the setting and use of occupational exposure limits
TRANSCRIPT

The Setting and Use ofOccupational Exposure LimitsCurrent practice

Contents
Foreword 1
Executive Summary 2
1. Current Perspectives on Occupational Exposure Limits 5
2. Use of Experimental and Human Studies in DerivingOccupational Exposure Limits 13
3. Measurement of Exposure 23
4. Risk Assessment 29
5. Setting and Using OELs 39
6. A Harmonized Approach 63
Annexes 67Annex 1Case Studies 68Annex 2Industry Proposal for Harmonization in Setting OELs 79
References 81Web publications 92
Notes 95
Acknowledgements 96

Mining and metals companies have a duty to protect the health of theirworkforce and the control of exposure to harmful materials is animportant part of this. Having consistent, internationally-recognizedOccupational Exposure Limits (OELs) that are based on sound science is a vital element for companies to provide the best protection for theirworkers.
ICMM members believe that harmonization of the way OELs are set andthe introduction of greater transparency in the process should be to thebenefit of everyone involved. Traditionally OELs have been set by variousgroups using a wide variety of available information – given thisbackground it is not surprising that there is considerable variation in the OELs in place. The result can be confusing for the companies andworkforces of an industry which operates internationally.
This publication presents current perspectives on the OEL setting processfrom the scientific review of health data, to risk acceptance criteria andthe consideration of socioeconomic factors. It is part of an ongoing ICMM project to develop an internationally harmonized approach, and anearlier draft of this publication was presented at a multi-stakeholderworkshop held in London in November 2005. (The report of the workshopis available as a separate ICMM publication).
For ICMM to achieve its goal of fostering a more harmonized approach, we recognize the need for dialogue and understanding among a widerange of stakeholders, companies and territories. Accordingly we wouldwelcome comment on this publication and on the broader initiative –details of which can be found on the ICMM website.
Paul MitchellPresident, ICMM
Foreword
The Setting and Use of Occupational Exposure Limits Current practice 1

The Setting and Use of Occupational Exposure Limits Current practice
The Institute of Environment and Health (formerlythe MRC Institute for Environment and Health) wascommissioned by the International Council onMining and Metals (ICMM) to prepare a drafttechnical position paper as a framework fordiscussion on how to advance the debate on aharmonized approach to setting occupationalexposure limits (OELs). The term OEL is a genericterm that refers to an occupational standard for theconcentration of a substance in workplace air. OELs may be defined in various ways, for example,as threshold limit values (TLVs), as developed bythe US American Conference of GovernmentalIndustrial Hygienists, or maximum exposure limitsor as time related airborne chemical concentrations,such as short-term exposure limits or ceilingvalues, among others.
While the document focuses, in particular, onmetals, metal compounds and other selectedsubstances of importance in the metals and miningindustries, the debate on harmonization of OELs isapplicable to all industrial chemicals.
The document serves as a working paper tosupport the objective of ICMM, which is to develop,a reasoned position, based on scientific,socioeconomic and technical considerations, inorder to influence and support movement towardsa common, global, harmonized approach to settingOELs, in the jurisdictions in which ICMM membercompanies operate. Harmonizing OELs is viewed,by ICMM, as an element in the promotion of asustainable and governance-based approach toreducing and minimizing the potential foroccupational diseases internationally. Furthermore,a harmonized approach to setting OELs wouldrepresent good business practice and wouldenhance equality for business operations acrossfirms and countries.
The ICMM goal is to develop a position on theharmonized approach to the review andestablishment of OELs that, while taking intoaccount the proportion of exposed workers that agiven limit should be expected to protect:• is based on a common definition of an OEL ;• is underpinned by evidence-based, best available
science;• is consistent in the application of risk assessment;• recognizes that any science-based value should
be achievable in terms of socioeconomic impacts and technical achievability; and
• is open and transparent to all stakeholders.
OELs to limit concentrations of substances inworkplace air have now been used for around acentury as a means of assessing and/or controllingworker exposure to a wide range of airbornesubstances (e.g. dusts, particles, aerosols, gases,vapours). These have included organic andinorganic substances and pharmaceuticals, andhave ranged from cotton dust, nicotine and coaldust, to specific chemicals such as chromic acidmist and vinyl chloride. OELs are not to beconfused with ambient air standards, which areused to protect the general population. OELs havebeen set on a wide variety of available informationand by various groups — some informalprofessional groups and some formalizedregulatory expert bodies. These groups haveevolved their own procedures and paradigms forrecommending limits, and their outputs may ormay not have been part of the national regulatoryframework. The information available on which tobase OELs has varied from a few informalobservations on worker health to a large publishedtoxicological and human-health database.
Given this background, it is not surprising that,worldwide, there has been a wide variation in thenumerical value of many OELs for the samesubstance, which has led to confusion and perhapsa lack of confidence, both among the socialpartners (industry and worker representatives),concerning health and cost implications, and alsoamong the regulators who have the responsibilityfor enforcement and assessment of industrycompliance.
Nonetheless, with industrial globalization, thevalue of harmonizing approaches to setting OELs isbecoming increasingly apparent. Harmonizationdoes not mean standardization; that is, it is not tobe expected that all jurisdictions should useidentical approaches and generate identicalstandards; rather, differences in approachesshould clearly reflect identifiable differences inscientific policy or scientific judgement, whichshould be communicated in a transparent manner.
Under national and international health and safetyregulations and guidelines, most employers,worldwide, are required to protect workers fromexposure to chemicals that may be harmful tohealth. Where health-based risk assessmentindicates workplace airborne exposure, appropriatecontrol measures may include consideration ofworker protection, which is usually provided by theutilization of OELs. This, in turn, promotes both
2
Executive Summary

The Setting and Use of Occupational Exposure Limits Current practice
Currently, there are no formally recognized,internationally agreed, harmonized methodologiesfor the development of OELs, although the generalprocedures and processes used would be broadlyagreeable to most standard-setting bodies.Recognizing that the development of OELs shouldbe based on best available science, reflect riskacceptance criteria and take account ofsocioeconomic consequences, technical feasibilityand the practicalities of measurement techniquesand assessing compliance, this document explores: • current perspectives on OELs across a range of
national and international organizations; • the use of data from experimental and human
studies in setting health-based OELs; • exposure measurement methodologies; • risk assessment methodologies; and• procedures for setting OELs in a number of
jurisdictions.
Reflecting the particular focus on metals andmining, several chemicals of particular relevancefor these industries are used as case studies within the report to illustrate some of the generalpoints made and explained herein. These are —nickel metal and nickel compounds, palladium and soluble palladium salts, lead, chromium andmanganese, as examples of metals important in the industry, and nitrogen dioxide, sulphurdioxide, sulphuric acid mists and crystalline silica.Metals provide a unique challenge when settingOELs as metal speciation (a variety of oxidationstates and of metal compounds) may affect healthimpact. Similarly, other parameters becomeimportant when considering gases, mists, andparticles of varying size and physical form, owing to deposition or absorption characteristics in therespiratory tract and the potential for acute orchronic effects. For each of the case studies,descriptions are given of measurement techniques,and comparisons are made of current OELs inselected countries and the procedures throughwhich they have been established.
Finally, a number of proposals are made forharmonization of approaches to setting OELs (seebelow). The goals of the ICMM (above) arediscussed — in particular the extent to which it isnecessary to establish a common definition of anOEL and the potential for doing so and also to whatextent numerical values for OELs can or should bemore standardized. The framework for aharmonized approach proposed herein sharesmany elements with proposals put forward byICMM member companies during the course of the
best practice in exposure control (e.g. by theimplementation of a hierarchy of control measures,from elimination of airborne exposure at source tosafe working practices and the use of personalprotective equipment) and the use of managementsystems to ensure compliance.
The primary objective in setting OELs is theprotection of workers from occupational illness ordisease, both locally, in the respiratory tract, andsystemically, by setting an occupational exposurelevel at which no adverse health effects can beanticipated, either in the short-term or during astandardized working lifetime. To this end OELsmay be set for both short-term exposures andlonger term, time-weighted average exposures. In addition to worker protection, OELs may be setfor the protection of the offspring of workers.Currently, the establishment of an OEL, generally,involves two phases. One phase, based on bestavailable science, is the development of either arecommended health-based limit, which is derivedfrom exposure–effect and exposure–response data,or, where a numerical health-based limit cannot beset (e.g. for compounds for which it is not possibleto identify a threshold for effects, such as genotoxiccarcinogens), a pragmatic numerical value basedon a risk assessment, a health statement or, forexample, a requirement to reduce levels as far asreasonably practicable. The other phase is thetranslation of a quantitative health-based limit intoa practical, operational limit. The second phasemay include several processes dealing with issuessuch as technical feasibility and economic factors.Thus, OELs may not always be simply health-basedlimits; pragmatism is often an essential element ofsetting an operational OEL. The differentapproaches to setting health-based limits, dealingwith non-threshold compounds and addressingpragmatic and operational issues that are adoptedby different jurisdictions are discussed in thereport.
3
The Setting and Use of Occupational Exposure Limits Current practice
present exercise. The ICMM proposals are annexedto this report.
The benefits of a harmonized approach includeincreased transparency about the uses andlimitations of an OEL, enhanced confidence in theprocess, pooling of resources across jurisdictionsand a clearer definition of protections for workers,globally. Essential in the derivation of an OEL isclear documentation of acceptable health risk froma scientific viewpoint and, where appropriate,transparent justification of the technological andsocioeconomic factors that may amend or refine afinal recommendation for an OEL.
A proposed framework for a harmonized approachto setting OELs is as follows.• Literature review of relevant scientific data
according to standardized criteria• Evaluation of literature review according to
standardized criteria• Selection of critical health endpoint(s)• Determination of whether critical effects are
threshold/non-threshold • Selection of key studies for OEL• Selection of point of departure• Selection of factors influencing uncertainty• Application of individual uncertainty factors to
each such influencing factor• Determination of composite uncertainty factor• Identification of non-scientific influences on
development of OEL• OEL• Discussion on the availability and accuracy of
sampling technology• Documentation and publication of all key steps,
above
Throughout this publication, in addition to thestandard references, electronic based resourcesare identified by red superscript numerals.Expanded descriptions including the relevant weblinks can be found in the web publications sectionon page 92.
4

Current Perspectives on Occupational Exposure Limits1.1 Introduction 61.2 Descriptions 8
1.2.1 Air limits 81.2.2 Biological limits 91.2.3 Occupational exposure limits in different jurisdictions 9
1.3 Other limit values 10

The Setting and Use of Occupational Exposure Limits Current practice
1.1 Introduction
This document has been prepared by the Instituteof Environment and Health (IEH) for theInternational Council on Mining and Metals (ICMM)in order both to provide a framework fordiscussions on a harmonized approach to settingoccupational exposure limits (OELs) and tofacilitate activities related to the development of acommon, global strategy to promote movementtowards such an approach. While the documentfocuses on metals and their compounds and otherselected substances of importance in the metalsand mining industries, the debate on harmonizationof OELs is applicable to all industrial chemicals.
The document supports an overall objective of theICMM, which is to develop, a reasoned position,based on scientific, socioeconomic and technicalconsiderations, in order to influence and supportmovement towards a common, global, harmonizedapproach to the review and establishment of OELs,in the jurisdictions in which ICMM membercompanies operate. This overall objective of ICMMis underpinned by the view that harmonization ofOELs is an important element in the promotion of a sustainable and governance-based approach toreducing and minimizing the potential foroccupational ill-health and disease. Furthermore, a harmonized approach to setting OELs wouldrepresent good business practice and wouldenhance equality for business operations acrossfirms and countries.
The goal is to develop a harmonized approach that,taking into account the proportion of exposedworkers that a given limit should be expected toprotect:• is based on a common definition of an OEL;• is underpinned by evidence-based, best available
science;• is consistent in the application of risk
assessment;• recognizes that any science-based value should
be achievable in terms of socioeconomic impacts and technical achievability; and
• is open and transparent to all stakeholders.
OELs to limit concentrations of substances inworkplace air have now been used since aroundthe turn of the 20th century. The first publishedreport on a permissible exposure level was forcarbon monoxide in Germany in 1883; otherexamples followed, including, in 1916, exposurelimits for dusts with high quartz content in South
African gold mines and, in 1921, the setting ofexposure limits, by the US Bureau of Mines, for 33substances encountered in the workplace (Cook,1986). Since then, OELs have been used as ameans of assessing and/or controlling workerexposure to a wide range of substances (e.g. dusts,particles, aerosols, gases, vapours). These haveincluded organic and inorganic substances andpharmaceuticals, and have ranged from cottondust, nicotine and coal dust, to specific chemicalssuch as chromic acid mist and vinyl chloride.
OELs are not to be confused with ambient airstandards, which are used to protect the generalpopulation. While OELs are derived to protectrelatively healthy workers during their workingcareer, environmental ambient air standardsprotect the weakest individuals (youngest, oldest,and physically compromised) 24 hours a day, everyday, for an average lifetime. Unlike some ambientair standards, exposure to levels at OELs will notnecessarily prevent discomfort or injury to all thoseexposed owing to wide ranges in individualsusceptibilities (Paustenbach, 2000).
OELs have been set on a wide variety of availableinformation and by various groups — someinformal professional groups and some formalizedregulatory expert bodies. These groups haveevolved their own procedures and paradigms forrecommending limits, and their outputs may ormay not have been part of the national regulatoryframework. The information available on which tobase OELs has varied from a few informalobservations on worker health to a large publishedtoxicological and human-health database.Furthermore, extensive national programs toupdate OELs across the world are not in place. The fact that some national OELs have not been re-reviewed in decades may be a factor that leads todifferences in numerical values between countries.
Given this background, it is not surprising that,worldwide, there has been a wide variation in thenumerical value of many OELs for the samesubstance, and this has led to confusion and,perhaps, a lack of confidence, both among thesocial partners (industry and workerrepresentatives), concerning health and costimplications, and also among the regulators whohave the responsibility for enforcement andassessment of industry compliance.
6
1. Current Perspectives onOccupational Exposure Limits

The Setting and Use of Occupational Exposure Limits Current practice
The objective in setting OELs is the protection ofworkers from occupational ill-health and disease,both locally, in the respiratory tract, andsystemically, by setting a highest occupationalexposure level at which no adverse health effectscan be anticipated in workers and their offspring.Currently, the establishment of an OEL, generally,involves two phases. One, phase, based on bestavailable science, is the development of arecommended health-based limit, which is derivedfrom exposure–effect and exposure–response data,or, where a health-based numerical limit cannot beset (e.g. for genotoxic carcinogens), a pragmaticnumerical value based on a risk assessment, ahealth statement or a requirement to minimizeexposure levels. The other phase is often thetranslation of a quantitative health-based limit intoa practical, operational limit. The second phasemay include several processes dealing with issuessuch as technical feasibility and economic factors.Thus, OELs may not always be simply health-basedlimits; pragmatism is often an essential element ofsetting an operational OEL.
While many organizations around the world developand use OELs, there are disparities in the OELvalues of different organizations and themethodologies use to derive them (Haber andMaier, 2002). This review seeks to identify thedifferences and similarities in the development anduse of OELs in different jurisdictions around theworld and to identify ways to make such standardsetting more harmonized and transparent.
Currently, there are no formally recognized,internationally agreed, harmonized methodologiesfor the development of OELs, although the generalprocedures and processes used would be broadlyagreeable to most standard-setting bodies.Recognizing that the development of OELs shouldbe based on best available science, reflect riskacceptance criteria and take account ofsocioeconomic consequences, technical feasibilityand the practicalities of measurement andassessing compliance, this document reviews: • current perspectives on OELs across a range of
national and international organizations (Section 1);
• the use of data from experimental and human studies in setting health-based OELs (Section 2);
• exposure measurement methodologies (Section 3);
• risk assessment methodologies (Section 4); and• procedures for setting OELs in a number of
jurisdictions (Section 5).
Reflecting a particular focus on the metals andmining industries, several chemicals of particularrelevance for these industries are used as casestudies within the report, to illustrate some of the general points made and explained herein.These are — nickel metal and nickel compounds,palladium and soluble palladium salts, lead,chromium and manganese, as examples of metalsimportant in the industry, and nitrogen dioxide,sulphur dioxide, sulphuric acid mists andcrystalline silica. For each of the case studies,descriptions are given of measurement techniques(Section 3.4), and comparisons are made of currentOELs in selected countries and the proceduresthrough which they have been established (Section5.7). Summaries of information underpinning thecase studies are given in Annex 1. The documentconcludes (Section 6) with a number of proposalsfor harmonization of approaches to setting OELs.Proposals put forward, separately, by ICMMmember companies can be found in Annex 2.
Metals and metal compounds and other chemicalsencountered during mining, production anddownstream uses cover a wide range ofsubstances, some of which can cause the totalspectrum of health outcomes, from minor irritationthrough to neurological illnesses and cancer; suchsubstances thus exemplify all the historical andregulatory issues that have been pertinent to theestablishment of OELs.
Owing to the scale of the task, preparation of thisdocument has relied strongly on review material.Recent reviews that have been cited include thoseby Haber and Maier (2002), which looks at some ofthe problems in setting air standards for metalsand mining related substances, the EuropeanUnion (EU) Scientific Committee on OccupationalExposure Limits (SCOEL; CEC 1999), whichdiscusses the methodology for the derivation ofOELs, and the UK Interdepartmental Group onHealth Risks from Chemicals (IGHRC) and itsforerunner (Risk Assessment and ToxicologySteering Committee, 1999a,b,c; IGHRC, 2003;2004), on approaches to risk assessment. A reviewby Paustenbach (2000) also provides a wealth ofbackground on the history and the biological basisfor OELs.
7

The Setting and Use of Occupational Exposure Limits Current practice
1.2 Descriptions
1.2.1 Air limits
There have been many descriptions of OELs, whichis the generic term now favoured by theInternational Labour Organization (ILO) and theWorld Health Organization (WHO) to describe arange of workplace air standards, many of whichhave very specific descriptions and are oftenrelated to regulatory or advisory frameworks.However, while recognizing potential pragmaticconstraints, whether these are set for regulatory orguidance purposes, they all generally adhere to thesame broadly accepted principle that OELs arelevels of substances in workplace air that arebelieved to be low enough to provide protection forworkers and their offspring from adverse effectsarising from breathing workplace air, even whenexposure is repeated on a regular basis over aworking lifetime (CEC, 1999).
Although countries such as the UK and Germanydeveloped some of the early air standards forworkplace control of some substances, it isgenerally accepted that the first country to developa systematic and comprehensive approach tosetting OELs was the USA. The AmericanConference of Governmental Industrial Hygienists(ACGIH; a professional organization of occupationalhygienists and other professionals fromuniversities or governmental institutions) firstpublished Maximum Allowable Concentrations(MACs) from 1946 (Stokinger, 1970; Stokinger,1981). These were later renamed TLVs. Similarapproaches were subsequently adopted by theDeutsche Forshungsgemeinschaft (DFG) inGermany (maximum workplace concentration,MAK, Maximale Arbeitsplatzkonzentrationen), theNetherlands and Scandinavia. The UK Health andSafety Executive (HSE) followed later with thesystem of maximum exposure limits (MELs) andoccupational exposure standards (OESs).
Although the two-OEL system in the UK hasrecently been replaced by a single OEL system ofworkplace exposure limits (WELs; HSE, 2005b), inwhich many of the existing MELs and OELs havebeen converted to WELs, for the purpose of thisreview, it has been more appropriate to refer to theformer MEL and OEL definitions, as it is for thesethat the documentation and supporting evidencefor UK OEL recommendations are available.
OELs to protect against ill health as a consequenceof long-term occupational exposures are usuallybased on the assumption that a worker can beexposed to a substance for a working life of 40years with 200 working days per year1, on the basisof a typical 8-hour (h) working day and a nominal40-h working week. Such an OEL is usually set asan 8-h time-weighted average (TWA; see alsoSection 3.3). OELs are set not just to protectworkers during their working lifetime but also toprotect them for the remainder of their lifetime andto protect their offspring. Short-term exposurelimits (STELs) may also be set for substances thatcause acute toxicity or to prevent adverse effectsthat may arise owing to peak exposures that arenot controlled by application of an 8-h TWA (CEC,1999). STELs are often set for 15 minutes (min).However some US Occupational Safety and HealthAdministration (OSHA) permissible exposure limits(PELs) have 30-min STELs; this also is the lengthof the TLV excursion limit.
Initially a major concern in setting OELs was thereduction of occupational exposure to chemicalsthat cause frank toxic effects, such ashepatotoxicity, neurotoxicity, nephrotoxicity, andcarcinogenicity. However, the majority of OELs, forexample the ACGIH TLVs and German MAKs, areactually set at levels intended to prevent sensoryirritation (Paustenbach, 2001), which may or maynot be the most sensitive endpoint.
Physicochemical and physiological characteristics,speciation and essentialityPhysicochemical properties will influence thedeposition and absorption characteristics of gases,mists and particles of varying size and form andwill therefore impact on the development of OELs.
A specific issue for metals is the setting of OELsfor different forms of the metal, which depends onthe degree to which speciation (different oxidationstates and the variety of metal compounds) affectstoxicological properties (Haber and Maier, 2002).Examples given in the case studies (Section 5.7 and Annex 1) include soluble nickel and palladiumsalts and different oxidation states of chromium.
While for many metals, toxic effects can occur athigh exposures, because many metals are‘essential’, insufficient intake can also lead toadverse health effects (Haber and Maier, 2002).Such considerations impact on the choice ofuncertainty factors in risk assessment (see Section
8

The Setting and Use of Occupational Exposure Limits Current practice
4.2). This special consideration does not occur formost other substances for which OELs are set.
1.2.2 Biological limits
Biological limits have developed into a number offorms, generally used for either exposure/uptakemonitoring (biological monitoring) or effectmonitoring (biological effect monitoring). Withbiological monitoring as an exposure measure, thechemical or the metabolite of the chemical ismeasured in a biological matrix such as urine,blood, or expired air, to estimate the uptake of thatchemical at a particular time; for example, themeasurement of cadmium in urine of cadmium-exposed workers. In biological effect monitoring, aneffect caused by the chemical or its metabolite onsome kind of biochemical or physiological functionin the body is measured; for example, reduction incholinesterase levels in plasma caused byexposure to organophosphorus pesticides.
Biological monitoring in general is to be seen as a complementary means of assessing workerexposure rather than an alternative to airmonitoring, as each provides different kinds ofinformation.
Broadly, two approaches to the derivation ofbiological limits are in use. Biological exposureindices (BEIs) are exemplified by the ACGIHapproach, in which the recommended BEI is based on the equivalent to the amount of that same chemical that would be taken into the bodyfrom exposure by inhalation to the current ACGIHOEL value over an 8-h period (ACGIH, 2003a). The other approach is the BiologischeArbeitsstofftoleranzwerte (biological tolerancevalue or BAT) used in Germany by the DFGCommission. These are said to be health-basedvalues; they are limits set on health effects andrepresent levels in the body at which no harm willoccur (DFG, 2004; DFG, 2005b). A similar approachis used in the UK for their Health Guidance Values,but in addition the UK HSE has also developed apragmatic Benchmark Guidance Value (BMGV),which is not health-based but is a practicalachievable level set at the 90th percentile ofavailable biological monitoring results, collectedfrom a representative sample of workplaces withgood occupational hygiene practices (HSE, 2002).
1.2.3 Occupational exposure limits in differentjurisdictions
There are relatively few bodies, worldwide, thatindependently set OELs; many jurisdictionssubstantially follow the methodology andguidelines from the EU SCOEL, German DFG, UKHSE, US ACGIH or US OSHA.
Descriptions of some national OELs aresummarized in Table 1.1. The processes fordeveloping and setting OELs in different countriesare described and compared in Section 5.2. The advisory or legal status of OELs in differentjurisdictions is indicated in the table. The status ofsuch limits may impact on the numerical value andapplication of the limit (also discussed further inSection 5).
Within the EU, competent national authorities orother relevant national institutions set OELs aslimits for concentrations of hazardous compoundsin workplace air. OELs for hazardous substancesrepresent an important tool for risk assessmentand management and valuable information foroccupational safety and health activities concerninghazardous substances1.
The US ACGIH TLVs are widely used both within andoutside the USA and have been adopted entirely indozens of countries. For example, the AustralianNational Occupational Health and SafetyCommission (NOHSC) initially adopted many of itsnational exposure standards (NESs) from theACGIH list of TLVs (NOHSC, 1999), as did the UKHSE until the early 1980s. However, within the USA,ACGIH TLVs are only recommendations and do nothave legal force1. The US OSHA sets regulatorylimits for the USA; these are published PELs, whichwere historically based on the ACGIH TLVs. Like theTLVs, PELs may include TWAs, action levels, ceilinglimits, STELs, excursion limits and in some casesBEIs1. The US National Institute for OccupationalSafety and Health (NIOSH) recommends, to OSHA,exposure levels that are protective to workers.These recommended exposure levels (RELs) haveno legal force; RELs also include TWAs, STELs,ceiling values and BEIs1.
9
1 The ACGIH policy statement on the use of TLVs is that they aredeveloped as guidelines to assist in the control of health hazards, andthat the recommendations or guidelines are intended for use in thepractice of industrial hygiene, to be interpreted and applied only by aperson trained in this discipline.

The Setting and Use of Occupational Exposure Limits Current practice
1.3 Other limit values
Apart from OELs to facilitate potential riskmanagement in the occupational environment,many other standards or maximum levels of achemical that should not be exceeded are relevantto risk management in the general population.Such standards or recommended maximum levelsmay be expressed, for example, as a concentrationof a chemical in a medium, such as air, water orfood, or may be expressed as an upper limit forhuman intake, such as amount ingested or inhaled.In the UK and elsewhere, some standards mayhave advisory status, such as soil guideline values,air or water quality standards or acceptable ortolerable daily intakes (ADIs and TDIs) for foodadditives and contaminants. Other standards, may,like OELs, be mandatory, for example standards forpesticides or veterinary residues in food stuffs(IGHRC, 2004).
10
The Setting and Use of Occupational Exposure Limits Current practice 11
Table 1.1: Occupational exposure limits in different jurisdictions
Continued over page
Country/Region
European Union(CEC, 1999)
Germany, Ausschlussfür Gafahrstoffe (AGS)
Germany(DFG, 2004)1
The Netherlands(Dutch ExpertCommittee onOccupational Standards,2000)
OEL
IOELVs (IndicativeOccupational Exposure LimitValues)
BLV (Binding Limit Value);risk of adverse health effectat specified levels when no-effect level cannot beidentified
TRK (TechnischeRichtkonzentrationen;technical guidanceconcentration)
MAK (MaximaleArbeitsplatzkonzentrationen,maximum concentration inworkplace); 8-h TWA
BAT (BiologischeArbeitsstofftoleranzwerte);biological tolerance value
MAC (Maximaal AanvaardeConcentraties, maximum airconcentration in workingarea); 8-h TWA and 15-minTWA
MAC-C (ceiling value)
Exposure–responserelationship only (genotoxiccarcinogens)
Regulatory/advisorystatus
Recommendation toMember States foradoption into nationallegislation
Common nationallegislation
Recommendations toAGS
Recommendations
Some legally binding,others administrativeand not legally binding
Specified exposurescenarios
Category 1, 2 or 3carcinogens;concentration inworkplace air that canbe reached using bestavailable technology
Substance-specificacceptable peakconcentrations anddurations defined; skinuptake indicated; MAK-values forcategory 3 and 4carcinogens for which aharmless minimumconcentration can bedetermined
Limits for substances inthe human body
In addition to OELs,special rules forindividual substances orsubstance groups suchas hydrocarbonmixtures, diesel engineemissions, or differenttypes of fibres and dust
No OEL for genotoxiccarcinogens
Workers protected(specified healthendpoints)
Healthy adults

The Setting and Use of Occupational Exposure Limits Current practice12
Table 1.1: Occupational exposure limits in different jurisdictions continued
* OES and MEL recently replaced by WEL (Workplace Exposure Limit)
Country/Region
UK(HSE, 2002)*
USA ACGIH(ACGIH, 2003a)1
USA NIOSH1
USA OSHA1
Australia(NOHSC, 1999)1
OEL
MEL (Maximum ExposureLimit); 8-h TWA or 15 minSTEL
OES (Occupational ExposureStandard); 8-h TWA or 15min STEL
BMGV (Biological MonitoringGuidance Value)
TLV (Threshold Limit Value)-TWA; 8-h TWA
TLV–STEL; 15-min TWA
TLV-C (ceiling)
REL (RecommendedExposure Level); TWA; STEL,ceiling value and BEI
PEL (Permissible ExposureLimit)
NES (National ExposureStandard) Airborne
Regulatory/advisorystatus
Legally enforceable
Legally enforceable
Non-statutory
No legal status in theUSA. May have legalstatus in other countries
No legal status in theUSA
No legal status in theUSA
No legal force,recommendations toOSHA
Regulatory; historicallybased on ACGIH TLVs
Advisory character,except where law, otherthan the NOHSC Act, orinstrument made undersuch a law, makes themmandatory; applicationof any NationalCommission documentin any particular Stateor Territory of Australiais prerogative of thatState or Territory
Specified exposurescenarios
Exposure reduced as farbelow level as possible;set for substances forwhich not possible todetermine NOAEL
Level to which exposureto be reduced; STEL,only, for substances, for which even briefexposure consideredcritical
Some OELs for multi-substance exposureprescribing processemissions like weldingfumes
Continuous exposurefor short period not tobe exceeded at any time
Concentration not to beexceeded any partworking day
Workers protected(specified healthendpoints)
(e.g. Carcinogensand asthmagens)
No indication of risk to health ofworkers exposed by inhalation dayafter day
Nearly all workers,day after day, forworking lifetime,without ill effect
(To protect fromirritation,chronic/irreversibletissue damage,narcosis)
Concentrations thatshould neitherimpair health norcause unduediscomfort tonearly all workers;(additionally, toguard againstnarcosis orirritation)2

Occupational Exposure Limits2.1 Experimental studies 14
2.1.1 Assessing study quality 142.1.2 General toxicity 142.1.3 Irritancy 162.1.4 Odour 162.1.5 Sensitization 162.1.6 Genotoxicity and cancer 162.1.7 Reproductive toxicity 18
2.2 Epidemiological studies and other studies in humans 182.2.1 Principles for using human studies in setting
occupational exposure limits 182.2.2 Exposure data in epidemiological studies 202.2.3 Data on sensory irritation 21
2.3 Mechanisms of toxicity 21

The Setting and Use of Occupational Exposure Limits Current practice
2.1.1 Assessing study quality
In the course of a toxicological review, many datafrom different sources and of different ages willneed to be considered. The OECD test guidelinesprovide a useful reference with which themethodology used to generate experimental datacan be compared, to judge their quality and validity.Although the guidelines do not provide a rigid studyprotocol, they can be used to make sure thatexperimental methodologies have includedimportant considerations, such as selection ofanimals, housing conditions, preparation ofanimals and doses, the number and sex of theanimals used, the dosage, administration,observations and pathological examinations (OECD,2000). The guidelines also give an indication of thefindings that the experimental report or publicationshould include. Deviations from the current OECDtest guideline do not render a study invalid, butthey should be scientifically justified. In addition, a lack of information does not mean that the studyis invalid, but rather that the validity cannot bejudged, so the results should be interpreted withcaution.
Another indication of the quality of a study iswhether it has been conducted to the OECDprinciples of Good Laboratory Practice (GLP), whichwere introduced in 1981. GLP embodies a set ofprinciples that provides a framework within whichlaboratory studies are planned, performed,monitored, recorded, reported and archived, andthe implementation of GLP compliance is verifiedby laboratory inspections and study audits. Moreinformation on GLP can be found on the OECDwebsite4.
Where studies have been conducted prior to OECDtest guideline adoption or GLP implementation,expert judgement is required to judge whether thestudies meet current standards and to what degreetheir outcome can contribute to the overalldatabase.
2.1.2 General toxicity
The most relevant information to set OELs derivesfrom 28- and 90-day inhalation studies. There areseveral OECD test guidelines to investigate thegeneral toxicity of a substance following short- orlong-term exposure. Table 2.1 summarizes theguidelines available and highlights those that relateto inhalation toxicity. The hazards of inhaledsubstances are influenced by inherent toxicity and
14
2. Use of Experimental and HumanStudies in Deriving OccupationalExposure Limits
Data from experimental and epidemiologicalstudies are used to derive health-based limits as afirst step in setting OELs (ECETOC, 1984). Whenavailable, data from human studies will generallybe preferred for the development of OELs; however,in the absence of human data or where such dataare few, experimental studies may be used as thebasis for developing OELs. Most organizationsdefine neither a minimal database nor a rigidhierarchy for selecting studies to be used inderiving OELs; instead a weight of evidenceapproach, which looks at all available data, isfrequently used (Haber and Maier, 2002).
2.1 Experimental studies
For many industrial chemicals, there is very littlehuman published data and thus a great reliancehas to be placed upon the available experimentalstudies. For many traditional chemicals, some ofthe studies available are quite old, going back tothe 1930s and 1940s, and they were oftenconducted to standards that would not be readilyacceptable now; therefore they have to beinterpreted with a great deal of caution.
The main source of widely accepted methodologiesfor in vitro and experimental animal toxicity testingis the Organization for Economic Co-operation andDevelopment (OECD) manual entitled ‘OECDGuidelines for the Testing of Chemicals’ (OECD,2000). The aim of the OECD guidelines is to makeavailable methodology, for each toxicity test, whichis sufficiently well defined to enable the tests to beconducted in a similar manner in differentlaboratories across the world, and to produceresults that will be acceptable to various regulatorybodies. By taking a harmonized approach it ishoped that wasteful duplication or repetition will beavoided. The OECD test guideline manual warnsthat when assessing the results of toxicologicaltesting on any chemical, the limitations of the testmust be borne in mind. Consideration must also begiven to the fact that extrapolations from animalsor in vitro test systems might not be accurate, andjudgement must be exercised as to whether aparticular method is suitable for testing thechemical in question, as the experimental designsare not designed to be appropriate to all chemicalsunder all exposure scenarios (OECD, 2000). Similarcriteria are described in the European CouncilDirective 67/548/EEC, with numerous updates3.

