
2.-103
9102
*- 101-J.4
99.
97
TFW55 A£6144
HYDROGORTISONE IV. AND PO.
I L
0 1 2 3 4 5 6 7TIME (HOURS)
TYPHOID STUDY B
TF # 54 AGE 40
TIME (HOURS)
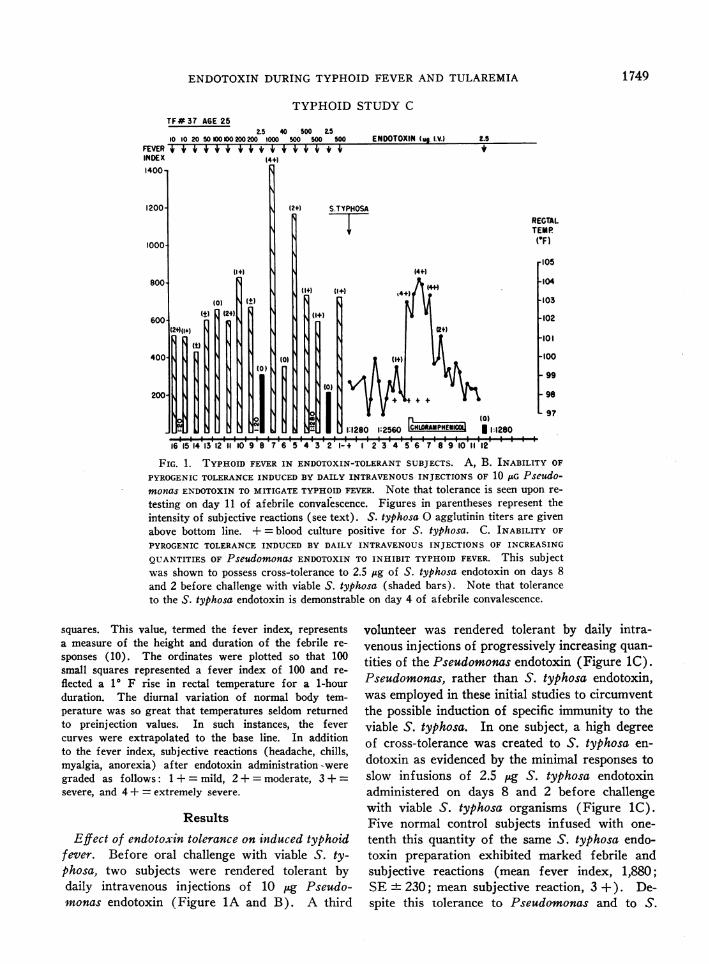
FIG. 2. A, B. ENDOTOXIN REACTIVITY DURING TYPHOID FEVER. Thesubjects were initially rendered tolerant by daily intravenous in-jections of increasing quantities of S. typhosa endotoxin. The toler-ant reaction to 2.5 /Ag S. typhosa endotoxin on day 21 is depicted bythe lower curves. The subsequent hyperreactivity during typhoidillness and decline of such reactivity during convalescence are shown.
1750
IL.a-
Ir
M
IU~1.41I--0LU
ENDOTOXIN DURING TYPHOID FEVER AND TULAREMIA 15
tfA&yphosa endotoxin, the subsequent clinical courseof illness after challenge with viable S. typhosa,including the pyrexia, toxemia, and bacteremia,was not mitigated, nor was the incubation periodprolonged when compared with a nontolerant con-trol group infected at the same time. Toleranceto the Pseudomonas and the S. typhosa. endotoxinswas again evident upon retesting after the thirdday of convalescence (Figure lA to C).
