the role of the left atrial appendage in maintaining atrial...
TRANSCRIPT

The role of the left atrial appendage
in maintaining atrial fibrillation
Disclosure
SentreHeart Incbull Consultant
bull Equity holder
Lone Star Heart Inc
Restore Maintain Protect
Role of LAA Ligation in Patients with Persistent or Longstanding Persistent AF
Electrical Isolation
Atrial debulking
LAA Exclusion
Catheter Ablation of
Long-Standing Persistent Atrial Fibrillation5-Year Outcomes of the Hamburg Sequential Ablation Strategy
Roland Richard Tilz MD Andreas Rillig MD Anna-Maria Thum Anita Arya MD Peter
Wohlmuth Andreas Metzner MD Shibu Mathew MD Yasuhiro Yoshiga MD Erik
Wissner MD Karl-Heinz Kuck MD Feifan Ouyang MD
JACC 2012601921ndash9
After the first ablation procedure sinus rhythm was
documented in 41 of 202 (203) patients
After multiple procedures sinus rhythm was maintained in 91
of 202 (450) patients
Role of LAA in AF
Automaticity cells
identified in the LAA
that leads to AT
LAA Triggers Reentrant
Circuits
Thrombus
Formation
Heterogeneous fiber
orientation and the
presence of
trabeculated muscle
influence wave
propagation and favor
the formation of
conduction
blockslow
conduction and
initiation of reentry
Guo et al Heart Rhythm 1117ndash25 2014
Fibrillating Areas Isolated within the Left Atrium after
Radiofrequency Linear Catheter Ablation
RostockhellipHaissaguerre JCE 17807-812 2006
Group I ndashStd BOX
Procedure (n=43)
Group II ndash Std BOX
Proc w LAA focal
ablation (n=56)
Group III ndash Std BOX
Proc w LAA electrical
Isolation (n=167)
P value
(Groups
1 vs 2 vs
3)
AF TypeRecurrence
by type
Total
Recurrences
Recurrence
by type
Total
Recurrences
Recurrence
by Type
Total
Recurrences
Follow Up
Months11+3 11+3 12+3 0910
PAF 3 (9)
32 (74)
3 (8)
38 (68)
1 (4)
25 (15) lt0001Pers AF 9 (28) 12 (32) 7 (28)
LS Pers
AF20 (36) 23 (61) 17 (68)
Circulation 2010122109-118
Left Atrial Appendage An Under recognized Trigger Site of Atrial
Fibrillation
LAA Isolation Improves Ablation Outcomes
Di Biase et al Circulation 2010122109-118
Unexpectedly High Incidence of Stroke and Left
Atrial Appendage Thrombus Formation after
Electrical Isolation of the Left Atrial Appendage for
Treatment of Atrial Tachyarrhythmias
An undescribed and under recognized complication
of left atrial catheter ablationAndreas Rillig MD Roland R Tilz MD Tina Lin MD Christian Heeger MD Anita
Arya PHD Andreas Metzner MD Shibu Mathew MD Erik Wissner MD Hisaki
Makimoto MD PHD Peter Wohlmuth Karl-Heinz Kuck MD Feifan Ouyang MD
LAA
thrombus
Mechanical standstill
Thrombus formation
LAA thrombus in 21 and three
patients had a stroke while on OAC
Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Disclosure
SentreHeart Incbull Consultant
bull Equity holder
Lone Star Heart Inc
Restore Maintain Protect
Role of LAA Ligation in Patients with Persistent or Longstanding Persistent AF
Electrical Isolation
Atrial debulking
LAA Exclusion
Catheter Ablation of
Long-Standing Persistent Atrial Fibrillation5-Year Outcomes of the Hamburg Sequential Ablation Strategy
Roland Richard Tilz MD Andreas Rillig MD Anna-Maria Thum Anita Arya MD Peter
Wohlmuth Andreas Metzner MD Shibu Mathew MD Yasuhiro Yoshiga MD Erik
