the science and practice of lsvt big & lsvt loud within the
TRANSCRIPT

9/21/2016
1
The Science and Practice of LSVT BIG & LSVT LOUD Within
the Home Health Setting:Building a Successful Clinical Program
This work was supported, in part, by the: National Institutes of Health - R01 DC1150, R21DC006078, R21 NS043711, Michael J. Fox Foundation, Parkinson Alliance and Davis Phinney Foundation
Learning Objectives
• Briefly discuss development and data on an efficacious speech treatment LSVT LOUD™
• Describe development and key aspects of limb motor treatment LSVT BIG™
• Describe the use of/adaptation of LSVT BIG and LSVT LOUD administered in the home.
• Describe the variety of patients that can be treated in the home.
• Discuss reimbursement for LSVT BIG and LSVT LOUD provided in the home setting.

9/21/2016
2
It is a “Stunning Time” to be in rehabilitation today
• Basic science evidence for the value of exercise in PD (classically drugs, surgery, today…)
• Identified key principles of exercise that drive activity-dependent neural plasticity
• Demonstrated that exercise can improve brain functioning (neural plasticity) and may slow disease progression
• Exercise is Medicine!Kleim & Jones, 2008; Ludlow et al, 2008
Legitimate Therapeutic OptionsTo provide symptomatic relief; improve function
Pharmacological(L-dopa)
Voice and Body Exercise
Neurosurgical(DBS-STN)
Zigmond et al, 2009

9/21/2016
3
Video Example:
• 59 year old female• 2.5 years post-diagnosis• On-meds pre and post video
Pre/post LSVT LOUD(Lee Silverman Voice Treatment)Intensive physical exercise of speech mechanism
Insert Short Shirley Video Here
9/21/2016
4
Patient case: Bernie
• 71 year-old, diagnosed with Parkinson’s disease in 1994
• Reason for referral: slowness and difficulty walking, history of falls, freezing
• Optimized on PD medications
• Hoehn & Yahr 3
Insert LSVT Walk BIG video here
9/21/2016
5
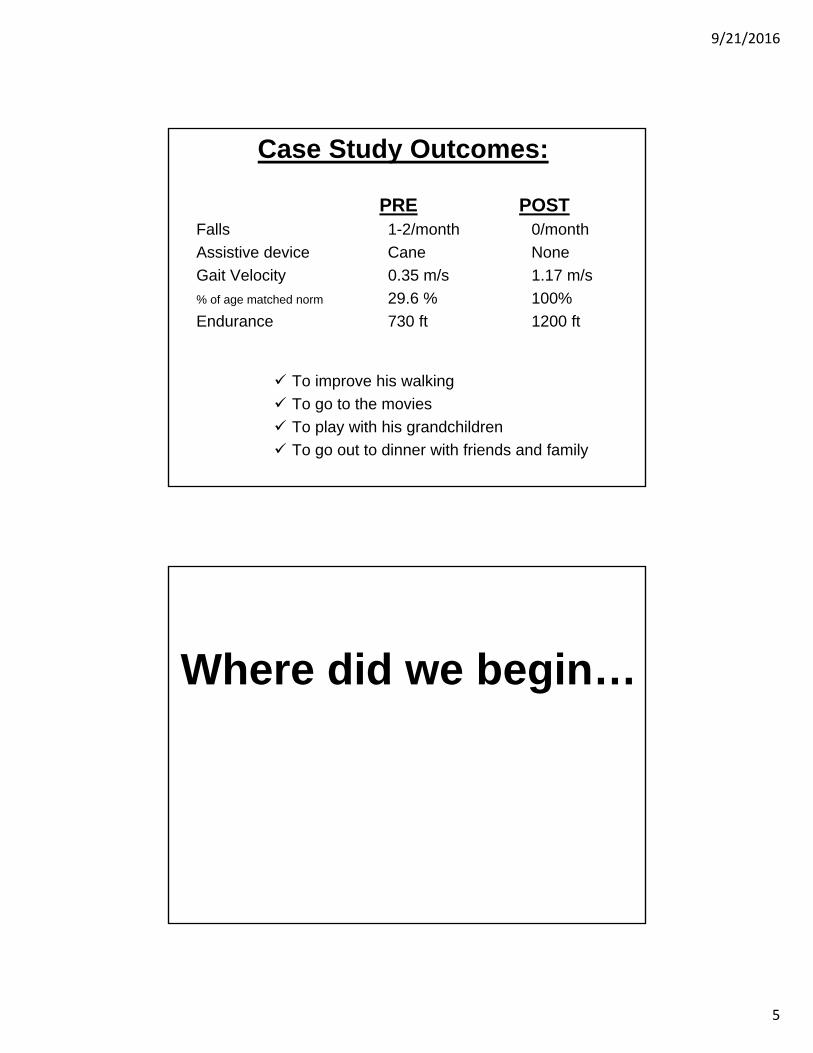
Case Study Outcomes:
Falls 1-2/month 0/month
Assistive device Cane None
Gait Velocity 0.35 m/s 1.17 m/s
% of age matched norm 29.6 % 100%
Endurance 730 ft 1200 ft
PRE POST
To improve his walking
To go to the movies
To play with his grandchildren
To go out to dinner with friends and family
Where did we begin…