Effect of typhoid fever on preinduced endotoxintolerance. The observations that unmitigated ty-phoid illness develops in man despite preinducedtolerance to bacterial endotoxins sufficient to pro-tect against febrile and toxic manifestations assevere as those seen during typhoid fever sug-gested initially that circulating endotoxin couldplay no major role in pathogenesis. Nevertheless,it remained to be demonstrated that the toleranceto endotoxin, although existing before and afterillness, was maintained during illness. Two vol-unteers were given daily intravenous injectionsof S. typhosa. endotoxin in increasing quantitiesover a 3-week period. The lowest curve in Fig-ure 2A illustrates the subsequent ability of thefirst subject to tolerate the intravenous administra-tion of 2.5 Mg S. typhosa endotoxin. The febrileresponse after this large dose of endotoxin wasminimal, and no subjective discomfort was evi-dent. Viable S. typhosa was now administeredorally. Despite the elevated S. typhosa 0 agglu-tinin titer, overt typhoid illness developed as inthe nontolerant control group. On the first dlayof illness, when the rectal temperature was 102.90F, 0.5 Mug S. typhoscs endotoxin was given intra-venously. The subsequent febrile and subjectiveresponses were so severe (upper curve, Figure2A) that 100 mg hydrocortisone was administeredintravenously and 100 mg orally to control thereactions. The subject was subsequently treatedwith chloramphenicol; after becoming afebrile forseveral days, relapse ensued when medication wasdiscontinued. On the third day of relapse, at atime when the rectal temperature was 99.7' F, 0.5j~g of S. typhosa endotoxin was again adminis-tered intravenously; the resulting febrile and sub-jective reactions were again intense (second fromtop curve, Figure 2A). After a second courseof antibiotic therapy, and after remaining afebrilefor 6 days, 0.5 iig of S. typhosa endotoxin given
intravenously now induced only a mild febrile re-sponse and a minimal subjective reaction (secondfrom bottom curve, Figure 2A). A similar reac-tion pattern to S. typhosa endotoxin was observedin the second volunteer (Figure 2B). This lattersubject, although tolerant to 2.5 ug of S. typhosaendotoxin given intravenously before typhoid ill-ness and possessing a high S. typhosa 0 agglu-tinin titer, developed unmitigated typhoid illnessafter oral administration of viable S. typhosa.Hyperreactivity occurred to 0.5 M~gof the endo-toxin given intravenously on the first day of ill-ness, as well as early in convalescence (36 hoursafter becoming afebrile), but a tolerant reactionwas again evident later in convalescence.To define more precisely the time at which hy-
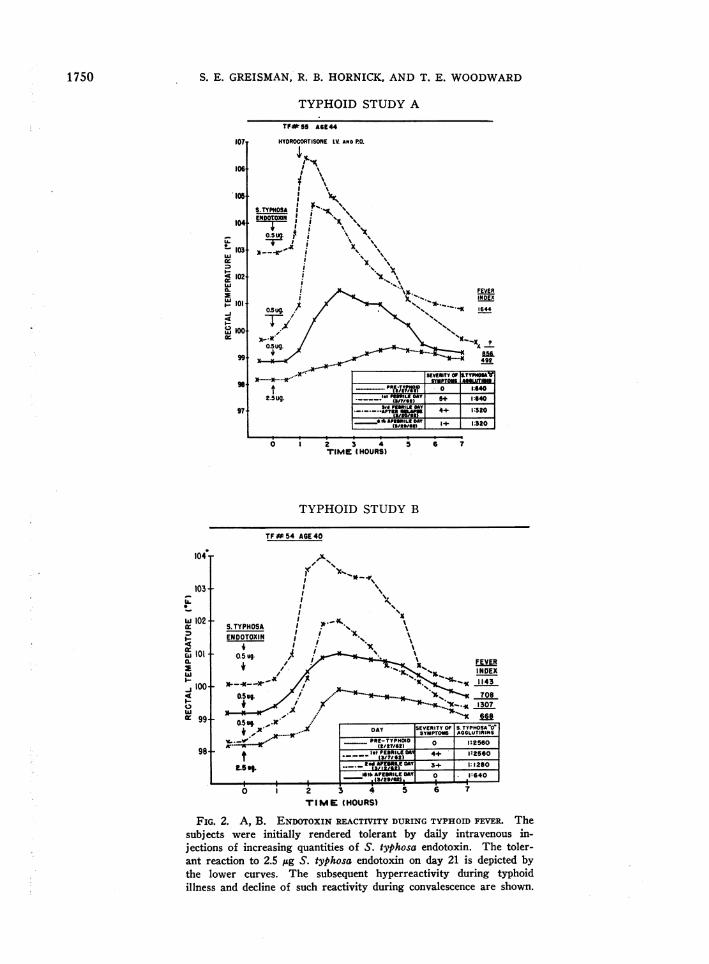
perreactivity to endotoxin appears and subsidesduring typhoid fever, and to determine the speci-ficity of such hyperreactivity, four additional sub-jects were rendered tolerant to Pseudomonasendotoxin by daily intravenous injections of 25
acx401.-Cl
LLA
v) 1250-xwQa40
12 1000-wC"CL-
6Zi- 750-W11cu
zLI
La S.-
'ut 500-11.-I
11
a,>Cuj jI= -4w- 250- tCc Zw:.I..L.!A
0-
S. TYPHOSA-F-
1_ INCUBATION_1
(T.F.90O
OVERT ILLNESS -I AFEBRILE CONVALESCENT
(4+1
I(01(C
II PERIOD
(3+1
I (X)= SUBJECTIVEREACTION
(0)
V- IT -i I I1I1 I11III1111
0 123456789 10 15 22 ~24 27 301DAY
FIG. 3. ENDOTOXIN REACTIVITY DURING TYPHOID FE-
VER. Typical reaction pattern depicting the stepwise de-velopment of hyperreactivity to 25 ug Pseudomonas en-dotoxin in a tolerant subject during the incubation phaseof typhoid fever and the stepwise decline of hyperreac-tivity during convalescence. Tolerance was induced be-fore challenge with viable S. typhosa by daily intrave-nous injections of Pseudomonas endotoxin increasingfrom, 25 to 250 M~gover a 30-day period. The initialcontrol reaction to 25 M~gof the endotoxin is shown bythe unshaded bar on the left.