The Setting and Use of Occupational Exposure Limits Current practice
by physical factors such as volatility and particlesize. These studies and considerations areparticularly important for setting OELs. It is alsoimportant to consider the explosive potential of testsubstances, and care should be taken to avoidgenerating explosive concentrations, therefore thetest concentration might be limited for somesubstances. Other important information that thestudy report should include is the concentration ofthe test substance, which should be kept asconstant as possible, and where particles aregenerated, what the particle size distribution andconsistency of this distribution was. The pathologicalexamination following inhalation exposure shouldthoroughly investigate the tissues of the respiratorytract. It is also important to note whether theanimals were exposed nose-only, head-only orwhether their whole bodies were exposed to thetest substance, as this might influence the patternof effects observed (OECD, 2000).
Tests for general toxicity can be used to assess thepotential of a substance to cause a large number ofeffects. The OECD test guidelines generally
recommend that pathological examinations of allthe major tissues and organs be conducted, as wellas haematological examinations and clinicalbiochemistry determinations. Body weights, foodconsumption and visual assessment of generalcondition should all be recorded (OECD, 2000).Yanagida et al. (2005) have shown a relationshipbetween OELs and the lethal dose 50 (LD50) valuesof rats or mice for metals and metallic compounds.
In addition to the test guidelines for general toxicitydescribed above, there are several test guidelinesthat relate to neurotoxicity. Most of these have beenspecifically designed to investigate the propertiesof organophosphate compounds, but OECD testguideline 424 can be used for other compounds totest for neurotoxic properties in rodents. This testcan be combined with the repeated dose toxicitytests, or conducted alone. This guidelinespecifically addresses administration via the oralroute, but it is acknowledged that the guidelinecould be adapted to other routes, includinginhalation (OECD, 2000).
15
Table 2.1: Summary of studies used to investigate the general toxicity of a substance
Source: OECD (2000)
OECD test guideline number
401
402
403
407
408
409
410
411
412
413
420
423
425
433
434
452
453
Title of guideline
Acute oral toxicity
Acute dermal toxicity
Acute inhalation toxicity (recently updated)
Repeated Dose 28-Day Oral Toxicity Study in Rodents
Repeated Dose 90-Day Oral Toxicity Study in Rodents
Repeated Dose 90-Day Oral Toxicity Study in Non-Rodents
Repeated Dose Dermal Toxicity: 21/28-day Study
Sub-chronic Dermal Toxicity: 90-day Study
Repeated Dose Inhalation Toxicity: 28-day or 14-day Study
Sub-chronic Inhalation Toxicity: 90-day Study
Acute Oral Toxicity - Fixed Dose Method
Acute Oral toxicity - Acute Toxic Class Method
Acute Oral Toxicity: Up-and-Down Procedure
Acute inhalation toxicity – fixed dose procedure
Acute dermal toxicity – fixed dose procedure
Chronic Toxicity Studies
Combined Chronic Toxicity/Carcinogenicity Studies

The Setting and Use of Occupational Exposure Limits Current practice
2.1.4 Odour
There is no OECD test guideline for odour.
2.1.5 Sensitization
There are two OECD test guidelines to investigatethe potential for substances to cause skinsensitization: OECD test guideline 406 (skinsensitization) and OECD test guideline 429 (skinsensitization — the local lymph node assay; OECD,2000). Neither of these tests is suitable for testinggaseous or particulate materials. There is no OECDguideline on how to test for respiratory sensitizingpotential, which for gaseous/particulate substancesis of more concern than skin sensitization.
Methodologies, which are based on the results ofskin and eye irritation tests conducted inexperimental animals, are available for settingpreliminary OELs for sensory irritants, until humandata become available (Paustenbach, 2001).
2.1.6 Genotoxicity and cancer
There are many OECD test guidelines that relate tothe potential of a test substance to cause geneticdamage and two guidelines for cancer (see Table2.3). In general, the two guidelines for cancer canbe adapted to any route of exposure, includinginhalation. Of paramount importance to thesestudies is the identity of the test substance. It isessential that composition, including majorimpurities, and the stability of the test substancebe known before the study is initiated. OECD testguidelines 451 and 453 provide some detail oninhalation studies, as the technical problemsinvolved are complex. Long-term exposures areusually based on projected industrial experiences
16
2.1.3 Irritancy
There are several OECD test guidelines todetermine the irritating potential of substances(see Table 2.2). There are no guidelines to assessthe potential for respiratory irritation, but such aneffect is likely to be detected in the tests forgeneral toxicity (OECD, 2000).
In the interest of animal welfare, OECDrecommends that studies into irritation/corrosiveproperties should not be conducted if thesubstance has predictable corrosive activity (e.g.strong acid or alkaline) or is highly toxic via thedermal route or if the substance did not produceirritation in an acute dermal toxicity test up to adose of 2000 mg/kg bw. The duration of the testshould also be sufficient to evaluate thereversibility of any effects (OECD, 2000).
The OECD test guideline for dermal irritation doesnot specifically discuss how to deal with gaseous or particulate materials, because it is generallyaccepted that dermal irritation is not of concern for these substances. OECD test guideline 405 doesprovide guidance on how to administer substancesto the eye and how to estimate the dose.
A comprehensive review of nearly 300 chemicalstested using the American Society for Testing andMaterials (ASTM) mouse bioassay or somevariation of the assay found that the concentrationscapable of producing a 50% decrease in respiratoryrate (RD50) for SW, CF1 and OF1 strains of malemice all predict TLVs, on the same basis, that is0.03xRD50. The strongest correlation between TLVand RD50 was found in male SW mice. The use ofdifferent strains provides a range of sensitivities(Schaper, 1993).
Table 2.2: Summary of OECD test guidelines for irritancy and corrosion
Source: OECD (2000)
OECD test guideline number
404
405
435
430
431
Title of guideline
Acute Dermal Irritation/Corrosion
Acute Eye Irritation/Corrosion
In Vitro Membrane Barrier Test Method for Skin Corrosion (adopted 2004)
In Vitro Skin Corrosion: Transcutaneous Electrical Resistance Test (TER)
In Vitro Skin Corrosion: Human Skin Model Test

The Setting and Use of Occupational Exposure Limits Current practice
(animals dosed for 6 h/day, 5 days/week), orpossible environmental exposures (animals dosed22–24 h/day, 7 days/week). Therefore it isimportant that the exposure period and frequencyof dosing are taken into account when extrapolatingthe results to humans. As previously mentioned, itis important that the exposure concentration isconstant and that the particle size distribution ofthe solid or liquid aerosol is maintained throughouttreatment (OECD, 2000).
Since no single assay has proved capable ofdetecting mammalian mutagens and carcinogens,it is usual practice to apply the assays in ‘batteries’.There are various approaches, and batteriesgenerally comprise two to five tests, which includetests on prokaryotic and eukaryotic cells and coverthe major genetic changes possible. Selection ofthe tests is dependent upon the knowncharacteristic of the test material. As a generalrule though, in vitro tests for gene mutation andchromosomal aberrations are conducted, andwhere the results from either of these tests arepositive further in vivo testing is conducted.
For gaseous or particulate materials, for which themost likely route of exposure is inhalation, the invitro tests can be adapted by testing in sealedculture vessels (OECD, 2000). The OECD testguideline manual gives references for acceptedmethods for testing gaseous or volatile materialsfor each test. The test guidelines relating to in vivogenotoxicity tests generally note that, whereappropriate, the inhalation route may be used, butthey do not discuss any special considerations.However, it would be reasonable to assume thatthe points of discussion for general toxicity testingand carcinogenicity testing for inhaled materialsalso apply to in vivo genotoxicity testing.
17
Source: OECD (2000)
Table 2.3: Summary of OECD test guidelines for genotoxicity and carcinogenicity
OECD test guideline number
Cancer
402
403
471
Genotoxicity
473
474
475
476
477
478
479
480
481
482
483
484
485
486
Title of guideline
Carcinogenicity Studies
Combined Chronic Toxicity/Carcinogenicity Studies
Bacterial Reverse Mutation Test
In vitro Mammalian Chromosomal Aberration Test
Mammalian Erythrocyte Micronucleus Test
Mammalian Bone Marrow Chromosomal Aberration Test
In vitro Mammalian Cell Gene Mutation Test
Genetic Toxicology: Sex-Linked Recessive Lethal Test in Drosophila melanogaster
Genetic Toxicology: Rodent Dominant Lethal Test
Genetic Toxicology: In vitro Sister Chromatid Exchange Assay in Mammalian Cells
Genetic Toxicology: Saccharomyces cerevisiae, Gene Mutation Assay
Genetic Toxicology: Saacharomyces cerevisiae, Miotic Recombination Assay
Genetic Toxicology: DNA Damage and Repair, Unscheduled DNA Synthesis in Mammalian Cells in vitro
Mammalian Spermatogonial Chromosome Aberration Test
Genetic Toxicology: Mouse Spot Test
Genetic Toxicology: Mouse Heritable Translocation Assay
Unscheduled DNA Synthesis (UDS) Test with Mammalian Liver Cells in vivo

The Setting and Use of Occupational Exposure Limits Current practice
identified. Case-control, historical cohort orlongitudinal prospective studies are the onlysatisfactory way to investigate long-term effects inhumans and provide sufficient evidence for riskassessment and development of OELs, as long asexposure is well characterized and potential biasesand confounders are well controlled (CEC, 1999;see also below).
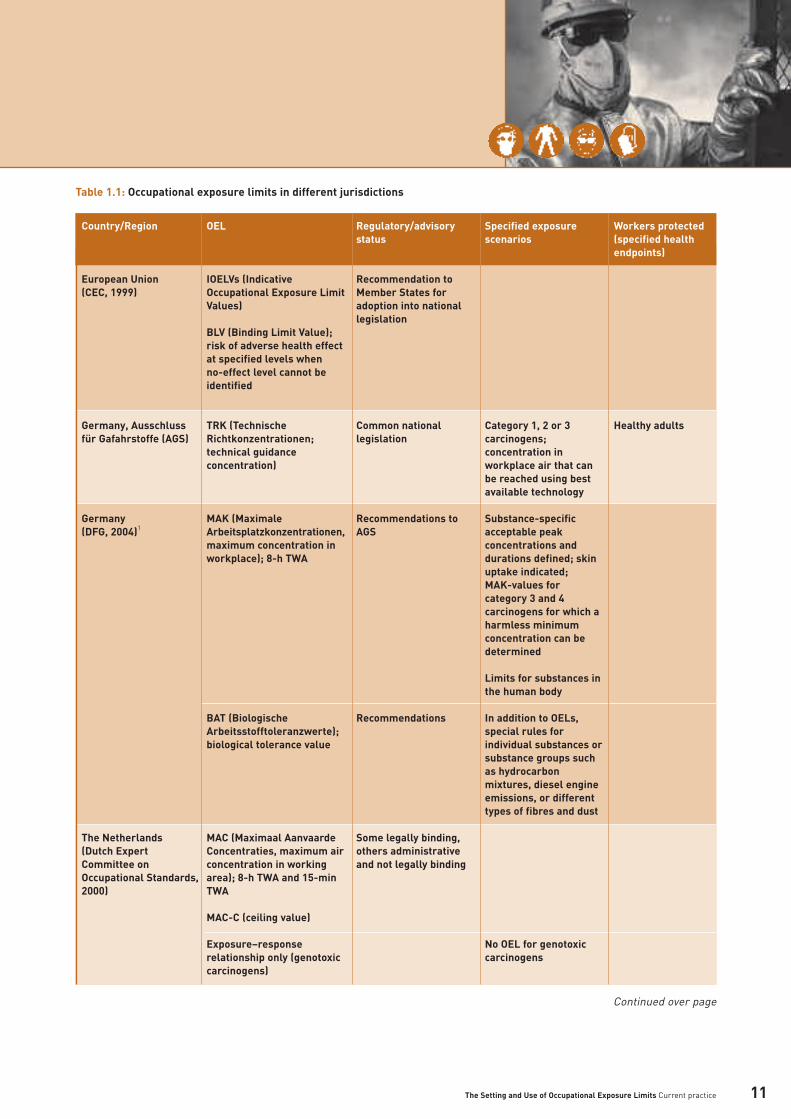
Guidelines on the use of epidemiological evidencein environmental health risk assessment have beenproduced by WHO (2000). The guidelines focus onthe use of epidemiological data for two distinctactivities — health hazard characterization, that is the identification of environmental hazards by the collection, evaluation and interpretation ofepidemiological and other evidence on anassociation between an environmental factor andhuman health; and health impact assessment,taken to mean the quantification of an expectedhealth burden related to an exposure in a particularpopulation. Some of the key guidance issummarized in Table 2.5.
A further initiative to develop reporting guidelinesfor observational epidemiological studies, includingcase–control, cohort, and cross-sectional studies— STandards of Reporting of OBservational studiesin Epidemiology (STROBE)5 — has recently beenestablished.
In interpreting epidemiological studies, accountmust be taken of bias, confounding and chance.Bias is caused by factors in the study that leaderroneously to a stronger or weaker associationbetween exposure and effect than actually exists;confounding occurs when there is an associationbetween the supposed causal factor that is underinvestigation and another factor that is alsoassociated with the endpoint under investigation.
18
2.1.7 Reproductive toxicity
There are several OECD test guidelines toinvestigate the potential for a substance to causereproductive or developmental effects (see Table2.4). The guidelines largely describe testing via theoral route of exposure, but also acknowledge thatfor some substances inhalation is more appropriateand that the test can be modified accordingly.Whatever the route of exposure, dosing shouldoccur at the same time each day (OECD, 2000).Although the OECD test guidelines do not discussissues specific to dosing via inhalation, it would bereasonable to assume that the points of discussionfor general toxicity testing also apply toreproductive and developmental toxicity testing.
2.2 Epidemiological studies and other studies inhumans
2.2.1 Principles for using human studies in settingoccupational exposure limits
Good quality epidemiology studies coupled withgood exposure assessments can yield the bestinformation for setting OELs for potential chronichealth effects, and for this reason good qualityhuman data, in particular, are preferred to animaldata for human health risk assessments. With theexception of volunteer studies, which mainlyaddress acute effects, exposure characterization inhuman studies is often limited and dose-responserelationships are rarely demonstrated. Suchconsiderations may limit the weight given to humanstudies in establishing OELs. While case-reportscannot, alone, provide a basis for establishing anOEL, they can be useful in indicating a relationshipbetween exposure and effect that merits furtherinvestigation, as can cross-sectional studies. Well-conducted volunteer studies can be usefulwhen a key adverse effect has already been
Table 2.4: Summary of OECD test guidelines for reproductive and developmental toxicity
Source: OECD (2000)
OECD test guideline number
414
415
416
421
422
Title of guideline
Prenatal Developmental Toxicity Study
One-Generation Reproduction Toxicity Study
Two-Generation Reproduction Toxicity Study
Reproduction/Developmental Toxicity Screening Test
Combined Repeated Dose Toxicity Study with the Reproduction/Developmental Toxicity Screening Test
The Setting and Use of Occupational Exposure Limits Current practice 19
Source: WHO (2000)
Table 2.5: Recommendations for use of epidemiological studies in health risk assessment
General
Precise description of exposure characteristics, exposure–response function
Distinguish acute from chronic effects of exposure
Health hazard characterization
Systematic review of evidence according to predefined protocol
• specification of questions to be addressed• justification for expertise of expert group assessing data• specification of methods for identifying relevant studies
Identification of relevant studies
• criteria for bibliographic searches • other search methods• use of publicly available / unpublished data
Assessment of validity of epidemiological studies
• evidence for strength of association (temporality, biological plausibility, coherence, consistency, specificity)• characterization of exposure–response• alternative explanations (chance, bias, confounding) • sensitivity analysis
Use of meta-analysis
• inclusive rather than exclusive• use of quality scores not recommended• account for publication bias• quantitative summary estimates (aggregative meta-analysis)
Drawing conclusions
• expert judgement• weighting of studies• contribution of non-epidemiological evidence to overall judgement• move to standardization of scales for weight of evidence
Health impact assessment
Protocol
• purpose of assessment• quantification of uncertainty• exposure metric (temporal and compositional, as required)• separate impact assessment for each of multiple health outcomes• well-defined process to derive exposure–response function, quality of exposure measurement, consistency of exposure
metrics across studies• baseline frequency of health outcomes• estimate population attributable cases
Interpretation
• assumptions and limitations• impact of uncertainty of findings

The Setting and Use of Occupational Exposure Limits Current practice
Such factors can be minimized or accounted for instudy design and analysis.
However, Pocock et al. (2004), in their review of asample of 73 epidemiological studies in generalpopulations, published since 2001 (37 cohort, 25case–control, 10 cross-sectional, 1 case–cohort),report some limitations in conduct and analysis of epidemiological studies. For example, while 67 articles included statistical adjustments forpotential confounders, few explained the choice of confounding variables. Furthermore, while 43studies performed subgroup analyses, interactiontests were rare (reported in 8 articles) and somestudies investigated multiple associations betweenexposure and outcome, increasing the likelihood offalse positive results. The authors also reportedevidence of publication bias. Some of the keyconclusions from the study are summarized inTable 2.6.
Epidemiology in the occupational setting has itsown peculiarities, which can both strengthen andweaken the possibility for drawing conclusionsabout causal relationships. These can includecontaminant exposure to a range of hazardoussubstances other than the one for which an answeris being sought and the potential loss of illemployees (caused by the substance of interest) in cross-sectional studies. In the first case, the
results may be complicated by confounders and inthe latter by an under-reporting bias.
Epidemiological data need to be evaluated carefullyto determine whether they are sufficient toestablish causality; criteria for judging causality arewell recognized (e.g. WHO, 2000). Sometimes, whilefew data for epidemiological or monitoring studiesare available in the published literature, ‘grey’literature, such as company records, may provideuseful information. However, developing OELs onthe basis of such data has the disadvantage of lackof transparency. If such data are to be used, itwould be helpful if they could be made openlyavailable in some form, for example in a supportingcriteria document, as was the case in a recentCriteria Document on manganese (IEH, 2004).
2.2.2 Exposure data in epidemiological studies
The goals of exposure assessment in occupationalepidemiology are to determine estimates of meanexposures for an occupational group and todetermine the homogeneity of exposure within andbetween the group (Rappaport, 1991b). Guidelinesfor good exposure assessment practice have beenput forward by IGHRC (2004).
Estimation of exposure is often made usingcategorical descriptors, based on job title and
20
Table 2.6: Recommendations for design and reporting of epidemiological studies
Source: Pocock et al. (2004)
Information on exclusion/refusals
Assessment of quality of data collected
Adequate size of study and power calculations
Rationale for categorizing quantitative exposure variables
Statistical cut off points not to be over interpreted
Rationale for selection and adjustment of potential confounders
Appropriate methods and interaction tests for subgroup analyzes — not to be over interpreted
Risk of false positives from multiple associations

The Setting and Use of Occupational Exposure Limits Current practice
duration of exposure; such procedures areparticularly used in retrospective exposureassessment. However, such estimates may havelimited value (Rappaport, 1991b). An analysis byRappaport et al. (1993) of 183 homogenousexposure groups (HEG; i.e. groups defined by jobtitle, location and other features of workenvironment, also described as similar exposuregroups (SEGs) or job exposure groups (JEGs))showed that only 20% of the HEGs were uniformlyexposed, while a similar proportion showed highvariation between workers.
An example of exposure reconstruction is thatconducted for several chromium (VI)-exposedoccupational cohorts in Ohio, USA. Historicalexposure information was often incomplete,qualitative or could not be defined on a worker-specific basis. Although exposure data were morerobust for later cohorts, such cohorts lackedsufficient latency for observations of any possibleincreased cancer risk. Exposure reconstructioninvolved exhaustive review of historical hygienerecords, reconstruction of worker histories,reconstruction of job titles over time andidentification of JEG areas, which were used torelate air-monitoring locations to job titles. TWA airborne exposures were calculated on thebasis of variability of airborne concentrations inJEG areas during an 8-h shift and expectedmovement of workers, by job title, through theplant (Proctor et al., 2004).
In their review of recently publishedepidemiological studies, Pocock and colleagues(2004) noted that, while in most studies (50/73),exposures were quantitative, they were usuallygrouped in ordered categories (42 articles) ratherthan analyzed as a continual variable. Yet fewarticles (22) gave the rationale for the choice ofcategories.
2.2.3 Data on sensory irritation
Many, if not most, airborne substances are able toproduce irritation to the nose and eyes and upperrespiratory tract at some concentration. Sensoryirritation (including perception of unpleasantodours) is a single exposure, thresholdphenomenon, which is mediated by damage ornervous stimulation via the vagus or trigeminalnerves. In some cases, it is hard to distinguishbetween irritation and unpleasant odour. Humandata on such effects are normally derived fromvolunteer or workplace studies. In many cases
OELs have been based on such irritant effects andoften there is a debate about whether these aretruly harmful or simply objectionable effects.(Paustenbach, 2001; Dalton, 2001; Meldrum, 2001).
2.3 Mechanisms of toxicity
Consideration of how mechanisms ofcarcinogenesis can be used in risk assessment(e.g. from IARC, 1992a) can give some insights intohow toxic mechanistic data might impact on riskassessment more generally.
Increased understanding of the critical biologicaleffects of carcinogenesis (or other toxicities) allowsthe possibility of using data from studies onputative intermediate effects or correlatedendpoints in the assessment of the risk of exposureto some specified substances.
Advances in technology and in understanding ofbiological and chemical processes have led toincreasing development and acceptance of testmethods based on mechanistic understanding(Blaauboer, 2003), such as molecular biology, cell-culture techniques, neurophysiologicalmeasurements, and proteomics, genomics andmetabolomics.
Molecular biological techniques can be increasinglyused in human biological monitoring studies tomeasure internal dose and help elucidateintermediate steps leading to toxicity and may havean increasing part to play in molecularepidemiology studies. For example, if it werepossible to measure, in humans, the occurrence ofsome intermediate effect, such as the occurrenceof a specific genetic mutation that is known to be aprerequisite for cancer occurrence, thenepidemiological studies with this effect as anoutcome could rapidly provide data for carcinogenicrisk assessment. As well as improving exposuremeasurement and detecting early biological effectsbelieved to form part of the toxicological process,molecular epidemiology studies can help in theelucidation of sources of interindividual variability,for example metabolic polymorphisms in humans.However, as noted by the International Agency forResearch on Cancer (IARC, 1992a), caution isneeded in interpreting studies on early biologicaleffects, as the use of biomarkers for early effectsdepends on knowledge about the significance of theeffect as a predictor of subsequent risk of cancer inhumans; this limits the use of such studies forcancer risk assessment.
21

The Setting and Use of Occupational Exposure Limits Current practice
Where, especially in the absence of good qualitydata from human studies, data from studies inexperimental animals are key to risk assessmentand subsequent development of OELs, evidenceabout whether an identified mechanism of toxicityin animals does or does not operate in humans isparticularly important.
As an example of the increasingly important role ofmechanistic considerations, IARC may now,exceptionally, classify agents as carcinogenic tohumans, even if the evidence for carcinogenicity inhumans is less than sufficient, if there is sufficientevidence of carcinogenicity in experimental animalsand strong evidence in exposed humans that theagent acts on a relevant mechanism ofcarcinogenesis. Conversely an agent may,exceptionally, be considered as not classifiable asto its carcinogenicity to humans despite sufficientevidence of carcinogenicity in experimental animalsif there is strong evidence that the mechanism ofcarcinogenicity in animals does not operate inhumans (IARC, 1992a).
22

Measurement of Exposure3.1 Estimating exposure 243.2 Quality of exposure measures 243.3 Short-term and long-term measures of exposure 253.4 Dose metrics 263.5 Measurement techniques 26

The Setting and Use of Occupational Exposure Limits Current practice
3.1 Estimating exposure
Good exposure assessment practice is necessaryfor effective assessment and management ofhealth risks from chemicals and for effectivemonitoring, control and enforcement of regulatorystandards. Aspects to be considered in exposureassessment include the sources and pathways ofexposure, the magnitude, duration and frequency ofexposure and population variability. Since thedegree of exposure may vary with time, the periodover which an exposure estimate is based cangreatly influence the result (IGHRC, 2004). With afocus on the concept of SEGs, Mulhausen andDamiano (1998) provide detail on basic exposurecharacterization, qualitative and quantitative riskassessment and priority setting, monitoring,interpretation and decision making,recommendations and reporting.
While traditional exposure assessment practiceshave assumed that exposure is uniform within aparticular job, exposure assessment should,ideally, take into account both within- and between-individual variability in exposure (Rappaport, 1991b;Symanski and Rappaport, 1994). Statisticalapproaches can be used to deal with variation inexposure within and between workers in a givenoccupational group (Rappaport et al., 1995). It hasbeen suggested that a statistical sampling strategy,designed to minimize variability in exposureassessment, should ideally begin with a randomsampling design, using a sufficient number ofworkers over a sufficient period of time to accountfor job rotation and the full range of possibleexposure and should allow for changes made to theproduction process or to the workforce, byconducting analyzes before and after any period ofchange; furthermore a sampling program shouldnot be restricted to particular times or phases ofthe production process (Symanski and Rappaport,1994). Weaver et al. (2001) have developed astatistical method to extend assessment ofworkplace exposures on a group-by-group basis toallow for simultaneous assessment of exposures,relative to some prescribed OEL, for multiplegroups within the same industry.
Assessing a worst-case scenario is a useful devicewhen a combination of low probability events mayhave a serious adverse impact. The worst-casescenario usually refers to a hypothetical situation in which everything that can plausibly happen tomaximize exposure does happen. Such anapproach usually overestimates exposure in aspecific situation. Reasonable worst-casescenarios may be applicable in occupationalsettings in order to define high-end exposures thatdo not exceed the maximum exposure that mightrealistically be likely to occur (IGHRC, 2004).
3.2 Quality of exposure measures
Those who provide exposure data are often remotefrom those who are responsible for its interpretationin an epidemiological study or exposure or riskcharacterization. Communication is important, as approaches used for making exposuremeasurements or estimates, assumptions madeand errors introduced can have a substantialimpact on the interpretation of the results (IGHRC,2004). As an example, exposure-monitoring datamay have been collected for compliance purposes,in which case, the worst-case rather than typicalexposure might have been sampled.
It is rare for ‘raw’ exposure data to appear in thepublished literature, and for the most partsummarized data are reported. Statistical analysisof exposure measurement data can producesummary measures, such as means, medians,percentiles and estimates of variability. Statisticalanalysis may highlight data gaps and unusualvalues or outliers (Mulhausen and Damiano, 1998;IGHRC, 2004).
It is now generally accepted that most exposuremeasurement data tend to fit a log normaldistribution, characterized by the geometric meanand geometric standard deviation. However, thearithmetic mean, as estimated by the samplemean, has been shown to be appropriate for anestimate of long-term exposure (Smith, 1987;Rappaport, 1991a,b). Any exposure assessment willbe subject to some degree of uncertainty, owing tolack of knowledge about factors that affectexposure, leading, potentially, to inaccurate orbiased estimates. Uncertainty analysis can beundertaken to help the end-user reach areasonable judgement about the validity of theexposure estimate (IGHRC, 2004).
24
3. Measurement of Exposure

The Setting and Use of Occupational Exposure Limits Current practice
It is generally recognized that better exposure data need to be reported. It might be generallyacceptable to present raw data on a web site, towhich a primary published article could makereference and which researchers and regulatorscould consult. A number of national occupationalexposure databases do exist that attempt to makesuch data available.
3.3 Short-term and long-term measures ofexposure
In many situations, exposures may be continuousbut fluctuate in level, as may be the case, forexample, at various stages during an industrialprocess. Many acute harmful effects, such asirritancy or pre-narcosis, are related to short-termpeaks in exposure. It is therefore important tomeasure short-term peaks, which might be missedin longer-term sampling undertaken to estimateaverage exposure. In the occupational setting,direct reading instruments can measure peaks forperiods as short as 15 seconds (IGHRC, 2004) orless (e.g. carbon monoxide can be measured in 1–3 second intervals).
Where onset of ill health is a consequence of long-term exposures to chemicals or mixtures ofchemicals, the more relevant and accessiblemeasure for exposure assessment is an exposureaveraged over a prolonged period of time. In anoccupational setting an 8-h TWA limit is asurrogate for a working lifetime, up to 40 years at 8 h/day, 5days/week, 52 weeks/year (IGHRC, 2004).However, there are many occupational scenarios,including many in mining and mineral processing,where such a week is rarely, if ever worked;instead shifts may last up to 12 h. In suchcircumstances OELs may need to be adjusted, if theworking week is different to a standard 40-h week(Brief and Scala, 1975; Hickey and Reist, 1977;Paustenbach, 1985).
While it is usually the case that the frequency ofpeak exposures is correlated with the long-termmean exposure, the frequency of peak exposuresover time may, in itself, be important for chronichealth effects. It has been suggested, for example,that a series of high intermittent peaks may causegreater damage than the same total dose receivedon a steady-sate basis over the same period oftime (IGHRC, 2004). ACGIH TLVs address this withthe application of excursion limit values. In theabsence of established STELs or ceiling values, an
8-h TWA is multiplied by 3 for an excursion limitvalue of 30 minutes and multiplied by 5 as asurrogate ceiling value (ACGIH, 2003a).
In contrast, in the case of exposure to organiccompounds that require metabolism to causetoxicity, it could be argued that peak exposuresmight reduce long-term risk, owing to saturation ofmetabolism. Indeed, physiologically basedtoxicokinetic modelling has demonstrated thatlong-term doses of metabolites of benzene,perchoroethylene and acrylonitrile resulting fromhighly variable exposures are marginally lower thanthose arising from constant exposure (Rappaport etal., 2005).
Nonetheless, notwithstanding potential impacts ofpeak exposures, Rappaport (1991b) has proposedthat cumulative exposure should be a validpredictor of damage, as long as rates of eliminationand repair are first order; even where this is notthe case, he proposes that damage is unlikely to beaffected by peak exposures as long as the meanexposure in less than 1/4–1/8 of that which givesrise to the threshold burden of damage. However, itshould be noted that the above arguments, whichreally relate to dose-delivery of active metabolite totarget tissue, may not apply so well to respiratorysensitizers, where there is some anecdotalevidence that induction of sensitivity is morerelated to effects from a number of high peakexposures than to lower steady state exposure.
Ulfvarson (1987) proposed three approaches tosetting better standards for the assessment ofconcentration peaks, as follows. For fast-actingsubstances (effect in less than 1 h) only ceilinglimits should be set. When structure analogy isjustified for narcotic and irritating gases, limitsshould be set at the same thermodynamic activity(relative saturation) rather than at the sameconcentration. TWA limits are appropriate forslowly absorbed and eliminated substances (hoursor more) but the possibility of total body burden, as an outcome of bioaccumulation, should beconsidered.
25