9/21/2016
6
“If only we can hear and understand her”Family of Mrs. Lee Silverman 1987
Administered in an intensive manner to to challenge the impaired system.
Techniques specific to PD-specific deficits!bradykinesia/hypokinesia
and kinesthetic awareness
(sensory deficit)
LSVT Programs

9/21/2016
7
SOFT
LOUD
HEALTHY LOUDNESS
Loud is more than a laryngeal event – spread of effects
TARGET
What are the LSVT LOUD exercises?Daily tasksFirst half of treatment sessionRescale amplitude of motor output through CORE Loud
• Sustained “ah” (minimum15 reps)• High/Low “ah” (minimum15 reps)• Functional phrases (minimum 50 reps)
Hierarchical speech tasks Second half of sessionTrain amplitude from CORE exercises into in context specific and variable speaking activities
• Week 1 – words, phrases• Week 2 – sentences• Week 3 – reading• Week 4 - conversation
MODE
Shorter, simple
Longer, more complex
9/21/2016
8
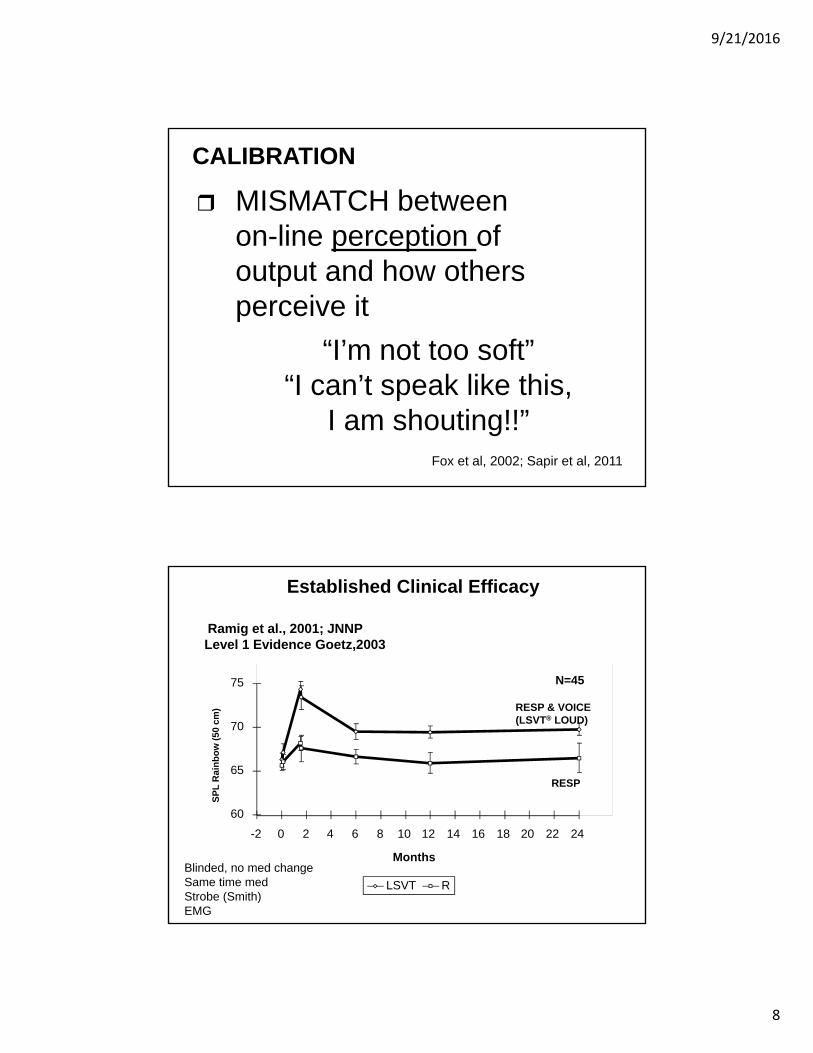
MISMATCH betweenon-line perception ofoutput and how othersperceive it
“I’m not too soft”“I can’t speak like this,
I am shouting!!”Fox et al, 2002; Sapir et al, 2011
CALIBRATION
Ramig et al., 2001; JNNPLevel 1 Evidence Goetz,2003
60
65
70
75
-2 0 2 4 6 8 10 12 14 16 18 20 22 24
Months
SP
L R
ain
bo
w (
50 c
m)
LSVT R
RESP & VOICE (LSVT® LOUD)
RESP
N=45
Blinded, no med changeSame time medStrobe (Smith)EMG
Established Clinical Efficacy