1751
S. E. GREISMAN, R. B. HORNICK, AND T. E. WOODWARD
RECTALTEMP T
IF.#44
TF.#42
T F.*43
T.F40AO
PFtJntI)mbeIAC FnIInnTnAVIM III106 'r_VuvmuN# rWuluVV| rfw I.V.106i-4 I
102-100 2/24/L6271798i 2/14/63
IM (4+)104ji102/ (2+)
100 5/1634/23/63
98106io4 ~~~~~(4+)104i-102/1
s5/6/63 (0)- 4/23/63 _
98106-104T (3+)102_
100I 5/2/63 (0)
98 t 4/23/63106-
TF 104:#41 102-
100-
(4+)
5/22/63 ( 1+)4/23/63
(HOURS)
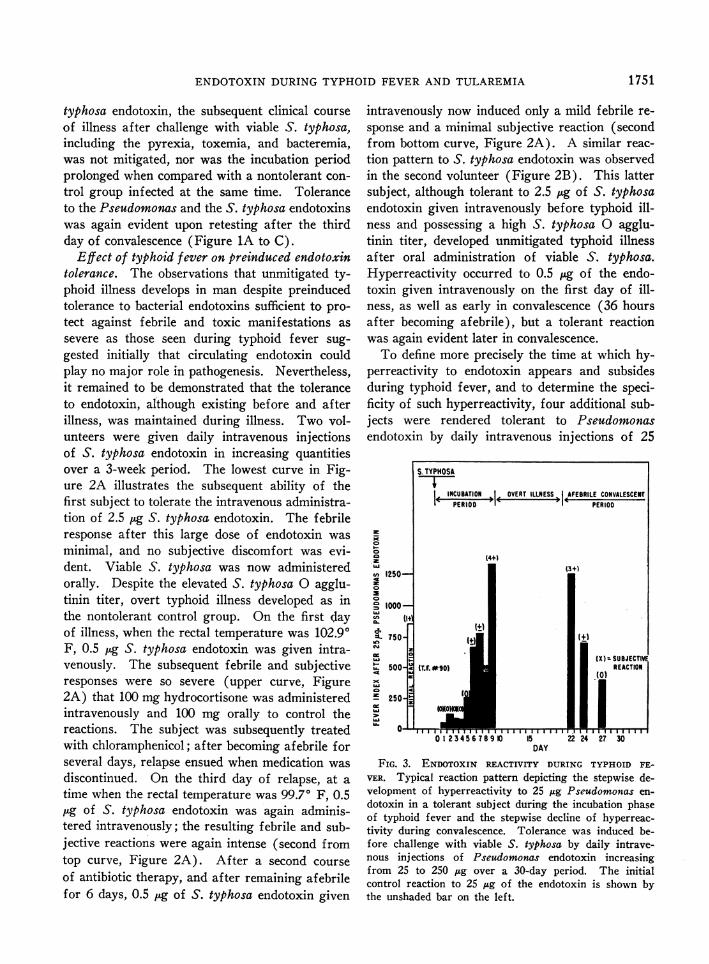
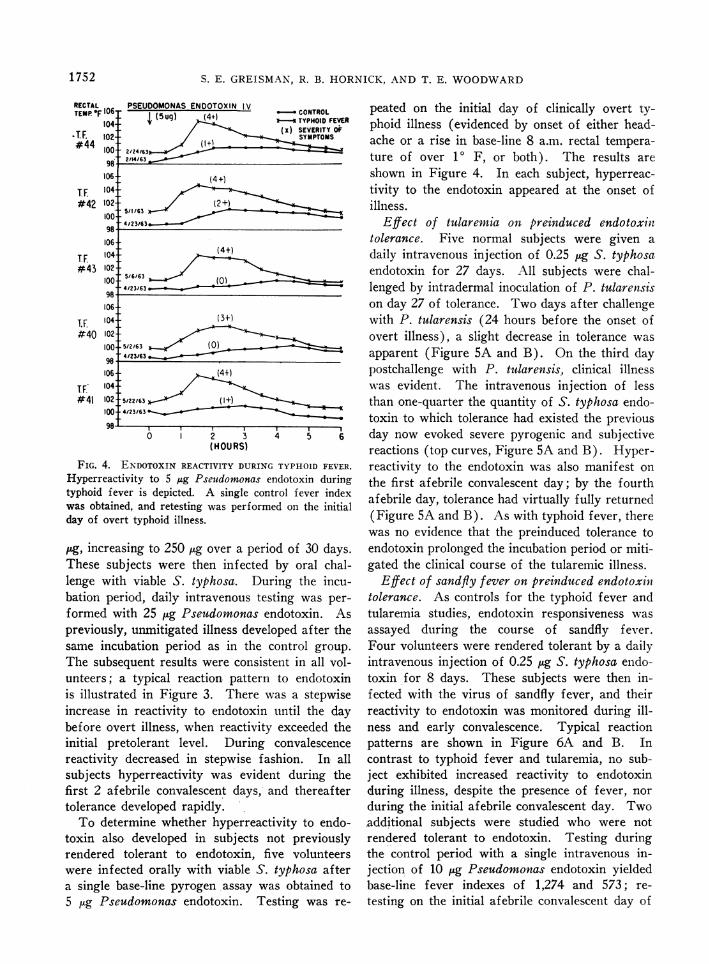
FIG. 4. ENDOTOXIN REACTIVITY DURINC
Hyperreactivity to 5 ,ug Pseudomonas e
typhoid fever is depicted. A single con
was obtained, and retesting was performday of overt typhoid illness.