The Setting and Use of Occupational Exposure Limits Current practice
3.4 Dose metrics
Depending on the nature of the chemical, certainkinds of dose (e.g. short-term, long-term,inhalable, respirable, soluble, insoluble, etc.)dictate the likelihood of disease.
In the case of beryllium, for example, prevention ofsensitization appears to be critical (see Section4.2.5); it is plausible that even stringent OELs mayhave little effect on disease, yet particle size andsolubility also appear to have a substantial impact.Thus a complex set of OELs, varying with particlecount, dust fraction and solubility, might be the wayforward (Paustenbach et al., 2001). Such thinkinghas been more recently reinforced with argumentsthat, for poorly soluble inert particles of lowtoxicity, most of the early increases in inflammatorymarkers in the lungs of experimental animals aremore closely related to particle size than to particlemass.
For dioxin, for example, an OEL that protectsagainst the putative chronic toxic effects shouldalso provide an ample margin of safety to preventchloracne following repeated, acute exposure(Leung et al., 1988). As another example, the UKguideline for asbestos is based on a cumulativeaction level in combination with short-term controllimits (HSE, 2001).
Generally, for irritants, it is the short-term limitsthat are needed; for systemic toxicants the 8-hTWA is more appropriate.
However, in the end, a balance will have to bestruck between setting and measuring exposuresthat are most closely related to the health effect ofconcern and having overly complex monitoring andmeasurement techniques that become prohibitiveand too difficult to use in the workplace.
3.5 Measurement techniques
Where and how exposure measurements are madecan have a major bearing on the results obtained.Direct methods of measurement monitor theexposure at the environment/person interface atthe moment it occurs. Such methods may be usedfor checking compliance. In occupationalmonitoring, where the source is already known,personal monitoring (within the breathing zone) is the generally accepted method. While staticmonitoring can be carried out anywhere in theworkplace and can be useful to identify emissionsources and check effectiveness of controls, OELsrelate directly to personal exposure and socompliance testing should continue to rely onpersonal monitoring (IGHRC, 2004).
In the occupational environment, many exposuresmay be to industrial dusts. As most industrial dustscontain particles of a wide range of sizes, theconcentrations of dusts in different size fractionsare important. When particle size selectivepersonal monitoring methods are utilized, the sizefractions most commonly measured are theinhalable (<100 µm) and the respirable (<10 µm)fractions (IGHRC, 2004). Particle size selection isvery much dependent on the sample lead and flowrate used. A number of national and internationaldocuments give guidance on the measurement ofconcentrations of inhalable and respirable dusts inair, for the purpose of monitoring workplaceexposure (e.g. ISO, 1995; HSE, 2000). ISO 7708 (ISO,1995) defines sampling conventions for the inhalable,thoracic and respirable fractions and methods forestimating extrathoracic and tracheobronchialconventions. Aerosols should be collected usingequipment that complies with such standards, whilerecognizing, as in ISO 7708, that it is only possible tomake a statement of probability that an instrument’scharacteristic falls within a certain range.
The ACGIH recommends particle size-selectiveTLVs (PSS-TLVs; ACGIH, 2003a). Three PSS–TLVsare defined as:• inhalable particle mass TLVs (IPM–TLVs) for
materials that are hazardous when deposited anywhere in the respiratory tract
• thoracic particulate mass TLVs (TPM–TLVs) for materials that are hazardous when deposited anywhere within the lung airways and the gas-exchange regions
• respirable particulate mass TLVs (RPM–TLVs) for materials that are hazardous when deposited in the gas-exchange region.
26

The Setting and Use of Occupational Exposure Limits Current practice
Analytical methods should follow well validatedmeasurement methodologies, such as those thathave been published by the HSE (2000) and NIOSH(e.g. see Table 3.1 and endnotes) among others.This will help ensure that collected exposure datawill be readily repeatable by other researchers andby those attempting to assess compliance (seeSection 5.3).
Biomonitoring can be an important method ofmonitoring exposure, uptake and early biological orphysiological changes. However, the application ofbiomonitoring is frequently limited by the availabilityof biomarkers. It has been successfully applied insome occupational health scenarios, where theconcentration of certain chemicals in biologicaltissues, such as lead in blood, can be directlyrelated to known health endpoints (IGHRC, 2004).
Examples of measurement techniques used forsome chemicals particularly relevant to metal andmining industries (see Case Studies, Section 5.7and Annex 1) are summarized in Table 3.1 on page 28.
27

The Setting and Use of Occupational Exposure Limits Current practice28
Table 3.1: Exposure measurement methods for case studies
Substance
Nickel and nickel sulphate(NiSO4)
Palladium and solublepalladium salt (e.g. palladium chloride)
Lead
Cr metal and CrIII
Cr VI
Manganese
Nitrogen oxide and dioxide
Sulphur dioxide
Sulphuric acid mists
Silica (crystalline)
Method
Sampling using cellulose ester (0.8 µm) or PVC (5 µm) membrane filter; measurement usinginductively coupled argon plasma, atomic emission spectroscopy; detection limit 0.2 µg/l and theworking range is 0.005–2.0 mg/m3 for a 500 l air sample6
Sampling using a Teflon membrane filter (flow rate unspecified) and measurement by X-rayfluorescence analysis. Lowest reported limit of detection 0.001–0.0005 µg/m3 (working rangeunspecified; WHO, 2002)
Sampling using cellulose ester (0.8 µm) or PVC (5 µm) membrane filter; measurement usinginductively coupled argon plasma, atomic emission spectroscopy; detection limit 0.2 µg/l and theworking range is 0.005–2.0 mg/m3 for a 500 l air sample6
Sampling (Cr metal, Cr III) using cellulose ester membrane (0.8 µm) filter; measurement using atomic absorption flame detection; detection limit 0.6 µg/l and the working range is0.05–2.5 mg/m3 for a 100 l air sample7
Sampling (Cr VI) using polyvinyl chloride membrane filter (5 µm); measurement using atomicabsorption flame detection; detection limit 0.2–7.0 µg/l and the working range is 0.001–5 mg/m3
for a 200 l air sample8
Sampling using cellulose ester membrane (0.8 µm) or polyvinyl chloride membrane (5 µm);measurement using inductively coupled argon plasma, atomic emission spectroscopy; detectionlimit 0.2 µg/l and the working range is 0.005–2.0 mg/m3 for a 500 l air sample6
Sampling (NO and NO2) using sorbent tubes with an oxidizer and triethanolamine-treatedmolecular sieve; measurement using visible absorption spectroscopy; detection limit 1 µg NO2
per sample and the working range for NO is 1.3–61 mg/m3 for a 1.5 l air sample and for NO2 is1–47 mg/m3 for a 5 l air sample9
Sampling using cellulose ester membrane (0.8 µm) filter and then collected on Na2CO3 treatedfilter; measurement using ion chromatography; detection limit 3 µg SO2 per sample and theworking range is 0.5–20 mg/m3 for a 100 l air sample10
Sampling using solid sorbent tubes; measurement using ion chromatography; detection limit 0.9 µg per sample and the working range is 0.01–5 mg/m3 for a 50 l air sample11
Sampling (respirable) at flow rate 2.2 l/min with pump fitted with nylon or Higgins-Dewell cycloneonto a 5mm polyvinyl chloride filter (flow rate is variable — and accuracy essential — based oncyclone used); measurement by visible spectrophotometry, detection limit 10 µg SiO2 per sample,working range of 0.04–5 µg/m3 for 500 l air sample, by X-ray powder diffraction, detection limit 5 µg SiO2 per sample, working range of 0.025–2.5 mg/m3 for 800 l air sample or by infra-redabsorption spectroscopy, detection limit 5 µg SiO2 per sample, working range 0.025–0.4 mg/m3 for 400 l air sample12

Risk Assessment4.1 Interpreting risk: acceptable and tolerable risk 304.2 Risk assessment methodology 30
4.2.1 Adverse effect levels: point of departure 314.2.2 Uncertainty factors 314.2.3 Dose-response relationships and the benchmark dose 334.2.4 Default factors in extrapolating from animals to
humans 334.2.5 Non-threshold agents 334.2.6 Advances in methodology 344.2.7 Estimating the size of the affected population 364.2.8 Expert judgement 36
4.3 Multiple exposures and multiple health endpoints 364.3.1 Occupational exposure limits for mixtures 364.3.2 Cumulative and aggregate exposure and
risk assessment 374.3.3 Determining critical health endpoint 37
4.4 Biological exposure limits 37
The Setting and Use of Occupational Exposure Limits Current practice
4.1 Interpreting risk: acceptable and tolerable risk
Varying descriptions of acceptability of risk areadopted by different organizations. In the case of OELs, the description and purpose of OELspromulgated by various organizations usuallycontain some expression of risk in terms of theintended level of protection.
In a broader sense HSE, for example, hasdeveloped a framework for the tolerability of riskthat describes risks ranging from the negligible to the unacceptable (Hester and Harrison, 1998). At one level there is what is described as broadlyacceptable risk; that is, risks that are considered to be acceptable, as they are typical of small risksthat do not cause people concern or cause them toalter their behaviour, and as they result only in asmall addition to background levels of risk. At theother extreme is unacceptable risk, which isconsidered intolerable, whatever the benefit.Between these two extremes lies the region oftolerable risk, where a balance has to be foundbetween risk and benefit. Tolerance of risk isstrengthened by control of risks, such that theyare as low as reasonably practical (ALARP).
The dividing lines between unacceptable/tolerableand tolerable/broadly acceptable may varyaccording to societal values and who is exposed tothe risk. The HSE has proposed that, for workers, a risk of death of 1 in 1,000 per year should be thedividing line between tolerable and unacceptablerisk. For the general public, the proposed dividingline between tolerable and unacceptable risk wouldbe 1 in 10,000 per year and a proposed broadlyacceptable individual risk of death would be 1 in 1,000,000 (Hester and Harrison, 1998).
As another example, the US EnvironmentalProtection Agency (EPA) assess risk tolerances forpesticides under the 1996 Food Quality protectionAct according to a standard of reasonable certaintyof no harm13.
4.2 Risk assessment methodology
A basic framework for the process of riskassessment — hazard identification, hazardcharacterization, exposure assessment and riskcharacterization — is well accepted (WHO, 1994).The aim of toxicological risk assessment is not,generally, to estimate the magnitude of any risk but to determine what assurance there may be fornegligible risk, in a specific exposure situation(IGHRC, 2003).
Hazard identification describes a qualitativeevaluation of available data (toxicological,epidemiological, biological, structural, etc; e.g. asdescribed in Section 2) to identify the types ofadverse effect that might result in humans as aconsequence of exposure to an agent(Paustenbach, 2003).
Hazard characterization describes the quantitativerelationship between exposure and the incidence of toxicity or adverse effect (Paustenbach, 2003). As such dose-response data are often limited forhumans, it is frequently necessary to extrapolatefrom data obtained from experimental animals tothe human situation. Such extrapolation requiresboth inter species adjustments and extrapolationfrom dose-response relationships at doses used inexperimental animals to doses to which the humanpopulation is likely to be exposed. For non-carcinogenic effects, which are not thought tooccur until a threshold level of exposure has beenreached, identification of a suitable level relative topotential harm may include several approaches,such as use of a no-observed-effect level (NOEL)with uncertainty factors, mathematical models with thresholds, the benchmark dose andphysiologically based pharmacokinetic (PBPK)modelling (see below).
Exposure assessment describes the nature andsize of the exposed population and the magnitudeand duration of the exposure (Paustenbach, 2003;see also Section 3). Increasingly probabilisticrather than deterministic methods are applied toexposure assessment (see below).
Finally risk characterization describes thelikelihood that a human population of interest willexperience any adverse effects associated with theagent of concern, under known conditions ofexposure (Paustenbach, 2003).
30
4. Risk Assessment

The Setting and Use of Occupational Exposure Limits Current practice
4.2.1 Adverse effect levels: point of departure
For the majority of toxicities a threshold or levelbelow which no adverse effect is likely to occur isassumed. Thus experimental studies are evaluatedto determine a dose without effect, that is, a No Observed Adverse Effect Level (NOAEL)2 in themost sensitive species, using the most sensitiveindicator of toxicity (e.g. Risk Assessment andToxicology Steering Committee, 1999c). There aresome differences in the definition of a NOAEL; forexample, the US Environmental Protection Agencydefines a NOAEL as ‘the highest exposure level atwhich there are no statistically or biologicallysignificant increases in the frequency or severity ofan adverse effect between the exposed populationand its appropriate control’; and the WHOInternational Program on Chemical Safety definesa NOAEL based on there being ‘no detectableadverse alteration of morphology, functionalcapacity, growth, development or lifespan of thetarget’. In the occupational environment, SCOELhas developed a severity scale for systemic andirritant effects, defining adversity as beginning atconcentrations that induce effects at a particularlevel on the scale; it has been suggested that suchan approach promotes transparency andconsistency (Haber and Maier, 2002).
In some cases, the available data do not allow aNOAEL to be established, instead a LowestObserved Adverse Effect Level (LOAEL) may beestimated, based, for example, on some minor(possibly) adverse effects at the lowest exposurelevel investigated (Fairhurst, 1995).
The point of departure (POD) is defined as theconcentration that, with the use of appropriateuncertainty factors (see 4.2.2, below), is used toderive the OEL. Usually this will be a NOAEL or aLOAEL, although the benchmark dose approach(see 4.2.3, below) may also be used.
4.2.2 Uncertainty factors
Approaches for dealing with uncertainties and theuse of uncertainty factors in risk assessment forchemicals used by UK Government departmentsand agencies have been reviewed (IGHRC, 2003).One key factor demonstrated in the IGHRC reviewwas that the uncertainty factors used in settingOELs were far smaller than those applied in otherareas of standard setting for human exposure tochemicals, such as exposure to pesticides, foodcontaminant residues and environmentalcontaminants.
Fairhurst (1995) describes how, ideally, a health-based exposure standard would be based on: • reliable data from human populations with
exposure to known levels of the chemical in question, with at least one level being a clear no-effect level for the health impact of concern; and
• confidence, based on physicochemical and toxicological parameters, that other possible health effects give no cause for concern in relation to the chemical in question.
However, generally, sufficient, quality data are notavailable to provide such a basis. Instead, usingavailable data normally requires extrapolationbetween species (i.e. interspecies variationbetween e.g. rats and humans), across species (i.e.intraspecies variation between, e.g. young healthyand elderly infirm individuals) and from high to lowdose (Fairhurst, 1995). If human data are notavailable, committees establishing OELs tend toapply extra uncertainty factors to an animal NOAELwhen setting OELs (Paustenbach, 2001). Thus theconventional approach is to identify a referencepoint, such as the NOAEL in experimental studies,and set a standard at a lower level of exposure thatis considered to meet whatever health protectioncriteria are to be met by the standard. The marginbetween the reference point and the establishedstandard is the ‘uncertainty factor’ (Fairhurst,1995).
Several variables, which are often formallyunquantifiable, influence the size of the uncertaintyfactor; it has been suggested that this means that itis not realistic to expect to establish a simplenumerical framework or set of rules for uncertaintyfactors that is free from ‘expert judgement’(Fairhurst, 1995). Indeed, ECETOC (1984) has notedthat the use of generalized mathematical schemesfor deriving uncertainty factors has limitations andshould not replace expert judgement.
31
2 Or No Observed Acute Effect Concentration (NOAEC).

The Setting and Use of Occupational Exposure Limits Current practice
Some factors that influence the size of theuncertainty factor are summarized in Table 4.1.
Despite some concerns about schemes forassigning numerical weightings for individualelements that affect uncertainty factors, forexample a factor ‘x’ to allow for interspeciesvariation and a factor of ‘y’ to allow for intraspeciesextrapolation, several such schemes have beenwidely adopted, notably for the determination ofADI values for contaminants or residues in food.Traditionally values of 10 (or fractions of 10) havebeen used for each element (Fairhurst, 1995),leading, for example, to the 100-fold margin ofsafety to account for uncertainties in intra- andinterspecies extrapolation (IGHRC, 2003). More recently, proposals to divide each of the 10-foldfactors for intra- and interspecies differences intosub-factors to allow for toxicokinetic andtoxicodynamic difference (3.2 for each) have alsoachieved wide acceptance (IGHRC, 2003). It shouldbe noted that, traditionally, the factor to account for human variability has been lower in settingoccupational limits than in setting limits for thegeneral public (for example an uncertainty factor of3, rather than 10, may be applied). This has beenbecause the working population is generally
considered to exclude some potentially sensitivegroups, such as children, the elderly and‘unhealthy’ adults (Haber and Maier, 2002).
Other uncertainties may arise owing to the inabilityof available studies to detect adverse healthimpacts; this may lead to the introduction ofuncertainty factors for the adequacy of thedatabase (Haber and Maier, 2002).
The rationale for the use of uncertainty factors, theareas of uncertainty covered and any numericaldefault values vary between organizations that setOELs. Furthermore, it is generally recognized thatvalues for uncertainty factors are established on acase-by-case basis. Recently, proposals forworking towards a more chemical-specific basis forthe derivation of uncertainty factors have been putforward (Haber and Maier, 2002).
32
Table 4.1: Influences on the size of the uncertainty factor
Source: Fairhurst (1995)
Availability of toxicological information
• amount of data• species — direct observation in humans reduces uncertainty• route of exposure — preferably route of relevance to route in humans• data quality• availability of NOAEL — in some cases only a LOAEL may be identifiable, usually requiring larger uncertainty factor
Nature and severity of principal adverse effects
• more severe the threat the greater the need to be certain of safety and the larger the uncertainty factor• small uncertainty factor if principal effect is clearly apparent and rapidly reversible (e.g. sensory irritation) and reliable data
from animals, with some human observations and little interspecies variation• large uncertainty factor if principal effect serious and irreversible (e.g. teratogenicity) and data for end-point limited
(e.g. from 1 rodent species only)
Nature of exposed population
• age and sex — greater variation, greater uncertainty about individual sensitivity• health status — greater variation, greater uncertainty about individual sensitivity• presence of checks — if exposure monitored and controlled, may be justification for reducing uncertainty factor
(e.g. applicable to occupational scenarios providing justification for smaller uncertainty factors than are applied to environmental standards for general population)
Degree of control achievable
• socioeconomic impact — large uncertainty factor where guarantee of safety very important, smaller e.g. in industrial setting where technical feasibility and economics become relevant

The Setting and Use of Occupational Exposure Limits Current practice
As an example of a numerical scheme, defaultvalues used in the Netherlands for OELs are asfollows: 3 for interspecies difference; 3 forintraspecies difference; 1–10 for differencesbetween experimental conditions and the exposurepattern of workers; and 1 for each of — type ofcritical effect; dose-response curve; confidence indata base (Dutch Expert Committee onOccupational Standards, 2000).
4.2.3 Dose-response relationships and thebenchmark dose
Recent approaches to setting OELs have includedestablishing dose-response curves, based on highquality studies, which represent a weight-of-evidence approach to identifying ‘safe’ levels ofexposure (Paustenbach, 2001).
The benchmark dose approach uses experimentaldose-response curves to determine a dosecorresponding to a predetermined response level,which can then be used as a POD for developingOELs. The advantages of the method are that ituses all dose-response data, a benchmark dosecan be determined even if an experimental studydid not identify a NOAEL and the POD is notrestricted to tested dose levels. The benchmarkdose approach could be applied to make better useof epidemiological data, by conducting dose-response modelling of exposure data onindividuals, rather than grouping individuals withsimilar exposure (see Section 2.2.2), as is often thecase (Haber and Maier, 2002).
4.2.4 Default factors in extrapolating from animalsto humans
When the POD for developing an OEL is derivedfrom animal data it is necessary to extrapolateexposure levels to humans; this may even includeroute-to-route extrapolation. Such extrapolationshould take account of differences in breathingrate, respiratory structure, bodyweight, depositionin the lung (for inhaled particles) and so on (Haberand Maier, 2002). Standard default factors may beused for some such extrapolations and PBPKmodelling and probabilistic modelling can also behelpful (see below).
4.2.5 Non-threshold agents
In some circumstances it is not possible to identifyreliably a threshold for the level at which anadverse effect does not occur; this is the case,most notably, for genotoxic carcinogens but mayalso apply to respiratory sensitizers.
CarcinogensDifferent approaches to the risk assessment ofcarcinogens are adopted by different organizations.Carcinogen classification schemes vary and whilesome organizations (e.g. ACGIH) set quantitativehealth-based OELs for carcinogens with a separatecategorization of carcinogenic potential, othersderive them only for carcinogens with thresholds(e.g. DFG, DECOS) or make only qualitativeevaluations of risk (e.g. most UK regulatoryauthorities; Risk Assessment and ToxicologySteering Committee, 1999c; Haber and Maier,2002).
SCOEL recognizes that although it may not bepossible to identify exposure levels below whichthere is no risk of carcinogenic effect, it can beassumed that the lower the exposure, the lower therisk of cancer (CEC, 1999). In the case of genotoxiccarcinogens, standard-setting bodies, such asSCOEL, will, if possible, provide a risk assessmentfor excess cancer cases estimated to occur at arange of exposure concentrations. This riskassessment is then carried forward forconsideration by the social partners who may takeinto account this risk, practicability andsocioeconomic consequences in aiming to establishan OEL. In the case of non-genotoxic carcinogens,it may be possible to identify, with reasonablecertainty, a threshold for the carcinogenic effect.This can then be the basis for setting an indicativeoccupational exposure limit value (IOELV).
While metals with positive results in genotoxicityassays are typically considered to be carcinogensfor which it is not possible to identify a thresholdreliably, metals can induce genotoxicity throughdiverse mechanisms, such as direct DNA reactivity,inhibition of DNA repair or formation of reactiveoxygen species. The identification of a particularpathway will affect whether or not the metal can beconsidered as a threshold or non-thresholdcarcinogen, for the purposes of setting an OEL(Haber and Maier, 2002). Such considerations arebecoming increasingly important, and Section 2.3
33

The Setting and Use of Occupational Exposure Limits Current practice
gives examples where understanding thetoxicological mechanism can assist greatly in bothhazard and risk assessment.
Respiratory sensitizersSensitization may be defined as a condition ofacquired specific (usually immunological) alterationin the responsiveness of a biological system,initiated to a sensitizing substance and, after anincubation period, characterized by evocation ofenhanced reactivity upon re-exposure to the sameor closely related substance. In the workplace,sensitizers may affect the respiratory system, the conjunctivae and the skin, but in the context of OELs the former two are most relevant. Such substances present a great problem for thesetting of OELs because once the airways havebecome hyper-responsive, further exposure to the substance, perhaps even to lesser, minutequantities, may cause respiratory symptoms thatmay range from a runny nose to severe asthma.Furthermore, not all workers who are exposed to asensitizer become hyper-responsive and it is notpossible to identify in advance all those who arelikely to become hyper-responsive. It is importantto distinguish substances that may trigger thesymptoms of asthma in people who may alreadyhave pre-existing hyper-responsiveness in theairways from those substances that do not inducethe disease themselves. The latter may be irritants,but are not respiratory sensitizers.
Most OELs for respiratory sensitizers are based onthe assumption that the OEL will limit the risk ofthe induction of the underlying immunologicalasthmatic condition as, once the condition isinduced, the limit is unlikely to produce anyprotection. Thus, following initial sensitization,subsequent exposure to even extremely low levelsof allergens can trigger severe, adverse healthimpacts, meaning that such sensitizers can beconsidered as non-threshold or very low thresholdchemicals. Many standards setting bodies,including ACGIH, use a sensitizer notation tohighlight these risks.
The problem in setting OELs for respiratorysensitizers is that the database is generally quitepoor and difficult to interpret and thus, for manyrespiratory sensitizers, the limits are somewhatpragmatic.
The potential complexities associated with settingOELs for sensitizers are exemplified by the case of beryllium. The focus has been to determinewhether an OEL could be set that would beprotective for chronic beryllium disease (CBD).CBD results from an immunological response to
beryllium particles, and subclinical CBD can bediagnosed by the blood lymphocyte proliferationtest. Sensitization to beryllium and thensubsequent exposure appear to be necessary forCBD to develop. Particle size, chemical form,concentration and genetic susceptibility are allfactors that appear to complicate the relationshipbetween airborne beryllium levels and CBD. Based on current understanding of the aetiology ofCBD, it has been suggested that a series of OELsfor different forms of beryllium rather a single OELfor all forms of beryllium might be appropriate(Paustenbach et al., 2001).
Although most allergens generally only causeadverse reactions in a small subset of thepopulation, the approach adopted in the UK, forexample, has been to set a MEL for occupationalexposure to such a material (Risk Assessment andToxicology Steering Committee, 1999c); althoughthis approach has since been reconsidered (HSC,2003).
4.2.6 Advances in methodology
PBPK modellingIt has been suggested that the ultimate approach to the replacement of default uncertainty factors(see above) has been the development ofphysiologically-based toxicokinetc/toxicodynamicmodelling, which predicts how a chemical ishandled in the body (Risk Assessment andToxicology Steering Committee, 1999b). Such PBPKmodels can be used to help improve extrapolationsbetween species, between dose levels and betweendifferent exposure scenarios (Blaauboer, 2003).
For example, in one study, PBPK modelling withMonte Carlo simulations (see below) was applied tothe theoretical derivation of OELs for selectedethylene glycol ethers. In the absence of adequatehuman exposure data to assess developmental andreproductive outcomes for glycol ethers, PBPKmodels for rats and humans were used to convertan animal NOEL to an exposure concentration thatwould result in an equivalent internal human dose(inter species variation). Monte Carlo simulation
34

The Setting and Use of Occupational Exposure Limits Current practice
was used, in addition, to refine inputs onpharmacokinetic variability between humans(intraspecies variability). Proposed OELsdetermined by the study were lower than the OSHA and ACGIH limits at the time. (Sweeney etal., 2001).
Quantitative structure-activity relationshipsIncreasing knowledge about molecular processesand chemical reactivity, leading to the identificationof molecular fragments with certain chemicalfunctionalities, may lead to an estimation of achemical’s reactivity in a biological system(Blaauboer, 2003).
For example, an association has been demonstratedbetween equilibrium dissociation constants fororganic acids and bases that produce irritation astheir primary adverse effect and their OELs. A physicochemical parameter may reasonably beconsidered to be a predictor of biological responsewhen the parameters are mechanisticallyassociated. Use of such parameters, in quantitativestructure activity relationships, might provideanother way to establish preliminary OELs, forexample for organic acids and bases and othercompounds with no existing limit (Leung andPaustenbach, 1998).
Identified relationships between the structure andbiological properties of chemicals can beprogramed into knowledge-based expert systemsthat can be used to assess the relationship betweencertain structures in the molecule and a variety oftoxicological endpoints (such as genotoxicity, skinsensitization etc). Other physicochemical properties,such as lipophilicity, hydrophilicity, molecularweight etc) may also impact on the relationshipbetween structure and toxicity; knowledge ofphysicochemical properties is also important to the understanding of biokinetic behaviour andbiotransformation pathways. As quantitativestructure-activity relationship models becomemore predictive of biological activity, they might beused for developing hypotheses about mechanismsof toxicity and might be integrated into riskassessment strategies (Blaauboer, 2003).
Probabilistic methodsHistorically, methods used to compare exposureand toxicity, in chemical risk assessment, havebeen deterministic in approach. Yet any health-based risk assessment should take account ofvariability (e.g. the natural variation betweenindividuals in sensitivity or between chemicalexposure levels) and uncertainty (e.g. lack ofknowledge in risk specification). Deterministicmethods for risk characterization deal withvariability and uncertainty by adopting a conservativeapproach, which has been considered appropriatefor regulatory purposes. However, such anapproach only works effectively for exposure to asingle substance from a single source and route; a conservative, deterministic approach may not be appropriate for multiple chemical exposures via multiple pathways. In contrast, a probabilisticapproach, in which outputs are expressed in theform of probabilities for each outcome, takesaccount of variability by replacing point estimateswith distributions (COT, 2002).
For example, Finley et al. (1994) proposed standarddistributions for common exposure factors, such asbodyweight, inhalation rate and time spent at onejob, for use in Monte Carlo models for screeningassessments to characterize health risks ofexposures; and in the study described above(Sweeney et al., 2001), Monte Carlo simulationswere used in conjunction with PBPK models toexamine OELs for ethylene glycol ethers.
Monte Carlo techniques were applied in a re-evaluation of exposure assessments in abenzene-exposed occupational cohort in the USA(Pliofilm Cohort) that has provided key input intocancer risk estimates for benzene and the settingof TLVs. Many discrepancies and criticisms ofearlier exposure estimates for the cohort had beenreported, so probabilistic techniques were used toimprove exposure assessment. Distributions ofbenzene exposures for various job categories in thecohort were estimated, based on input parameterscovering the likely range of exposure values, takinginto account likely decreases in workplaceconcentrations over time; probability distributionswere also estimated for other parameters,including dermal exposure, respirator use andefficiency, and weekly working hours (Williams andPaustenbach, 2003).
35

The Setting and Use of Occupational Exposure Limits Current practice
A probabilistic approach can also provide aframework for incorporating uncertainty and expertjudgment into risk assessment (COT, 2002).
4.2.7 Estimating the size of the affected population
In some cases it may be possible to estimate theproportion of an exposed population that would beaffected at different levels of exposure and thus toestimate the proportion that could be protected bysetting an OEL at different limits. This has beendone for formaldehyde, for example, whereevaluation of experimental studies, volunteer studies,surveys and epidemiological data identified thatasthmatics were not especially sensitive to theairways effects of formaldehyde and permittedestimations of the percentages of workers thatcould be expected to exhibit various signs of irritationat different levels of exposure. For example, 5–25%of workers might report eye irritation associatedwith 15 min to 6 h exposure to 0.5–1 ppmformaldehyde, although responses rates around20% are near background response levels; an OELof 0.3 ppm would protect nearly all workers; and aceiling value of 1 ppm for up to 15 min wouldprotect at least 75% of workers. (Paustenbach etal., 1997).
4.2.8 Expert judgement
Expert judgement is a term used to describe theprocess by which knowledgeable persons on asubject arrive at a decision based on both theavailable information and their expert or consideredopinions, underpinned by their experience, usuallytaking into account some kind of paradigm. When itcomes to setting OELs, the gaps in knowledge canbe quite vast and thus it is necessary to useinformation from related chemicals as a ‘readacross’ to help predict effects. It is also commonfor expert committees to apply uncertainty factorsin an ad hoc fashion, again based on expertjudgements. This will take into account the severityof the most serious effect, the quality of thedataset, including gaps in knowledge, and thenumber of workers that might be exposed in thepopulation. In the past, it was quite common forexpert judgement not to be apparent in thedeliberations of such committees, but nowadays,owing to better transparency in decision-making, itis usual to be able to see where science ends andexpert judgement begins.
4.3 Multiple exposures and multiple healthendpoints
4.3.1 Occupational exposure limits for mixtures
The majority of OELs are set for single compoundsor substances, although some have been set forsubstances that may contain a common element or radical, for example ‘tungsten compounds’ and‘isocycanates’ (HSE, 2005b). A few OELs may be setfor complex mixtures of variable composition suchas ‘rubber fume’ or ‘welding fume’. In the case ofhydrocarbons, which are normally supplied ascomplex mixtures, some jurisdictions haverecommended the use of a reciprocal calculation,so that producers and suppliers of mixedhydrocarbon blends can derive an appropriate ‘in-house’ OEL (HSE, 2005b). In this specific case,the procedure covers aliphatic hydrocarbons in the range C5 to C15, cycloalkanes in the range C5 toC16 and aromatic hydrocarbons. It excludeshalogenated or oxygenated hydrocarbons and onlyapplies to vapours, not mists. The calculation toreach the mixture OEL is as follows:
FRa FRb FRn
1/OELSOL = + +OELa OELb OELn
where OELsol = OEL of the hydrocarbon solventmixture (mg/m3); OELa = OEL of component ‘a’(mg/m3); and FRa = fraction (w/w) of component ‘a’in the solvent mixture.
When it comes to assessing the potential healtheffects from exposure to more than one substancein the workplace, a number of strategies can beapplied, but that of the ACGIH is one that seemsthe most widely practiced in one form or another.
ACGIH adopts the approach that the combinedeffect of a mixture of two or more hazardoussubstances, which act on the same target organ,should be given primary consideration, rather thanthe effects of each substance individually. Thus, inthe absence of information to the contrary, theeffects of the different hazards should be consideredas additive. However, if the chief effects of a seriesof different substances are not additive but actindependently (e.g. on different target organs), thenthe OEL for the mixture is considered to beexceeded only when at least one member of theseries exceeds its OEL (ACGIH, 2003a).
36