9/21/2016
9
Advances in Clinical Efficacy(Ramig et al, 1995; 1996; 2001a; 2001b; Goetz, 2003)
Cross-system effects, Neural changes
Spielman, Borod (2003)
(facial expression)
El-Sharkawi, Logemann(2002)
(swallowing)
Smith, M. (1995)
(adduction)
Ramig & Dromey(1996)
(aerodynamics)
Baker (1998),
Luschei (1999) (EMG)
P. Fox, Liotti(2003)
Narayana (2010)
(PET) Dromey, (1995) (articulation)
Sapir (2007; 2010)
(articulatory acoustics)
Smith,A. (2001)(STI)
Taskoff (2001)
(perceptual)
Huber, Stathopoulos, (2003)
(respiratory kinematics)
LSVT LOUD® LSVT BIG ®
(Ebersbach et al, 2010; Farley & Koshland, 2005; Fox, et al., 2012)

9/21/2016
10
What are the fundamentals of LSVT BIG?
TARGET: Bigness (amplitude)
MODE: Intensive and High Effort
CALIBRATION: GeneralizationSensoryInternal cueingNeuropsychological changes
Standardized, research-based, specific protocol
BIG (Large amplitude whole body movement)Single Target - Triggers Activation across motor systems
SMALLBIG
TARGET

9/21/2016
11
Delivery– Certified LSVT BIG Physical/Occupational
Therapist• 1:1 intervention
Time of Practice– 4 consecutive days per week for 4 weeks
– 16 sessions in one month
– 60 minute sessions
– Daily carryover assignments (30 days/entire month)
– Daily homework (30 days/entire month)
MODE
MISMATCH betweenon-line perception ofoutput and how others perceive it
“I had no idea how small my world had become”
“I can’t move like this, people will think I am crazy!!”
CALIBRATION

9/21/2016
12
Problem in self-perception/awareness -do not recognize movements
are small or slow
Produce slow, small movements
Reducedamplitude of motor output
Self-cueing deficits -continue scaling reduced
amplitude of movement patterns
PRE-TREATMENT
Fox et al., 2012
Improve self-perception/awarenessof amplitude required to
produce normalmovement amplitude
Produce larger movements
INCREASEamplitude of motor output
Improve self-cueing/attention to action -habitually scale increased amplitude
of movement patterns
TREATMENT FOCUS
Fox et al., 2012

9/21/2016
13
LSVT BIG: Data
Comparing Exercise in Parkinson’s Disease —The Berlin LSVT BIG Study (2010, Movement Disorders)Georg Ebersbach,1* Almut Ebersbach,1 Daniela Edler,1 Olaf Kaufhold,1 Matthias Kusch,1
Andreas Kupsch,2 and Jo¨rg Wissel3

9/21/2016
14
Comparing Exercise in Parkinson’s Disease —The Berlin LSVT BIG Study (2010, Movement Disorders)Georg Ebersbach,1* Almut Ebersbach,1 Daniela Edler,1 Olaf Kaufhold,1 Matthias Kusch,1
Andreas Kupsch,2 and Jo¨rg Wissel3
FIG. 2. UPDRS motor score (blinded rating), mean change from baseline (vertical bars 5 standard deviations). Change between baseline and follow up at week 16 was superior in BIG (interrupted line) compared to WALK (dotted line) and HOME (solid line), P <0.001. ANCOVA did not disclose significant differences between in intermediate and final assessments.
What about Fine Motor Tasks?
• Even small movements are TOO SMALL in people with PD! – Examples: writing, buttoning, teeth brushing, stirring
9/21/2016
15
Initial 3/15/2010
Discharge 4/8/2010
Generalized Amplitude: Uncued writing post-treatment and untrained during therapy
Buttoning BIG Video
Insert short buttoning revised

9/21/2016
16
LSVT BIG: Treatment Protocol
OVERVIEW – PROTOCOL
• 4 consecutive days a week for 4 weeks
• 16 sessions in 1 month
• 60 minute sessions