Mg, increasing to 250 Mg over a peril
These subjects were then infectedlenge with viable S. typhosa. Duibation period, daily intravenous tesformed with 25 ug Pseudomonas ei
previously, unmitigated illness develsame incubation period as in the (
The subsequent results were consistunteers; a typical reaction patternis illustrated in Figure 3. There Mincrease in reactivity to endotoxinbefore overt illness, when reactivityinitial pretolerant level. Duringreactivity decreased in stepwise fasubjects hyperreactivity was evideifirst 2 afebrile convalescent days,tolerance developed rapidly.To determine whether hyperreact
toxin also developed in subjects r
rendered tolerant to endotoxin, fiwere infected orally with viable S.a single base-line pyrogen assay wz
5 ug Pseudomonas endotoxin. Te
CONTROL peated on the initial day of clinically overt ty-(Tx}SEVVERIT phoid illness (evidenced by onset of either head-
SYMPTOMS ache or a rise in base-line 8 a.m. rectal tempera-ture of over 10 F, or both). The results areshown in Figure 4. In each subject, hyperreac-tivity to the endotoxin appeared at the onset ofillness.
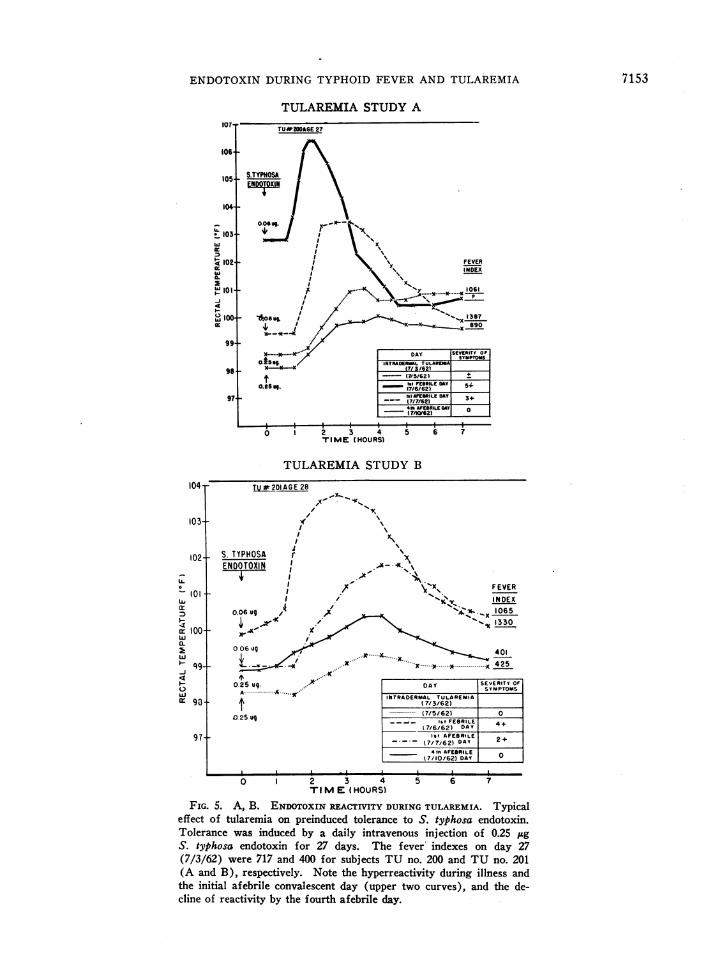
Effect of tularermia on preinduced endotoxilltolerance. Five normal subjects were given adaily intravenous injection of 0.25 jug S. typhosaendotoxin for 27 days. All subjects were chal-lenged by intradermal inoculation of P. tularenisison day 27 of tolerance. Two days after challengewith P. tularensis (24 hours before the onset ofovert illness), a slight decrease in tolerance wasapparent (Figure 5A and B). On the third daypostchallenge with P. tularensis, clinical illnesswas evident. The intravenous injection of lessthan one-quarter the quantity of S. typhosa endo-toxin to which tolerance had existed the previous
4 5 6 day now evoked severe pyrogenic and subjectivereactions (top curves, Figure 5A and B). Hyper-
J TYPHOID FEVER. reactivity to the endotoxin was also manifest onndotoxin during the first afebrile convalescent day; by the fourthtrol fever index afebrile day, tolerance had virtually fully returneded on the initial
(Figure 5A and B). As with typhoid fever, therewas no evidence that the preinduced tolerance to
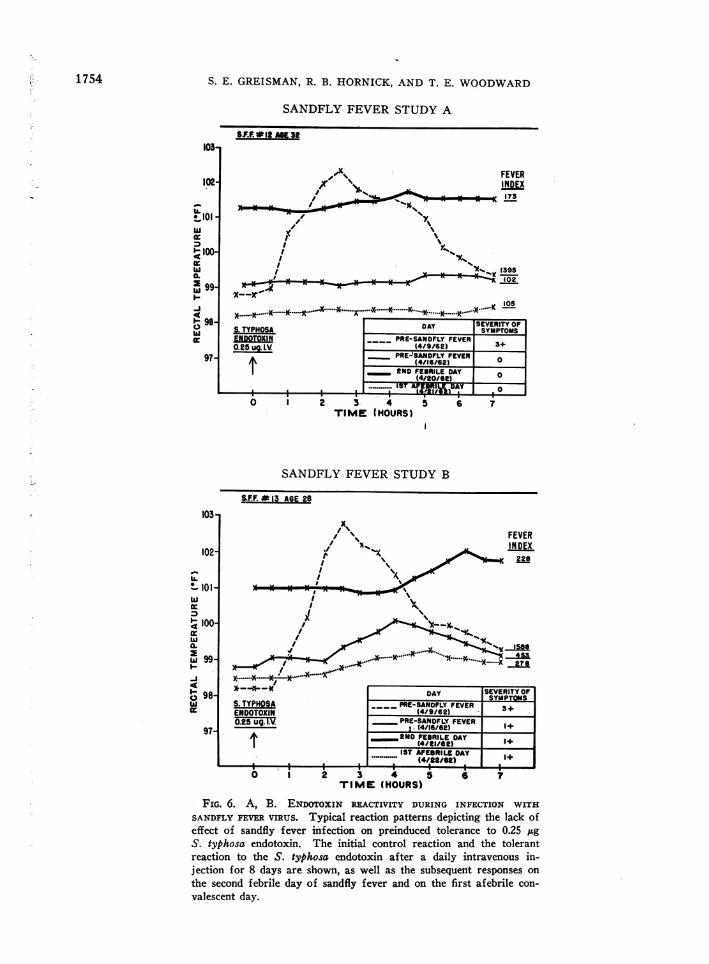