The Setting and Use of Occupational Exposure Limits Current practice
Interactive processes are divided into potentiation(combined effect greater than additive) andantagonism (combined effect less than additive;COT, 2002). Combinations where synergistic actionor potentiation occur are currently dealt with on acase-by-case basis (ACGIH, 2003a).
4.3.2 Cumulative and aggregate exposure and riskassessment
In recent years, much attention has been given todeveloping newer risk assessment methodologiesto deal with human exposure to mixtures ofchemicals. One major area of concern has beenthat of a variety of low-level exposure to pesticidesthrough foodstuffs. Much work has been done inthis area by the US EPA and their definitions of theterms cumulative and aggregate have permeatedthrough other areas of human exposure tomixtures of chemicals.
Aggregate exposure refers to exposure to onechemical from all sources. Cumulative exposurerefers to exposure to multiple chemicals that havea common mechanism of action (COT, 2002). Both need to be taken into account in riskassessment, as exposure to multiple substancesmay result in several different types of combinedaction.
4.3.3 Determining critical health endpoint
It is often common to think that OELs are based ononly one serious, harmful effect of a substance.However, many chemical substances are able toproduce a constellation of toxic or harmful effects— some acute effects, which are produced underhigh exposure conditions and some chronic effects,which are produced over extended periods ofexposure and in the absence of acute effects. When setting OELs, most committees will expect to review a complete dossier of human and animaldata, which represents the complete spectrum ofpotential health endpoints and takes into accountall the exposure scenarios under which workersmight be exposed, even under poor practices oraccidental situations.
With all this available data, it should be possible todraw up a toxicological and ill health profile for alllikely acute and chronic effects and, ideally, dose-response relationships for these. From such data,both short-term and long-term OELs can bederived, in order to prevent most of theseconditions, but at the same time taking intoaccount all other conditions. If a substance is agenotoxic carcinogen, this would be the ‘leadeffect’; normally, no OEL based on a NOEL wouldbe derived and the level would be set so low that it would be unlikely that other effects would beexpected. It is often common to have acute effectsprevented by a short-term limit, such as a 15-minSTEL, set on one health endpoint, such asirritation, and chronic effects prevented by an 8-hTWA, based on a systemic effect at an organ suchas the kidney.
4.4 Biological exposure limits
As noted in Section 1.2.2, biological exposurelimits, such as BEIs or BATs, may be used foreither biological monitoring, in which case theworker is simply being used as a way of collectingthe chemical or metabolite of the chemical within abiological matrix, or biological effect monitoring,where the same matrix may be used to examineearly and reversible non-clinical changes. Eithermay be used as part of a regulatory or advisoryframework, as part of risk assessment and riskmanagement, and monitoring tools have beendeveloped with variable applications. As anexample, the monitoring of lead workers for bloodlead (biological monitoring) is virtually mandatoryand, in terms of risk assessment and management,is used both as a way of monitoring build-up oflead and as a means of indicating the need toremove people from further exposure if a certainlevel is reached. Concurrent zinc protoporphyrinanalysis (biological effect monitoring) can also helppinpoint how long ago lead exposure occurred.
In setting biological exposure limits, a lot ofinformation has to be obtained and guidance givenas to when to collect samples, how to interpretthem and the ethical implications of their use. For example, many metals have long half-lives,which means their excretion might become quitestable; therefore, unless there is a need to monitorany weekly build up in levels, the timing ofsampling at the end of a working week is notespecially critical.
37

The Setting and Use of Occupational Exposure Limits Current practice38
The importance of biological monitoring andbiological effect monitoring is that they provideinformation for risk assessment that may beotherwise unattainable from air monitoring alone.Biological monitoring and biological effectmonitoring both take into account, for example,factors such as skin uptake, individual workinghabits (including hand-to-mouth contact) anduptake from other sources of exposure to the samesubstance that might be experienced outside theworking environment, from past-times, hobbies orsecondary occupations.
Setting and Using OELs5.1 Factors that influence setting of occupational
exposure limits 405.2 Comparison of the process between
countries/jurisdictions 405.2.1 European Union 405.2.2 Germany 415.2.3 The Netherlands 415.2.4 Nordic countries 415.2.5 UK 465.2.6 USA 465.2.7 Australia 47
5.3 Assessing compliance 475.4 Assessment of socioeconomic impacts 48
5.4.1 Cost–benefit assessment 485.4.2 Regulatory impact assessment 49
5.5 Technical feasibility 505.6 Safety impact 50
5.6.1 Reducing and controlling exposures 505.6.2 Variability and susceptibility 51
5.7 Case studies 515.7.1 Nickel and nickel compounds 515.7.2 Palladium and soluble palladium salts 525.7.3 Lead 535.7.4 Chromium 545.7.5 Manganese 555.7.6 Nitrogen dioxide 575.7.7 Sulphur dioxide 585.7.8 Sulphuric acid mists 595.7.9 Silica (crystalline) 605.7.10 Overall summary on case studies 61

The Setting and Use of Occupational Exposure Limits Current practice
5.1 Factors that influence setting of occupationalexposure limits
Health-based OELs can be established when it ispossible, based on scientific evidence, to identify aclear threshold dose below which exposure is notexpected to lead to an adverse response (see alsoSection 4.2.1). For adverse effects for which it isnot possible to identify such a threshold reliably(Section 4.2.5), where it may be assumed that anylevel of exposure carries some finite risk, OELsmust be established pragmatically, at levelsconsidered to carry a sufficiently low level of risk(CEC, 1999).
As noted by Haber and Maier (2002) some of thediversity apparent in the development of OELsacross different organizations arises from differentrisk management approaches, such as determiningappropriate levels of residual risk to an exposedpopulation or weighing health-based limits withtechnical feasibility or economic impact.Paustenbach (2000) notes other factors that mightaccount for diversity in OELs, as follows: differencesin philosophical objectives of the limits and theuntoward effects they are meant to eliminate orminimize; differences in the predominant age andsex of workers; length of the working week;economic considerations in different countries; anddifferences in enforcement. It is also worth notingthat many OEL-setting groups must work within aprescribed regulatory framework with specificdefinitions of certain terms.
Differing views as to the proportion of people that itis thought should be protected from adverse healtheffects (see Section 4.2.7, above) or, indeed, theadverse impacts against which it is deemednecessary to protect workers (Paustenbach, 2000)might affect approaches to setting OELs andnumerical values for OELs. For example, while insome countries irritation is accepted as a criticaleffect (Remaeus, 2001), in the USA it is acceptedthat some workers exposed at the OEL mightexperience some degree of transient irritation oreven more substantial impacts (ACGIH, 2003a).
Nonetheless, it should be recognized that theACGIH TLVs, which are the world’s most recognizedand adopted OELs, are purportedly entirely health-based and do not take factors such as riskmanagement, technical feasibility or economicimpact into account in their development.
5.2 Comparison of the process betweencountries/jurisdictions
Summaries of information on procedures forsetting OELs in some EU member states and innon-member states are provided by the EuropeanAgency for Safety and Health at Work (EU-OSHANetwork, 1998–2005)1 and in the review by Walterset al. (2003). Useful summaries of the OEL settingprocesses of the US ACGIH, German DFG, UK HSEand other organizations are also given in NOHSC(1999). However, it should be recognized thatextensive national programs to update OELs acrossthe world are not in place. The fact that somenational OELs have not been re-reviewed in decadesmay be another factor leading to differences innumerical values between countries. Furthermore,although groups such as the ACGIH, HSE and DFGproduce annual updates, these should not bemistaken for annual reviews of all substanceslisted therein. While recognizing the importance ofnational OEL guidelines, it should be acknowledgedthat there are no OELs for the vast majority of thethousands of chemicals that are used routinely inindustry. As a result, many businesses haveestablished their own in-house limits (Paustenbachand Langner, 1986). This particularly applies to thepharmaceutical industry, which has to deal with alarge number of biologically active substances withpharmacological as well as toxic properties.
General procedures in different regions arecompared and contrasted in Table 5.1. Some general principles are outlined below,region-by-region.
5.2.1 European Union
Walters et al. (2003) note strong similaritiesbetween national systems for setting and usingOELs in a number of countries in the EU. The ACGIH lists of TLVs and practices in Nordiccountries and in Germany have been influential.However, there are national differences in settingOELs and in their status and use.
Based on scientific evaluations, SCOELrecommends OELs to the Directorate-General (DG)for Employment, Social Affairs and EqualOpportunities. While adopting a case-by-caseapproach to recommending health-based OELs,general procedures followed by SCOEL include thefollowing (CEC, 1999):• collection of data on hazards of the substance
and determination of adequacy of database;
40
5. Setting and Using OELs

The Setting and Use of Occupational Exposure Limits Current practice
• identification of critical adverse effect(s);• identification of relevant studies on critical
effects;• establishment of threshold or non-threshold
mechanism (if latter OEL will be pragmatically based);
• assessment of dose-response data and establish NOAEL (or LOAEL);
• decision on whether STEL required in addition to 8-h TWA;
• establishment of numerical value for 8-h TWA at or below NOAEL (or LOAEL), incorporating appropriate uncertainty factor(s);
• establishment of numerical value for STEL; and• documentation of entire process.
5.2.2 Germany
Germany has two types of OEL — the MAK valuesand classifications proposed and published by theDFG (2005b) and the values published in theTechnische Regeln für Gefahrstoffe (TRGS 900 forOELs; TRGS 903 for BAT values; DFG, 2004).
Derivation of a MAK value is based on identificationof the most sensitive health parameter, taking into account both local and systemic effects. The minimum database for derivation of a MAKvalue is, normally, a NOAEL from a valid 90-dayinhalation study in experimental animals. Knowneffects of structural analogues may be taken intoaccount (DFG, 2005b). The values published in theTRGS 900 comprise MAK values, binding values ofSCOEL and values proposed by other institutions,which have been evaluated and accepted by theAusschuss für Gefahrstoffe (AGS), a committee ofthe Federal Ministry of Labour and Social Affairs. In general these are based on the current status of knowledge about the health hazards, typicalindustrial use and safety and hygiene requirements(DFG, 2004). The influence of the MAK, TRK(Technische Richtkonzentrationen; technicalguidance concentration) and BAT values are greatly enhanced worldwide, as the values anddocumentation are available in English.
5.2.3 The Netherlands
The Netherlands has two types of health-basedOELs (legally binding and administrative) withdiffering bases and status. OELs were initiallybased, extensively on the ACGIH TLVs.
Unlike many other organizations, the Committee on Updating of Occupational Exposure Limits of the Health Council of the Netherlands outlinesminimum data requirements for the developmentof OELs; data on acute toxicity and repeated-dosetoxicity are required, and a multi-dose study in a relevant species, using a relevant route ofadministration and evaluating a range of endpointsis required, as a minimum (Haber and Maier, 2002).
Legally binding OELs are based upon the health-based recommended occupational exposure level(HBR-OEL) provided by the Dutch ExpertCommittee on Occupational Standards (DECOS) ofthe Health Council but socioeconomic feasibility isalso taken into account. The legal status is basedon the Dutch Occupational Law, and the LabourInspectorate controls the implementation. In ayearly working program, the Ministry of SocialAffairs and Employment sets limit values in a‘three-steps’ program. First a scientific evaluationof data is made by DECOS leading to an HBR-OEL;a key study is identified as the basis for derivingthe recommended level. In step 2, the Social andEconomic Council advises the State Secretary onthe feasibility of using the health-based valuederived by DECOS or recommends a differentvalue. In step 3 the State Secretary sets aregulatory OEL (Dutch Expert Committee onOccupational Standards, 2000).
Administrative OELs are not legally binding.However, to protect workers, such levels shouldnot be exceeded. They are derived mostly fromother member states of the EU or from ACGIHTLVs1. The values and documentation are publishedin English as well as Dutch and thus are widelyavailable and used worldwide.
5.2.4 Nordic countries
Although, as described in Table 5.1, the scientificbasis for OELs is common to all Nordic countries,based on an evaluation by the Nordic Expert Group(NEG) of scientific criteria documents, OELs areestablished at a national level and the actualnumerical value may differ between countries. The criteria for setting OELs can only be partially
41

The Setting and Use of Occupational Exposure Limits Current practice42
Table 5.1: Setting OELs in different jurisdictions
* As a general rule OELs will use, as preferred values, multiples of given integers in ppm or mg/m3
Region
EU (CEC, 1999)
Germany (DFG, 2004; DFG, 2005b)
Netherlands (DECOS, 2000)
Nordic countries(Lundberg, 1991)
Process
Expert committee
SCOEL scrutinizes criteriadocuments and advises EC
DFG Commission for theInvestigation of HealthHazards of ChemicalCompounds in the Work Area
DECOS a committee of theHealth Council of theNetherlands
Social and EconomicCouncil advises StateSecretary
NEG finalizes criteriadocument
National regulatoryauthorities set OELs
Review of data
Criteria documents fromnational limit settingsystems or documentscommissioned directly by EC
Detailed literature reviewmade available toCommission
Review by a Netherlandsresearch institute
Criteria documentproduced by scientist inone of Nordic countries
Criteria document used to produce nationalconsensus report
OEL set at national level,based on scientific andother factors
Publication
Detailed scientificdocument (with OEL) onEU website (up to 2002)14
MAK: detailed scientificdocumentation in Englishin Occupational Toxicants
BAT: in English inBiological ExposureValues for OccupationalToxicants
Annual List of MAK andBAT Values
Detailed scientificdocument with OEL alsoavailable on website
Final scientific documentfrom NEG published inArbete och Hälsa andsent to nationalregulatory authorities
Swedish reportspublished in Arbete ochHälsa others notpublished but publiclyavailable
Underlying [non-scientific] data for OELnot published but publicly available
Risk assessment
Quantitive
8-h TWA, 15-min STEL
8-h TWA, (MAK and BAT),15-min excursionvalue (MAK)
8-h and 15-minTWA, ceiling value,exposure–response forgenotoxic carcinogens
Numerical OEL notproposed in NEG criteria document

The Setting and Use of Occupational Exposure Limits Current practice 43
Continued over page
Qualitative
Notation: skin Riskphrases
Carcinogens: no MAK orBAT values; categoricaldescriptors used
Notations: skinabsorption, cancer,sensitization, prenataltoxicity, germ cellmutagenicity
Regulatory status
Recommendation by SCOELto EC DG for Employment,Social Affairs and EqualOpportunities
OEL published by DG inOfficial Journal hasregulatory status
MAK values incorporated incommon nationallegislation
State Secretary setsregulatory OEL; somelimits administrative only
OEL has legal status inDenmark and Sweden;recommended values inFinland, Norway andIceland
Transparency
Key studies
Identified in backgrounddocumentation
Identifiable in backgrounddocumentation
Identified in publisheddocumentation
Critical effect defined
Not clearly identified inpublished documentation
Uncertainty factors
Identified in backgrounddocumentation
MAK generally at level ofNOAEL in humans or 1/2 NOAEL in animals
Overall assessment factor,consideration given tousing default values,details given in publisheddocumentation
Preferred value system*
1, 2, 5 ppm or mg/m3 x 10n
1, 2, 5 ml/m3 or mg/m3 x 10n
1, 2, 5 mg/m3 x 10n
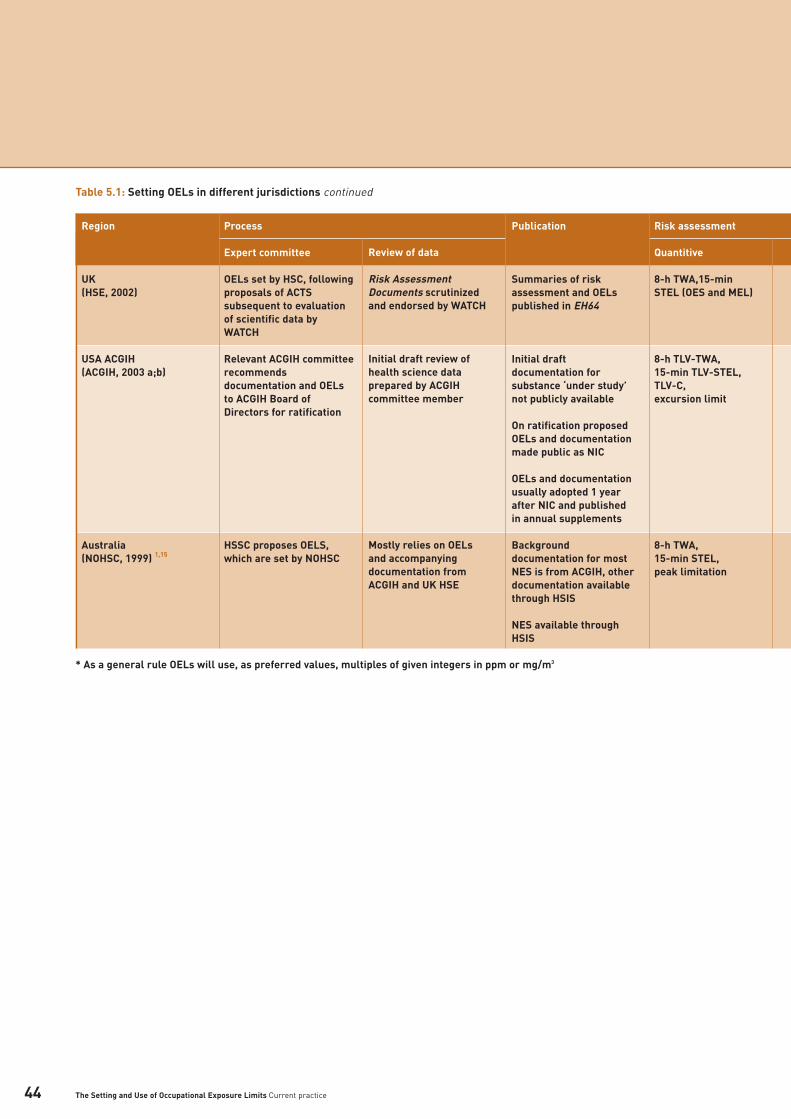
Table 5.1: Setting OELs in different jurisdictions continued
* As a general rule OELs will use, as preferred values, multiples of given integers in ppm or mg/m3
Region
UK(HSE, 2002)
USA ACGIH(ACGIH, 2003 a;b)
Australia (NOHSC, 1999) 1,15
Process
Expert committee
OELs set by HSC, followingproposals of ACTSsubsequent to evaluationof scientific data byWATCH
Relevant ACGIH committeerecommendsdocumentation and OELsto ACGIH Board ofDirectors for ratification
HSSC proposes OELS,which are set by NOHSC
Review of data
Risk AssessmentDocuments scrutinizedand endorsed by WATCH
Initial draft review ofhealth science dataprepared by ACGIHcommittee member
Mostly relies on OELs and accompanyingdocumentation fromACGIH and UK HSE
Publication
Summaries of riskassessment and OELspublished in EH64
Initial draftdocumentation forsubstance ‘under study’not publicly available
On ratification proposedOELs and documentationmade public as NIC
OELs and documentationusually adopted 1 yearafter NIC and publishedin annual supplements
Backgrounddocumentation for mostNES is from ACGIH, otherdocumentation availablethrough HSIS
NES available throughHSIS
Risk assessment
Quantitive
8-h TWA,15-min STEL (OES and MEL)
8-h TLV-TWA,15-min TLV-STEL,TLV-C,excursion limit
8-h TWA,15-min STEL,peak limitation
The Setting and Use of Occupational Exposure Limits Current practice44
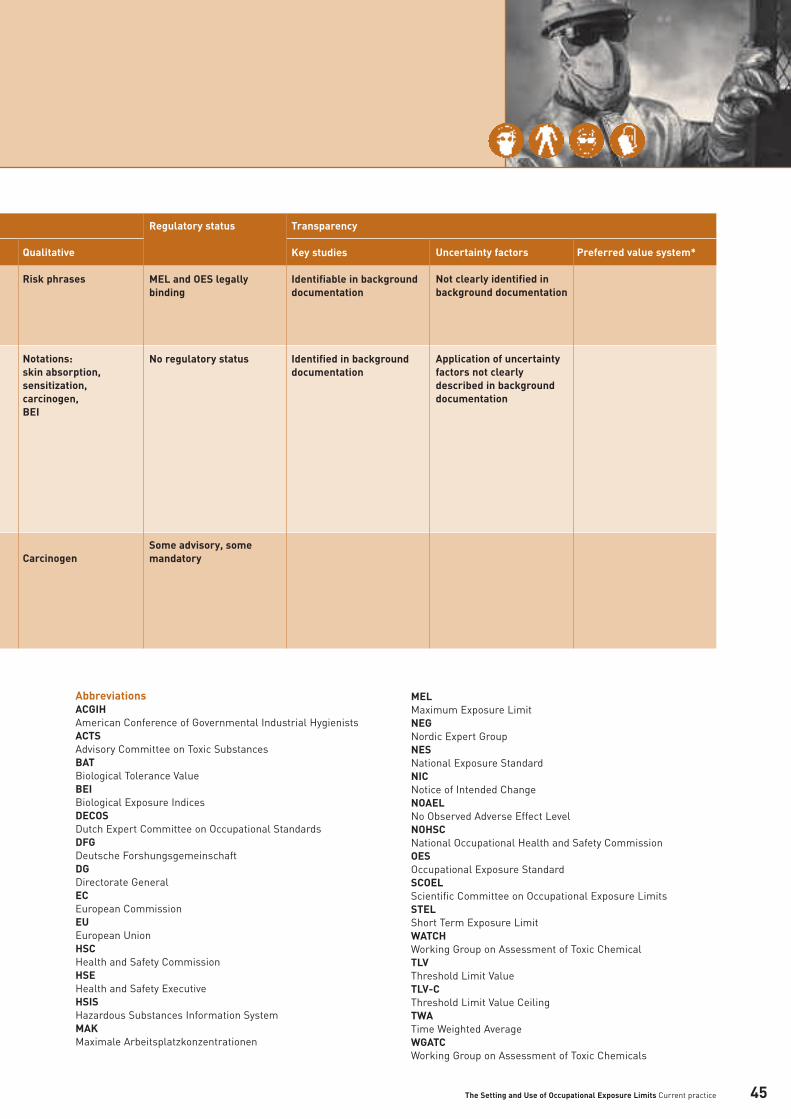
AbbreviationsACGIH American Conference of Governmental Industrial Hygienists ACTS Advisory Committee on Toxic SubstancesBATBiological Tolerance ValueBEI Biological Exposure IndicesDECOS Dutch Expert Committee on Occupational Standards DFG Deutsche Forshungsgemeinschaft DG Directorate General ECEuropean CommissionEU European UnionHSCHealth and Safety Commission HSEHealth and Safety ExecutiveHSISHazardous Substances Information SystemMAKMaximale Arbeitsplatzkonzentrationen
MELMaximum Exposure LimitNEGNordic Expert GroupNESNational Exposure StandardNICNotice of Intended ChangeNOAELNo Observed Adverse Effect Level NOHSCNational Occupational Health and Safety Commission OESOccupational Exposure StandardSCOEL Scientific Committee on Occupational Exposure Limits STEL Short Term Exposure Limit WATCHWorking Group on Assessment of Toxic ChemicalTLVThreshold Limit ValueTLV-CThreshold Limit Value CeilingTWA Time Weighted AverageWGATCWorking Group on Assessment of Toxic Chemicals
Qualitative
Risk phrases
Notations:skin absorption,sensitization,carcinogen,BEI
Carcinogen
Regulatory status
MEL and OES legallybinding
No regulatory status
Some advisory, somemandatory
Transparency
Key studies
Identifiable in backgrounddocumentation
Identified in backgrounddocumentation
Uncertainty factors
Not clearly identified inbackground documentation
Application of uncertaintyfactors not clearlydescribed in backgrounddocumentation
Preferred value system*
The Setting and Use of Occupational Exposure Limits Current practice 45

The Setting and Use of Occupational Exposure Limits Current practice
identified, as published criteria documents are onlyavailable for some substances; for many othersOELs have been set based on documentation fromACGIH, for example (Lundberg, 1991).
5.2.5 UK
OELs in the UK function under the Control ofSubstances Hazardous to Health Regulations(COSHH) and its mirror legislation in NorthernIreland. The Working Group on the Assessment andControl of Chemical Hazards (formerly the WorkingGroup on Assessment of Toxic Chemicals; WATCH)evaluates toxicological, occupational hygiene andanalytical data, which are reviewed in ‘RiskAssessment Documents’ and other sources, andacts as a technical subcommittee of the AdvisoryCommittee on Toxic Substances (ACTS). ACTSrecommends new OELs or revisions to existingOELs, and the Health and Safety Commission (HSC)approves the OELs (HSE, 2002).
Carcinogenicity, reproductive toxicity, and irritationand sensitization potential are considered whenpreparing a proposal for an OEL. Some hazardoussubstances may not be assigned OELs and/or havetheir own specific legislation, including airstandards, most notably asbestos and lead (HSE,2002).
Under the former two-OEL system, for a substanceto be assigned an OES it had to meet threeindicative criteria concerning expectations of lackof injury, from both long-term and short-termhigher exposures, and practicability of compliance.If these three criteria could not be met, thesubstance became a candidate for a MEL. MELs were usually reserved for carcinogens,respiratory sensitizers and other substances thatpresent a serious hazard for which no thresholdcan be established (HSE, 2002).
As noted in Section 1.2.1, the HSC has recentlyreplaced OESs and MELs by a single OEL, the WEL;the new OEL framework came into force in the firsthalf of 2005 (HSC, 2003; HSE, 2005b).
5.2.6 USA
ACGIH is a not-for-profit professional organization,developed in the mid 1940s, which represents awide range of industrial hygiene expertise andopinion. Its committees propose TLV and BEIguidelines for use in making decisions about safelevels of exposures to chemical and physical agentsin the workplace; however, it is not a standardssetting body in the USA (ACGIH, 2003a).Nonetheless, while ACGIH guidelines do not haveregulatory status in the USA, they are very widelyused in other national OEL processes.
The ACGIH TLVs and BEIs are solely health-based,with no consideration given to economic ortechnical feasibility; however the ACGIHrecommends that its guidelines should not beadopted as standards without analysis of otherfactors necessary to appropriate risk managementdecisions (ACGIH, 2003a).
Substances are nominated and selected forevaluation, based on selection criteria that takeinto account scientific evidence and workplaceexperience (NOHSC, 1999). Lists of substances‘under study’ are published annually, as anotification and invitation for interested parties tosubmit data and comments to the relevantcommittee. For each nominated substance,members of the appropriate committee prepare areview of the scientific literature relevant to theestablishment of a guideline value. The committeemay modify the review prior to its adoption as the‘Documentation’ to support a recommended TLV orBEI. The documentation and proposed guidelinesare recommended to the ACGIH Board of Directorsfor ratification and, once ratified, the proposals are published as a notification of intended change(NIC) and the draft documentation is made publiclyavailable (ACGIH, 2003a).
The documentation supporting TLVs and BEIstransparently indicates the scientific bases thatlead to the committees’ recommended guidelinevalues. The documentation considers only heath-based criteria. The impacts of the guideline onindustry, socioeconomic factors or the method orprocesses for measurement of the value(s) are notconsidered.
The guidelines published as NICs are considered to be trial limits for one year, during which timeinterested parties may submit comments (ACGIH,2003a). Thus, while it does not consult with
46

The Setting and Use of Occupational Exposure Limits Current practice
employer or employee representatives informulating proposed standards, the ACGIHprocess incorporates consultation though theannual publication of the NIC (NOHSC, 1999), andwithin the NIC process external considerations may come into play. However, such considerationswould not necessarily result in the raising of aguideline value. Instead a given chemical’s valuemight remain on the NIC for an extended period oftime (e.g. beryllium or wood dust) or eventually beremoved from the NIC, which would indicate that itwas not planned for adoption.
It has been suggested that the ACGIH process forsetting TLVs changed during the 1990s to facilitatethe adoption of sufficiently protective standards(Smith and Mendeloff, 1999).
OSHA PELs are enforceable regulatory limits in the USA. Initially, from 1971, limits were based onthe ACGIH TLVs. Currently OSHA has around 500PELs for some 300 chemical substances used inindustrial settings. In establishing standards,recommendations are made by one of the OSHAAdvisory Committees, all of which includerepresentation from management, labour and stateagencies; thus OSHA standards have both inputfrom and impact on industry1. OSHA deliberationson OELs take into account the feasibility ofachieving levels and incorporate a formalizedprocess for the estimation of risk magnitude(Rappaport, 1993).
NIOSH has statutory responsibility to recommendexposure limits that are protective to workers andhas identified RELs for some 700 hazardoussubstances. Recommendations for OSHA and otherOEL setting institutions are made through NIOSHcriteria documents1.
The American Industrial Hygiene Association (AIHA)has published 107 workplace environmentalexposure level guidelines (WEELs), which representworkplace environmental exposures levels to whichit is thought nearly all individuals could berepeatedly exposed without experiencing adversehealth impacts. Background information and therationale for the WEEL are published with theWEEL values16. WEELs are considered forchemicals for which no alternative guideline hasbeen established, often because they are producedin low quantities or have low toxicity (Paustenbachand Langner, 1986).
5.2.7 Australia
Initially an Exposure Standards Expert WorkingGroup (ESEWG) recommended NESs for individualsubstances; NESs are set by the NOHSC, whichconsists of employee and employer organizations,trade unions, and industry and governmentrepresentatives. The ESEWG is no longer inexistence. In 1997, following an organizational re-focus, NOHSC established the HazardousSubstances Sub Committee (HSSC) to maintain thescientific integrity of the national hazardoussubstances regulatory package. The NOHSC hadrelied extensively on published standards andbackground documentation from the ACGIH TLVsand has adopted those found to be acceptable. A smaller number of substances (e.g. respirablecrystalline silica) are reviewed in detail by theHSSC, and appropriate values are assigned1.
The NOHSC has a program to review and updateNESs, in particular to address the time lag betweenNESs and comparable systems overseas. The UKHSE OELs are currently used as a basis for a fasttrack system in the overall process (NOHSC, 1999).
5.3 Assessing compliance
Compliance checking usually involves the collectionand analysis of samples in a prescribed fashion andcomparison of the measured concentration, oftentaking into account statistical significance, with theappropriate OEL. Compliance testing comprises,typically, one-to-one comparisons of measured airlevels and OELs (IGHRC, 2004). However, it shouldbe recognized that the measurement andcomparison of airborne levels and compliancetesting are limited by the availability of appropriatereference standards and analytical capabilities. For compliance purposes, substances that cancause known harmful effects from peak exposuresare usually subject to a 15-min STEL and/or ceilingvalue (IGHRC, 2004). The AIHA ExposureAssessment Strategies Committee recommendsthat the exposure distribution profile of a SEGshould be controlled such that the 95th percentileexposure is less than the OEL (specifically, forAIHA, the OSHA PEL) for both short-term and TWAexposure limits and that, in principle, long-termexposure to chemicals associated with chronicdisease should be evaluated against a long-termaverage exposure level or mean of the exposureprofile17.
47