Wissner MD Karl-Heinz Kuck MD Feifan Ouyang MD
JACC 2012601921ndash9
After the first ablation procedure sinus rhythm was
documented in 41 of 202 (203) patients
After multiple procedures sinus rhythm was maintained in 91
of 202 (450) patients
Role of LAA in AF
Automaticity cells
identified in the LAA
that leads to AT
LAA Triggers Reentrant
Circuits
Thrombus
Formation
Heterogeneous fiber
orientation and the
presence of
trabeculated muscle
influence wave
propagation and favor
the formation of
conduction
blockslow
conduction and
initiation of reentry
Guo et al Heart Rhythm 1117ndash25 2014
Fibrillating Areas Isolated within the Left Atrium after
Radiofrequency Linear Catheter Ablation
RostockhellipHaissaguerre JCE 17807-812 2006
Group I ndashStd BOX
Procedure (n=43)
Group II ndash Std BOX
Proc w LAA focal
ablation (n=56)
Group III ndash Std BOX
Proc w LAA electrical
Isolation (n=167)
P value
(Groups
1 vs 2 vs
3)
AF TypeRecurrence
by type
Total
Recurrences
Recurrence
by type
Total
Recurrences
Recurrence
by Type
Total
Recurrences
Follow Up
Months11+3 11+3 12+3 0910
PAF 3 (9)
32 (74)
3 (8)
38 (68)
1 (4)
25 (15) lt0001Pers AF 9 (28) 12 (32) 7 (28)
LS Pers
AF20 (36) 23 (61) 17 (68)
Circulation 2010122109-118
Left Atrial Appendage An Under recognized Trigger Site of Atrial
Fibrillation
LAA Isolation Improves Ablation Outcomes
Di Biase et al Circulation 2010122109-118
Unexpectedly High Incidence of Stroke and Left
Atrial Appendage Thrombus Formation after
Electrical Isolation of the Left Atrial Appendage for
Treatment of Atrial Tachyarrhythmias
An undescribed and under recognized complication
of left atrial catheter ablationAndreas Rillig MD Roland R Tilz MD Tina Lin MD Christian Heeger MD Anita
Arya PHD Andreas Metzner MD Shibu Mathew MD Erik Wissner MD Hisaki
Makimoto MD PHD Peter Wohlmuth Karl-Heinz Kuck MD Feifan Ouyang MD
LAA
thrombus
Mechanical standstill
Thrombus formation
LAA thrombus in 21 and three
patients had a stroke while on OAC
Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Restore Maintain Protect
Role of LAA Ligation in Patients with Persistent or Longstanding Persistent AF
Electrical Isolation
Atrial debulking
LAA Exclusion
Catheter Ablation of
Long-Standing Persistent Atrial Fibrillation5-Year Outcomes of the Hamburg Sequential Ablation Strategy
Roland Richard Tilz MD Andreas Rillig MD Anna-Maria Thum Anita Arya MD Peter
Wohlmuth Andreas Metzner MD Shibu Mathew MD Yasuhiro Yoshiga MD Erik
Wissner MD Karl-Heinz Kuck MD Feifan Ouyang MD
JACC 2012601921ndash9
After the first ablation procedure sinus rhythm was
documented in 41 of 202 (203) patients
After multiple procedures sinus rhythm was maintained in 91
of 202 (450) patients
Role of LAA in AF
Automaticity cells
identified in the LAA
that leads to AT
LAA Triggers Reentrant
Circuits
Thrombus
Formation
Heterogeneous fiber
orientation and the
presence of
trabeculated muscle
influence wave
propagation and favor
the formation of
conduction
blockslow
conduction and
initiation of reentry
Guo et al Heart Rhythm 1117ndash25 2014
Fibrillating Areas Isolated within the Left Atrium after
Radiofrequency Linear Catheter Ablation
RostockhellipHaissaguerre JCE 17807-812 2006
Group I ndashStd BOX
Procedure (n=43)