od of 30 days. endotoxin prolonged the incubation period or miti-by oral chal- gated the clinical course of the tularemic illness.ring the incu- Effect of sandfly fever on preinduced endotoxin;ting was per- tolerance. As controls for the typhoid fever andndotoxin. As tularemia studies, endotoxin responsiveness wasLoped after the assayed during the course of sandfly fever.control group. Four volunteers were rendered tolerant by a dailyLent in all vol- intravenous injection of 0.25 jug S. typhosa endo-to endotoxin toxin for 8 days. These subjects were then in-
vas a stepwise fected with the virus of sandfly fever, and theiruntil the day reactivity to endotoxin was monitored during ill-exceeded the ness and early convalescence. Typical reactionconvalescence patterns are shown in Figure 6A and B. Inshion. In all contrast to typhoid fever and tularemia, no sub-nt during the ject exhibited increased reactivity to endotoxinand thereafter during illness, despite the presence of fever, nor
during the initial afebrile convalescent day. Two:ivity to endo- additional subjects were studied who were notiot previously rendered tolerant to endotoxin. Testing duringyve volunteers the control period with a single intravenous in-typhosa after jection of 10 jg Pseudomonas endotoxin yieldedas obtained to base-line fever indexes of 1,274 and 573; re-:sting was re- testing on the initial afebrile convalescent day of
1752
,t
ENDOTOXIN DURING TYPHOID FEVER AND TULAREMIA
TULAREMIA STUDY A
106-
105+
104+
* 103
< 102
a-
4
w lo0Jx
TU*2006AE 27
S.TYPHOSA
99-
984
97
0 I~~~~~~~~~~~~~~~~~~~~~~~~O 1 2 4HTlIME t(HOURS)
TULAREMIA STUDY B
S.El
TUj201AGE 28
I ~~~~~~\TYPHOSA
11 l's''.NDOTOXIN
I
/, \'Xs FEVERI / '%'s INDEX
0.06 ug O/
_X 1065;
>< .o- "t ~~~~~~~~~1330006ug40
......X 425
0.2 5 ug9. X DAY SEVERITY OFA
SYMPTOMS
INTRADERMAL TULAREMIA
025 ug
0 2 3 4TIME (HOURS)
5 6 7
FIG. 5. A, B. ENDOTOXIN REACTIVITY DURING TULAREMIA. Typicaleffect of tularemia on preinduced tolerance to S. typhosa endotoxin.Tolerance was induced by a daily intravenous injection of 0.25 ,ugS. typhosa endotoxin for 27 days. The fever indexes on day 27(7/3/62) were 717 and 400 for subjects TU no. 200 and TU no. 201(A and B), respectively. Note the hyperreactivity during illness andthe initial afebrile convalescent day (upper two curves), and the de-cline of reactivity by the fourth afebrile day.