The Setting and Use of Occupational Exposure Limits Current practice
Biological monitoring can complement airmonitoring and can be especially useful wherethere is likely to be significant absorption fromroutes other than inhalation or where control ofexposure depends on respiratory protective devices (HSE, 2002).
However, the effectiveness of compliance testing inassessing risk has been questioned. Although OELstend to be set assuming long-term exposure,enforcement, generally, involves short-termcomparisons of measured air levels based on verysmall numbers of measurements (Rappaport et al.,1998). Whereas, in compliance testing, theprobability of compliance is, generally, related tothe exceedance (the likelihood that anymeasurement would exceed the OEL), using,instead, the probability of over exposure (defined asthe likelihood that individual risk — a function ofcumulative exposure — exceeds the risk inherent in an OEL) as a measure of individual risk, Tornero-Velez et al. (1997) demonstrated that compliancetesting can significantly underestimate health riskwhen sample sizes are small. Thus while, withtypical sample sizes, the probability of compliancemay be high, large proportions of the exposedpopulation may have individual risks greater thanthe risk inherent in the OEL.
According to Mulhausen and Damiano (1998) thecurrent approach has moved from compliancemonitoring, which focuses on the high riskworkers, to comprehensive exposure assessment,which addresses the situation for all workers at allexposures on all days. An exposure assessmentstrategy is proposed for an industrial hygieneprogram that encompasses: • basic characterization of the workplace work
force and exposures; • exposure assessment to identify acceptable,
uncertain and unacceptable exposure profiles for SEGs;
• updating and reassessment of acceptable exposure profiles;
• further information gathering for uncertain exposure profiles; and
• health hazard controls for unacceptable exposures.
5.4 Assessment of socioeconomic impacts
Economic analysis compares the costs and benefitsof options, one of which, usually, is to continue withthe current choice; that is to do nothing. To analyzefully the options available, both the costs andoutcomes (benefits) of the proposal should beconsidered. The main types of economic analysisused are cost-effectiveness, cost-utility and cost-benefit analysis/cost benefit assessment (CBA;e.g. Schmid, 1995; Jefferson et al., 1996).
5.4.1 Cost–benefit assessment
CBA is a tool used to quantify, in monetary terms,as many of the costs and benefits of a proposal aspossible, including factors, such as health status,that have no market in which choices and trade-offs can be determined (DH, 1995). Since 1982, theUK HSC has required CBAs for all major health andsafety proposals, unless the costs are negligible.Costs and benefits are included in the consultationprocess for OELs and, since October 1998, theyhave been discussed within the regulatory impactassessment (RIA) framework (see section 5.4.2below; HSC, 2002a).
Uncertainties in estimations of the costs of controlsand in validation of exposure compliance data, bothof which may vary with each substance, will impacton CBAs/RIAs. Quantification of the benefits of anOEL may also be difficult; it is usually based onhow far the OEL reduces the risk to workers, using dose–effect information. However, whendose–effect information is unavailable, for examplein the case of non-threshold carcinogens, othermethods have been developed to estimate thebenefits of an OEL (HSC, 2005a). Improved employeerecruitment and retention, improved productivityand a reduction in product loss may result fromother, more general and less quantifiable, potentialbenefits of an OEL, as identified by the UK HSC andlisted below (HSC, 2005a).
• Definition of a level playing field for all workers• Definition of adequate control• Provision of clearer guidance on the level
considered to be reasonably practicable• Provision of a standard for new users• Reduction/limitation of scope for ‘discretion’ by
enforcing authority• Provision of consistency with international
developments• Reinforcement/improvement of good practice• Encouragement of proper reporting of ill-health
48

The Setting and Use of Occupational Exposure Limits Current practice
• Promotion of more effective health surveillance• General reduction in ambient air contamination
The UK ACTS uses CBA and RIA as tools fordecision-making for OELs and recognizes thebenefits and uncertainties when making theirrecommendations. These tools are also importantin identifying the socioeconomic impact of theproposed OEL; although, the HSC states that this is not the over-riding determining factor (HSC,2005a).
The use of CBA alone as a measure for assessing a proposal affecting health could be criticised forforcing monetary constraints onto issues thatinvolve well-being and the value of life, andbecause of the inherent difficulties associated withascribing monetary value to health improvements(e.g. The Presidential/Congressional Commissionon Risk Assessment and Risk Management, 1997).
5.4.2 Regulatory impact assessment
RIA is a policy tool used to assess the impact oncosts, benefits and risks of any proposedregulation. It is an evidence-based process, whichprovides an analysis of a range of options forchange, by identifying objectives, risks, alternativesto legislation, business (and other) sectorsaffected, equity and fairness, benefits and costsand unintended consequences (RIU, 2003).
A case study for RIA — assessing the cost-benefitsof reducing an OELThe use of RIA by government authorities in orderto facilitate the setting of OELs is illustrated by thefollowing case study3, which examines the processused by the UK HSE to assess the costs andbenefits associated with determining a new WELfor respirable crystalline silica (see also Section5.7.9).
The current UK OEL for respirable crystalline silicais a MEL of 0.3 mg/m3; however, when the COSHHregulations were introduced in 1989, the OEL was0.1 mg/m3. The MEL was introduced with theexpectation that those industries already complyingwith an exposure level of 0.1 mg/m3 shouldcontinue to do so. The HSC is now in the process ofissuing a consultative document for a proposednew WEL of 0.1 mg/m3 18.
The HSC conducted a RIA and took its findings intoaccount in reaching its proposal to lower thecurrent MEL18. Four potential revised limits wereconsidered in the RIA — 0.3 (current), 0.1 (pre-1992limit), 0.05 or 0.01 mg/m3. In order to determinewhich would be most appropriate, the criticalhealth effects of lung cancer, fatal silicosis andsilicosis were considered in terms of cost andbenefit for each of the proposed limits. The benefitswere identified as monetary values placed onmedical costs, human costs (pain and suffering)and productivity losses. The benefits, over sixtyyears, from preventing cases of fatal silicosis, lungcancer and silicosis at each of the limits wereassessed and the total prevented costs (benefits)can be seen in the Table 5.2, which also indicatesthe costs associated with implementing the fourproposed new limits.
49
3 A more detailed case study can be included, if required, when thebackground documents are confirmed as publicly available, (HSE, 2005a;HSC, 2005b).
Table 5.2: Summary table of benefits and costs over 60 yrs from preventing silicosis, fatal silicosis and lung cancer for each WEL proposed for respirable crystalline silica18
Benefits
Costs
0.3 mg/m3 (£ Million)
39.4 to 78.8
5.1 to 5.3
0.1 mg/m3 (£ Million)
209 to 414
638 to 650
0.05 mg/m3 (£ Million)
340 to 671
3,453 to 3,603
0.01 mg/m3 (£ Million)
515 to 1,015
12,024 to 14,663

The Setting and Use of Occupational Exposure Limits Current practice
The recommendation of the RIA for respirablecrystalline silica is that the current WEL of 0.3mg/m3 needs to be reduced, on the grounds of thehealth risks associated with this level of exposure.However, the RIA concluded that lowering the WEL to 0.01 mg/m3 or 0.05 mg/m3 would havemajor economic implications for UK industry andwould not be enforceable in all instances, givenlimitations in current sampling and analyticalmethods. Therefore, the RIA recommendation for a revised WEL (8-h TWA) of 0.1 mg/m3 was madefor respirable crystalline silica on the grounds ofsignificant health benefit at a level at whichindustry could meet the costs of compliancewithout major economic implications18.
It should be borne in mind that the use of RIA inthe process used to set OELs would only apply toregulatory authorities and governments thatconsider economic factors in addition to health-based factors in deriving their OELs.
5.5 Technical feasibility
The case study of silica (above) also illustratesissues about the impact of technical feasibility onOELs. The HSE RIA found that available samplingand analytical methods would not be sufficientlyrobust to determine compliance at the lower of thefour limits considered18.
5.6 Safety impact
5.6.1 Reducing and controlling exposures
It should be recognized that OELs, as such, donothing to protect workers from exposure tohazardous substances in the workplace. It is onlywhen they are applied (compliance and enforcement),as part of a broader framework of exposurecontrol, that they have any use. There are othermeans to reduce worker exposure to substancesthat must be applied.
In the UK, for example, COSHH regulations19
specify processes to minimize worker exposure tohazardous substances. For example, employerswho undertake work that is liable to exposeemployees to substances hazardous to health arerequired to provide to employees suitable andsufficient information, instruction and training,including information about the chemicals being
handled, appropriate precautions to be taken byemployees to safeguard themselves and theircolleagues, and the results of exposure monitoring and health surveillance activities.Principles governing control of exposure includethe use of a safer substitute (where available),hygiene measures, engineering controls,controlling exposure at source and, as a finalprotective measure, the use of personal protectiveequipment. This is broadly in line with theprovisions of the EU Chemical Agents Directive,which applies to all member states20.
Recognizing that it is not possible to assign aspecific OEL to every chemical in use, ‘ControlBanding’ is being developed as a complementaryapproach to protecting worker health21. Much of thedevelopment of control banding derives from theUK HSE COSHH Essentials, which provide web-based step-wise guidance for the control of healthrisks from chemicals22.
The principle of the COSHH Essentials is that, if theuser follows the guidance, then it is likely that theyare complying with good hygiene practice and thatany relevant OELs will be complied with. It alsocovers control advice on the very many substanceswithout specific OELs. Under COSHH Essentials,hazard assessment for the individual substancesdoes not rely on specific toxicological assessment,but on ‘hazard banding.’ The system does not caterfor carcinogens or respiratory sensitizers, forwhich expert advice is recommended22. To assist, inparticular, small and medium-sized enterprises indeveloping countries, the ILO has been developinga Workplace Chemical Control Toolkit, usingCOSHH Essentials as a model21.
In control banding, a chemical is assigned to a‘band’ for control purposes, based on hazardclassification and potential for exposure. Hazardclassification uses the EU Risk Phrases (Health and Safety Commission, 1999), which in Europe are assigned to potentially harmful chemicals, to allocate chemicals to one of six hazard groups (A–E for inhalation and S for skin). Potential forexposure is determined by the scale of use and theability to become airborne, including informationon whether the material is a gas, vapour or dust,and handling procedures. Based on these factors, a chemical is assigned to one of four controlstrategies21:• general ventilation (i.e. good industrial hygiene
practice);• engineering control (i.e. local exhaust ventilation);
50

The Setting and Use of Occupational Exposure Limits Current practice
• containment (i.e. enclosed process); or• specialist guidance.
Employing a similar good hygiene control strategy,the AIHA (Mulhausen and Damiano, 1998) alsopropose a hierarchy of control:• elimination of the process, equipment or
materials giving rise to the exposure;• substitution with a less hazardous process,
equipment or material;• engineering controls;• work practice controls and employee training;• administrative controls; and• proper selection fitting and use of personal
protective equipment.
In general, the two examples above demonstratethat, worldwide, there is good consensus on whatconstitutes good hygiene control to reduce workerexposure to hazardous substances in the workplace,although there may be subtle differences as to howOELs may be used.
5.6.2 Variability and susceptibility
Variability in the response of humans to occupationalor other exposures can be due to true differencesin exposure or it can be due to differences infactors such as toxicokinetic or toxicodynamicparameters, the impact of existing disease orinjury, or loss of physiological function or reserve.Variability describes the normal spread of valuesfor a biological parameter, such as lung function,or for a biological response, such as irritation.Variability may also describe factors such as age,gender, weight and genetic polymorphisms.Susceptible individuals may be those whoseresponse to an exposure falls at the extremes of a variability distribution curve. Susceptibility maybe related to immunological or genetic factors.How individuals that fall at the lower end of avariability curve or that are idiosyncraticallysusceptible should be treated is an importantfactor in risk management (IEH, 2002). These areimportant issues for the setting of OELs and haveto be reviewed in relation to occupational groupsand exposure to occupational toxicants.
5.7 Case studies
Descriptions for the establishment of OELs by fiveinternational authorities (EU SCOEL, German DFG,Netherlands DECOS, UK HSE4 and US ACGIH) havebeen included, where available, for the followingnine case studies of relevance to metal and miningindustries: nickel and nickel compounds, palladiumand palladium salts, lead, chromium metal and itstri- and hexavalent compounds, manganese,nitrogen dioxide, sulphur dioxide, sulphuric acidmists and silica. Summary tables for the setting of OELs for these case studies can be found inAnnex 1.
Metals provide a unique challenge when settingOELs owing to factors related to metal speciationand health risks. Similarly gases, mists andparticles of different size and physical form alsoadd other health parameters of concern owing todifferent deposition and absorption characteristicsin the respiratory tract and the potential for bothacute and chronic sequelae.
5.7.1 Nickel and nickel compounds
Nickel (CAS No. 7440-02-0) is a silvery-whitetransition metal with hard, malleable and ductileproperties. It is a trace element occurring in soils, air, water and the biosphere. The major use of nickel is in the production of stainless steeland other corrosion and heat-resistant alloys.Other uses include coinage, in alkaline batteries,magnets, welding rods and as catalysts forhydrogenation of fats. The soluble nickel compound,nickel sulphate (CAS No. 7786-81-4), is the mostimportant form of nickel in ambient air and itsprincipal use is in electroplating. Workers can beexposed to nickel dusts and fumes in a wide range of occupations spanning many industries.Exposure is associated with hypersensitivity andthe induction and maintenance of contact dermatitis.
51
4 UK OELs are reported herein as MELs and OESs, not as the recentlyadopted WELs.

The Setting and Use of Occupational Exposure Limits Current practice
OELsThe solubility of nickel metal and nickel saltsinfluences the toxic effects. For this reasonauthorities have set separate limits for differentnickel species. The ACGIH have established fourseparate 8-h TWAs for nickel and its inorganiccompounds, including nickel subsulphide: nickelmetal, 1.5 mg/m3; insoluble nickel compounds 0.2 mg/m3; soluble nickel compounds 0.1 mg/m3;and nickel subsulphide 0.1 mg/m3. All of therecommended TLVs are for inhalable nickelparticulate (ACGIH, 2003b). The UK HSE MELs (8-h TWA) are 0.5 mg/m3 for nickel metal andinsoluble inorganic nickel compounds and 0.1 mg/m3 for soluble inorganic nickel compounds.No MAK value has been established for nickelmetal or nickel compounds because of evidence forcarcinogenic effects from human or experimentalanimal studies (DFG, 2004). The German TRGS 900limits for metallic nickel, nickel sulphide andsulphide containing ores, nickel oxide and nickelcarbonate are 0.5 mg/m3, and the limit for nickelcompounds in the form of inspirable droplets is0.05 mg/m3. Nickel and nickel compounds are onthe priority list for SCOEL but no recommendationhas been made to date. DECOS have not set ahealth-based recommended OEL (HBR-OEL) fornickel but have published an evaluation of theeffects of nickel and its compounds onreproduction.
Key studies and critical effectsThe UK HSE published summary of the basis forthe MELs for nickel and insoluble inorganiccompounds (0.5 mg/m3 8-h TWA) and soluble nickelcompounds (0.1 mg/m3 8-h TWA) did not providereferences for the key studies used to identify thecritical effects on which the MEL recommendationswere based. The critical effects observed fromhuman studies were skin sensitization, causingdermatitis — commonly known as ‘nickel rash’,respiratory sensitization and non-malignant lungdisease. Studies in nickel refinery workers show anexcess risk from lung and nasal sinus cancers atexposure levels ranging from 5–400 mg/m3 (asnickel — specific forms stated to be unknown) butno association has been made at exposure levelsup to 1 mg/m3 (HSE, 2001).
The ACGIH recommended the TLVs for nickel (1.5 mg/m3 inhalable nickel particulate) based onthe potential for dermatitis and pneumoconiosisand for soluble compounds (0.1 mg/m3 inhalablenickel particulate) based on the potential forpulmonary damage, dermatitis and suspectedcancer risk. The key studies cited were the NTPstudies on selected nickel compounds, in rats andmice (NTP, 1996a; 1996b; 1996c). However, therewas no evidence of carcinogenicity following nickelsulphate inhalation (ACGIH, 2003b).
Uncertainty factorsIn the rationale for the ACGIH documentation forthe derivation of TLVs for nickel and soluble nickelcompounds, the key studies cited were the NTPstudies on nickel compounds (NTP, 1996a; 1996b;1996c), which found biological and histologicalchanges in rats and mice at 0.1–1.0 mg/m3, totalaerosol; however, it is not stated or apparent thatan uncertainty factor was used to account for dataextrapolation from animals to humans (ACGIH,2003b).
Overview for nickel and nickel sulphateNickel and nickel compounds are relevant to themining and metal industry. The toxic effects arerelated to the solubility of the compounds. TheACGIH and HSE have different OELs for nickelmetal (1.5 and 0.5 mg/m3 respectively) and thecritical effects on which these OELs were basedalso differed. The ACGIH and HSE set identicalOELs for soluble nickel compounds, but the criticaltoxic effects on which these were based differedbetween the two organizations, which makes acomparison of the rationale for the OELs difficult.
5.7.2 Palladium and soluble palladium salts
Palladium (CAS No. 7440-05-3) is a silvery-white,ductile metal with the lowest density and lowestmelting point of all the platinum group metals(ruthenium, rhodium, palladium, osmium, iridiumand platinum). The metal is known to absorbdifferent gases, most notably, hydrogen. Extraction of palladium from ores requires complex aqueous chemical processing and themetal is usually highly disseminated with otherplatinum metals in ores, such as nickel sulphites.Palladium is an important, powerful catalyst inindustry and is also used in dental and electricalindustries23. Palladium salts vary in solubility fromreadily soluble in water, such as palladiumdichloride (PdCl2), to insoluble in water, such aspalladium iodide (PdI2)24.
52

The Setting and Use of Occupational Exposure Limits Current practice
OELsNo OEL has been established for palladium and itscompounds by the SCOEL, DFG, DECOS, HSE orACGIH. The DFG have examined palladium and itscompounds but no MAK value is set because ofinsufficient toxicological information from humanand experimental animal studies (DFG, 2004).Consequently, this compound would be aninteresting substance on which to determinewhether the approaches used to set OELs bydifferent authorities could be harmonized.
5.7.3 Lead
Lead (CAS No. 7439-92-1) is a heavy, highly ductile,bluish-grey metal, which readily dulls in air. It ishighly dense, soft and malleable; it is resistant tocorrosion, has a low melting point (327.5°C) andopacity to gamma and X-rays. For these reasons,lead has been used in a wide variety of applications,such as in metal sheeting, in batteries andchemical manufacture and in the production ofalloys, such as solder, gun-metal and bullets. Lead is a rare metal in the earth’s crust and ismined from seam deposits around the world. It also occurs as sulphite ores, the most common is lead sulphide (galena), and extraction is bysmelting. As a consequence of legislation to banthe use of leaded petrol in industrialized countries,both environmental levels and blood leadconcentrations in the general population havedecreased. Occupational exposure to lead occursduring the mining of the metal, in the production of lead metal and its compounds, manufacture of batteries, and in the pottery, shipbuilding,construction, demolition and scrap industries (EC,2002).
OELsThe SCOEL recommendation for lead is 0.1 mg/m3
8-h TWA and the ACGIH TLV (8-h TWA) is 0.05 mg/m3 (EC, 2002). On the basis of evidence of carcinogenicity for soluble lead compounds in animals and inadequate evidence inepidemiological studies, lead is assigned an A3,‘confirmed animal carcinogen with unknownrelevance to humans’ notation by the ACGIH(2003a). In the UK, a limit of 0.15 mg/m3 has beenset but lead is regulated separately from all othersubstances under the ‘Control of Lead at Work’(CLAW) regulations (1998). The German DFG hasnot established a MAK value for lead but hasassigned a carcinogenicity notation 3B because in vitro or animal studies have shown evidence forcarcinogenic effects but no evidence for genotoxic
effects (DFG, 2004). No value has been establishedfor lead metal by the DECOS.
Key studies and critical effectsThe rationale for the SCOEL recommendation wasbased on the critical effect of central nervoussystem (CNS) disturbances observed in key studiesby Lai et al. (1997) and Kentner and Fischer (1993).The OEL based on avoiding CNS effects is alsoassumed to protect against the peripheral nervoussystem (PNS) and renal toxicity and possibly therisk from renal cancer (EC, 2002).
The HSE summary criteria for the OEL for leadstates that the limit was set on the basis of thecritical health effects of anaemia, followed byeffects on the nervous system and kidney damage.However, the key studies on which these criticaleffects were identified were not cited in thepublished summary document and the criticaleffects were discussed in relation to blood-leadconcentrations of 80 µl/l, at which point anaemiaoccurs, and 100 µl/l, at which point CNS effects and gastrointestinal symptoms become apparent.The rationale for the limit of 0.15 mg/m3 for leadwas set in conjunction with the blood-leadstandard, and it was recognized that therelationship between airborne lead concentrationsand blood-lead levels is not clearly established(HSE, 2001; 2003).
The rationale for the TLV-TWA of 0.05 mg/m3 set by the ACGIH for lead and its inorganic compoundswas based on the BEI for lead, since blood-leadconcentrations are more strongly related to healtheffects than atmospheric lead concentrations. The ACGIH identified blood dyscrasias, reducednerve conduction velocities, peripheralneuropathies, possible kidney dysfunction, alteredspermatogenesis, impaired intellectual developmentin children exposed in utero and carcinogenicity asadverse health effects. The recommended TLV isintended to minimize the risk from these collectivetoxic effects; no single study was selected as key tothe TLV recommendation (ACGIH, 2003b).
Uncertainty factorsThe SCOEL and ACGIH have not stated the use ofuncertainty factors in their documents for the basisof their occupational and biological exposure limits.
53

The Setting and Use of Occupational Exposure Limits Current practice
Overview for leadThe lowest OEL was set by the ACGIH, which alsohad a comprehensive rationale for the basis of therecommendation. The HSE and ACGIH adoptedsimilar approaches in recommending that theairborne OEL be based on the biological exposurelimit for lead because blood lead concentrationsare more closely related to adverse health effects.SCOEL recommend that the setting of an OEL forlead is more difficult than other substancesbecause only part of occupational exposure occursvia inhalation.
5.7.4 Chromium
Chromium (CAS No. 7440-47-3) occurs naturally inthe earth’s crust as chromite, a substance fromwhich all chromium compounds and chromiummetal are derived. Chromium exists in manyoxidation states; however, in occupational use,most commonly found are the trivalent andhexavalent forms, such as chromates anddichromates. Chromium metal (O) is used in theproduction of stainless steel and other alloys(Arbetslivsinstitutet, 2000). Chromium (VI)compounds are used in plating and anodisingsolutions, in the production of pigments and dyes,tanning agents, wood preservatives, photographicsensitizers, and as catalysts in certain refractorymaterials. Trivalent chromium (as found inchromite ore) is a naturally occurring, essentialtrace element. For healthy adults, the UK ExpertVitamin and Mineral Group (EVM) for upper safetylimits have recommended a guidance level of 0.15 mg/kg bw/day for dietary intake of chromium(III) and the Committee on Medical Aspects of Foodand Nutrition Policy (COMA) report recommendsabove 0.025 mg/day for adults. Chromium (VI)compounds have variable water solubility, rangingfrom highly soluble to virtually insoluble, and thisinfluences their bioavailability and hence toxiceffects.
OELsThe US ACGIH and UK HSE have similarapproaches and have set the same 8-h TWA TLVsor OESs for chromium metal and trivalentcompounds (0.5 mg/m3) and a lower 8-h TWA TLVor MEL of 0.05 mg/m3 for hexavalent compoundsowing to strong evidence for serious health effects(HSE, 2002). The German DFG has not establishedOELs for chromium and its compounds since it isnot their policy to establish OELs when there isgood evidence for a human cancer risk but solublechromium (VI) compounds have been assigned withan ‘S’ notation because of evidence for human skinsensitization (Greim, 1996). For hexavalentchromium compounds the German TRGS 900 listsTRKs of 0.005 mg/m3 and 0.1 mg/m3, for specificworkplaces.
The DECOS have no HBR-OEL for Cr metal dustand insoluble Cr(III) compounds owing to lack oftoxicological data. The 8h-TWA HBR-OEL forsoluble Cr(III) and Cr(IV) compounds (as inhalabledust) are 0.06 mg/m3 and 0.05 mg/m3, respectively.No HBR-OEL value was set for Cr(VI) compoundsalthough a thorough assessment of the health riskswas made and an estimation of the additionalcancer mortality risk was derived by thecommittee. All the health-based limits forchromium do not include workers sensitized tochromium, who are perceived as being at extrarisk. DECOS recommend that sensitized individualsshould not be placed in employment that could putthem at risk of chromium exposure (Dutch ExpertCommittee on Occupational Standards, 1992).
Key studies and critical effectsThe key study used by DECOS to derive the HBR-OEL for soluble Cr(III) compounds was a study byJohansson et al. (1987) in which a minimalobserved adverse effect level (MOAEL) of 0.6 mg/m3
was identified in rabbits. A study by Lee et al.(1989) was used to identify a LOAEL of 0.5 mg/m3
for the critical effect of minute fibrotic pleuritis inrats exposed to Cr(IV) compounds during a 2-yearinhalation study. The critical effect of Cr(VI)compounds is lung carcinogenicity, as identified inepidemiological studies, lung cancer cases listedby Langård (1990), and animal carcinogenicitystudies and mutagenicity tests. DECOS used theMancuso (1975) study to estimate an additionalcancer mortality risk of 4 x 10-3 after 40 years ofoccupational exposure to 2 µg/m3 as inhalable dust.
54

The Setting and Use of Occupational Exposure Limits Current practice
The UK HSE identified carcinogenicity, sensitizationand the ability to cause ulcers as the critical healtheffects for chromium (VI) compounds and based theMEL on these and the absence of no-effect levels.Key studies were not cited in the publishedsummary rationale for setting the limit (HSE, 2001).
The ACGIH adopted a TLV (8-h TWA) of 0.5 mg/m3
for chromium metal in 1931, which has remained,based on the lack of adverse health effects inworkers from chromium industry. However,reference was made to reviews by the IARC (1990)and the HSE (1989), which concluded that owing toinadequacies in studies, there is insufficientinformation to assess the carcinogenicity ofmetallic chromium; an A4 notation, ‘not classifiableas a human carcinogen’, was assigned (ACGIH,2003a). The TLV (8-h TWA) for chromium (III)compounds is also 0.5 mg/m3, based on reports ofdermatitis in workers exposed to trivalentchromium compounds by Freget and Horsman(1964) and changes of low pathophysiologicalsignificance in animal inhalation studies byHenderson et al. (1979) and Johansson andcolleagues (Johansson, 1986a; 1986b; Johansson et al., 1987). The TLV (8-h TWA) for solublechromium (VI) compounds is 0.05 mg/m3, based onevidence from animal studies for non-carcinogeniceffects (Laskin et al., 1969) and kidney damage(Major, 1922; Hunter and Roberts, 1933). The TLV (8-h TWA) for soluble chromium (VI) compounds is 0.01 mg/m3 on the basis of the large body ofevidence for lung cancer in chromium workers(Machle and Gregorius, 1948; WHO, 1988; ATSDR,1989; HSE, 1989; IARC, 1990). ACGIH has alsoadopted BEIs for chromium (VI), as total chromiumin urine, of 25 µg/l at the end of shift at the end of a workweek and 10 µg/l increase during a shift(ACGIH, 2004a). More recently, the HSE hasadopted a BMGV of 10 µmol chromium/molcreatinine in urine, with a post-shift sampling time(HSE, 2005b).
Uncertainty factorsDECOS applied an uncertainty factor of 10 to theHBR-OELs for soluble Cr(III) and Cr(IV) compounds.These factors were comprised of two factors of x 3— one to allow for extrapolation from animal datato humans and one because a LOAEL or MOAELwas used as a starting point rather than a NOAEL.The use of uncertainty factors was not applicable tothe risk evaluation of Cr(VI) compounds (DutchExpert Committee on Occupational Standards,1992).
The use of uncertainty factors was not stated andcould not be inferred from the publication for thebasis of the US TLV-TWA for chromium metal andchromium compounds (ACGIH, 2003a).
Overview for chromiumChromium is an interesting substance for a casestudy because it has various oxidation states andsolubilities, and hence various toxicities. It istherefore necessary to evaluate chromium metal,trivalent and hexavalent compounds separately andmost authorities assigning OELs have addressedthis important issue of speciation. There isagreement between the ACGIH TLV and the HSEOES for chromium metal and chromium (III)compounds (8-h TWA 0.5 mg/m3). There is alsoagreement between the limits for chromium (VI)compounds (8-h TWA 0.05 mg/m3) although theUSA also has a separate, lower TLV (8-h TWA) of0.01 mg/m3 for insoluble compounds. The lack of aDFG MAK value is based on the genotoxicity ofchromium (VI) compounds and the absence ofthreshold effects associated with lungcarcinogenicity. Given that there is no threshold fora carcinogenic substance, DECOS has taken theapproach of deriving an additional cancer mortalityrisk estimate for Cr(VI) compounds.
5.7.5 Manganese
Manganese (CAS No. 7439-96-5) is a Group VIIbtransition metal; it exists in several oxidation states(II, III, IV, VI and VII) and forms a range of inorganicand organometallic compounds. Most OELsconsider the inorganic forms of the metal.Manganese occurs naturally and is mined for usein the production of ferrous and non-ferrous metalalloys, including those essential to steel making.Iron and steel production account for 85–95% of themanganese market. Manganese is an essentialelement; it is involved in bone formation and aminoacid, cholesterol and carbohydrate metabolism; itis a component of several enzymes and activatesothers. For healthy adults, estimated acceptable oradequate dietary intakes range from 1–12.2 mgmanganese/day (IEH, 2004).
55