9/21/2016
17
LSVT BIG Treatment SessionMaximal Daily Exercises1.Floor to Ceiling – 8 reps2.Side to Side – 8 each side3.Forward step – 8 each side4.Sideways step – 8 each side5.Backward step – 8 each side6.Forward Rock and Reach –10 each side (working up to 20) 7.Sideways Rock and Reach –10 each side (working up to 20)
Functional Component Tasks
5 EVERYDAY TASKS– 5 reps each For example:
-Sit-to-Stand
-Pulling keys out of pocket
-Opening cell phone (flip phone)
Hierarchy TasksPatient identified tasks:
Getting out of bed
Playing golf
In and out of a car
Build complexity across 4 weeks of treatment towards long-term goal
Walking BIG
Distance/time may vary
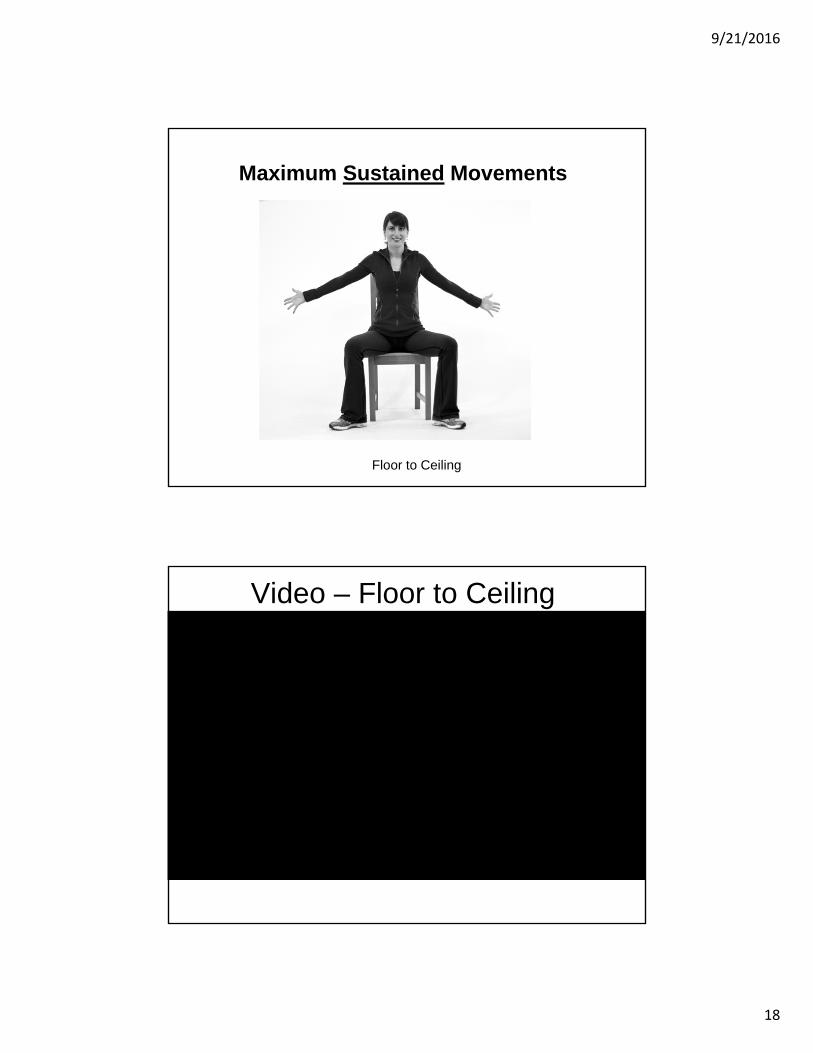
Maximum Sustained Movements
Floor to Ceiling Side to Side
9/21/2016
18
Maximum Sustained Movements
Floor to Ceiling
Video – Floor to Ceiling
Insert HH DVD clip of this exercise

9/21/2016
19
Maximum Sustained Movements
Side to Side
Video – Side to Side
Insert HH DVD clip of this exercise

9/21/2016
20
Multidirectional Repetitive MovementsStep and Reach
Forward Step Sideways Step Backward Step
Multidirectional Repetitive Movements Step and Reach
Forward Step

9/21/2016
21
Video – Step Forward
Insert HH DVD clip of this exercise
Multidirectional Repetitive Movements Step and Reach
Sideways Step

9/21/2016
22
Video Step Sideways
Insert HH DVD clip of this exercise
Multidirectional Repetitive Movements Step and Reach
Backward Step

9/21/2016
23
Video – Step Backward
Insert HH DVD clip of this exercise
Multidirectional Repetitive MovementsRock and Reach
Sideways Rock and Reach Forward/Backward Rock and Reach

9/21/2016
24
Multidirectional Repetitive MovementsRock and Reach
Forward/Backward Rock and Reach
Video Forward Rock and Reach
Insert HH DVD clip of this exercise

9/21/2016
25
Multidirectional Repetitive MovementsRock and Reach
Sideways Rock and Reach
Video – Sideways Rock and Reach
Insert HH DVD clip of this exercise