Group II ndash Std BOX
Proc w LAA focal
ablation (n=56)
Group III ndash Std BOX
Proc w LAA electrical
Isolation (n=167)
P value
(Groups
1 vs 2 vs
3)
AF TypeRecurrence
by type
Total
Recurrences
Recurrence
by type
Total
Recurrences
Recurrence
by Type
Total
Recurrences
Follow Up
Months11+3 11+3 12+3 0910
PAF 3 (9)
32 (74)
3 (8)
38 (68)
1 (4)
25 (15) lt0001Pers AF 9 (28) 12 (32) 7 (28)
LS Pers
AF20 (36) 23 (61) 17 (68)
Circulation 2010122109-118
Left Atrial Appendage An Under recognized Trigger Site of Atrial
Fibrillation
LAA Isolation Improves Ablation Outcomes
Di Biase et al Circulation 2010122109-118
Unexpectedly High Incidence of Stroke and Left
Atrial Appendage Thrombus Formation after
Electrical Isolation of the Left Atrial Appendage for
Treatment of Atrial Tachyarrhythmias
An undescribed and under recognized complication
of left atrial catheter ablationAndreas Rillig MD Roland R Tilz MD Tina Lin MD Christian Heeger MD Anita
Arya PHD Andreas Metzner MD Shibu Mathew MD Erik Wissner MD Hisaki
Makimoto MD PHD Peter Wohlmuth Karl-Heinz Kuck MD Feifan Ouyang MD
LAA
thrombus
Mechanical standstill
Thrombus formation
LAA thrombus in 21 and three
patients had a stroke while on OAC
Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Catheter Ablation of
Long-Standing Persistent Atrial Fibrillation5-Year Outcomes of the Hamburg Sequential Ablation Strategy
Roland Richard Tilz MD Andreas Rillig MD Anna-Maria Thum Anita Arya MD Peter
Wohlmuth Andreas Metzner MD Shibu Mathew MD Yasuhiro Yoshiga MD Erik
Wissner MD Karl-Heinz Kuck MD Feifan Ouyang MD
JACC 2012601921ndash9
After the first ablation procedure sinus rhythm was
documented in 41 of 202 (203) patients
After multiple procedures sinus rhythm was maintained in 91
of 202 (450) patients
Role of LAA in AF
Automaticity cells
identified in the LAA
that leads to AT
LAA Triggers Reentrant
Circuits
Thrombus
Formation
Heterogeneous fiber
orientation and the
presence of
trabeculated muscle
influence wave
propagation and favor
the formation of
conduction
blockslow
conduction and
initiation of reentry
Guo et al Heart Rhythm 1117ndash25 2014
Fibrillating Areas Isolated within the Left Atrium after
Radiofrequency Linear Catheter Ablation
RostockhellipHaissaguerre JCE 17807-812 2006
Group I ndashStd BOX
Procedure (n=43)
Group II ndash Std BOX
Proc w LAA focal
ablation (n=56)
Group III ndash Std BOX
Proc w LAA electrical
Isolation (n=167)
P value
(Groups
1 vs 2 vs
3)
AF TypeRecurrence
by type
Total
Recurrences
Recurrence
by type
Total
Recurrences
Recurrence
by Type
Total
Recurrences
Follow Up
Months11+3 11+3 12+3 0910
PAF 3 (9)
32 (74)
3 (8)
38 (68)
1 (4)
25 (15) lt0001Pers AF 9 (28) 12 (32) 7 (28)
LS Pers
AF20 (36) 23 (61) 17 (68)
Circulation 2010122109-118
Left Atrial Appendage An Under recognized Trigger Site of Atrial
Fibrillation
LAA Isolation Improves Ablation Outcomes
Di Biase et al Circulation 2010122109-118
Unexpectedly High Incidence of Stroke and Left
Atrial Appendage Thrombus Formation after
Electrical Isolation of the Left Atrial Appendage for
Treatment of Atrial Tachyarrhythmias
An undescribed and under recognized complication
of left atrial catheter ablationAndreas Rillig MD Roland R Tilz MD Tina Lin MD Christian Heeger MD Anita
