the role of the allied health professional in cp and health (icf) a global model to guide clinical...
TRANSCRIPT

THE ROLE OF
PHYSIOTHERAPY IN
THE DISABLED CHILD
Red Cross War Memorial
Children’s Hospital
Physiotherapy
Samantha van Deventer
Janine Victor

INTRODUCTIONThe Disabled Child
• WHO and The International Classification of Functioning,
Disability and Health (ICF)
Health Condition(disorder or disease)
Participation
Restriction
Activity
Limitation
Body Function &
Structure
Environmental
Factors
Contextual Factors
Personal
Factors

THE DISABLED CHILD
• Moderate to severe physical disability
• Spectrum of motor impairments
• Congenital or acquired
• Including but not limited to:
Cerebral Palsy
Traumatic Brain Injury
Spina Bifida
Spinal Cord Injury
Neuromuscular Disease
• The Global burden of Disease: ≈ 9.5 million children 0 -14 yrs with
disability of which 1.3 million are classified as severely disabled

ROLE OF PHYSIOTHERAPY
• Physiotherapists focus on gross motor skills and
functional mobility, including positioning, transitional
movements, use and issue of assistive devices
• Postural management programme
• Positioning
• Education, training and support
• Multi-disciplinary team involvement
• Physiotherapist’s role in palliation
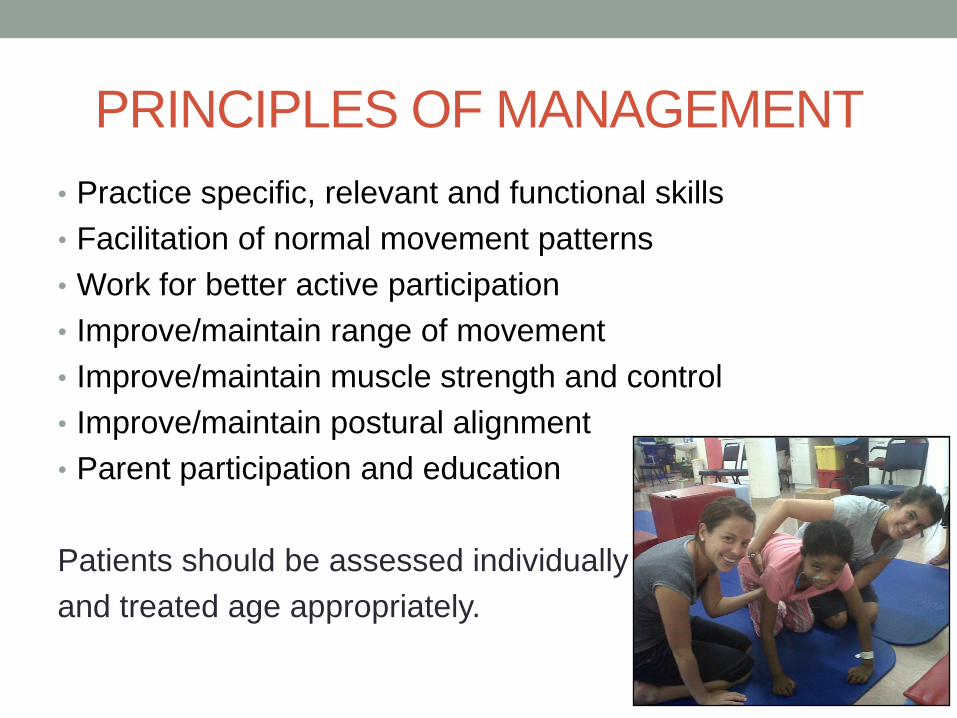
PRINCIPLES OF MANAGEMENT
• Practice specific, relevant and functional skills
• Facilitation of normal movement patterns
• Work for better active participation
• Improve/maintain range of movement
• Improve/maintain muscle strength and control
• Improve/maintain postural alignment
• Parent participation and education
Patients should be assessed individually
and treated age appropriately.

APPROPRIATE MANAGEMENT
• Importance of early referral and intervention
• Anticipate progression/effects of condition
Initial / Evolving stage Plateau Stage Palliative Stage

POSTURAL MANAGEMENT
PROGRAMME• 24 hours
• Variation in environment, activity and intervention
• Positively impacting on posture and function
• Enhanced communication and participation
• Transitioning through stages of life
Positioner
Wedge
Standing frame
Wheelchair (seating system)