The Setting and Use of Occupational Exposure Limits Current practice
OELsCurrent OELs (8-h TWA) in the USA, Germany, and UK are 0.2, 0.5 and 0.5 mg/m3, respectively(HSE, 2003). A recently published criteria documentfor inorganic forms of manganese, which wasproduced for consideration by the SCOEL, proposeda limit of 0.1 mg/m3 for respirable manganese, withan additional limit of 0.5 mg/m3 for inhalablemanganese (IEH, 2004).
Key studies and critical effectsThe key studies used to make the recommendationin the IEH (2004) criteria document for SCOEL wereby Roels et al. (1992), in which subtle neurologicaleffects were observed in approximately 15% ofworkers exposed to 0.2 mg/m3, Gibbs et al. (1999),in which no effect was observed at an averagerespirable concentraion of 0.04 mg/m3, and Myerset al. (2002), in which no effect was observed at 0.2 mg/m3 (equivalent to 0.04–0.08 mg/m3
respirable concentration). The criteria documentconcluded that limiting exposure to 0.1 mg/m3 forrespirable manganese would prevent most workersfrom developing small, non-clinical decrements inmotor neurobehavioural function. The 0.5 mg/m3
limit for inhalable manganese was proposed as asafeguard against significant exposures fromgastrointestinal routes, subsequent to inhalation.However, it was noted that there was insufficientevidence to evaluate the effects over a workinglifetime. It was also considered that measurementsof workplace concentrations in air should bepossible at the level proposed, and that neither ashort-term limit nor skin notation was necessary(IEH, 2004).
Derivation of the German MAK value was alsobased on the critical toxic effects to the CNS foundin the studies by Roels and Lauwerys (Roels et al.,1987a; 1992) and in studies by Wennberg, Iregrenand colleagues (Iregren, 1990; Wennberg et al.,1991; 1992) and Mergler et al. (1994). The lowestaverage concentration shown to cause slightneurotoxic syptoms was approximately 0.25 mg/m3.However, given concerns about different samplingand measurement techniques in different locations,the MAK value was set at 0.5 mg/m3 for total dust(Greim, 1999). The German OELs for the inhalablefraction of manganese have been classified with apregnancy risk group rating C; that is, no reason tofear a risk of damage to the embryo or fetus whenMAK and BAT values are observed (DFG, 2004).
The HSE replaced the 2002 OES (8-h TWA) of 5 mg/m3 for manganese and its inorganiccompounds with an MEL of 0.5 mg/m3 (8-h TWA) in2003 (HSE, 2003). The rationale for the OES waswithdrawn but to date no documentation has beenpublished to replace this.
The rationale for the 0.2 mg/m3 ACGIH TLV-TWA for manganese was also based on CNS effects and manganism, from the same studies as thoseconsidered by IEH and Germany, and lung andreproductive effects (Lauwerys et al., 1985; Roelset al., 1987a; 1992). ACGIH concluded that thelowest exposure concentration of manganese atwhich early effects on the CNS could be detectedwas unknown and therefore the TLV was chosen as the recommended level at which the potentialfor pre-clinical adverse effects in the lungs andCNS and adverse effects on the fertility of maleworkers are reduced (ACGIH, 2003b).
Uncertainty factorsIn the IEH (2004) criteria document, no uncertaintyfactor was used to derive the proposed levelsbecause the recommendations were based onhuman data and non-clinical endpoints onlydetectable using specific test procedures. Similarly no uncertainty factor was used in theGerman MAK evaluation (Greim, 1999), and ACGIH(2003b) gives no information on the use ofuncertainty factors in the derivation of the TLV.
Overview for manganeseIn summary, manganese has been chosen as acase study because of its essentiality and becauseit has a threshold, albeit the subject of debate, forits neurotoxic effects. The OELs for Germany, UK,and the USA, and in the recent criteria documentfor SCOEL are comparable, with similar criteriabeing used in their derivation. The IEH criteriadocument for manganese gave the clearestrationale for a limit of 0.1mg/m3 and may be usedas a basis for a forthcoming SCOELrecommendation.
56

The Setting and Use of Occupational Exposure Limits Current practice
5.7.6 Nitrogen dioxide
Nitrogen dioxide (NO2; CAS No. 10102-44-0) is areddish-brown gas that is produced naturally bybacteria, volcanic activity, lightning and oxidation ofnitric oxide (NO) in the atmosphere. Sources of NO2
from human activity include diesel exhaust,cooking/heating with non-vented gas appliancesand tobacco smoke (Dutch Expert Committee onOccupational Standards, 2004). NO2 is mainly usedas an intermediate in the formation of NO, but alsoas a nitrating or oxidising agent, for example inrocket fuels, and as a catalyst for sulphuric acid.The route of exposure most relevant to the miningindustry is during the use of dynamite, but workersfrom the chemical and gas welding industries arealso exposed (Dutch Expert Committee onOccupational Standards, 2004).
OELsThe UK HSE OES for NO2 of 5.7 mg/m3 (8-h TWA)and 9.6 mg/m3 (15-min STEL) were withdrawn in2003 (HSE, 2002; 2003) on the grounds that theywere ‘unsafe’ owing to ‘evidence to show thatinhalation exposure at that level on a day to daybasis would cause various degrees of harm toworkers’ health’25. It is not clear if the HSE haveplans to introduce a new WEL for NO2. However,the US ACGIH TLV-TWA (8-h) of 5.6 mg/m3 andSTEL of 9.4 mg/m3 are similar to the HSE, whichsuggests that perhaps the TLVs need review.
The standards recommended by DECOS are 0.4 mg/m3 (8-h TWA) and 1.0 mg/m3 (15-min STEL),which are considerably lower than the ACGIH TLVs (Dutch Expert Committee on OccupationalStandards, 2004). The German DFG has notestablished a MAK for NO2 and has classified it with a 3B notation. The rationale for the DFGevaluation is based on genotoxic effects in vitro,suspected genotoxicity in vivo, tumour promotingactivity and the analogy to the mechanism of action of ozone (DFG, 2005a; 2005b).
Key studies and critical effectsThe database used to derive the DECOS, 8-h TWAHBR-OEL lacked epidemiological data so thecommittee used the large number of animalstudies as a basis for the recommended limit. The critical effect involved the respiratory tract andincludes increased airway resistance, enhancedsusceptibility to bacterial or viral airway infectionsand long-term irreversible damage to the lungtissue. The lowest-observed-effect level (LOEL)
from robust animal studies was 0.96 mg/m3,although a LOEL of 0.65 mg/m3 was identified inless robust studies showing morphological changesto the lungs. The 15-min HBR-OEL for NO2 wasbased on the complete set of human data fromsingle-exposure studies, which determinedsignificant toxicological effects on lung functionand increased airway resistance at concentrationsas low as 2.9 mg/m3 (Frampton et al., 1991).However, taking the collection of studies as awhole, the recommended STEL was based on theNOAEL of 1 mg/m3 (Dutch Expert Committee onOccupational Standards, 2004).
The key studies used to derive the ACGIH TLV wereearly studies in humans and animals. In particular,Kosmider et al. (1972) reported slight changes inpulmonary vital capacity in workers exposed to NO2
at 0.4–2.7 ppm (0.8–5.2 mg/m3). The ACGIH (2003b)assigned the A4, ‘not classifiable as a humancarcinogen’, notation to NO2, based on a lack ofevidence for carcinogenicity in animal studies byWagner and colleagues and Freeman andcolleagues (Wagner et al., 1965; Freeman et al.,1966; 1968).
Uncertainty factorsThere was no stated use of uncertainty factors inthe published rationales for the ACGIH TLV. No overall uncertainty factor was used by DECOS to derive the 8-h TWA HBR-OEL because theuncertainty from intraspecies differences iscounterbalanced by the uncertainty arisingbetween the continuous exposure of theexperimental animals in studies used to derive theOEL and the shorter duration of exposure for aworker (8h/day, 5d/week). No uncertainty factor forinterspecies differences was used because theNOAEL derived from animal studies was within anarrow concentration range for three differentspecies. No uncertainty factor for intraspeciesdifferences was used for the STEL HBR-OELbecause the NOAEL used to derive the limit camefrom a large and consistent database of humanstudies (ACGIH, 2003b; Dutch Expert Committee onOccupational Standards, 2004).
Overview for nitrogen dioxideThere is a lack of consistency in both the value andthe approach used to set OELs for NO2 and theissue of what was practical for industry has guidedthe establishment of historical values. The limit setby DECOS represents the most robust rationale fora health-based limit.
57

The Setting and Use of Occupational Exposure Limits Current practice
5.7.7 Sulphur dioxide
Sulphur dioxide (SO2; CAS No. 7446-09-5) is awater-soluble, non-flammable, colourless gas or liquid with a pungent, suffocating odour. The presence of SO2 in the atmosphere resultsfrom anthropogenic activity and natural sources.Anthropogenic sources include the burning of coaland fuel oils, production, refining and use ofnatural gas and petroleum, and natural sourcesinclude sea spray, volcanic activity, decompositionof biological matter and anaerobic microbiologicalactivity. SO2 is mainly used as a catalyst or as areducing or oxidising agent in many differentcommercial uses including the pulp and paper,petroleum and food industries. In the mineralindustry, SO2 has several applications: as flotationdepressants for sulphide ores; to pre-reduce ferricto ferrous ions during the electro-winning ofcopper from leach solutions containing iron; toinitiate precipitation of metallic selenium fromselenous acid; as a by-product of coppermetallurgy; and to reduce hexavalent chromium to its less toxic trivalent form in chrome wastedisposal. Workplace exposures to SO2 relevant tothe metal industry arise in the production of steel,copper, nickel, zinc, cobalt, aluminium and othermetals, when sulphidic ores or sulphuric impuritiesof the ores are sintered, roasted or melted (IARC,1992b).
OELsThe UK HSE 8-h TWA OES of 5.3 mg/m3 and the 15-min STEL OES of 13 mg/m3 were withdrawn in2003 (HSE, 2002; 2003) on the grounds that theywere ‘unsafe’ owing to ‘evidence to show thatinhalation exposure at that level on a day-to-daybasis would cause various degrees of harm toworkers’ health25. It is not clear if the HSE haveplans to introduce a new WEL for SO2. The USACGIH 8-h TWA-TLV of 2 ppm (5.3 mg/m3) and 15-min STEL of 5 ppm (13 mg/m3) are identical tothe withdrawn HSE OELs, which suggests thatperhaps the TLVs need review.
DECOS recommends a 15-min STEL of 0.7 mg/m3
(no 8-h TWA HBR-OEL has been established forSO2, owing to lack of long-term exposure animalstudies and epidemiological studies) and identifiesworkers with asthma and, possibly, workers withischaemic heart disease as ‘at risk’ groups (DutchExpert Committee on Occupational Standards,2003b).
The German DFG has set a MAK value of 1.3 mg/m3
for SO2 (DFG, 2005b; 2005c).
Key studies and critical effectsThe DECOS HBR-OEL STEL (15-min TWA) of 0.7 mg/m3 was based on the critical effect of anincreased susceptibility to airway infections andchronic irritation. The key studies used to identify a NOAEL of 2.0 mg/m3 were short-term inhalationstudies in humans by Stacy et al. (1983) andSchachter et al. (1984). In both studies, theparticipants took moderate exercise sessions andlung function tests were performed before andafter exposure for four hours and 40 minutes,respectively (Dutch Expert Committee onOccupational Standards, 2003b).
The German MAK value is based on human datathat show no effect on lung function in volunteerstudies after 2-hour exposures to 0.5 ppm(Schachter et al., 1984) or in workers exposed tolong-term average concentrations of 0.67 to 0.78 ppm (Broder et al., 1989; Kremer et al., 1994;1995).
The critical effect used to derive the ACGIH TLV forSO2 was a human study, reported in a publicationby the US Department of Health, Education andWelfare, in which bronchoconstriction occurredfollowing inhalation at 5 ppm or more (DHEW,1969). The ACGIH assigned an A4, ‘not classifiableas a human carcinogen’ notation to SO2, based onevidence for cocarcinogenic action, although Laskin et al. (1976) reported an absence ofsquamous cell carcinomas in the respiratory tractof rodents (ACGIH, 2003b).
Uncertainty factorsDECOS (Dutch Expert Committee on OccupationalStandards, 2003b) used an uncertainty factor of 3 toadjust for interindividual differences owing to thelimited number of participants in the key studies(Stacy et al., 1983; Schachter et al., 1984) and datashowing variation in studies by Islam et al. (1992;1994). There is no mention of the use of uncertaintyfactors in the rationale for the basis of the ACGIHTLVs for SO2 (ACGIH, 2003b).
58
The Setting and Use of Occupational Exposure Limits Current practice
Overview for sulphur dioxideThe OELs for SO2 differ between authorities. The ACGIH TLV recommendation was based on datafrom before 1977. More recent studies have shownthat this limit may be unsafe and the UK HSE haswithdrawn its comparable OES for SO2. The DECOShas the most comprehensive rationale for the HBR-OEL for SO2 but this is a STEL (15-min TWA) only.The database for health effects in both humans andanimals is limited, particularly regarding long-termexposures and long-term concentration–responserelationships. These data are required to establishan 8-hr TWA OEL.
5.7.8 Sulphuric acid mists
Sulphuric acid (H2SO4; CAS No. 7664-93-9) is adense, oily, odourless liquid that is colourless whenpure but may be dark brown. It is a stronglycorrosive, non-flammable, dehydrating reagent thatreacts exothermically with water and alcohol(ACGIH, 2001). Sulphuric acid is used in a diverserange of industries, such as in the manufacture offood, glue, dyestuff, parchment and petroleum, andit is used as a battery electrolyte and forelectroplating. Of greater relevance to the miningand metal industry, sulphuric acid is used innonferrous metallurgy, copper, zinc, iron and steelproduction and as a leaching agent during theextraction of uranium and copper from ore26.
OELsCurrent 8-h TWA OELs in Germany and the USA are0.1 and 0.2 mg/m3, respectively. The UK HSE 8-h TWA OES of 1 mg/m3 was withdrawn in 2003(HSE, 2002; 2003). It is not clear if the HSE haveplans to introduce a new WEL for sulphuric acid.
Key studies and critical effectsThe MAK value classification was based on thecritical effect of changes to mucociliary clearance,in humans, at concentrations of 0.3 mg/m3.Owing to the lack of data in humans on the effectsof long-term exposure, the MAK value was reducedto 0.1 mg/m3. Based on studies in mice and rabbits(actual studies unspecified), the NOEL forembryotoxic effects is 5 mg/m3; therefore the MAKvalue is thought to be sufficient to protect againstprenatal toxic effects. There is no experimentalevidence to suggest mutagenicity, genotoxicity,carcinogenicity or tumour-promoting effects and noevidence to suggest sensitizing effects fromsulphuric acid mists (Greim, 2001).
DECOS have classified sulphuric acid mists ascarcinogenic, based on evidence from the availableepidemiological studies showing an associationbetween workers exposed to inorganic mistscontaining sulphuric acid and laryngeal cancer(Dutch Expert Committee on OccupationalStandards, 2003a). DECOS considered supportingevidence from animal studies was limited, since alifetime study in hamsters exposed to 100 mg/m3
showed no carcinogenic effects. The committeeconcluded that sulphuric acid mist acts as a non-stochastic genotoxic carcinogen and thereforerecommended that an exposure limit be derivedusing a threshold model; however, a limit is yet tobe set.
The US ACGIH TLV (8-h TWA) of 0.2 mg/m3
(thoracic particulate mass; ACGIH, 2004b) is basedon altered tracheobronchial particle clearancemechanisms among normal and asthmaticvolunteers (Leikauf et al., 1981; Lippmann et al.,1982; Leikauf et al., 1984; Lippmann et al., 1987;Spektor et al., 1989) and on pulmonary functionchanges among asthmatic individuals at levelsabove about 350 µg/m3 (Koenig et al., 1985; Utell etal., 1989). The ACGIH have issued sulphuric acidwith a TLV carcinogenicity notation of A2,‘suspected human carcinogen’, based on thepossibility of an association between laryngealcancer and exposure to sulphuric acid, and stronglyrecommend that further studies be considered(ACGIH, 2003a).
Uncertainty factorsThe German MAK value appears to haveincorporated an uncertainty factor of 3 to allow forlack of knowledge about long-term effects (Greim,2001). No other authority used uncertainty factorsin the process to establish OELs.
Overview for sulphuric acid mistsThe German MAK value and US TLV are similar andboth are based on changes to mucociliaryclearance in humans.
59

The Setting and Use of Occupational Exposure Limits Current practice
5.7.9 Silica (crystalline)
Quartz is found in almost all types of rock, sands,clays, gravels and shales and is, therefore,particularly relevant to the mining and quarryingindustries, such as black coal and ore mining.Many different forms of crystalline silica exist inthe occupational setting including crystallinecristobalite (CAS No. 14464-46-1), crystallinequartz (CAS No. 14808-60-7), crystalline tridymite(CAS No. 15468-32-3) and crystalline tripoli (CASNo. 1317-95-9). Exposure to crystalline silica hasbeen identified as the cause of the lung diseasesilicosis, a slowly progressive, irreversible disease that takes years to develop and whichcauses fibrous nodules to develop in the lungs.Much recent debate has centred around theevidence as to whether silica is able to cause lungcancer in non-silicotics as well as silicotics and inwhich occupational settings such risks may occur(IARC, 1997).
OELsThere is no German MAK value for crystalline silica(respirable quartz, cristobalite and tridymite dust).Quartz has been classified in carcinogenic category1, and the DFG propose that reducing silicosisamong workers would decrease the incidence oflung cancer (Greim, 2000).
DECOS have set an health-based limit (HBR-OEL8-h TWA) for crystalline silica (quartz, cristobaliteand tridymite) of 0.075 mg/m3 (Dutch ExpertCommittee on Occupational Standards, 1992).
The UK HSE 8-h TWA MEL for respirable crystallinesilica dust is 0.3 mg/m3 (HSE, 2002). The rationalefor setting this limit was influenced by the levelreasonably practicable for industry. However, thislevel is currently under review by ACTS becausecurrent evidence suggests that an MEL of 0.3 mg/m3 is not sufficient to protect workers fromlung disease. The WEL for respirable crystallinesilica remains at 0.3 mg/m3 until a proposal toreduce the value to 0.1 mg/m3 (8-h TWA) has beenformally agreed but HSE believes that the new WELis reasonably practicable for industry to meet.
In 2002, the SCOEL issued a recommendation tothe EC that, to control against silicosis, the OEL forrespirable crystalline silica should be reduced to0.05 mg/m3 (8-h TWA; HSC, 2005b).
The ACGIH had evaluated four substancescontaining crystalline silica separately andassigned a TLV at 0.05 mg/m3 (8-h TWA) forcristobalite (respirable particulate fraction), quartz(respirable) and tridymite (respirable particulatefraction) and at 0.1 mg/m3 of contained respirablequartz particulate (8-h TWA) for tripoli. However,the documentation and TLV for tripoli werewithdrawn in the 2005 NIC and crystalline silica(quartz and cristobalite) is subject to an NIC.Furthermore, the ACGIH have assigned thecarcinogenicity notation A2, ‘suspected humancarcinogen’ (ACGIH, 2003a). The NIC for quartz andcristobalite is 0.025 mg/m3 as respirable fraction.Australia after long debate has adopted an OEL of0.1 mg/m3 (Klerk et al., 2002).
Key studies and critical effectsIn support of the German MAK classification, anevaluation of nine relevant epidemiological studiesfound evidence for an excess of deaths in workersexposed to respirable dust of crystalline silicacompared to the general population. Although itwas concluded that an association betweenexposure to quartz or cristobalite is associated withincreased relative lung cancer risk, the mechanismfor this was unclear. It was proposed that impairedpulmonary clearance in workers with silicosiscould promote the development of lung cancerbecause of inadequate clearance of other lungtoxins. Evidence to support the carcinogenicity ofcrystalline silica was provided by studies in rats,where exposure to quartz via inhalation has beenassociated with an increase in the incidence of lungtumours but a similar effect has not been producedin studies using other rodents, such as hamstersand mice (Greim, 2000).
DECOS has designated quartz silica as a non-stochastic genotoxic carcinogen, with theimplication that quartz has a threshold of effect(Dutch Expert Committee on OccupationalStandards, 1998). The critical health effects havebeen identified as silicosis and lung cancer. The keystudy that identified a NOAEL of 0.075 mg/m3 forsilicosis was a mortality study of granite workersby Costello and Graham (1988). A significantlyincreased incidence of lung cancer was associatedwith long-term exposure to respirable quartz at0.16 mg/m3 but not at 0.05 mg/m3 (Guènel et al.,
60

The Setting and Use of Occupational Exposure Limits Current practice
1989). The HBR-OEL (8-h TWA) for respirablequartz dust was set at 0.075 mg/m3 on the basis ofthe NOAEL for silicosis. This limit for quartz is alsoused for tridymite and cristobalite because DECOSstate that data for these substances are too limitedto derive separate limits (Dutch Expert Committeeon Occupational Standards, 1992).
The UK HSE MEL for respirable crystalline silicadust is based on the critical human health effect ofsilicosis although a NOEL has not been established.Exposures to a level of 1 mg/m3 are associated withhealth effects that may start as silicosis but thenprogress to massive fibrosis (HSE, 2001; 2002; 2003).
The critical effects for the ACGIH TLV-TWA of 0.05 mg/m3 for crystalline silica (quartz, cristobaliteand tridymite) were fibrosis and silicosis. The TLVis set in recognition that fibrosis in workersexposed at levels near 0.1 mg/m3 is not detectableby X-ray analysis and concern that fibrosis fromsilicosis is a risk factor for lung cancer, asidentified in key studies by Hnidzo and colleagues(Hnizdo and Sluis-Cremer, 1993; Hnizdo et al.,1993). The ACGIH assigned crystalline silica withthe carcinogenicity notation A2, ‘suspected humancarcinogen’, owing to the lack of epidemiologicalevidence for an increased risk of lung canceramong workers without silicosis and the lack ofstrong evidence for carcinogenicity in animals. The only positive finding came from inhalationstudies in rats, which the ACGIH noted are a poormodel for effects in humans (ACGIH, 2003b). The quartz OEL, in particular, was based on theconcept that the magnitude of toxicity isproportional to the quantity of quartz in the dust.The ACGIH rationale also recognizes that this TLVis subject to uncertainties regarding the quality ofthe epidemiological database and advises thatexposures should be as low as possible below thislimit.
Uncertainty factorsThe DECOS and ACGIH have not stated the use ofuncertainty factors in their documents for the basisof deriving OELs for crystalline silica.
Overview for crystalline silicaThe US TLV of 0.05 mg/m3 is the lowest limit forcrystalline silica, based on data from studiespublished in 1993. The Dutch HBR-OEL of 0.075 mg/m3 has a rationale published in 1992 andtherefore does not consider the data used by theACGIH. While current HSE OELs are based on pastfeasibility of measurement, new recommendationsare in place and a new standard is under review27.The absence of a MAK value is in keeping with theDFG policy on carcinogenic substances.
In summary, there is some discrepancy betweenthe values and rationales used to set these OELsalthough there is a trend amongst authorities toreduce exposures to the lowest level reasonablypracticable. Silicosis is a key feature in theevaluations of all standard setting organizationsreviewed above.
5.7.10 Overall summary on case studies
The case studies review the approaches used byfive different authorities to derive OELs forsubstances of particular relevance to the miningand metal industries. The UK HSE, German DFGand EU SCOEL set legally binding OELs, and insetting them a review committee takes into account economic and technical feasibility factorsas well as health-based recommendations. The Netherlands DECOS and US ACGIH set health-based OELs, but in the Netherlands, forexample, the Ministry of Social Affairs andEmployment evaluates the DECOS HBR-OELs inconjunction with feasibility data from the SocialEconomic Council, before legally binding OELs areset. Consequently, OELs are practical limits, a factthat contributes further to variability betweendifferent countries.
No one authority has more or less conservativeOELs and the use of key studies, critical effects anduncertainty factors is very variable. There is a lackof transparency in some of the publishedrationales. Often, the limits themselves and thesupporting documents are several years old, andsome might be reviewed in the light of more recentdata. The case studies, therefore, illustrate theneed for greater transparency and a moreconsistent approach when deriving health-basedlimits.
61

The Setting and Use of Occupational Exposure Limits Current practice
For countries within the EU, OELs should comply with EU legislation, which is based onrecommendations from SCOEL. SCOELrecommendations could be used as a foundationfor steps towards harmonization betweenauthorities on a global scale. Historically, bothwithin and outside the EU, there has been a degree sharing of both OELs and approaches in the setting of OELs. For example, the AustralianNOHSC has made use of the ACGIH TLVs and iscognisant of the approaches used by the UK HSEand German DFG in deriving their national limits(NOHSC, 1999).
62

A Harmonized Approach6.1 Initiatives on harmonization 64
6.1.1 Harmonizing review activities 646.1.2 Initiatives on a minimum data set 646.1.3 Harmonizing approaches to developing occupational
exposure limits for sensory irritants 646.2 Benefits of harmonization 646.3 Good practice in identifying and handling hazards 656.4 Recommendations for harmonization 65
6.4.1 Reviewing the literature 656.4.2 Risk assessment 66
6.5 Proposed code of practice for setting occupational exposure limits 66

The Setting and Use of Occupational Exposure Limits Current practice
6.1 Initiatives on harmonization
Harmonization does not mean standardization; that is, it is not to be expected that all jurisdictionsshould use identical approaches and generateidentical standards, rather differences inapproaches should clearly reflect identifiabledifferences in scientific policy or scientificjudgement, which should be communicated in atransparent manner. (e.g. Haber and Maier, 2002).
6.1.1 Harmonizing review activities
The work of the NEG (Section 5.2.4, above), inpreparing scientific criteria documents to underpinOEL setting, already exemplifies a harmonizedapproach to the evaluation of scientific databetween the five countries concerned.Implementation of proposals, for example betweenNEG, DECOS and the US NIOSH, to write jointcriteria documents would further promoteharmonization at this level (Lundberg, 1991). This only involves seven countries, but thisprinciple could be extended to encompass manyothers. In practice, there is already intensiveinteraction between the different European nationalcommittees, the SCOEL and the US TLV committee.For example, members of DECOS are alsomembers of the German DFG committee, membersof the DFG committee attend the TLV committeeand members of the major European nationalcommittees are members of SCOEL. The result isan extensive exchange of original publications anddocuments so that the data from which thedifferent committees derive their OELs are more or less the same.
6.1.2 Initiatives on a minimum data set
Requirements for a minimum data set for thedevelopment of OELs have been discussed. While itmight be thought that the absence of a minimumdata set would reduce confidence in the ability toprovide any meaningful guidance, the absence ofany OEL, even one based on limited information, isnot helpful in the occupational situation. It hasbeen proposed that a strategy for communicatingthe strength of the evidence used in deriving anOEL could be helpful (Haber and Maier, 2002).
6.1.3 Harmonizing approaches to developingoccupational exposure limits for sensory irritants
Most OEL setting groups in Europe and the ACGIHappear to use similar approaches to dealing withsensory irritants, and there have been recentefforts to further harmonize approaches(Paustenbach, 2001; Triebig, 2002), including arecent workshop sponsored by the MAK28.SCOEL has established a set of criteria to helpensure greater consistency in approaches tosetting OELs for sensory irritants (Meldrum, 2001).As sensory irritation will continue to be animportant aspect of OEL setting for manysubstances, at least for short-term exposure limits, this could be one area where harmonizationwould be extremely helpful.
6.2 Benefits of harmonization
The value of harmonizing approaches to settingOELs is becoming increasingly apparent withindustrial globalization, yet OELs set in variousregions and jurisdictions are often different. In thereview by Haber and Maier (2002) the need forharmonization, using mining and metal compoundsas case studies, was addressed. Four reasons forharmonization were identified, as follows.
• Increased transparency of health-based OELs, clarifying their uses and limitations
• Enhanced confidence in the process used to derive OELs by communicating key scientific criteria
• Pooling of resources among OEL setting bodies, increasing coverage of substances with no OEL, decreasing time to update OELs
• Increased provision for similar levels of worker health protection globally by increasing consistency in scientific criteria used as basis for deriving OELs
Clearly, there may be many other benefits ofharmonizing activities in the setting of OELs, butthe above are considered to represent a goodstarting list.
Haber and Maier (2002) reviewed the differentapproaches to, for example, uncertainty factors andcarcinogenicity used by the ACGIH, DECOS and theDFG, for chromium and its compounds, and forcopper, lead, manganese and silica. As a result,they made the following recommendations tofacilitate harmonization.
64
6. A Harmonized Approach

The Setting and Use of Occupational Exposure Limits Current practice
• Improve transparency and completeness of OEL documentation and identify strengths and weaknesses
• Provide greater accessibility to grey literature• Increase dissemination/publication of studies
that evaluate several endpoints but find no effect• Develop approaches for characterizing the overall
confidence in OELs• Harmonize the consideration of severity in the
identification of the POD• Harmonize definition of minimum data set for
development of OEL• Harmonize approach for interspecies
extrapolation• Harmonize default uncertainty factors used in
developing OELs• Harmonize approach for consideration of
speciation and essentiality of metals
6.3 Good practice in identifying and handlinghazards
It is worth noting that OELs are only one tool thatcan be used to control exposure to hazardoussubstances in the workplace (see also 5.6.1) and,even then, they are only part of a broader controlframework that involves compliance with the OEL,by good practice and measurements and inspectionby regulators. The control banding approach tocontrolling exposure to chemicals, currently beingdeveloped, shifts the paradigm towards morecontrol by following good practice with less relianceupon OELs and occupational hygiene measurement.Nonetheless, it is recognized that soundly basedand well respected OELs will continue to be animportant and fundamental cornerstone of goodoccupational hygiene control of occupationally-used substances.
6.4 Recommendations for harmonization
6.4.1 Reviewing the literature
As currently practiced between some standardsetting bodies (e.g. Lundberg, 1991), although on a limited basis, the production of reviews of theliterature on scientific data as backgrounddocumentation for setting OELs, including data onphysicochemical properties, occupational hygienedata, toxicological and mechanistic data and humanhealth data, could be a shared activity, with onereview produced for and used by all organizationssetting OELs. Such reviews could be evaluated andadopted on behalf of all standard setting bodies byan independent expert group.
Whether or not such an approach to produce singlereview documents is appropriate, or would becurrently acceptable, reviews of scientific datapertinent to setting OELs should all be prepared toa set of agreed basic criteria for inclusion andanalysis of data and studies, such as the criteriaadopted in the EU (CEC, 1992).
All such background documentation should also beevaluated, whether by an independent expert groupacting for all or several standard setting bodies orby individual standard setting bodies, according topredefined and consistent criteria, and all reviewsthat underpin OELs should be in the public domain.
The background documentation should clearlyidentify all elements of the process of evaluatingthe scientific literature and should identify keyhealth impacts for setting OELs and/or determiningthat no health-based OEL can be set (e.g. forsubstances with an effect for which no thresholdcan be reliably identified) and key studies to beused in setting OELs for threshold substances.
The process to set an OEL must be efficient. Ideally an OEL review, including a literature reviewand preparation of a report, peer review by thescientific community and consideration by thesocial partners and regulators, should becompleted within one year.
One advantage of establishing a centralized expertgroup to oversee and evaluate collation and reviewof data pertinent to setting OELs would be moretimely evaluations of new OELs and re-evaluationsof existing OELs than are currently possible. This would be even better facilitated if a centralizedfinancial resource could be made available for suchactivities.
65

The Setting and Use of Occupational Exposure Limits Current practice
6.4.2 Risk assessment
An evaluation of the pertinent scientific datashould, therefore, result in the identification ofcritical health effects and key studies for thedevelopment of OELs.
Where uncertainty factors are then applied indeveloping OELs, these should be clearlydescribed. As has been recommended (RiskAssessment and Toxicology Steering Committee,1999a), although uncertainty factors are oftenpresented as single numbers, scientific and non-scientific influences on decisions about uncertaintyfactors should be clearly described when chemicalrisk assessments are made publicly available.Transparency would be improved if individualcomponents of a composite risk factor were to beclearly identified.
All non health-based influences that impact on theOEL should also be described, such as issues oftechnical feasibility and socioeconomic benefit and risk.
All elements of the decision making process shouldbe documented and, as with the backgroundscientific review, all documentation, including thefinally adopted OELs, should be readily available inthe public domain.
Where appropriate all documentation, including the initial literature review, should be publishedtogether.
6.5 Proposed code of practice for settingoccupational exposure limits
• Literature review of relevant scientific data according to standardized criteria
• Evaluation of literature review according to standardized criteria
• Selection of critical health endpoint(s)• Determination of whether critical effects are
threshold/non-threshold • Selection of key studies for OEL• Selection of POD• Selection of factors influencing uncertainty• Application of individual uncertainty factors to
each such influencing factor• Determination of composite uncertainty factor• Identification of non-scientific influences on
development of OEL• OEL• Discussion on the availability and accuracy of
sampling technology• Documentation and publication of all key steps,
above
Proposals put forward, separately, by ICMMmember companies can be found in Annex 2.
66

AnnexesAnnex 1 Case Studies 68Annex 2Industry Proposal for Harmonization in Setting OELs 79