Arya PHD Andreas Metzner MD Shibu Mathew MD Erik Wissner MD Hisaki
Makimoto MD PHD Peter Wohlmuth Karl-Heinz Kuck MD Feifan Ouyang MD
LAA
thrombus
Mechanical standstill
Thrombus formation
LAA thrombus in 21 and three
patients had a stroke while on OAC
Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Role of LAA in AF
Automaticity cells
identified in the LAA
that leads to AT
LAA Triggers Reentrant
Circuits
Thrombus
Formation
Heterogeneous fiber
orientation and the
presence of
trabeculated muscle
influence wave
propagation and favor
the formation of
conduction
blockslow
conduction and
initiation of reentry
Guo et al Heart Rhythm 1117ndash25 2014
Fibrillating Areas Isolated within the Left Atrium after
Radiofrequency Linear Catheter Ablation
RostockhellipHaissaguerre JCE 17807-812 2006
Group I ndashStd BOX
Procedure (n=43)
Group II ndash Std BOX
Proc w LAA focal
ablation (n=56)
Group III ndash Std BOX
Proc w LAA electrical
Isolation (n=167)
P value
(Groups
1 vs 2 vs
3)
AF TypeRecurrence
by type
Total
Recurrences
Recurrence
by type
Total
Recurrences
Recurrence
by Type
Total
Recurrences
Follow Up
Months11+3 11+3 12+3 0910
PAF 3 (9)
32 (74)
3 (8)
38 (68)
1 (4)
25 (15) lt0001Pers AF 9 (28) 12 (32) 7 (28)
LS Pers
AF20 (36) 23 (61) 17 (68)
Circulation 2010122109-118
Left Atrial Appendage An Under recognized Trigger Site of Atrial
Fibrillation
LAA Isolation Improves Ablation Outcomes
Di Biase et al Circulation 2010122109-118
Unexpectedly High Incidence of Stroke and Left
Atrial Appendage Thrombus Formation after
Electrical Isolation of the Left Atrial Appendage for
Treatment of Atrial Tachyarrhythmias
An undescribed and under recognized complication
of left atrial catheter ablationAndreas Rillig MD Roland R Tilz MD Tina Lin MD Christian Heeger MD Anita
Arya PHD Andreas Metzner MD Shibu Mathew MD Erik Wissner MD Hisaki
Makimoto MD PHD Peter Wohlmuth Karl-Heinz Kuck MD Feifan Ouyang MD
LAA
thrombus
Mechanical standstill
Thrombus formation
LAA thrombus in 21 and three
patients had a stroke while on OAC
Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Fibrillating Areas Isolated within the Left Atrium after
Radiofrequency Linear Catheter Ablation
RostockhellipHaissaguerre JCE 17807-812 2006
Group I ndashStd BOX
Procedure (n=43)
Group II ndash Std BOX
Proc w LAA focal
ablation (n=56)
Group III ndash Std BOX
Proc w LAA electrical
Isolation (n=167)
P value
(Groups
1 vs 2 vs
3)
AF TypeRecurrence
by type
Total
Recurrences
Recurrence
by type
Total
Recurrences
Recurrence
by Type
Total
Recurrences
Follow Up
Months11+3 11+3 12+3 0910
PAF 3 (9)
32 (74)
3 (8)
38 (68)
1 (4)
25 (15) lt0001Pers AF 9 (28) 12 (32) 7 (28)
LS Pers
AF20 (36) 23 (61) 17 (68)
Circulation 2010122109-118
Left Atrial Appendage An Under recognized Trigger Site of Atrial
Fibrillation
LAA Isolation Improves Ablation Outcomes
Di Biase et al Circulation 2010122109-118
Unexpectedly High Incidence of Stroke and Left
Atrial Appendage Thrombus Formation after
Electrical Isolation of the Left Atrial Appendage for
Treatment of Atrial Tachyarrhythmias
An undescribed and under recognized complication
of left atrial catheter ablationAndreas Rillig MD Roland R Tilz MD Tina Lin MD Christian Heeger MD Anita