9/21/2016
26
• Rolling
• Floor to Stand
• Getting in or out of bed
• Sit to stand
• Sit & reach
• Stand & reach
• Walk & reach
• Walk & turn
• Stand & turn
Functional Component TASKS
Functional Components – Patient DRIVEN!
Sit to stand BIG
Video - Sit to Stand
Insert HH DVD clip of this exercise
9/21/2016
27
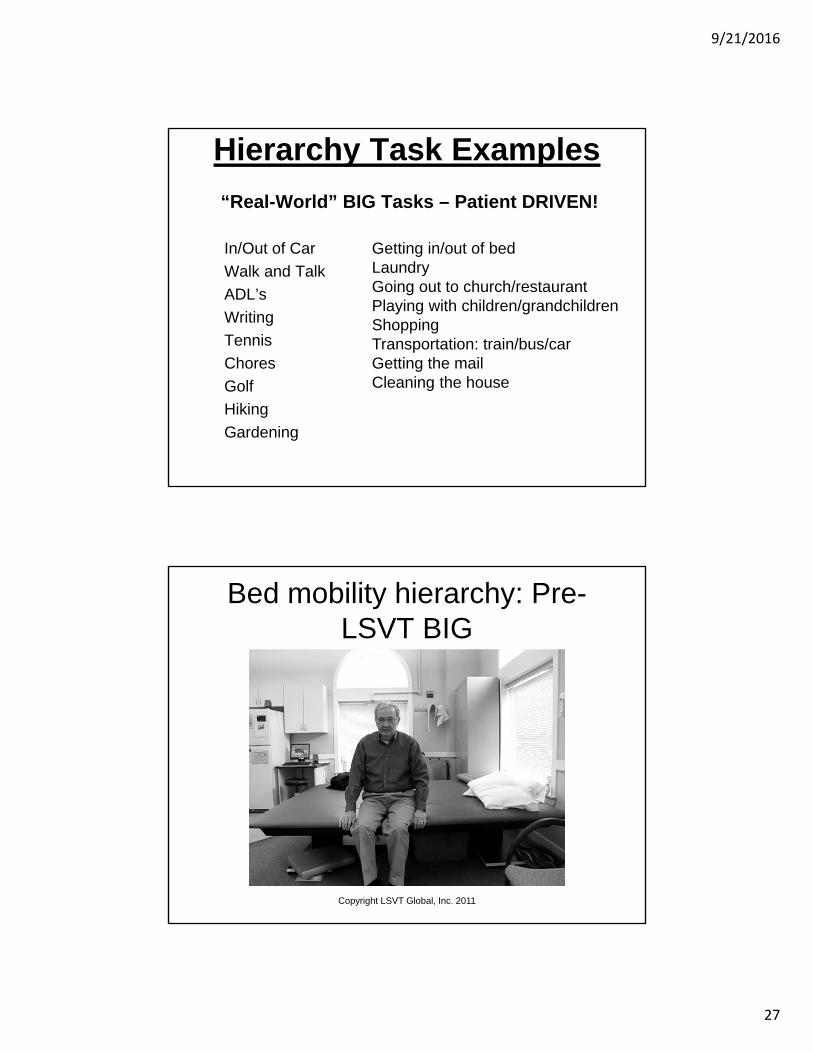
Hierarchy Task Examples
“Real-World” BIG Tasks – Patient DRIVEN!
In/Out of Car
Walk and Talk
ADL’s
Writing
Tennis
Chores
Golf
Hiking
Gardening
Getting in/out of bedLaundryGoing out to church/restaurantPlaying with children/grandchildrenShoppingTransportation: train/bus/carGetting the mailCleaning the house
Bed mobility hierarchy: Pre-LSVT BIG
Copyright LSVT Global, Inc. 2011

9/21/2016
28
Bed mobility hierarchy: Post-LSVT BIG
Copyright LSVT Global, Inc. 2011
LSVT BIG TREATMENT GOAL
People with Parkinson disease will use their bigger movements
“automatically” in everyday living –
and there will belong-term carryover
of increased amplitude use!

9/21/2016
29
The Bottom Line• Advances in neuroscience have provided
neurobiological and behavioral evidence supporting the positive impact of exercise-based protocols in
people with PD
• There is a rapidly growing literature in physical therapy/exercise protocols in humans with PD
• LSVT Programs have been developed and studied over the past 20 years
• LSVT BIG is one type of physical therapy program that has potential to offer improvements in movement
and quality of life for people with PD
LSVT BIG® and LSVT LOUD®
in the Home Health Setting:
BIG challenge or
BIG opportunity?