7153
104 r-
103+
102+
LL
!- 101
100,a.i-
w
09w
0
1--
97-
*....... (7/5/62 0____-4- Ist FEBRILE 4+
7/6/62) DAYIst AFEBReLE
(7/7/62) DAY 2+41h AFEBROLE
1 7/10/62) DAY I__
T
S. E. GREISMAN, R. B. HORNICK, AND T. E. WOODWARD
SANDFLY FEVER STUDY A
S.F.PP12 AKe3
FEVER
s~~~~~~~~~~~~~~~~~~~IIDEX173
I'I a
> 1395-_---~ 102
.Y...............K......
2 3 4TIM.E (HOURS)
SANDFLY FEVER STUDY B
SF.F.*13 AGE 28
S. TYPHOSAENDOTOXINOP25 ug. IV.
t(4/A226IL) UAY(4/22/62)
* aIA.- I0 I I a
1 2 3 4 5TIME (HOURS)
I6 7
FIG. 6. A, B. ENDoTOXIN REACTIVITY DURING INFECTION WITH
SANDFLY FEVER VIRUS. Typical reaction patterns depicting the lack ofeffect of sandfly fever infection on preinduced tolerance to 0.25 IxgS. typhosa endotoxin. The initial control reaction and the tolerantreaction to the S. typhosa endotoxin after a daily intravenous in-jection for 8 days are shown, as well as the subsequent responses on
the second febrile day of sandfly fever and on the first afebrile con-valescent day.
1754
-I
I-IC),
103*
102-
IL.I-, lot
* 100-
0.10
XU 99--Jo4
98-
97
SEVERITY OFISYMPTOMSDAY___ PRE-SANDFLY FEVER 3+
(4/9/62) ______
PRE-SANDFLY FEVER.* (4/16/62) 1+
in NtD) FEBRILE DAYl(4/21/62 1+
Isr *Prasoo a n^v
ENDOTOXIN DURING TYPHOID FEVER AND TULAREMIA
sandfly fever 1 week later yielded fever indexesof 1,013 and 460, respectively. Such tolerance isconsistent with that expected after a single intra-venous test dose of the endotoxin 1 week previ-ously (7).
Discussion
Hyperreactivity to bacterial endotoxins, em-ploying lethality as a criterion, occurs during avariety of infectious illnesses induced in laboratoryanimals (11, 12). In evaluating possible mecha-nisms for such hyperreactivity, the parameter forjudging hyperreactivity to endotoxin during in-fection must be carefully considered. Thus, al-though induced tolerance to bacterial endotoxinsis accompanied by resistance to most of its toxicactivities (13), the converse cannot be assumed,i.e., that hyperreactivity to endotoxin, measuredby lethality, indicates that its other toxic activitiesare enhanced. Indeed, it has been demonstratedthat the enhanced susceptibility to the lethal ac-tivity of endotoxin seen in laboratory animalsduring infection with Mycobacterium tuberculosisis not accompanied by enhanced pyrogenic re-sponses (14, 15). These findings indicate thatgeneralized changes in metabolic activity of thehost during active infection need not per se aug-ment pyrogenic responsiveness; such observationsare important in the analysis of augmented pyro-genic responses to endotoxin during infection inman.
Detailed data describing alterations in respon-siveness to the pyrogenic activity of endotoxinduring induced infection in laboratory animalswith agents other than Myobacteria are not avail-able. In man, increased reactivity to the pyrogenicactivity of Brucella endotoxin has been establishedduring active brucellosis (16). Specific hyper-sensitivity induced by the infection was suggestedas the mechanism underlying such hyperreactivityto the Brucella endotoxin. Our present studiesdemonstrate that augmented pyrogenic responsesto bacterial endotoxin also occur in man duringtwo other infectious diseases, typhoid fever andtularemia. We emphasize that a real augmentationof pyrogenic responsiveness to endotoxin occursduring illness in that the increments in body tem-perature were consistently greater in both rate andmagnitude, and usually duration, i.e., fever indexeswere higher than those seen during the control
period. This is in sharp distinction to observationsby Bannister in man (17) and by Atwood andKass in rabbits (18), wherein the injection ofendotoxin during fever induced by exposure to ahot environment led to increments in body tem-perature (rate, magnitude, and duration) nogreater than those seen under normal environ-mental conditions. Although body temperaturesafter endotoxin were higher in the hot environ-ment, the initial temperatures were correspond-ingly elevated; these reactions represent additiverather than hyperreactive pyrogenic responses toendotoxin.The unique opportunity to study the present
volunteers before infection permitted observationsbearing on the mechanism and significance oftheir hyperreactivity to endotoxin during infec-tion: a) Since the role of acquired hypersensitivityin the production of hyperreactivity to endotoxinremains unproven, it is significant that augmentedpyrogenic responses, occurred to Pseudomonasendotoxin during typhoid fever and to S. typhosaendotoxin during tularemia. Certainly, therefore,the hyperreactivity cannot be attributed to hyper-sensitivity restricted to the specific endotoxin pos-sessed by the infectious agents. Whether thehyperreactivity is more intense to endotoxins pre-pared from the homologous infecting organismsremains to be quantitated.