The Setting and Use of Occupational Exposure Limits Current practice
A comparison of OELs and how they were set forselected case studies of compounds that areparticularly relevant to the metals and miningindustry is presented in Tables A1–A9.
68
Annex 1 Case Studies
AbbreviationsACGIH American Conference of Governmental Industrial Hygienists BATBiological Tolerance ValueBEI Biological Exposure IndicesCNICentral Nervous SystemDECOS Dutch Expert Committee on Occupational Standards DFG Deutsche Forshungsgemeinschaft EUEuropean UnionHBR-OELHealth Based Recommended Occupational Exposure Level HSEHealth and Safety ExecutiveLOAELLowest Observed Adverse Effect LevelMAKMaximale ArbeitsplatzkonzentrationenMELMaximum Exposure LimitMOAELMinimal Observed Adverse Effect LevelNOAELNo Observed Adverse Effect Level OELOccupational Exposure LimitOESOccupational Exposure StandardPNSPeripheral Nervous SystemSCOEL Scientific Committee on Occupational Exposure LimitsSTEL Short Term Exposure Limit TLVThreshold Limit ValueTWATime Weighted Average

The Setting and Use of Occupational Exposure Limits Current practice 69
Table A1.1: Nickel metal
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
No recommendation
No MAK set
HBR-OEL, 8-h TWA, 0.05 15-min TWA, 0.1
MEL, 8-h TWA, 0.5(HSE, 2002)
8-h TWA, 1.5 (I)(ACGIH, 2003a)
Key study/Critical effect
Sensitization, cancer (keystudies not provided)
Dermatitis,pneumoconiosis
Risk assessment process
Uncertainly factor: nonestated
NOAEL not identified but0.004 mg/m3 producedminimal effects in animals
In vitro evidence forclastogenicity
Comments
On priority list but norecommendation to date
Has been evaluated but noMAK value assignedbecause classified as acarcinogen
Fertility anddevelopmental toxicitypublication but HBR-OELpublication in Dutch
Published basis for thisOEL lacking transparency
Insufficient data torecommend a STEL or‘Skin’ or ‘Sensitization’notations; TLV-TWAexpressed as inhalablenickel particulate ratherthan ‘total’ nickelparticulate as it is arespiratory hazard

The Setting and Use of Occupational Exposure Limits Current practice70
Table A1.2: Nickel sulphate
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
No recommendation
No MAK set
HBR-OEL, 8-h TWA, 0.05 15-min TWA, 0.1
MEL, 8-h TWA, 0.1(HSE, 2002)
8-h TWA, 0.1 (I)(ACGIH, 2003a)
Key study/Critical effect
Sensitization, cancer (key studies not cited inrationale)
NTP Studies in rats andmice identified pulmonarydamage, CNS, irritation,dermatitis as the criticaleffects (NTP, 1996a;1996b; 1996c)
Risk assessment process
Uncertainty factor: nonestated
NOAEL not identified but0.004 mg/m3 producedminimal effects in animals.
In vitro evidence forclastogenicity
Uncertainty factor: Nonestated
Evidence for inflammatorychanges in rats and mice at0.06 and 0.11 mg/m3; noevidence for carcinogenicityvia inhalation of nickelsulphate
Comments
On priority list but norecommendation to date
Has been evaluated but no MAK value assignedbecause classified as acarcinogen
Fertility anddevelopmental toxicitypublication but HBR-OELpublication in Dutch
Published rationale forthis OEL lackingtransparency
TLV-TWA expressed asinhalable nickelparticulate rather than‘total’ nickel particulatebecause of the associationbetween nickel exposureand sinus cancer

The Setting and Use of Occupational Exposure Limits Current practice 71
Table A2: Palladium metal and salts
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
No recommendation
No MAK value
No HBR-OEL
No OEL
No TVL
Key study/Critical effect Risk assessment process Comments

The Setting and Use of Occupational Exposure Limits Current practice72
Table A3: Lead metal
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
8-h TWA, 0.1
Biological limit value,30 µg/dl (EC, 2002)
No value set
HBR-OEL, 8-h TWA, 0.06 for men and 0.04 for women
8-h TWA, 0.15 No STEL
Biological limits forworkers, 50 µg/dl, 25 µg/dl for womenof reproductive age,40 µg/dl for child <18 y (HSE, 2001;2003)
8-h TWA, 0.05 BEI, 30 µg/dl at non-critical sampling time
Women of child-bearing age at risk ifblood-lead exceeds 10 µg/dl(ACGIH, 2003a)
Key study/Critical effect
CNS, PNS, kidney(Kentner and Fischer,1993; Lai et al., 1997)
N/A
Anaemia, nervous systemeffects and kidney damage(key studies not cited)
CNS, blood, kidney;reproductive effects (keystudies not cited in theTLV recommendation)
Risk assessment process
Uncertainty factor: nonestated
Based on the LOAEL forneurobehavioural effects of40 µg/dl; assumption thatavoiding CNS effects willprotect against other toxiceffects on the PNS andkidneys (including renalcancer); no NOAEL can bederived using availabledata
Uncertainty factor: N/A
Based on potentialcarcinogenic effects
Uncertainty factor: Nonestated
Based on critical healtheffects observed as blood-lead concentrations
Uncertainty factor: nonestated
Based on critical healtheffects observed as blood-lead concentrations
Comments
Other routes of exposurecontribute to blood-leadand so lead is moredifficult to set an OEL forthan other substances
Minimize exposure ofwomen at childbearingage to lead
Published rationale
HBR-OEL evaluation(1980) in Dutch
Lead has its own Controlof Lead at WorkRegulations (1998) andtherefore is not regulatedby COSHH (2002)
Blood lead concentrationrather than air leadconcentration is theprincipal method ofmonitoring lead exposurein the workplace; allsources of lead-exposureare therefore covered
Lead has A3 notation,Confirmed AnimalCarcinogen with UnknownRelevance to Humans butinsufficient information torecommend ‘Skin’ or‘Sensitization’ notations

The Setting and Use of Occupational Exposure Limits Current practice 73
Table A4: Chromium
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
No recommendation
Cr: No valueCrIII: No valueCrVI: (sol and insol)No value
Cr: No value
CrIII: 8-h TWA, 0.06
CrIV: 8-h TWA, 0.05
CrVI (sol and insol): No value
Cr and CrIII:OES, 8-h TWA, 0.5
CrVI:MEL, 8-h TWA, 0.05(HSE, 2002)
Cr and CrIII:8-h TWA, 0.5
CrVI (sol): 8-h TWA 0.05
CrVI (insol): 8-h TWA 0.01 (ACGIH,2003a)
CrVI (urine): BEI increase,(end shift) 10 µg/l,(endweek) 30 µg/l(ACGIH, 2004a)
Key study/Critical effect
Cancer
Lung toxicity (Johanssonet al., 1987)
Lung toxicity (Lee et al.,1989)
Lung Cancer
Ulceration, sensitization,cancer (key studies notcited)
Irritation, dermatitis(Fregert and Horsman,1964; Henderson, 1979;Johansson, 1986a; 1986b;Johansson et al., 1987)
Liver, kidney, respiratory(Laskin et al., 1969)
Cancer, irritation (Machleand Gregorius, 1948;WHO, 1988; ATSDR, 1989;HSE, 1989; IARC, 1990)
Risk assessment process
Uncertainty factor: N/A
No HBR-OEL due to lack ofdata
MOAEL and uncertaintyfactor (x10)
NOAEL and uncertaintyfactor (x10)
No HBR-OEL becausegenotoxic carcinogen
Uncertainty factor: nonestated
No NOAEL could beidentified; basis for limitunclear
Uncertainty factor: nonestated
Cr metal TLV based onhistorical limit; LOAEL forCrIII salts 0.5 mg/m3
(ACGIH, 2003a)
Comments
Unpublished riskassessment approach
Based on cancerclassification and lack ofthreshold effects
The Netherlands has 8-hor 15-min TWA MaximalAccepted Concentration(MAC) OELs for Cr and allCr compounds despite thelack of DECOS HBR-OELs(Dutch Expert Committeeon OccupationalStandards, 1992)
No published rationale forCr metal and CrIII
Rationale lackingtransparency; substanceswere not distinguishedbetween solubility on thebasis that it would beimpracticable todistinguish them inpractice (HSE, 2001)
A1 notation, confirmedHuman Carcinogen’ forCrVI (sol and insol)

The Setting and Use of Occupational Exposure Limits Current practice74
Table A5: Manganese
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
No recommendation
MAK, 8-h TWA, 0.5
BAT (blood, endshift(s)), 20 µg/l(DFG, 2004)
No HBR-OEL set
MEL, 8-h TWA, 0.5(HSE, 2003)
TLV, 8-h TWA, 0.2(ACGIH, 2003a)
Key study/Critical effect
CNS effects (Roels et al.,1987b; Iregren, 1990;Wennberg et al., 1991;1992; Mergler et al., 1994)
CNS effects (manganism),lung toxicity (Lauwerys etal., 1985; 1987a; Roels etal., 1992), reproductiveeffects (Lauwerys et al.,1985)
Risk assessment process
No uncertainty factors used
LOAEL 0.25 mg/m3
observed from criticalstudies in Swedenequivalent to 0.5 mg/m3
using dust monitoringequipment in Germany
Uncertainty factor: nonestated
LOAEL unknown; OELbased on evidence for aworsening of pre-clinicalneurological symptomsafter exposure ends
Comments
No ‘Sensitization’ notation
Effects on reproduction —publication but no OELrecommendation;currently underevaluation
No published rationaleavailable since thealteration of an OES to anMEL
Insufficient data torecommend ‘Skin’,‘Sensitization’ or‘Carcinogenicity’ notations

The Setting and Use of Occupational Exposure Limits Current practice 75
Table A6: Nitrogen dioxide
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
No recommendation
No MAK value
8-h TWA, 0.415-min STEL, 1.0(Dutch ExpertCommittee onOccupationalStandards, 2004)
OES, 8-h TWA, 5.7(withdrawn)OES, 15-min STEL,9.6 (withdrawn) (HSE, 2003)
8-h TWA, (3 ppm) 5.715-min STEL, (5 ppm) 9.6 (ACGIH, 2003a)
Key study/Critical effect
Pulmonary effects,fibrosis (Kubota et al.,1987; Miller et al., 1987;Frampton et al., 1991)
Irritation, pulmonaryoedema (Wagner et al.,1965; Freeman et al., 1966;Kosmider et al., 1972)
Risk assessment process
No overall uncertaintyfactor used although theuse of uncertainty factorswas discussed
HBR-OEL based on animaldata due to a lack of humandata; NOAEL of 0.38 mg/m3
in animal studies wasrounded to 1 decimal placeto give the HBR-OEL
Uncertainty factor: nonestated
Comments
DFG evaluation andcategory 3B carcinogenbut no MAK value set
Transparent, robustrationale
A4 notation, notclassifiable as a HumanCarcinogen

The Setting and Use of Occupational Exposure Limits Current practice76
Table A7: Sulphur dioxide
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
No recommendation
MAK, 1.3 (DFG, 2004)
15-min STEL, 0.7(Dutch ExpertCommittee onOccupationalStandards, 2003b)
OES, 8-h TWA, 5.3(withdrawn)OES, 15-min STEL, 13(withdrawn) (HSE, 2003)
8-h TWA, 2 ppm 15-min STEL, 5 ppm(ACGIH, 2003a)
Key study/Critical effect
Lung function (Broder etal., 1989; Kremer et al.,1994; Kremer et al., 1995)
Respiratory irritation(Stacy et al., 1983;Schachter et al., 1984)
Respiratory irritation,bronchoconstriction(Speizer and Frank, 1966;DHEW, 1969; Amdur, 1969)
Risk assessment process
Uncertainty factor of 3 usedto account for intraspeciesdifferences (Islam et al.,1992; Islam et al., 1994)
NOAEL of 2 mg/m3 forshort-term exposure anduncertainty factor used toderive STEL
Uncertainty factor: nonestated
Based onbronchoconstriction at 5 ppm
Comments
Category 3B carcinogen
No ‘Skin’ or ‘Sensitization’notation
DECOS recognizes needfor 8-h TWA HBR-OEL butinsufficient data for longterm exposure
A4 notation, notClassifiable as a HumanCarcinogen (Laskin et al.,1976)

The Setting and Use of Occupational Exposure Limits Current practice 77
Table A8: Sulphuric acid mists
* mg/m3 unless otherwise stated** Desirable but suitable measurement technique currently not available
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
8-hTWA, 0.0515-min STEL, 0.1**(proposed; SCOEL,2005)
MAK, 8-h TWA, 0.1(DFG, 2004)
No HBR-OEL set
OES, 8-h TWA, 1(withdrawn)(HSE, 2003)
TLV, 8-h TWA, 0.2(ACGIH, 2004b)
Risk assessment process
Uncertainty factor of 3 usedto extrapolate effects tolong-term exposures(Greim, 2001)
LOAEL 0.3 mg/m3;laryngeal cancer assumedto be caused by severelocal irritation because ofabsence of genotoxiceffects (Greim, 2001)
EU category 1, carcinogenicto humans
Uncertainty factor: nonestated
Comments
Unpublished
Category 4 carcinogen; no‘Sensitization’ or ‘Skin’notation (Greim, 2001)
Classified as carcinogenicbut no HBR-OELevaluation available
A2 notation, suspectedHuman Carcinogen
Key study/Critical effect
Irritancy, laryngeal cancer
Decreased mucociliaryclearance, lung function(key studies not cited)
Cancer
Changes in mucociliaryclearance (Leikauf et al.,1981; Lippmann et al.,1982; Leikauf et al., 1984;Lippmann et al., 1987;Spektor et al., 1989) andpulmonary function(Koenig et al., 1985; Utellet al., 1989)

Table A9: Silica (crystalline)
* mg/m3 unless otherwise stated
Country/Region
EU SCOEL
German DFG
The NetherlandsDECOS
UK HSE
USA ACGIH
OEL mg/m3*
No recommendation
No MAK set (DFG, 2004)
HBR-OEL, 8h-TWA, 0.075(respirable quartz,cristobalite andtridymite)
MEL, 8-h TWA, 0.3(HSE, 2002)Proposed WEL, 8-h TWA, 0.1
TLV, 0.05 (respirablequartz, cristobaliteand tridymite; ACGIH,2003a)
Key study/Critical effect
Nine key cohort studies(Cherry et al., 1988;Costello and Graham,1988; Guènel et al., 1989;Merlo et al., 1991; Chen etal., 1992; Costello et al.,1995; Dong et al., 1995;Checkoway et al., 1997)critical effects weresilicosis, lung cancer
Silicosis and lung cancer(Costello and Graham,1988; Guènel et al., 1989)
Silicosis (key studies notcited; HSE, 2001)
Lung fibrosis, silicosis,cancer (Hnizdo and Sluis-Cremer, 1993; Hnizdo etal., 1993)
Risk assessment process
Uncertainty factor: N/A
Silica was evaluated but noMAK value assignedbecause classified inCarcinogen category 1(Greim, 2000)
Limit based on the NOAELfor silicosis followingexposure to respirablequartz
Uncertainty factor: noneused
Uncertainty factor: nonestated
No NOAEL established;MEL based on levelreasonably practicable byindustry
Concern for role of fibrosisas a risk factor for lungcancer prompted ACGIH toreduce TLV from 0.1 to 0.05mg/m3
Comments
DFG recommendpreventing silicosis toreduce cancer risk basedon increased incidence oflung cancer in workerswith silicosis
A2 notation, suspectedHuman Carcinogen; anotice of intent to lowerthe TLV further to 0.025mg/m3
The Setting and Use of Occupational Exposure Limits Current practice78
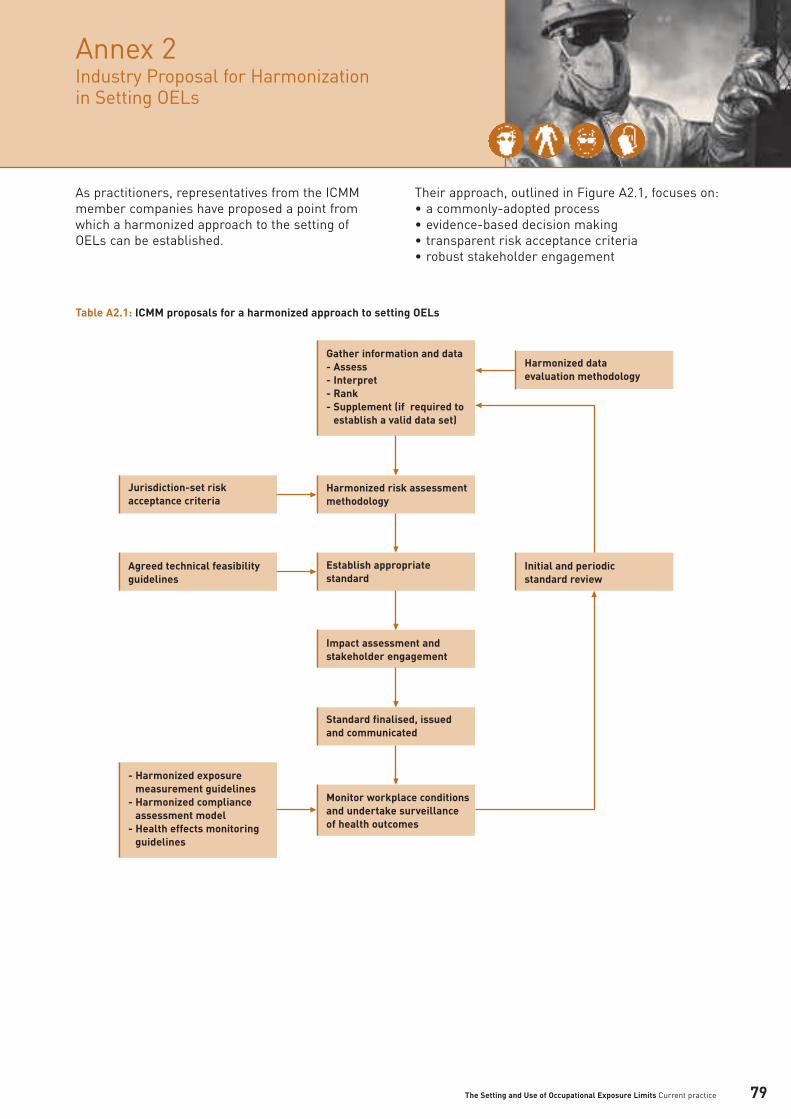
As practitioners, representatives from the ICMMmember companies have proposed a point fromwhich a harmonized approach to the setting ofOELs can be established.
Their approach, outlined in Figure A2.1, focuses on:• a commonly-adopted process• evidence-based decision making• transparent risk acceptance criteria• robust stakeholder engagement
Annex 2 Industry Proposal for Harmonization in Setting OELs
The Setting and Use of Occupational Exposure Limits Current practice 79
Table A2.1: ICMM proposals for a harmonized approach to setting OELs
Gather information and data- Assess- Interpret- Rank- Supplement (if required to
establish a valid data set)
- Harmonized exposure measurement guidelines
- Harmonized compliance assessment model
- Health effects monitoring guidelines
Harmonized risk assessmentmethodology
Jurisdiction-set riskacceptance criteria
Establish appropriatestandard
Agreed technical feasibilityguidelines
Initial and periodicstandard review
Harmonized dataevaluation methodology
Impact assessment andstakeholder engagement
Standard finalised, issuedand communicated
Monitor workplace conditionsand undertake surveillanceof health outcomes

The Setting and Use of Occupational Exposure Limits Current practice80
The approach seeks to achieve harmonization andagreement for the science-based elements of OELsetting, such as the collection and evaluation ofdata, and provides OEL-setting organizations withthe opportunity to apply risk acceptance criteriaconsistent with their respective community norms.
Specific elements of the model relate to:
Harmonized data evaluation methodologyA proposal to develop and agree a systematicmethodology by which data and evidence can beevaluated, assessed and agreed.
Harmonized risk assessment methodologyA proposal to establish, through wide stakeholderengagement a standardized approach toundertaking risk assessments on exposures andhealth effects.
Jurisdiction-set risk acceptance criteriaRecognition that risk acceptance criteria will varybetween national and community groupsdependent on their cultural acceptance of risks.
Agreed technical feasibility guidelinesRecognition that current scientific methods limitthe lower levels of detectablity of agents in theworkplace.
Impact assessment and stakeholder engagementRecognition that the impacts, costs and benefits ofchanged exposure standards need to be understoodand that a wide range of stakeholders need to beengaged.
Exposure measurement and compliance guidelinesA proposal to establish and agree guidelines toensure that all stakeholders understand howexposures are to be measured and compliance is tobe assessed.
Periodic reviews of OELsRecognition that reviews or changes to existingOELs need to follow the same harmonizedapproach and should consider the results ofworker health surveillance where available.

ReferencesWeb publications 92

The Setting and Use of Occupational Exposure Limits Current practice
ACGIH (2003a) 2003 TLVs and BEIs®
Based on the Documentation of the ThresholdValues for Chemical and Physical Agents andBiological Exposure Indices. American Conference of Governmental IndustrialHygienists, Cincinnati OH, USA.
ACGIH (2003b) Documentation of the Threshold Limit Values andBiological Exposure Indices (Seventh Edition).American Conference of Governmental IndustrialHygienists, Cincinnati OH, USA.
ACGIH (2004a) Chromium (VI), Water-Soluble Fume.American Conference of Governmental IndustrialHygienists, Cincinnati OH, USA.
ACGIH (2004b) Sulfuric Acid.American Conference of Governmental IndustrialHygienists, Cincinnati OH, USA.
Amdur, M.O. (1969) Toxicological appraisal of particulate matter,oxides of sulfur and sulfuric acid.J Air Pollut Control Assoc, 19, 638-646.
Arbetslivsinstitutet (2000) Scientific Basis for Swedish OccupationalStandards XXI.National Institute for Working Life, Stockholm,Sweden.
ATSDR (1989) Toxicological Profile for Chromium.(ATSDR/TP-88/10).Agency for Toxic Substances and Disease Registry,US Department of Health and Human Services,Research Triangle Park, USA.
Blaauboer, B.J. (2003) The integration of data on physico-chemicalproperties, in vitro-derived toxicity data andphysiologically based kinetic and dynamic asmodelling a tool in hazard and risk assessment - acommentary.Toxicol Letts, 138, 161-171.
Brief, R.S. and Scala, R.A. (1975) Occupational exposure limits for novel workschedules.Am Ind Hyg Assoc J, 36, 467-469.
Broder, .I, Smith, J.W., Corey, P. and Holness, L. (1989) Health status and sulfur dioxide exposure of nickelsmelter workers and civic laborers.J Occup Med, 31, 347-353.
CEC (1992) Occupational Exposure Limits Criteria Documents:Guidance Note on the Content and Layout.(EUR 13776). Office for Official Publications of theEuropean Communities, Luxembourg.
CEC (1999) Methodology for the Derivation of OccupationalExposure Limits: Key Documentation.(EUR 19253 EN). Commission of the EuropeanCommunities, Brussels, Belgium.
Checkoway, H., Heyer, N.J., Seixas, N.S., Welp,E.A.E., Demers, P.A., Hughes, J.M. and Weill, H. (1997) Dose-response associations of silica withnonmalignant respiratory disease and lung cancermortality in the diatomaceous earth industry.Am J Epidemiol, 145, 680-688.
Chen, J., McLaughlin, J.K., Zhang, J.Y., Stone, B.J.,Luo, J., Chen, R.A., Dosemeci, M., Rexing, S.H., Wu, Z., Haerl, F.J., McCrawley, M.A. and Blot, W.J. (1992) Mortality among dust-exposed Chinese mine andpottery workers.J Occup Med, 34, 311-316.
Cherry, N.M., Burgess, G.L., Turner, S. andMcDonald, J.C. (1988) Crystalline silica and risk of lung cancer in thepotteries. Occup Environ Med, 55, 779-785.
Cook, W.A. (1986) Occupational Exposure Limits-Worldwide.American Journal of the Hygiene Association, Ohio, USA.
Costello. J., Castellan, R.M., Swecker, G.S. andKullman, G.J. (1995) Mortality of a cohort of U.S. workers employed inthe crushed stone industry.Am J Ind Med, 27, 625-640.
Costello, J. and Graham, W.G.B. (1988) Vermont granite worker’s mortality study. Am J Ind Med, 13, 483-497.
82
References

The Setting and Use of Occupational Exposure Limits Current practice
COT (2002) Risk Assessment of Mixtures of Pesticides andSimilar Substances. (Report of the Committee on Toxicity of Chemicalsin Food, Consumer Products and the Environment).Food Standards Agency, London, UK.
Dalton, P. (2001) Evaluating the human response to sensoryirritation: Implications for setting occupationalexposure limits.Am Ind Hyg Assoc J, 62, 723-729.
DFG (2004) List of MAK and BAT Values 2004 (40). Wiley-VCH, Weinheim, Germany.
DFG (2005a) Nitrogen dioxide. In: Occupational Toxicants and MAK Values, Volume 21 (English translation available online). Wiley-VCH, Weinheim, Germany.
DFG (2005b) Occupational Toxicants and MAK Values, Volume 21.(English translation available online). Wiley-VCH, Weinheim, Germany.
DFG (2005c) Sulphur dioxide. In: Occupational Toxicants and MAK Values,Volume 22. (English translation available online, in press). Wiley-VCH, Weinheim, Germany.
DH (1995) Policy Appraisal and Health. Department of Health, London, UK.
DHEW (1969) Air Quality Criteria for Sulfur Oxides. U.S. Department of Health, Education and Welfare,Washington DC, USA.
Dong, D., Xu, G., Sun, Y. and Hu, P. (1995) Lung cancer among workers exposed to silica dustin Chinese refractory plants.Scand J Work Environ Health, 21, 69-72.
Dutch Expert Committee on OccupationalStandards (1992) Health-Based Recommended OccupationalExposure Limits for Chrystalline Forms of SiliconDioxide (Free Silica) (RA 5/92). Dutch Expert Committee on OccupationalStandards, The Hague, Netherlands.
Dutch Expert Committee on OccupationalStandards (1998) Quartz: Evaluation of Carcinogenicity andGenotoxicity.(Publication No. 1998/02 WGD). Health Council of the Netherlands(Gezondheidsraad), The Hague, Netherlands.
Dutch Expert Committee on OccupationalStandards (2000) Health-based Reassessment of AdministrativeOccupational Exposure Limits, (2000/15OSH). Health Council of the Netherlands(Gezondheidsraad), The Hague, Netherlands.Available [October 2004] at; www.gr.nl/pdf.php?ID=45
Dutch Expert Committee on OccupationalStandards (2003a) Strong Inorganic Acid Mists Containing SulphuricAcid. (2003/07OSH). Health Council of the Netherlands(Gezondheidsraad), The Hague, Netherlands.
Dutch Expert Committee on OccupationalStandards (2003b) Sulphur Dioxide. (2003/08OSH). Health Council of the Netherlands(Gezondheidsraad), The Hague, Netherlands.www.gr.nl/pdf.php?ID=876
Dutch Expert Committee on OccupationalStandards (2004) Nitrogen Dioxide. (2004/01OSH). Health Council of the Netherlands(Gezondheidsraad), The Hague, Netherlands.www.gr.nl/pdf.php?ID=900
EC (2002) Lead and its Inorganic Compounds.(SCOEL/SUM/83 Final). Scientific Committtee onOccupational Exposure Limits (SCOEL), Luxemborg.
ECETOC (1984) Considerations Regarding the Extrapolation ofBiological Data in Deriving Occupational ExposureLimits. (Report No.10). Ecology and Toxicology Centre,European Chemical Industry, Brussels, Belgium.
83

The Setting and Use of Occupational Exposure Limits Current practice
Fairhurst, S. (1995) The uncertainty factor in the setting of occupationalexposure standards. Ann Occup Hyg, 39, 375-385, (English.)
Finley, B., Proctor, D., Scott, P., Harrington, N.,Paustenbach, D. and Price, P. (1994) Recommended distributions for exposure factorsfrequently used in health risk assessment. Risk Anal, 14, 533-553.
Frampton, M.W., Morrow, P.E., Cox, C., Gibb, F.R.and Speers, D.M. (1991) Effect of nitrogen dioxide exposure on pulmonaryfunction and airway reactivity in normal subjects.Am Rev Resp Dis, 142, 522-527.
Freeman, G., Furiosi, N.J. and Haydon, G.B. (1966) Effects of continuous exposure of 0.8 ppm NO2 onrespiration of rats. Arch Environ Health, 13, 454-456.
Freeman, G., Stephens, R.J., Crane, S.C. andFuriosi, N.J. (1968) Lesion of the lung in rats continously exposed totwo parts per million of nitrogen dioxide. Arch Environ Health, 17, 181-192.
Fregert, S. and Horsman, H. (1964) Allergy to trivalent chromium. Arch Dermatol, 90, 4-6.
Gibbs, J.P., Crump, K.S., Houck, D.P., Warren, P.A.and Mosley, W.S. (1999) Focused medical surveillance: A search forsubclinical movement disorders in a cohort of U.S.workers exposed to low levels of manganese dust.Neurotoxicology, 20, 299-314.
Greim, H. (1996) Chromium(VI) compounds. In: Occupational Toxicants, Volume 7, Critical Datafor Evaluation of MAK Values and Classification ofCarcinogens. Wiley, London, UK. 33-35.
Greim, H. (1999) Manganese and its inorganic compounds.In: Occupational Toxicants, Volume 14, Critical Datafor Evaluation of MAK Values and Classification ofCarcinogens. Wiley, London, UK. 293-328.
Greim, H. (2000) Silica, crystalline: Quartz dust, cristobalite dustand tridymite dust (respirable fraction). In: Occupational Toxicants, Volume 14, Critical Datafor Evaluation of MAK Values and Classification ofCarcinogens.Wiley, London, UK. 205-271.
Greim, H. (2001) Sulfuric acid. In: Occupational Toxicants, Volume 15, Critical Datafor Evaluation of MAK Values and Classification ofCarcinogens.Wiley, London, UK. 165-222.
Guènel, P., Hojberg, G. and Lynge, E. (1989) Cancer incidence among Danish stone workers.Scand J Work Environ Health, 15, 265-270.
Haber, L.T. and Maier, A. (2002) Scientific criteria used for the development ofoccupational exposure limits for metals and othermining-related chemicals. Regul Toxicol Pharmacol, 36, 262-279.
Health and Safety Commission (1999) Approved Guide to the Classification and Labellingof Substances and Preparations Dangerous forSupply.HSE Books, Sudbury, UK.
Henderson, R.F. (1979) Early damage indicators in the lung. III.Biochemical and cytological response of the lung toinhaled metal salts.Toxicol Appl Pharmacol, 50, 123-135.
Hester, R.E. and Harrison, R.M. (Eds.) (1998) Risk Assessment and Risk Management.Royal Society of Chemistry, Cambridge, UK.
Hickey, J.L.S. and Reist, P.C. (1977) Application of occupational exposure limits tounusual work schedules. Am Ind Hyg Assoc J, 38, 613-62.1
Hnizdo, E., Murray, J., Sluis-Cremer, G.K. andThomas, R.G. (1993) Correlation between radiological and pathologicaldiagnosis of silicosis: An autopsy population basedstudy. Am J Ind Med, 24, 427-445.
84