Arya PHD Andreas Metzner MD Shibu Mathew MD Erik Wissner MD Hisaki
Makimoto MD PHD Peter Wohlmuth Karl-Heinz Kuck MD Feifan Ouyang MD
LAA
thrombus
Mechanical standstill
Thrombus formation
LAA thrombus in 21 and three
patients had a stroke while on OAC
Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Group I ndashStd BOX
Procedure (n=43)
Group II ndash Std BOX
Proc w LAA focal
ablation (n=56)
Group III ndash Std BOX
Proc w LAA electrical
Isolation (n=167)
P value
(Groups
1 vs 2 vs
3)
AF TypeRecurrence
by type
Total
Recurrences
Recurrence
by type
Total
Recurrences
Recurrence
by Type
Total
Recurrences
Follow Up
Months11+3 11+3 12+3 0910
PAF 3 (9)
32 (74)
3 (8)
38 (68)
1 (4)
25 (15) lt0001Pers AF 9 (28) 12 (32) 7 (28)
LS Pers
AF20 (36) 23 (61) 17 (68)
Circulation 2010122109-118
Left Atrial Appendage An Under recognized Trigger Site of Atrial
Fibrillation
LAA Isolation Improves Ablation Outcomes
Di Biase et al Circulation 2010122109-118
Unexpectedly High Incidence of Stroke and Left
Atrial Appendage Thrombus Formation after
Electrical Isolation of the Left Atrial Appendage for
Treatment of Atrial Tachyarrhythmias
An undescribed and under recognized complication
of left atrial catheter ablationAndreas Rillig MD Roland R Tilz MD Tina Lin MD Christian Heeger MD Anita
Arya PHD Andreas Metzner MD Shibu Mathew MD Erik Wissner MD Hisaki
Makimoto MD PHD Peter Wohlmuth Karl-Heinz Kuck MD Feifan Ouyang MD
LAA
thrombus
Mechanical standstill
Thrombus formation
LAA thrombus in 21 and three
patients had a stroke while on OAC
Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
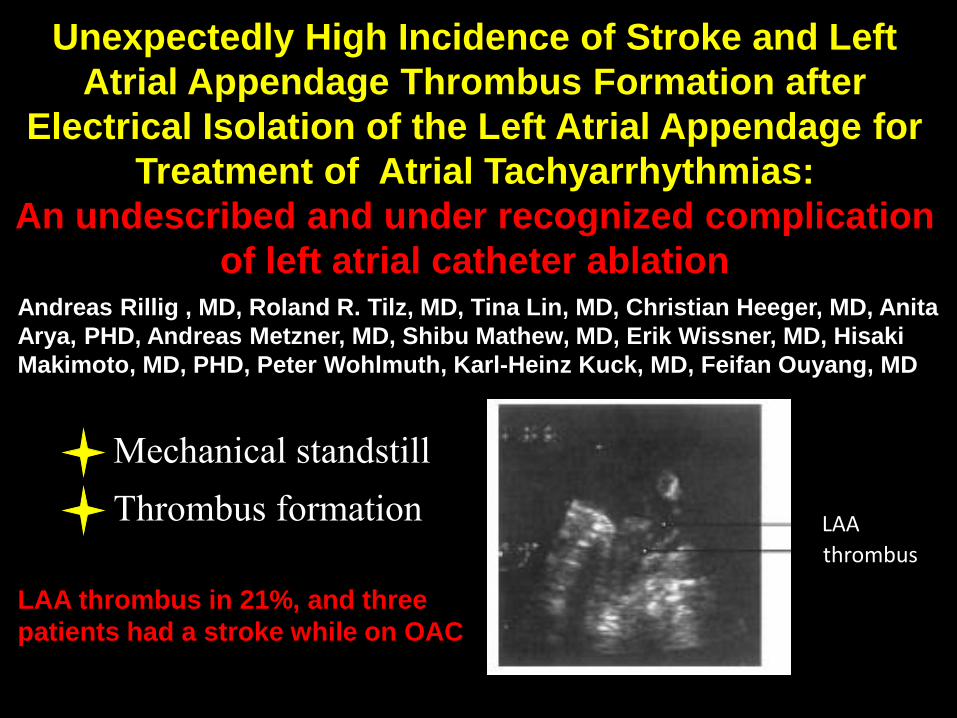
Unexpectedly High Incidence of Stroke and Left
Atrial Appendage Thrombus Formation after
Electrical Isolation of the Left Atrial Appendage for
Treatment of Atrial Tachyarrhythmias
An undescribed and under recognized complication
of left atrial catheter ablationAndreas Rillig MD Roland R Tilz MD Tina Lin MD Christian Heeger MD Anita
Arya PHD Andreas Metzner MD Shibu Mathew MD Erik Wissner MD Hisaki
Makimoto MD PHD Peter Wohlmuth Karl-Heinz Kuck MD Feifan Ouyang MD
LAA
thrombus
Mechanical standstill
Thrombus formation
LAA thrombus in 21 and three
patients had a stroke while on OAC
Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Sick et al JACC 2007
When should you exclude the
LAA Before or After PVI
Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Feasibility and Safety of Combined
PVI and LAA closure
Ablation for Atrial Fibrillation in Combination With Left Atrial
Appendage Closure First Results of a Feasibility Study
Martin J Swaans MD Martijn C Post MD PhD Benno JWM Rensing MD PhD
Lucas VA Boersma MD PhD
J Am Heart Assoc 2012
Combined catheter ablation and left atrial appendage closure as a
hybrid procedure for the treatment of atrial fibrillation
Calvo N Salterain N Arguedas H Macias A Esteban A Garciacutea de Yeacutebenes M1
Gavira JJ Barba J Garciacutea-Bolao I
Europace 2015
Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Sick et al JACC 2007
PVI and LAA electrical isolation
should be done before LAA closure
with an LAA implant
AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