9/21/2016
30
Challenges• Patient complexity and
disease severity
• Coordination with other health care providers coming into the home
• Specific knowledge needed to support reimbursement and provision of LSVT BIG in the home
Opportunities• Evaluation of real world
function in context
• Training in context- BIG Walking, exercises, etc.
• Increased ease creating salient Functional Component Tasks, Hierarchies and Carryover Assignments
• Caregiver training in context
• Reduced “travel fatigue” for patient
LSVT BIG and Home Health• Traditional home health practice
– Medicare Part A covers skilled need in homebound patients with chronic conditions
– Typically later stage patients with complex medical history
• Outpatient in the home– Medicare Part B reimbursement for home and
community-based care
• ”House calls” -- cash-based practices– All stages of patients --– Done in privacy of home at client’s
convenience

9/21/2016
31
Implementation of Intensity
• Is it Reimbursable?
• Is it Practical and Feasible?
• Can patients with Advanced PD or frailty handle therapy 4x/week?
• Is it Applicable to Varied Practice Settings?
YES!
• Eminently reimbursable
– Patients make significant progress
– Medical necessity readily proven in PD
– People with progressive disease get better, even in advance PD!
– Real world experience with 1000+ patients

9/21/2016
32
Is it Reimbursable in Home Health?
YES!– Medicare Part A covers care for homebound
patients
• Jimmo vs. Sebelius– 2013 lawsuit in which resulted in Medicare
covering maintenance as long as skilled care is required.
– Easy to demonstrate LSVT BIG is skilled care
Practical and feasible • High rate of attendance and participation
• May require education of administration and scheduling changes
• Intensity within sessions scaled to patient’s capabilities
• Intensity and repetition across sessions needed even MORE with advanced PD/more complex presentation
9/21/2016
33
Applicable to varied practice settings
• Able to regulate intensity and adapt or progress movements according to patient abilities and safe parameters
• Successful implementation in home health, outpatient, skilled nursing facilities, private practice, etc.
• Can be provided by PT and OT together
LSVT BIG Across the Continuum
THEREFORE:
• LSVT BIG can be started by in-patient therapist
• Transferred to Home Care therapist
• Then to an Outpatient therapist as they improve.
Know your network!!

9/21/2016
34
Later Stage PD patients
• Home Health may be first and only setting
• Home Health LSVT BIG is still LSVT BIG…– Skilled care with first episodes and tune ups
– Basic ADL focus
– PT/OT split
– Caregiver focus
– Single focus on amplitude
LSVT BIG and Maintenance Care
• Marking G codes – Required by Medicare to differentiate patients
who receive skilled care for maintenance purposes
• Skilled home health: Remember that later stage PD patients are not necessarily maintenance patients!– Differentiated with G codes when training for
hand off to caregivers
– Focus on Function to meet Conditions of Participation!

9/21/2016
35
LSVT BIG and Skilled Home Health Documentation
• Starts with OASIS C1 comprehensive assessment
– Establishes “reasonable and necessary” using functional scores for M1800’s
– Establishes criteria for PT/OT collaborative delivery of LSVT BIG
• 2x4 week frequencies each for PT and OT delivering coordinated LSVT BIG protocol
LSVT BIG and Skilled Home Health Documentation
• Break down into Long Term Goals/Short Term Goals
• Focus on calibration improvements for functional tasks
• Focus on clear identification of patient goals and degree of disease self-management
• Focus on graded improvements in caregiver competency for advanced patients

9/21/2016
36
LSVT BIG and Skilled Home Health Outcomes
• LSVT BIG skill contributes to agency publicly reported outcomes and STAR ratings
• Clinical framework for reducing falls, meeting identified skilled need, improving publicly reported outcome ratings for agencies
Practical Tips for Implementation and
Documentation