The Setting and Use of Occupational Exposure Limits Current practice
Hnizdo, E. and Sluis-Cremer, G.K. (1993) Risk of silicosis in a cohort of white South Africangold miners. Am J Ind Med, 24, 447-457.
HSC (2003) Proposals to Introduce a New OccupationalExposure Limits (OEL) Framework.(Consultation Document 198). Sudbury, UK, HSE Books. Available [November 2004] at;www.hse.gov.uk/consult/condocs/cd189.htm
HSC (2005a) Annex 2 - Explanatory Note-Cost BenefitAssessment Methodology for Regulatory ImpactAssessment and Application to OccupationalExposure Limits: An Overview. In: Control of Substances Hazardous to HealthRegulations 2002, Proposals for New MaximumExposure Limits (Consultative Document). HSE Books, Sudbury, UK.
HSC (2005b) Annex 3 - Summary of the regulatory impactassessment (RIA) for respirable crystalline silica.In: Proposal for a Workplace Exposure Limit forRespirable Crystalline Silica. HSE Books, Sudbury, UK. 1-9.
HSC (2005) Proposal for a Workplace Exposure Limit forRespirable Crystalline Silica. (Consultation Document). HSE Books, Sudbury, UK.
HSE (1989) The Toxicity of Chromium and InorganicChromium. (Toxicity Review 21). Health and Safety Executive, London, UK.
HSE (2000) General Methods for the Sampling and GravimetricAnalysis of Respirable and Total Inhalable Dust.(Methods of the Determination of HazardousSubstances (MHDS) 14/3). HSE Books, Sudbury, UK.
HSE (2001) EH64 Summary Criteria for Occupational ExposureLimits. HSE Books, Sudbury, UK.
HSE (2002) Occupational Exposure Limits 2002. (EH40/2002). HSE Books, Sudbury, UK.
HSE (2003) EH40/2002 Occupational Exposure Limits:Supplement 2003. HSE Books, Sudbury, Suffolk.
HSE (2005a) A Regulatory Impact Assessment (RIA) onProposals to Reduce the UK OccupationalExposure Limit for Respirable Crystalline Silica(RCS) - draft for consultation. (Consultative Document).HSE Books, Sudbury, UK.
HSE (2005b) EH40/2005 Workplace Exposure Limits. HSE Books, Sudbury, Suffolk.
Hunter, W.C. and Roberts, J.M. (1933) Experimental study of the effects of potassiumbichromate on the monkey’s kidney. Am J Pathol, 9, 133-147.
IARC (1990) IARC Monographs on Evaluation of CarcinogenicRisks of Chemicals to Humans. Vol 49, Chromium, Nickel and Welding.International Agency for Research on Cancer, Lyon, France.
IARC (1992a) Mechanisms of Carcinogenesis in RiskIdentification. (IARC Scientific Publication 116).International Agency for Research on Cancer (IARC),Lyon, France.
IARC (1992b) IARC Monographs on Evaluation of CarcinogenicRisks to Humans.Vol 54, Occupational Exposures to Mists, Vapoursfrom Strong Inorganic Acids and Other IndustrialChemicals.International Agency for Cancer Research, Lyon,France.
85

The Setting and Use of Occupational Exposure Limits Current practice
IARC (1997) IARC Monographs on Evaluation of CarcinogenicRisks to Humans. Vol 68, Silica, Silicates, Coal Dust and Para-AramidFibrils.The International Agency for Cancer Research,Lyon, France,
IEH (2002) IEH Report on Variability and Susceptibility inHuman Response to Occupational Exposure toChemicals in the UK. (Report R13). MRC Institute for Environment and Health,Leicester, UK.
IEH (2004) Occupational Exposure Limits: Criteria Documentfor Manganese and Inorganic ManganeseCompounds. (Web Report W17). MRC Institute for Environment and Health,Leicester, UK.
IGHRC (2003) Uncertainty Factors: Their Use in Human HealthRisk Assessment by UK Government (CR9). MRC Institute for Environment and Health,Leicester, UK.
IGHRC (2004) Guidelines for Good Exposure Practice for HumanHealth Effects of Chemicals (CR10). MRC Institute for Environment and Health,Leicester, UK.
Iregren, A. (1990) Psychological test performance in foundry workersexposed to low levels of manganese.Neurotoxicol Teratol, 12, 673-675.
Islam, M.S., Neuhann, H.F., Grzegowski, E. andOberbarnscheidt, J. (1992) Bronchomotoric effect of low concentration ofsulphur dioxide in young healthy volunteers. Fres Environ Bull, 1, 541-546.
Islam, M.S., Oberbarnscheidt, J. and Schlipköter,H.W. (1994) Non-specific responsiveness to hyperventilation oflow doses of sulfur dioxide and cols air of non-smoking healthy volunteers of different ages.Zbl Hyg, 195, 556-566
ISO (1995) ISO 7708: Air Quality - Particle Size FractionDefinitions for Health-Related Sampling.International Organization for Standardization,Geneva, Switzerland.
Jefferson, T., Demichel, V. and Mugford, M. (1996)Elementary Economic Evaluation in Health Care.BMJ Publishing Group, London, UK.
Johansson, A. (1986a) Rabbit alveolar macrophages after inhalation ofhexa- and trivalent chromium.Environ Res, 39, 372-385.
Johansson, A. (1986b) Rabbit lung after inhalation of hexa- and trivalentchromium. Environ Res, 41, 110-119.
Johansson, A., Robertson, B. and Curstedt, T. (1987)Alveolar macrophage abnormalities in rabbitsexposed to low concentrations of trivalentchromium. Environ Res, 44, 279-293.
Kentner, M. and Fischer, T. (1993) Biomonitoring bei beruflicher Bleibelastung -Untersuchungen zur Belastungs- undBeanspruchungssituation an 134 Beschäftigteneiner Akkumulatorenfertigung in Zeitraum von1982 bis 1991.Berufsgenossenschaft der Feinmechanik undElektrotechnik, Köln, Germany.
Klerk, N.H., Ambrosini, G.L. and Musk, A.W. (2002)A Review of the Australian Occupational ExposureStandard for Crystalline Silica.University of Western Australia, Australia.
Koenig, J.Q., Morgan, M.S., Horike, M. and Pierson, W.E. (1985) The effects of sulfur oxides on nasal and lungfunction in adolescents with extrinsic asthma. J Allergy Clin Immunol, 76, 813-818.
Kosmider, V.S., Ludyga, K. and Misiewicz, A. (1972)Experimentelle und klinische untersuchungen uberemphysembilden de wirkung der stickstoffoxyde. Zentralbl Arbeitsmed, 22, 362-368.
86
The Setting and Use of Occupational Exposure Limits Current practice
Kremer, A.M., Pal, T.M., Boleji, B., Schouten, J.P.and Rijcken, B. (1994) Airway hyperresponsiveness, prevalence of chronicrespiratory symptoms, and lung function inworkers exposed to irritants. Occup Environ Med, 51, 3-13.
Kremer, A.M., Pal, T.M., Schouten, J.P. and Rijcken, B. (1995) Airway hyperresponsiveness in workers exposed tolow levels of irritants. Eur Respir J, 8, 53-61.
Kubota, K., Murakami, M., Takenaka, S., Kawai, K.and Kyouo, H. (1987) Effects of long -term nitrogen dioxide exposure onrat lung: Morphological observations. Environ Health Perspect, 73, 157-169.
Lai, J.S., Wu, T.N., Liou, S.H., Shen, C.Y., Guu, C.F.,Ko, K.N., Chi, H.Y. and Chang, P.Y. (1997) A study of the relationship between ambient leadand blood lead among lead battery workers. Int Arch Occup Environ Health, 69, 295-300.
Langård, S. (1990) One hundred years of chromium and cancer: Areview of epidemiological evidence and selectedcase reports. Am J Ind Med, 17, 189-215.
Laskin, S., Kuschner, M. and Drew, R.T. (1969)Studies in pulmonary carcinogenesis.In: Hanna, M.G., Nettesheim, P. and Gilbert, J.R., (Eds.)Inhalation Carcinogenesis, pp 321-351. Atomic Energy Commission, Oak Ridge TN, USA.
Laskin, S., Kuschner, M. and Sellakumar, A. (1976)Combined carcinogen-irritant animal inhalationstudies.In: Aharonson, E.F., Ben-David, A. and Klingberg,M.A., (Eds.) Air Pollution and the Lung. p -190.John Wiley and Sons, New York, USA.
Lauwerys, R., Roels, H. and Genet, P. (1985) Fertility of male workers exposed to mercury vaporor manganese dust: A questionnaire study. Am J Ind Med, 7, 171-176.
Lee, K.P., Ulrich, C.E. and Geil, R.G. (1989) Inhalation toxicity of chromium dioxide dust to ratsafter two years exposure.Sci Total Environ, 86, 83-108.
Leikauf, G., Yeates, D.B. and Wales, K.A. (1981) Effects of sulfuric acid aerosol on respiratorymechanics and mucocillary particle clearance inhealthy nonsmoking. Am Ind Hyg Assoc J, 42, 273-281.
Leikauf, G.D., Spektor, D.M. and Albert, R.E. (1984) Dose-dependent effects of submicrometer sulfuricacid aerosol on particle clearance from ciliatedhuman lung airways. Am Ind Hyg Assoc J, 45, 285-292.
Leung, H-W., Murray, F.J. and Paustenbach, D.J. (1988) A proposed occupational exposure limit for 2,3,7,8-tetrachlorodibenzo-p-dioxin. Am Ind Hyg Assoc J, 49, 466-474.
Leung, H-W. and Paustenbach, D. (1998) Setting occupational exposure limits for irritantorganic acids and bases based on their equilibriumdissociation constants. Appl Ind Hyg, 3, 115-118.
Lippmann, M., Gearheart, J.M. and Schlesinger, R.B. (1987) Basis for particle size-selective tlv for sulfuric acidaerosols. Appl Ind Hyg, 2, 188-199.
Lippmann, M., Schlesinger, R.B. and Leikauf, G. (1982) Effects of sulfuric acid aerosols on respiratorytract airways. Ann Occup Hyg, 26, 677-690.
Lundberg, P. (1991) The Nordic Expert Group, an inter-Nordic projectfor assessment of occupational risks. Sci Total Environ, 101, 17-24.
Machle, W. and Gregorius, F. (1948) Cancer of the respiratory system in the U.S.chromate producing industry.Public Health Reps, 63, 1114-1127.
Major, R.H. (1922) Studies on a case of chromic acid nephritis.John Hopkins Hospital Bulletin, 33, 56-61.
87

The Setting and Use of Occupational Exposure Limits Current practice
Mancuso, T.F. (1975)Consideration of chromium as an industrialcarcinogen. In: International Conference of Heavy Metals in theEnvironment. pp 343-356.Toronto, Canada.
Meldrum, M. (2001) Setting occupational exposure limits for sensoryirritants: The approach in the European Union. Am Ind Hyg Assoc J, 62, 730-732.
Mergler, D., Huel, G., Bowler, R., Iregren, A.,Belanger, S., Baldwin, M., Tardif, R., Smargiassi, A.and Martin, L. (1994) Nervous system dysfunction among workers withlong-term exposure to manganese. Environ Res, 64, 151-180.
Merlo, F., Constantine, M., Reggiardo, G., Ceppi, M.and Puntoni, R. (1991) Lung cancer risk in refractory brick workersexposed to crystalline silica: A retrospective cohortstudy. Epidemiology, 2, 299-305.
Miller, F.J., Graham, J.A., Raub, J.A. and Illing, J.W. (1987) Evaluating the toxicity of urban patterns of oxidantgases. II. Effects in mice form chronic exposure tonitrogen dioxide.J Toxicol Environ Health, 21, 99-112.
Mulhausen, J.R. and Damiano, J. (1998) A Strategy for Assessing and ManagingOccupational Exposures. American Industrial Hygiene Association Press,Fairfax, USA.
Myers, J.E., teWaterNaude, J.M., Abie Zogoe, H.B.,Fourie, M., Naik, I., Theodorou, P., Tassell, H., Daya,A. and Thompson, M. (2002) Two Phase Longitudinal or Prospective Study of theNervous System Effects of OccupationalEnvironmental Exposures on Mineworkers orProcessing Plant Workers at Two ManganeseMines.Safety in Mines Research Advisory Committee(SIMRAC), Capetown, South Africa.
NOHSC (1999) National Hazardous Substances RegulatoryPackage. Substances Subject to Limitations onExposure (National Exposure Standards). Policiesfor Maintenance and Improvement. National Occupational Health and SafetyCommission, Australia.www.nohsc.gov.au/OHSLegalObligations/HazSubstancesAndDngGoods/NES/exposurestandards
NTP (1996a) Toxicology and Carcinogenesis Studies of NickelOxide in F344/N Rats and B6C3F1 Mice (InhalationStudies). (Technical Report Series No. 451, DHHS (NIH) Pub No.94-3363).National Toxicology Program, Research TrianglePark NC, USA.
NTP (1996b) Toxicology and Carcinogenesis Studies of NickelSubsulfide in F344/N Rats and B6C3F1 Mice(Inhalation Studies). (Technical Report Series No. 453, DHHS (NIH) Pub No.94-3369). National Toxicology Program, Research TrianglePark NC, USA.
NTP (1996c) Toxicology and Carcinogenesis Studies of NickelSulfate Hexahydrate in F344/N Rats and B6C3F1Mice (Inhalation Studies).(Technical Report Series No. 454, DHHS (NIH) Pub No.94-3370). National Toxicology Program, Research TrianglePark NC, USA.
OECD (2000) OECD Guidelines for the Testing of Chemicals (uptoand including Thirteenth Addendum): Volumes 1and 2.Organization for Economic Co-operation andDevelopment, Paris, France.
Paustenbach, D. (2001) Approaches and considerations for settingoccupational exposure limits for sensory irritants:Report of recent symposia. Am Ind Hyg Assoc J, 62, 697-704.
88

The Setting and Use of Occupational Exposure Limits Current practice
Paustenbach, D., Alarie, Y., Kulle, T., Schachter, N.,Smith, R., Swenberg, J., Witschi, H. and Horowitz, S.B. (1997) A recommended occupational exposure limit forformaldehyde based on irritation. J Toxicol Environ Health, 50, 217-263.
Paustenbach, D. and Langner, R. (1986) Corporate occupational exposure limits: Thecurrent state of affairs. Am Ind Hyg Assoc J, 47, 809-818.
Paustenbach, D.J. (1985) Occupational exposure limits, pharmacokinetics,and unusual work schedules. In: Patty’s Industrial Hygiene and Toxicology,Volume 3.John Wiley and Sons, London, UK. 111-277.
Paustenbach, D.J. (2000) The history and biological basis of occupationalexposure limits for chemical agents. In: Harris, R. (Ed.) Patty’s Industrial Hygiene and Toxicology.John Wiley and Sons, New York, USA. 1903-2000.
Paustenbach, D.J. (2003) Health risk assessment and practice of industrialhygiene. In: Perkins, J.L. (Ed.) Modern Industrial Hygiene, Volume 2.Lee Hung Scientific Pte Ltd, USA.
Paustenbach, D.J., Madl, A.K. and Greene, J.F. (2001) Identifying an appropriate occupational exposurelimit (OEL) for beryllium: Data gaps and currentresearch initiatives. Appl Occup Environ Hyg, 16, 527-538.
Pocock, S.J., Collier, T.J., Dandreo, K.J., de Stavola,B.L., Goldman, M.B., Kalish, L.A., Kasten, L.E. andMcCormack, V.A. (2004) Issues in the reporting of epidemiological studies:A survey of recent practice.Br Med J, 329, 883-888.
Proctor, D.M., Panko, J.P., Liebig, E.W. andPaustenbach, D.J. (2004) Estimating historical occupational exposure toairborne hexavalent chromium in a chromateproduction plant: 1940-1972. J Occup Environ Hyg, 1, 752-767.
Rappaport, S.M. (1991a) Assessment of long-term exposure to toxicsubstances in air. Ann Occup Hyg, 35, 61-121.
Rappaport, S.M. (1991b) Selection of the measures of exposure forepidemiology studies. Appl Occup Environ Hyg, 6, 448-457.
Rappaport, S.M. (1993) Threshold limit values, permissible exposurelimits, and feasibility: The bases for exposure limitsin the United States. Am J Ind Med, 23, 683-694.
Rappaport, S.M., Kromhout, H. and Symanski, E. (1993) Variation of exposure between workers inhomogeneous exposure groups. Am Ind Hyg Assoc J, 54, 654-662.
Rappaport, S.M., Kupper, L.L. and Lin, Y.S. (2005) On the importance of exposure variability to thedoses of volatile organic compounds. Toxicol Sci, 83, 224-236.
Rappaport, S.M., Lyles, R.H. and Kupper, L.L. (1995) An exposure-assessment strategy accounting forwithin- and between-worker sources of variability.Ann Occup Hyg, 39, 469-495.
Rappaport, S.M., Tomero-Velez, R., Symanski, E.,Kromhout, H. and Yu, R.C. (1998) Response to Paul Hewett’s “comments relating toTornero-Velez et al.: Compliance versus risk inassessing occupational exposures”. Risk Anal, 18, 669-671.
Remaeus, B. (2001) Occupational exposure limits in Sweden -socioeconomic and technological aspects.In: Occupational Exposure Limits - Approaches andCriteria. Proceedings from a NIVA Course Held in Uppsala,Sweden, 24-28 September 2001. National Institute for Working Life, Sweden. 41-46.
Risk Assessment and Toxicology SteeringCommittee (1999a) From Risk Assessment to Risk Management:Dealing with Uncertainty. (cr6). Institute for Environment and Health, Leicester, UK.
89

The Setting and Use of Occupational Exposure Limits Current practice
Risk Assessment and Toxicology SteeringCommittee (1999b) Physiologically-based Pharmacokinetic Modelling:A Potential Tool for Use in Risk Assessment. (cr4).Institute for Environment and Health, Leicester, UK.
Risk Assessment and Toxicology SteeringCommittee (1999c) Risk Assessment Approaches used by Governmentfor Evaluating Human Health Effects of Chemicals.(cr2).Institute for Environment and Health, Leicester, UK.
RIU (2003) A Quick Guide To Regulatory Impact Assessment.Regulatory Impact Unit, Cabinet Office, London, UK.Available [January 2005] at;www.cabinetoffice.gov.uk/regulation/docs/ria/pdf/ria_quick_guide.pdf
Roels, H., Ghyselen, P. and Buchet, J.P. (1992)Assessment of the permissible exposure level tomanganese in workers exposed to manganesedioxide dust. Br J Ind Med, 49, 25-34.
Roels, H., Lauwerys, R. and Buchet, J.P. (1987a)Epidemiological survey among workers exposed tomanganese: Effects on lung, central nervoussystem, and some biological indices. Am J Ind Med, 11, 307-327.
Roels, H., Lauwerys, R., Genet, P., Sarhan, M.J., de Fays, M., Hanotiau, I. and Buchet, J.P. (1987b)Relationship between external and internalparameters of exposure to manganese in workersfrom a manganese oxide and salt producing plant.Am J Ind Med, 11, 297-305.
Schachter, E.N., Witek, T.J. and Beck, G.J. (1984) Airway effects of low concentrations of sulfurdioxide: Dose-response characteristics. Arch Environ Health, 39, 34-42.
Schaper, M. (1993) Development of a database for sensory irritantsand its use in establishing occupational exposurelimits. Am Ind Hyg Assoc J, 54, 488-544.
Schmid, G.P. (1995) Understanding the essentials of economic-evaluation. J AID, 10, S6-S13.
SCOEL (2005) Recommendation of the Scientific Committee onOccupational Exposure Limits for Sulphuric Acid. (SCOEL/SUM/105 revised final - In Press). Health, Security and Hygiene Unit, EuropeanCommission, Luxembourg.
Smith, J.S. and Mendeloff, J.M. (1999) A quantitative analysis of factors affecting PELsand TLVs for carcinogens.Risk Anal, 19, 1223-1234.
Smith, T.J. (1987) Exposure assessment for occupationalepidemiology.Am J Ind Med, 12, 249-268.
Speizer, F.E. and Frank, N.R. (1966) The uptake and release of SO2 by the human nose.Arch Environ Health, 12, 725-728.
Spektor, D.M., Yen, B.M. and Lippmann, M. (1989)Effect of concentration and cumulative exposure toinhaled sulfuric acid on tracheobronchial particleclearance in healthy humans. Environ Health Perspect, 79, 167-172.
Stacy, R.W., Seal, E.J., House, D.E., Green, J.,Roger, L.J. and Raggio, L. (1983) A survey of effects of gaseous and aerosolpollutants on pulmonary function of normal males.Arch Environ Health, 38, 104-115.
Stokinger, H.E. (1970) Criteria and procedures for assessing the toxicresponses to industrial chemicals. In: Permissible Levels of Toxic Substances in theWorking Environment. World Health Organization, Geneva, Switzerland.
Stokinger, H.E. (1981) Threshold Limit Values: Part 1.In: Dangerous Properties of Industrial MaterialsReport.Wiley-Interscience, UK. 8-13.
Sweeney, L.M., Tyler, T.R., Kirman, C.R., Corley,R.A., Reitz, R.H., Paustenbach, D.J., Holson, J.F.,Whorton, M.D., Thompson, K.M. and Gargas, M.L. (2001) Proposed occupational exposure limits for selectethylene glycol ethers using PBPK models andMonte Carlo simulations. Toxicol Sci, 62, 124-139.
90

The Setting and Use of Occupational Exposure Limits Current practice
Symanski, E. and Rappaport, S.M. (1994) An investigation of the dependence of exposurevariability on the interval between measurements.Ann Occup Hyg, 38, 361-372.
The Presidential/Congressional Commission onRisk Assessmemt and Risk Management (1997) Risk Assessment and Risk Management inRegulatory Decision Making. (Final Report).The Presidental/Congressional Commission onRisk Assessment and Risk Management,Washington DC, USA.
Tornero-Velez, R., Symanski, E., Kromhout, H., Yu, R.C. and Rappaport, S.M. (1997) Compliance versus risk in assessing occupationalexposures. Risk Anal, 17, 279-292.
Triebig, G. (2002)Chemosensory irritation and the setting ofoccupational exposure limits.Int Arch Occup Environ Health, 75, 281-282,(English. 5 BIZZ)
Ulfvarson, U. (1987) Assessment of concentration peaks in settingexposure limits for air contaminants atworkplaces, with special emphasis on narcotic and irritative gases and vapors.Scand J Work Environ Health, 13, 389-398.
Utell, M.J., Mariglio, J.A. and Morrow, P.E. (1989) Effects of inhaled acid aerosols on respiratoryfunction: The role of endogenous ammonia.J Aerosol Med, 2, 141-147.
Wagner, W.D., Duncan, B.R., Wright, P.G. andStokinger, H.E. (1965) Experimental study of threshold limit of NO2.Arch Environ Health, 10, 455-466.
Walters, D., Grodzki, K. and Walters, S. (2003) The Role of Occupational Exposure Limits in theHealth and Safety Systems of EU Member States.HSE Books, Sudbury, UK. Available [November 2004] at;www.hse.gov.uk/research/rrhtm/rr172.htm
Weaver, M.A., Kupper, L.L., Taylor, D., Kromhout, H., Susi, P. and Rappaport, S.M. (2001) Simultaneous assessment of occupationalexposures from multiple worker groups. Ann Occup Hyg, 45, 525-542.
Wennberg, A., Hagman, M. and Johansson, L. (1992)Preclinical neurophysiological signs ofparkinsonism in occupational manganeseexposure. Neurotoxicology, 13, 271-274.
Wennberg, A., Iregren, A., Struwe, G., Cizinsky, G.,Hagman, M. and Johansson, L. (1991) Manganese exposure in steel smelters, a healthhazard to the nervous system. Scand J Work Environ Health, 17, 255-262.
WHO (1988) Chromium.(International Program on Chemical Safety,Environmental Health Criteria, 61). World Health Organization, Geneva, Switzerland.
WHO (1994) Assessing the Human Health Risks of Chemicals:Derivation of Guidance Values for Health-BasedExposure Limits.(International Program on Chemical Safety,Environmental Health Criteria 170).World Health Organization, Geneva, Switzerland.
WHO (2000) Evaluation and Use of Epidemiological Evidence forEnvironmental Health Risk Assessment. GuidelineDocument. World Health Organization, Regional Office forEurope, Copenhagen, Denmark. www.euro.who.int/document/e68940.pdf
WHO (2002) Palladium. (International Program on Chemical Safety,Environmental Health Criteria, 226).World Health Organization, Geneva, Switzerland.Available [January 2005] at;www.inchem.org/documents/ehc/ehc/ehc226.htm
Williams, P.R.D. and Paustenbach, D.J. (2003)Reconstruction of benzene exposure for thepliofilm cohort (1936-1976) using Monte Carlotechniques. J Toxicol Environ Health, 66, 677-781.
Yanagida, H., Dai, Q. and Yanagisawa, Y. (2005)Methodology for predicting OEL from rodent LD50
values for metals and metallic compounds. Environ Sci Technol, 39, 371-376.
91

The Setting and Use of Occupational Exposure Limits Current practice
1EU-OSHA Network (1998–2005) Dangerous Substances Occupational ExposureLimits. Available [October 2004] athttp://europe.osha.eu.int/good_practice/risks/ds/oel
2NOHSC Guidance Note on the Interpretation ofExposure Standards for Atmospheric Contaminantsin the Occupational Environment.[NOHSC:3008(1995)] 3rd Edition (Updated forAmendments). Available [January 2005] atwww.nohsc.gov.au/OHSInformation/NOHSCPublications/fulltext/toc/H3-34.htm
3EEC (1967) Council Directive 67/548/EEC of 27 June 1967 onthe approximation of laws, regulations andadministrative provisions relating to theclassification, packaging and labelling ofdangerous substances.Official Journal, 196, 0001–0098. Available [June 2005] athttp://europa.eu.int/smartapi/cgi/sga_doc?smartapi!celexapi!prod!CELEXnumdoc&lg=en&numdoc=31967L0548&model=guichett
4OECD Good Laboratory Practice.Available [January 2005] atwww.oecd.org/about/0,2337,en_2649_34381_1_1_1_1_1,00.html
5STROBE (2004) STROBE Statement. Available [November 2004] atwww.strobe-statement.org/1513.html
6NIOSH (1994) Manual of Analytical Methods.(NMAM) Fourth Edition. Available [December 2004] atwww.cdc.gov/niosh/nmam/pdfs/7300.pdf
7NIOSH (1994) Manual of Analytical Methods.(NMAM) Fourth Edition. Available [December 2004] atwww.cdc.gov/niosh/nmam/pdfs/7024.pdf
8NIOSH (1994) Manual of Analytical Methods.(NMAM) Fourth Edition. Available [December 2004] atwww.cdc.gov/niosh/nmam/pdfs/7600.pdf
9NIOSH (1994) Manual of Analytical Methods. (NMAM) Fourth Edition. Available [December 2004] atwww.cdc.gov/niosh/nmam/pdfs/6014-1.pdf
10NIOSH (1994) Manual of Analytical Methods.(NMAM) Fourth Edition. Available [December 2004] atwww.cdc.gov/niosh/nmam/pdfs/6004.pdf
11NIOSH (1994) Manual of Analytical Methods. (NMAM) Fourth Edition. Available [December 2004] atwww.cdc.gov/niosh/nmam/pdfs/7903.pdf
12NIOSH (1994) Manual of Analytical Methods. (NMAM) Fourth Edition. Available [December 2004] atwww.cdc.gov/niosh/nmam/pdfs/7601.pdf; www.cdc.gov/niosh/nmam/pdfs/7500.pdf;www.cdc.gov/niosh/nmam/pdfs/7602.pdf
13EPA (2000) Science Policy Council Handbook: RiskCharacterization.US Environmental Protection Agency. Available [May 2005] athttp://epa.gov/osa/spc/htm/rchandbk.pdf
92
Web publications

The Setting and Use of Occupational Exposure Limits Current practice
14Summary of SCOEL recommendations 2002-1997.European Commission, Scientific Publications. Available [January 2005] athttp://europa.eu.int/comm/employment_social/ealth_safety/publicat/pubsci1_en.htm
15NOHSC (2004) Hazardous Substances Information System.Available [January 2005] atwww.nohsc.gov.au/applications/hsis/
16AIHA Publications Available [May 2005] atwww.sheilapantry.com/safchemhaz/books/aihatitles.htm#1931504601
17AIHA (2002) AIHA’s White Paper on Permissible Exposure Limits (PELs).Available [May 2005] atwww.aiha.org/GovernmentAffairs-PR/html/GAWPpermexpo.htm
18ACT (2004) Proposals to introduce a new WEL for Silica.Available [March 2005] at www.hse.gov.uk/aboutus/hsc/iacs/acts/251104/paper35.pdf
19COSHH (2002) Statutory Instrument 2002 No. 2677 The Control ofSubstances Hazardous to Health Regulations 2002.Available [March 2005] atwww.hmso.gov.uk/si/si2002/20022677.htm;
COSHH (2004) Statutory Instrument 2004 No. 3386 The Control ofSubstances Hazardous to Health (Amendment)Regulations 2004. Available [March 2005] atwww.legislation.hmso.gov.uk/si/si2004/20043386.htm
20EEC (1989) Council Directive of 12 June 1989 on the introductionof measures to encourage improvements in thesafety and health of workers at work (89/391/EEC).Official Journal, L 183, 1. Available [June 2005] at http://europa.eu.int/eur-lex/lex/LexUriServ/LexUriServ.do?uri=CELEX:31989L0391:EN:HTML
21ILO (1996–2005) SafeWork Chemical Control Banding.International Labour Organization.Available atwww.ilo.org/public/english/protection/safework/ctrl_banding/
22HSE COSHH Essentials. Health and Safety Executive. Available [March 2005] atwww.coshh-essentials.org.uk/
23WebElements Essential information on palladium. Available [January 2005] atwww.webelements.com/webelements/elements/text/Pd/key.html
24The Radiochemistry of Palladium Available [March 2005] at www.radiochemistry.org/periodictable/pdf_books/pdf/rc000009.pdf
25Proposals to Withdraw Nine Occupational ExposureStandards (OESs).Available [March 2005] atwww.hse.gov.uk/aboutus/hsc/meetings/2003/080403/c46.pdf
26TOXNET Hazardous Substances Database (HSDB).Available [January 2005] athttp://toxnet.nlm.nih.gov/cgi-bin/sis/search/f?./temp/~sjg9st:1
93

The Setting and Use of Occupational Exposure Limits Current practice
27HSE (2003) Chemical Hazard Alert Notice 35 - RespirableCrystalline Silica. Available [December 2004] at www/hse.gov.uk/pubns/chan35.htm
28IfADo (2004) Evaluation of chemosensory effects due to occupational exposures.Available [May 2005] atwww.ifado.de/de/aktivitaeten/tagungen/infospeaker.php
94

The Setting and Use of Occupational Exposure Limits Current practice 95
Notes

This is a report by the Institute of Environment andHealth (IEH) for the International Council on Miningand Metals. The IEH was established at CranfieldUniversity in November 2005. The research andconsultancy activities of the institute are principallyfunded through specific grants, contracts and awardsby UK Government Departments and Agencies.
The ICMM OELs Working Group is thanked for itsreview of the publication and its contribution to thisstage of ICMM’s goal of achieving a HarmonizedApproach to Setting Occupational Exposure Limits.
Institute of Environment and HealthCranfield UniversitySilsoe Bedfordshire MK45 4DT
www.silsoe.cranfield.ac.uk/ieh/
The views expressed in this publication do notnecessarily reflect those of ICMM.
Published by ICMM, London, UK.
©2007, the International Council on Mining andMetals
Reproduction of this publication for educational orother non-commercial purposes is authorizedwithout prior written permission from the copyrightholders provided the source is fully acknowledged.Reproduction of this publication for resale or othercommercial purposes is prohibited without priorwritten permission of the copyright holders.
ICMM (2007). The Setting and Use of OccupationalExposure Limits: Current practice
ISBN: 978-0-9553591-2-5
Written by: Linda Shuker, Kathryn James, Joe Massey and Len LevyDesign: DuoPrint: Quadracolor Limited
Available online and in hard copy from ICMM,www.icmm.com, [email protected]
This book is printed on Challenger Offset 250gsmand 120gsm. The paper is made from ECF(Elemental Chlorine Free) wood pulps, acquiredfrom sustainable forest reserves, and is fullyrecyclable with no harmful residue. Accordant toEMAS and ISO 14001 the international standardthat specifies a process for controlling andimproving a companies environmental performance.
The Setting and Use of Occupational Exposure Limits Current practice96
Acknowledgements


Email: [email protected] [email protected]
www.icmm.com
ICMM – The International Council on Mining and Metals
The International Council on Mining and Metals (ICMM) is a CEO-led organization comprising many of the world’s leading mining and metals companies as well as regional, national and commodity associations, all of which are committed to improving their sustainabledevelopment performance and to the responsibleproduction of the mineral and metal resources societyneeds.
ICMM’s vision is a viable mining, minerals and metalsindustry that is widely recognized as essential formodern living and a key contributor to sustainabledevelopment.
Our library at www.goodpracticemining.com has casestudies and other examples of leading practices.