AF ablation post LAA closurePatient
()
LAA-closure
device
(size)
Time from
LAA-closure to
LA-ablation
(days)
PAFPersAFPrevious LA-
ablation
Index
procedure
Follow-up
Device related
complications
assessed by
TEE
(days)
Follow-up
ATAF-
recurrence
(longest
follow-up
days)
Follow-up
Clinical
complications
1ACP
(22mm)234 PAF - CPVI 0 (759) 0 (622) 0
2WATCHMAN
(33mm)182 PAF CPVI CPVI 0 (778) 1 (778) 0
3WATCHMAN
(21mm)133 PAF - CPVI 0 (464) 0 (466) 0
4WATCHMAN
(24mm)105 PersAF CPVI
Ablation of
anterior line
ostial potentials
and mitral
isthmus line
0 (504) 0 (400) 0
5WATCHMAN
(24mm)41 PAF - CPVI 0 (187) 0 (188) 0
6WATCHMAN
(27mm)92 PAF -
CPVI
Ablation of an
anterior line
0 (218) 1 (218) 0
7WATCHMAN
(27mm)756 PersAF
CPVI and LAA-
isolation via
ablation of
anterior and
mitral isthmus
line
Re-isolation of
LAA via mitral
isthmus line
0 (1006) 0 (1006) 0
8WATCHMAN
(27mm)63 PersAF -
CPVI
Ablation of
CFAEs in CS
and LA anterior
line and mitral
isthmus line
Thrombus (113) 1 (673) 0
Heeger Tilz Heart Rhythm accepted for publication
C D
LA
WATCHMAN
AV
LA
WATCHMAN
AV
Thrombu
s
CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