9/21/2016
37
What is “Advanced” PD?Modified Hoehn and Yahr Scale
• STAGE 0 = No signs of disease.• STAGE 1 = Unilateral disease.• STAGE 1.5 = Unilateral plus axial involvement.• STAGE 2 = Bilateral disease, without impairment of balance.• STAGE 2.5 = Mild bilateral disease, with recovery on pull test.• STAGE 3 = Mild to moderate bilateral disease; some postural
instability; physically independent.• STAGE 4 = Severe disability; still able to walk or
stand unassisted. • STAGE 5 = Wheelchair bound or bedridden unless aided.
Goetz CG, Poewe W, Rascol O, et al. Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: status and recommendations. Mov Disord. 2004;19(9):1020-28.
Recommended Assessment Tools for Patients with
Advanced PD• PT: Berg, TUG, 10 meter Walk, ABC
• OT: PASS, MOCA or SLUMS, 9 Hole Peg
9/21/2016
38
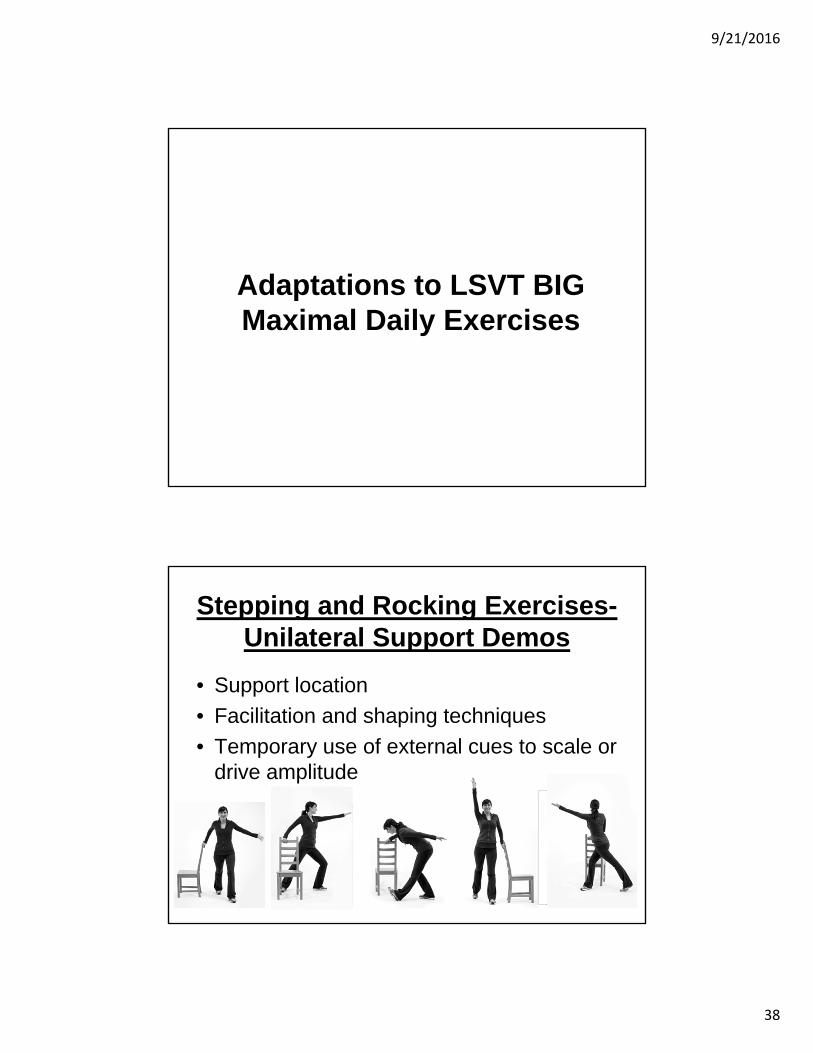
Adaptations to LSVT BIG Maximal Daily Exercises
Stepping and Rocking Exercises-Unilateral Support Demos
• Support location
• Facilitation and shaping techniques
• Temporary use of external cues to scale or drive amplitude
This image cannot currently be displayed.
This image cannot currently be displayed.
This image cannot currently be displayed.

9/21/2016
39
Stepping and Rocking Exercises-Seated Adaptations
Stepping and Rocking Exercises-Seated Adaptations

9/21/2016
40
LSVT BIG Exercises Adapted to Supine
SUSTAINED STEPPING ROCKING
LSVT BIG Exercises Adapted to Supine

9/21/2016
41
Case Example
Tony: H&Y Stage 4
• 82 y/o homebound male, retired, PD x 8 years, co-morbidities including HTN, atrial fibrillation, dementia, Stage II sacral decubitus ulcer, incontinence, hallucinations with Mirapex
• Lives in two story home, garage ramp, with devoted elderly wife with intermittent paid caregiver support
• Postural changes and skin breakdown as a result of disease progression (marked kyphosis, leaning left unless continually cued)
• Interests: Golf (riding golf cart, putting), dinner and socializing with large extended family

9/21/2016
42
Functional Component Tasks
1. Sit to Stand
2. Rolling BIG in Bed
3. Stepping BIG at toilet
4. Throwing off bedcovers BIG
5. Reaching for tissue BIG
Hierarchy: Bed Transfers• Week One: Blocked practice
• Week Two: Short sequences, primary caregiver providing cues, sheets vs. sheets plus comforter on bed, varied clothing (pajamas vs. daytime clothing)
• Week Three: longer sequence, primary and paid caregiver providing cues, varied lighting, varied weight of bedclothes eg. added blankets
• Week Four: whole sequence, environmental distractors (television, nearby conversations), internal distractors (urgency for toileting), time constraints, directing new caregiver

9/21/2016
43
Home Health Short Term Goals for Tony
• Short Term Goals– Patient will remove varied-weight bedcovers
using caregiver-cued BIG movements 50% of the time
– Patient will move supine to sidelying with caregiver-cued BIG movements with varied clothing/bed clothing, 50% of the time
– Patient will move sidelying to sitting with rail assist and caregiver-cued BIG movements 50% of the time
Home Health Long Term Goals for Tony
• Long Term Goals– Patient will complete safe transfer supine to
bed edge sit with single caregiver cue to initiate sequence for BIG rolling, and Standby Assistance for BIG sidelying to sit with rail support, 100% of the time
– Patient will independently provide verbal instruction to paid or novice caregiver for set up and positioning for successful completion of BIG transfer supine to bed edge sit 100% of the time
9/21/2016
44
Tony’s Outcomes
• Transfers supine to bed edge sit with single verbal cue, using rail assistance
• Able to instruct caregiver verbally and understandably in steps to sequence for BIG transfer supine to bed edge sit
Video Examples