POSTURAL MANAGEMENT
PROGRAMMEo Immature skeletal and neuromuscular system
oBiomechanical alignment
oConsiderations should be given to:
Assistive device for play, feeding,
relaxing and independence
Stretching positions
Sleeping positions
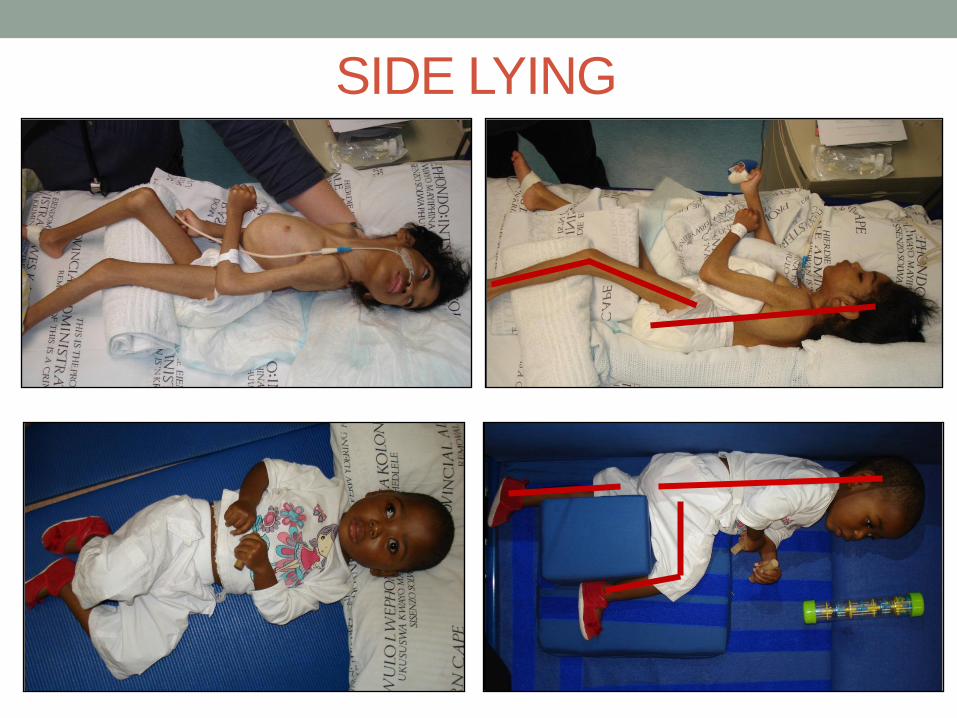
SIDE LYING

WEDGE
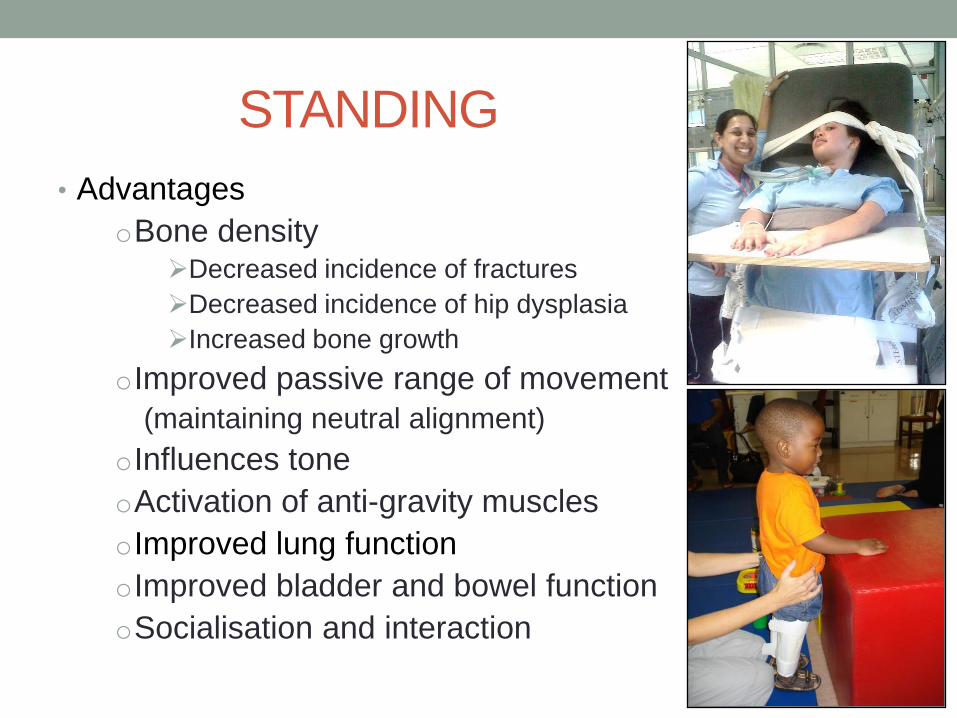
STANDING
• Advantages
oBone densityDecreased incidence of fractures
Decreased incidence of hip dysplasia
Increased bone growth
oImproved passive range of movement
(maintaining neutral alignment)
oInfluences tone
oActivation of anti-gravity muscles
oImproved lung function
oImproved bladder and bowel function
oSocialisation and interaction