CTA of Watchman device
Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Does left atrial appendage closure improve the
success of pulmonary vein isolation Results
of a randomized clinical trialAlexander Romanov Evgeny Pokushalov Sergey Artemenko Akmal
Yakubov Ilya Stenin Evgeny Kretov Oleg Krestianinov Igor Grazhdankin
Dejan Risteski Alexander Karaskov Jonathan S Steinberg
J Interv Card Electrophysiol 449-16 2015
LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

LAA ligation and PVI
IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

IV
C
MV
SVC
LAA ligation with PVI Cox Maze III
LAA exclusion as adjunctive therapy to PVI
for the treatment of AF What is the rationale
- Elimination of atrial arrhythmias arising from the LAA
- Left atrial debulkingreduction results in decreased left
atrial dispersion
Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Prasad SM J Thorac Cardiovasc Surg 20031261822-28
Benefit of LAA Closure
ldquoCut and sewrdquo
Cox-Maze
Cox J et al J Thorac Cardiovasc
Surg 1999118833-840
AF Hx TE No OAC
AF No TE No OAC
AF Hx TE OAC
AF No TE OAC
AF No Risk No TE No OAC
Post maze No OAC No LAA
LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

LAA
LA
LA
LAA
1 cmLAA Suture Endo
EndoLA
H
LAA ligation results in a permanent
transmural lesion
Bartus et al Circ Arrhythmia 7764-767 2014
LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

LAA closure enables a more
complete ablation procedure
Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Ligament of Marshall
Kim et al JACC 361324-7 2000
Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Localized reentry within the left atrial appendage
arrhythmogenic role in patients undergoing
ablation of persistent atrial fibrillationHocini M Shah AJ Nault I Sanders P Wright M Narayan SM Takahashi Y Jaiumls P Matsuo S
Knecht S Sacher F Lim KT Cleacutementy J Haiumlssaguerre M
Heart Rhythm 2011 Dec8(12)1853-61
The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

The Effects of LAA Ligation on
LAA Electrical Activity Frederick T Han MD1 Krzysztof Bartus MD PhD 2 Dhanunjaya Lakkireddy MD3 Francia
Rojas MD4 Jacek Bednarek MD PhD5 Boguslaw Kapelak MD PhD2 Magdalena Bartus
PhD 6 Nitish Badhwar MBBS FHRS7 Mathew Earnest MD3 Miguel Valderrabano MD4
Randall J Lee MD PhD789
N = 30 N = 38
Han et al Heart Rhythm 11864ndash870 2014
A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

A B C
D
Han et al Heart Rhythm 2014
Bipolar recordings Unipolar recordings
Pre
Post
PostPre
Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Sequential Percutaneous LAA ligation and
pulmonary vein isolation in patients with persistent
AF Initial results of a feasibility study
Nitish Badhwar Dhanunjaya Lakkireddy Mitsuharu Kawamura Frederick T Han
Sivaraman K Iyer Brian S Moyers Thomas A Dewland Chris Woods Ryan Ferrell
Jayanth Nath Mathew Earnes Randall J Lee
20
25
30
35
40
45
50
55
60
Pre-ligation Post-ligation Post-PVI 2 months after PVI
Recurrent-AF(n-1)
SR (n=9)
Badhwar et al JCE 2015
Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Effect of Endoepicardial Percutaneous Left Atrial Appendage
Ligation on Arrhythmia Burden in Patients with Atrial
Fibrillation
Afzal et al Heart Rhythm 2015
LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

LAA-LA Registry
0
10
20
30
40
50
60
70
LARIAT +Ablation
Ablation Only Total
Recurrence Rate
Lakkireddy et al
2469
4269
66138
JACC EP 2015
bull 69 consecutive patients undergoing LAA ligation with LARIAT system followed by AF ablation vs ablation only
bull Primary Outcome Recurrence of AF 12M
ndash Defined as recurring AF episodes gt30 sec via 24hr holter monitor
bull AF recurrence was lower in the LARIAT group (35 vs 61 p=0028) after the first ablation
bull Fewer patients in the LARIAT group needed repeat ablation (16 vs 33 p=0018)
bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

bull Multi-center prospective randomized trial
bull Comparing LAA ligation and PVI versus
PVI in patients with persistent and
longstanding persistent AF
aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