b) Augmented pyrogenic responsiveness to en-dotoxin appeared during the later portion of theincubation phase of typhoid illness and persistedduring early convalescence, occurring before andafter overt clinical illness. It cannot be attributed,therefore, simply to a summation of toxic effectsin the overtly ill host. Moreover, since the en-hanced pyrogenic responses occurred in the ab-sence of elevations of rectal temperature, resettingof the thermoregulatory mechanisms appears un-likely as an explanation. The unaltered pyrogenicresponses to endotoxin in control subjects in-fected with the virus of sandfly fever provideadditional evidence to exclude nonspecific effectsof infection or fever per se. The absence of aug-mented pyrogenic reactivity to endotoxin duringfever induced by a hot environment, as mentionedpreviously (17, 18), is also consistent with thisthesis.
c) Augmented pyrogenic responses occurredregardless of whether a high degree of tolerance
1755
S. E. GREISMAN, R. B. HORNICK, AND T. E. WOODWARD
to the endotoxin was induced before infection byrepeated daily intravenous injections or whetheronly a single control intravenous base-line testwas performed. It is not yet certain, however,whether the hyperreactivity involves the inhibitionof those mechanisms that participate in toleranceor whether the tolerance mechanisms remain func-tional and offer some partial protection, i.e.,whether a significant difference in the degree ofhyperreactivity to endotoxin exists between thosesubjects with and without preinduced tolerance.
d) The hyperreactivity to bacterial endotoxinduring typhoid fever and tularemia, in contrast tobrucellosis (16), wanes rapidly once convales-cence begins. This temporal course of the subsi-dence of the hyperreactivity to endotoxin recon-ciles an apparent conflict in earlier reports. Hey-man and Beeson (19) observed hyperreactivityto the pyrogenic action of endotoxin during con-valescence from typhoid fever and tularemia,whereas Neva and Morgan (6) and subsequentlyour own group reported tolerance (7). It isimportant that the former investigators tested fortolerance on the second to third afebrile convales-cent days, whereas the latter investigators testedafter the third afebrile day. It is during thisearly convalescent period that the transition fromhyper- to hyporeactivity is in progress.
e) Endotoxin tolerance has been suggested toplay an important role in recovery from gram-negative bacterial infections such as typhoid fe-ver (6). This thesis appears untenable, since 1)induction of endotoxin tolerance sufficient to pro-tect against febrile and toxic manifestations assevere as those seen during overt infection failedto prolong the incubation phase or mitigate sub-sequent typhoid or tularemic illness, 2) tolerancedid not develop during overt illness, 3) recoveryfrom typhoid fever, after initiation of chloram-phenicol therapy, commenced while hyperreactivityto endotoxin was still apparent, and 4) recoveryfrom typhoid fever, before the advent of chloram-phenicol therapy, has been reported while hyper-reactivity to endotoxin was still evident (19).
f) It has been suggested that since tolerance to
endotoxin develops readily in normal subjects, cir-culating endotoxin can play no major role in thoseinfections in which fever is sustained (4, 5).This argument against implicating endotoxin, at
least with regard to the- pathogenesis of typhoidfever and tularemia, is no longer tenable. On thecontrary, the present findings show that the hostremains capable of hyperreacting to minute quan-tities of endotoxin that may be released from theinfecting microbes. Such findings, in conjunctionwith prior evidence for the release of physiologi-cally active quantities of endotoxin during typhoidfever (7, 20), suggest an important role for cir-culating endotoxin in the pathogenesis of thisillness.
Studies in man are currently in progress to de-fine the mechanisms responsible for the augmentedpyrogenic reactions to bacterial endotoxins duringtyphoid fever and tularemia.
Summary
The present studies evaluate the importance ofbacterial endotoxin in the pathogenesis of typhoidfever and tularemia in man. Induction of endo-toxin tolerance sufficient to protect against febrileand subjective toxic manifestations as severe asthose seen during overt infection failed to pro-long the incubation period or mitigate the sub-sequent clinical course of induced typhoid fever ortularemia. Although such findings appeared tomilitate against the importance of endotoxin inthe pathogenesis of these illnesses, testing duringovert infection revealed profound alterations inreactivity to endotoxin characterized by markedlyaugmented pyrogenic and subjective responses.This hyperreactivity to endotoxin occurred re-gardless of whether a high degree of tolerancewas induced before infection by repeated dailyintravenous injections of endotoxin or whetheronly a single injection was given intravenously toestablish a base-line response. The hyperreac-tivity was not restricted to the endotoxin preparedfrom the infectious agent; increased reactivity wasseen to Pseudomonas endotoxin during typhoidfever and to S. typhosa endotoxin during tulare-mia. Temporal studies after ingestion of vi-able S. typhosa indicated a stepwise onset of hy-perreactivity to Pseudomonas endotoxin during theincubation period, with hyperreactivity consistentlypresent 24 hours before overt illness, and stepwisesubsidence of reactivity during convalescence, withtolerance after the third afebrile day. Controlstudies in febrile subjects infected with the virus
1756

ENDOTOXIN DURING TYPHOID FEVER AND TULAREMIA
of sandfly fever revealed no alteration in prein-duced tolerance to S. typhosa endotoxin.The present studies refute the concept that en-
dotoxin tolerance plays an important role in re-
covery from typhoid fever or that the ability ofnormal man to develop tolerance to endotoxin pre-
cludes the importance of circulating endotoxin inthe pathogenesis of sustained infectious illnesses.The mechanisms for the hyperreactivity to the py-
rogenic activity of endotoxin during typhoid fe-ver and tularemia in man are unknown and are
currently under study.