9/21/2016
45
Side to Side in home
Sit to Stand In Home

9/21/2016
46
Big Walking In Home
Tips for Success When Implementing LSVT BIG
and LSVT LOUD Program

9/21/2016
47
Address Scheduling Challenges
• Challenge #1: Home Health visits may include vital sign and physical assessment, adding to total visit time
• Challenge #2: Management pressures to reduce weekly frequency to fit number of visits for maximizing reimbursement
• Challenge #3: Medical frailty/co-morbidities may affect plan of care and frequency due to missed visits
The LSVT BIG TEAM Approach!LSVT BIG Certified OT & COTAs
LSVT BIG Certified PTs & PTAs• PTAs or OTAs who are involved in the administration of LSVT BIG must
successfully complete an LSVT BIG Training and Certification Workshop. The PTA or OTA will not be able to deliver the treatment independent of a Certified LSVT BIG PT or OT.
• LSVT BIG Certified PTAs and OTAs may perform tasks as prescribed, directed, and supervised by an LSVT BIG certified PT or OT respectively.
• Assessment of the PTA’s or OTA’s skills with assigned tasks by the supervising PT or OT respectively should be an ongoing, integral element of supervision with frequent feedback provided.

9/21/2016
48
Teaming together with the LSVT LOUD certified SLP’s
• Cross refer- screen and educate
• Screen for need for tune-ups
• Support calibration- don’t let a soft voice slip by
• Understand what that person’s “best” healthy voice quality sounds like
• Educate on functional tasks (e.g. BIG posture or BIG walking) that could be reinforced by the LSVT LOUD clinician
Address Reimbursement Challenges
• Challenge #1: Non-Medicare plans require prior authorization
• Challenge #2: Clear documentation of homebound status required each visit, up to #16, to be 100% reimbursible
• Challenge #3: Skill documentation focusing on therapist actions in modeling, shaping, adding complexity required with functional outcome focus
• Challenge #4: Reimbursement for PT and/or OT requires OASIS functionals score = Medical Necessity

9/21/2016
49
Tune-Up Recommendations
• Establish frequency and number of visits based on assessment findings– Range: 0 -16 visits! Average 4-6 visits
– Continue to follow patients every 3-12 months• More Frequent (every 3-4 months): Atypical PD,
Cognitive Impairments, with changes to DBS
• Less frequent: IPD, Young, healthy, very motivated and adherent to HEP, good support, active
– Remember….PD is forever! You are an important partner on their journey!
Tune-ups are legitimate reimbursable “care” for people with degenerative diseases.
You should establish the tracking schedule for f/u prior to discharge
standard of care.

9/21/2016
50
General Documentation Reminders
– What is skilled?• Requires YOUR skill, instruction and intervention
as a therapist to achieve the goals.
• Could not have been done by lay persons or a care partners or by the patients themselves without you in the picture
– What is medically necessary?• Therapy required for improved safety, quality of life,
decreased disability, etc.
– Is there reasonable expectation of significant progress?
• How can you show that improvement?
Therapy and Homework Quantification Variables
Time to complete daily tasks; functional tasks # reps completed, with comments on your
shaping, assessing and modifying patient behavior
Step size Duration of sustained postures “reported functional improvements” HR average across a session/Borg effort Progression in hierarchies Changes in amount of cued vs. uncued trials
9/21/2016
51
Statements Supporting Reimbursement
• Mrs. P increased amplitude of upper extremity movements which enabled her to write lists and sign her name legibly on documents.
• Mr. G is now able to don his socks and shoes without his wife’s help or cueing and in less than 1 minute, by using increased amplitude and effort.
Marketing LSVT Programs

9/21/2016
52
LSVT BIG and LSVT LOUD Improve Outcomes...
LSVT BIG Reduces Fall Risk...

9/21/2016
53
In Summary• LSVT BIG and LSVT LOUD are adaptable
for patients at all stages of Parkinson’s Disease
• LSVT BIG and LSVT LOUD are applicable and practical for patients within the home setting using principles of intensity and single focus
• LSVT BIG and LSVT LOUD are reimbursable and important tools in developing comprehensive plans of care and improving publicly reported outcomes
“It is possible to take charge of your life, even with Parkinson’s.
It is possible for your will to override your brain.
It is possible to have Power Over Parkinson’s”
~Sharon KhaLSVT BIG and LSVT LOUD Graduate

9/21/2016
54
QUESTIONS??