aMAZE Trial
Hypothesisbull The LAA is a critical structure in the maintenance of
persistent and longstanding persistent AF and LAAligation will decrease the recurrence of AF in patientswith persistent and longstanding persistent AF
Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Protocol Synopsis
Principal Purpose Evaluate the additional efficacy of LARIAT LAA ligation
to decrease the 12-month rate of AF and to confirm an
acceptable safety profile
Patient Population Patients (18-80 yo) with documented persistent or
longstanding persistent AF (lt 3 yrs continuous AF)
planned for catheter ablation
Design Prospective multicenter RCT (21)
Bayesian Adaptive Design 400 ndash 600 subjects total
~50 sites
2 randomized stages Stage 1 le 175 subjects interim
safety and performance analysis of first 100
Investigational Tx LARIAT LAA ligation followed by PVI catheter ablation
(separated by gt4 weeks)
Control Tx PVI catheter ablation without LAA ligation
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Primary Endpoints
Primary
Effectiveness
Endpoint
Freedom from episodes of AF gt 30 seconds and no
requirement for new Class I or III AAD therapy at 12
months post PVI measured by 24-hr holter or
symptomatic event monitoring
Primary Safety
Endpoint
The incidence of significant LARIAT device or procedure-
related SAEs occurring within 30 days after the LAA
ligation procedure (Performance Goal)
consistent with HRS 2012 Consensus Guidelines (Table 5)
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Freedom from episodes of AF gt 30 seconds at
12M post-index PVI follow-up defined as
bull Any episode of AFATAFL gt 30 sec
bull Documented by 24-hour holter ( 6 amp 12M)
bull No requirement for new Class I or III AAD
therapy prescribed for AF following the 90-day
blanking period
bull No catheter ablation procedures post index PVI
(aside from ablation for right-sided AFL)CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Effectiveness Endpoint Definition
30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

30-day CEC adjudicated LARIAT device- or procedure-related SAEs
bull Serious injury to cardiac related structure requiring surgical intervention
bull Bleedingndash ge 2 units PRBC administered in post-op day 1 or 2 periodndash Organ structure injury requiring interventionndash Fatal
bull Pericarditis hemothorax and or pneumothorax requiring surgical treatment
bull Vascular injury requiring surgical treatment hospital admission or PRBC transfusion
bull Pseudoaneurysm Arteriovenous fistula on imaging or direct visualization
bull Pericardial effusions requiring surgical interventionCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Primary Safety Events
bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

bull Effectiveness Endpoint (Superiority)
ndash Powered to detect an absolute difference of
15 between treatment and control
ndash Max sample size allows for observed clinically
significant difference of 10 as statistically
significant
bull Primary Safety Endpoint (Performance Goal)
ndash Compared against a prospectively defined
performance goal (PG) of 10
bull Expected rate of 6 w statistical margin
Primary Endpoint Assumptions
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Understanding the Trial Format
bull Study conducted in two stages
ndash Initial (Stage 1) followed by a pivotal stage (Stage
2)
ndash All patients from both stages will be included in the
primary analysis
bull Interim data review of first 100 patients enrolled with
30-day follow-up will be reviewed by Data Monitoring
Committee (DMC) for endorsement to expand
bull Enrollment will continue to a maximum of 175 subjects
during Stage 1 analysis and review
aMAZE TrialCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Expansion Stage 1 2
Expansion Rules ndash aligned with futility rules in the interim analyses
bull 30-day primary safety endpoint rate futility bound probability lt0025
bull Corresponds to approximately 9 or fewer safety events in the first 67 LARIAT patients
and
bull Data Monitoring Committee review of overall safety and performance (including closure) identifies no significant issues or trends of concern
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Notable Secondary Endpoints
bull LARIAT Technical Success
ndash Successful placement of the LARIAT System pre-tied suture around the LAA to achieve effective LAA ligation
ndash Defined as le1 plusmn 1mm diameter residual communication w LA
ndash Assessed by TEE color Doppler confirmed by Imaging Core Lab immediately post LARIAT (acute) 30-45D post LARIAT and 12M post-PVI
CONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107
Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107

Notable Secondary Endpoints
bull 30D post PVI MAE
bull Stroke systemic embolism +- death of any cause post PVI
bull Freedom from AFATAFL recurrence gt 30 sec following 90 day blanking period with or without AAD
bull Incidence of re-intervention (ie catheter or surgical ablation) for recurrence at 12M post-index PVI
bull Incidence of DC conversions re-intervention for recurrence amp cardiac hospitalizations at 12M post-index PVI
adjudicated by CECCONFIDENTIALFor amaze Trial Investigators OnlyFDA IDE G150107