Acknowledgments
The authors express their deepest appreciation to thevolunteers who contributed so faithfully to these studies;to Mr. Paul Sharpley, who assisted in the care of thesepatients; to Mr. James W. Curran, Commissioner of theMaryland Department of Correction; to Mr. William F.Steiner, Chief Warden of the Maryland House of Cor-rection; and to the other officials of the Maryland Houseof Correction for their generous cooperation and in-terest, without which these studies could not have beenaccomplished.
References1. Greisman, S. E., R. B. Hornick, F. A. Carozza, Jr.,
and T. E. Woodward. Effect of endotoxin tol-erance on human typhoid fever. Trans. Ass.Amer. Phycns 1962, 75, 170.
2. Favorite, G. O., and H. R. Morgan. Effects pro-
duced by the intravenous injection in man of a
toxic antigenic material derived from Eberthellatyphosa: clinical, hematological, chemical, andserological studies. J. clin. Invest. 1942, 21, 589.
3. Morgan, H. R. Resistance to the action of the en-
dotoxins of enteric bacilli in man. J. dlin. Invest.1948, 27, 706.
4. Beeson, P. B. Discussion of W. W. Spink, Thesignificance of endotoxin in brucellosis: experi-mental and clinical studies. Trans. Ass. Amer.Phycns 1954, 67, 292.
5. Atkins, E. Pathogenesis of fever. Physiol. Rev.1960, 40, 580.
6. Neva, F. A., and H. R. Morgan. Tolerance to theaction of endotoxins of enteric bacilli in patientsconvalescent from typhoid and paratyphoid fe-vers. J. Lab. dlin. Med. 1950, 35, 911.
7. Greisman, S. E., R. B. Hornick, F. A. Carozza, Jr.,and T. E. Woodward. The role of endotoxinduring typhoid fever and tularemia in man. I.Acquisition of tolerance to endotoxin. J. dlin.Invest. 1963, 42, 1064.
8. Webster, M. E., J. F. Sagin, M. Landy, and A. G.Johnson. Studies on the 0 antigen of Salmonellatyphosa. I. Purification of the antigen. J. Im-munol. 1955, 74, 455.
9. Nesset, N. M., J. McLallen, P. Z. Anthony, and L. G.Ginger. Bacterial pyrogens. I. Pyrogenic prepa-ration from a Pseudomonas species. J. Amer.pharm. Ass., sci. Ed. 1950, 39, 456.
10. Beeson, P. B. Tolerance to bacterial pyrogens. I.Factors influencing its development. J. exp. Med.1947, 86, 29.
11. Abernathy, R. S., G. M. Bradley, and W. W. Spink.Increased susceptibility of mice with brucellosisto bacterial endotoxins. J. Immunol. 1958, 81, 271.
12. Suter, E., and E. M. Kirsanow. Hyperreactivity toendotoxin in mice infected with Mycobacteria.Induction and elicitation of the reactions. Im-munology 1961, 4, 354.
13. Thomas, L. The physiological disturbances pro-duced by endotoxins. Ann. Rev. Physiol. 1954,16, 467.
14. Hall, C. H., Jr., and E. Atkins. Studies on tuber-culin fever. I. The mechanism of fever in tuber-culin hypersensitivity. J. exp. Med. 1959, 109,339.
15. Suter, E. Hyperreactivity to endotoxin after infec-tion with BCG. Studies on its distinguishingproperties. J. Immunol. 1964, 92, 49.
16. Abernathy, R. S., and W. W. Spink. Studies withBrucella endotoxin in humans: the significance ofsusceptibility to endotoxin in the pathogenesis ofbrucellosis. J. dlin. Invest. 1958, 37, 219.
17. Bannister, R. G. Anhidrosis following intravenousbacterial pyrogen. Lancet 1960, 2, 118.
18. Atwood, R. P., and E. H. Kass. Relationship ofbody temperature to the lethal action of bacterialendotoxin. J. dlin. Invest. 1964, 43, 151.
19. Heyman, A., and P. B. Beeson. Influence of vari-ous disease states upon the febrile response tointravenous injection of typhoid bacterial pyro-gen. J. Lab. clin. Med. 1949, 34, 1400.
20. Greisman, S. E., R. B. Hornick, F. A. Carozza, Jr.,and T. E. Woodward. The role of endotoxin dur-ing typhoid fever and tularemia in man. II. Al-tered cardiovascular responses to catecholamines.J. dlin. Invest. 1964, 43, 986.
1757