STANDING

THE WHEELCHAIR

THE WHEELCHAIR
• Extensive Research
• Major role under Physio- and Occupational Therapy
• Human Rights Framework – Ability rather than DISablility
• Full assessment of child considering:
Diagnosis
Age
Functional abilities
Postural deviations
Deformities
Environment
Function

THE WHEELCHAIR

THE WHEELCHAIR
Pressure Mapping
BEFORE AFTER

BUGGY

POSTURE CHAIR

WHEELCHAIR
Hybrid Dual Terrain Chair

WHEELCHAIR
Active Urban chair

MOTORISED WHEELCHAIR
Motorised Chair

EDUCATION AND TRAINING
• Caregiver’s acceptance and understanding of child’s
disability
• Child’s capabilities in optimum position
• Focus on abilities rather than disabilities
• Caregiver main role-player:
Therapy manager
Caregiver included in decisions re: therapy,
frequency and intensity
Goal setting
Therapy incorporated into daily routine

MULTIDISCIPLINARY COLLABORATION
• Ideally collaboration between role players across
disciplines to meet common goals
• Therapy and management of one role player directly
influences that of another

PHYSIOTHERAPY AND PALLIATIVE
CARE
Symptom control: • Suctioning
• Supportive chest physio
• Importance of movement
• Pain relief
Support for the patient & family• Positions of rest/comfort
• Back care
• Independence
• Distraction
• Enhanced QOL

THANK YOU

REFERENCES
• Armstrong, W., Borg, J., Krizack, M., Lindsley, A., Mines, K., Pearlman, J., Reisinger, K. &
Sheldon, S. (2008). Guidelines on the provision of Manual Wheelchairs in less resourced
settings. Publications of the World Health Organization. Geneva.
• Bax, M., Goldstein, M., Rosenbaum, P., Leviton, A. & Paneth. N. (2005). Proposed definition
and classification of cerebral palsy. Developmental Medicine and Child Neurology. 47: 571-
576.
• Big Shoes., Hospice Palliative Care Association of South Africa. (2012). Management of
Common Symptoms and Problems in Paediatric Palliative Care. Clinical Guidelines.
• Google Images
• Gough, M. (2009). Continuous postural management and the prevention of deformity in
children with cerebral palsy. Developmental Medicine & Child Neurology. 51: 105-110.
• Gunel, M.K. (2011) Physiotherapy for Children with Cerebral Palsy, Epilepsy in Children –
Clinical and Social Aspects, Dr. Zeljka Petelin Gadze (Ed.)
• http://www.who.int/mediacentre/factsheets/fs352/en/index.html
• http://www.who.int/topics/disabilities/en/
• Laakso, L. (2006). The role of physiotherapy in palliative care. Australian Family Physician.
35(10): 781.

REFERENCES• Michaud, L.J. et al (2004). Prescribing Therapy Services for Children with Motor Disabilities.
American Academy of Pediatrics. 113 (6) 1836 – 1838.
• Pin, T.W. (2007). Effectiveness of Static Weight-Bearing Exercises in Children with Cerebral Palsy. Pediatric Physical Therapy. 19: 62-73.
• Pineda, V. S. (2008). It’s About Ability. An explanation of the Convention of the Rights of Persons with Disabilities. United National Children’s Fund (UNICEF)
• Quin, S., Clarke, J. & Murphy-Lawless, J.(2005). Report on a Research Study of the Palliative Care Needs of Children in Ireland. Department of Health and Children, The Irish Hospice Foundation and the Faculty of Paediatrics.
• Rosenbaum, P. (2009). Cerebral Palsy in the 21st Century: Is There Anything Left to Say? Neuropediatrics. 40: 56-60.
• Saloojee, G.M., Rosenbaum, P.R. & Stewart, A.V. (2011). Using caregivers’ perception of rehabilitation services for children with Cerebral Palsy at public sector hospitals to identify the components of an appropriate service. South African Journal of Physiotherapy. 67(3).
• Scheffler, E. (2010). Basic wheelchair and seating training. Provincial Government of the Western Cape, Department of Health.
• Scheffler, E. (2012). Intermediate wheelchair and seating training. Disability and Rehabilitation Consultancy Services.
• Stewart, D. & Rosenbaum, P. (2003). The International Classification of Functioning, Disability, and Health (ICF) A Global Model to Guide Clinical thinking and Practice in Childhood Disability. CanChild Centre for Childhood Disability Research.